Embed Size (px)
Citation preview

Acta Paediatr Suppl421:33-8. 1997
Role of placental cytokines and inflammation in vertical transmission of HIV infection WT Shearer’, J Reuben’, B-N Lee2, EJ Popek3, DE Lewis4, HH Hammill’, IC Hanson’, MW Kline’ and C Langston3 Departments .f Pediatrics‘, Patho10gy~~ Microbiology and Immunology4, and Obstetrics and Gynecology’, Baylor College of Medicine, Texas Children’s Hospital; and the Immunology Laboratory’, Universitj of Texas MD Anderson Cancer Center, Houston. ?x, USA
Shearer WT, Reuben J, Lee B-N, Popek El, Lewis DE, Hammill HH, Hanson IC, Kline MW, Langston C. Role of placental cytokines and inflammation in vertical transmission of HIV infection. Acta Prediatr 1997;Suppl421:33-8. Stockholm. ISSN 0803-5326
In light of new evidence suggesting that maternal human immunodeficiency virus (HIV) infection produces at least a three-fold increase in the number of early spontaneous abortions, it is important to search for factors that may predispose to fetal wastage. Immunological factors are thought to play an important role in permitting the HLA-disparate fetus to continue to term, despite powerful maternal immune forces capable of rejection. In the context of a heightened incidence of spontaneous abortion in HIV infection, evidence is now accumulating that implicates an imbalance in immune factors in contributing to this fetal loss. Soluble immune factors, such as cytokines, have been suggested as contributing agents to recurrent spontaneous abortions. Inflammatory cytokines-interleukin 1 f l , interleukin 6 and tumor necrosis factor alpha-have been measured in isolated placental trophoblastic cells in HIV-infected and non-infected pregnant women in an attempt to explore this hypothesis. These inflammatory cytokines and their messenger RNAs were significantly elevated before and after stimulation in HIV-infected women, supporting the belief that HIV- infected women present their fetuses a milieu of imbalanced immune factors capable of contributing to immunological rejection. In addition, these elevated inflammatory cytokine levels may contribute to HIV disease progression in fetuses by virtue of activation of HIV gene transcription factors similar to what has been demonstrated in in vitro systems. We therefore propose that HIV infection in pregnant women produces an altered state of certain soluble immune factors, which in concert with other immune factor abnormalities, such as loss of immune selection in the fetal thymus, predisposes the fetus to advanced HIV infection and possible spontaneous abortion. 0 Cytokines, HW, placenta, trophoblast
WTShearer, Department ofAllergy and Immunology, Texas Children’s Hospital, 6621. Fannin St., MC 1-3291, Houston, TX 77030, USA
The human placenta is thought to serve as an immuno- logical barrier, protecting the fetus from the mother’s immune system itself, HLA-haploidentical in most circum- stances. The factors responsible for this barrier effect of the placenta are incompletely understood, but are thought to include: (i) absence of a maternal cytotoxic T cell response to the fetus; (ii) resistance of natural killer cell activity; (iii) secretion of hormones and cytokines that are anti-inflam- matory and immunosuppressive; and (iv) expression of immunologically non-reactive HLA-G on fetal trophoblast cells (1). These protective factors are thought to play important roles in preventing HIV vertical transmission because several studies have documented a disturbance of maternal immunity during pregnancy that may facilitate HIV vertical transmission. Several investigations have documented a more rapid fall in CD4+ cells in HIV- infected women during pregnancy compared to the post- partum period, findings compounded by the changes in total lymphocyte count of normal pregnant women (2-5). A more recent study suggests that pregnancy causes more of a decrease in T-helper cell function (secretion of L-2) in HIV-infected women as compared to non-infected women
(6). Moreover, T-helper cell function returned towards normal more slowly in HIV-infected women after parturi- tion. Finally, there was much more of an alteration in the memory and naive T-cell sets of the blood in HIV-infected pregnant women as compared to non-infected pregnant women.
The mechanism whereby the HIV-infected mother infects her fetus is thought to be either by an infected maternal cell entering the fetal circulation or by direct maternal-to-fetal cell transfer of HIV. Maternal cell-free virus is thought to be capable of infecting the fetus. Factors capable of increasing maternal-to-fetal HIV transmission are thought to include maternal immunosuppression (7) and inflammation of placental membranes (8,9). Detection of latent HIV has been made in fetal tissues as early as 8 weeks of gestation (10). Cytokines are soluble substances secreted by immune cells that have the ability to upregulate HIV expression and production in latently infected cells (1 1). Tumor necrosis factor alpha (TNF-a), an inflamma- tory cytokine, has been shown to increase HIV production by activating the transcription factor IW-hm,B (NFkB) (12). Interleukin 6 (IL-6) causes chronically infected
6 Scandinavian University Press 1997. ISSN 0803-5326
34 WT Shearer et al. ACTA P&DIP.TR SUPPL J21 (1997)
immune cells to begin HIV production (1 3). The human placenta contains cells capable of producing cytokines that have a major impact on the length of pregnancy. It is well known that abnormal cytokine patterns exist in women with recurrent spontaneous abortions ( I 4). Thus, study of the human placenta with regard to specific cell-derived cytokine production might be of considerable interest in understanding how the placenta protects most infants from HIV vertical transmission.
Expression profiles of inflammatory cytokines in placental trophoblasts in HIV-infected pregnant women Placental trophoblastic cells are epithelial cells of fetal origin that resemble macrophages with respect to invasive behaviour, ability to form syncytia, expression of surface membrane CD14, F, receptors, cytokines and cytokine receptors (1 5). Moreover, placental trophoblasts secrete certain cytokines that have the potential to upregulate the expression and secretion of HIV in latently infected T cells and macrophages (1 6). For example, TNF-a and JL-6 have been shown to be capable of increasing HIV expression and production in chronically infected cell lines, possibly by activating transcription factors such as NFkB (17). To begin to assess the roles of inflammatory cytokines in transmission of HIV infection from mothers to their infants, we measured the in vitro production of TNF-a, IL-16 and IL-6 in placental trophoblastic cells harvested from placentas of HIV-infected and non-infected women (delivered at term) with and without stimulation by lipo- polysaccharide (LPS) (18). Also, we measured the expres- sion of mRNA for identical placental trophoblastic cell
cultures obtained from placentas of HIV-infected and non- infected women (1 8).
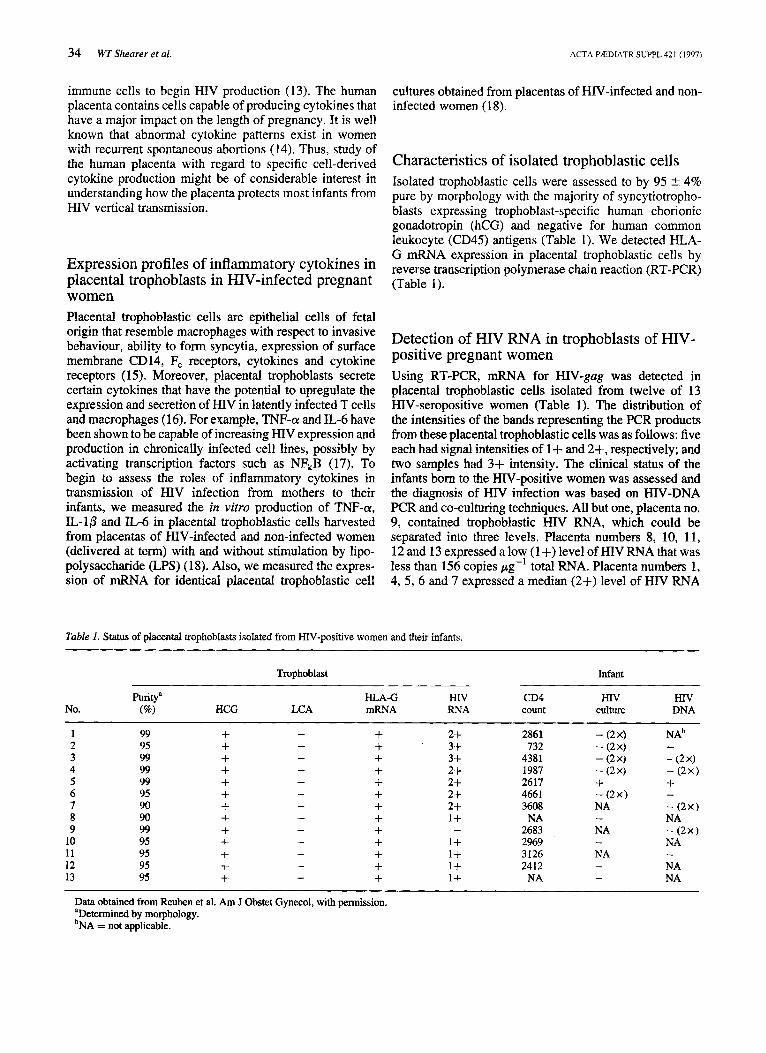
Characteristics of isolated trophoblastic cells Isolated trophoblastic cells were assessed to by 95 2 4% pure by morphology with the majority of syncytiotropho- blasts expressing trophoblast-specific human chorionic gonadotropin (hCG) and negative for human common leukocyte (CD45) antigens (Table 1). We detected HLA- G mRNA expression in placental trophoblastic cells by reverse transcription polymerase chain reaction (RT-PCR) (Table 1).
Detection of HIV RNA in trophoblasts of HIV- positive pregnant women Using RT-PCR, mRNA for HIV-gag was detected in placental trophoblastic cells isolated from twelve of 13 HIV-seropositive women (Table 1). The distribution of the intensities of the bands representing the PCR products from these placental trophoblastic cells was as follows: five each had signal intensities of 1+ and 2+, respectively; and two samples had 3+ intensity. The clinical status of the infants born to the HIV-positive women was assessed and the diagnosis of HIV infection was based on HN-DNA PCR and co-culturing techniques. All but one, placenta no. 9, contained trophoblastic HIV RNA, which could be separated into three levels. Placenta numbers 8, 10, 11 , 12 and 13 expressed a low (1 +) level of HIV RNA that was less than 156 copies pg-' total RNA. Placenta numbers 1, 4, 5, 6 and 7 expressed a median (2+) level of HIV RNA
Table 1. Status of placental trophoblasts isolated from HIV-positive women and their infants. ~ ~ ~ ~ ~ ~ ~ ~ ~~~
Trophoblast Infant
puritya €LA-G HIV CD4 HIV HN No. (Q1 HCG LCA mRNA RNA count culture DNA
1 99 + - + 2+ 2861 - (2x1 N A ~ 2 95 + + 3+ 732 - (2x1 3 99 + + 3+ 4381 - (2x1 - (2x1 4 99 + + 2+ 1987 - (2x1 - (2x1 5 99 + - + 2+ 2617 + + 6 95 + + 2+ 4661 - (2x) 7 90 + + 2+ 3608 NA - (2x) 8 90 + + 1+ NA - NA 9 99 + 2683 NA - (2X) +
10 95 + - + 1+ 2969 - NA 11 95 + - + I+ 3126 NA - 12 95 + - + 1+ 2412 - NA 13 95 + - + 1+ NA - NA
- - - -
- - - -
- -
Data obtained from Reuben et al. Am J Obstet Gynecol, with permission. aDetennined by morphology. bNA = not applicable.
ACTA PRDIATR SUPPLJZI (1997) Plucenrul cprokities and injlanitncirion in vertical HIV transmission 35
that was between 157 and 1000 copies pg-' total RNA. Placenta numbers 2 and 3 expressed the highest level (3+) of HIV RNA, which represented more than a 1000 copies pg-' total RNA.
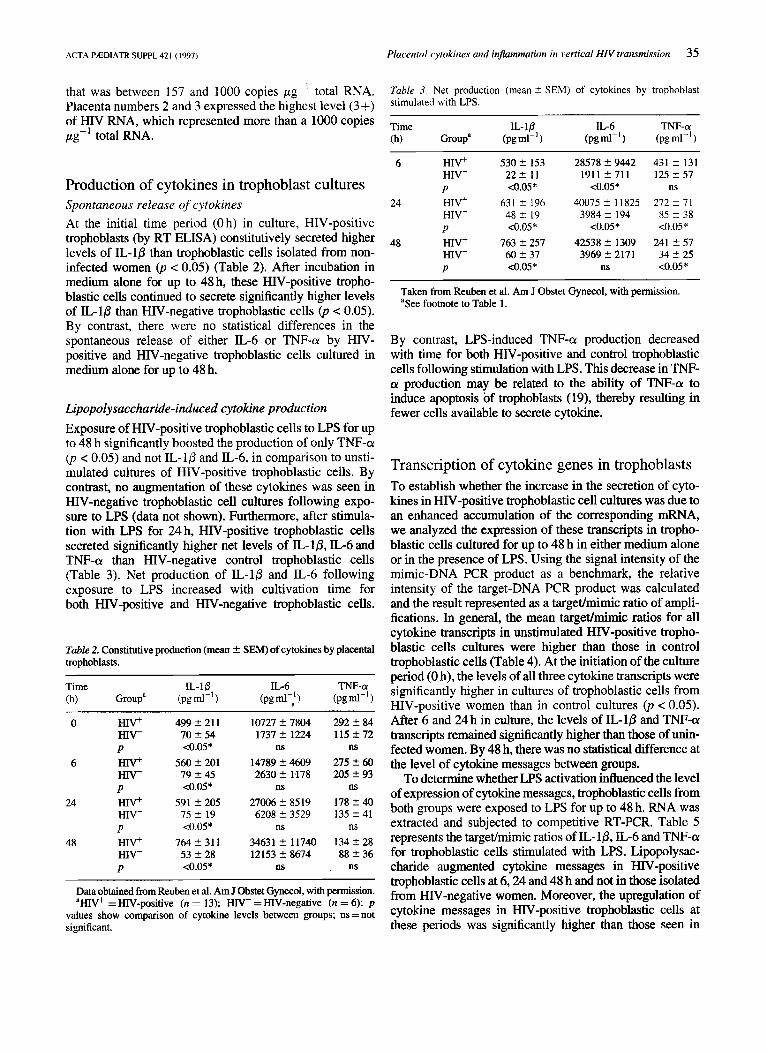
Table 3. Net production (mean 5 SEM) of cytokines by trophoblast stimulated with LPS.
Time IL-10 IL-6 TNF-a (h) Group' (pgml-I) (pg mi-' ) (pg m1-I )
Production of cytokines in trophoblast cultures Spontaneous release of cytokines At the initial time period (Oh) in culture, HIV-positive trophoblasts (by RT ELISA) constitutively secreted higher levels of IL-16 than trophoblastic cells isolated from non- infected women (p < 0.05) (Table 2). After incubation in medium alone for up to 48 h, these HIV-positive tropho- blastic cells continued to secrete significantly higher levels of IL-10 than HIV-negative trophoblastic cells (p < 0.05). By contrast, there were no statistical differences in the spontaneous release of either IL-6 or TNF-(r by HIV- positive and HIV-negative trophoblastic cells cultured in medium alone for up to 48 h.
Lipopolysaccharide-induced cytokine production Exposure of HIV-positive trophoblastic cells to LPS for up to 48 h significantly boosted the production of only TNF-a! 0) < 0.05) and not IL-16 and IL-6, in comparison to unsti- mulated cultures of HIV-positive trophoblastic cells. By contrast, no augmentation of these cytokines was seen in HIV-negative trophoblastic cell cultures following expo- sure to LPS (data not shown). Furthermore, after stimula- tion with LPS for 24 h, HIV-positive trophoblastic cells secreted significantly higher net levels of IL-lP, IL-6 and TNF-a than HIV-negative control trophoblastic cells (Table 3). Net production of IL-16 and IL-6 following exposure to LPS increased with cultivation time for both HIV-positive and HIV-negative trophoblastic cells.
Table 2. Constitutive production (mean ? SEM) of cytokines by placental trophoblasts.
~
0 HIV+
6 HN+
24 HIV+
48 HIV+
HIV- P
H N - P
HIV- P
HIV- P
499 5 211 70 -t- 54 <0.05*
560 t- 201 79 2 45 <0.05*
591 t- 205 75 5 19 <0.05*
764 2 311 53 2 28 <0.05*
10727 ? 7804 1737 2 1224
ns 14789 2 4609 2630 ? 1178
ns 27006 2 8519 6208 ? 3529
ns 34631 2 I1740 12153 2 8674
ns
292 ? 84 115 2 72
ns 275 2 60 205 ? 93
ns 178 ? 40 135 ? 41
ns 134 2 28 88 ? 36
. ns
Data obtained from Reuben et al. Am J Obstet Gynecol, with permission. 'HIV+ = HIV-positive (n = 13); HIV- = HIV-negative (n = 6); p
values show comparison of cytokine levels between groups; ns = not significant.
6 HIV+
24 HIV+
48 HIV+
HIV- P
HIV- P
HIV- P
530 ? 153 2 2 2 I I 4.05*
631 ? 196 4 8 2 19 <0.05*
763 2 257 60 2 37 <0.05*
28578 ? 9442 1911 2711
<0.05* 40075 ? 11 825
3984 ? 194 <0.05*
42538 2 1309 3969 ? 2171
ns
431 ? 131 125 5 57
ns 212 5 71
85 2 38 <0.05*
241 5 57 34 5 25 <0.05*
Taken from Reuben et al. Am J Obstet Gynecol, with permission. 'See footnote to Table 1.
By contrast, LPS-induced TNF-a! production decreased with time for both HIV-positive and control trophoblastic cells following stimulation with LPS. This decrease in TNF- a production may be related to the ability of TNF-a to induce apoptosis of trophoblasts (19), thereby resulting in fewer cells available to secrete cytokine.
Transcription of cytokine genes in trophoblasts To establish whether the increase in the secretion of cyto- kines in HIV-positive trophoblastic cell cultures was due to an enhanced accumulation of the corresponding mRNA, we analyzed the expression of these transcripts in tropho- blastic cells cultured for up to 48 h in either medium alone or in the presence of LPS. Using the signal intensity of the mimic-DNA PCR product as a benchmark, the relative intensity of the target-DNA PCR product was calculated and the result represented as a targetlmimic ratio of ampli- fications. In general, the mean target/mimic ratios for all cytokine transcripts in unstimulated HIV-positive tropho- blastic cells cultures were higher than those in control trophoblastic cells (Table 4). At the initiation of the culture period (0 h), the levels of all three cytokine transcripts were significantly higher in cultures of trophoblastic cells from HIV-positive women than in control cultures (p < 0.05). After 6 and 24 h in culture, the levels of IL-l/3 and TNF-a transcripts remained significantly higher than those of unin- fected women. By 48 h, there was no statistical difference at the level of cytokine messages between groups.
To determine whether LPS activation influenced the level of expression of cytokine messages, trophoblastic cells from both groups were exposed to LPS for up to 48 h. RNA was extracted and subjected to competitive RT-PCR. Table 5 represents the targetlmimic ratios of IL-16, IL-6 and TNF-a for trophoblastic cells stimulated with LPS. Lipopolysac- charide augmented cytokine messages in HIV-positive trophoblastic cells at 6,24 and 48 h and not in those isolated from HIV-negative women. Moreover, the upregulation of cytokine messages in HIV-positive trophoblastic cells at these periods was significantly higher than those seen in
36 WT Shearer et ul. ACTA PEEDIATK SUPPL421 (19971
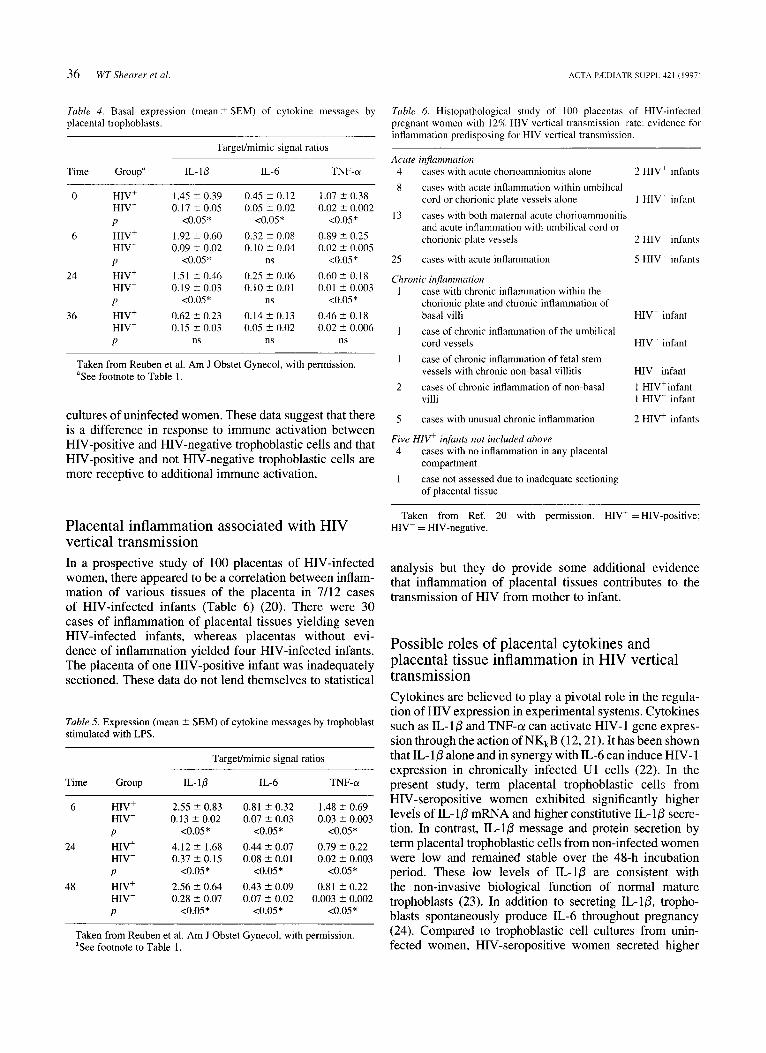
Tuble 4. Basal expression ( m e a n t SEM) of cytokine messages by placental trophoblasts.
Targeumimic signal ratios
Time Groupa IL- 1 p IL-6 TNF-ol
0 HIV+
6 HIV+
24 HIV+
36 HIV+
HIV- P
HIV- P
H I T P
HIV- P
1.45 2 0.39 0.17 ? 0.05
<0.05* 1.92 t 0.60 0.09 ? 0.02
<0.05* 1.51 t 0.46 0.19 t 0.03
<0.05* 0.62 2 0.23 0.15 t 0.03
ns
0.45 C 0.12 0.05 C 0.02
<0.05* 0.32 t 0.08 0.10 2 0.04
ns 0.25 Z 0.06 0.10 2 0.01
ns 0 .142 0.13 0.05 2 0.02
ns
1.07 2 0.38 0.02 ? 0.002
<0.05* 0.89 t 0.25 0.02 2 0.005
<0.05* 0.60 t 0.18 0.01 C 0.003
<0.05* 0.46 2 0.18 0.02 2 0.006
ns
Taken from Reuben et al. Am J Obstet Gynecol, with permission. aSee footnote to Table 1.
cultures of uninfected women. These data suggest that there is a difference in response to immune activation between HIV-positive and HIV-negative trophoblastic cells and that HIV-positive and not HIV-negative trophoblastic cells are more receptive to additional immune activation.
Placental inflammation associated with HIV vertical transmission In a prospective study of 100 placentas of HIV-infected women, there appeared to be a correlation between inflam- mation of various tissues of the placenta in 7/12 cases of HIV-infected infants (Table 6) (20). There were 30 cases of inflammation of placental tissues yielding seven HIV-infected infants, whereas placentas without evi- dence of inflammation yielded four HIV-infected infants. The placenta of one HIV-positive infant was inadequately sectioned. These data do not lend themselves to statistical
Table 5. Expression (mean 2 SEM) of cytokine messages by trophoblast stimulated with LPS.
Targeumimic signal ratios
Time Group L I P IL-6 TNF-or
6 HIV+ 2.55 2 0.83 0.81 t 0.32 1.48 2 0.69 HIV- 0.13 2 0.02 0.07 2 0.03 0.03 2 0.003 P <0.05* <0.05* <0.05*
HIV- 0.37 2 0.15 0.08 2 0.01 0.02 2 0.003 24 HIV+ 4.12 t 1.68 0.44 2 0.07 0.79 t 0.22
P <0.05* <0.05* <0.05*
HIV- 0.28 C 0.07 0.07 2 0.02 0.003 2 0.002 P <0.05* <0.05* <0.05*
Taken from Reuben et al. Am J Obstet Gynecol, with permission. aSee footnote to Table 1.
48 HIV+ 2.56 t 0.64 0.43 L 0.09 0.81 2 0.22
Tuble 6. Histopathological study of 100 placentas of HIV-infected pregnant women with 12% HIV vertical transmission rate: evidence for inflammation predisposing for HIV vertical transmission.
Acute injammarion 4 cases with acute chorioamnionitis alone 2 HIV+ infants 8
13
cases with acute inflammation within umbilical cord or chorionic plate vessels alone cases with both maternal acute chorioamnionitis and acute inflammation with umbilical cord or chorionic plate vessels
I HIV+ infant
2 HIV+ infants
25 cases with acute inflammation 5 HIV+ infants
Chronic injammation 1 case with chronic inflammation within the
chorionic plate and chronic inflammation of basal villi HIV- infant
1 case of chronic inflammation of the umbilical cord vessels H I T infant
1 case of chronic inflammation of fetal stem vessels with chronic non-basal villitis HIV+ infant
2 cases of chronic inflammation of non-basal 1 HIV'infant villi 1 HIV- infant
5 cases with unusual chronic inflammation 2 HIV+ infants
Five H I P infants not included above 4
1
cases with no inflammation in any placental compartment case not assessed due to inadequate sectioning of placental tissue
Taken from Ref. 20 with permission. HIV' = HIV-positive; HIV- = HIV-negative.
analysis but they do provide some additional evidence that inflammation of placental tissues contributes to the transmission of HIV from mother to infant.
Possible roles of placental cytokines and placental tissue inflammation in HIV vertical transmission Cytokines are believed to play a pivotal role in the regula- tion of HIV expression in experimental systems. Cytokines such as IL- 10 and TNF-(r can activate HIV- 1 gene expres- sion through the action of NKkB (12,21). It has been shown that IL- 10 alone and in synergy with IL-6 can induce HIV-1 expression in chronically infected U1 cells (22). In the present study, term placental trophoblastic cells from HIV-seropositive women exhibited significantly higher levels of IL-10 mRNA and higher constitutive IL-10 secre- tion. In contrast, IL-10 message and protein secretion by term placental trophoblastic cells from non-infected women were low and remained stable over the 48-h incubation period. These low levels of IL-10 are consistent with the non-invasive biological function of normal mature trophoblasts (23). In addition to secreting IL- 10, tropho- blasts spontaneously produce IL-6 throughout pregnancy (24). Compared to trophoblastic cell cultures from unin- fected women, HIV-seropositive women secreted higher

ACTA PEDIATR SUPPL. 421 (1997)
constitutive levels of IL-6, which were augmented by stimu- lation with LPS. Thus, the secretion in IL-6 in the tropho- blastic cell cultures of HIV-positive women are more likely to be due to the concomitant increase of IL-1P (25,26). This observation may be more suggestive of co-existing inflam- matory conditions in response to co-infections that are more likely to occur in HIV-seropostive women (9, 27).
Tumor necrosis factor alpha is expressed within human placental villi during normal pregnancy and can induce apoptosis in cultures of trophoblasts. (19). This is consis- tent with the observation of diminished viability in 2-day- old trophoblastic cell cultures (data not shown). The study shows that with LPS stimulation the production of TNF-a is significantly augmented in HIV-positive trophoblastic cells. The TNF-a production peaked at 6 h and declined thereafter, and the production of TNF-a from 6-h tropho- blastic cell cultures of HIV-positive women is significantly higher than that of HIV-negative control subjects. The production of IL-1 has been found to be enhanced in placentas during labor and intrauterine infection (28). Other studies (29) reported that pretreatment of tropho- blastic cell cultures with TNF-a and IL-1P can stimulate adhesion of HIV-infected MOLT-4 cells to the trophoblasts in a time-dependent manner. The significantly higher level of TNF-a and IL-10 produced by the trophoblastic cell cultures of HIV-positive women provide a possible mechanism for cytokine-upregulated cell-mediated HIV infection in the trophoblasts.
In this study, a positive association was found between the HIV infection in the trophoblasts, as judged by HIV- RNA PCR, and the spontaneous secretion of IL-1P in the cultural supernatant. Nevertheless, based on the prelimin- ary data, there was no correlation between the level of IL- 1 /3 production and the transcription level of the P50 subunit of NFkB (Y = 0.39) (data not shown). Although specific inducers of NFkB can stimulate virus production, their effects vary by cell types. For example, TNF-a can induce virus production in certain cell lines, with the effect varying with the cell type (30). Our failure to detect any association between IL-lP and NFkB may represent the differences in cell types or the presence of antiviral systems that might adversely affect the induction
This study reveals that the upregulated production of inflammatory cytokines is more prevalent in the tropho- blastic cell cultures of HIV-positive women. However, the increased cytokine production and the HIV mRNA level are not correlative and suggest that indeed additional fac- tors may be necessary for the control of HIV expression in trophoblasts. Such factors may include acute chorioamnio- nitis and chronic villitis of the placenta, which have been shown to predispose an infant to acquire HIV infection from its mother.
NFkB by IL-lP. ,
References 1. Beer AE, Kwak JYH, Ruiz J. Reproductive immunology. In: Rich
2
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
RR, et al. editors. Organ-specific inflammatory diseases. 1996: 1537- 50 Biggar RJ, Pahwa S, Minkoff H, Mendes H, Willoughby A, Landesman S, et al. Immunosuppression in pregnant women infected with human immunodeficiency virus. Am J Obstet Gynecol 1989: 161: 1239-44 Minotti PG, Liomba G. Dallabetta GA, Hoover DR, Chiphangwi JD, Saah A. T lymphocyte subsets during and after pregnancy: analysis in human immunodeficiency virus type- 1 infected and uninfected Malawian mothers. J Infect Dis 1992; 165: I 116-9 Dinsmoor MJ, Christmas JT. Changes in T-lymphocyte subpopula- tions during pregnancy complicated by human immunodeficiency virus infection. Am J Obstet Gynecol 1992; 167: 1575-9 St Louis ME, Kamenga M, Brown C, Nelson AM, Manzila T, Batter V, et al. Risk for perinatal HIV- I transmission according to maternal immunologic, virologic, and placental factors. JAMA 1993;
Rich KC, Siege1 JN, Jennings C, Rydman RJ, Landay AL. CD4' lymphocytes in perinatal human immunodeficiency virus (HIV) infection: evidence for pregnancy-induced immune depression unin- fected and HIV-infected women. J Infect Dis 1995; 172: 1221-7 Boyer PJ, Dillon M, Navaie M, Deveikis A, Keller M, O'Rourke S, et al. Factors predictive of maternal-fetal transmission of HIV-I. Preliminary analysis of zidovudine given during pregnancy andor delivery. JAMA 1994; 271: 1925-30 Nelson AM, Firpo A, Kamenga M, Davachi F, Angritt P, Mullick FG. Pediatric AIDS and perinatal HIV infection in Zaire: epidemiologic and pathologic findings. In: Greco MA, Rotterdam H, Anderson V, Kahn EL, editors. Progress in AIDS pathology. Vol 111. Blue Bel, PA: Field & Wood, 1992: 1-33 Chadwani S, Greco MA. Mittal K, Antoine C, Drasinski K, Borkowsky W. Pathology and human immunodeficiency virus expression in placentas of seropositive women. J Infect Dis 1991;
Lewis SH, Reynolds-Kohler C, Fox HE, Nelson JA. HIV-I in trophoblastic and villous Hofbauer cells, and haematologic precursors in eight-week fetuses. Lancet 1990; 35: 5465-8 Griffin GE, Leung K, Folks TM, Kunkel S, Nabel GJ. Activation of HIV gene expression during monocyte differentiation by induction of NF-kB. Nature 1989; 339: 2868-80 Folks TM, Clouse KA, Justement J, Rabson A, Duh E, Kehrl JH, et al. Tumor necrosis factor 01 induces expression of human immuno- deficiency virus in a chronically infected T-cell clone. Proc Natl Acad Sci USA 1989; 86: 2365-8 Reickman P, Poli G , Kehrl JH, Fauci AS. Activated B lymphocytes from human immunodeficiency virus-infected individuals induced virus expression in infected T cell and promonocyte cell line, U1. J Exp Med 1991; 173: 1-5 Hill JA, Polgar K, Anderson DJ. T-helper I-type immunity to tropho- blast in women with recurrent spontaneous abortion [preliminary communication] JAMA 1995; 273: 1933-6 Guilvert L, Robertson SA, Wegmann TG. The trophoblast as an integral component of a macrophage-cytokine network. Immunol Cell Biol 1993; 71: 49-57 Jokhi PP, King A, Sharkey AM, Smith SK, Loke YW. Screening for cytokine messenger ribonucleic acids in purified human decidual lymphocyte populations by the reverse-transcriptase polymerase chain reaction. J Immunol 1994; 153: 4427-35 Schnittman SM, Singer KH, Greenhouse JJ, Stanley SK, Wichard LP, Haynes BF, et al. Thymic microenvironment induced HIV expres- sion: physiologic secretion of IL-6 by thymic epithelial cells upregu- lated virus expression in chronically infected cells. J Immunol 1991; 147: 2553-8 Lee B-N, Li S, Popek E, Hammill H, Erickson N, Helfgott A, et al. Expression profiles of inflammatory cytokines in human placental trophoblasts isolated from HIV' gravidae [abstract]. XI International Conference on AIDS, Vancouver, British Columbia, July 1996 Yui J, Garcia-Lloret M, Wegmann TG, Guilhert LJ. Cytotoxicity of tumor necrosis factor-alpha and gamma-interferon against primary human placental trophoblasts. Placenta 1994; 15: 819-35
269: 2853-9
1634: 1134-8

38 WT Shearer et ar. ACTA PEDIATR SUPPL 421 (1997)
20. Popek EJ, Langston C, Lewis D, Hammill H, Hanson C, Hawkins E, et al. Placental pathology in 100 liveborn infants of HIV-seropositive women: a prospective study. In preparation
21. Osborn L, Kunkel S, Nabel GJ. Tumor necrosis factor a! and inter- leukin 1 stimulate the human immunodeficiency virus enhancer by activation of the nuclear factor KB. Proc Natl Acad Sci USA 1989; 86:
22. Poli G, Kinter AL, Fauci AS. Interleukin 1 induces expression of the human immunodeficiency virus alone and in synergy with interleukin 6 in chronically infected U1 cells: inhibition of inductive effects by the interleukin 1 receptor antagonist. Proc Natl Acad Sci USA 1994;
23. Librach CL, Feigenbaum SL, Bass KE, Cui TY, Verastas N, Sadovsky Y, et al. Interleukin- 1 beta regulates human cytotrophoblast metalloproteinase activity and invations in v im. J Biol Chem 1994;
24. Kameda T, Matsuzaki N, Sawai K, Okada T, Saji F, Matsuda T, et al. Production of interleukin-6 by normal human trophoblast. Placenta 1990; 11: 205-13
25. Yagel S, Casper RF, Powell W, Parhar RS, Lala PK. Characterization of pure human first-trimester cytotrophoblast cells in long-term
2336-40
91: 108-12
269: 17125-31
culture: growth pattern, markers, hormone production. Am J Obstet Gynecol 1989; 160: 938-45
26. Musuhior K, Matsuzaki N, Nishino E, Taniguchi T, Kameda T, Li F, et al. Trophoblast-derived interleukin-1 (IL-I) stimulates release of human chorionic gonadotropin by activate IL-6 and IL-6-receptor system in first trimester human trophoblasts. J Clin Endocrinol Metab 1991; 72: 594-601
27. Romero R, Mazor M. Infection and preterm labor. Clin Obstet Gynecol 1989; 31: 553-84
28. Taniguchi T, Matsuzaki N, Kameda T, Shimoya K, JOT, Saji F, et al. The enhanced production of placental interleukin- 1 during labor and intrauterine infection. Am J Obstet Gynecol 1991; 165: 131-7
29. Schwartz DH, Sharma UK, Penmen EJ, Blakemore K. Adherence of human immunodeficiency virus-infected lymphocytes to fetal placenta cells: a model of maternal fetal transmission. Proc Natl Acad Sci USA 1995; 92: 978-82
30. Matsuyama T, Hamamoto Y, Soma G, Mizuno D, Yamamoto N, Kobayashi N. Cytocidal effect of tumor necrosis factor on cells chronically infected with human immunodeficiency virus (HIV): enhancement of HIV replication. J Virol 1989; 63: 2504-9
![Synthetic PreImplantation Factor (PIF) prevents … pathway leads to activa-tion of the uterine and placental endothelium and the release of embryotoxic cytokines [9, 10]. We hypothesize](https://img.dokumen.tips/doc/110x75/5d3f20cc88c993860c8caa18/synthetic-preimplantation-factor-pif-prevents-pathway-leads-to-activa-tion-of.jpg)
![From Inflammation to Fibrosis—Molecular and Cellular ...From Inflammation to Fibrosis—Molecular and Cellular ... nisms, including chemical mediators such as cytokines [7].](https://img.dokumen.tips/doc/110x75/5e8c28cec98289453a14f8d1/from-inflammation-to-fibrosisamolecular-and-cellular-from-inflammation-to.jpg)



























