Embed Size (px)
Citation preview

Cytokines
• Cytokines are small secreted proteins which mediate and regulate immunity, inflammation, and hematopoiesis.
• They generally (although not always) act over short distances and short time spans and at very low concentration.
• They act by binding to specific membrane receptors, which then signal the cell via second messengers, often tyrosine kinases, to alter its behavior (gene expression).
• Responses to cytokines include increasing or decreasing expression of membrane proteins (including cytokine receptors), proliferation, and secretion of effector molecules.
• Cytokines may act on the cells that secrete them (autocrine action), on nearby cells (paracrine action), or in some instances on distant cells (endocrine action).

Cytokine Activities
• Cytokines are made by many cell populations, but the predominant producers are helper T cells (Th) and macrophages.
• The largest group of cytokines stimulates immune cell immune cell proliferation and differentiation. proliferation and differentiation.
• This group includes – Interleukin 1 (IL-1), which activates T cells; – IL-2, which stimulates proliferation of antigen-activated T and B
cells; – IL-4, IL-5, and IL-6, which stimulate proliferation and
differentiation of B cells; – Interferon gamma (IFNg), which activates macrophages;

Q. What effect would a defect in the gene that makes the gamma chain have?

HypersensitivityThere are four different types of hypersensitivities that result from different responses of the immune system:
• There are 3 types of immediate hypersensitivities that depend on the interaction of antigens with antibodies : Type I, Type II, and Type III.
• Type I (IgE-mediated or anaphylactic-type) • Mechanism: This is the most common type of hypersensitivity,
seen in about 20% of the population. IgE is made in response to an allergen .
• In allergic individuals, the levels of IgE may be thousands of times higher than in those without allergies.
• Possibly this is due to a higher number of Th2 cells which produce IL-4, a cytokine that can increase production of IgE, and a lower number of Th1 cells that produce gamma-interferon, a cytokine that decreases IgE production.

The Fc portion of IgE binds to the surface of mast cells and basophils When the allergen cross-links the Fab portions of the mast cell-bound IgE, this triggers histamine release by the mast cell, a process called degranulation, and the synthesis of other inflammatory mediators such, leukotrienes, prostaglandins, and cytokines that contribute to inflammation (these act as chemoattractants).
These agents cause the early phase of allergic reactions that appears within minutes after exposure to the antigen.

Type I hypersensitivity is treated symptomatically with such agents as:
• a. epinephrine. Epinephrine relaxes smooth muscle, constricts blood vessels, and stimulates the heart. It is used for severe systemic reactions.
• b. antihistamines . Antihistamines block the binding of histamine to histamine receptors on target cells.
• Severity may be reduced by desensitization shots (allergy shots). It is thought that when very dilute allergen is given by injection, it stimulates the production of IgG
• IgG then act as blocking antibodies to bind and neutralize much of the allergen in secretions before it can bind to the deeper cell-bound IgE on the mast cells in the connective tissue.
• A new experimental approach to treating and preventing Type-I hypersensitivity involves giving the person with allergies injections of monoclonal antibodies that have been made against the Fc portion of human IgE.
IgE
IgG
Q. how could mothers and children have the same allergic reactions?

Type II (Antibody-dependent cytotoxicity) • Mechanism: Either IgG or IgM is made against normal self
antigens
opsonization of the host cells whereby phagocytes stick to host cells by way of IgG, and discharge their lysosomes and ;
activation of the classical complement pathway causing
MAC lysis of the cells
ADCC destructionof the host cells whereby NK cells attach to the Fc portion of the antibodies. The NK cell then release pore-forming proteins called perforins and proteolytic enzymes called granzymes. Granzymes pass through the pores and activate the enzymes that lead to apoptosis of the infected cell by means of destruction of its structural cytoskeleton proteins and by chromosomal degradation.
EX• MS• Lupus• Pernicious anemia

MS & MG• Higher levels of Ab to the
myelin basic protein during flare up
• Myelin BP (insulation around nerve cells)
• Nerve cells become exposed • Eventual destruction of the
nerve cell • --------------------------------• Ab to achl receptors• Ab comes in and blocks the
ability of AC to bind to the muscle receptor
• Therefore the muscle cannot function

Type III (Immune complex-mediated) • Mechanism: This is caused when soluble antigen-antibody
(IgG or IgM) complexes, which are normally removed by macrophages in the spleen and liver, form in large amounts and overwhelm the body . These small complexes lodge in the capillaries, pass between the endothelial cells of blood vessels - especially those in the skin, joints, and kidneys - and become trapped on the surrounding basement membrane beneath these cells . The antigen/antibody complexes then activate the classical complement pathway . This may cause:
• a. massive inflammation, due to complement protein
• b. influx of neutrophils, due to complement protein , resulting in neutrophils discharging their lysosomes and causing tissue destruction and furthes inflammation
• c. MAC lysis of surrounding tissue cells, due to the membrane attack complex,
Ex• Rheumatoid Arthritis• Lupus


Delayed Hypersensitivity (Type IV) • Delayed hypersensitivity is cell-
mediated rather than antibody-mediated.
• Mechanism: Delayed hypersensitivity is the same mechanism as cell-mediated immunity. T8-lymphocytes become sensitized to an antigen and differentiate into cytotoxic T-lymphocytes while Th1 type T4-lymphocytes become sensitized to an antigen and produce cytokines . CTLs, cytokines, and/or macrophages then cause harm rather than benefit .
• MS• Scleroderma• Inflammatory bowel disease (Th17)• Type 1 Diabetes
– MHC II– T reg Failure
Regulatory T cells
• Regulatory T cells (also known as suppressor T cells) are a specialized subpopulation of T cells that act to suppress activation of the immune system and thereby maintain immune system homeostasis and tolerance to self.
• Similar to other T cells, regulatory T cells develop in the thymus. The latest research suggests that regulatory T cells are defined by expression of the forkhead family transcription factor FOXP3 (forkhead box p3).
• Expression of FOXP3 is required for regulatory T cell development and appears to control a genetic program specifying this cell fate. The large majority of Foxp3-expressing regulatory T cells are found within the major histocompatibility complex (MHC) class II restricted CD4-expressing (CD4+) helper T cell population and express high levels of the interleukin-2 receptor alpha chain (CD25).

Vitamin D
• Vitamin D is a potent immune system modulator.
• The VDR is expressed by most cells of the immune system, including T cells
• T-helper cells are essentially in charge of modulating autoimmunity.
• Th1 cells release pro-inflammatory cytokines that lead to tissue damage associated with autoimmunity.
• Th2 cells release anti-inflammatory cytokines that balance Th1 activity, so that an appropriate immune response can occur.
• T-regs are responsible for maintaining self-tolerance, so that our immune system does not react against the body and drive an autoimmune condition.
• Researchers have recently determined that, with inadequate levels of vitamin D, there is an over-expression of Th1 cells (Tc, TNF-alpha, IF gamma) and an under-expression of Th2 cells and T-regs.3 Indeed, in vivo studies in the laboratory have demonstrated that vitamin D therapy leads to a reduction in the autoimmune Th1 response and a reduction of symptoms of experimental inflammatory bowel disease, rheumatoid arthritis, type 1 diabetes, and multiple sclerosis.

Treatments
1. Plasmaporesis
2. Drugs that inhibit mitosis (mexotrexate)
3. Removal of spleen
4. Blocking Ab
Animal ModelHuman disease Inducing Ag
NOD Type 1 diabetes Unknown
NZB Lupus Unknown
Expt Autoimmune MG Myasthenia Gravis Achl receptors
Expt autoimmune EM MS MBP/PLP

Mimicry ? • Proteins show high levels of homology
• reduction in diet in animal models showed low levels of AID • Leptin assoc with obesity• Leptin( high homology with IL-2)• Therefore it acts like a cytokine• Found in assoc with fats• Leptin higher in females• Therefore increase in T helper 1 cells, Tc, Mac, Neu, IF-gamma, TNF alpha
In females• TH1 response (Tc etc)• most effective way of getting rid of infectious agents
In males• Get TH2 response (IL4,IL5 Ab)• high infections• Low AI disease


Cancer

2006 Estimated US Cancer Cases*
*Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder.Source: American Cancer Society, 2006.
Men720,280
Women679,510
31% Breast
12% Lung & bronchus
11% Colon & rectum
6% Uterine corpus
4% Non-Hodgkin lymphoma
4% Melanoma of skin
3% Thyroid
3% Ovary
2% Urinary bladder
2% Pancreas
22% All Other Sites
Prostate 33%
Lung & bronchus 13%
Colon & rectum 10%
Urinary bladder 6%
Melanoma of skin 5%
Non-Hodgkin4% lymphoma
Kidney 3%
Oral cavity 3%
Leukemia 3%
Pancreas 2%
All Other Sites 18%

2006 Estimated US Cancer Deaths*
ONS=Other nervous system.Source: American Cancer Society, 2006.
Men291,270
Women273,560
26% Lung & bronchus
15% Breast
10% Colon & rectum
6% Pancreas
6% Ovary
4% Leukemia
3% Non-Hodgkin lymphoma
3% Uterine corpus
2% Multiple myeloma
2% Brain/ONS
23% All other sites
Lung & bronchus 31%
Colon & rectum 10%
Prostate 9%
Pancreas 6%
Leukemia 4%
Liver & intrahepatic 4%bile duct
Esophagus 4%
Non-Hodgkin 3% lymphoma
Urinary bladder 3%
Kidney 3%
All other sites 23%

Cancer: Inside and Outside Factors
Age
Obesity
Weak immune system
AlcoholDietSmoking
Cancer
AlcoholDietSmokingCarcinogensViruses
HormonesDiet
Age Age
Cancer
Time

Breast Cancer Statistics
AGE IS the MOST
IMPORTANT RISK FACTOR
Median Age of Diagnosis is
Between 60-65

CancerGeneral Ideas
• Epithelial in origin
• Rapid proliferation of cells
• Cells found where they shouldn’t be
• BenignBenign = ability to proliferate, but somewhat limited, no movement
• MalignantMalignant= ability of growth to migrate and invade surrounding tissues
• Tumor Ag very rare (ex PSA = prostate specific)
• Cancer is clonal in origin
• All cancers are heterogeneous
• Selection process sets up heterogeneity

Cancer Origins
• Cancer is clonal in origin
• Combination of genetic and epigenetic events
• Mutations arise due to deletions, duplications, inversions, translocations.
normal
Tu

What influences cancer?Environment/lifestyle• Certain lifestyle choices are known to increase your
risk of cancer. • Smoking, drinking excessively, excessive exposure to
the sun or frequent blistering sunburns. - U.S. smoking lung cancer- China smoked or pickled foods stomach cancer
Your environment
• The environment around you may contain harmful chemicals that can increase your risk of cancer.
• Even if you don't smoke, you might inhale secondhand smoke if you go places where people are smoking or you live with someone who smokes.
• Chemicals in your home or work environment, such as asbestos and benzene, also are associated with an increased risk of cancer.
Heredity• Certain cancers run in families (<10%)• Breast cancer • Retinoblastoma (cancer affecting the eye)

What causes cancer?
• Cancer begins with damage (mutations) in your DNA.
• Normal cells often develop mutations in their DNA, but they have the ability to repair most of these mutations.
• Or, if they can't make the repairs, the cells often die (apoptosis). However, certain mutations aren't repaired, causing the cells to grow and become cancerous.
• Mutations also cause cancer cells to live beyond a normal cell life span. This causes the cancerous cells to accumulate.
• The initial genetic mutation is just the beginning of the process by which cancer develops. Scientists believe you need a number of changes within your cells in order to develop cancer

Steps in cancer progression
• An initiator to cause a genetic mutation. Sometimes you're born with this initial genetic mutation. Other times a genetic mutation is caused by forces within your body, such as hormones, viruses and chronic inflammation. Genetic mutations can also be caused by forces outside of your body, such as ultraviolet (UV) light from the sun or cancer-causing chemicals (carcinogens) in your environment.
• Promotion to cause rapid cell growth. Promoters take advantage of genetic mutations created by initiators. Promotors cause cells to divide rapidly. This could lead to a tumor. Promoters could be inherited, could come from inside your body or could come from outside your body.
• Progression to cause cancer to become aggressive and spread. Progression involves genetic damage that results in the conversion of benign tumors into malignant neoplasms capable of invading adjacent tissues and metastasizing to distant sites Without a progressor a tumor may remain benign and localized.
Tom Slaga
•Sencar Mice (Sci Park)
•SENCAR is derived from SENsitivity to CARcinogenesis
•Carcinogen (tobacco tar ) put on backs of mice
•Didn't get cancer •Added phorbol myristate acetate (PMA)
•Became cancerous

Cancer is very heterogeneousBecause of: Large # of cells
Mechanism for selection is achieved byhaving high levels of proliferation andapoptosis occurring.
This will allow the more robust cells tobe selected for
Can survive acidic conditions High CO2 Low nutrientrequirements (MEM)
These cells may be able tomake all factors that arerequired for growth/progressionto occur
The cell is now autonomous toits environment

HMEC’s (human mammary epithelial cells)
• Senescent at G1 stage (G0)
• Cells were undergoing rapid proliferation and apoptosis
• Selection is going to occur here
• For cells to start growing, they need to silence other genes (Tumor supressor genes TSG’s)
• Ex Rb, p53, p16
So what allows tumor cells to form?
Mutation in proto-oncogenes(oncogenes) gas pedal, cell prolif
K.O. tumor suppressor genes, removal of cell brake
Normal cell cycle = 18-24 hoursTumor cell cycle = 6 hours
P16 methylationHoxA9 downregulationBrakes released allowingCells to proliferate

Tumor suppressor genes, or more precisely, the proteins for which they code, either have a dampening or repressive effect on the regulation of the cell cycle or promote apoptosis, and sometimes do both. The functions of tumor suppressor proteins fall into several categories including:
– Repression of genes that are essential for the continuing of the cell cycle. If these genes are not expressed, the cell cycle will not continue, effectively inhibiting cell division.
– Coupling the cell cycle to DNA damage. As long as there is damaged DNA in the cell, it should not divide. If the damage can be repaired, the cell cycle can continue.
– If the damage can not be repaired, the cell should initiate apoptosis, or programmed cell death, to remove the threat it poses for the greater good of the organism.

P 53 Roles– Most cancers (60%) have a defective p 53– There is probably 100% defective p 53 pathways involved – in cancer
Function of p53 – Checks integrity of the DNA that is about to be replicated. – Is the DNA worth repairing if there are mutations – If yes allows replication – If not Apoptosis – Rechecks integrity of replicated DNA at checkpoint 2 – Therefore the system is setup to stop tumor formation.
There are 3 major functions that it is involved with inside the cell.
1. Blocks proliferation (p21 p16) 2. Transcribes DNA repair genes 3. Induced apoptosis

How does p53
exert its function?• p21 = major block
for cyclin D• p16 = blocks prolif
pathway ras---erk---akt

Tobaccoaminostilbene arsenic benz[a]anthracene benz[a]pyrene benzene benzo[b]fluoranthenebenzo[c]phenanthrene benzo[f]fluoranthene cadmium chrysene dibenz[a c]anthracenedibenzo[a e]fluoranthene dibenz[a h]acridine dibenz[a j]acridine dibenzo[c g]carbazoneN-dibutylnitrosamine 2,3-dimethylchrysene indeno[1,2,3-c d]pyrene S-methylchryseneS-methylfluoranthene alpha-naphthylamine nickel compounds N-nitrosodimethylamine
N-nitrosomethylethylamine N-nitrosodiethylamine N-nitrosonornicotine N-nitrosoanabasineN-nitrosopiperidine polonium-210
Mutations in p53 • “Hotspots” are regions where mutations appear to occur more frequently • In p53 sequenced from cancer cells, many mutations are in DNA binding domain

Tumor Suppressors
Al Knudsen (Cal Tech) Idea that there was a cancer causing gene proposed Looked at 100 families for Rb (cancer of the eye) • R L • Family A - - • B + - • C + + • Postulated that there was an element of inheritance • ie the ability to not get Rblast was inherited in a dominant fashion • the ability to get Rb was inherited in a recessive fashion
Bob Weinberg • 1985 • Isolated and cloned the Rb gene • Showed that they problem was a result of a deletion • Rb+ = wt • Rb- = mutant (deletion) • Rb is a tumor suppressor (act likes the brakes)

• Note • Rb needs to be unattached for E2F to work • Therefore in the G1 phase E2F is off • Phos-ate Rb to release it from E2F • CDK/Cyclin D/Rb/E2F

PTEN as a tumor suppressor of AKT
Avian erythroblastosis virusBishop and Varmus
Looked at RNA virus• Worked with chicken retrovirus (RNA) RSV• Found to be harmless.• One out of 10,000 developed cancer (leukemia)• Isolated out the retrovirus from that chicken• Infected 100 new chicks with the isolated “cancer causing strain”• 100% of the chick got cancer
• So how did this happen?• Idea that there was some sort of conversion from the previous, non-lethal strain to
this new “cancer causing strain”.LTR GAG Pol ENV LTR Follow-up work showed:• That Erb B section of cancer causing strain had high homology to EGFR (epidermal
growth factor receptor)• Proposed that a previous normal gene making EGFR had now changed, mutated,
into this cancer causing oncogene• The EGFR was regarded as a proto-oncogene (HER2 neu)

How Oncogenes Cause Cancer • The change of an proto-oncogene from normal to
cancerous function (oncogene) can be caused by a simple point mutation in the sequence of a gene.
• For example, a change in the ras oncogene, • Because the signal delivered by the ras oncoprotein is
continuously delivered, the cell continues to grow and divide. This unabated growth may lead to cancer development


There is an exchange of cytokines and growth factors between the Tu cells and the surrounding cells
In the early stages, this support is needed but eventually the Tu cell with become independent of its surroundings Increasing # of genetic events will cause this independence
Microenvironment of cancer cells
Landscaper Mac
B
T
Adipose
Nu
Tu
NKNitric OxideGranzymesPerforin

Gatekeeper• Hereditary forms of cancer • ex Rb • If mutation in one allele, will lead to cancer state • Ex BRCA 1/2 in breast cancer • Single mutation gives rise to cancer
Caretaker• P 53 as a caretaker• Caretakers are normally DNA repair genes • Therefore it is important for the tumor cell to knock out
these genes

Diet
Do Weight and Diet Affect Breast Cancer Recurrence?
fat tissue produces the hormone estrogen, and estrogen plays a role in the growth of some breast cancers.
Dietary fat: Some studies did tie high levels of dietary fat to a higher risk ofrecurrence. •Sat Fat, •Trans fats, •Fatty red meat •
•high-fiber diets, because fiber moves food, fluid, and potential toxins through the body faster, reducing the chance that the body will absorb them.
•certain vitamins and other compounds in fruits and vegetables that might stop or slow down the growth of cancer cells.
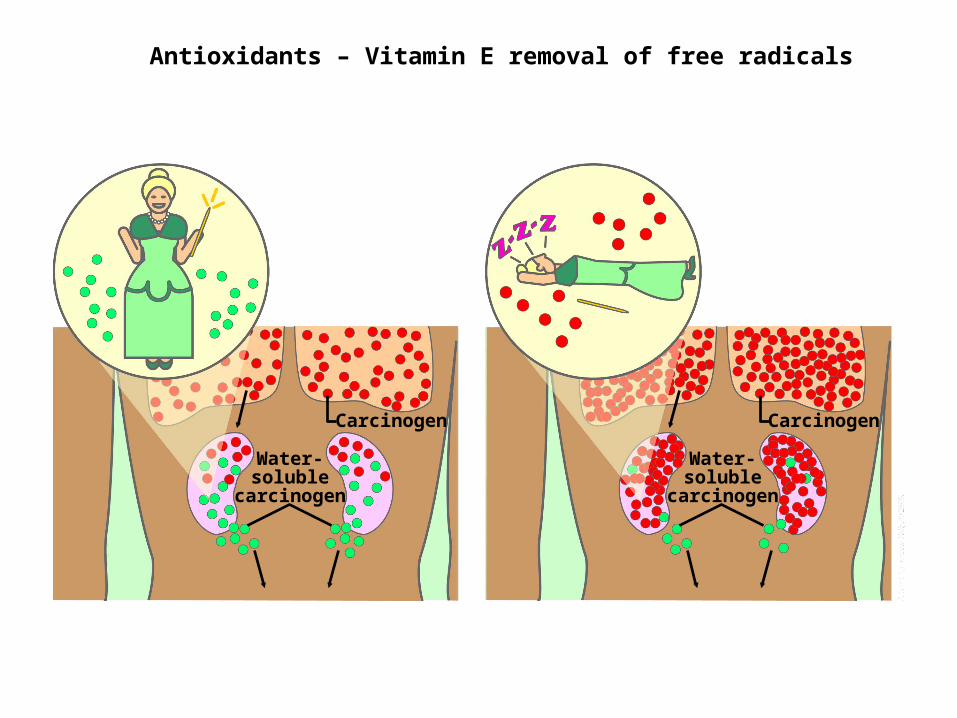
Water-soluble carcinogen
Carcinogen
Water-soluble carcinogen
Carcinogen
Antioxidants – Vitamin E removal of free radicals

Diet cont.
• Weight: Some studies showed that the risk of recurrence in women who were overweight at diagnosis increased by about a third (for example, the risk of recurrence could go from 6% to 8%).
• Caloric reduction (40%) has been shown to reduce incidence/growth of cancer
Possible Hypothesis• Adiposites have high cytokine release causing high
macrophage /eisinophils presence may lead to the formation of free radicals and subsequent DNA damage.
• Problems– Making people stick to a particular diet is easier said than done!!

ER Status in breast cancer cells70% +30% -


Aromatase inhibitors
• Aromatase inhibitors lower the amount of estrogen in post-menopausal women who have hormone-receptor-positive breast cancer. The hormone estrogen delivers growth signals to the hormone receptors.
• With less estrogen in the body, the hormone receptors receive fewer growth signals, and cancer growth can be slowed down or stopped.
• Before menopause, the ovaries produce most of a woman's estrogen, so reducing estrogen from other sources has little or no effect. But in post-menopausal women, most of the body's estrogen is made from another hormone, androgen.
• Aromatase inhibitors stop the enzyme called aromatase from turning androgen into (17 beta estradiol)-----estrogen, lowering the amount of estrogen produced OUTSIDE the ovaries.
• That means less estrogen in the bloodstream, less estrogen reaching estrogen receptors, and less cancer cell growth.

Immune System Evasion
• release of immunosuppressive cytokines
• Decoy Receptors
• downregulation of MHC I expression
• lack of costimulation (B7)
• interference with apoptotic pathways

Trojan Horse’ Technology Destroys Blood Supply to Cancer Tumors in Mice
• Dr. Michael Rosenblum, in mice demonstrated it could selectively destroy blood vessels supplying human solid tumors without harming the vasculature of normal tissue.
• “This is like a ‘Trojan horse’ approach to kill the blood vessels that supply solid tumors.
• using the vascular endothelial growth factor (VEGF) as a carrier to deliver a toxic agent selectively to the tumor’s blood supply – in effect, starving the tumor.
• VEGF is one of the predominant factors responsible for angiogenesis – the ability of a tumor to create new blood vessels to maintain growth and metastasize.
• The researchers chose the genetically engineered toxin gelonin to link to the VEGF “carrier” because it does not cause damage to normal blood vessels as do other toxins that have been explored for use in anti-tumor therapies,

T reg as a target• CD25 • FOXP3 • CD4 • Target Treg cells via CD25 (IL-2 alpha chain)• Tc cells not kept in check and can attack tumor cell• Side effect is induction of Autoimmunity (T reg prevent this via maintenance
of tolerance)• Transient application necessary to overcome this Gene Therapy• Attach FOXp3 promoter with gelonin to KO T reg's
Boosting the Immune System• CTLA-4 functions as a negative regulator of Tc proliferation. • B7 required for Tc stilumation • Following stimulation transcritption of CTLA-4 occurs and begins to reduce
Tc proliferation • Blockage of CTLA-4 allows increase in Tc proliferation and enhanced
response to tumors
TreatmentsSurgery is used to remove a tumor that is localized in a tissue or organ. The surgeon
removes the cancer cells or the tumor completely. Some healthy cells may also be removed to make sure that all the cancer is gone. Surgery is often combined with chemotherapy and/or radiation to ensure all cancer cells are removed.
Radiation is one of the most common treatments for cancer. The radiologist aims a beam of high-energy rays, such as X-rays and gamma rays, directly onto a tumor using a radiotherapy machine. These beams of radiation are many times more powerful than those produced in ordinary x-ray machines, in that they can damage and destroy cancer cells causing the tumor to shrink and even remove it completely. In order to focus the beam accurately onto the tumor, many X-rays films and Computer Tomography (CT) scans are taken to identify the exact position of the tumor.
Chemotherapy usually consists of a combination of several anti-cancer drugs.. It may be given alone or in combination with radiation therapy.
Biological Therapy is a treatment that uses the body own natural defense system known as the immune system. (TIL)Biotherapy is designed to repair, stimulate, and improve the ability of the patient's immune system to fight cancer. Biological therapy uses substances such as antibodies which home in directly to the site of the cancer. It is used either alone, or in conjunction with other conventional treatments such as surgery, radiation and chemotherapy.

Good Luck!!!!
Thanks for a great last semester