Embed Size (px)
Citation preview

Critical Review
Role of MicroRNAs in Cardiac Hypertrophy and Heart Failure
Nan Wang1,2, Zhen Zhou1,2, Xinghua Liao1,2 and Tongcun Zhang1,21Key Laboratory of Industrial Microbiology, Ministry of Education, Tianjin, China2College of Biotechnology, Tianjin University of Science and Technology, Tianjin, China
Summary
MicroRNAs (miRNAs) are a class of endogenous, highly con-served, small noncoding RNAs that regulate gene expressionpost-transcriptionally. Recent studies have demonstrated thatmiRNAs are aberrantly expressed in the cardiovascular system.The implications of miRNAs in cardiovascular disease haverecently been recognized, representing the most rapidly evolv-ing research field. Gain- and loss-of-function studies in micemodels have identified distinct roles for specific miRNAs duringcardiac hypertrophy, heart failing, and myocardial infarction.In the present article, the currently relevant findings on therole of miRNAs in cardiac hypertrophy and heart failure willbe summarized and the target genes and signaling pathwayslinking these miRNAs will be discussed. Furthermore, we focuson the use of miRNA mimics and antagonists (antagomirs) astools for disease therapy in the cardiovascular system in thefuture. Taken together, the recent studies showed that miRNAsare key regulators of gene expression in cardiovascular biologyand suggested the potential importance of miRNAs as diagnos-tic markers and therapeutic targets for cardiovasculardisease. � 2009 IUBMB
IUBMB Life, 61(6): 566–571, 2009
Keywords microRNAs; cardiac hypertrophy; heart failure; cardiovas-
cular disease; antagomirs.
INTRODUCTION
MicroRNAs (miRNAs) are endogenous, single-stranded,
small, �22-nucleotide (nt) noncoding RNAs that regulate target
gene. The first miRNA assigned to a specific function was lin-
4, which targets lin-14 during temporal pattern formation in
Caenorhabditis elegans (1). Since then, a variety of miRNAs
have been discovered. More than 500 miRNAs have been
cloned and sequenced in humans, and the estimated number of
miRNA genes is as high as 1,000 in the human genome (2).
miRNAs are estimated to regulate the expression of more than
a third of human protein-coding genes (3). Therefore, miRNAs
are important regulators of gene expression in various disease
and development processes. Initially, the importance of miR-
NAs is mainly discussed in regulating oncogenesis and tumor
suppression. Altered patterns of miRNAs expression may
increase cell proliferation and decrease apoptosis to involve
cancer initiation and progression (4). Recently, since 2005, the
exciting research on the biological roles of miRNAs in the
mammalian cardiovascular system has become a most rapidly
evolving field. Several studies have demonstrated the impor-
tance of miRNAs not only in cardiovascular development, but
also in cardiovascular disease (5–8). In the present article, the
currently relevant findings on the role of miRNAs in cardiac hy-
pertrophy and heart failure will be summarized and the target
genes and signaling pathways linking these miRNAs in the con-
text will be discussed.
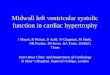
In mammals, the majority of miRNAs are located within
introns of either protein-coding or noncoding host genes (9).
miRNAs are initially transcribed as long RNA precursors
called primary miRNAs that requires the RNase III enzyme
Drosha in the nucleus to be trimmed into premature miRNAs
(Fig. 1). The latter precursor, characterized by a 33-nt stem-
loop or hairpin structure of 60–70-nt, are exported to the cyto-
plasm where they are subsequently cropped to become mature
miRNAs of 21–26-nt in length, by another RNase III enzyme
Dicer. One strand of the mature miRNA is incorporated in the
so-called miRNA-induced silencing complex (miRISC). Inter-
action with miRNA recognition elements that are mainly
located in the 30-untranslated region (UTR) of target messen-
ger RNAs leads to the degradation or translational inhibition
with subsequent protein repression (10). On the one hand, if
the pairing between the guide miRNA and the target RNA is
imperfect, then the RISC complex will inhibit the protein
translation of that RNA. On the other hand, if there is a per-
fect match, then the target mRNA will be cleaved (11).
Address correspondence to: Prof. Tongcun Zhang, College of Bio-
technology, Tianjin University of Science and Technology, Tianjin
300457, China. Tel: 186 2260 602 099. Fax: 186 2260 602 298.
E-mail: [email protected]
Received 18 February 2009; accepted 9 March 2009
ISSN 1521-6543 print/ISSN 1521-6551 online
DOI: 10.1002/iub.204
IUBMB Life, 61(6): 566–571, June 2009

Nucleotides 2 through 8 at the 50 end of the miRNA, termed
the seed sequence, are the most important determinants of
mRNA target selection. However, other nucleotides and
mRNA secondary structure in the regions surrounding the tar-
get sequence also influence the association of miRNAs with
their targets (3). It has been predicted that each single miRNA
can have [1,000 target genes and each single protein-coding
gene can be regulated by multiple miRNAs (3).
SPECIFIC EXPRESSION PROFILE OF MIRNA IN THEHEARTS
The expression profile of miRNAs seems to be tissue-cell
specific. Cheng et al. have implemented microarray technology
to analyze the expression of hundreds of miRNA in the normal
mouse (C576BJ) hearts (12). Overall, 157 of 233 arrayed miR-
NAs were found in normal mouse hearts, and 64 of these were
highly expressed. Their data also suggest the miRNA expression
profile in rat carotid artery is different from that in the rat heart.
The different expression profiles in different tissues implied that
the physiological functions of miRNAs in each tissue could be
unique. In addition, miRNA expression profiles can change
during cardiac development, and many miRNAs that are only
normally expressed at significant levels in the fetal human heart
are re-expressed in cardiac disease, such as heart failure. Fur-
thermore, also miRNAs whose expression is not restricted in
the heart may have important cardio-specific factions (13). So
this needs to be tested in the future.
EXPRESSION PROFILES OF miRNAs IN THE CARDIACHYPERTROPHY AND HEART FAILING
In response to injury and stress (such as hypertension, ische-
mic heart disease, aortic stenosis, and endocrine disorders), the
adult heart undergoes hypertrophic growth and cardiac remodel-
ing to compensate for sustaining cardiac output and impairing
cardiac function (14, 15). Cardiac hypertrophy, which is charac-
terized by an increase in cell size and/or myofibrillar without a
change in myocyte number, often leads to heart failure by acti-
vating intracellular signaling pathways and transcriptional medi-
ators in cardiac myocytes. Cardiac hypertrophy is also accompa-
nied by re-activation of ‘‘fetal’’ cardiac genes normally
expressed in the heart before birth (14). Given the emerging
research articles focus on miRNA and cardiac disease, it is
Figure 1. Biogenesis of miRNAs and their molecular mechanism in gene regulation.
567MicroRNAs IN CARDIAC HYPERTROPHY AND HEART FAILURE

therefore reasonable to hypothesize that miRNAs play important
roles in cardiac hypertrophy and heart failure.
Using miRNA microarrays, several groups have found the
global miRNA expression profile in mouse models that were
made hypertrophic by transverse aortic binding (TAB) or trans-
genic calcineurin. Olson identified 28 differentially expressed
miRNAs common to TAC and calcineurin-mediated hypertro-
phy and found that many of these were also overexpressed in
failing human hearts (7). The two models of pathological car-
diac hypertrophy demonstrated that the expression of miRNAs
are both up- and downregulated during differently induced car-
diac hypertrophy. Sayed et al. reported an array of more than
50 microRNAs with expression that progressively changes dur-
ing development of pressure-overload cardiac hypertrophy and
identified miR-1 as among the earliest microRNAs downregu-
lated during hypertrophy (6).
Importantly, miRNA expression profiles during hypertrophic
growth have also been reported to occur in human failing
hearts. Indeed, about more than 80% of induced and repressed
miRNAs were regulated in the same direction in fetal and fail-
ing heart tissue compared with healthy adult control left ven-
tricle (5). The most consistent changes were upregulation of
miR-21, miR-29b, miR-129, miR-210, miR-211, miR-212,
miR-423, and downregulation of miR-30, miR-182, and miR-
526. Clinical studies showed that a total of 43 out of 87 miR-
NAs detected are aberrantly expressed in hearts with ischemic
cardiomyopathy, dilated cardiomyopathy or aortic stenosis
(16). In a recently published article, miRNAs expression pat-
terns are examined in two types of human heart failure: idio-
pathic dilated cardiomyopathy and ischemic cardiomyopathy.
Their results demonstrate that subsets of miRNAs are differen-
tially regulated in each of these disease state etiologies and
each etiology demonstrated dysregulation of unique sets of
miRNAs (17). Taken together, the aforementioned data showed
that miRNAs were aberrantly expressed in hypertrophic hearts
and the results were confirmed by in vitro and in vivo studies
of cardiac hypertrophy.
MicroRNAs AND CARDIAC HYPERTROPHY ANDHEART FAILURE
More profound functions for these microRNAs in cardiac
biology have been revealed by gain- and loss-of-function stud-
ies. The overexpression of some miRNAs that are upregulated
in hypertrophic hearts induces cardiac myocyte hypertrophy,
whereas the overexpression of some miRNAs that are down-
regulated in hypertrophic hearts prevents cardiac myocyte hy-
pertrophy. Olson reported that miR-23a, miR-23b, miR-24,
miR-195, and miR-214, all of which were upregulated during
cardiac hypertrophy, appeared to be capable of inducing cardiac
hypertrophy, appeared to be capable of inducing hypertrophic
growth in cadiomyocytes (7). A transgenic approach revealed
that myocardial overexpression of miR-195 in mice was suffi-
cient to induce pathological cardiac growth and heart failure
within several weeks after birth (Fig. 2). However, the target
genes for miR-195 relevant to hypertrophy have not been stud-
ied. Moreover, the authors found that overexpression of miR-
214, which are also upregulated during hypertrophy, could not
evoke an adverse cardiac remodeling response. These studies
indicated that only some specific miRNAs were key regulators
in cardiac hypertrophy program.
Elegant work from Olson lab demonstrated that miR-208,
encoded by an intron 27 of the a-MHC gene, is required for
cardiomyocyte hypertrophy, fibrosis (18). The study showed
that miR-208 knockout mice are viable and exhibit no apparent
gross developmental defects. However, upon induction of TAC
pressure-overload, the mice had a blunted hypertrophic and
fibrotic response. Moreover, the miR-208-deficient mice failed
to upregulate b-MHC but instead increased a-MHC expression
to compensate. MiR-208 may integrate b-MHC by repressing
the thyroid hormone receptor associated protein 1 (Thrap1), a
cofactor of the thyroid hormone receptor (Fig. 2). The 30UTR
of Thrap1 is targeted directly by miR-208 and Thrap1 protein
levels were elevated in miR-208 null hearts (18).
MiR-21, a miRNA implicated in tumor-related cell growth
and apoptosis (19, 20), is upregulated in response to agonist-
induced cardiac hypertrophy in cell culture experiments and in
pressure-overload induced hypertrophy in vivo. Tatsuguchi et al.
used overexpression and knockdown approaches to demonstrate
that miR-21 repress hypertrophy in neonatal rat cardiomyocyte
in vitro (21). However, another study points to a different role
of miR-21 in cardiac hypertrophy. Cheng et al. reports that inhi-
bition of miR-21 expression is able to decrease cardiac myocyte
hypertrophy stimulated by both (angiotensin II) Ang II and
(phenylephrine) PE (12). Moreover, Thum et al. demonstrated
that miR-21 resulted in the cellular hypertrophy and activation
of a fetal gene program (5). It should be noted that controver-
sies exist among these studies. In 2008, Thum shows that
miRNA-21 regulates the ERK-MAP kinase signaling pathway
in cardiac fibroblasts, which has impacts on global cardiac
structure and function. MiR-21 levels are increased selectively
in fibroblasts of the failing heart, augmenting ERK-MAP kinase
activity through inhibition of sprouty homologue 1 (Spry1)
Figure 2. Diagram depicting the miRNA and their target genes,
which have been reported for their participation in cardiac hy-
pertrophy and heart failure.
568 WANG ET AL.

(Fig. 2) (8). Clearly, further analysis of the molecular pathways
modulated by miR-21 in different biological systems is needed
to better understand the biological function of this miRNA.
Sucharov et al. recently reported the role of miR-100 and
miR-92 in the hypertrophic process by their mimics and inhibi-
tors (17). The expression of miR-100 is increased in the failing
heart. Upregulation of miR-100 in neonatal rat cardiac ventricu-
lar myocytes results in repression of the adult genes aMyHC
and SERCA and increases isoproterenol-mediated upregulation
of the fetal genes ANF and bMyHC. Interestingly, downregula-
tion of miR-100 prevented isoproterenol-mediated repression of
aMyHC and SERCA but not the induction of the fetal isoforms,
suggesting that inhibition of miR-100 specifically regulates
expression of genes involved in ISO-mediated repression of the
adult isoforms. Unlike miR-100, miR-92 is downregulated in
heart failure. Inhibition or upregulation of miR-92 has a
minimal effect on the regulation of fetal or adult gene expres-
sion. These results suggest that the role of miRNAs in heart dis-
ease is specific and not all miRNAs affect global aspects of the
disease.
miR-1 and miR-133, which belong to the same transcrip-
tional unit, are expressed at low levels in mouse and human
models of cardiac hypertrophy (22). Notably, miR-1 and miR-
133 expression was consistently downregulated both in patho-
logical and physiological hypertrophy as demonstrated in mice
subjected to TAC, Akt-overexpressing transgenic mice or exer-
cise-trained wild-type mice, respectively (22). In vitro, overex-
pression of miR-133 or miR-1 inhibited cardiac hypertrophy.
Importantly, in vivo inhibition of miR-133 by a single infusion
of an antimiRNA antisense oligonucleotide (AMO) against
miR-133 caused marked and sustained cardiac hypertrophy.
This occurs through the regulation of different targets: RhoA, a
GDP-GTP exchange protein regulating cardiac hypertrophy;
Cdc42, a signal transduction kinase implicated in hypertrophy;
and Nelf-A (negative elongation factor A)/WHSC2 (Wolf-
Hirschhorn syndrome candidate 2), a nuclear factor involved in
cardiogenesis (Fig. 2) (21). Duisters et al. recently reported that
connective tissue growth factor (CTGF), which is a key mole-
cule in the process of fibrosis, is a direct target of miR-133 and
miR-30 (23).
MiR-1 is specifically expressed in cardiac precursor cells,
and the miR-1 gene is a direct transcriptional target of muscle
differentiation regulators, including SRFs (serum-response fac-
tors), MyoD (myogenic differentiation factor D) and Mef2
(myocyte-enhancing factor 2) (24). Abdellatif’s group found
that miR-1 was singularly downregulated as early as day 1, per-
sisting through day 7, after TAC-induced hypertrophy in a
mouse model (6). Overexpression of miR-1 carried by adenovi-
rus vector inhibited its in silico-predicted growth-related targets,
including Ras guanosine-triphosphatase-activating protein,
cyclin-dependent kinase 9, fibronectin, and Ras homolog
enriched in brain, in addition to protein synthesis and cell size
(Fig. 2). Wagner et al. recently injected the fragments of either
the coding region or the related microRNA miR-1 into fertilized
mouse eggs (25). This microinjecting led to high levels of
expression of homologous RNA, resulting in an epigenetic
defect, cardiac hypertrophy. In this case, paramutation increased
rather than decreased expression of Cdk9.
Both miR-1 and miR-133 are proposed to regulate the
expression of growth-related genes. Intriguingly, a recent report
suggested that miR-1 and miR-133 might also have a distinct
role in the regulation of cardiomyocyte apoptosis: miR-1 seems
to be proapoptotic, whereas miR-133 appears antiapoptotic (26).
Moreover, in cell-based experiments, a recent study shows that
downregulation of miR-133b is sufficient to induce hypertrophic
gene expression while overexpression of miR-133b attenuates
aspects of b-AR-mediated changes in gene expression (17).
These studies show that miR-133 and miR-1 are key regulators
of cardiac hypertrophy, suggesting their fundamental role in the
development of disease and, as such, potential targets and/or
agents of novel therapies.
MicroRNAs AND MYOCARDIAL IFARCTION
Acute myocardial infarction (MI) due to coronary artery
occlusion is accompanied by a pathological remodeling
response that includes hypertrophic cardiac growth and fibrosis,
which impair cardiac contractility. Olson group show that MI in
mice and humans also results in the dysregulation of specific
miRNAs, which are similar to but distinct from those involved
in hypertrophy and heart failure (27). Among the MI-regulated
miRNAs are members of the miR-29 family, which are downre-
gulated in the region of the heart adjacent to the infarct. The
miR-29 family targets a cadre of mRNAs that encode proteins
involved in fibrosis, including multiple collagens, fibrillins, and
elastin. Downregulation of miR-29 with anti-miRs in vitro and
in vivo induces the expression of collagens, whereas overexpres-
sion of miR-29 in fibroblasts reduces collagen expression. So,
miR-29 acts as a regulator of cardiac fibrosis and represents a
potential therapeutic target for tissue fibrosis in general.
MicroRNAs-BASED THERAPEUTICS FOR HEARTDISEASE
The identification of microRNA as important regulators has
led to the development of many ideas by which these micro-
RNAs can be used as tools for disease therapy in the cardiovas-
cular system. First, it is apparent that miRNA expression pat-
terns are dynamically regulated during disease. Thus, it is likely
that miRNA expression patterns will be used for biomarkers or
diagnosis indicators and prognosis, as shown recently for
numerous forms of heart disease. Second, it is also conceivable
that miRNA mimics could be developed to enhance the expres-
sion of beneficial miRNAs. Customized anti-miRs or miR
mimics directed against specific mRNA targets can also be
envisioned. Third, chemically engineered oligonucleotides,
termed ‘antagomirs’ have been developed and proven to be effi-
cient and specific silencers of endogenous miRNAs in mice
569MicroRNAs IN CARDIAC HYPERTROPHY AND HEART FAILURE

(28). Chemical modifications and cholesterol conjugations have
been shown to stabilize and facilitate intravenous delivery of
antagomirs. This approach resulted in a marked reduction of the
corresponding miRNAs in different organs such as liver, lung,
kidney, skin, bone marrow, skeletal, and cardiac muscle. The
silencing effect was considerably sustained over time probably
because of a long half-life of endogenous miRNAs (13, 29).
Antagomirs interact with miRNAs in the cytoplasm and lead to
specific miRNA downregulation when injected systemically or
locally. However, this feature of miRNAs could be a two-edged
sword that brings about ‘off-target’ side effects. It is well
known that single miRNAs are predicted to have multiple
mRNA targets (many into the hundreds). So, specificity of
drug-like oligonucleotides is of great importance to minimize
off-target effects. Toxicity of chemical modifications used to
facilitate cellular uptake and prevent degradation also represents
an important consideration (30). Clearly, caution and future
studies directed at understanding the pathways regulated by car-
diac miRNAs are needed before clinical treatments.
CONCLUSION
Recent studies provide clear evidence that miRNAs modulate
a diverse spectrum of cardiac functions with developmental,
(patho)physiological, and clinical implications. The biology of
miRNAs in cardiovascular disease is a young research area and
an emerging field. Although much progress has been made to-
ward establishing miRNAs as important regulators in cardiovas-
cular biology, we are just beginning to understand this role of
novel gene regulators and further studies were needed. More
importantly, identifying their gene targets and signaling path-
ways responsible for their cardiovascular effects is critical for
future studies. Dissection and characterization of the signaling
pathways leading to cardiac hypertrophy has led to a wealth of
knowledge about this condition both physiological and patho-
logical. The role of miRNAs in the pathogenesis of the heart
and vessel points to a possibility of miRNAs as targets for treat-
ment of cardiovascular disease. Taken together, these recent
reports show that miRNA play a powerful role in cardiovascular
systems and are sure to open the door to previously unappreci-
ated medical therapies.
ACKNOWLEDGEMENTS
This work was financially supported by National Natural Sci-
ence Foundation of China (No.30800561) and Scientific
Research Foundation of Tianjin University of Science and
Technology (20080409).
REFERENCES1. Wightman, B., Ha, I., and Ruvkun, G. (1993) Posttranscriptional regula-
tion of the hetero-chronic gene Lin-14 by Lin-4 mediates temporal pat-
tern-formation in C. elegans. Cell 75, 855–862.
2. Berezikov, E., Guryev, V., van de Belt, J., Wienholds, E., Plasterk, R.
H., and Cuppen, E. (2005) Phylogenetic shadowing and computational
identification of human microRNA genes. Cell 120, 21–24.
3. Lewis, B. P., Burge, C. B., and Bartel, D. P. (2005) Conserved seed
pairing, often flanked by adenosines, indicates that thousands of human
genes are microRNA targets. Cell 120, 15–20.
4. Calin, G. A. and Croce, C. M. (2007) Chromosomal rearrangements and
microRNAs: a new cancer link with clinical implications. J. Clin.Invest. 117, 2059–2066.
5. Thum, T., Galuppo, P., Wolf, C., Fiedler, J., Kneitz, S., van Laake, L.
W., Doevendans, P. A., Mummery, C. L., Borlak, J., Haverich, A.,
Gross, C., Engelhardt, S., Ertl, G., and Bauersachs, J. (2007) Micro-
RNAs in the human heart: a clue to fetal gene reprogramming in heart
failure. Circulation 17, 258–267.
6. Sayed, D., Hong, C., Chen, I. Y., Lypowy, J., and Abdellatif, M. (2007)
MicroRNAs play an essential role in the development of cardiac hyper-
trophy. Circ Res. 16, 416–424.
7. van Rooij, E., Sutherland, L. B., Liu, N., Williams, A. H., McAnally, J.,
Gerard, R. D., Richardson, J. A., and Olson, E. N. (2006) A signature
pattern of stress-responsive microRNAs that can evoke cardiac hypertro-
phy and heart failure. Proc. Natl. Acad. Sci. USA 28, 18255–18260.
8. Thum, T., Gross, C., Fiedler, J., Fischer, T., Kissler, S., Bussen, M.,
Galuppo, P., Just, S., Rottbauer, W., Frantz, S., Castoldi, M., Soutschek,
J., Koteliansky, V., Rosenwald, A., Basson, M. A., Licht, J. D., Pena, J.
T., Rouhanifard, S. H., Muckenthaler, M. U., Tuschl, T., Martin, G. R.,
Bauersachs, J., and Engelhardt, S. (2008) MicroRNA-21 contributes to
myocardial disease by stimulating MAP kinase signalling in fibroblasts.
Nature 18, 980–984.
9. Rodriguez, A., Griffiths-Jones, S., Ashurst, J. L., and Bradley, A. (2004)
Identification of mammalian microRNA host genes and transcription
units. Genome Res. 14, 1902–1910.
10. Ruby, J. G., Jan, C. H., and Bartel, D. P. (2007) Intronic microRNA
precursors that bypass Drosha processing. Nature 448, 83–86.
11. Hutvagner, G. and Zamore, P. D. (2002) A microRNA in a multiple-
turnover RNAi enzyme complex. Science 297, 2056–2060.
12. Cheng, Y., Ji, R., Yue, J., Yang, J., Liu, X., Chen, H., Dean, D. B., and
Zhang, C. (2007) MicroRNAs are aberrantly expressed in hypertrophic
heart: do they play a role in cardiac hypertrophy? Am. J. Pathol. 170,1831–1840.
13. Thum, T., Catalucci, D., and Bauersachs, J. (2008) MicroRNAs: novel
regulators in cardiac development and disease. Cardiovasc. Res. 1, 562–570.
14. McKinsey, T. A. and Olson, E. N. (2005) Toward transcriptional thera-
pies for the failing heart: chemical screens to modulate genes. J. Clin.
Invest. 115, 538–546.15. Wang, Z., Luo, X., Lu, Y., and Yang, B. (2008) miRNAs at the heart
of the matter. J. Mol. Med. 86, 771–783.
16. Ikeda, S., Kong, S. W., Lu, J. Bisping, E., Zhang, H., Allen, P. D.,
Golub, T. R., Pieske, B., and Pu, W. T. (2007) Altered microRNA
expression in human heart disease. Physiol. Genomics 31, 367–373.
17. Sucharov, C., Bristow, M. R., and Port, J. D. (2008) miRNA expression
in the failing human heart: functional correlates. J. Mol. Cell. Cardiol.45, 185–192.
18. van Rooij, E., Sutherland, L. B., Qi, X., Richardson, J. A., Hill, J., and
Olson, E. N. (2007) Control of stress-dependent cardiac growth and
gene expression by a microRNA. Science 316, 575–579.
19. Chan, J. A., Krichevsky, A. M., and Kosik, K. S. (2005) MicroRNA-21
is an antiapoptotic factor in human glioblastoma cells. Cancer Res. 65,
6029–6033.
20. Cheng, A. M., Byrom, M. W., Shelton, J., and Ford, L. P. (2005) Anti-
sense inhibition of human miRNAs and indications for an involvement of
miRNA in cell growth and apoptosis. Nucleic Acids Res. 33, 1290–1297.
21. Tatsuguchi, M., Seok, H. Y., Callis, T. E., Thomson, J. M., Chen, J. F.,
Newman, M., Rojas, M., Hammond, S. M., and Wang, D. Z. (2007)
570 WANG ET AL.

Expression of microRNAs is dynamically regulated during cardiomyo-
cyte hypertrophy. J. Mol. Cell. Cardiol. 42, 1137–1141.
22. Care, A., Catalucci, D., Felicetti, F., Bonci, D., Addario, A., Gallo, P.,
Bang, M. L., Segnalini, P., Gu, Y., Dalton, N. D., Elia, L., Latronico,
M. V., Høydal, M., Autore, C., Russo, M. A., Dorn, G. W., Ellingsen,
O., Ruiz-Lozano, P., Peterson, K. L., Croce, C. M., Peschle, C., and
Condorelli, G. (2007) MicroRNA-133 controls cardiac hypertrophy.
Nat. Med. 13, 613–618.23. Duisters, R. F., Tijsen, A. J., Schroen, B., Leenders, J. J., Lentink, V.,
van der Made, I., Herias, V., van Leeuwen, R. E., Schellings, M. W.,
Barenbrug, P., Maessen, J. G., Heymans, S., Pinto, Y. M., and
Creemers, E. E. (2009) miR-133 and miR-30 regulate connective tissue
growth factor. Implications for a role of microRNAs in myocardial ma-
trix remodeling. Circ. Res. 104, 170–178.
24. Zhao, Y., Samal, E., and Srivastava, D. (2005) Serum response factor
regulates a muscle-specific microRNA that targets Hand2 during cardio-
genesis. Nature 436, 214–220.
25. Wagner, K. D., Wagner, N., Ghanbarian, H., Grandjean, V., Gounon,
P., Cuzin, F., and Rassoulzadegan, M. (2008) RNA induction and inher-
itance of epigenetic cardiac hypertrophy in the mouse. Dev. Cell. 14,962–969.
26. Xu, C., Lu, Y., Pan, Z., Chu, W., Luo, X., Lin, H., Xiao, J., Shan, H.,
Wang, Z., and Yang, B. (2007) The muscle-specific microRNAs miR-1
and miR-133 produce opposing effects on apoptosis by targeting
HSP60, HSP70 and caspase-9 in cardiomyocytes. J. Cell. Sci. 120,
3045–3052.
27. van Rooij, E., Sutherland, L. B., Thatcher, J. E., DiMaio, J. M.,
Naseem, R. H., Marshall, W. S., Hill, J. A., and Olson, E. N. (2008)
Dysregulation of microRNAs after myocardial infarction reveals a role
of miR-29 in cardiac fibrosis. Proc. Natl. Acad. Sci. USA. 2, 13027–
13032.
28. Krutzfeldt, J., Rajewsky, N., Braich, R., Rajeev, K. G., Tuschl, T., Man-
oharan, M., and Stoffel, M. (2005) Silencing of microRNAs in vivo
with ‘antagomirs’. Nature 438, 685–689.
29. Kim, V. N. (2005) MicroRNA biogenesis: coordinated cropping and
dicing. Nat. Rev. Mol. Cell. Biol. 6, 376–385.
30. van Rooij, E., Liu, N., and Olson, E. N. (2008) MicroRNAs flex their
muscles. Trends Genet. 24, 159–166.
571MicroRNAs IN CARDIAC HYPERTROPHY AND HEART FAILURE