Embed Size (px)
Citation preview

Robot-Assisted Partial Nephrectomy*
Shyam Sukumar, M.D., and Craig G. Rogers, M.D.
Abstract
Robot-assisted partial nephrectomy (RAPN) is a viable option for patients and surgeons who desire a minimallyinvasive alternative for the performance of nephron-sparing surgery (NSS). NSS has become the norm for themanagement of small renal masses. Numerous series have shown favorable outcomes for RAPN. RAPN has ashortened learning curve and eases the transition to minimally invasive NSS. We describe the indications,preparation, instrumentation, setup, technique, and complications for transperitoneal RAPN using a two- orthree-arm approach. We also suggest strategies and tips so that surgeons early in the learning curve caneffectively anticipate, avoid, and, if inevitable, manage complications.
Introduction
Radical nephrectomy has traditionally been consideredthe ‘‘gold standard’’ for the management of small renal
masses.1 With the recognition of the burden of occult renalinsufficiency at presentation2 and with the refinement insurgical techniques, however, partial nephrectomy has nowbecome the norm for the management of localized renal tu-mors.3,4 Evidence attesting to the underutilization of partialnephrectomy5,6 and the convalescence benefits of a minimallyinvasive approach have made minimally invasive partial ne-phrectomy an accepted alternative to open partial nephrec-tomy (OPN).
Laparoscopic partial nephrectomy (LPN) has been shownto have excellent functional and oncologic outcomes that arecomparable to those of open surgery.7,8 It is technically moredemanding to perform, however, and has a prohibitivelearning curve. Robot-assisted partial nephrectomy (RAPN)may help overcome the technical challenges of LPN and offersan easier transition to minimally invasive partial nephrecto-my.9 Numerous reports10–14 have discussed the outcomes ofRAPN with the da Vinci� Surgical System (Intuitive SurgicalInc, Sunnyvale, CA). RAPN has been shown to have ashortened learning curve.15,16 We describe our transperitonealtechnique for RAPN and discuss strategies for the preventionand management of complications.
Indications
Partial nephrectomy offers comparable oncologic outcomesto radical nephrectomy for small renal masses with the ad-vantage of preservation of renal function and improved
overall survival.2,17,18 Indications for partial nephrectomyinclude patients with bilateral tumors, renal insufficiency, anda solitary functioning kidney, but may also include patientswith a normal contralateral kidney. LPN has demonstratedsimilar oncologic outcomes to those of OPN with improvedconvalescence.4 RAPN may extend the benefits of a minimallyinvasive partial nephrectomy to a wider section of patientsand surgeons. All patients eligible for LPN are also candidatesfor RAPN.9 As surgeons have gained more experience, theindications for RAPN have broadened to include more chal-lenging cases—tumors > 4 cm, multiple tumors, hilar loca-tion, and completely endophytic masses.19–22
Contraindications
Renal insufficiency may be a relative contraindication, anda traditional open approach with cold ischemia should beconsidered. Extensive previous abdominal surgery is also arelative contraindication for a minimally invasive approach,although the feasibility of RAPN in selected patients withprevious abdominal surgery has been demonstrated.23
Preoperative workup and patient preparation
Patients who are being considered for RAPN should un-dergo a staging workup with an abdominal CT or MRI, andchest radiography. Clinical suspicion of advanced disease ormetastasis should entail additional imaging, such as a chestCT, head CT, and bone scan. A full blood workup with testsfor electrolytes, blood urea nitrogen, liver function, and co-agulation studies are also in order. Anticoagulants should bestopped 5 to 7 days before surgery. A bowel preparation, suchas magnesium citrate, may be administered the day before
Vattikuti Urology Institute, Henry Ford Hospital, Detroit, Michigan.*A coordinating article with video is available in Videourology 25=1 at www.liebertonline.com=vid=doi=full=10.1089=vid.2010.0117
JOURNAL OF ENDOUROLOGYVolume 25, Number 2, February 2011ª Mary Ann Liebert, Inc.Pp. 151–157DOI: 10.1089=end.2010.0672
151

surgery. On the night before surgery, patients are instructednot to drink or eat anything after midnight.
Instruments and equipment
The console surgeon may choose from a number of roboticinstruments (Intuitive Surgical Inc, Sunnyvale, CA) that servedifferent purposes. The surgeon may use the Hot Shears�
monopolar curved scissors or monopolar cautery hook in thedominant hand and the fenestrated bipolar grasper, Pro-Grasp,� or PK� dissecting forceps in the nondominant hand.Robotic instruments that are available for the optional thirdrobotic arm include the ProGrasp, double fenestrated grasper,and the dual blade retractor. Robotic needle driver(s) are usedfor sutured renal reconstruction. The nondominant handgrasping instruments may be used as a needle driver persurgeon preference to reduce cost.
The various robotic instruments offer different relativeadvantages. The monopolar curved scissors can be used fordissection, tumor excision, and cauterization. The monopolarhook may be used occasionally for blunt dissection of the hilarvessels and to delineate tissue planes. The ProGrasp or fen-estrated bipolar grasper instruments can both be useful for
atraumatic dissection of vessels and tumor, but the ProGraspis athermal. The fine tips of the PK dissecting forceps orMaryland bipolar forceps may be useful for precise cauter-ization of small vessels. The assistant uses a variety of lapa-roscopic instruments, including scissors, grasper, bulldog orSatinsky clamps, Hem-o-lok� clips and appliers (Teleflex,Research Triangle Park, NC), needle drivers, and a specimenretrieval bag.
Operative Technique
Patient positioning and trocar placement
After induction of general anesthesia, an orogastric tubeand Foley catheter are placed, and the patient is positioned inthe flank position with the affected side up. The table may bemildly flexed to increase the space for ports; however, thekidney rest is not used. All pressure points are padded, andthe patient is secured to the table with strong tape. Pneumo-peritoneum is achieved, and trocars are placed under direct
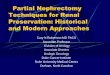
FIG. 1. Port placement for robot-assisted partial nephrec-tomy. C¼ camera port; R¼working robotic ports; 3rd¼third robotic arm; A¼ assistant port.
FIG. 2. Bowel mobilization. B¼ bowel.
FIG. 3. Renal hilar dissection. (a) Use of the third arm (arrow) to allow for two-handed hilar dissection; (b) Exposure ofrenal artery (RA) and renal vein (RV) for hilar clamping.
152 SUKUMAR AND ROGERS

vision. The 12-mm port for the robotic camera can be placedlaterally or medially per surgeon preference. Port positioningis demonstrated in Figure 1.
In the medial camera position, ports are placed at a wideangle toward the renal hilum. In the lateral camera position,the ports are placed in a diamond configuration with thecamera port closest to the kidney. A port for the third roboticarm may be placed in a caudal position away from otherports. Assistant ports are placed medially. For right-sidedcases, we have found a 15-mm assistant port to be useful for
facilitating faster needle exchanges, laparoscopic sponge andspecimen bag deployment. The robot is docked posteriorly ata slight angle over the shoulder.
Bowel mobilization
The colon is mobilized medially by incising along the whiteline of Toldt to expose the kidney (Fig. 2). A relatively avascularplane between the posterior mesocolon and the Gerota fascia isdeveloped using both sharp and blunt dissection. Attachmentsof the kidney to the spleen or liver are released. Care is taken toavoid inadvertent thermal injury to bowel or other structures.
Hilar dissection
With medial reflection of the colon, the ureter and the go-nadal vein are exposed. The ureter is lifted anteriorly offthe psoas muscle, and dissection proceeds cranially toward therenal hilum. The third robotic arm can be used to lift the kidneyanteriorly and place the hilum on stretch, allowing two-handeddissection of the renal hilum (Fig. 3a). The renal vein can beidentified by tracing the gonadal vein proximally to its insertionin the renal vein on the left side or to its insertion in the inferiorvena cava just caudal to the hilum on the right side. The renalartery is posterior to the renal vein. The hilar vessels are dis-sected in preparation for clamping (Fig. 3b). A laparoscopicDoppler probe (Vascular Technology Inc, Nashua, NH) can alsobe used to identify hilar vessels before clamping and to confirmadequate parenchymal ischemia after clamping (Fig. 4).
Tumor identification
The Gerota fascia is opened to expose the tumor along witha sufficient amount of normal parenchyma. Intraoperative
FIG. 4. Use of flexible Doppler ultrasonography under ro-botic control (arrow) to facilitate hilar dissection.
FIG. 5. TilePro display of intraoperative ultrasonographic image to help locate and delineate tumor. Arrows indicatelocation of tumor. P¼ laparoscopic ultrasound probe. (Aloka, Tokyo, Japan)
ROBOT-ASSISTED PARTIAL NEPHRECTOMY 153

ultrasonography is important for accurate identification of thelocation, depth, and borders of the tumor, thereby ensuringcomplete oncologic control with negative margins. A lapa-roscopic ultrasound probe is introduced through the assistantport. The live intraoperative images are displayed as a pictureon picture display on the console screen using the TilePro�functionality24 (Fig. 5). The margins of resection are scored withcautery after demarcating them with the ultrasound probe.
Hilar clamping
Before clamping, all necessary material, including stitchesand instruments, are ensured to be at hand so that resectionand renorrhaphy can be performed efficiently under warmischemia. Intravenous mannitol may be administered beforeclamping to facilitate osmotic diuresis to aid in renal protec-tion. Hilar clamping can be performed using either laparo-scopic bulldog clamps or a Satinsky clamp. If bulldog clampsare used, the renal artery is clamped first, followed by the vein(Fig. 6). For select exophytic tumors, resection may be per-formed with just the renal artery clamped or without hilarclamping. For endophytic, larger, or centrally placed tumors,both the renal artery and vein are clamped. The Satinksyclamp needs a dedicated port, and care must be taken to avoid
collisions with other instruments. Robotic bulldog clamps,applied by the console surgeon using the robotic ProGrasp,are also available (Klein Surgical Inc., San Antonio, TX andScanlan International, St. Paul, MN).
Tumor excision
Sharp cold excision of the tumor is carried out with anadequate margin of normal parenchyma (Fig. 7). The mag-nification that is afforded by the stereoscopic robotic camera issufficient to identify collecting system entry without a ureteralcatheter in most cases, but preplacement of a ureteral cathetermay be used per surgeon preference. The assistant uses suc-tion to ensure visualization and to provide counter traction.The resected tumor is then placed aside for later retrieval.
Renal reconstruction
The robotic instruments are then replaced by robotic needledrivers for sutured renal reconstruction. Renorrhaphy isperformed in two layers. All sutures are anchored with aknot and a Hem-o-lok clip and are secured using the slidingHem-o-lok clip technique.25 The base of the resection bed issutured. This deep layer closure may be performed with apoliglecaprone or polyglactin suture in a running fashion,
FIG. 6. (a) Renal vein clamping using laparoscopic bulldog clamps (solid arrow) after clamping of the renal artery (brokenarrow). (b) Robotic bulldog clamps applied by console surgeon using robotic ProGrasp.
FIG. 7. Tumor excision. FIG. 8. Inner layer renorrhaphy.
154 SUKUMAR AND ROGERS

incorporating vessels and repairing the collecting system de-fects (Fig. 8). The renal capsule is closed using larger suturesand needles and secured with Hem-o-lok clips (Fig. 9). Aftertightening the Hem-o-lok clips, additional throws may beplaced in a running or mattress fashion. With polyglactinrenorrhaphy, additional clips may be needed to anchor theclips to prevent them from sliding back.
A recent modification is to use barbed suture for renor-rhaphy (V-loc, Covidien, Mansfield, MA, or Quill SRS, An-giotech Pharmaceuticals Inc, Vancouver, British Columbia,Canada), which allows for efficient two-handed renorrhaphywithout the need to maintain tension on throws and withoutslippage of sutures or clips (Fig. 10).
Removal of hilar clamps
After completing the renorrhaphy, hilar clamps are re-moved. If bulldog clamps were used, the venous clamp isremoved first, followed by the arterial clamp. If oozing ispresent, a laparoscopic sponge can be used to apply pressureand the Hem-o-lok clips can be retightened. A second dose ofmannitol may be given after hilar unclamping.
Specimen retrieval
A laparoscopic extraction bag is inserted through an as-sistant port, and the specimen is retrieved. A Jackson-Pratt
drain can be placed through a lateral port. The specimen isextracted from the assistant port incision, and the fascia andskin are closed.
Postoperative care
Serial hemoglobin levels are followed in the recovery roomand postoperative period. Intravenous fluids, analgesics, an-tibiotics, and prophylaxis for deep vein thrombosis are ad-ministered as per institutional protocol. On the morning aftersurgery, the Foley catheter is removed, ambulation begins,and the diet is advanced. The drain is observed for output,and the drain fluid is sent for determination of a creatininelevel. If no creatinine elevation is noted, the drain may beremoved. The length of stay is usually about 2 days.
Management of Complications
Hemorrhage
Careful dissection and good exposure can help preventsignificant intraoperative hemorrhage. Venous bleeding canusually be controlled by direct pressure with a sponge or in-strument while the insufflation pressure is increased. Smallbleeders can be cauterized or clipped, but sutured repairmay be indicated for larger vascular injuries. Renal paren-chymal bleeding during hilar clamping may occur because of
FIG. 9. Capsular renorrhaphy.(a) A CT-1 needle passedthrough renal capsule toclose defect; (b) Sliding cliprenorrhaphy technique tosecure sutures.
FIG. 10. Barbed suture. (a) Inner renorrhaphy suture: A six inch 3-0 V-loc suture on a V-20 needle (26 mm tapered, similar toan SH needle). A knot (arrowhead) and Hem-o-lok clip (arrow) have been placed to anchor the initial throw outside the renalcapsule; (b) Outer capsular suture: Twelve inch 2-0 V-loc suture on GS-21 needle (36 mm tapered, similar to a CT-1 needle)cut to 7 to 8 inches and anchored with a knot (arrowhead) and Hem-o-lok clip (arrow).
ROBOT-ASSISTED PARTIAL NEPHRECTOMY 155

insufficient arterial occlusion or unclamped accessory vessels.The renal vein may be unclamped to reduce renal congestion.The hilum may be occluded en bloc with a Satinsky clamp or along bulldog clamp. Inadequate renorrhaphy may result inbleeding after the hilum is unclamped. Pneumoperitoneummay be transiently increased and direct compression appliedwhile the sliding clip renorrhaphy clips are retightened. Thesurgeon should be prepared for open conversion for uncon-trolled bleeding.
A fall in serial hematocrit values relative to baseline post-operative levels along with clinical symptoms usually heraldspostoperative hemorrhage. Close monitoring of vital signs andtranfusions as needed are usually sufficient for postoperativebleeding. Delayed postoperative hemorrhage may result froma pseudoaneurysm or arteriovenous fistula and may presentas gross hematuria. It is important to suspect a vascular com-plication when a patient presents postoperatively with hema-turia. CT=MR angiography may be used as an initial diagnostictest for mild hematuria. More pronounced bleeding shouldbe managed by renal angiography with the option of an-gioembolization in the same setting. Operative explorationand, possibly, a nephrectomy may be the only recourse ifangioembolization fails to control bleeding.
Bowel injury
Unrecognized bowel injury is a potential complication ofany abdominal procedure and may occur from port or in-strument insertion or from cautery. Bowel injuries that arerecognized intraoperatively necessitate immediate repair,and there should be a low threshold for an intraoperativegeneral surgery consultation. Postoperatively, clinical signsof a bowel injury could include trocar site pain, abdominaldistention, nausea, enteric output from a drain, fever, andleukocytosis. A CT scan with oral and intravenous contrastmay help identify an injury and recognize intra-abdominalcollections.
Urine leak
If there is clinical evidence of a urine leak postoperatively(elevated drain creatinine levels, high drain output, etc.), thedrain should be left in place and the urine output monitored.CT urography should be considered for persistent leakage orsymptoms to assess for an urinoma and to ascertain the po-sition of the drain relative to the collection. The position of thedrain may need to be changed or a percutaneous drain placedif there is an undrained collection. Serial imaging may be used
to monitor for resolution of the urinoma. Retrograde place-ment of a ureteral stent should be considered if there is per-sistent high volume drainage or evidence of distal obstructionon the CT urogram.
Review of the Literature
A brief description of selected major published series isshown in Table 1 (in chronologic order). RAPN appears tohave a shorter learning curve when compared with alterna-tive minimally invasive techniques.15,16 Outcomes frommultiple series10–13,26 have confirmed the safety and feasibil-ity of RAPN in the management of small renal masses, in-cluding complex renal tumors.19–22 Recent comparativestudies12,13 have demonstrated favorable-to-equivalent out-comes for RAPN when compared with LPN, particularly inregard to decreased warm ischemia time. Novel technicaldevelopments include use of TilePro,24 the third roboticarm,24 sliding-clip renorrhaphy,25 laparoscopic Doppler ul-trasonography,27 and selective clamping techniques.28
Conclusion
RAPN is a safe and feasible alternative for minimally in-vasive NSS with a shorter learning curve than LPN. RAPNextends the benefits of minimally invasive NSS to a widersection of surgeons and patients and may be an acceptablealternative to LPN for small renal masses.
Disclosure Statement
No competing financial interests exist.
References
1. Robson CJ, Churchill BM, Anderson W. The results of rad-ical nephrectomy for renal cell carcinoma. J Urol 1969;101:297–301.
2. Huang WC, Levey AS, Serio AM, et al. Chronic kidneydisease after nephrectomy in patients with renal corticaltumours: A retrospective cohort study. Lancet Oncol 2006;7:735–740.
3. Gill IS, Aron M, Gervais DA, Jewett MA. Clinical practice.Small renal mass. N Engl J Med 2010;362:624–634.
4. Fergany AF, Hafez KS, Novick AC. Long-term results ofnephron sparing surgery for localized renal cell carcinoma:10-year followup. J Urol 2000;163:442–445.
5. Hollenbeck BK, Taub DA, Miller DC, et al. Nationalutilization trends of partial nephrectomy for renal cell
Table 1. Summary of Major Published Series
Variable Rogers19 Aron14 Rogers10 Benway13 Wang12 Benway11
Number of cases 14 12 148 129 40 183Mean tumor Size (cm) 2.4 2.4 2.8 2.9 2.5 2.9Mean operative time 192 242 197 189 140 210Mean EBL (mL) 230 329 183 155 136 131.5Mean WIT (min) 31 23 27.8 19.7 19 23.9Mean LOS (d) 2.6 4.7 1.9 2.4 2.5 NRComplications (%) 0 4 9 (6.1) 11 (8.5) 8 (20) 15 (8.2)Positive margin (%) 0 none 6 (4) 5 (3.9) 1 7 (3.8)Mean follow-up (months) 3 7.4 18 (12–23) NR NR 16
EBL¼ estimated blood loss; WIT¼warm ischemia time; LOS¼ length of stay.
156 SUKUMAR AND ROGERS

carcinoma: A case of underutilization? Urology 2006;67:254–259.
6. Miller DC, Hollingsworth JM, Hafez KS, et al. Partial ne-phrectomy for small renal masses: An emerging quality ofcare concern? J Urol 2006;175:853–858.
7. Allaf ME, Bhayani SB, Rogers C, et al. Laparoscopic partialnephrectomy: Evaluation of long-term oncological outcome.J Urol 2004;172:871–873.
8. Lane BR, Gill IS. 5-Year outcomes of laparoscopic partialnephrectomy. J Urol 2007;177:70–74.
9. Rogers CG, Patard JJ. Open to debate. The motion: Roboticpartial nephrectomy is better than open partial nephrec-tomy. Eur Urol 2009;56:568–570.
10. Rogers CG, Menon M, Weise ES, et al. Robotic partial ne-phrectomy: A multiinstitutional analysis. J Robotic Surg2008;2:141–143.
11. Benway BM, Bhayani SB, Rogers CG, et al. Robot-assistedpartial nephrectomy: An international experience. Eur Urol2010;57:815–820.
12. Wang AJ, Bhayani SB. Robotic partial nephrectomy versuslaparoscopic partial nephrectomy for renal cell carcinoma:Single-surgeon analysis of > 100 consecutive procedures.Urology 2009;73:306–310.
13. Benway BM, Bhayani SB, Rogers CG, et al. Robot assistedpartial nephrectomy versus laparoscopic partial nephrec-tomy for renal tumors: a multi-institutional analysis ofperioperative outcomes. J Urol 2009;182:866–872.
14. Aron M, Koenig P, Kaouk JH, et al. Robotic and laparoscopicpartial nephrectomy: A matched-pair comparison from ahigh-volume centre. BJU Int 2008;102:86–92.
15. Mottrie A, De Naeyer G, Schatteman P, et al. Impact of thelearning curve on perioperative outcomes in patients whounderwent robotic partial nephrectomy for parenchymalrenal tumours. Eur Urol 2010;58:127–132.
16. Deane LA, Lee HJ, Box GN, et al. Robotic versus standardlaparoscopic partial=wedge nephrectomy: A comparison ofintraoperative and perioperative results from a single insti-tution. J Endourol 2008;22:947–952.
17. Huang WC, Elkin EB, Levey AS, et al. Partial nephrectomyversus radical nephrectomy in patients with small renal tu-mors—is there a difference in mortality and cardiovascularoutcomes? J Urol 2009;181:55–62.
18. Thompson RH, Boorjian SA, Lohse CM, et al. Radical ne-phrectomy for pT1a renal masses may be associated withdecreased overall survival compared with partial nephrec-tomy. J Urol 2008;179:468–473.
19. Rogers CG, Singh A, Blatt AM, et al. Robotic partial ne-phrectomy for complex renal tumors: Surgical technique.Eur Urol 2008;53:514–521.
20. Rogers CG, Metwalli A, Blatt AM, et al. Robotic partial ne-phrectomy for renal hilar tumors: multi-institutional analy-sis. J Urol 2008;180:2353–2356.
21. Patel MN, Krane LS, Bhandari A, et al. Robotic partial ne-phrectomy for renal tumors larger than 4 cm. Eur Urol2010;57:310–316.
22. Gong Y, Du C, Josephson DY, et al. Four-arm robotic partialnephrectomy for complex renal cell carcinoma. World J Urol2010;28:111–115.
23. Petros FG, Patel MN, Kheterpal E, et al. Robotic partial ne-phrectomy in the setting of prior abdominal surgery. BJU Int2010. In press.
24. Rogers CG, Laungani R, Bhandari A, et al. Maximizingconsole surgeon independence during robot-assisted renalsurgery by using the Fourth Arm and TilePro. J Endourol2009;23:115–21.
25. Benway BM, Wang AJ, Cabello JM, Bhayani SB. Roboticpartial nephrectomy with sliding-clip renorrhaphy: Techni-que and outcomes. Eur Urol 2009;55:592–599.
26. Scoll BJ, Uzzo RG, Chen DY, et al. Robot-assisted partialnephrectomy: A large single-institutional experience. Urol-ogy 2010;75:1328–1334.
27. Hyams ES, Kanofsky JA, Stifelman MD. LaparoscopicDoppler technology: Applications in laparoscopic pyelo-plasty and radical and partial nephrectomy. Urology 2008;71:952–956.
28. Viprakasit DP, Altamar HO, Miller NL, Herrell SD. Selectiverenal parenchymal clamping in robotic partial nephrectomy:Initial experience. Urology. 2010;76:750–753.
Address correspondence to:Craig G. Rogers, M.D.
Vattikuti Urology InstituteHenry Ford Health System2799 W. Grand Boulevard
Detroit, MI-48202
E-mail: [email protected]
Abbreviations Used
CT¼ computed tomographyLPN¼ laparoscopic partial nephrectomyNSS¼ nephron-sparing surgery
OPN¼ open partial nephrectomyMR¼magnetic resonance
MRI¼magnetic resonance imagingRAPN¼ robot-assisted partial nephrectomy
ROBOT-ASSISTED PARTIAL NEPHRECTOMY 157