Embed Size (px)
DESCRIPTION
Regional anaesthesia
Citation preview
Tutorial COMPACTMehrkens H.-H., Geiger P., Winckelmann J.Department of Anesthesiology/Intensive Care Medicine and Pain TherapyUlm Rehabilitation Hospital and University Clinic
PERIPHERAL REGIONAL ANAESTHESIA
2nd Expanded Edition
RKU_Umschlag_eng2.indd 1 18.08.09 14:04

Preface
After so many of our colleagues have expressed the wish for a pocket edition of our Peripheral Regional Anesthesia Tutorial published by the Ulm Reha-bilitation Hospital (RKU), we have now complied by offering this compact version. The fundamentals contained in this condensed guide still grow from the now almost 20 years of clini-cal and practical experience gained in our hospital. This book differs from the previous, more comprehensive Tutorial Script in that it includes many new developments and supplemental information. These shall be incorporated into the next edition of the tutorial script and its coming Internet version.
It is here that I would like to extend my very special thanks to the managing Senior Physician of our Department, Dr. Peter Geiger. Without his tireless assistance, the production of the compact version of this pocket tutorial would not have been possible. Additional thanks go to B. Braun Melsungen, whose continuing technical and financial support have been invalu-able for the completion of this work.
Ulm, June 2004 Prof. H.-H. Mehrkens, M.D.
Prof. H.-H. Mehrkens, M.D. Director, Dept. of Anesthesiology/Intensive Care Medicine
RKU_Compact_e_V6_neu.indd 1 21.09.09 14:00
2
Preface to the 2nd Expanded Edition
Now, five years after the first pocket edition of the “Peripheral Regional An-esthesia Tutorial” appeared, the time is right to pay tribute to the rapid-paced developments taking place in this field of medicine. In doing so, we have made special efforts to include ultrasound-guided nerve block techniques when-ever we felt it was sensible. Certainly, our daily routine has become unimagi-nable without visualization of the nerves we want to block. At the same time, we believe that nerve stimulation and ultrasonographic visualization are not competing methods. In-deed, seeing as not every block is equally suited for one or the other of the two, a command of both is required. In many cases, combining ultrasound with nerve stimulation yields major advan-tages.
Nerve blocks guided by ultrasound thrive on visual dynamics. For that reason, we have intentionally refrained from using static pictures of needle positions or of the local anaesthetic’s spread around the target structures. Instead, this booklet has placed par-ticular emphasis on the “ultrasonographic normal situs” at typical puncture sites, which should assist the reader in identifying key structures. Motion images shall be made available on an updated Tutorial DVD soon.
P. M. Geiger, M.D. Medical Director, Department of Anesthesiology/Intensive Care Medicine and Pain Therapy
RKU_Compact_e_V6_neu.indd 2-3
3
-e , -
. c d -l
y d
It is here that I would like to extend my special thanks to Prof. H.-H. Mehrkens, MD, my predecessor and the initiator of the “Tu-torial Series”, who regularly takes time off from his retirement to lend us his valuable advice. My managing senior physician, Dr. Jörg Winckelmann, also deserves great recognition for his untir-ing commitment to the production of this new edition. Not least, I would like to thank B. Braun Melsungen AG: without the com-pany’s support, this project would not have been possible. We authors hope that this current pocket-sized version will be used effectively and we are equally looking forward, as in the past, to its readers’ critiques and constructive suggestions on the Internet Forum www.nerveblocks.net.
Ulm, August 2009 P. M. Geiger, MD
21.09.09 14:00
4
General
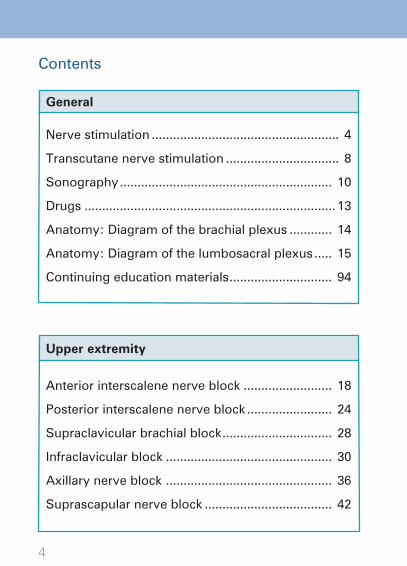
Contents
Nerve stimulation ..................................................... 4
Transcutane nerve stimulation ................................ 8
Sonography ............................................................ 10
Drugs ....................................................................... 13
Anatomy: Diagram of the brachial plexus ............ 14
Anatomy: Diagram of the lumbosacral plexus ..... 15
Continuing education materials ............................. 94
Upper extremity
Anterior interscalene nerve block ......................... 18
Posterior interscalene nerve block ........................ 24
Supraclavicular brachial block ............................... 28
Infraclavicular block ............................................... 30
Axillary nerve block ............................................... 36
Suprascapular nerve block .................................... 42
RKU_Compact_e_V6_neu.indd 4-5
5
Lower extremity
Psoas compartment block .................................... 46
Femoral nerve block ............................................. 50
Saphenous nerve block ........................................ 56
Obturator nerve block ........................................... 62
Parasacral sciatic nerve block .............................. 68
Transgluteal sciatic nerve block ........................... 72
Anterior sciatic nerve block .................................. 76
Subtrochanteric sciatic nerve block ..................... 80
Lateral distal sciatic nerve block ........................... 84
Popliteal sciatic nerve block .................................. 90
21.09.09 14:00
6
Nerve stimulation
Catheter technique
•Unipolarneedlesinaplasticintroducerofvaryinglengths e.g.: Contiplex® D Sets with a flexible and non-wired catheter or Contiplex® S (B. Braun Melsungen AG)
Single shot technique
•Unipolarneedlesofvaryinglength e.g., Stimuplex® D or Stimuplex® D Plus for ultrasound-
guided nerve blocks (B. Braun Melsungen AG)
Nerve stimulator
• Currentrangefrom1.0–0.1mA• Pulseduration0.1ms(mixednerve)
1.0 ms (sensory nerve)• Constantsquarewavepulseoverawideimpedancerange
e.g. Stimuplex® HNS 11 and Stimuplex® HNS 12 (B. Braun Melsungen AG)
RKU_Compact_e_V6_neu.indd 6-7
7
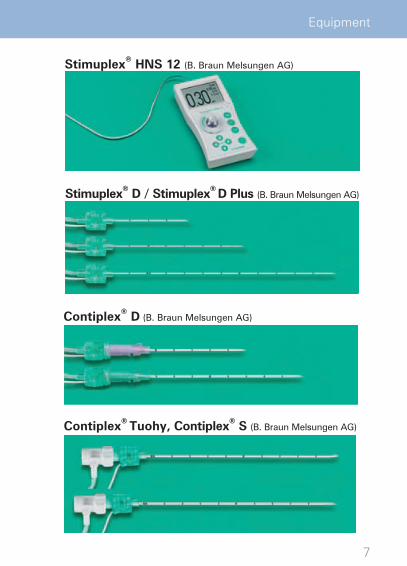
Equipment
Contiplex® D (B. Braun Melsungen AG)
Stimuplex® HNS 12 (B. Braun Melsungen AG)
Contiplex® Tuohy, Contiplex® S (B. Braun Melsungen AG)
Stimuplex® D / Stimuplex® D Plus (B. Braun Melsungen AG)
21.09.09 14:00

8
Transdermal nerve stimulation
Stimulation and injection technique
1. Initial current 1.0 mA
2. Pulse duration 0.1 ms (mixed nerve) or
3.Thresholdcurrent0.3–0.2mA
4.Aspirationtest5–10mlLAinjectedslowly
5. Increase to 1.0 mA initial current No stimulatory response
6. Administration of remaining LA 1.0 mA
7. Catheter placement after primary LA administration
Upper extremity: Approx. 3 cm beyond the end of the introducer sheath
Lower extremity: Approx. 4 cm beyond the end of the introducer sheath
8. Catheter aspiration test
Recurring stimulatory response: may indicate (partial) intra-vascular needle position. Attempt careful aspiration, perform reinjection slowly with constant verbal moni-toring.
use the SENS mode setting on the stimulator
RKU_Compact_e_V6_neu.indd 8-9
9
Block technique
•Prerequisite:superficiallocationofthenerves•Changethesettingsonthenervestimulatorto:Pulseduration1.0ms,baselineamplitude2.5–3.0mA,•Goodconductivityofthepentip(electrodegel,water)•Continuousimpedancedisplay(HNS12)canbehelpfulas
an indirect measure of “unimpeded” current flow
Technique
Areas of application
•Forprimaryorientationbeforeblockinganerve•Todemonstratespecificstimulatoryresponses(for training purposes)
Stimuplex® Pen / Stimuplex® Guide
The Stimuplex Pen can be used together with the nerve stimulator to locate nerves transdermally and to trigger the corresponding motor response.PEG (Percutaneous Electrode Guidance)The Stimuplex® Guide first induces percutaneous stimulation with the sterile needle and then the actual nerve block.
21.09.09 14:00
10
Sonography
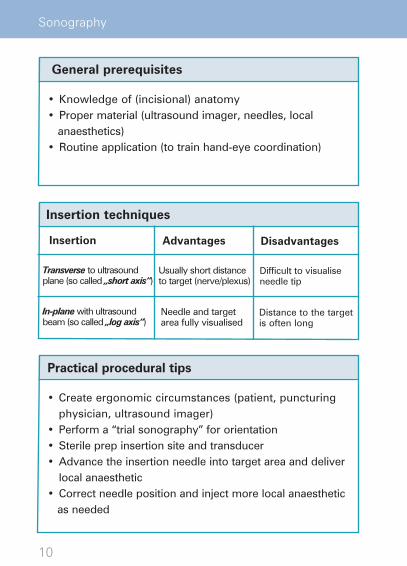
Practical procedural tips
•Createergonomiccircumstances(patient,puncturingphysician, ultrasound imager)
• Performa“trialsonography”fororientation•Sterileprepinsertionsiteandtransducer•Advancetheinsertionneedleintotargetareaanddeliver
local anaesthetic•Correctneedlepositionandinjectmorelocalanaesthetic as needed
Transverse to ultrasound plane (so called „short axis“)
In-plane with ultrasound beam (so called „log axis“)
General prerequisites
•Knowledgeof(incisional)anatomy•Proper material (ultrasound imager, needles, local anaesthetics)•Routine application (to train hand-eye coordination)
Distance to the targetis often long
Usually short distance to target (nerve/plexus)
Difficult to visualise needle tip
Needle and target area fully visualised
Advantages DisadvantagesInsertion
Insertion techniques
RKU_Compact_e_V6_neu.indd 10-11


11
Technique
Short axis (out-of-plane technique)
Long axis (in-plane technique)
21.09.09 14:00
12
Equipment
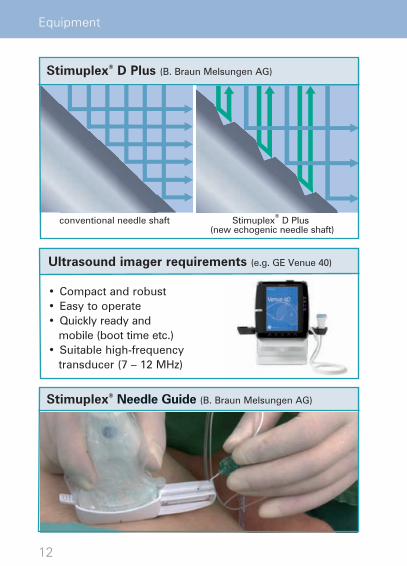
Stimuplex® D Plus (B. Braun Melsungen AG)
Stimuplex® Needle Guide (B. Braun Melsungen AG)
Ultrasound imager requirements (e.g. GE Venue 40)
•Compactandrobust•Easytooperate•Quicklyreadyand mobile (boot time etc.)•Suitablehigh-frequencytransducer(7–12MHz)
conventional needle shaft Stimuplex® D Plus
(new echogenic needle shaft)
RKU_Compact_e_V6_neu.indd 12-13

13
Drugs
Drugs
Conventional, medium-acting local anesthetics (LA) like• prilocaine•mepivacaine
and long-acting ones like • ropivacaine• bupivacaine.
For anesthesia, we prefer a combination of • prilocaine1%(20–40ml)andropivacaine0.5–0.75% (10–20ml).
This combination has the advantage that a LA with com-parably low toxicity is given primarily and inadvertent intravascular injections mostly occur during the prodromal stage. Subsequently, a long-acting LA is administered to achieve a blockade of sufficient duration.
Foranalgesia,0.2%ropivacaineisgenerallyadministered.The preferred mode of delivery is through a PCA pump equipped with basal rate and bolus settings or by continu-ous infusion through the nerve catheter. Intermittant bolus injections are rarely used.
21.09.09 14:00
14
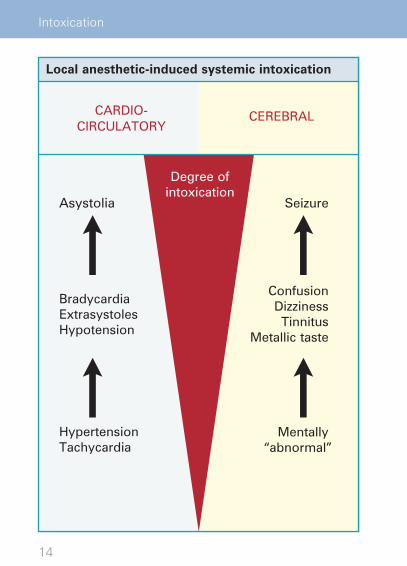
Intoxication
CARDIO-CIRCULATORY
CEREBRAL
Asystolia
BradycardiaExtrasystolesHypotension
HypertensionTachycardia
Seizure
ConfusionDizzinessTinnitus
Metallic taste
Mentally “abnormal”
Degree ofintoxication
Local anesthetic-induced systemic intoxication
RKU_Compact_e_V6_neu.indd 14-15

15
Drugs
21.09.09 14:00
16
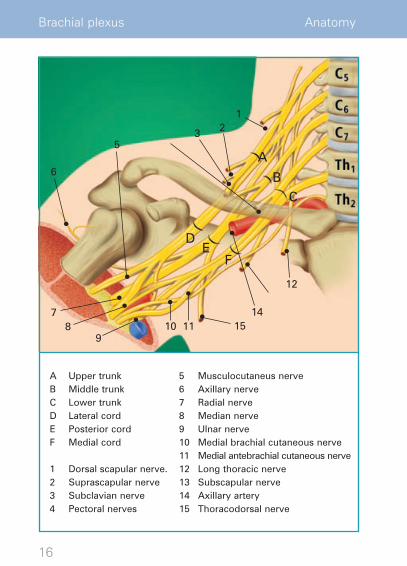
A Upper trunkB Middle trunkC Lower trunkD Lateral cordE Posterior cordF Medial cord
1 Dorsal scapular nerve.2 Suprascapular nerve3 Subclavian nerve4 Pectoral nerves
5 Musculocutaneus nerve6 Axillary nerve7 Radial nerve 8 Median nerve9 Ulnar nerve10 Medial brachial cutaneous nerve11 Medial antebrachial cutaneous nerve 12 Long thoracic nerve13 Subscapular nerve14 Axillary artery15 Thoracodorsal nerve
Brachial plexus Anatomy
A
BC
DE
F
123
5
6
78
910 11
12
1415
RKU_Compact_e_V6_neu.indd 16-17

17
1 Lateral femoral cutaneous nerve
2 Femoral nerve
3 Genitofemoral nerve
4 Sciatic nerve
5 Obturator nerve
6 Pudendal nerve
Lumbosacral plexus Anatomy
1
2
3
4 5 6
21.09.09 14:00

18
Nerve stimulation
Approach according to Meier
Contraindications
•Contralateralphrenicandrecurrentparesis
Side effects / complications
•Horner´ssyndrome•Phrenicparesis•Recurrentparesis•Vesselpuncture(externaljugularvein)
Anatomical landmarks
•Sternocleidomastoidmuscle•Superiorthyroidnotch•Scalenusgap•VIB(verticalinfraclavicularblockade)point
Indications
•Operativeproceduresontheshoulder,proximalupperarm and lateral clavicle
•Analgesia
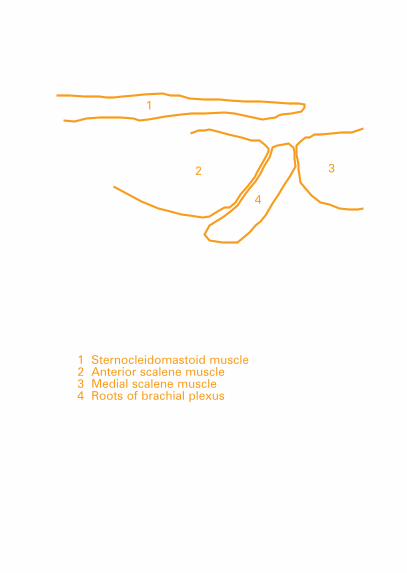
1 Sternocleidomastoid muscle,
2 Thyroid notch, 3 Puncture site
RKU_Compact_e_V6_neu.indd 18-19

19
1
23
Anterior interscalene nerve block
Anatomical landmarks
21.09.09 14:00
20
Nerve stimulation
Blockade technique The patient lies supine, head turned slightly to contralateral side, shoulder and arm positioned comfortably.
Puncture site:Posterior edge of the sternocleidomastoid muscle at the level ofthethyroidnotch(1.5–2cmabovethecricoid).Insertiondirection tangential to the course of the plexus in the direction of the VIB point or anterior axillary line.
Puncturedepth:2–4cm.
Positive stimulatory response from the upper trunk (lateral cord): biceps and/or brachial muscle.
Dosage
20–40mlLA
Catheter technique
e.g. Contiplex® D-Set, 55 mmAdvance the soft plastic catheter max. 3 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex® D, 50 mm
RKU_Compact_e_V6_neu.indd 20-21
21
?contralateral
level
direction
(lateral
What to do when ...?
Stimulation of the axillary nerve (deltoid mus-cle) or radial nerve (triceps muscle) occurs:Leave the needle in place u Administer LA.
Stimulation of the suprascapular nerve (leva-tor scapulae muscle) occurs: The insertion direction is too lateral and dorsal u Retract the needle, advance it markedly more to the ventral and somewhat more medial.
Stimulation of the phrenic nerve (unilateral singultus) occurs: The insertion direction is too ventral and medial u Retract the needle, ad-vance it slightly more to the lateral and dorsal.
Blood is aspirated: Retract the needle, check direction of puncture u Readvance needle.
Potential errors and hazards
Always avoid a medial direction of puncture:•Riskofpuncturinglargevessels(carotidand
vertebral arteries, internal jugular vein).•Riskofintrathecalinjection=highspinal!
(Most suitable and reliable stimulatory response: bicepsand/orbrachialmuscle=mostlateralpart of plexus [C5])
Anterior interscalene nerve block
!
?
21.09.09 14:00

22
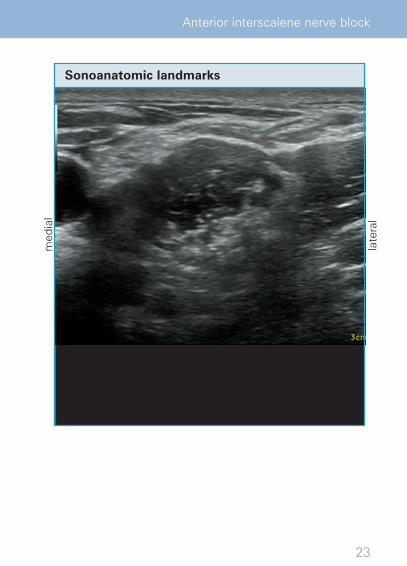
Sonography
Nerve block techniqueShort axis is preferable (catheter placement), long axis possiblefor Single shot
Sonoanatomic landmarks:- Sternocleidomastoid muscle- Scalenus anterior and scalenus medius muscles- Nerve roots of the brachial plexus
Blockade objective:Infiltrateatleastthesuperiorroots(C5–C7)withlocalanaes-thetic. As a general rule, 15 - 20 ml will suffice.
Practical tip:The ideal insertion site is most successfully located by tilting the transducer from the supraclavicular to the interscalene position, following the plexus fibres.
RKU_Compact_e_V6_neu.indd 22-23
23
-
e ,
Anterior interscalene nerve block
Sonoanatomic landmarks
med
ial
late
ral
21.09.09 14:01

24
Nerve stimulation
Approach according to Pippa
Contraindications
•Contralateralphrenicandrecurrentparesis
Side effects / complications
•Horner´ssyndrome•Phrenicparesis•Recurrentparesis•Vesselpuncture
Indications
•Operativeproceduresontheshoulder,proximalupperarm and lateral clavicle
•Analgesia
Anatomical landmarks
•SpinousprocessC7(vertebraprominens)•SpinousprocessC6•Cricoid•Sternocleidomastoidmuscle
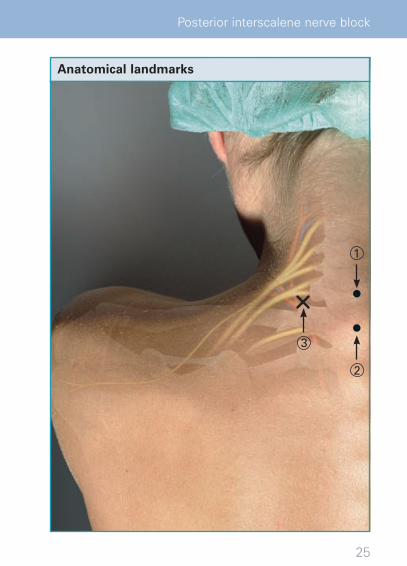
1 C6, 2 C7, 3 Puncture site
RKU_Compact_e_V6_neu.indd 24-25
25
site
1
2
3
Posterior interscalene nerve block
Anatomical landmarks
21.09.09 14:01

26
Nerve stimulation
Blockade technique Patient is in axially aligned recumbent position (or seated); the cervical spine is flexed backwards; shoulder and arm are relaxed.
Puncture site:3 cm midline between the two spinous processes C6 and C7, Insertiondirection5–10°tothelateral,aimedattheheightofthe cricoid.
Puncturedepth:6–8cm,dependingonthedistancebetweenpuncture site and posterior edge of the sternocleidomastoid muscle.
A promising stimulatory response elicited from the upper trunk (lateral sheath): biceps muscle and/or brachial muscle and/or deltoid muscle.
Dosage
30–50mlLA
Catheter technique
e.g. Contiplex®D-Set,80–110mmAdvance the soft plastic catheter max. 3 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex®D,80–100mm
RKU_Compact_e_V6_neu.indd 26-27

27
?; e
, f
d
k r
What to do when ...?
Stimulation of the axillary nerve (deltoid mus-cle) or radial nerve (triceps muscle) occurs:Leave needle in situ u Inject a slow, fraction-ated dose of local anaesthetic.
Stimulation of the suprascapular nerve (leva-tor scapulae muscle) occurs: Insertion direc-tion too lateral u Retract the needle, advance it slightly to the medial and slightly deeper.
Stimulation of the phrenic nerve (unilateral singultus) occurs: Insertion direction too deep and too medial uRetract the needle, advance it more to the lateral and less deep.
Blood is aspirated: retract the needle, check puncture direction uReadvance the needle.
Potential errors and hazards
Always avoid a medial insertion direction:•Riskofpuncturingthevertebralartery.•Riskofintrathecalinjection=highspinal!
(Most suitable and reliable stimulatory re-sponse: bicepsand/orbrachialmuscle=mostlateralpart of plexus [C5])
Posterior interscalene nerve block
!
?
21.09.09 14:01

28
Sonography
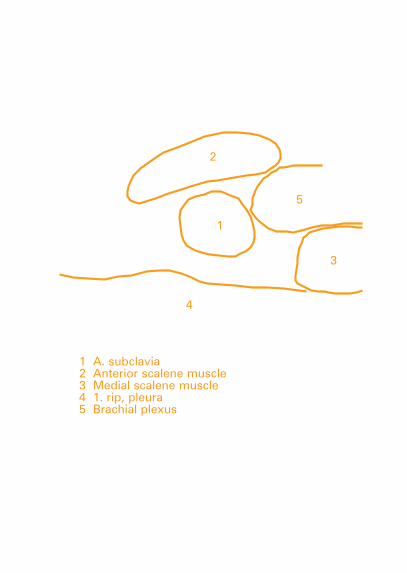
Preliminary note:The supraclavicular plexus block is a classic indication for the use of ultrasound guidance since it can reliably depict delicate structures like the subclavian artery and the pleura, in particular. Or, stated the other way around: Do not perform supraclavicular blocks without ultrasound.
Nerve block technique:Long (single-shot technique) and short axis (catheter tech-nique) possible
Sonoanatomic landmarks:- Anterior scalene and middle scalene muscles- Subclavian artery- First rib- Pleura
Blockade objective:To infiltrate all parts of the plexus (here: trunks) with local anaesthetic.
RKU_Compact_e_V6_neu.indd 28-29

29
for depict
pleura, perform
local
Supraclavicular brachial block
Sonoanatomic landmarks
med
ial
late
ral
21.09.09 14:01
30
Nerve stimulation
Approach according to Kilka, Geiger, Mehrkens
Contraindications
•Chestdeformities•Healed,butdislocated(shortened)fractureoftheclavicle
Side effects / complications
•Horner´ssyndrome•Phrenicparesis•Vesselpuncture(cephalicvein,subclavianarteryandvein)•Pneumothorax
Indications
•Operativeproceduresonthedistalupperarm,forearmand hand
•Analgesia
Anatomical landmarks
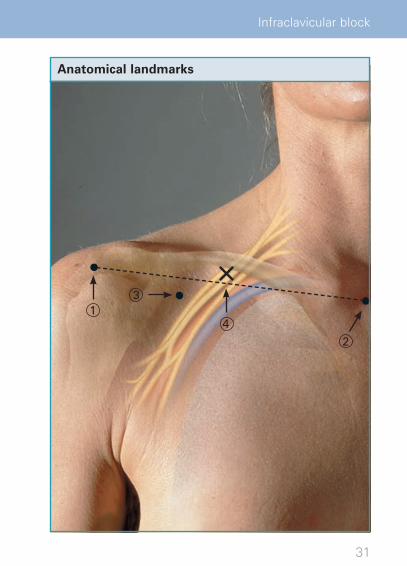
•Suprasternalnotch•Lateraledgeoftheacromion• Infraclavicularfossa
1 Lateral edge of acromion, 2 Suprasternal notch,
3 Infraclavicular fossa, 4 Puncture site
RKU_Compact_e_V6_neu.indd 30-31
31
s
2
31
4
Infraclavicular block
Anatomical landmarks
21.09.09 14:01

32
Nerve stimulation
Blockade technique The patient is supine, with his hand relaxed on abdomen.
Puncture site:Half the distance between the jugular fossa and the ventral endof theacromion–directlyunderneath theclavicle. (Themedial edge of Mohrenheim’s fossa is used to confirm the insertion site). Insertion direction must be absolutely perpen-dicular to the supporting surface (operating table).
Puncturedepth:2–4cm.
Positive stimulatory response from the posterior cord:ExtensororflexormuscleD1–3(=radialormediannerve).
Dosage
30–50mlLA
Catheter technique
e.g. Contiplex® D-Set, 55 mmAdvance the soft plastic catheter max. 3 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex® D, 50 mm
RKU_Compact_e_V6_neu.indd 32-33
33
?abdomen.
ventral
the -
.
What to do when ...?Lateral landmarks (ventral apophysis of acro-mion) cannot be found: Palpation of the clavicle from medial to lateral leads to the acromioclavic-ular joint u The lateral edge of the acromion is located ventral and lateral. Palpation of the crest of the scapula from dorsal to lateroventral leads to the acromion and stops at the correct site.
Stimulation of the musculocutaneous nerve (bi-ceps muscle = lateral cord) occurs: Puncture is too medial and superficial u Retract the needle, shiftitsubcutaneouslytothelateral(0.3–0.5cm)andthenadvanceitperpendicularly(!)ap-prox.0.5–1cmdeeperthanbefore.
Blood is aspirated: Puncture site is too medial or too far away from the lower clavicular edge u Re-tract the needle, check lateral landmarks (ventral apophysis of the acromion) and readvance the needle.
Potential errors and hazards•Puncturetoomedial(establishalateralland-
mark as described above).•Punctureisnotperformedinaperpendicular
direction.•Puncturedepthorientation:estimateddistance
between surface and palpable lower clavicular margin + 1 cm (Beware > 4 cm in persons with asthenic physiques ).
Infraclavicular block
!
?
21.09.09 14:01

34
Sonography
Preliminary note:As a general rule, ultrasound visualization of the infraclavicu-lar cords is less pronounced than of the supraclavicular. It may sometimes be helpful to extend the arm.
Nerve block technique:Short and long axis possible
Sonoanatomic landmarks:- Subclavian artery and vein- Pectoralis major and minor muscles - Pleura
Blockade objective:To infiltrate all cords with local anaesthetic
RKU_Compact_e_V6_neu.indd 34-35


35
It
Infraclavicular block
Sonoanatomic landmarks
cran
ial
caud
al
21.09.09 14:01
36
Nerve stimulation
Approach according to de Jong
Contraindications
•Noparticular
Side effects / complications
•Haematomaiftheradialarteryisinjured
Indications
•Operativeproceduresontheelbow,forearmandhand•Analgesia
Anatomical landmarks
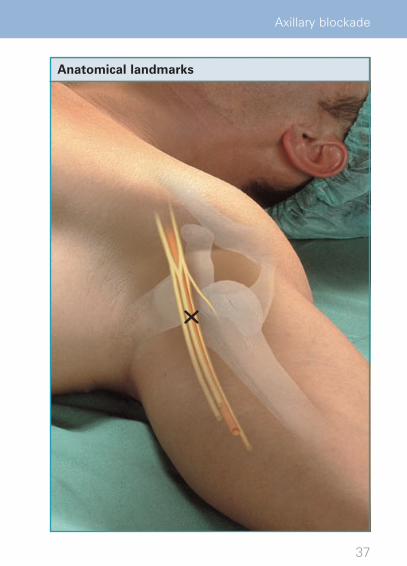
•Axillaryartery•Coracobrachialismuscle•Medialbicipitalgroove•Pectoralismajorandminormuscles
= Puncture site
RKU_Compact_e_V6_neu.indd 36-37
37
Axillary blockade
Anatomical landmarks
21.09.09 14:01
38
Nerve stimulation
Blockade technique With the patient supine, the shoulder joint is abducted 90°,elbowjointextended90°.
Puncture site:Slightly above the axillary artery in the gap between artery and coracobrachialis muscle, at the highest point in the axilla and slightly beneath the pectoralis major muscle.
Inserttheneedleapprox.30°paralleltotheaxillaryartery,tak-ing a very superficial course.
Puncturedepth:1–3cm.
A promising stimulatory response elicited from the median nerve or, rather, from the radial nerve: flexor digitorum mus-cles / extensor digitorum muscles.
Dosage
30–50mlLA
Catheter technique
e.g. Contiplex® D-Set, 55 mm Advance the soft plastic catheter 5 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex® D, 50 mm
RKU_Compact_e_V6_neu.indd 38-39

39
?90°,
artery axilla
-
median -
What to do when ...?
There is no stimulatory response:The puncture has probably gone too deep u Re-tract the needle and advance at a flatter (more tan-gential) angle, watching out for any “fascial click“.
Stimulation of the musculocutaneous nerve:The needle is not positioned within the neurov-ascular sheathu Retract the needle, advance it less deep and more tangential to the artery.
Potential errors and hazards
•Puncturetoodeep.•Difficultiesidentifyingtheaxillaryartery.
Axillary blockade
!
?
21.09.09 14:01

40
Sonography
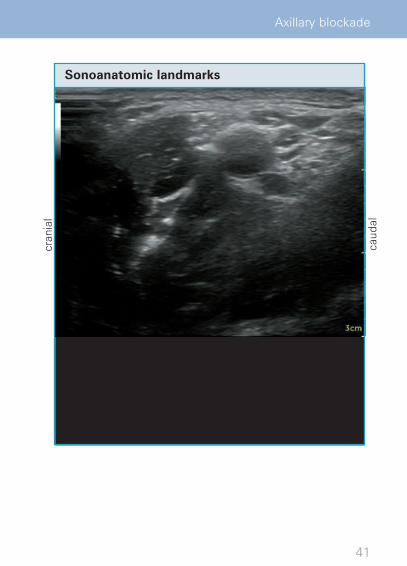
Nerve block technique:Short axis is preferable
Sonoanatomic landmarks:- Axillary artery and vein- Triceps brachii muscle
Blockade objective:To infiltrate all four main nerves of the brachial plexus with local anaesthetic
RKU_Compact_e_V6_neu.indd 40-41

41
Axillary blockade
Sonoanatomic landmarks
cran
ial
caud
al
21.09.09 14:01
42
Nerve stimulation
Approach according to Meier
Contraindications
•Noparticular
Side effects / complications
•Noparticular
Indications
•Frozenshoulder(forpainmanagementandmobilizationtherapy)
•Analgesia
Anatomical landmarks
•Spineofscapula
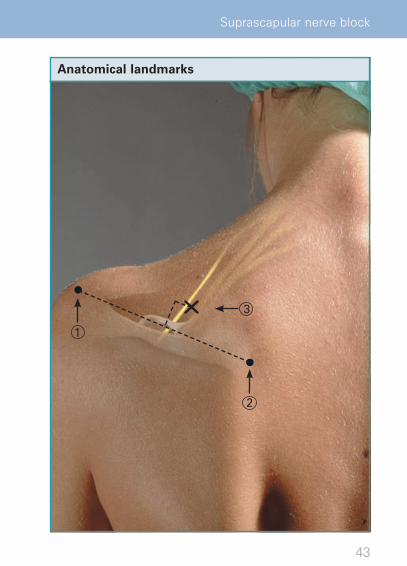
1 Lateral end of the spine of scapula,
2 Medial end of the spine of scapula, 3 Puncture site
RKU_Compact_e_V6_neu.indd 42-43
43
2
3
1
Suprascapular nerve block
Anatomical landmarks
21.09.09 14:01
44
Nerve stimulation
The patient is seated, hand on their contralateral shoulder.
1–2cmcranialandmedialtothemid-spine.Insertiondirec-tion approx. 45° caudad and lateral towards the humerushead.
Puncturedepth:3–5cm.
Positive stimulatory response: supraspinatus or infraspinatus muscles.
Dosage
10–20mlLA
Catheter technique
e.g. Contiplex® D-Set, 55 mmAdvance the soft plastic catheter < 3 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex® D, 50 mm
RKU_Compact_e_V6_neu.indd 44-45
45
?-
infraspinatus
What to do when ...?
There is no stimulation response:Try to find the floor of the supraspinous fossa or retract the needle and advance it at a flatter angle towards the humerus head.
Note two important aspects:1. A muscular stimulatory response is not im-
perative to achieve blockade. 2. The suprascapular nerve is not involved in the(sensory)skinsupplyoftheshoulder!
Potential errors and hazards•Punctureismadetoodeepandsteep.
Suprascapular nerve block
!
?
21.09.09 14:01
46
Nerve stimulation
Approach according to Chayen
Contraindications
•Extremehyperlordosis(relative)•Coagulationdisorders
Side effects / complications
•Vesselpuncture(paravertebralveins)•Disseminationsimilartoepiduralanesthesia(contralateral)•High(total)spinalanesthesia
Indications
•Operativeproceduresinthelumbarplexussupplyarea• Incombinationwithproximalsciaticnerveblockforcom-
plicated operations on the whole leg distal to the hip (total knee arthroplasty, cruciate ligament replacement ...)
•Analgesia
Anatomical landmarks
•Posteriorsuperioriliacspine• Iliaccrest•SpinousprocessL4•CostalprocessL5
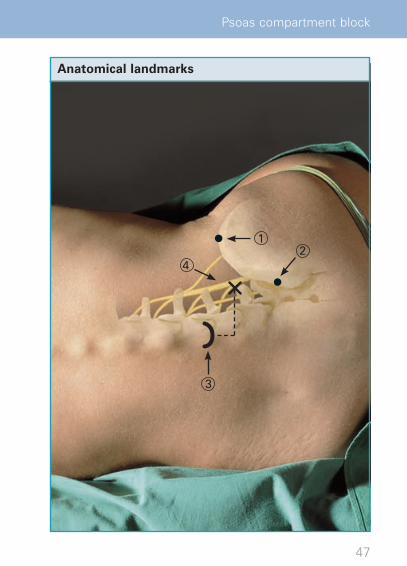
1 Iliac crest, 2 Posterior superior iliac spine,
3 Spinous process L 4, 4 Puncture site
RKU_Compact_e_V6_neu.indd 46-47
47
2
3
4
1
Psoas compartment block
Anatomical landmarks
21.09.09 14:01

48
Nerve stimulation
Blockade technique The patient is in the lateral recumbent position (or seated), the cervical spine is flexed backwards.
Puncture site:3 cm caudad and 4 cm paramedian to the spinous process of L4. Sagittal insertion direction; upon contact with the trans-verse process of L5, retract needle slightly, correct downward and advance over the transverse process (2 cm). Alternatively: Divide the connecting line between the spinous process of L4 and the posterior superior iliac spine in thirds; insert the needle at the transition from the medial to lateral third.
Puncturedepth:6–10cm.
Positive stimulatory response from the femoral nerve: quadri-ceps muscle (usually the vastus lateralis muscle). Puncture is also possible at the level of the transverse process L4; now ad-vance the caudad aligned needle under the transverse process.
Dosage
30–50mlLA,testdose5ml
Catheter technique
e.g. Contiplex®D-Set,80–110mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex®D,80–120mm
RKU_Compact_e_V6_neu.indd 48-49
49
?the
f -d : 4 e
-s -.
What to do when ...?Stimulation of the obturator nerve (contrac-tion of the adductor group) occurs: Puncture direction is too medial uRetract the needle, then lateralize it somewhat.
Stimulation of the fourth lumbar nerve (= lum-bosacral trunk, contractions in the peroneal group) occurs:Puncture direction is much too medial u Re-tract the needle; advance it markedly in the lateral direction.
No transverse process contact and no stimulatory response is achieved:Puncture site and/or direction may be too lat-eral u Check the distance between puncture site and midline (max. 4 cm), and, if needed, adjust the puncture direction to the patient‘s position. Adequate stimulatory response may also be possible without prior transverse proc-esscontact!
Potential errors and hazardsAlways avoid a medial puncture direction (towards the spinal column)!•Riskofepiduralorevenintrathecaldissemina-
tion of the LA. Perform a test dose.
Psoas compartment block
!
?
21.09.09 14:01
50
Nerve stimulation
Femoral nerve block
Contraindications
•Noparticular
Side effects / complications
•Vesselpuncture(ofthefemoralveinorartery)
Indications
•Operativeproceduresinareassupplyingthefemoraland lateral femoral cutaneous nerves
• Incombinationwithproximalsciaticnerveblock,op-erative procedures on the whole leg (from distal thigh to foot)
•Analgesia
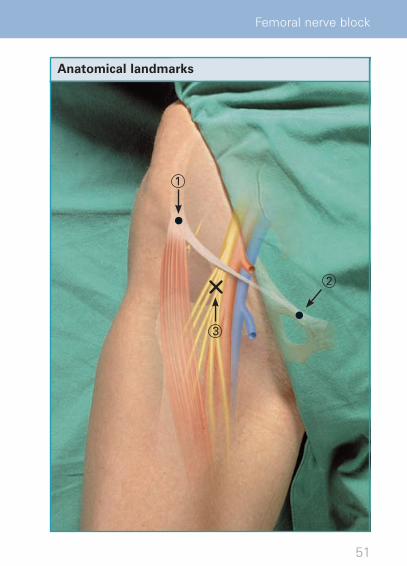
Anatomical landmarks
•Groin•Femoralartery•Anteriorsuperioriliacspine•Pubictubercle• Inguinalligament
1 Anterior superior iliac spine,
2 Pubic tubercle, 3 Puncture site
RKU_Compact_e_V6_neu.indd 50-51
51
spine,
2
3
1
Femoral nerve block
Anatomical landmarks
21.09.09 14:01
52
Nerve stimulation
Blockade technique The patient lies on his back, his leg loosely abducted and turned to the outside.
Puncture site:2cmcaudadtothegroin,1–2cmlateraltothefemoralar-tery.Puncturedirection:30–45°cranialparalleltotheartery.
Puncturedepth:2–4cm.
Positive stimulatory response from the femoral nerve: Rectus muscle of the thigh (“dancing patella“).
Dosage
20–40mlLA
Catheter technique
e.g. Contiplex® D-Set, 55 mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex® D, 50 mm
RKU_Compact_e_V6_neu.indd 52-53

53
?and
-artery.
Rectus
What to do when ...?
Stimulation of the sartorius muscle (medial contraction) occurs:Puncture direction usually too medial u Retract the needle, and shift it slightly to the lateral.
Direct stimulation of the sartorius muscle (rare):Puncture direction is usually too lateral u Shift the needle slightly to the medial.
Femoral artery puncture:Retract the needle u Shift puncture direction to the lateral.
Potential errors and hazards•LA injection in the case of sartorius muscle
stimulation.
Femoral nerve block
!
?
21.09.09 14:01
54
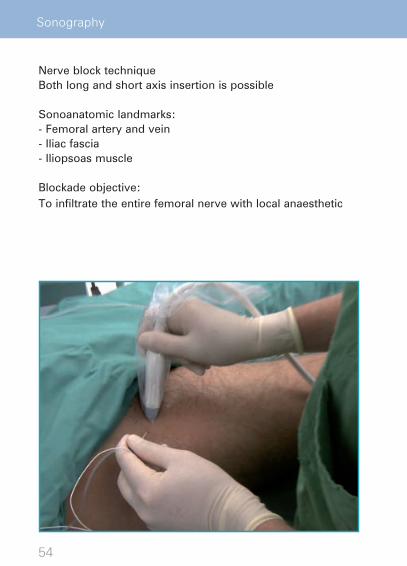
Sonography
Nerve block techniqueBoth long and short axis insertion is possible
Sonoanatomic landmarks:- Femoral artery and vein- Iliac fascia- Iliopsoas muscle
Blockade objective:To infiltrate the entire femoral nerve with local anaesthetic
RKU_Compact_e_V6_neu.indd 54-55

55
Femoral nerve block
Sonoanatomic landmarks
late
ral
med
ial
21.09.09 14:01

56
Nerve stimulation
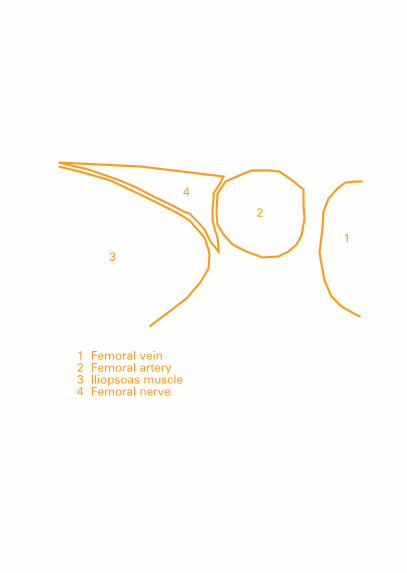
Saphenous nerve block
Contraindications
•Noparticular
Side effects / complications
•Noparticular
Indications
•Operativeproceduresintheareasupplyingthesaphen-ous nerve
• Incombinationwithdistalsciaticnerveblockforopera-tions on the whole lower leg and foot
•Analgesia
Anatomical landmarks
•Patellarcrest•Sartoriusmuscle•Vastusmedialismuscle
= Puncture site
RKU_Compact_e_V6_neu.indd 56-57

57
Saphenous nerve block
Anatomical landmarks
21.09.09 14:01

58
Nerve stimulation
Blockade technique The patient is supine on his back, with the extended leg in a neutral position, rotated slightly outwardly.
Puncture site:Approx.2–4cmcranialandmedialtothesuperioredgeofthe patella. Insert needle perpendicularly into the palpable space between the sartorius muscle and the vastus medialis muscle. Insert the needle perpendicular through the muscle up to the subsartorial fatty tissue.
Puncturedepth:3–5cm.
Electrical paresthesias at the medial calf at a pulse duration of 1.0 ms and/or a motor response from the muscular branches of the sartorius muscle are promising responses.
Dosage
10–15mlLA
Catheter technique
e.g. Contiplex®D-Set,55–80mmAdvance the soft plastic catheter 3 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex®D,50–80mm
RKU_Compact_e_V6_neu.indd 58-59
59
?a
ofpalpable medialis muscle
of branches
What to do when ...?
Motor stimulatory response from the sartorius muscle is a promising response: u Inject local anaesthetic
Patient is uncooperative:Femoral nerve block (as described above) with reduced LA volume (20 ml).Alternative technique: Subcutaneous infiltra-tion below the medial knee joint from the me-dial head of the gastrocnemius muscle to the tibialtuberosity(10–15mlLA).
Potential errors and hazards•Noparticular.
Saphenous nerve block
!
?
21.09.09 14:01
60
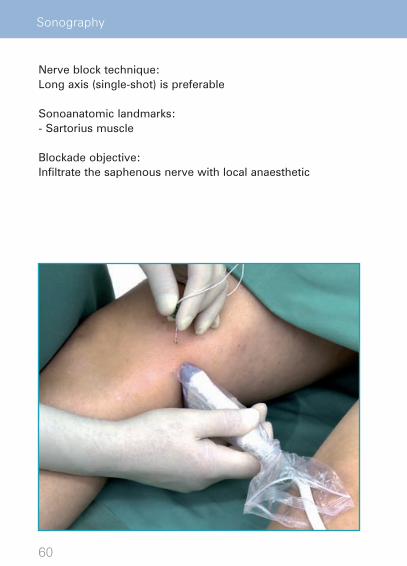
Sonography
Nerve block technique:Long axis (single-shot) is preferable
Sonoanatomic landmarks:- Sartorius muscle
Blockade objective:Infiltrate the saphenous nerve with local anaesthetic
RKU_Compact_e_V6_neu.indd 60-61

61
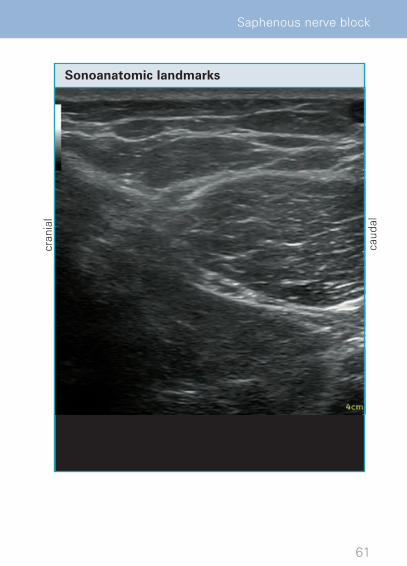
Saphenous nerve block
Sonoanatomic landmarks
cran
ial
caud
al
21.09.09 14:01

62
Nerve stimulation
Obturator nerve block
Contraindications
•Noparticular
Side effects / complications
•Vesselpuncture(obturatorarteryorvein)
Indications
•Suppressionoftheadductorreflexfortransurethrallateral bladder wall resection
•Treatmentofadductorspasm•Adjuncttofemoralnerveblocksforpostoperative
medial knee joint pain •Analgesia
Anatomical landmarks
•Originoftheadductorlongusmuscle•Pubictubercle•Femoralartery•Anteriorsuperioriliacspine
1 Adductor longus muscle, 2 Puncture site
RKU_Compact_e_V6_neu.indd 62-63

63
Obturator nerve block
Anatomical landmarks
1
2
21.09.09 14:01

64
Nerve stimulation
Blockade technique The patient is supine on his back, his leg is rotated outwardly and abducted.
Puncture site:5 – 10 cmbeneath the pubic tubercle directly lateral to thetendon origin of the adductor longus muscle. Puncture direc-tion approx. 45° craniolateral pointing towards the anteriorsuperior iliac spine.
Puncturedepth:4–6cm.
Positive stimulatory response from adductor group.
Dosage
10–15mlLA
Catheter technique
e.g. Contiplex® D-Set, 80 mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex® D, 80 mm
RKU_Compact_e_V6_neu.indd 64-65
65
?outwardly
-
anterior
What to do when ...?
Persistent adductor spasm despite (proper) obturator nerve block occurs:Perform an additional femoral nerve block, which will block any accessory obturator nerve that runs together with femoral nerve.
Note:The adductor reflex for transurethral lateral bladder wall can only be reliably suppressed by a separate obturator nerve block (not by a femoralnerveblocknorspinalanesthesia!).
Potential errors and hazards•Noparticular.
Obturator nerve block
!
?
21.09.09 14:01
66
Sonography
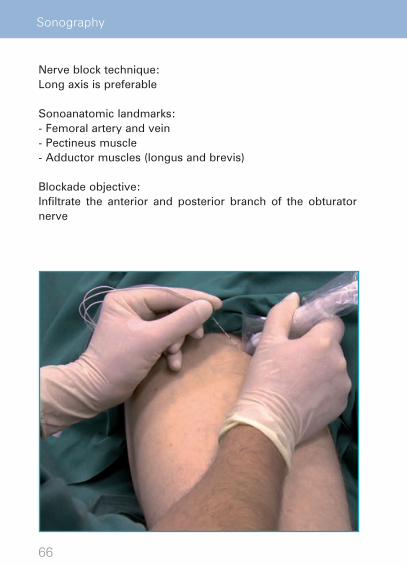
Nerve block technique:Long axis is preferable
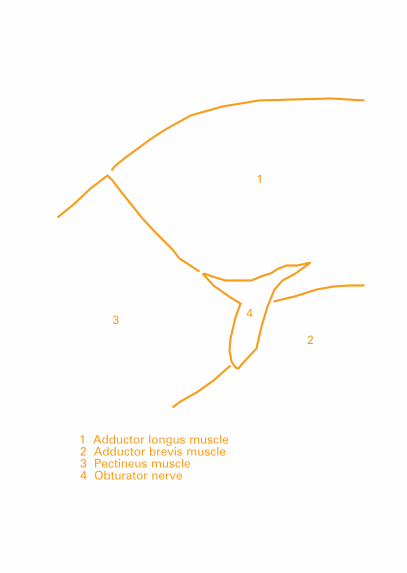
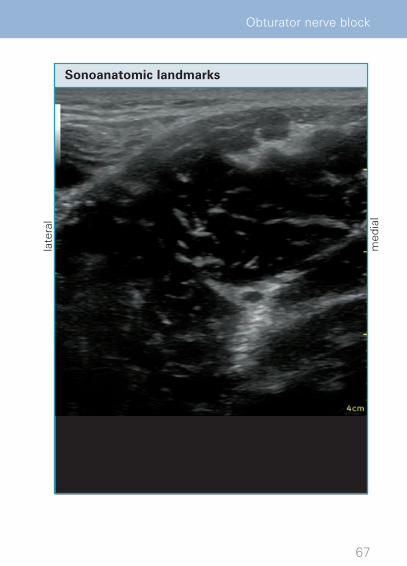
Sonoanatomic landmarks:- Femoral artery and vein- Pectineus muscle - Adductor muscles (longus and brevis)
Blockade objective:Infiltrate the anterior and posterior branch of the obturator nerve
RKU_Compact_e_V6_neu.indd 66-67
67
obturator
Obturator nerve block
Sonoanatomic landmarks
late
ral
med
ial
21.09.09 14:01
68
Nerve stimulation
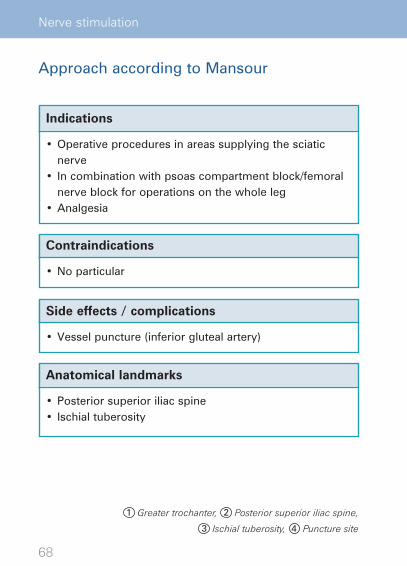
Approach according to Mansour
Contraindications
•Noparticular
Side effects / complications
•Vesselpuncture(inferiorglutealartery)
Indications
•Operativeproceduresinareassupplyingthesciaticnerve
• Incombinationwithpsoascompartmentblock/femoralnerve block for operations on the whole leg
•Analgesia
Anatomical landmarks
•Posteriorsuperioriliacspine• Ischialtuberosity
1 Greater trochanter, 2 Posterior superior iliac spine,
3 Ischial tuberosity, 4 Puncture site
RKU_Compact_e_V6_neu.indd 68-69

69
2
34
1
Parasacral sciatic nerve block
Anatomical landmarks
21.09.09 14:01

70
Nerve stimulation
Blockade technique The patient is placed in the lateral recumbent position, hip flexed45°,knee flexed70°,orbothkneesagainst theabdo-men (favorable when combined with a psoas compartment block).
Puncture site:Approx.5–6cmcaudadtotheposteriorsuperioriliacspinealong the connecting line to the ischial tuberosity. Insertion direction20–30°caudadtomidlinebetweenischialtuberos-ity and greater trochanter.
Puncturedepth:6–8cm.
Promising stimulatory response from the tibial and peroneal nerves: Extensors and/or flexors of feet/toes, ischiocrural muscle group
Dosage
20–30mlLA
Catheter technique
e.g. Contiplex®D-Set,80–110mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex®D,80–120mm
RKU_Compact_e_V6_neu.indd 70-71

71
?hip -
compartment
Insertion
-
peroneal ischiocrural
What to do when ...?
Bone contact occurs:Shift puncture site further caudad or puncture direction more caudad.
No stimulatory response is elicited:Shift puncture direction more caudad and lateral.
Potential errors and hazards
•LAinjectionuponstimulatoryresponsefromthe gluteal muscles.
Parasacral sciatic nerve block
!
?
21.09.09 14:01

72
Nerve stimulation
Approach according to Labat
Contraindications
•Noparticular
Side effects / complications
•Vesselpuncture(inferiorglutealartery)
Indications
•Operativeproceduresinareassupplyingthesciaticnerve
• Incombinationwithpsoascompartmentblock/femoralnerve block for operations on the whole leg
•Analgesia
Anatomical landmarks
•Posteriorsuperioriliacspine•Greatertrochanter•Sacralhiatus
1 Greater trochanter, 2 Posterior superior iliac spine,
3 Ischial tuberosity, 4 Sacral hiatus, 5 Puncture site
RKU_Compact_e_V6_neu.indd 72-73

73
2
3
4
1
Transgluteal sciatic nerve block
Anatomical landmarks
5
21.09.09 14:01
74
Nerve stimulation
Blockade technique The patient is placed in the lateral recumbent position; hip flexed45°,kneeflexed70°(“stablerecumbentposition“).
Puncture site:4–5cmmediocaudalonthemid-perpendicularlinesbetweengreater trochanter and posterior superior iliac spine; con-necting line between the greater trochanter and sacral hiatus intersects the insertion point at the mid-perpendicular line. Insertion direction perpendicular to the surface.
Puncturedepth:5–8cm.
Promising stimulatory response from the tibial and peroneal nerves: Extensors and/or flexors of feet/toes, ischiocrural muscle group
Dosage
20–30mlLA
Catheter technique
e.g. Contiplex®D-Set,80–110mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex®D,80–100mm
RKU_Compact_e_V6_neu.indd 74-75
75
?hip
-
hiatus line.
peroneal ischiocrural
What to do when ...?
Contractions of the gluteus maximus muscle (= direct muscular stimulation or stimulation of the muscular branches of the gluteal mus-cle): Continue to advance the needle until the typical response is elicited.
Bone contact, no stimulatory response: Correct insertion direction to midline between greater trochanter and ischial tuberosity.
Potential errors and hazards
•LAinjectionuponstimulatoryresponsefrom the gluteal muscles.
Transgluteal sciatic nerve block
!
?
21.09.09 14:01
76
Nerve stimulation
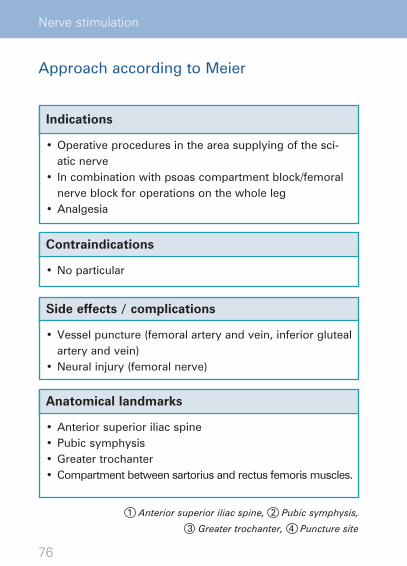
Approach according to Meier
Contraindications
•Noparticular
Side effects / complications
•Vesselpuncture(femoralarteryandvein,inferiorglutealartery and vein)
•Neuralinjury(femoralnerve)
Indications
•Operativeproceduresintheareasupplyingofthesci-atic nerve
• Incombinationwithpsoascompartmentblock/femoralnerve block for operations on the whole leg
•Analgesia
Anatomical landmarks
•Anteriorsuperioriliacspine•Pubicsymphysis•Greatertrochanter• Compartmentbetweensartoriusandrectusfemorismuscles.
1 Anterior superior iliac spine, 2 Pubic symphysis,
3 Greater trochanter, 4 Puncture site
RKU_Compact_e_V6_neu.indd 76-77

77
2
3
4
1
Anterior sciatic nerve block
Anatomical landmarks
21.09.09 14:01

78
Nerve stimulation
Blockade technique The patient is supine on his back, with the leg in a neutral position.
Puncture site:Divide into thirds the line connecting the anterior superior iliac spine and the middle of the pubic symphysis. A perpendicular line at the transition from the medial to the middle third inter-sects a parallel line to the inguinal ligament through the greater trochanter at the insertion point. Palpate the muscle compart-ment and, using two fingers, press against the femur, forcing the vessels to the medial. Insert the needle sagittally and 70 –80°tothecranial,withouttouchingthefemur.Alternatively, target the muscle compartment about 8-10 cm caudad of the femoral nerve insertion site
Puncturedepth:8–15cm.
Positive stimulatory response from the peroneal or tibial nerves: extensors or flexors of the foot/toes.
Dosage
20–30mlLA
Catheter technique
e.g. Contiplex® D-Set, 110 mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex®D,100–150mm
RKU_Compact_e_V6_neu.indd 78-79
79
?.
c r -r -g 0
m
tibial
What to do when ...?
Primary femur contact occurs: Insertion point too far to the lateral u Retract the needle and shift insertion to the medial.
Primary vessel puncture (femoral vein or ar-tery): Insertion too far medial u Retract the needle and shift the insertion to the lateral.
Deep vessel puncture (gluteal artery and vein): Correct insertion direction slightly to the lateral.
Stimulation of femoral nerve branches: Retract the needle and “bypass“ stimulation area.
Potential errors and hazards
•Aneutrallegpositionisimperative.
Anterior sciatic nerve block
!
?
21.09.09 14:01
80
Nerve stimulation
Approach according to Guardini
Contraindications
•Status secondary to total ipsilateral hip replacement (relative)
Side effects / complications
•Noparticular
Indications
•Operativeproceduresintheareasupplyingofthesci-atic nerve
• Incombinationwithpsoascompartmentblock/femoralnerve block for operations on the whole leg
•Analgesia
Anatomical landmarks
•Greatertrochanter• Ischialtuberosity
1 Greater trochanter,
2 Ischial tuberosity, 3 Puncture site
RKU_Compact_e_V6_neu.indd 80-81

81
Subtrochanteric sciatic nerve block
Anatomical landmarks
2
3
1
21.09.09 14:01
82
Nerve stimulation
Blockade technique The patient is supine, with the leg in a neutral position or ro-tated slightly inwards. Padding under the lower leg and pelvic helps with orientation.
Puncture site:Approx.2 cmdorsal and3 –4 cmdistal to thegreater tro-chanter. Insertion direction horizontal and somewhat cranial towards the ischial tuberosity without femur contact.
Puncturedepth:6–10cm.
Positive stimulatory response from the peroneal or tibial nerves: extensors and/or flexors of feet/toes, ischiocrural muscle group
Dosage
20–30mlLA
Catheter technique
e.g. Contiplex®D-Set,80–110mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex®D,80–100mm
RKU_Compact_e_V6_neu.indd 82-83

83
?-tated slightly inwards. Padding under the lower leg and pelvic
-cranial
tibial ischiocrural
What to do when ...?
Femur contact occurs: Insertion too far ventral u Move insertion more to the dorsal.
No stimulatory response is elicited: u Direct insertion a little to the ventral and emphasize inward rotation in the hip joint.
Alternative technique:Leg is rotated slightly inward with flexed knee joint “upright“ on the table. Puncture site: 2–3cmcaudadfromthemid-point of the line connecting greater trochanter and ischial tuberosity. Insert the needle in the cranial and slightly medial direction (modified dorsodorsal access according to Raj).
Potential errors and hazards
•Makesurethatthelegisinaneutralposition(with a slight inward rotation).
Subtrochanteric sciatic nerve block
!
?
21.09.09 14:01

84
Preliminary note:It is occasionally difficult to visualise the nerves due to their deep location (with linear high-frequency transducer).
Block technique:Long axis is preferable, short axis possible
Sonoanatomic landmarks:Gluteal muscles
Blockade objective:To infiltrate the entire nerve with local anaesthetic
Sonography
RKU_Compact_e_V6_neu.indd 84-85


85
p
Subtrochanteric sciatic nerve block
Sonoanatomic landmarksla
tera
l
med
ial
21.09.09 14:01

86
Nerve stimulation
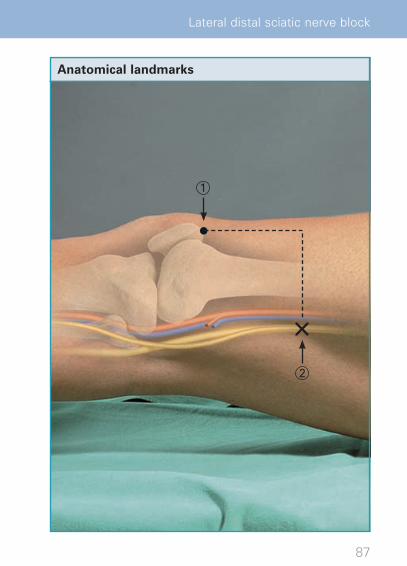
Lateral distal sciatic nerve block
Contraindications
•Stent(relative)
Side effects / complications
•Vesselpuncture(poplitealartery/vein)
Indications
•Operativeproceduresintheareassupplyingthesciaticnerve on the whole lower leg and foot
• Incombinationwithsaphenousnerveblockforopera-tions of the whole lower leg
•Analgesia
Anatomical landmarks
•Patellarcrest•Vastuslateralismuscle•Longheadofthebicepsfemorismuscle
1 Patellar crest, 2 Puncture site
RKU_Compact_e_V6_neu.indd 86-87
87
Lateral distal sciatic nerve block
Anatomical landmarks
2
1
21.09.09 14:01

88
Nerve stimulation
Blockade technique The patient is supine on his back, with the leg in a neutral po-sition (rotated slightly inwards), padding under the lower leg.
Puncture site:Approx.3–8cmabovethepatellainthelateralmusclecom-partment between lower edge of the vastus lateralis muscle and biceps femoris muscle. Insertion direction slightly dor-socranial.
Puncturedepth:3–5cm.
Positive stimulatory response from the peroneal or tibial nerves: extensors or flexors of the foot/toes.
Dosage
20–40mlLA
Catheter technique
e.g. Contiplex®D-Set,55–80mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex®D,50–80mm
RKU_Compact_e_V6_neu.indd 88-89

89
?-leg.
-muscle
-
tibial
What to do when ...?
No stimulatory response is elicited: Insertion direction is usually too far ventral u Correct to the dorsal.
Femur contact occurs:Puncture site and/or insertion direction too far to the ventral u Check puncture site, correct to dorsal if needed; shift insertion direction more to the dorsal.
Vessel puncture popliteal artery/vein:Puncture too deep and too ventral u Retract the needle, correct insertion direction to the dorsal, reduce insertion depth.
Potential errors and hazards
•Makesurethatthelegisinaneutralposition (with a slight inward rotation).
Lateral distal sciatic nerve block
!
?
21.09.09 14:01
90
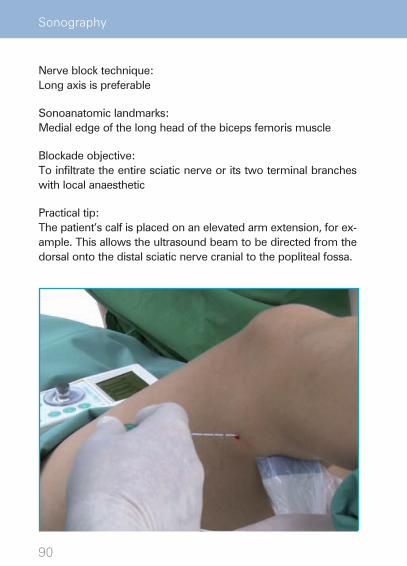
Nerve block technique:Long axis is preferable
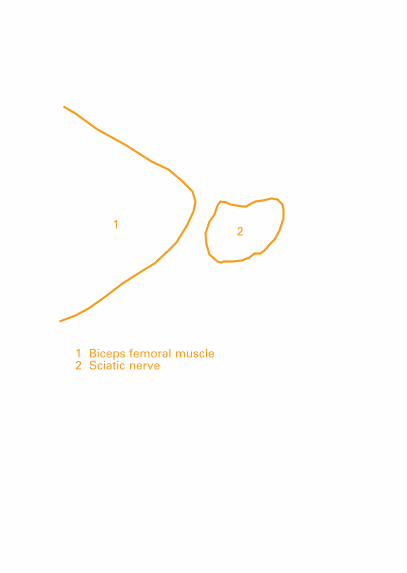
Sonoanatomic landmarks:Medial edge of the long head of the biceps femoris muscle
Blockade objective:To infiltrate the entire sciatic nerve or its two terminal branches with local anaesthetic
Practical tip:The patient’s calf is placed on an elevated arm extension, for ex-ample. This allows the ultrasound beam to be directed from the dorsal onto the distal sciatic nerve cranial to the popliteal fossa.
Sonography
RKU_Compact_e_V6_neu.indd 90-91

91
s
e
Lateral distal sciatic nerve block
Sonoanatomic landmarks
late
ral
med
ial
21.09.09 14:01
92
Nerve stimulation
Popliteal sciatic nerve block
Contraindications
•Stent(relative)
Side effects / complications
•Vesselpuncture(poplitealartery/vein)
Indications
•Operativeproceduresintheareasupplyingthesciaticnerve of the lower leg and foot
•Operationsonthewholelowerextremityincombinationwith a saphenous nerve block.
•Analgesia
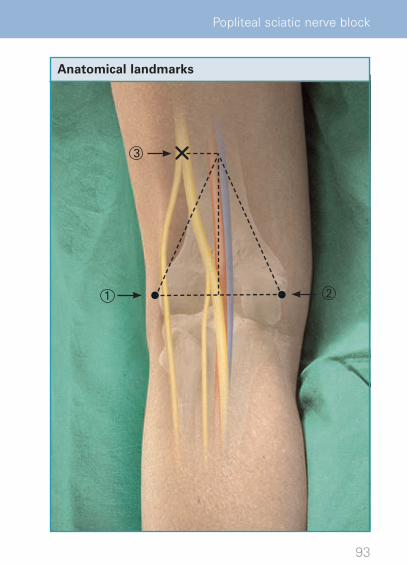
Anatomical landmarks
•Poplitealfossa•Poplitealfold•Longheadofthebicepsfemorismuscle•Medialandlateralepicondyleofthefemur
1 Lateral epicondyle of the femur,
2 Medial epicondyle of the femur, 3 Puncture site
RKU_Compact_e_V6_neu.indd 92-93
93
2
3
1
Popliteal sciatic nerve block
Anatomical landmarks
21.09.09 14:01
94
Nerve stimulation
Blockade technique The patient is either in the prone position or lying on his side, leg extended.
Puncture site:Approx.8–12cmabovethefoldofthepoplitealfossaatthemedial edge of the biceps femoris muscle, laterally marking thepoplitealfossa.Insertiondirectionapprox.30°cranialandslightly medial.
Puncturedepth:2–4cm.
Positive stimulatory response from the peroneal and tibial nerves: extensors or flexors of the foot/toes.
Dosage
20–40mlLA
Catheter technique
e.g. Contiplex® D-Set, 55 mmAdvance the soft plastic catheter < 4 cm beyond the end of the introducer sheath.
Single shot technique
e.g. Stimuplex® D, 50 mm
RKU_Compact_e_V6_neu.indd 94-95
95
?side,
marking
tibial
What to do when ...?
Femur contact occurs:Insertion too deep and too medial Retract the needle u Correct puncture direction or insertion site to the lateral , reduce insertion depth.
Vessel puncture popliteal artery/vein:Puncture too deep and too medial Retract the needle u Correct insertion direction to the lat-eral, reduce insertion depth.
Potential errors and hazards
•Puncturesiteistoofarcaudad(poplitealfold): It may be that the tibial nerve (med.) and peroneal nerve (lat.) are separated so far apart that complete blockade cannot be achieved with a single LA injection at the two sciatic branches.
Popliteal sciatic nerve block
!
?
21.09.09 14:01

www.nerveblocks.net
Online Tutorial and Discussion Forum
Other publications appearing in this series
• Brochure(DINA4) Peripheral Regional Anesthesia at the Ulm Rehabilitation Hospital
• InteractiveDVDTutorial Peripheral Regional Anesthesia at the Ulm Rehabilitation Hospital
These materials can berequested at your B. Braun partner in your country
B. Braun Melsungen AGCarl-Braun-Straße 134212 MelsungenGermanyTel. +49 5661 71 4657Fax. +49 5661 75 4657 E-mail: [email protected]
The state of medical knowledge is subject to constant change due to new research and clinical evidence. The authors of this book have been very careful to comply with the current state of the art. Nevertheless, users of this information carry their own responsi-bility and liability when establishing the diagnosis and implementing therapy.
The Tutorial was made possible by the kind support of B. Braun Melsungen AG.
Nr. 6064605
RKU_Compact_e_V6_neu.indd 96 21.09.09 14:01
B

The Tutorial was made possible by the kind support of B. Braun Melsungen AG.
RKU_Umschlag_eng2.indd 2 18.08.09 14:04
B. 03. Nr. 6064605 . /1 B01 10







![rks igyh ckr] lcls igys rks t,lk fd /hW HkB us dgk] tWj Sd ... ckr rks ;g g, fd Vgn¬q rku dh iwjh u¬y cckZn gks xB g,6 Vgnq¬rku dh iwjh jsl cckZn gks x;h g,3Sd gh tkfr e X 'knh](https://img.dokumen.tips/doc/110x75/5b0c27f77f8b9af65e8b8fb8/rks-igyh-ckr-lcls-igys-rks-tlk-fd-hw-hkb-us-dgk-twj-sd-ckr-rks-g-g-fd.jpg)

![VŠB – Technická univerzita Ostrava Fakulta strojní Katedra … · 2019. 1. 13. · Rsk šikmost posuzovaného profilu [-] Rku špičatost posuzovaného profilu [-] kinetická](https://img.dokumen.tips/doc/110x75/6100cd6269d616760a2dbc28/vb-a-technick-univerzita-ostrava-fakulta-strojn-katedra-2019-1-13-rsk.jpg)




![3JMZ3Y OPUTW WVKP W- 0] / NK]SI IWSRK RKU^ ^VNK … filekyuno rku^ ^vnk z5oufmk jqmooll1p wu](https://img.dokumen.tips/doc/110x75/5e05120afd716104770915f6/3jmz3y-oputw-wvkp-w-0-nksi-iwsrk-rku-vnk-rku-vnk-z5oufmk-jqmooll1p-wu.jpg)











![3JMZ3Y OPUTW WVKP W- 0] / NK]SI IWSRK RKU^ ^VNK …kyuno rku^ ^vnk z5oufmk jqmooll1p wu](https://img.dokumen.tips/doc/110x75/5e54d2f84e70d678a947c7ea/3jmz3y-oputw-wvkp-w-0-nksi-iwsrk-rku-vnk-kyuno-rku-vnk-z5oufmk-jqmooll1p.jpg)


