Embed Size (px)
Citation preview
Rivaroxaban in SPAF:
Efficacy, safety and cardio-vascular profile
Hans Rickli, St.Gallen
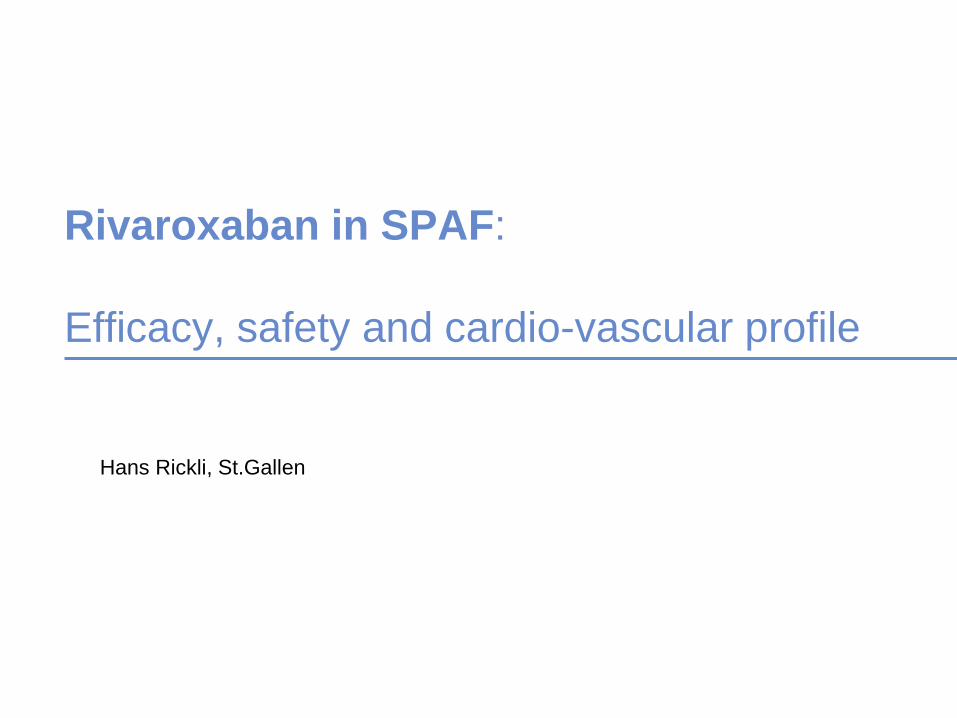
CHADS2 Distribution Across SPAF Trials
• Dabigatran and apixaban: evaluated across a spectrum of stroke risk
categories
• Rivaroxaban: evaluated in patients at high risk of stroke
Connolly N Engl J Med 2009;361:1139; Patel N Engl J Med 2011365:883; Granger N Engl J Med 2011;365:981; Ruff Am Heart J 2010;160:635
CHADS2 Score
%
*CHF or LVEF ≤40%;
#CHF or LVEF ≤35%
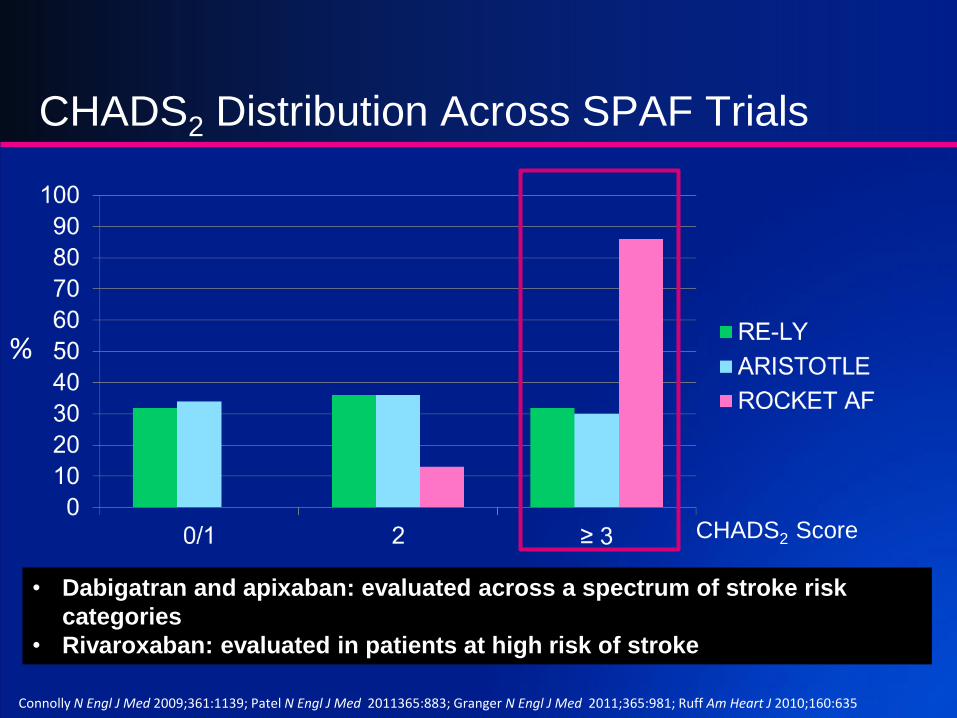
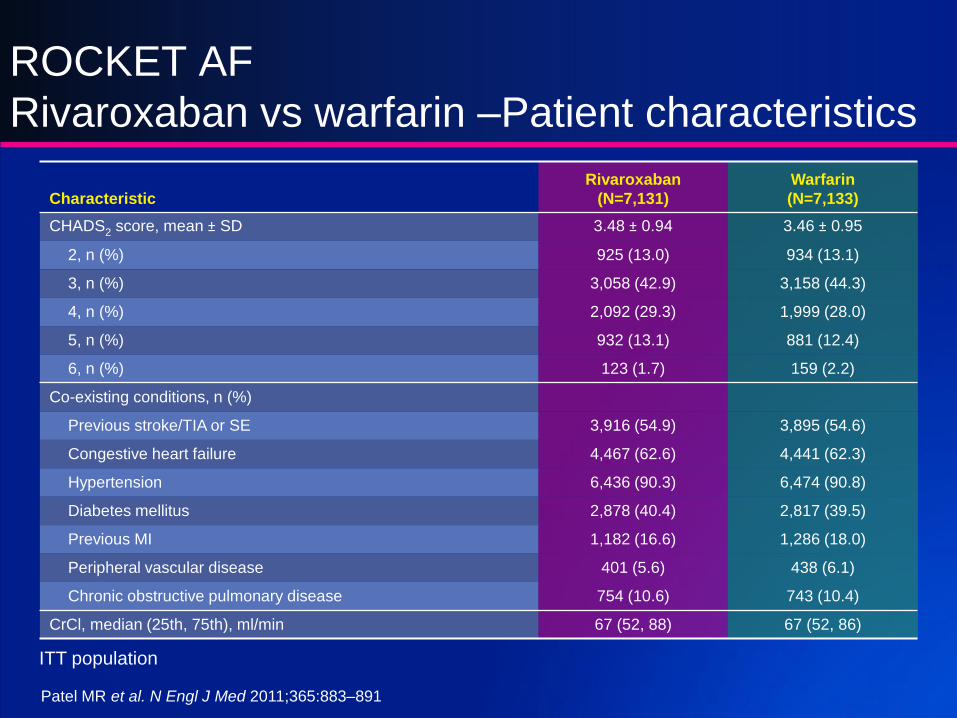
With over 11’000 patient-years of exposure, the ROCKET AF trial
provides the largest prospective experience involving high-risk
elderly patients with AF using oral anticoagulation with rivaroxaban
Connolly N Engl J Med 2009;361:1139; Patel N Engl J Med 2011365:883;Granger N Engl J Med 2011;365:981; Ruff Am Heart J 2010;160:635
Patient Characteristics Across SPAF
Trials
*#
% of Study Patients
#
Characteristic
Rivaroxaban
(N=7,131)
Warfarin
(N=7,133)
CHADS2 score, mean ± SD 3.48 ± 0.94 3.46 ± 0.95
2, n (%) 925 (13.0) 934 (13.1)
3, n (%) 3,058 (42.9) 3,158 (44.3)
4, n (%) 2,092 (29.3) 1,999 (28.0)
5, n (%) 932 (13.1) 881 (12.4)
6, n (%) 123 (1.7) 159 (2.2)
Co-existing conditions, n (%)
Previous stroke/TIA or SE 3,916 (54.9) 3,895 (54.6)
Congestive heart failure 4,467 (62.6) 4,441 (62.3)
Hypertension 6,436 (90.3) 6,474 (90.8)
Diabetes mellitus 2,878 (40.4) 2,817 (39.5)
Previous MI 1,182 (16.6) 1,286 (18.0)
Peripheral vascular disease 401 (5.6) 438 (6.1)
Chronic obstructive pulmonary disease 754 (10.6) 743 (10.4)
CrCl, median (25th, 75th), ml/min 67 (52, 88) 67 (52, 86)
ITT population
Patel MR et al. N Engl J Med 2011;365:883–891
ROCKET AF
Rivaroxaban vs warfarin –Patient characteristics
1 20
5
6
4
3
2
1
0
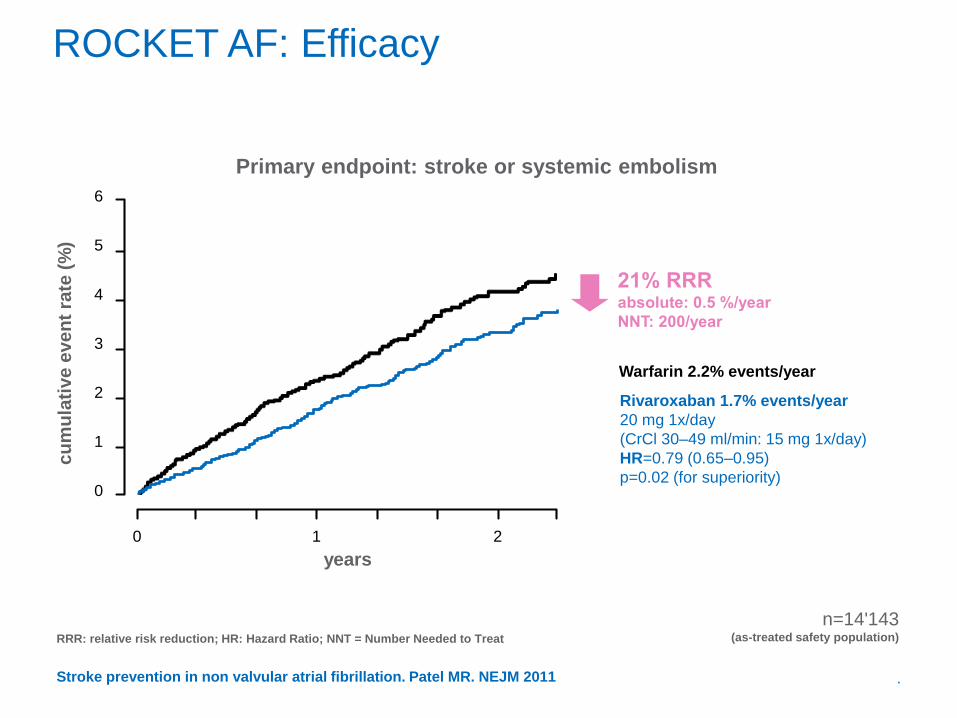
Warfarin 2.2% events/year
Rivaroxaban 1.7% events/year
20 mg 1x/day
(CrCl 30–49 ml/min: 15 mg 1x/day)
HR=0.79 (0.65–0.95)
p=0.02 (for superiority)
years
n=14'143 (as-treated safety population)
ROCKET AF: Efficacy
Primary endpoint: stroke or systemic embolism
.
RRR: relative risk reduction; HR: Hazard Ratio; NNT = Number Needed to Treat
cu
mu
lati
ve
eve
nt
rate
(%
)
Stroke prevention in non valvular atrial fibrillation. Patel MR. NEJM 2011
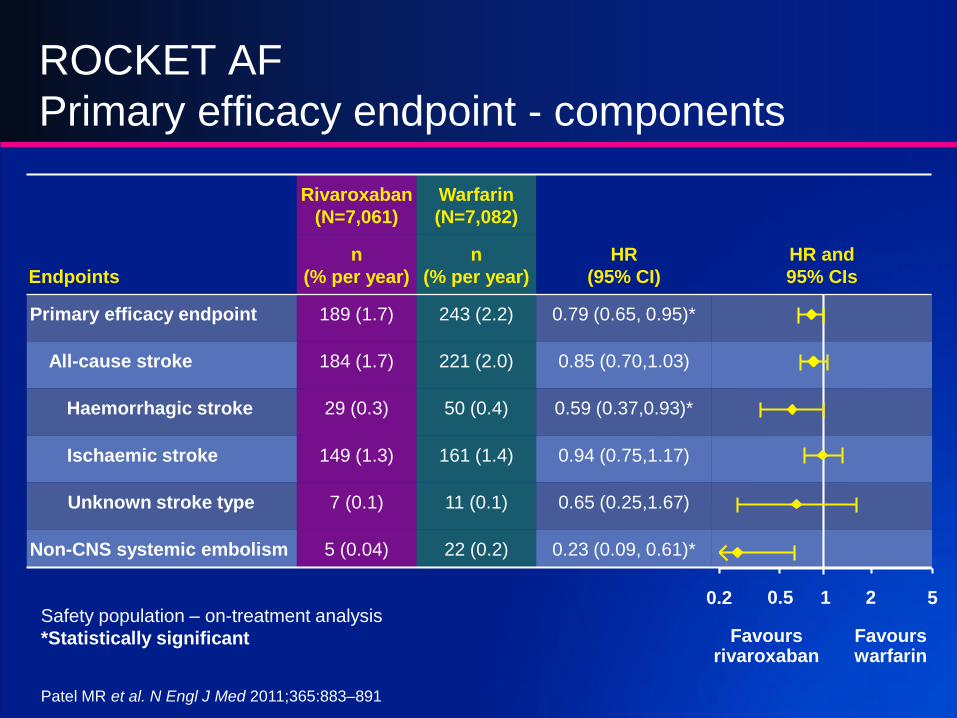
Endpoints
Rivaroxaban
(N=7,061)
Warfarin
(N=7,082)
HR
(95% CI)
HR and
95% CIs
n
(% per year)
n
(% per year)
Primary efficacy endpoint 189 (1.7) 243 (2.2) 0.79 (0.65, 0.95)*
All-cause stroke 184 (1.7) 221 (2.0) 0.85 (0.70,1.03)
Haemorrhagic stroke 29 (0.3) 50 (0.4) 0.59 (0.37,0.93)*
Ischaemic stroke 149 (1.3) 161 (1.4) 0.94 (0.75,1.17)
Unknown stroke type 7 (0.1) 11 (0.1) 0.65 (0.25,1.67)
Non-CNS systemic embolism 5 (0.04) 22 (0.2) 0.23 (0.09, 0.61)*
ROCKET AF
Primary efficacy endpoint - components
Safety population – on-treatment analysis
*Statistically significant
0.2 0.5 1 2 5
Favoursrivaroxaban
Favours warfarin
Patel MR et al. N Engl J Med 2011;365:883–891
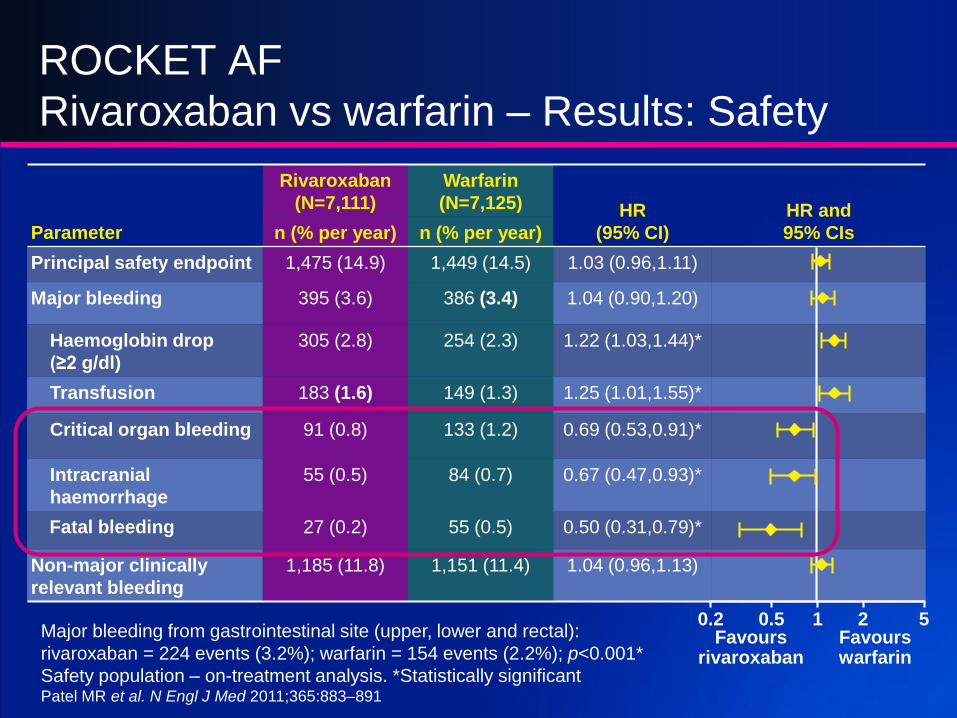
Parameter
Rivaroxaban
(N=7,111)
Warfarin
(N=7,125) HR
(95% CI)
HR and
95% CIsn (% per year) n (% per year)
Principal safety endpoint 1,475 (14.9) 1,449 (14.5) 1.03 (0.96,1.11)
Major bleeding 395 (3.6) 386 (3.4) 1.04 (0.90,1.20)
Haemoglobin drop
(≥2 g/dl)
305 (2.8) 254 (2.3) 1.22 (1.03,1.44)*
Transfusion 183 (1.6) 149 (1.3) 1.25 (1.01,1.55)*
Critical organ bleeding 91 (0.8) 133 (1.2) 0.69 (0.53,0.91)*
Intracranial
haemorrhage
55 (0.5) 84 (0.7) 0.67 (0.47,0.93)*
Fatal bleeding 27 (0.2) 55 (0.5) 0.50 (0.31,0.79)*
Non-major clinically
relevant bleeding
1,185 (11.8) 1,151 (11.4) 1.04 (0.96,1.13)
ROCKET AF
Rivaroxaban vs warfarin – Results: Safety
Major bleeding from gastrointestinal site (upper, lower and rectal):
rivaroxaban = 224 events (3.2%); warfarin = 154 events (2.2%); p<0.001*
Safety population – on-treatment analysis. *Statistically significant
0.2 0.5 1 2 5Favours
rivaroxabanFavours warfarin
Patel MR et al. N Engl J Med 2011;365:883–891
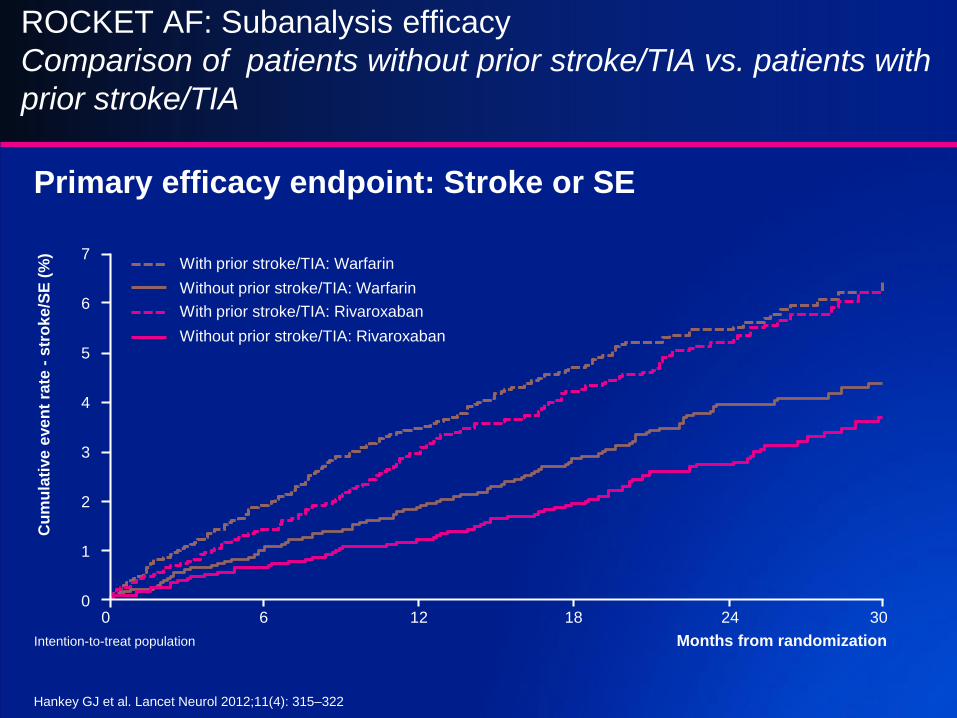
ROCKET AF: Subanalysis efficacy
Comparison of patients without prior stroke/TIA vs. patients with
prior stroke/TIA
Cu
mu
lati
ve
eve
nt
rate
-s
tro
ke
/SE
(%
)
Months from randomization
0
1
2
3
0
4
5
6
7
306 12 18 24
With prior stroke/TIA: Warfarin
Without prior stroke/TIA: Warfarin
With prior stroke/TIA: Rivaroxaban
Without prior stroke/TIA: Rivaroxaban
Primary efficacy endpoint: Stroke or SE
Intention-to-treat population
Hankey GJ et al. Lancet Neurol 2012;11(4): 315–322
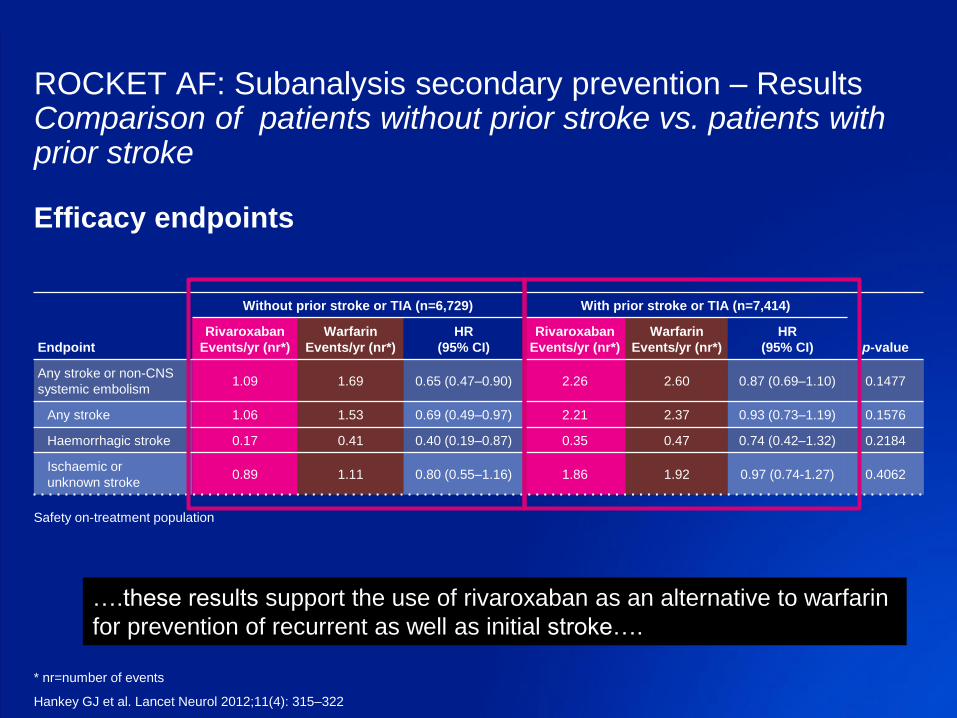
ROCKET AF: Subanalysis secondary prevention – ResultsComparison of patients without prior stroke vs. patients withprior stroke
Endpoint
Without prior stroke or TIA (n=6,729) With prior stroke or TIA (n=7,414)
p-value
Rivaroxaban
Events/yr (nr*)
Warfarin
Events/yr (nr*)
HR
(95% CI)
Rivaroxaban
Events/yr (nr*)
Warfarin
Events/yr (nr*)
HR
(95% CI)
Any stroke or non-CNS
systemic embolism1.09 1.69 0.65 (0.47–0.90) 2.26 2.60 0.87 (0.69–1.10) 0.1477
Any stroke 1.06 1.53 0.69 (0.49–0.97) 2.21 2.37 0.93 (0.73–1.19) 0.1576
Haemorrhagic stroke 0.17 0.41 0.40 (0.19–0.87) 0.35 0.47 0.74 (0.42–1.32) 0.2184
Ischaemic or
unknown stroke0.89 1.11 0.80 (0.55–1.16) 1.86 1.92 0.97 (0.74-1.27) 0.4062
Efficacy endpoints
Safety on-treatment population
* nr=number of events
Hankey GJ et al. Lancet Neurol 2012;11(4): 315–322
….these results support the use of rivaroxaban as an alternative to warfarin
for prevention of recurrent as well as initial stroke….
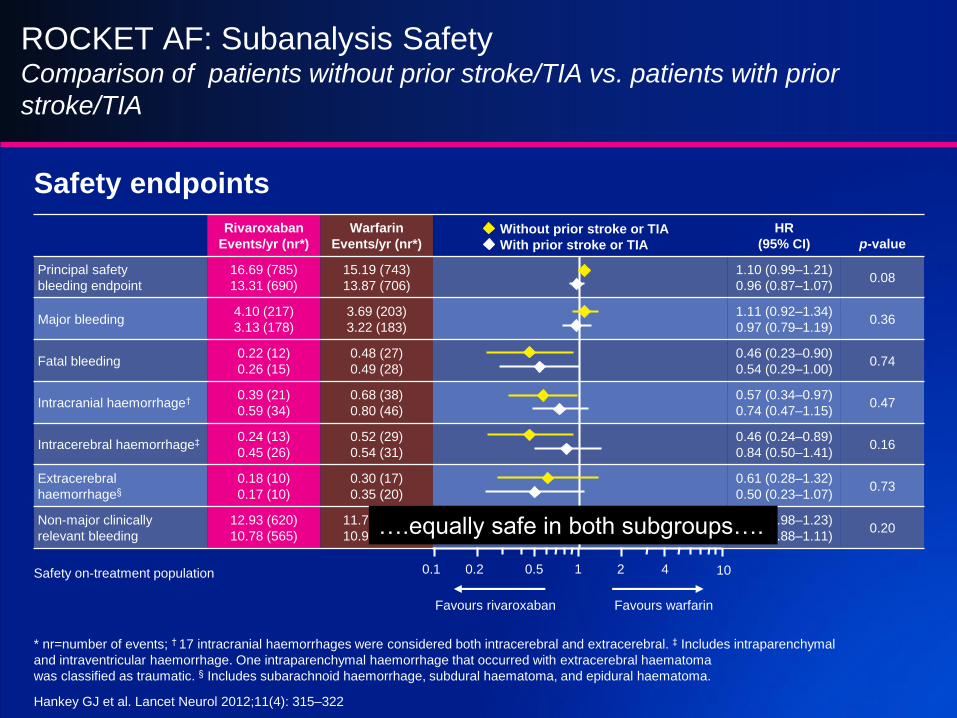
ROCKET AF: Subanalysis SafetyComparison of patients without prior stroke/TIA vs. patients with prior
stroke/TIA
Rivaroxaban
Events/yr (nr*)
Warfarin
Events/yr (nr*)
HR
(95% CI) p-value
Principal safety
bleeding endpoint
16.69 (785)
13.31 (690)
15.19 (743)
13.87 (706)
1.10 (0.99–1.21)
0.96 (0.87–1.07)0.08
Major bleeding4.10 (217)
3.13 (178)
3.69 (203)
3.22 (183)
1.11 (0.92–1.34)
0.97 (0.79–1.19)0.36
Fatal bleeding0.22 (12)
0.26 (15)
0.48 (27)
0.49 (28)
0.46 (0.23–0.90)
0.54 (0.29–1.00)0.74
Intracranial haemorrhage† 0.39 (21)
0.59 (34)
0.68 (38)
0.80 (46)
0.57 (0.34–0.97)
0.74 (0.47–1.15)0.47
Intracerebral haemorrhage‡ 0.24 (13)
0.45 (26)
0.52 (29)
0.54 (31)
0.46 (0.24–0.89)
0.84 (0.50–1.41)0.16
Extracerebral
haemorrhage§
0.18 (10)
0.17 (10)
0.30 (17)
0.35 (20)
0.61 (0.28–1.32)
0.50 (0.23–1.07)0.73
Non-major clinically
relevant bleeding
12.93 (620)
10.78 (565)
11.78 (585)
10.98 (566)
1.10 (0.98–1.23)
0.99 (0.88–1.11)0.20
Safety endpoints
Safety on-treatment population
Without prior stroke or TIA
With prior stroke or TIA
* nr=number of events; † 17 intracranial haemorrhages were considered both intracerebral and extracerebral. ‡ Includes intraparenchymal
and intraventricular haemorrhage. One intraparenchymal haemorrhage that occurred with extracerebral haematoma
was classified as traumatic. § Includes subarachnoid haemorrhage, subdural haematoma, and epidural haematoma.
Hankey GJ et al. Lancet Neurol 2012;11(4): 315–322
101
Favours warfarin
0.1 0.2 0.5 2 4
Favours rivaroxaban
….equally safe in both subgroups….
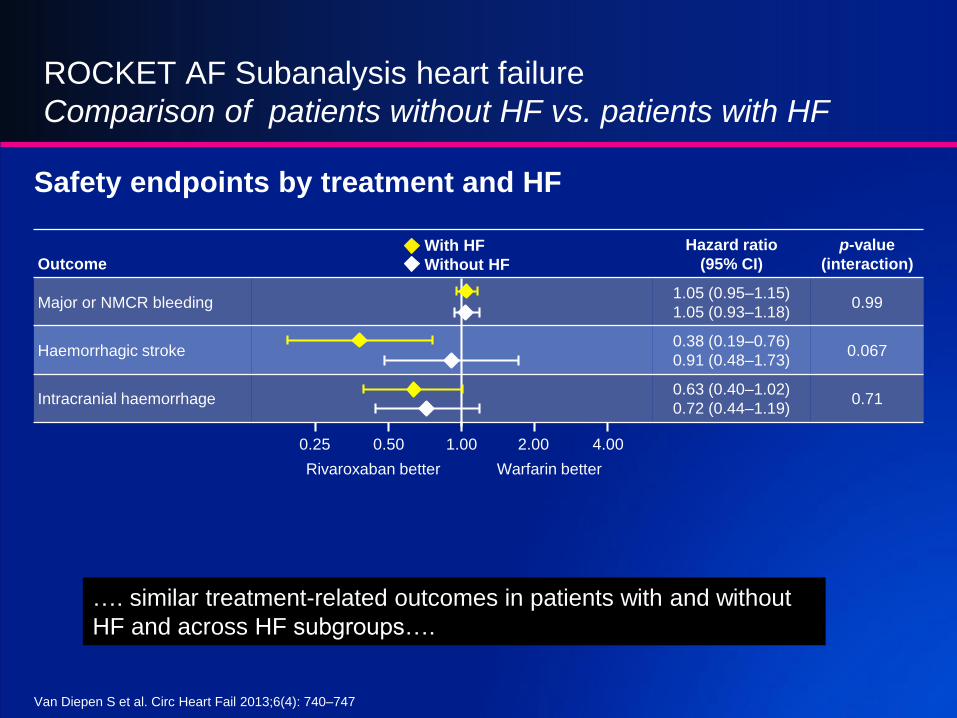
ROCKET AF Subanalysis heart failure
Comparison of patients without HF vs. patients with HF
Outcome
Hazard ratio
(95% CI)
p-value
(interaction)
Major or NMCR bleeding1.05 (0.95–1.15)
1.05 (0.93–1.18)0.99
Haemorrhagic stroke0.38 (0.19–0.76)
0.91 (0.48–1.73)0.067
Intracranial haemorrhage0.63 (0.40–1.02)
0.72 (0.44–1.19)0.71
Van Diepen S et al. Circ Heart Fail 2013;6(4): 740–747
Rivaroxaban better Warfarin better
1.00 2.00 4.000.500.25
With HF
Without HF
Safety endpoints by treatment and HF
…. similar treatment-related outcomes in patients with and without
HF and across HF subgroups….
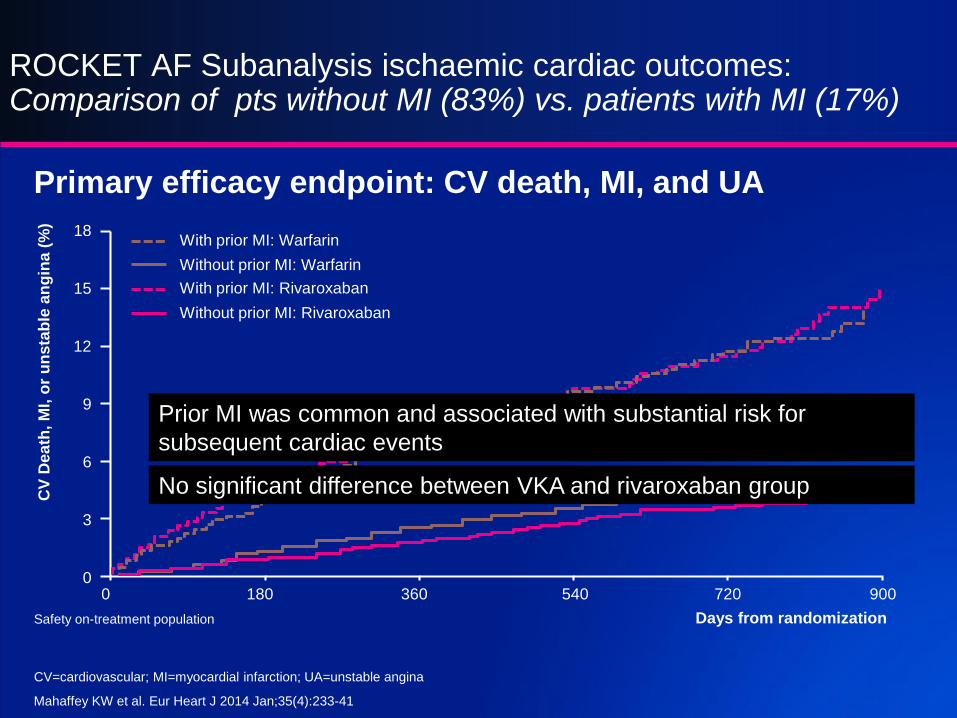
ROCKET AF Subanalysis ischaemic cardiac outcomes:Comparison of pts without MI (83%) vs. patients with MI (17%)
Primary efficacy endpoint: CV death, MI, and UA
Mahaffey KW et al. Eur Heart J 2014 Jan;35(4):233-41
CV
Dea
th, M
I, o
r u
ns
tab
le a
ng
ina
(%
)
Days from randomization
0
3
6
9
0
12
15
18
900180 360 540 720
With prior MI: Warfarin
Without prior MI: Warfarin
With prior MI: Rivaroxaban
Without prior MI: Rivaroxaban
Safety on-treatment population
CV=cardiovascular; MI=myocardial infarction; UA=unstable angina
Prior MI was common and associated with substantial risk for
subsequent cardiac events
No significant difference between VKA and rivaroxaban group
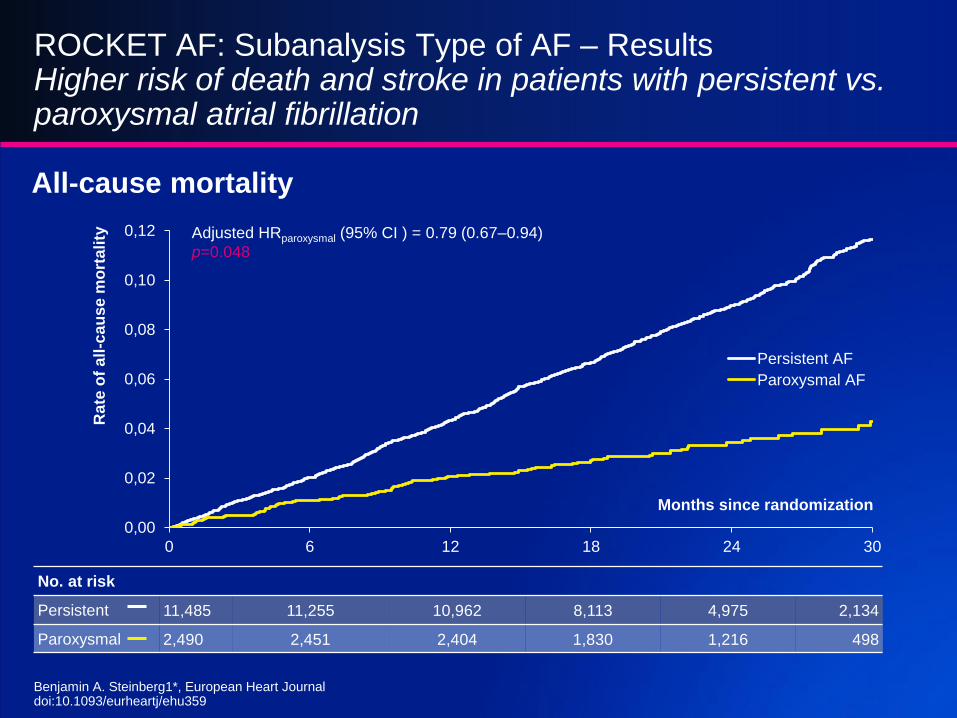
ROCKET AF: Subanalysis Type of AF – ResultsHigher risk of death and stroke in patients with persistent vs. paroxysmal atrial fibrillation
All-cause mortality
0,00
0,02
0,04
0,06
0,08
0,10
0,12
0 6 12 18 24 30
Ra
te o
f a
ll-c
au
se
mo
rtali
ty
Months since randomization
Persistent AF
Paroxysmal AF
Adjusted HRparoxysmal (95% CI ) = 0.79 (0.67–0.94)
p=0.048
No. at risk
Persistent 11,485 11,255 10,962 8,113 4,975 2,134
Paroxysmal 2,490 2,451 2,404 1,830 1,216 498
Benjamin A. Steinberg1*, European Heart Journaldoi:10.1093/eurheartj/ehu359
Lip YH, Windecker S et. al EHJ 2014.
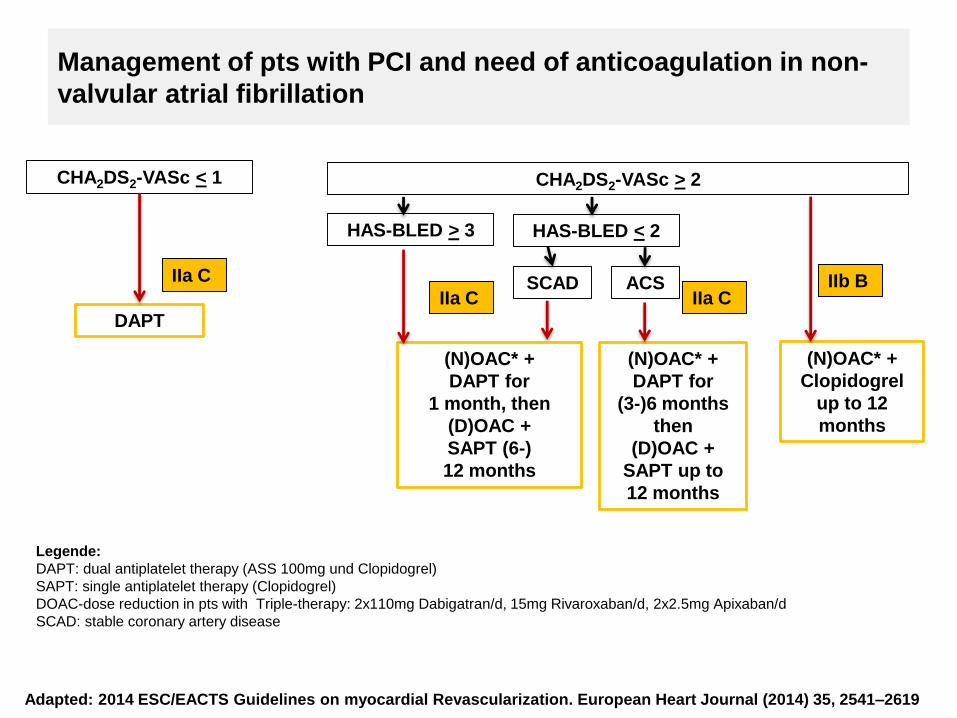
Management of pts with PCI and need of anticoagulation in non-
valvular atrial fibrillation
CHA2DS2-VASc < 1 CHA2DS2-VASc > 2
DAPT
IIa C
(N)OAC* +
Clopidogrel
up to 12
months
IIb BSCAD ACS
HAS-BLED < 2
IIa C
(N)OAC* +
DAPT for
(3-)6 months
then
(D)OAC +
SAPT up to
12 months
HAS-BLED > 3
IIa C
(N)OAC* +
DAPT for
1 month, then
(D)OAC +
SAPT (6-)
12 months
Adapted: 2014 ESC/EACTS Guidelines on myocardial Revascularization. European Heart Journal (2014) 35, 2541–2619
Legende:
DAPT: dual antiplatelet therapy (ASS 100mg und Clopidogrel)
SAPT: single antiplatelet therapy (Clopidogrel)
DOAC-dose reduction in pts with Triple-therapy: 2x110mg Dabigatran/d, 15mg Rivaroxaban/d, 2x2.5mg Apixaban/d
SCAD: stable coronary artery disease
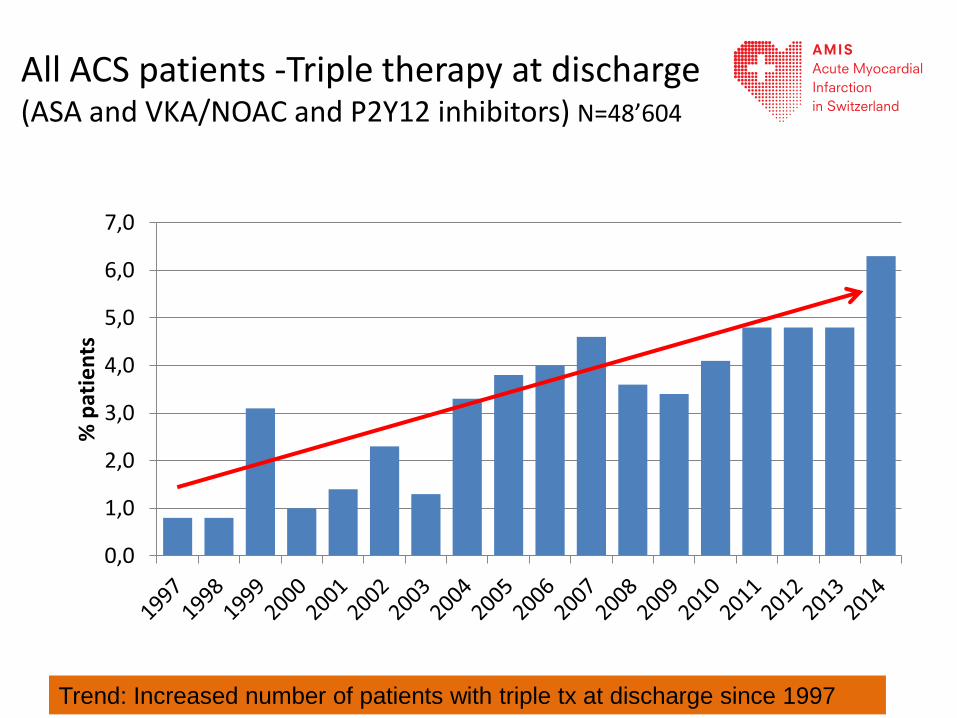
All ACS patients -Triple therapy at discharge (ASA and VKA/NOAC and P2Y12 inhibitors) N=48’604
0,0
1,0
2,0
3,0
4,0
5,0
6,0
7,0
% p
atie
nts
Trend: Increased number of patients with triple tx at discharge since 1997
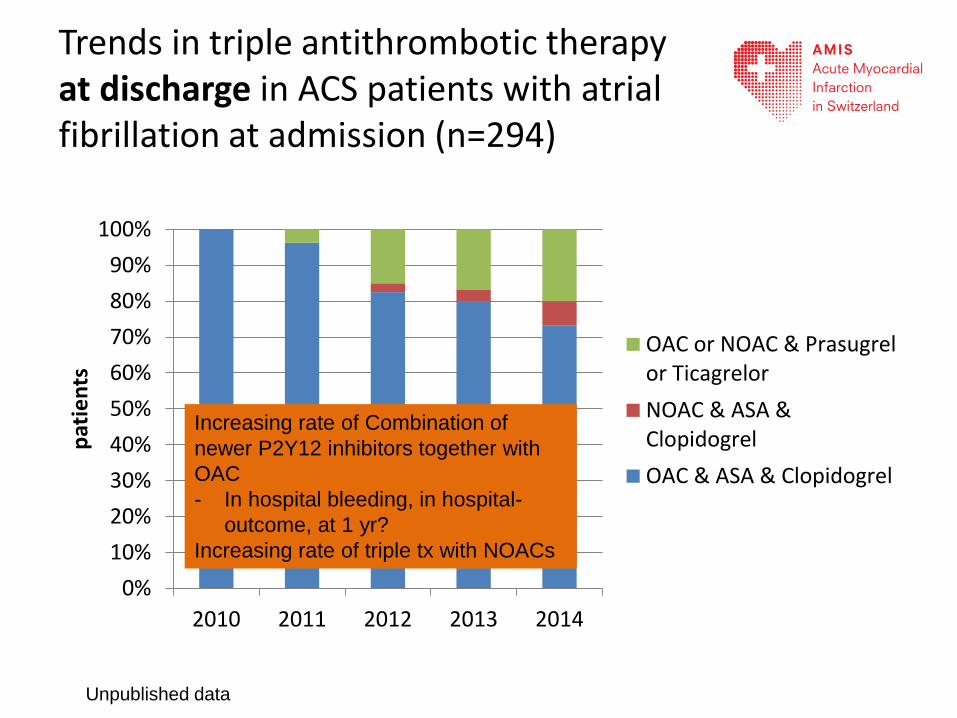
Trends in triple antithrombotic therapy at discharge in ACS patients with atrial fibrillation at admission (n=294)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2010 2011 2012 2013 2014
pat
ien
ts
OAC or NOAC & Prasugrelor Ticagrelor
NOAC & ASA &Clopidogrel
OAC & ASA & Clopidogrel
Increasing rate of Combination of
newer P2Y12 inhibitors together with
OAC
- In hospital bleeding, in hospital-
outcome, at 1 yr?
Increasing rate of triple tx with NOACs
Unpublished data
Open question: Potential Role (Risks and benefits)
of NOACs in ACS
no interaction with (dual) antiplatelet therapy on both efficacy
and bleeding in the AF trials with NOAC
it might be assumed that
the respective advantages of the NOAC over VKA are maintained
in dual or triple therapy.
In addition, there was also no interaction between SAPT vs. DAPT
in the ACS trials with the NOACs apixaban and rivaroxaban
Not enough data of the AMIS-plus population to make any
conclusion – more data needed!
Summary I
• ROCKET provides the largest prospective experience
involving high-risk elderly patients with AF comparing
Warfarin vs. Rivaroxaban
• Efficacy: Significantly fewer cases of haemorrhagic stroke
were observed in patients on rivaroxaban
• Safety: less fatal/intracranial bleedings and more
gastrointestinal bleedings in patients on rivaroxaban
Summary II
• Subanalysis:
– Consistent efficacy and safety of rivaroxaban compared with warfarin in
pts without prior stroke and with prior stroke
– similar treatment-related outcomes in patients with and without HF and
across HF subgroups
– Prior MI was common (17%) and associated with substantial risk for
subsequent cardiac events
– Persistent Afib subgroup associated with higher subsequent all-cause
mortality rate
Summary III
• An increasing number of ACS patients with Afib in Switzerland
gets triple antithrombotic therapy with NOACs
– In contrast of to the guidelines – a substantial number of ACS Afib
patients is treated with Prasugrel or Ticagrelor in combination with
anticoagulation (VKA or NOACs)
• Ongoing Rivaroxan Study (PIONEER-PCI) is addressing the safety
aspects of this clinically important question (PCI in Afib)
Back-up information
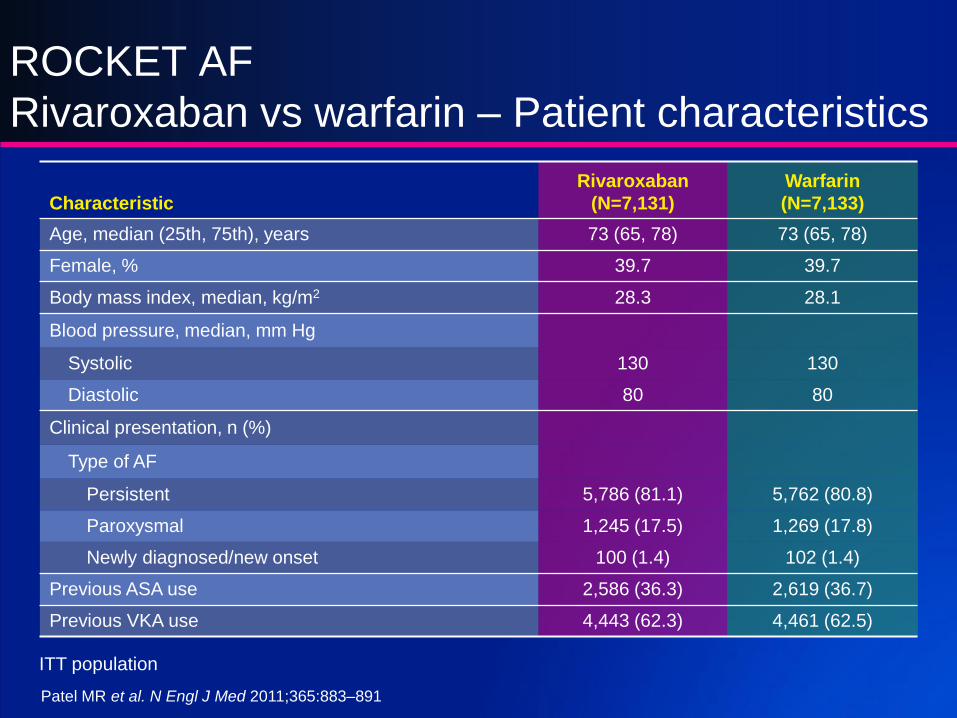
ROCKET AF
Rivaroxaban vs warfarin – Patient characteristics
Characteristic
Rivaroxaban
(N=7,131)
Warfarin
(N=7,133)
Age, median (25th, 75th), years 73 (65, 78) 73 (65, 78)
Female, % 39.7 39.7
Body mass index, median, kg/m2 28.3 28.1
Blood pressure, median, mm Hg
Systolic 130 130
Diastolic 80 80
Clinical presentation, n (%)
Type of AF
Persistent 5,786 (81.1) 5,762 (80.8)
Paroxysmal 1,245 (17.5) 1,269 (17.8)
Newly diagnosed/new onset 100 (1.4) 102 (1.4)
Previous ASA use 2,586 (36.3) 2,619 (36.7)
Previous VKA use 4,443 (62.3) 4,461 (62.5)
ITT population
Patel MR et al. N Engl J Med 2011;365:883–891
ROCKET AF
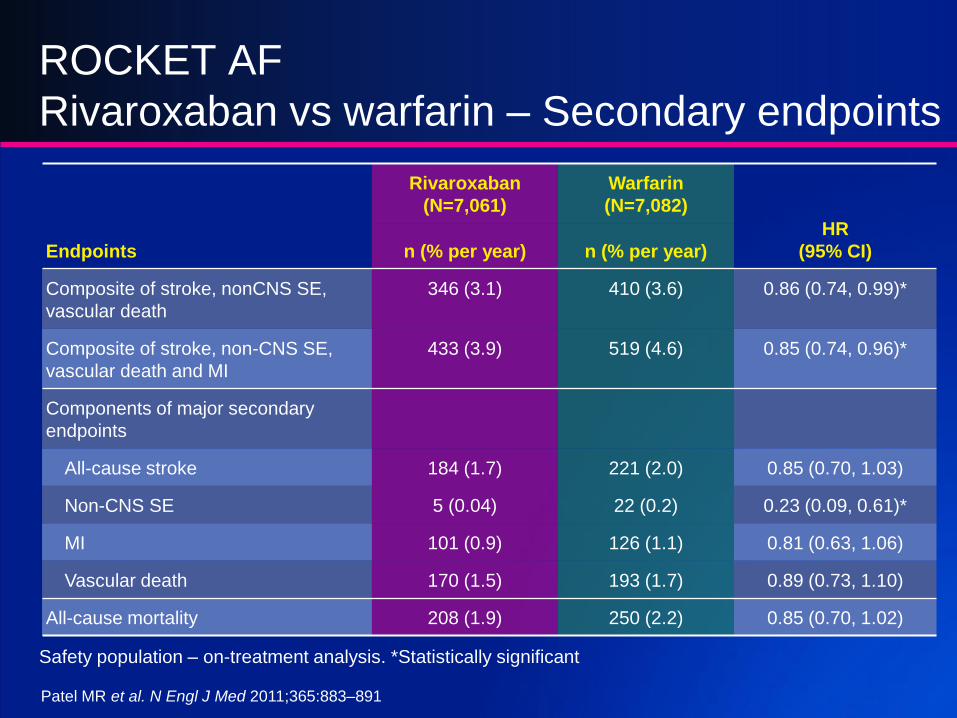
Rivaroxaban vs warfarin – Secondary endpoints
Safety population – on-treatment analysis. *Statistically significant
Endpoints
Rivaroxaban
(N=7,061)
Warfarin
(N=7,082)
HR
(95% CI)n (% per year) n (% per year)
Composite of stroke, nonCNS SE,
vascular death
346 (3.1) 410 (3.6) 0.86 (0.74, 0.99)*
Composite of stroke, non-CNS SE,
vascular death and MI
433 (3.9) 519 (4.6) 0.85 (0.74, 0.96)*
Components of major secondary
endpoints
All-cause stroke 184 (1.7) 221 (2.0) 0.85 (0.70, 1.03)
Non-CNS SE 5 (0.04) 22 (0.2) 0.23 (0.09, 0.61)*
MI 101 (0.9) 126 (1.1) 0.81 (0.63, 1.06)
Vascular death 170 (1.5) 193 (1.7) 0.89 (0.73, 1.10)
All-cause mortality 208 (1.9) 250 (2.2) 0.85 (0.70, 1.02)
Patel MR et al. N Engl J Med 2011;365:883–891
L.C
H.H
C.0
1.2
015.0
581-D
E/E
N
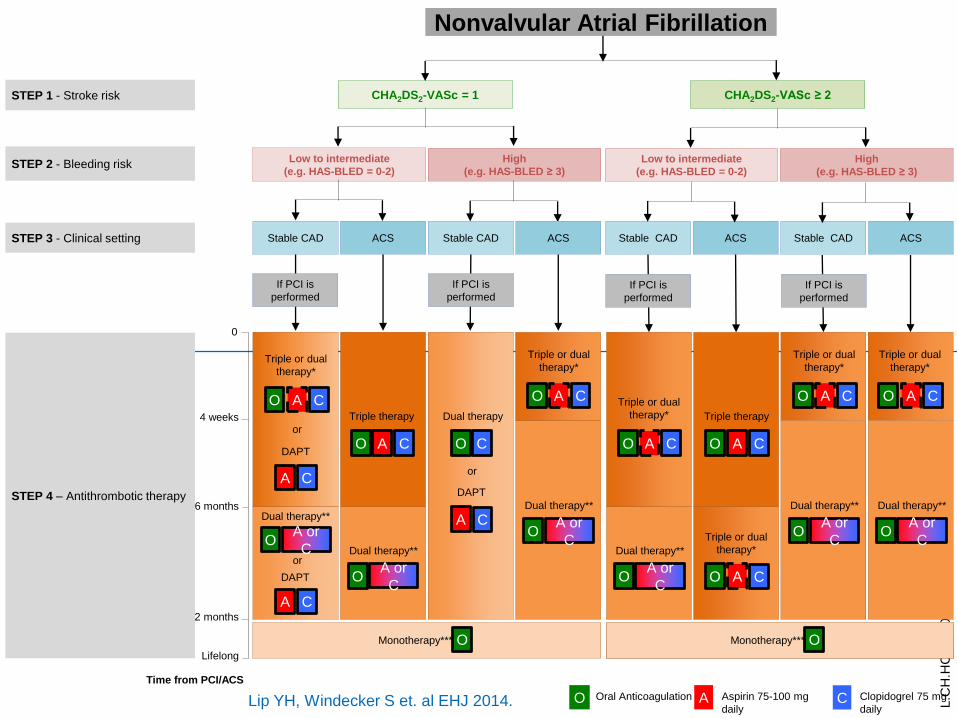
Low to intermediate
(e.g. HAS-BLED = 0-2)
High
(e.g. HAS-BLED ≥ 3)
CHA2DS2-VASc = 1 CHA2DS2-VASc ≥ 2
Nonvalvular Atrial Fibrillation
0
4 weeks
12 months
6 months
STEP 2 - Bleeding risk
STEP 1 - Stroke risk
STEP 3 - Clinical setting Stable CAD ACS Stable CAD ACS
Lifelong
Stable CAD ACS Stable CAD ACS
Low to intermediate
(e.g. HAS-BLED = 0-2)
High
(e.g. HAS-BLED ≥ 3)
STEP 4 – Antithrombotic therapy
Time from PCI/ACS
A CO
A C
O
A C A or
CO
Dual therapy**
A CO A CO
Triple therapy
A CO
A CO
A CO
Triple or dual
therapy*
A CO
Triple or dual
therapy*
Triple or dual
therapy*
Triple or dual
therapy*
DAPT
DAPT
Dual therapy**
A CO Oral Anticoagulation Aspirin 75-100 mg
daily
Clopidogrel 75 mg
daily
OMonotherapy***
A or
CO
Dual therapy**
A or
CO
Dual therapy**
A or
CO
Dual therapy**
A or
CO
Dual therapy**
A or
C
O
Dual therapy
or
OMonotherapy***
or
A CO
Triple or dual
therapy*
Triple or dual
therapy*
C
Triple therapy
A C
DAPT
or
If PCI is
performed
If PCI is
performedIf PCI is
performed
If PCI is
performed
Lip YH, Windecker S et. al EHJ 2014.
L.C
H.H
C.0
1.2
015.0
581-D
E/E
N
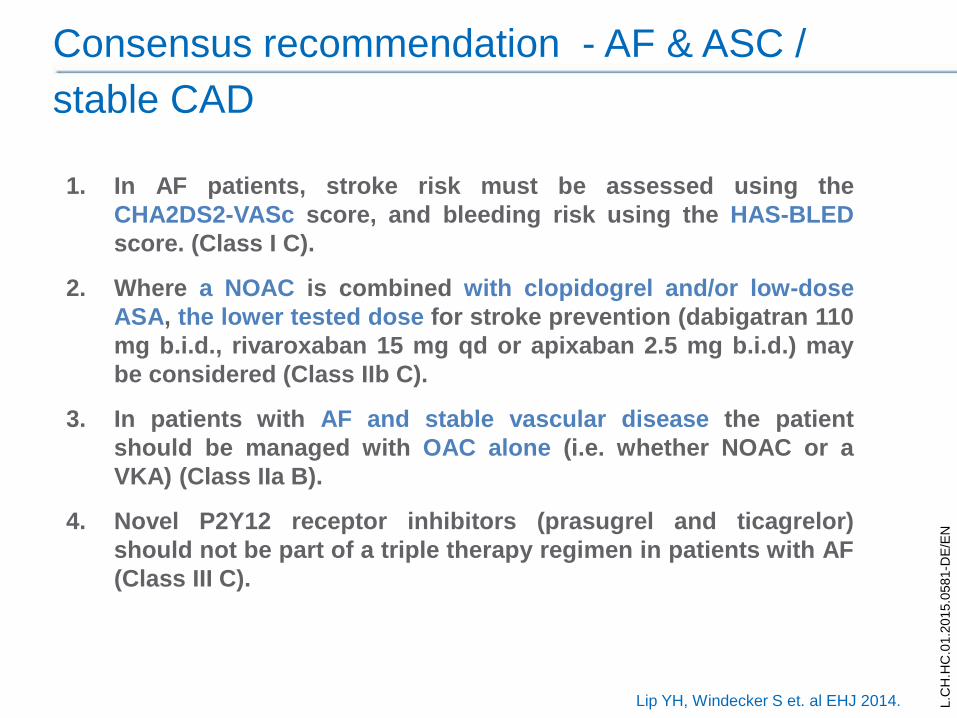
Consensus recommendation - AF & ASC /
stable CAD
1. In AF patients, stroke risk must be assessed using the
CHA2DS2-VASc score, and bleeding risk using the HAS-BLED
score. (Class I C).
2. Where a NOAC is combined with clopidogrel and/or low-dose
ASA, the lower tested dose for stroke prevention (dabigatran 110
mg b.i.d., rivaroxaban 15 mg qd or apixaban 2.5 mg b.i.d.) may
be considered (Class IIb C).
3. In patients with AF and stable vascular disease the patient
should be managed with OAC alone (i.e. whether NOAC or a
VKA) (Class IIa B).
4. Novel P2Y12 receptor inhibitors (prasugrel and ticagrelor)
should not be part of a triple therapy regimen in patients with AF
(Class III C).
Lip YH, Windecker S et. al EHJ 2014.
L.C
H.H
C.0
1.2
015.0
581-D
E/E
N
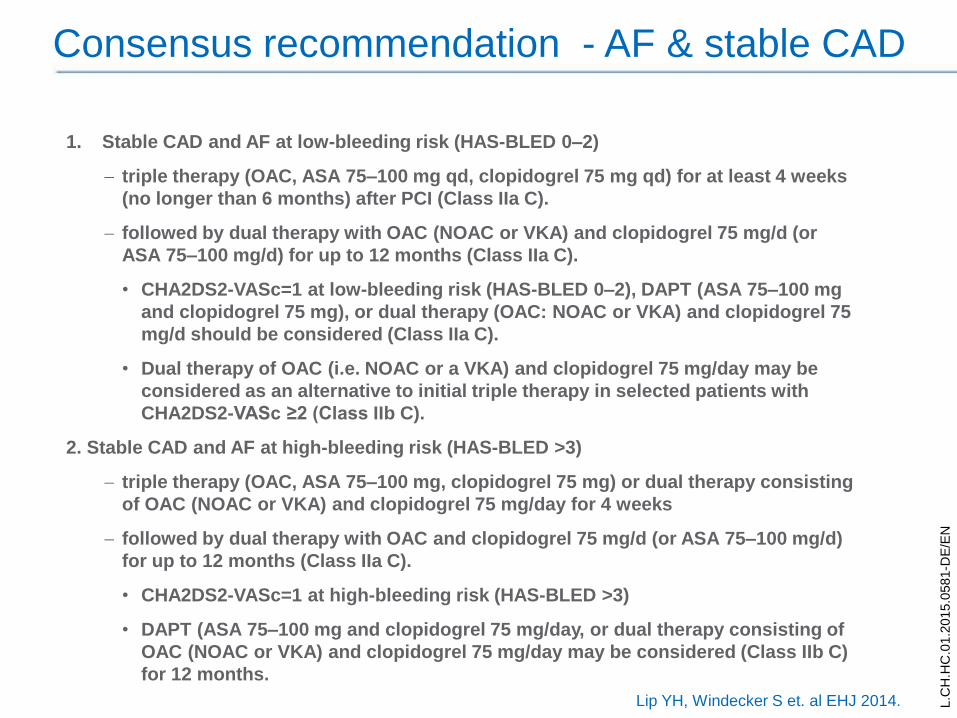
Consensus recommendation - AF & stable CAD
1. Stable CAD and AF at low-bleeding risk (HAS-BLED 0–2)
triple therapy (OAC, ASA 75–100 mg qd, clopidogrel 75 mg qd) for at least 4 weeks
(no longer than 6 months) after PCI (Class IIa C).
followed by dual therapy with OAC (NOAC or VKA) and clopidogrel 75 mg/d (or
ASA 75–100 mg/d) for up to 12 months (Class IIa C).
• CHA2DS2-VASc=1 at low-bleeding risk (HAS-BLED 0–2), DAPT (ASA 75–100 mg
and clopidogrel 75 mg), or dual therapy (OAC: NOAC or VKA) and clopidogrel 75
mg/d should be considered (Class IIa C).
• Dual therapy of OAC (i.e. NOAC or a VKA) and clopidogrel 75 mg/day may be
considered as an alternative to initial triple therapy in selected patients with
CHA2DS2-VASc ≥2 (Class IIb C).
2. Stable CAD and AF at high-bleeding risk (HAS-BLED >3)
triple therapy (OAC, ASA 75–100 mg, clopidogrel 75 mg) or dual therapy consisting
of OAC (NOAC or VKA) and clopidogrel 75 mg/day for 4 weeks
followed by dual therapy with OAC and clopidogrel 75 mg/d (or ASA 75–100 mg/d)
for up to 12 months (Class IIa C).
• CHA2DS2-VASc=1 at high-bleeding risk (HAS-BLED >3)
• DAPT (ASA 75–100 mg and clopidogrel 75 mg/day, or dual therapy consisting of
OAC (NOAC or VKA) and clopidogrel 75 mg/day may be considered (Class IIb C)
for 12 months.
Lip YH, Windecker S et. al EHJ 2014.
L.C
H.H
C.0
1.2
015.0
581-D
E/E
N
Consensus recommendation - AF & stable CAD
3. Long-term antithrombotic therapy with OAC (NOAC or
VKA) (beyond 12 months) is recommended in all patients
(Class I B).
Combination OAC plus single antiplatelet therapy
(clopidogrel 75 mg/day or ASA 75–100 mg/day)] may be
considered in very selected cases, e.g. stenting of the
left main, proximal left anterior descending, proximal
bifurcation, recurrent MIs, etc. (Class IIb, C).
4. Gastric protection with PPIs should be considered in
patients with OAC plus antiplatelet therapy (Class IIa, C).
Lip YH, Windecker S et. al EHJ 2014.
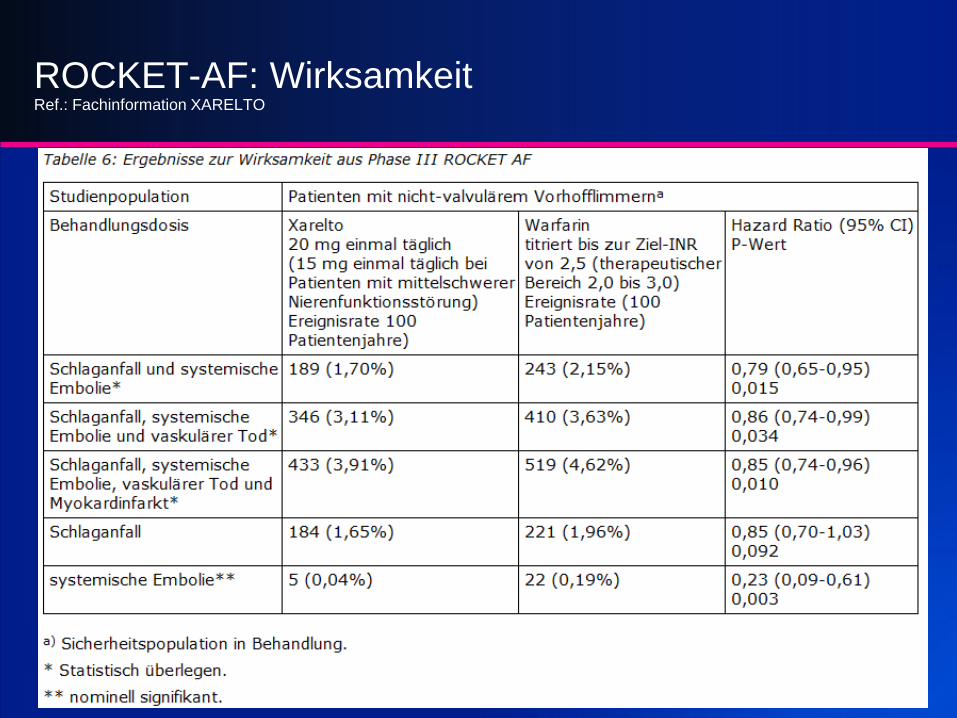
ROCKET-AF: WirksamkeitRef.: Fachinformation XARELTO











![[2014서울국제공연예술제(SPAF) 라인업 소개]theater.arko.or.kr/Down/Board/201407/[서울국제공연...- 1 - [2014서울국제공연예술제(SPAF) 라인업 소개] 1](https://img.dokumen.tips/doc/110x75/5e68370ab1c6071fc247607e/2014oeeoeeoespaf-e-oeeoe-oeeoee-.jpg)