Embed Size (px)
Citation preview

Pediatr Blood Cancer 2008;51:375–379
Risk Factors for Readmission After Initial Diagnosis in ChildrenWith Acute Lymphoblastic Leukemia
Tamra L. Slone, MD,1,2* Rachna Rai,1 Naveed Ahmad, MD, MPH,2 and Naomi J. Winick, MD1,2
INTRODUCTION
In the United States, 2,500 children are diagnosed annually with
acute lymphoblastic leukemia (ALL) [1,2]. With improvements in
the treatment of ALL, cure rates now approach 80% [1,2]. However,
infectious complications continue as a major cause of morbidity and
mortality [3–5]. Many studies have evaluated potential prognostic
factors for infection among children with ALL hospitalized for
fever and neutropenia, after achieving remission. These studies
have identified risk factors that differentiate those most likely to
have a serious infection versus those likely to recover quickly and
uneventfully [6–8]. As a result, common criteria for safe discharge
following an admission for fever and neutropenia have been
established and include a rising absolute neutrophil count (ANC),
resolution of fever, and negative blood cultures [6–8].
During induction therapy, when neutropenia results from
leukemia as well as chemotherapy induced myelosuppression,
evidence of bone marrow and blood count recovery can be delayed
and fever is variably attributed to infection and/or the primary
disease [9]. Additionally, no data are available regarding the risk of
readmission for fever and/or infection following initial hospital
discharge after diagnosis of ALL. This retrospective cohort study
was designed to evaluate the risk factors for readmission during the
induction phase of therapy.
METHODS
Design
A retrospective review of the records of all patients, between the
ages of 1 and 19 years, with B-precursor ALL, newly diagnosed
at Children’s Medical Center Dallas between January 1, 2001 and
May 31, 2005 was conducted. The study was approved by the
Institutional Review Board of the University of Texas Southwestern
Medical Center at Dallas. Eligible patients had to have received their
entire course of induction therapy at our center and had to have been
discharged from the hospital during induction.
Definitions
Fever was defined as at least one oral temperature of 38.58C or
two consecutive temperatures of greater than 38.08C in a 24-hr
period according to our institutional policy. Induction was defined
as the first 28 days of chemotherapy following diagnosis. Infection
was defined as a positive microbiological culture (CSF, blood,
and/or urine), clinical findings of abscess or cellulitis, and/or
radiologic evidence of deep-seated soft tissue infection (i.e.,
pneumonia, typhlitis, osteomyelitis, or evidence of fungal disease).
Urine cultures were excluded if multiple bacteria were isolated and/
or if there were less than 50,000 CFU/ml of bacteria. The absolute
phagocyte count (APC) was calculated as 0.01� (%bandsþ% neutrophilsþ% monocytes)� total leukocyte count [10].
Treatment
All patients received a three- or four-drug induction regimen
based on National Cancer Institute risk group criteria [11]. The
three-drug induction included vincristine, asparaginase, and a
corticosteroid (dexamethasone or prednisone) as well as intrathecal
therapy. The four-drug induction added daunorubicin. The patients
were treated according to COG AALL0232, COG AALL0331,
CCG 1991, POG 9806, POG 9900/9906, or our institutional DFW
protocol. All of the anthracycline containing four-drug inductions
used prednisone, except the DFW protocol, which employed
Background. Specific hospital discharge criteria following theinitial diagnosis of children with acute lymphoblastic leukemia(ALL) have not been reported. This retrospective cohort study wasdesigned to identify risk factors for readmission during inductiontherapy, to assist with development of discharge guidelines.Procedure. We reviewed the records of 142 consecutive childrenwith newly diagnosed B-precursor ALL and found 129 eligiblepatients. Chi square, t-test, and multivariate logistic regressionanalysis were used to compare differences in absolute neutrophilcount (ANC), NCI risk status, age, type of corticosteroid adminis-
tered, and other potential risk factors for readmission duringinduction therapy. Results. ANC at initial hospital discharge wasthe only significant predictor of readmission for fever duringinduction therapy (P¼0.006) by multivariate analysis. Specificallyan ANC �200/mm3 at discharge had the strongest association withreadmission for fever (OR 3.3, 95% CI 1.422, 7.729). Conclusion. AnANC >200/mm3, in a clinically stable patient, is associatedwith minimal risk of readmission during induction therapy followingthe initial diagnosis of ALL. Pediatr Blood Cancer 2008;51:375–379. � 2008 Wiley-Liss, Inc.
Key words: acute lymphoblastic leukemia; children; fever; induction; infection; neutropenia
� 2008 Wiley-Liss, Inc.DOI 10.1002/pbc.21553
——————1Division of Hematology-Oncology, Department of Pediatrics,
University of Texas Southwestern Medical Center at Dallas, Dallas,
Texas; 2Children’s Medical Center Dallas, Dallas, Texas
Presented as a poster presentation at the 19th Annual Meeting of the
American Society of Pediatric Hematology/Oncology and 2006
Annual Pediatric Academic Societies Meeting, San Francisco, CA,
April 2006. Rai R, Slone T, Ahmad N, and Winick N. Evaluation of
fever in children with acute lymphoblastic lymphoma (ALL) during
induction chemotherapy, Pediatr Blood Cancer 2006;46:687.
Grant sponsor: National Center for Research Resources (NCRR), a
component of the National Institutes of Health (NIH); Grant number:
KL2RR024983; Grant sponsor: NIH Roadmap for Medical Research.
*Correspondence to: Tamra L. Slone, Department of Pediatrics,
University of Texas Southwestern Medical Center, 5323 Harry Hines
Blvd., Dallas, TX 75390-9063.
E-mail: [email protected]
Received 8 November 2007; Accepted 28 January 2008

dexamethasone. Pneumocystis carinii prophylaxis was initiated
during induction. According to institutional practice, the following
discharge criteria were utilized: (1) afebrile for a minimum of 24 hr,
(2) negative cultures for a minimum of 48 hr, (3) clinically
stable and not toxic in appearance, (4) tolerating oral medications,
(5) discharge teaching had been satisfactorily completed, and
(6) reliable transportation for emergencies and return visits had been
established.
Statistical Analysis
The primary outcome was readmission for any reason during the
induction phase of therapy. The clinical and laboratory charac-
eristics of these two patient groups (readmitted or not) were
compared utilizing Chi-square, Fisher’s exact test, and t-test, where
appropriate. Two-sided tests of significance were utilized and a
P< 0.05 was specified as statistically significant. Clinical and
laboratory differences that were statistically significant between
the two patient groups and other clinically meaningful factors were
included in a multivariate model by conditional backward stepwise
logistic regression. Please refer to Table I for a list of variables
analyzed. A receiver operating characteristic (ROC) curve was also
generated based on the results of the multivariate analysis. SPSS
version 15.0 (SPSS, Inc., Chicago, IL) statistical software was used
for all analyses.
RESULTS
There were 142 patients with newly diagnosed precursor B-cell
ALL between January 1, 2001 and May 31, 2005. Twelve patients
received at least part of their induction therapy at another institution
and one patient was never discharged from the hospital during
induction. Therefore, there were 129 eligible patients. Two patients
without a complete blood cell count within 48 hr of discharge were
excluded from analyses of ANC, APC, or platelet counts at initial
discharge. Demographic characteristics are detailed in Table II.
Fever and Infection During Initial Diagnostic Admission
Twenty-five of the 129 patients had fever at diagnosis or during
their initial hospitalization; seven (28%) were readmitted during
induction therapy with fever. Conversely, there were 104 children
who did not have fever during their initial admission and 24 (23%)
were readmitted.
Ten patients had had positive blood cultures during their initial
admission, and six were readmitted. Three were readmitted with
bacteremia due to a different organism from that cultured during the
initial hospital stay. Four other patients initially presented with
pneumonia, cellulitis, or a urinary tract infection without a positive
blood culture and none were readmitted for fever or infection. The
remaining 115 patients did not have a documented infection during
their initial hospitalization.
The only death among the 129 patients studied occurred in
a child with a blood culture positive for coagulase negative
staphylococcus during her initial hospitalization. This child was
discharged with an ANC of 14/mm3 to complete a course of van-
comycin at home on day 8 of induction. She was readmitted on day
12 with fever; Klebsiella pneumoniae, E. coli, and Candida
tropicalis were cultured from her blood within 48 hr, and she died
on day 26 of induction from a disseminated Candida infection.
Readmission During Induction
Of the 129 eligible patients, 50 (39%) were readmitted during
induction, with six (5%) requiring readmission twice (for a total
of 56 admissions). Thirty-one (62%) of the readmissions during
induction therapy were for fever. One patient was readmitted
for dehydration but was also found to have cellulitis of her port
site and bacteremia, without fever. Four variables were statistically
significant when evaluating readmission for fever by bivariate
analysis: ANC at initial discharge, APC at initial discharge, positive
blood culture during initial admission, and platelet count at
discharge (Tables III and IV).
Nineteen patients (38% of readmissions) were readmitted
primarily for reasons other than fever during induction; one of these
patients was readmitted twice. The reasons for readmission were
hyperglycemia (N¼ 3), pain (N¼ 3), altered mental status or seizures
(N¼ 3), dehydration (N¼ 3), pancreatitis (N¼ 2), abdominal
distention (N¼ 1), intussusception (N¼ 1), constipation (N¼ 1),
Pediatr Blood Cancer DOI 10.1002/pbc
TABLE I. Variables Analyzed in Bivariate and MultivariateAnalysis to Compare Those Who Were Readmitted to Those WhoWere Not
Bivariate variables
Age at diagnosis
WBC count at diagnosis
Hemoglobin at diagnosis
Platelet count at diagnosis
Ethnicity
Antibiotics prior to diagnosis
Fever prior to diagnosis
Fever during initial admission
Antibiotics during initial admission
Antifungals during initial admission
Positive blood culture during initial admission
Tissue infection during initial admission
Day of initial discharge
ANC at discharge
APC at discharge
Platelet count at discharge
Prednisone versus dexamethasone
Use of daunorubicin
Use of daunorubicin and dexamethasone
Day 8 marrow status
Day 15 marrow status
Day 29 marrow status
Insulin dependent
Rising versus stable/decreasing ANCa
Rising versus stable/decreasing APCa
Rising versus stable/decreasing platelet counta
Multivariate variables
ANC at discharge
Positive blood culture during initial admission
Age at diagnosis
Use of daunorubicin
Insulin dependent
Tissue infection during initial admission
Day of discharge
WBC, white blood cell count; ANC, absolute neutrophil count; APC,
absolute phagocyte count. aRising versus stable/decreasing ANC, APC,
and platelet count were determined by comparing the discharge value to
the next value obtained (i.e., day 8 or day 15 value).
376 Slone et al.

anemia (N¼ 1), and epistaxis (N¼ 1). There were no variables
predictive of readmission for reasons other than fever.
ANC at Initial Discharge
By multivariate analysis, ANC was the only variable found to
be a significant predictor of readmission for fever (P¼ 0.006).
The mean ANC at discharge for those readmitted was 335/mm3
compared to 681/mm3 for those who were not. Patients discharged
with an ANC <500/mm3 were not statistically significantly more
likely to be readmitted (P¼ 0.056, OR 2.45, 95% CI 0.962–6.236)
than those with an ANC >500/mm3. All values equal to or below
an ANC of 400/mm3 were statistically significant; therefore, an
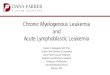
ROC curve was generated to determine the most predictive ANC at
discharge of readmission to the hospital for fever (Fig. 1). A cutoff
value of ANC �200/mm3 had the highest sensitivity and specificity
for predicting the need for readmission for fever (sensitivity¼0.645, specificity¼ 0.651). The specificity decreased significantly,
with a small rise in sensitivity, using a cutoff value of ANC
�300/mm3 or �400/mm3.
Thirty-one patients were readmitted for fever, with twenty (65%)
having had an ANC �200/mm3 at initial discharge. Twenty of the
54 (37%) patients initially discharged with an ANC �200/mm3
were readmitted compared to only 11 of the 73 (15%) patients with
ANC >200/mm3 (P¼ 0.004, odds ratio of 3.32, 95% CI 1.422,
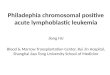
7.729). Twelve children (60%) readmitted following discharge with
an ANC �200/mm3 had either a positive blood culture (N¼ 11) or
cellulitis (N¼ 1) upon readmission whereas only two (18%) of the
patients readmitted after initial discharge with an ANC >200/mm3
had a positive blood culture (Fig. 2).
The average ANC at readmission for the 31 patients readmitted
for fever was 101/mm3. Only five of these patients had an ANC
>200/mm3 at readmission and none had an identified infection.
All 14 infections occurred in patients readmitted with an ANC
<200/mm3.
DISCUSSION
Several published studies have evaluated patients, in remission,
admitted with fever and neutropenia, so as to determine factors that
predict sepsis and/or deep-seated soft tissue infections. We used a
multivariate analysis to evaluate risk factors for readmission
after the initial diagnosis of ALL, though published observations
support the clinical significance of an ANC <200/mm3. In one
report, 37 children who remained hospitalized throughout induction
had 43 episodes of fever. Those with an ANC<200/mm3 were more
likely to have a documented infection [12]. In a separate report,
among 20 patients undergoing induction, six of the nine with an
ANC <200/mm3, readmitted for fever, had a severe infection [13].
Lastly, Jones et al. found that patients undergoing induction or
reinduction following relapse, discharged after an episode of
fever and neutropenia (N¼ 37) with an ANC <300/mm3 were at
significantly higher risk of being readmitted with fever. None of
the patients with an ANC >300/mm3 were readmitted versus 15 of
21 (71%) of those discharged with more severe neutropenia [14].
Discharge during induction therapy with an ANC >200/mm3, in
this review, was relatively safe with only 2 of 73 (2.7%) readmitted
Pediatr Blood Cancer DOI 10.1002/pbc
TABLE II. Demographic Characteristics of the 129 EvaluablePatients With Newly Diagnosed B-Precursor ALL
N (%)
Age
1–10 years 98 (76)
>10 years 31 (24)
Race
White 54 (42)
Hispanic 53 (41)
African American 13 (10)
Asian 5 (3.9)
Other 3 (2.3)
Native American 1 (0.8)
WBC at diagnosis (per/mm3)
<50,000 111 (86)
>50,000 18 (14)
Induction
Without daunorubicin 61 (47)
With daunorubicin 68 (53)
CNS status
CNS 1 88 (68)
CNS 2 39 (30)
CNS 3 2 (1.6)
Treatment protocol
POG 9900/9906 79 (61)
DFW/institutional protocol 32 (25)
AALL0232 8 (6.2)
AALL0331 6 (4.7)
POG 9806 3 (2.4)
CCG 1991 1 (0.8)
WBC, white blood cell count; CNS, central nervous system; POG,
Pediatric Oncology Group; DFW, Dallas Fort Worth Institutional
Protocol; CCG, Children’s Cancer Group.
TABLE III. Comparison of Patient Characteristics at Diagnosis and Discharge Between Those Readmitted for Fever and Those WhoWere Not
Clinical characteristic Readmission mean (range) (N¼ 31) No readmission mean (range) (N¼ 98) P-value
Age at diagnosis 5.4 years (1.7–16.3) 7.2 years (1.33–18.15) 0.06
ANC at dischargea (/mm3) 335 (10–1700) 681 (0–5016) 0.006APC at discharge (/mm3) 347 (10–1768) 732 (0–5016) 0.003Total WBC count� 103 at diagnosis (/mm3) 27 (0.8–131) 33 (0.6–688) 0.68
Day of dischargeb 4.6 days (2–11) 4.4 days (2–19) 0.70
ANC, absolute neutrophil count; APC, absolute phagocyte count; WBC, white blood cell. aThree patients did not have CBC within 48 hr of discharge
and are therefore excluded from ANC, APC, and platelet count at discharge; bThe number of days of hospitalization between the start of induction
chemotherapy and day of discharge, inclusively; does not include the period before the start of chemotherapy.
Readmission Factors for Acute Lymphoblastic Leukemia 377

with infection. This is in comparison to 12 of 54 (22%) admitted
with infection after discharge with an ANC <200/mm3. One of the
children discharged with severe neutropenia died after readmission
with sepsis. The death may have been avoidable since the child had
been discharged on single agent vancomycin while neutropenic.
Data support the continued administration of broad-spectrum
antibiotics in the face of severe neutropenia, to avoid ‘‘break-
through’’ Gram-negative sepsis [15,16].
By multivariate analysis, ANC at hospital discharge was the only
variable predictive of readmission during induction for fever and/or
infection. Patients discharged with an ANC �200/mm3 were
significantly more likely to be readmitted with fever and were more
Pediatr Blood Cancer DOI 10.1002/pbc
TABLE IV. Comparison of Other Patient Characteristics Between Those Readmitted for Fever andThose Who Were Not
Readmission
(N¼ 31)
No readmission
(N¼ 98) P-value
Odds ratio
(95% CI)
Fever at presentation/initial admission
Yes 7 18 0.61 0.76 (0.3, 1.8)
No 24 80
Antibiotics prior to diagnosis
Yes 21 69 0.78 1.24 (0.5, 3.2)
No 10 29
Positive blood culture during initial admission
Yes 6 4 0.013 5.64 (1.5, 21.5)
No 25 94
Day 8/15 marrow statusa
M1 18 60 0.82 1.14 (0.4, 3.5)
M2/M3 5 19
Corticosteroid
Prednisone 11 26 0.34 0.66 (0.3, 1.6)
Dexamethasone 20 72
Daunorubicin
No 13 48 0.49 1.33 (0.6, 3.0)
Yes 18 50
Daunorubicin and dexamethasone
Either (not both) 24 74 0.83 0.90 (0.3, 2.3)
Both 7 24
Insulin dependent
No 27 91 0.46 1.93 (0.5, 7.1)
Yes 4 7
M1, <5% blasts; M2, 5–25% blasts; M3, >25% blasts. aDay 29 marrow status not shown because only one
patient was M2/M3. Minimal residual disease values were not available on most of the patients and were not
analyzed.
Fig. 1. Receiver operator curve (ROC) which evaluates ANC at initial
discharge as a predictor for readmission for fever and/or infection.
Fig. 2. Comparison of patients with ANC >200/mm3 and ANC
�200/mm3 at initial discharge upon readmission for fever. ANC,
absolute neutrophil count.
378 Slone et al.

likely to have documented infection upon readmission. If one used
ANC>200/mm3 as a discharge criterion in this study, it would have
prolonged the stay of 54 patients and potentially prevented
the readmission of twenty patients (60% of them with infections).
The use of an ANC �300 or �400/mm3, also significant by
bivariate analysis, would have prolonged the initial hospital stay
for 12 or 20 additional patients, while only potentially preventing
2 or 3 readmissions, respectively. None of the patients in these
groups had documented infection at readmission. Although pre-
vious studies have demonstrated that a rising ANC and/or APC is
an effective guide for hospital discharge [6–8], we did not find
on bivariate analysis that a rising ANC, APC, or platelet count
at initial discharge was associated with a decreased risk of
readmission (statistics not shown). Moreover, those children with
a higher ANC at initial discharge were not more likely to have
had evidence of bone marrow recovery with a rising ANC, APC,
or platelet count than those children with an ANC <200/mm3 at
discharge.
Though an increased risk of sepsis and death has been associated
with induction therapies that include dexamethasone and an
anthracycline [17], there was no correlation between the use of
dexamethasone with daunorubicin and readmission for fever and/or
infection in the current study. This may reflect the small number of
patients who underwent a four-drug induction with dexamethasone;
only 31 of the 92 patients (34%) who received dexamethasone also
received daunorubicin.
Limits of this study include the retrospective nature of the
review. Patients were also treated on several different protocols
based on date of diagnosis and the corresponding open trial.
However, though post-induction therapy differed significantly, the
induction regimens used in these protocols were similar; typically
described as either three or four drug induction regimens. Lastly,
although the review included 129 consecutive patients, there were a
limited number of children with positive blood cultures or tissue
infections at diagnosis and a limited number with hyperglycemia
during induction therapy. This obscured the evaluation of these
variables.
In conclusion, our study demonstrates that neutropenia,
specifically an ANC <200/mm3, at the time of hospital discharge
is the strongest predictor of readmission during induction therapy
for fever and/or infection in children with newly diagnosed ALL.
Children with an ANC >200/mm3 at initial discharge had a low
incidence of readmission with infection. This finding supports the
use of an ANC threshold of 200/mm3 as one of the determinants of
safe hospital discharge for patients with newly diagnosed precursor
B-cell ALL. Therefore, those children with an ANC �200/mm3
should be monitored closely as an inpatient or outpatient, due to the
increased risk of infection.
ACKNOWLEDGMENT
We would like to thank Dr. George Buchanan and Dr. Charles
Quinn for their contributions to this project. This publication
was supported by Grant number KL2RR024983, titled, ‘‘North and
Central Texas Clinical and Translational Science Initiative’’ (Milton
Packer, M.D., PI) from the National Center for Research Resources
(NCRR), a component of the National Institutes of Health (NIH), and
NIH Roadmap for Medical Research, and its contents are solely
the responsibility of the authors and do not necessarily represent
the official views of the NCRR or NIH. Information on NCRR is
available at http://www.ncrr.nih.gov/. Information on Re-engineering
the Clinical Research Enterprise can be obtained from http://
nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.
REFERENCES
1. Pui CH, Evans WE. Acute lymphoblastic leukemia. N Engl J Med
1998;339:605–615.
2. Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia.
N Engl J Med 2006;354:166–178.
3. Jagarlamudi R, Kumar L, Kochupillai V, et al. Infections in acute
leukemia: An analysis of 240 febrile episodes. Med Oncol 2000;17:
111–116.
4. Rubnitz J, Lensing S, Zhou Y, et al. Death during induction therapy
and first remission of acute leukemia in childhood. Cancer 2004;
101:1677–1684.
5. Meir M, Balawi I, Meer H, et al. Fever and granulocytopenia in
children with acute lymphoblastic leukemia under induction
therapy. Saudi Med J 2001;22:423–427.
6. Mullen CA, Buchanan GR. Early hospital discharge of children
with cancer treated for fever and neutropenia: Identification and
management of the low-risk patient. J Clin Oncol 1990;8:1998–
2004.
7. Hodgson-Viden H, Grundy P, Robinson J. Early discontinuation of
intravenous antimicrobial therapy in pediatric oncology patients
with febrile neutropenia. BMC Pediatr 2005;5:10.
8. Lucas KG, Brown AE, Armstrong D, et al. The identification of
febrile, neutropenic children with neoplastic disease at low risk for
bacteremia and complications of sepsis. Cancer 1996;77:791–
798.
9. Bodey GP, Buckley M, Sathe YS, et al. Quantitative relationships
between circulating leukocytes and infection in patients with acute
leukemia. Ann Intern Med 1966;64:328–340.
10. Buchanan GR. Approach to treatment of the febrile cancer patient
with low-risk neutropenia. Hematol Oncol Clinic North Am 1993;
7:919–935.
11. Smith M, Arthur D, Camitta B, et al. Uniform approach to risk
classification and treatment assignment for children with acute
lymphoblastic leukemia. J Clin Oncol 1996;14:18–24.
12. Peng LH, Keng TC, Sinniah D, et al. Fever in children with acute
lymphoblastic leukemia. Cancer 1981;47:583–587.
13. Wolk JA, Stuart MJ, Stockman JA, et al. Neutropenia, fever, and
infection in children with acute lymphoblastic leukemia. Am J Dis
Child 1977;131:157–158.
14. Jones GR, Konsler GK, Dunaway RP, et al. Risk factors for recurrent
fever after the discontinuation of empiric antibiotic therapy for
fever and neutropenia in pediatric patients with a malignancy or
hematologic condition. J Pediatr 1994;124:703–708.
15. Pizzo PA, Ladisch S, Robichaud K. Treatment of Gram-positive
septicemia in cancer patients. Cancer 1980;45:206–207.
16. Pizzo PA. Management of fever in patients with cancer and treatment-
induced neutropenia. N Engl J Med 1993;328:1323–1332.
17. Hurwitz CA, Silverman LB, Schorin MA, et al. Substituting
dexamethasone for prednisone complicates remission induction
in children with acute lymphoblastic leukemia. Cancer 2000;88:
1964–1969.
Pediatr Blood Cancer DOI 10.1002/pbc
Readmission Factors for Acute Lymphoblastic Leukemia 379