Embed Size (px)
Citation preview

Acute Lymphoblastic LeukemiaAcute Lymphoblastic Leukemia
Minimal Residual Disease as a
Surrogate Response Endpoint
ASH/FDA WorkshopWashington DC
June 25, 2005

COG ALL Risk GroupsB-Precursor ALL
COG ALL Risk GroupsB-Precursor ALL
• NCI Risk Groups• CNS Disease• Trisomies 4, 10, & 17• TEL/AML 1• MLL• BCR-ABL• Chromosomes <44• Rapidity of Response• MRD - End of Induction
Low Risk
Standard Risk
High Risk
Very High Risk

Early ResponseEarly Response
• Takes into account host and tumor variables that influence sensitivity and resistance• Prednisone “prephase” (BFM)• Fall in peripheral blasts after one week of
multiagent induction (St. Jude)• Day 7 blast content in bone marrow (CCG)

Historical Control(HC) CCG-1800s/1922 series vs.Current CCG-1950/60s(1956s) series
EFS Outcome by Day 7 Marrow(Remission at End of Induction)
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12 14
M1 HC (n=2026)
M2 HC (n=913)
M3 HC (n=969)
M1 1956s (n=1904)
M2 1956s (n=1119)
M3 1956s (n=1089)5 Year EFS:
HC Current
M1 80.4% 82.6%
M2 74.0% 74.6%
M3 67.9% 69.0%
Pro
bab
ility
Years Followed

0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 1 2 3 4 5 6 7 8 9 10 11 12
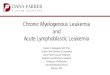
CCG-1882: Augmented Therapy Improves EFS for Patients with an SER (M3 Marrow at day 7)
Pro
bab
ility
Years Followed (from Randomization)
8-Year EFS RHR
BFM 52.3%(s.d. 6.5%) 1.9
Augmented BFM 70.2%(s.d. 6.7%) Baseline
Augmented BFM (n=155)
BFM (n=156)
Log Rank p=.0006
Nachman et al., NEJM 338: 1663-1671, 1998
DATA UPDATED DEC 2004

Assessment of Early Response: Integration of MRD into Clinical Trials
Assessment of Early Response: Integration of MRD into Clinical Trials
• Morphologic assessment is a crude, but accurate and reproducible way to identify patients likely to have good or bad outcomes
• PCR or flow cytometric assessment of MRD• More sensitive and could be more accurate way to
identify groups for risk-adapted therapy• Results will vary based on:
• MRD timepoint analyzed• Therapy prior to MRD analysis• Sensitivity of MRD assay utilized

Major Techniques Used to Assess MRD in Leukemia
Major Techniques Used to Assess MRD in Leukemia
• Flow cytometry detection of leukemia associated phenotypes• Applicable in almost all cases• Fast, relatively inexpensive• Less sensitive than molecular methods
• Probably sensitive enough for identification of HR patients
• PCR amplification of antigen receptor loci (Ig or TCR)• Applicable to ~80% of cases• Laborious and expensive (10 x flow), but very sensitive
• Better for identification of LR patients??• PCR amplification of fusion transcripts only suitable for
defined molecular subgroups such as Ph+ ALL (40%)

Prognostic Significance of End Induction MRD: BFM-Austria
Prognostic Significance of End Induction MRD: BFM-Austria
• Many pilot studies show that MRD levels early in therapy are predictive of outcome
.01%-.1%<.01%
>0.1%
Dworzak et al. Blood 99: 1952, 2002
N=17

Early ResponseEarly Response• All studies show correlation between MRD and
outcome
End Induction MRD
Percent of Patients
EFS
(3 year)
No MRD 42% to 75% > 90%
< 10-3 20% to 42%
> 10-2 5% to 16% 26% to 28%

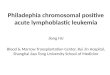
AEIOP ALL 2000/ALL-BFM 2000: Risk Stratification
AEIOP ALL 2000/ALL-BFM 2000: Risk Stratification
• Standard risk group (SR)• Prednisone good response + M1 day 33 AND• Negative MRD (<10-4) at day 33 and week 12 AND• No t(9;22) or t(4;11)
• Medium risk group (MR)• Prednisone good response + M1 day 33 AND• No t(9;22) or t(4;11) AND• Not SR or HR on MRD criteria
• High risk group (HR)• Prednisone poor response or not M1 day 33 OR• t(9;22) or t(4;11) OR• MRD >10-3 at week 12

MRD-SR .97, SE=.03 (N= 39, 1 event)MRD-MR .77, SE=.05 (N=160, 23 events)MRD-HR .38, SE=.06 (N=114, 57 events)
years
p: 1-2 .05 1-3 .0001 2-3 .0001
dsm
c040
5.ta
b 1
3AP
R05
P
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5
AIEOP + ALL-BFM 2000, EFS (4 years)
Risk Group HR 95 by MRD Risk Groups
Pts enrolledSep/Jul 00–Oct 04(Status April 05)
Data courtesy of Valentino Conter and Martin Schrappe

Reducing Disease Burden Pre-Transplant Improves OutcomesReducing Disease Burden Pre-Transplant Improves Outcomes
Uzunel et al. Blood 2001

TumorTumor
Dx
d29
POG ALinC17 to Date:> 2,000 samples
received95% compliance
MRD Sensitivity 1/1000 - 1/10,00024 hr turn around
28.6% of patients positive; Median .069%
Residual Disease Monitoring at End Induction: Flow Cytometry
Residual Disease Monitoring at End Induction: Flow Cytometry

0
20
40
60
80
100
120
140
160
180
End Induction Marrow 534/1937 (28%) of Cases Positive Overall
End Induction Marrow 534/1937 (28%) of Cases Positive Overall
No. ofcases +
<.01 .01-.1 .1-1.0 1.0-10 >10
Percent Leukemic CellsMichael Borowitz

Day 29 Flow MRD Correlates with NCI Risk Group
Day 29 Flow MRD Correlates with NCI Risk Group
0
5
10
15
20
25
30
>.01% >0.1%
std risk n=1046high risk n=546
% MRD +
MRD level
Median .043% LRMedian .14% HR
Michael Borowitz

Day 29 Flow MRD Correlates with Day 8 Morphologic Assessment of ResponseDay 29 Flow MRD Correlates with Day 8 Morphologic Assessment of Response
0
10
20
30
40
50
>0.01% >0.1%
<5%5-24%>25%
Day 8 MarrowBlasts
%MRD +(n=1879)
MRD level
p<.001
Michael Borowitz

Prognostic Significance of MRD - 9906Prognostic Significance of MRD - 9906
EVENT-FREE SURVIVAL
0
20
40
60
80
100
0 1 2 3 4 5
Years
Pro
bab
ility
(%
)
MRD>.01% MRD Negative
p-value=0.00304
n=79
n=156

0
20
40
60
80
100
0 1 2 3 4 5
Years
Pro
babi
lity
(%)
Negative
0.01-0.1
0.1-1.0
> 1.0 p-
Minimal Residual Disease 9906Minimal Residual Disease 9906
169
2133
24p=.0054

Challenges of Marrow RelapseChallenges of Marrow Relapse
• Despite the success in treating newly diagnosed ALL, outcomes following marrow relapse remain poor• Many relapses occur in favorable risk patients• It is difficult to predict response to retrieval
therapy• Attempts to further intensify therapy have
generally not led to improvements in outcome

Obstacles to Successful Treatment for Relapsed ALL
Obstacles to Successful Treatment for Relapsed ALL
• Remission re-induction failures
• Early second relapse
• Regimen-related toxicity

Remission Re-induction RatesRemission Re-induction Rates
Remission induction/re-induction rates
Newly diagnosed ALL
> 98%
Late marrow relapse
> 90%
Early marrow relapse
~ 75%

Obstacles to Successful Treatment for Relapsed ALL
Obstacles to Successful Treatment for Relapsed ALL
• Depth of second CR is shallow• 30-40% of patients who achieve a second
remission develop an early subsequent recurrence
• Significant regimen-related toxicity • Toxic death rates of 3-8% on average• Further intensification likely to be of limited
value

Higher Risk Relapse: Common Therapeutic Approaches
Higher Risk Relapse: Common Therapeutic Approaches
Early Marrow/T-cell Late Marrow/Early EM
Chemotherapy Alt Donor SCT
Matched Related Donor Transplant
Block 1 Block 2 Block 3
Early Marrow Late Marrow Early CNS Early Testicular
Common Re-induction

Introduction of New Agents in Patients with Very High Risk of Treatment FailureIntroduction of New Agents in Patients with Very High Risk of Treatment Failure
Re-induction
Block 1
Re-induction
Block 2
Reduction Phase
VCR, Pred, PEG, Adr
Re-induction
Block 3
ARA-C, ASPCTX, VP-16, MTX
VCR, Pred, PEG, Adr
ARA-C, ASPCTX, VP-16, MTX
MR
D
Time
MRD
MRDEpratuzumab
Pilot I
New Agent Pilot
Correlate with 4 month EFS

BLOCK 1 BLOCK 2 BLOCK 3
VCR days 1,8,15,22 CTX days 1-5 ARA-C days 1,2,8,9PRED days 1-29 VP-16 days 1-5 L-ASP days 2,9PEG days 2,8,15,22 IT MTX (ITT) days 1,22 DOXO day 1 *HD MTX day 22IT ARA-C day 1 (*count dependent)IT MTX days 15 ,29 (CNS -) ITT days 8,15,22,29 (CNS +)
* Imatinib is also given in combination with chemotherapy for Ph+ relapse
COG: AALL01P2COG: AALL01P2

AALL01P2 Study Design
Continuation Therapy
MRD
ARM A
MRD
MRD
Block 2
MRD
MRD
ARM B
Block 2
MRD
Block 1Block 1
Block 3
Block 3
On Study
Randomization
CNS + patients non-randomly assigned to ARM B
DNA Arrays DNA Arrays

MRD Detection During Treatment of Relapse: AALL01P2
MRD Detection During Treatment of Relapse: AALL01P2
Time
Point
MRD+ Median MRD level
1 66/101(65%) 0.73%
2 31/63 (49%) 0.19%
3 16/46 (35%) 0.34%
Slide courtesy of Mike Borowitz, MD, PhD

Correlation of MRD with Time of First Relapse: AALL01P2
Correlation of MRD with Time of First Relapse: AALL01P2
Time
Point
MRD+
Early Relapse
MRD+
Late
Relapse
p value
131/41 (76%)
14/29 (48%)
.018
218/22 (82%)
9/21
(43%).009
39/15
(60%)
3/19
(16%).01
Borowitz, et al. ASH 2004

Kinetics of MRD Response:Good Responders (34/46)Kinetics of MRD Response:Good Responders (34/46)
0.001
0.01
0.1
1
10
100
1 2 3
Time point
% M
RD
(n=15)
(n=8)
(n=11)

Epratuzumab: Mechanism of ActionEpratuzumab: Mechanism of Action
• Highly selective for CD22 positive B-precursor and B-Cells
• Alters lymphocyte adhesion & homing
• Reacts across B-cell lymphoma subtypes
• Minimal activity with normal non-lymphoid tissues
• Mechanisms of action:• Antibody-dependent cellular cytotoxicity• Complement-mediated lysis
6C-C
7C-C
2C-C
5C-C
3C-C
1C-C
4C-C
Leonard and LinkSeminars in Oncol 2002
CD22Epratuzumab
Carnahan et alClin CA Res 2003
Human IgG1
Murine CDRs

New Agent Initiatives: EpratuzumabADVL04P2 (Early Relapse)
New Agent Initiatives: EpratuzumabADVL04P2 (Early Relapse)
Block 1 Block 2 Block 3
MRD
Triple Induction
Phase 2
Block 1 Block 2 Block 3
Triple InductionReduction Phase
6 dose levels
Response
Phase 1
E-mab

MRD – Surrogate EndpointMRD – Surrogate Endpoint
• MRD Endpoints• MRD + vs. MRD-
• End Induction• Pre – BMT (after block 3)
• Median MRD Value• Slope of MRD Reduction
• R1, R2, R3

ConclusionsConclusions
• MRD is a Powerful Predictor of Outcome • MRD Measurements Can be Integrated into
Multi-institutional Trials• MRD Can Be Used To Track Response to New
Agents in the Context of Multiagent Re-induction• Data Indicates That MRD can Be Used as an
Endpoint to Assess Efficacy• Prioritize New Agents for Conventional Trials• Gain Accelerated Approval

Steve HungerNaomi Winick
Elizabeth RaetzMichael Borowitz
AcknowledgementsAcknowledgements