Embed Size (px)
Citation preview
Drug-Resistant Tuberculosis
Richard Kohler, MDTB Consultant, Indiana State Department of Health
Division of Infectious DiseasesIndiana University School of Medicine

Drug-Resistant Tuberculosis: Overview
Definitions Epidemiology Diagnosis Treatment Prevention

Definitions
• Drug-resistant TB: Resistance to isoniazid (INH) or rifampin (RIF)
or pyrazinamide (PZA) or ethambutol (ETH)• Multidrug-resistant (MDR) TB:
Resistance to INH and RIF (and possibly others)
• Extensively drug-resistant (XDR)TB: Resistance to INH, RIF, fluoroquinolones, and
amikacin/kanamycin and/or capreomycin

TB Drug Resistance: Epidemiology
Indiana United States World

TB Drug Resistance: Indiana
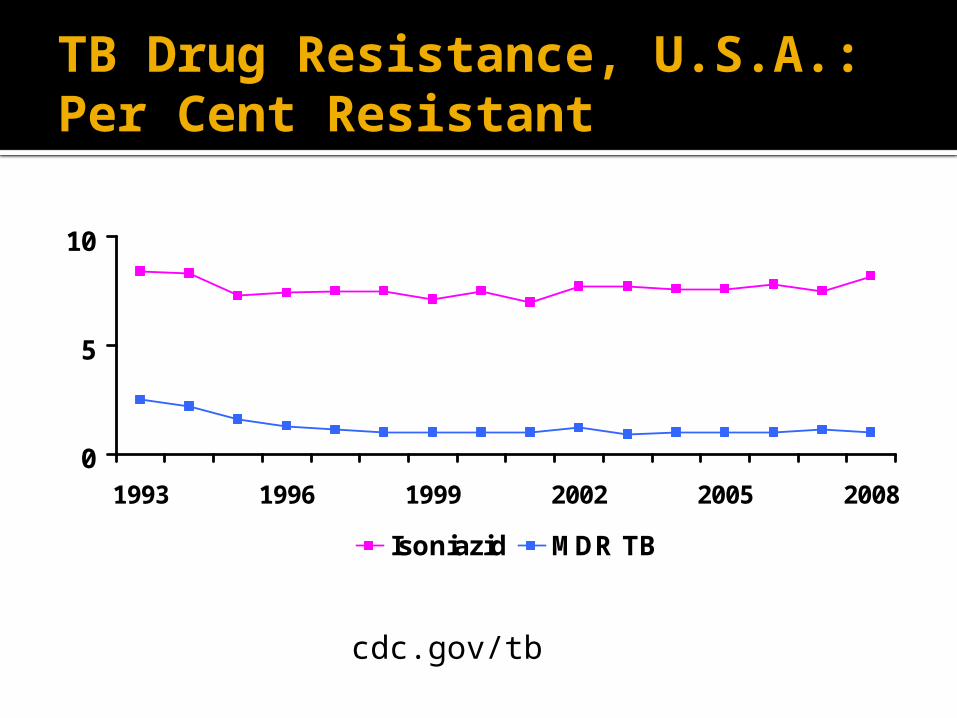
TB Drug Resistance, U.S.A.: Per Cent Resistant
0
5
10
1993 1996 1999 2002 2005 2008
Isoniazid MDR TB
cdc.gov/tb

Primary MDR TBUnited States, 1993–2008*
0
100
200
300
400
500
1993 1996 1999 2002 2005 2008
0
1
2
3
No. of Cases Percentage
*Updated as of May 20, 2009.Note: Based on initial isolates from persons with no prior history of TB. MDR TB defined as resistance to at least isoniazid and rifampin.

Drug-Resistant TB: Indiana, U.S.A.
Primary multi-drug-resistant TB is not often seen in Indiana and occurs in roughly 1/200 cases in the U.S.A.

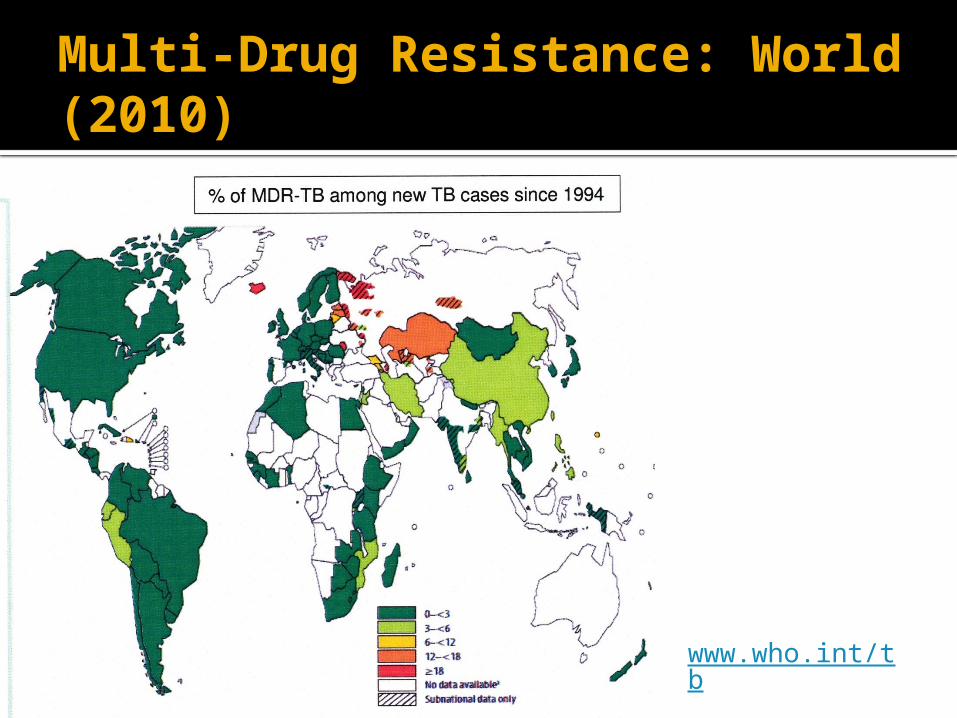
WHO estimates 440,000 MDR-TB cases emerge every year, with more than 110,000 deaths (2008).
www.who.int/tb
Primary MDR TB: Worldwide
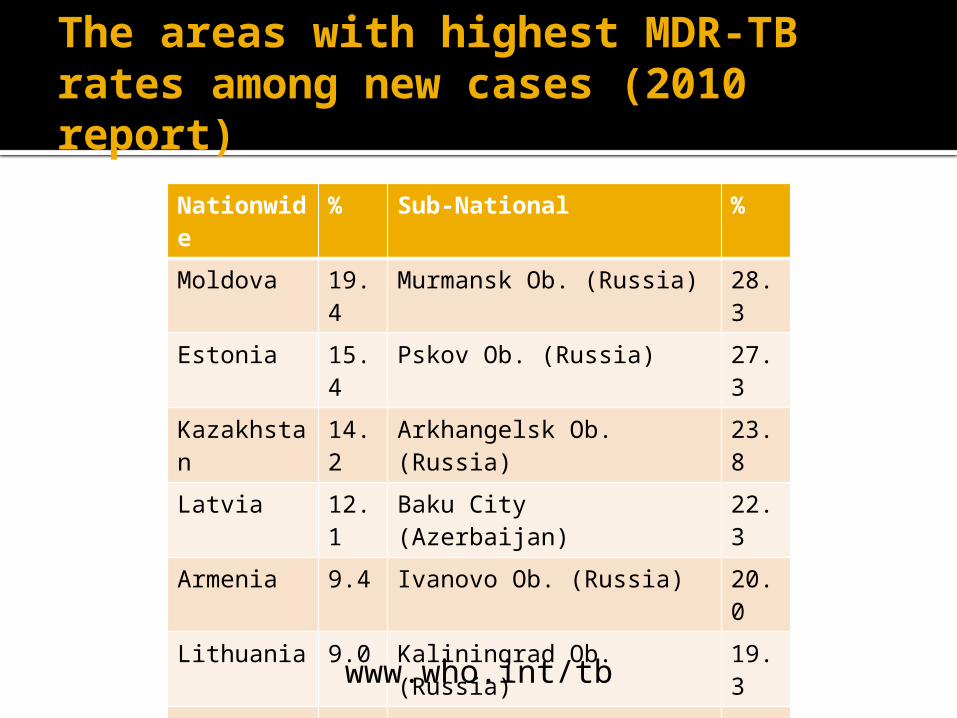
The areas with highest MDR-TB rates among new cases (2010 report)
Nationwide % Sub-National %
Moldova 19.4 Murmansk Ob. (Russia) 28.3
Estonia 15.4 Pskov Ob. (Russia) 27.3
Kazakhstan 14.2 Arkhangelsk Ob. (Russia) 23.8
Latvia 12.1 Baku City (Azerbaijan) 22.3
Armenia 9.4 Ivanovo Ob. (Russia) 20.0
Lithuania 9.0 Kaliningrad Ob. (Russia) 19.3
Georgia 6.8 Belgorod Ob. (Russia) 19.2
China 5.7 Dushanbe/Rudaki (Tajikistan) 16.5
Jordan 5.4 Mary El Republic (Russia) 16.1
Peru 5.3 Donetsk Ob. (Russia) 16.0
www.who.int/tb
Worldwide TB Drug Resistance(2010 Report) MDR-TB Survey Findings:
MDR-TB, on average, in 3.6% of all TB cases Highest ever incidence in parts of northwest Russia
(Murmansk, Archangelsk, Pskov) (24-28%) 50% of all cases in China and India Downward trends Estonia and Latvia Sustained declines in Hong Kong and USA, stable low
levels in western Europe Only 22 or 46 countries in Africa have data. Estimated only 7% of patients identified and notified.
www.who.int/tb

Drug Resistant TB Epidemiology: Summary
MDR and XDR TB are not common in Indiana, the USA, western Europe, or Japan.
MDR TB accounts for a high percentage of TB in countries that were formerly a part of the USSR.
Half the world’s cases exist in China and India. MDR TB incidence/prevalence is unknown for
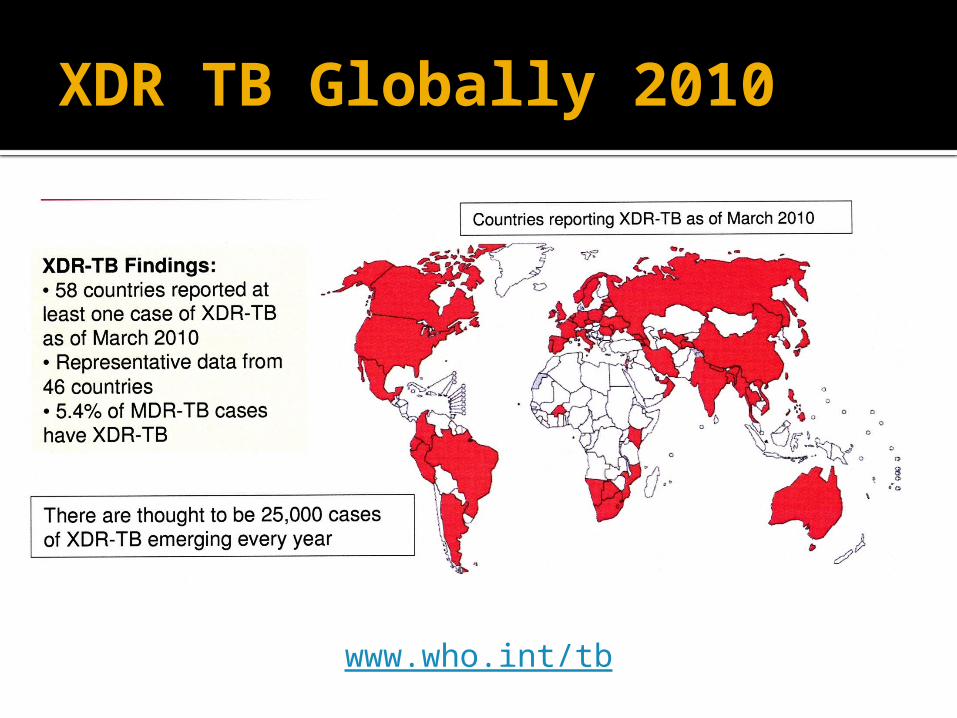
much of Africa. XDR TB exists in at least 58 countries and
accounts for about 5% of cases of MDR TB.

Drug-Resistant TB: Origins
Where does drug resistant TB come from?
Drug-Resistant TB: Perspective
Number of mycobacteria in a pulmonary cavity: 1,000,000,000 (109)
Frequency of mutants that are resistant to any single drug: ~ 1 in 1,000,000. (106)
Number of bacilli in cavity already resistant to each drug: ~ 1,000.
Most (all?) patients with pulmonary TB have organisms in their bodies resistant to all single TB drugs at the outset of therapy.

Drug-Resistant TB: Origins
Mono-resistant organisms are there from the start.
Inadequate multi-drug therapy can select out the mono-resistant organisms.
Mono-resistant organisms, particularly if transmitted to a new human, can then grow up to achieve large numbers, with new mutants now resistant to both the original drug and with additional mutations to other drugs. If that person is inadequately treated …

Diagnosing Drug-Resistant TB
Suspect it based on epidemiologic grounds or on clinical course.
Ultimately requires laboratory confirmation

Risk Factors for MDR-TB
History of prior treatment for TB Especially if poor compliance (psychosocial
barriers, addictions, side effects), no DOT. Drug selection errors (including erroneously
treating active TB with treatment for latent TB) Contact with patients with MDR-TB. Patients who fail to convert sputum cultures
by 4 months

Recognition of MDR TB: Lab Identification
Traditional drug susceptibility testing. Liquid medium: takes 4-5 weeks Solid medium: takes 6-8 weeks
Detection of gene mutations that confer drug resistance Nucleic acid amplification tests (PCR:
polymerase chain reaction + hybridation)▪ Hours to run

Because of the low prevalence of MDR TB in the USA and the standard use of RIPE therapy for the initiation phase, reliance on slow susceptibility testing methods is acceptable.
In a high MDR prevalence setting, standard susceptibility test methods are too slow.
Recognition of MDR TB: Lab Identification in USA

Molecular/Genetic Detection of Drug-Resistant TB ~95% of rifampin-resistant TB strains carry
mutations along an 81 base pair region of a particular TB gene (rpoB)
~85% of INH-resistance is readily detected by genetic testing.
Because most rifampin-resistant isolates in many locales (including US) are also INH-resistant, rapid genetic testing for rifampin resistance should identify mostly MDR strains.
http://www.cdc.gov/tb/topic/laboratory/rapidmoleculartesting/MolDSTreport.pdf “Report of Expert Consultations on Rapid Molecular Testing to Detect Drug-Resistant Tuberculosis in the United States”

Rifampin-R Gene Detection for Rapid Diagnosis of TB and of Rif Resistance
Boehme CC et al.; NEJM 2010;363:1005-1015

Rapid Genetic Test for Rifampin Resistance
CATEGORY MTB/RIF (+) MTB/RIF (-)
All culture positive 2821/2955 (95.5%) (92.7 – 97.8%)*
Culture (+)/Smear (+) 2244/2262 (99.2%)(98.2 – 99.8%)*
Culture (+)/Smear (-) 577/693 (83.2%)(72.5 – 90.2%)*
Culture (-)/Clinical (+) 31/105 (29.3%)
No TB (Culture/Smear/Clinical) 2423/2457 (98.6%)(98.1 – 99.2%)*
Rifampin Resistant 209/211 (99.1%)
Rifampin Susceptible 506/506 (100%)
MDR 195/200 (97.5%)
* Depending on whether test done once on unprocessed specimen or thrice (two processed, one unprocessed) specimens
Boehme CC et al.; NEJM 2010;363:1005-1015
MDR-TB Diagnosis: Current Status
Very rapid combined diagnosis of TB and confirmation of rifampin susceptibilty is technologically possible.
Technology remains too expensive for most areas of the world in which it is needed. Machine purchase cost. Maintenance
▪ Otherwise less costly than standard drug susceptibility testing.

Drug-Resistant TB: Treatment
Mono Resistant MDR XDR

Drug-Resistant TB: Treatment
INH monoresistance RPE for 6-9 months, or 4 months after sputum
conversion. 95% success in 107 patients in 1987 trial (Hong
Kong) Rifampin monoresistance
IPS for 9 months. IPE for at least 12 months. Some recommend 18
months after sputum conversion Role of supplemental quinolone unclear
Schluger, N.; UpToDate 2010 (last update 5/3/10)

MDR Tuberculosis: Treatment
Fluoroquinolone + PZA + ethambutol + injectable agent + additional drug. Treat 18-24 months.
Fluoroquinolone + (PZA or ethambutol) + injectable agent + two additional drugs. Treat 24 months.
Additional drugs: Pick from: Ethionamide, cycloserine, PAS, linezolid Clarithromycin, amoxicillin-clavulanate
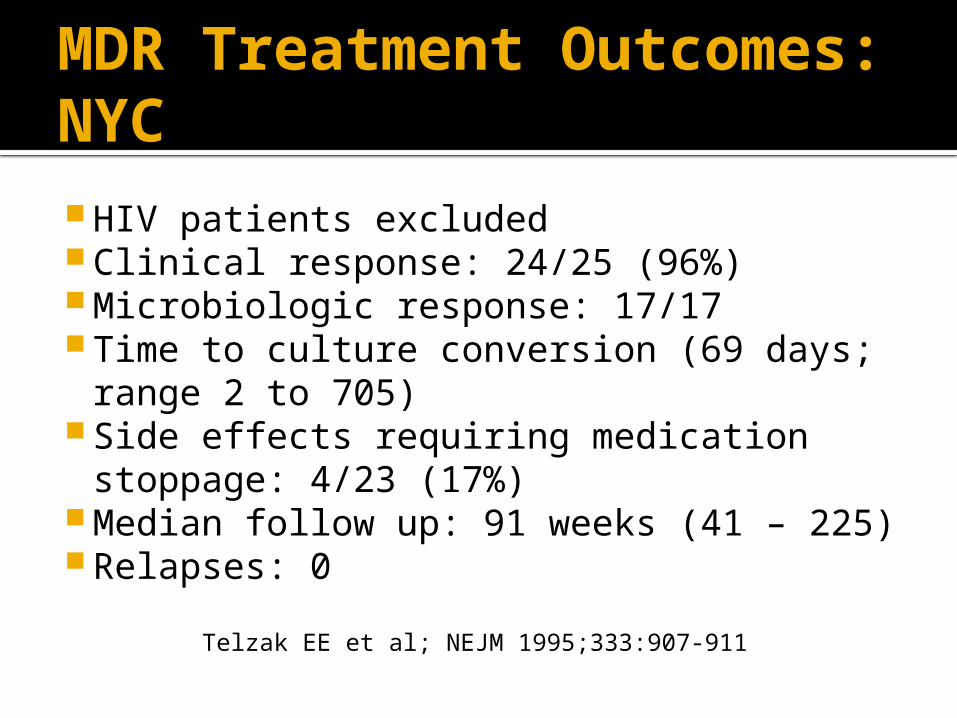
HIV patients excluded Clinical response: 24/25 (96%) Microbiologic response: 17/17 Time to culture conversion (69 days; range 2 to
705) Side effects requiring medication stoppage:
4/23 (17%) Median follow up: 91 weeks (41 – 225) Relapses: 0
MDR Treatment Outcomes: NYC
Telzak EE et al; NEJM 1995;333:907-911
MDR Treatment Strategy: NYC
Use at least three effective drugs. All patients (25) were treated with a fluoroquinolone.
Other drugs used: ethionamide (13), PZA (12), aminoglycoside (11), cycloserine (11), capreomycin (8), PAS (4), clofazimine (2).
Mean duration of oral drugs: 568 days. Mean duration of injectable drugs: 252 days. Surgery used for 3/25.
Telzak EE et al; NEJM 1995;333:907-911
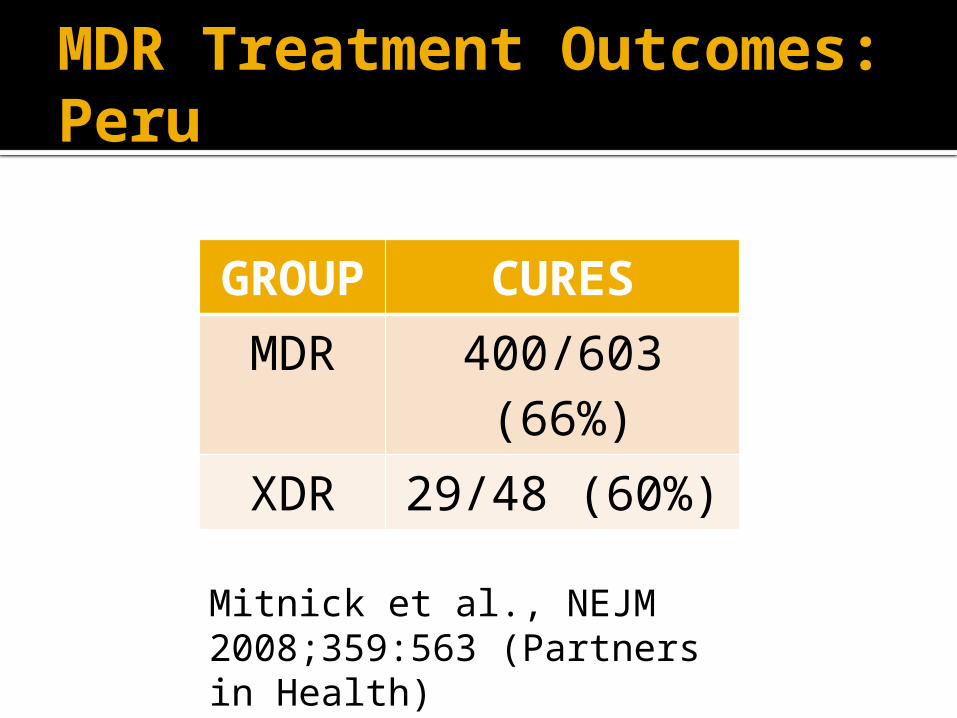
MDR Treatment Outcomes: Peru
GROUP CURESMDR 400/603 (66%)XDR 29/48 (60%)
Mitnick et al., NEJM 2008;359:563 (Partners in Health)

MDR/XDR Treatment Strategy: Peru
Cases mostly recognized as standard regimen failures.
Drug susceptibility testing at or near MDR/XDR regimen initiation.
Five effective drugs (Susceptible, or not used within 30 days, including FQ + injectable)*
18+ months rx (at least 8 for injectable) Supervised daily therapy Adverse event management algorithms
If five effective drugs not possible: Treat longer than 18 months (and longer than 8
months for injectables. Add other drugs▪ Previously susceptible but clinically failed drugs.▪ Clarithromycin, amoxicillin-clavulanate, clofazimine,
rifabutin. Surgery
MDR/XDR Treatment Strategy: Peru (2)

XDR, Peru: Treatment Regimens
Number of drugs: XDR 5.3 + 1.3 Frequency of drug use in regimens:
Cycloserine: 100% Amoxicillin-clavulanate: 100% Clofazimine: 98% PAS: 96% Moxifloxacin: 72% Ethionamide: 66% Capreomycin: 53% Clarithromycin: 45%

MDR Treatment: Summary (USA)
18-24 months of treatment. Four drugs that are active. If possible use aminoglycoside (at least 6
months) + fluoroquinolone (e.g., moxifloxacin) - ~85% cure rates.
Plus two other drugs DOT

TB drug in development. Works very well in animal models. Studied in randomized control comparison
with placebo. All patients had MDR-TB. All patients treated with additional five
drugs, typically ofloxacin + injectable + ethionamide + PZA + cycloserine or terizodone
MDR TB: Diarylquinolone TMC207

MDR TB: Diarylquinolone TMC207
Impact on Sputum Cultures
and Time to Conversion
Diacon AH et al.; NEJM 2009;360:2397-2405
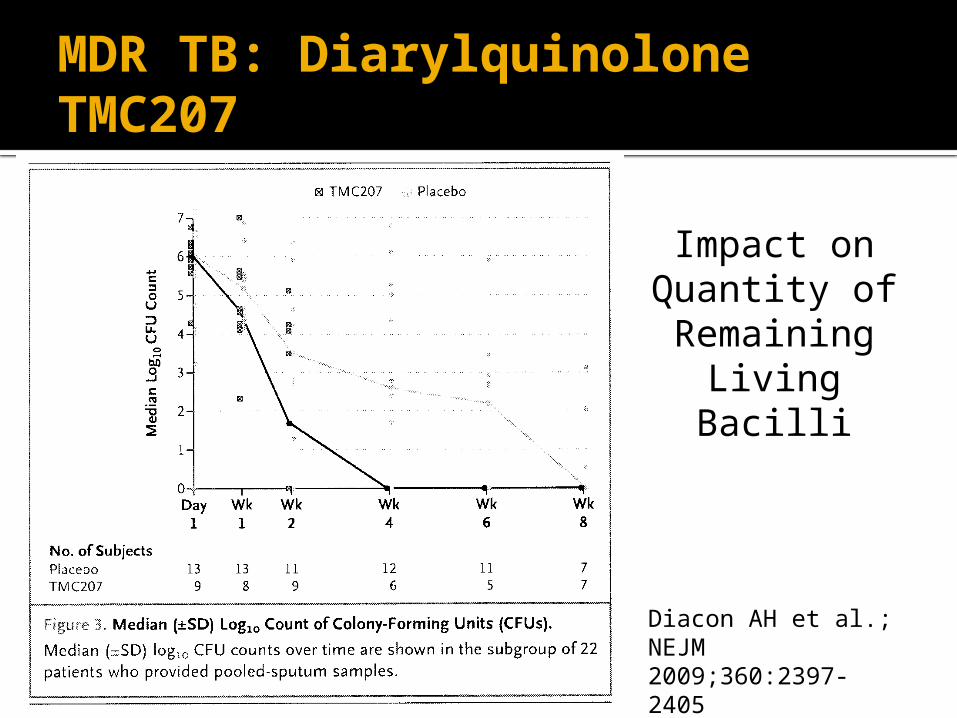
MDR TB: Diarylquinolone TMC207
Impact on Quantity of
Remaining Living Bacilli
Diacon AH et al.; NEJM 2009;360:2397-2405
Prevention: Treatment of Latent MDR TB
Optimal approach unknown. Expert opinion:
Select two drugs to which the index case isolate is known.▪ E.g., pyrazinamide + [ethambutol or fluoroquinolone]
Duration: 6-12 months
Horsburgh, CR. UpToDate (last update 5/20/10

Drug Resistant TB: Summary
Big problem worldwide. Not yet in USA. We remain vulnerable.
Technology for rapid detection of MDR-TB needed in high prevalence areas. Seems to be available. Not affordable most places that need it.
Treatment not as successful for MDR/XDR cases but still 60% or better. Expensive. Difficult.


MDR Worldwide 1994-2009
Nathanson et al.; NEJM 2010;363:1050-1058
WHO 2008 Report: Conclusions
Highest rates ever recorded of MDR-TB. Severely limited laboratory capacity has meant
limited data availability in Africa (only 22 of 46 countries have data).
Insufficient efforts in many areas of the world to treat and control MDR-TB
Equipment to rapidly diagnose MDR-TB in 1 week instead of 3 months exists but most patients cannot access such services
Extraordinary measures are needed in Eastern Europe: rapid detection, effective care, access to drugs

Patients in Whom to Suspect MDR TB
Recurrence after prior treatment, especially if DOT was not used.
Failure to convert sputum culture. Known contact with MDR patient.