Embed Size (px)
Citation preview

Review ArticleUpdate on the Clinical Effect of AcupunctureTherapy in Patients with Gouty Arthritis: SystematicReview and Meta-Analysis
Wei-wei Lu, Jin-ming Zhang, Zheng-tao Lv, and An-min Chen
Department of Orthopedics, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology,Wuhan, Hubei 430030, China
Correspondence should be addressed to An-min Chen; [email protected]
Received 17 May 2016; Revised 1 August 2016; Accepted 24 August 2016
Academic Editor: Deborah A. Kennedy
Copyright © 2016 Wei-wei Lu et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objective. The aim of this study is to evaluate the clinical efficacy and safety of acupuncture therapy in the treatment of acutegouty arthritis. Methods. A literature search of PubMed, EMBASE, ISI Web of Science, CENTRAL, and CNKI was conductedfrom the inception date of each database up to October 2015. Two investigators screened each article independently and wereblinded to the findings of the other reviewer. Data was extracted according to the predetermined collection form. Meta-analysiswas performed. Results. We analyzed data from 28 RCTs involving 2237 patients with gouty arthritis. Compared with conventionalpharmacological treatments acupuncture was more effective in rendering patients free from symptoms after 24 hours, loweringserum urate, alleviating pain associated with gouty arthritis, and decreasing the ESR; regarding CRP, no statistically significantdifference was found. In addition, the frequency of adverse events in acupuncture treatment was lower than that in controlgroup. Conclusion. Based on the findings of our study, we cautiously suggest that acupuncture is an effective and safe therapy forpatients with gouty arthritis. However, the potential beneficial effect of acupuncturemight be overstated due to the methodologicaldeficiency of included studies. High quality RCTs with larger scale are encouraged.
1. Introduction
Gouty arthritis is a disorder of purine metabolism and resultsfrom monosodium urate (MSU) crystal deposition in andaround the joints caused by longstanding hyperuricaemia,which is defined as a serum uric acid (sUA) concentrationexceeding the limit of sUA solubility (6.8mg/dL) [1, 2]. Thischronic inflammatory condition ismediated byMSU crystalsand characterized by recurrent attacks of monoarthritisor polyarthritis [3]. Gouty arthritis is the most prevalentinflammatory arthritis in developed countries, especiallyin elder men; and the incidence was reported to increaseover the past 20 years [4]. Quality of life is impairedduring intercritical periods and during flares in addition toassociated comorbidities such as obesity, diabetes mellitus,hypertension, hyperlipidaemia, and chronic renal disease[5–7]. Without proper treatment, acute gouty arthritis canprogress into a chronic, deforming, and physically disabling
disease through the development of tophi, joint destruction,and persistent pain [8, 9].
The American College of Rheumatology (ACR) andEuropean League Against Rheumatism (EULAR) guidelinesfor the pharmacologic management of acute gouty arthri-tis include oral colchicine, nonsteroidal anti-inflammatorydrugs (NSAIDs), and corticosteroids [10, 11]. However, theside effects associated with pharmacological agents restricttheir long-term use. Some authors have pointed out thatmanagement of gouty arthritis is often suboptimal and thatflares are inevitable, necessitating better strategies to handleattacks [12].
Complementary and alternative medicine (CAM) iswidely advocated to face the increasing demand for nonphar-macological approaches. As a mainstream of CAM therapy,acupuncture based on traditional Chinese medicine (TCM)theory has been commonly used for the treatment of goutyarthritis in Chinese cultures. A previous systematic review
Hindawi Publishing CorporationEvidence-Based Complementary and Alternative MedicineVolume 2016, Article ID 9451670, 14 pageshttp://dx.doi.org/10.1155/2016/9451670

2 Evidence-Based Complementary and Alternative Medicine
had reported the clinical effect of acupuncture in relievingpain and decreasing serum uric acid, whereas only tenRCTs were included, the heterogeneity among studies wasnot discussed, and the security of acupuncture therapy wasnot confirmed [13]. Recently, new literatures to evaluatethe efficacy and safety of acupuncture therapy for goutyarthritis are emerging. Therefore, an updated meta-analysisis required.
2. Methods
This systematic review was conducted in accordance with thePreferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [14].
2.1. Search Strategy. A comprehensive literature search ofPubMed, EMBASE, CENTRAL, ISI Web of Science, andCNKI was conducted. All the above databases were searchedfrom their inception dates up to the latest issue (October2015), without language restriction. Medical subject headings(MeSH) and free text words were combined to retrieve allthe potential studies. MeSH were modified based on thespecifications of each database. The following search strategywas used for the literature search in PubMed, CENTRAL,and ISI Web of Science: (“Gout” or Gout or gouts) and(“Acupuncture Therapy” or acupuncture or moxibustionor acupoint or acupressure or acustimulation). For CNKI,search terms were “Zhen” and “Tongfeng”. In addition, thebibliographies of relevant systematic reviews and clinicalguidelines were manually searched. The reference section foreach study was also searched.
2.2. Types of Participants. To be included in our system-atic review, the enrolled subjects had to be diagnosed asgouty arthritis according to ascertained diagnostic criteria:European League Against Rheumatism (EULAR) criteria,the American Rheumatism Association (ARA) preliminaryclassification criteria for acute gout 1977 [15], Mexico 2010[16], Netherland 2010 [17], or the Criteria of Diagnosis andTherapeutic Effect of Diseases and Syndromes in TCM issuedby the State Administration of TCM [18]. No restrictions onrace, age, and sex were imposed.
2.3. Interventions. Patients in experimental groups mainlyreceived acupuncture therapy (including manual acupunc-ture and electroacupuncture), either alone or in combina-tion with pharmacological treatment or TCM treatment,without differentiating different acupuncture techniques,acupoints selection, or needle materials. Patients in con-trol groups were treated with western medicine (includingcolchicine, allopurinol, indomethacin, benzbromarone, cele-coxib, probenecid, meloxicam, and ibuprofen); no specifictypes of drugs were imposed.
2.4. Outcome Measurements. The primary outcome measurewas clinical effect and the frequency of adverse events inboth groups; the secondary outcomemeasurements includedclinical parameters associated with acute gouty arthritis, suchas serum uric acid, pain intensity using visual analogue scale
(VAS), erythrocyte sedimentation rate (ESR), and C-reactiveprotein (CRP).
2.5. Types of Publication. The included studies were requiredto be randomized controlled trials aiming to assess theefficacy of acupuncture therapy for gouty arthritis. Articlesregarding animal experiments, reviews articles, case reports,or expert experience reports were excluded.
2.6. Data Extraction. Two investigators (Wei-wei Lu and Jin-ming Zhang) screened each article independently and wereblinded to the findings of the other reviewer. According to thepredetermined inclusion criteria, two reviewers performedstrict screening to identify qualified articles independently,and they extracted data from these eligible articles usinga standardized data collection form, which included firstauthor, year of the publication, study design, baseline char-acteristics for participants in different groups, diagnosticcriteria of gouty arthritis, interventions and control treat-ment, main outcome assessments, duration of treatments,and adverse events.
Any disagreement between the two reviewers wasresolved through discussion until a consensus was reached.The third review author (Jin-ming Zhang) was consulted if aconsensus could not be reached.
2.7. Quality Assessment. Cochrane Collaboration’s tool wasutilized to assess the risk of bias in the selected RCTs,which was based on seven items: random sequence gen-eration, allocation concealment, blinding of participantsand personnel, blinding of outcome assessment, incompleteoutcome data, selective reporting, and other sources ofbias [19]. Two reviewers assessed the risk of bias amongstudies independently; the results were compared afterwards.Disagreements regarding the risk of bias assessment weresettled by discussion and consensus between reviewers.
2.8. Data Synthesis and Analysis. The enrolled participantswere dichotomized into being cured and not cured to expressthe intervention effect. Odds ratio (OR) and the associated95% confidence intervals (CIs) were calculated for clinicaleffect and frequency of adverse events. The mean difference(MD) for changes from baseline in the continuous variableswas calculated using the same methodology. Random effectmodel was employed for meta-analysis, since the homo-geneity of the included studies could not be guaranteed.The chi-squared test and the Higgins 𝐼2 test were used toassess the heterogeneity among studies (𝑃 > 0.1 and 𝐼2indicate acceptable heterogeneity). Forest plot and funnel plotwere generated via RevMan 5.3 (Copenhagen: the NordicCochrane Centre, the Cochrane Collaboration, 2014).
Metaregression was performed using Stata version 12.0(StataCorp LP, USA) to find the possible source of het-erogeneity, such as acupuncture type, treatment duration,and whether combined with other therapy. Begg’s rankcorrelation test and Egger’s linear regression test were used toevaluate the publication bias if the number of included studieswas greater than ten.

Evidence-Based Complementary and Alternative Medicine 3
3. Results
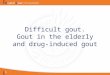
3.1. Literature Search Results. An initial search of RCTsyielded 379 potential literature citations, including 27 fromPubMed, 8 from CENTRAL, 57 from EMBASE, 30 from ISIWeb of Science, 255 from CNKI, and additional two recordsfromother sources. 47 articleswere deleted because theywereduplicates for retrieving. According to the prespecified inclu-sion criteria, 66 potentially relevant studies were selectedand retrieved for a full-text assessment after reading theirtitles and abstracts. Of the remaining 66 studies, two weredeleted because they were non-RCTs, two were duplicatesfor publication, one study did not provide available data,and 33 studies employed uncomfortable intervention. A totalof 28 studies [20–47] were deemed eligible for inclusion inthis review. The literature screening process is presented in aflowchart in Figure 1.
3.2. Study Characteristics. The main characteristics ofincluded studies are summarized in Table 1. The 28 studiesincluded a total of 1174 patients in acupuncture group and1063 patients in control group. Subjects were diagnosed asgouty arthritis according to either the criteria stipulated byUS Rheumatology Association or the criteria stipulated byState Administration of TCM. The age of enrolled subjectsranged from 18 to 80 years. All the studies were conductedby Chinese investigators in a single center and publishedbetween 2002 and 2015. Clinical efficacy of acupuncture wasevaluated by all studies, but only ten of them analyzed thesafety in both groups.
Patients in acupuncture group received manual acupunc-ture or electroacupuncture; the acupoints selection was basedonTCMmeridian theory.The acupuncture was applied aloneor in combination with other treatment, such as Chineseherbal medicine, acupoint injection, and local blocking ther-apy. Acupuncture therapy was administered daily or everytwo days, the needles were retained for 20 to 30 minutes foreach session, and the treatment course ranged from 5 days to28 days. The detailed information is listed in Table 2.
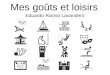
3.3. Quality Assessment. The risk of bias among studies wasassessed using Cochrane Collaboration’s tool. All studiesincluded the suggested randomization, half of the studies[22, 28, 29, 34–38, 41–43, 45–47] reported the methodof random sequence generation, and five studies [24, 27,30, 31, 39] were judged to high risk of bias because thepatients were arranged according to their registration order.No study reported detail about allocation concealment. Theblinding of outcome assessment was judged to unclear riskof bias because no studies mentioned blinding of outcomeassessment. The blinding of participants and personnel wasjudged to high risk of bias as it was impossible to carry outin our included studies. When it comes to incomplete data,only four studies [27, 34, 41, 47] provided the number ofdropouts and reason for withdrawal. All the studies reportedthe prespecified outcomemeasurements. Baseline similaritiesseemed to be achieved by each study: no statistical differenceswere detected in age, gender, or symptom duration. Fivestudies [24, 27, 30, 31, 39] were judged to high risk of bias
while the other 23 were unclear risk of bias. Judgementsabout each risk of bias item for each included study weresummarized in Figures 2 and 3.
3.4. Clinical Effect. All the included studies employed clinicaleffect as outcome assessment; the therapeutic effect wasevaluated in accordance with the Criteria of Diagnosis andTherapeutic Effect of Diseases and Syndromes in TCM issuedby the State Administration of TCM in 1994 [18].The patientswere defined as complete resolution of acute attack when thejoints swelling, pain, and redness disappeared with normallaboratory indices 24 hours after the treatment, improvedwhen symptoms and signs alleviated with laboratory indicesimproved, or failed when the symptoms and laboratoryindices did not have improvement. Thus, the patients inexperimental and control groups were dichotomized as com-plete resolution and not completely resolved; OR and 95%CI in each study were calculated based upon the raw data.The combined effects of 28 individual studies showed thatacupuncture therapy could further improve the clinical curerate compared with western medicine (OR 2.71; 95% CI 2.22,3.32; 𝑃 < 0.00001); the results of heterogeneity test indicatedno obvious heterogeneity (𝑃 = 0.24, 𝐼2 = 15%) (Figure 4).
3.5. Uric Acid. Twenty-two studies [20, 25–39, 41–43, 45–47]measured blood uric acid as outcome; changes from baselinewere calculated. Data extracted from 22 individual studiesshowed that heterogeneity existed (𝑃 < 0.00001, 𝐼2 = 85.1%);random effects model was utilized for statistical analysis.Pooled data suggested that acupuncture therapy could furtherdecrease uric acid than western pharmacological treatment(MD 41.30; 95% CI 24.86, 57.74; 𝑃 < 0.00001) (Figure 5).
3.6. Pain Intensity (VAS Score). Seven studies [29, 33, 34, 41,43, 46, 47] that measured pain intensity using VAS scorewere identified. Data extracted showed obvious heterogeneityin the consistency of study results (𝑃 < 0.00001, 𝐼2 =94%); random effects model was employed. Among theseven studies, six found that acupuncture therapy couldfurther improve the VAS score than pharmacological therapy,whereas Liu et al. reported an opposite result. The com-bination of results showed that acupuncture could furtherimprove pain associated with acute gouty arthritis (MD 1.92;95% CI 0.96, 2.87; 𝑃 < 0.0001) (Figure 6).
3.7. ESR. Five studies [25, 30, 33, 34, 43] reported onESR; only one study found statistically significant differenceregarding the decrease of ESR in acupuncture group andcontrol group. The heterogeneity was acceptable (𝑃 = 0.25,𝐼2= 26%); the pooled data showed that acupuncture therapy
was better than western medicine in decreasing ESR (MD1.75; 95% CI 0.11, 3.38; 𝑃 = 0.04) (Figure 7).
3.8. CRP. Four studies [25, 30, 33, 34] measured CRP asoutcome; statistically significant difference was detected inonly one study. No obvious heterogeneity was found (𝑃 =0.23, 𝐼2 = 30%); the combined data showed no significantdifference in decreasing CRP between acupuncture and

4 Evidence-Based Complementary and Alternative Medicine
PubMed = 27
EMBASE = 57
ISI Web of Science = 30
CENTRAL = 8
Additional records identifiedthrough other sources (n = 2)
Totally identified (n = 379)
Records after the duplicateswere removed (n = 332)
Records excluded(n = 266)
Full-text articles excluded,with reasons (n = 38)
Non-RCT = 2
Duplicates = 2
Unavailable data = 1
Uncomfortableintervention = 33
Full-text articlesassessed for eligibility
(n = 66)
Studies included inqualitative synthesis
(n = 28)
Studies included inquantitative synthesis
(meta-analysis)(n = 28)
CNKI = 255
Duplicates (n = 47)
Figure 1: Flow diagram of the literature selection.

Evidence-Based Complementary and Alternative Medicine 5
Table1:Ch
aracteris
ticso
fRCT
sidentified
intheliteraturesearch.
Stud
yPo
pulatio
n(E/C
)Age
(meanor
range)
Diagn
ostic
criteria
Outcomem
easurements
Adversee
vents
Baiyin
2014
[20]
43/44
E:27–56;C:
28–54
ARA
1977
Clinicaleffect,uricacid
NR
Chenle2015
[21]
25/25
E:25–58;C:
23–6
0ARA
1977
Clinicaleffect
NR
Gon
gandCh
en2014
[22]
60/60
NR
ARA
1977
Clinicaleffect
NR
Gui
andCh
en2014
[23]
32/28
E:28–6
5;C:
26–6
2SA
TCM
1994
Clinicaleffect
Yes
Hee
tal.2008
[24]
30/30
E:28–6
7;C:
30–6
5SA
TCM
1994
Clinicaleffect
Yes
Huetal.2010[25]
68/60
E:45.42±11.46
;C:46.74±11.22
ARA
1977
Clinicaleffect,uricacid,C
RP,E
SRYes
Jinetal.2012[26]
30/30
E:23-67;C:
25–6
6ARA
1977
Clinicaleffect,uricacid
Yes
Lietal.2013[27]
31/29
E:49.67±19.3;C
:46.52±10.29
ARA
1977
Clinicaleffect,uricacid
Yes
Liuetal.200
8[28]
56/44
E:34–70:C:
33–74
SATC
M1994
Clinicaleffect,uricacid
NR
Liuetal.2014[29]
44/41
E:20–50;C:
18–52
ARA
1977
Clinicaleffect,uricacid,V
ASscore
Yes
Liu2014
[30]
87/87
E:44
.1;C:
43.4
ARA
1977
Clinicaleffect,uricacid,C
RP,E
SRYes
Ma2
002[31]
48/30
E:31–78;C:
29–72
ARA
1977
Clinicaleffect,uricacid
NR
Ma2
004[32]
42/30
E:31–78;C:
29–72
ARA
1977
Clinicaleffect,uricacid
NR
Wang2013
[33]
40/20
E:23–70;C:
23–70
ARA
1977
Clinicaleffect,ES
R,CR
P,uricacid
Yes
Wuetal.2012[34]
34/32
E:32–6
0;C:
33–6
3SA
TCM
1994
Clinicaleffect,uricacid,C
RP,E
SR,V
ASscore
NR
Xietal.200
6[35]
66/64
E:50.1±5.2;C:
45.1±6.1
ARA
1977
Clinicaleffect,uricacid,V
ASscore
NR
Xiee
tal.2007
[36]
30/30/30
E:40
–70;C1
:42–69;C
2:43–7
1ARA
1977
Clinicaleffect,uricacid
NR
Xiee
tal.2009
[37]
30/30
E:32–6
5;C:
40–6
7SA
TCM
1994
Clinicaleffect,uricacid
Yes
Yan2009
[38]
40/20
E:35–75;C:
38–76
ARA
1977
Clinicaleffect,uricacid
Yes
Yinetal.200
5[39]
40/30/30
E1:36–
72:E2:31–6
9:C:
34–76
SATC
M1994
Clinicaleffect,uricacid
NR
Zhang2010
[40]
28/29
E:38–79;C:
29–80
SATC
M1994
Clinicaleffect
NR
Zhao
2007
[41]
30/30
E:31–6
8;C:
30–70
SATC
M1994
Clinicaleffect,uricacid,V
ASscore
NR
Zhao
etal.200
9[42]
30/30
E:33–70;C:
32–7
1ARA
1977
Clinicaleffect,uricacid
NR
Zhou
etal.2012[43]
80/80
E:36–6
5;C:
37–6
4SA
TCM
1994
Clinicaleffect,uricacid,V
ASscore,ES
RNR
Zhou
2014
[44]
20/20
E:18–4
8;C:
17–50
SATC
M1994
Clinicaleffect
NR
Zong
etal.2011[45]
20/20
E:34–72;C:
30–70
ARA
1977
Clinicaleffect,uricacid
NR
Zouetal.200
6[46]
30/30/30
E1:32–70;E
2:31–72;C:
35–7
1SA
TCM
1994
Clinicaleffect,uricacid,V
ASscore
NR
Zouetal.200
7[47]
30/30
E:32–70;C:
31–72
SATC
M1994
Clinicaleffect,uricacid,V
ASscore
NR
Note.E:experim
ent;C:
control;N
R:no
treported;CR
P:C-
reactiv
eprotein;ESR
:erythrocytesedimentatio
nrate;TCM
:traditio
nalC
hinesemedicine;VA
S:visualanalogue
scale;ARA
1977:the
American
Rheumatism
Associatio
nprelim
inaryclassifi
catio
ncriteria
fora
cute
gout
1977;SAT
CM1994:the
Criteria
ofDiagn
osisandTh
erapeutic
Effecto
fDise
ases
andSynd
romes
inTradition
alCh
ineseMedicineissuedby
theState
Administratio
nof
Tradition
alCh
ineseM
edicine.

6 Evidence-Based Complementary and Alternative MedicineTa
ble2:Detailsof
interventio
nin
acup
unctureg
roup
sand
controlgroup
s.Stud
yAc
upun
ctureintervention
Con
trol
Duration
Baiyin
2014
[20]
MA(A
ship
oint)2
5min,oncea
day,plus
Chineseh
erbalm
edicine
Colchicine0
.5mgtwicea
day,
allopu
rinol50
mgtwicea
day
15days
Chenle2015
[21]
MA(A
ship
oint,G
b34,Sp10,St35,EX
-LE4
,S34,E
X13)
25min,oncea
day,plus
Chineseh
erbal
medicine
Colchicine0
.5mgtwicea
day,
allopu
rinol50
mgtwicea
day
15days
Gon
gandCh
en2014
[22]
MA(A
ship
oint),everyo
ther
day
Allo
purin
ol50
mg3tim
esad
ay20
days
Gui
andCh
en2014
[23]
MA(A
ship
oint,Sp9,St36,Sp6,Li11,
Gv14),oncea
day,plus
Chineseh
erbalm
edicine
Allo
purin
ol100m
g3tim
esad
ay,
colchicine
0.5m
g/ho
ur10
days
Hee
tal.2008
[24]
EA(A
ship
oint,St36,Sp6,Ki3,Sp4)
20min,oncea
day,plus
acup
oint
injection
Colchicine0
.5mg3tim
esad
ay,
indo
metacin
25mg3tim
esad
ay10
days
Huetal.2010[25]
MA(G
b11,Cv
6,Ki3,B4
0)30
min,oncea
day,plus
Chineseh
erbalm
edicine
Indo
metacin
25mg3tim
esad
ay,
allopu
rinol100m
g3tim
esad
ay21
days
Jinetal.2012[26]
MA(Sp6
,Sp9,L
i11,S34,Sp10,H3,L15),oncea
day,plus
Chineseh
erbalm
edicine
Allo
purin
ol100m
gtwicea
day
7days
Lietal.2013[27]
MA(Sp6
,St36,Sp9,St40
,Sp10,Li11,
Li4,Lr3)
15min,oncea
day,plus
Chineseh
erbalm
edicine
Colchicine0
.5mg3tim
esad
ay21
days
Liuetal.200
8[28]
EA(A
ship
oint,Sp1,L
r3,Sp6
,St40,Sp9,Gb34)
30min,oncea
day,plus
localblockingtherapy
Allo
purin
ol100m
g3tim
esad
ay,
indo
metacin
25mg3tim
esad
ay7days
Liuetal.2014[29]
MA(surroun
dedthed
iseased
region
),on
cead
ay,pluse
xternalC
hinese
herbalmedicine
Colchicine0
.5mgtwicea
day,
celecoxib200m
gtwicea
day
7days
Liu2014
[30]
MA(Sp10,Sp6,St36,St40,Sp9,Li11,
Li4,Lr3)
30min,oncea
day,plus
Chineseh
erbalm
edicine
Benzbrom
aron
e50m
gon
cead
ay14
days
Ma2
002[31]
MA(Sp6
,Ki3,Sp10,Li11)3
0min,oncea
day
Indo
metacin
25mg3tim
esad
ay,
allopu
rinol100m
g2-3tim
esad
ay28
days
Ma2
004[32]
MA(Bl23,Bl22,C
v3,C
v4,Sp10,Sp6,Ki3)
30min,oncea
day
Allo
purin
ol100m
g2-3tim
esad
ay28
days
Wang2013
[33]
MA(A
ship
oint,K
i3,Sp9,B
60,Li11,L
i4,L
r3)2
0min,oncea
day,plus
Chineseh
erbalm
edicine
Colchicine0
.5mg3tim
esad
ay14
days
Wuetal.2012[34]
EA2H
z(St36,St40,Aship
oint)3
0min,oncea
day,plus
bloo
dlettin
gColchicine0
.5mg3tim
esad
ay,
allopu
rinol100m
g3tim
esad
ay6days
Xietal.200
6[35]
MA(A
ship
oint,Sp6
,Sp10,Sp9,Li4,Li11)
30min,oncea
day
Meloxicam
7.5mgon
cead
ay20
days
Xiee
tal.2007
[36]
EA(Sp6
,Sp9,St40)
30min,oncea
day
Allo
purin
ol100m
g3tim
esad
ay,
prob
enecid
250m
g3tim
esad
ay10
days
Xiee
tal.2009
[37]
MA(surroun
dedthed
iseased
region
)30m
in,oncea
day
Allo
purin
ol100m
g3tim
esad
ay,
indo
metacin
25mg3tim
esad
ay15
days
Yan2009
[38]
MA(A
ship
oint,K
i3,Sp6
,St36,B6
0,St40
,Lr3)3
0min,oncea
day,plus
bloo
dlettin
gAllo
purin
ol100m
gtwicea
day
14days
Yinetal.200
5[39]
EA(St36,St40
,Aship
oint)3
0min,oncea
day;EA
plus
weste
rnmedicine
Allo
purin
ol100m
g3tim
esad
ay,
indo
metacin
25mg3tim
esad
ay6days
Zhang2010
[40]
MA30
min,oncea
day,plus
weste
rnmedicine
Indo
metacin
25mg3tim
esad
ay6days
Zhao
2007
[41]
MA(St36,Sp6,Aship
oint),on
cead
ayIndo
metacin
25mg3tim
esad
ay,
allopu
rinol100m
g3tim
esad
ay6days
Zhao
etal.200
9[42]
EA(A
ship
oint,Li4,St36,Gb34,Sp10,B
60,K
i3)3
0min,oncea
day,plus
bloo
dlettin
gProb
enecid
250m
gtwicea
day
10days
Zhou
etal.2012[43]
MA(Sp10,St36,Sp6
,Li11,G
b34)
30min,oncea
day,plus
infrared
irradiatio
nIndo
metacin
25mg3tim
esad
ay5d
ays
Zhou
2014
[44]
MA(A
ship
oint,Li11,Sp10,Sp6,Gv14,Lr3,St36)3
0min,oncea
day,plus
Chineseh
erbalm
edicine
Ibup
rofen300m
gtwicea
day
7days
Zong
etal.2011[45]
MA(A
ship
oint,Sp9,St36,Sp6,Li11,L
i4,S34)3
0min,oncea
day,plus
moxa-moxibustio
nAllo
purin
ol100m
g3tim
esad
ay,
indo
metacin
25mg3tim
esad
ay6days
Zouetal.200
6[46]
EA100H
z(St36,Sp6
)30m
in,oncea
day;EA
2Hz(
St36,Sp6
)30m
in,oncea
day
Allo
purin
ol100m
g3tim
esad
ay,
indo
metacin
25mg3tim
esad
ay6days
Zouetal.200
7[47]
EA2H
z(St36,Sp6
)30m
in,every
otherd
ay,plusa
cupo
intinjectio
nAllo
purin
ol100m
g3tim
esad
ay,
indo
metacin
25mg3tim
esad
ay6days
Note.EA
:electroacup
uncture;MA:m
anualacupu
ncture;A
ship
oint:painspot;Sp10:Xu
ehai;Sp9
:Yinlin
gquan;
St36:zusanli;Ki3:taixi;G
b11:touq
iaoyin;C
v6:qihai;Sp6
:sanyinjiao;Li11:
quchi;Lr3:taicho
ng;B
l23:
shenyu;B
l22:sanjiaoyu;
Cv3:zhon
gji;St40
:fenglon
g;B6
0:Ku
nlun
;St35:du
bi;E
X-LE
4:neixiyan;S34:liangqiu;
EX13:h
eding;Gv14:dazhui;Sp4
:gon
gsun
;B40
:weizhon
g;H3:shaohai;L15:chize;Li4:hegu;C
v4:
guanyuan;B
12:fengshi.

Evidence-Based Complementary and Alternative Medicine 7
Rand
om se
quen
ce g
ener
atio
n (s
elect
ion
bias
)Baiyin 2014
Chenle 2015
Gong and Chen 2014
Gui and Chen 2014
He et al. 2008
Hu et al. 2010
Jin et al. 2012
Li et al. 2013
Liu et al. 2008
Liu et al. 2014
Liu 2014
Ma 2002
Ma 2004
Wang 2013
Wu et al. 2012
Xie et al. 2007
Xie et al. 2009
Xi et al. 2006
Yan 2009
Yin et al. 2005
Zhang 2010
Zhao 2007
Zhao et al. 2009
Zhou et al. 2012
Zhou 2014
Zong et al. 2011
Zou et al. 2006
Zou et al. 2007
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
Blin
ding
of p
artic
ipan
ts an
d pe
rson
nel (
perfo
rman
ce b
ias)
Blin
ding
of o
utco
me a
sses
smen
t (de
tect
ion
bias
)
Inco
mpl
ete o
utco
me d
ata (
attr
ition
bia
s)
Sele
ctiv
e rep
ortin
g (r
epor
ting
bias
)
Oth
er b
ias
?
?
+
?
?
?
+
+
?
?
+
+
+
+
+
?
+
+
+
?
+
+
+
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
+
?
?
?
?
?
?
+
?
?
?
?
?
?
+
?
?
?
?
?
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
Figure 2: Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.

8 Evidence-Based Complementary and Alternative Medicine
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of biasUnclear risk of biasHigh risk of bias
(%)
Figure 3: Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
control therapy (MD −0.26; 95% CI −1.42, 0.90; 𝑃 = 0.66)(Figure 8).
3.9. Adverse Events. Among the included studies, ten [23–27, 29, 30, 33, 37, 38] reported adverse events associatedwith acupuncture or western medicine. The reported adverseevents mainly included gastrointestinal tract reaction, centralnervous system reaction, leukopenia, skin rash, and faintingduring acupuncture treatment. Except two studies [26, 38],eight studies found a higher prevalence of adverse events inthe control group than that in the acupuncture group. Thepooled OR showed a statistically significant lower risk ofadverse events in acupuncture group when compared withwestern medicine (OR 0.08, 95% CI 0.03, 0.23; 𝐼2 = 34%)(Figure 9).
3.10. Metaregression. Metaregression was conducted byresidual (restricted) maximum likelihood (REML) withKnapp-Hartung modification. Three possible factors thatmay contribute to heterogeneity among studies were tested:acupuncture type (manual acupuncture or electroacupunc-ture), combined therapy (whether the patients were treatedwith acupuncture alone or combined with other treatment),and duration of treatment (within a week or longer than aweek). The results of metaregression were listed in Table 3.Combined therapy and duration of treatment were notstatistically correlated with the heterogeneity in uric acid orVAS score. Acupuncture type administered could explain20.20% and 23.55% of the heterogeneity in uric acid and VASscore, respectively. However, the correspondence betweenacupuncture type and heterogeneity within VAS score didnot reach a statistical difference.
3.11. Publication Bias. Publication biases were presented byfunnel plots (Figures 10 and 11), and the resulting graphs showno obvious asymmetry for clinical effect and uric acid. Begg’stest (clinical effect: 𝑧 = 0.86, 𝑃 = 0.392; uric acid: 𝑧 = 0.94,
𝑃 = 0.346) andEgger’s test (clinical effect: 𝑡 = 1.00,𝑃 = 0.325;uric acid: 𝑡 = 0.46, 𝑃 = 0.650) also indicated no statisticallysignificant publication bias.
4. Discussion
Our current study analyzed data from28RCTs involving 2237patients that aimed to assess the therapeutic effect and safetyof acupuncture for gouty arthritis. Based on the findings ofour study, acupuncture could further improve the clinicaleffective rate and decrease uric acid and VAS score whencompared with western medicine. The risk of adverse eventswas significantly lower in acupuncture group. Regarding thedecrease in CRP and ESR, the results remain debatable.
The application of different acupuncture modalities bydifferent investigators can greatly affect curative effect ofacupuncture therapy [48]. The acupuncture proceduresshould be performed according to syndromes differentiationbased on TCM theory. In the selected studies, acupunctureintervention was administered alone [22, 31, 32, 35–37, 41,46] or in combination with other therapies, which includedChinese herbal medicine [20, 21, 23, 25–27, 29, 30, 33, 44],acupoint injection [24, 47], local blocking therapy [28],bloodletting [34, 38, 42], infrared irradiation [43], moxa-moxibustion [45], and western medicine [39, 40]. Regardlessof the type of the additional therapy, acupuncture therapywas mainly received in experimental groups. The acupointselection was inconsistent among included studies; never-theless, Sp6, St36, and Ashi point were the most commonlyused acupoint. In our present study, data was combinedwithout differentiating acupoint selection and acupuncturetechniques. Thus, the results indicate an overall clinicalefficacy and definite conclusion could not be drawn.
Gouty arthritis is one of themost common indications forwhich patients seek complementary and alternative medicinetreatment, even though the use of CAM was relatively low,compared with reported rates of between 28% and 90% in

Evidence-Based Complementary and Alternative Medicine 9
Study or subgroup
Baiyin 2014Chenle 2015Gong and Chen 2014Gui and Chen 2014He et al. 2008Hu et al. 2010Jin et al. 2012Li et al. 2013Liu et al. 2008Liu et al. 2014Liu 2014Ma 2002Ma 2004Wang 2013Wu et al. 2012Xi et al. 2006Xie et al. 2007Xie et al. 2007Xie et al. 2009Yan 2009Yin et al. 2005Yin et al. 2005Zhang 2010Zhao 2007Zhao et al. 2009Zhou et al. 2012Zhou 2014Zong et al. 2011Zou et al. 2006Zou et al. 2007
Total (95% CI)
Total events
Events
371133112237112029415621191314371818202215262
1116428
171114
652
Total
432560323068303156448748424034663030304030402830308020203030
1204
Events
126
108
17206
1118324910667
146
10117
1212179
184
1057
351
Total
442560283060302944418730302032643030302030302930308020203030
1093
Weight
3.0%2.5%4.5%2.9%3.0%5.9%2.6%3.2%5.0%1.9%7.4%3.8%3.0%2.6%3.0%5.3%2.7%3.1%3.1%2.9%3.3%3.6%0.6%2.8%3.1%6.3%1.9%1.7%2.5%2.9%
100.0%
M-H, random, 95% CI
16.44 [5.54, 48.82]2.49 [0.74, 8.35]
6.11 [2.62, 14.27]1.31 [0.44, 3.92]2.10 [0.71, 6.22]2.39 [1.16, 4.90]2.32 [0.72, 7.41]2.98 [1.04, 8.51]1.55 [0.70, 3.44]
3.84 [0.96, 15.37]1.40 [0.76, 2.58]1.56 [0.60, 4.02]3.30 [1.12, 9.74]1.12 [0.35, 3.59]2.50 [0.85, 7.37]4.56 [2.12, 9.81]
6.00 [1.89, 19.04]3.00 [1.05, 8.60]3.45 [1.19, 9.99]2.27 [0.75, 6.89]1.50 [0.54, 4.17]2.79 [1.05, 7.40]
2.15 [0.18, 25.19]1.90 [0.62, 5.86]2.67 [0.92, 7.70]3.81 [1.92, 7.55]
2.67 [0.65, 10.97]5.67 [1.25, 25.61]2.89 [0.86, 9.74]2.88 [0.95, 8.72]
2.71 [2.22, 3.32]
Acupuncture Western medicine Odds ratio Odds ratio
M-H, random, 95% CI
0.02 0.1 1 10 50Favours control Favours acupuncture
Heterogeneity: 𝜏2 = 0.05; 𝜒2 = 34.02, df = 29 (P = 0.24); I2 = 15%
Test for overall effect: Z = 9.72 (P < 0.00001)
Figure 4: Forest plot of acupuncture therapy versus western medicine: clinical effect.
patients with rheumatoid arthritis (RA) and more than 80%in those with osteoarthritis (OA) [49, 50].The goal of therapyin an acute gout attack is prompt and safe termination of painand inflammation [51]. Our results suggest that acupuncturetherapy could further improve pain when compared withwestern medicine, but, in terms of inflammation attenuation,the results remain debatable.
When treating gouty arthritis one needs to treat acuteattacks and lower excess stores of uric acid to achievedissolution of monosodium urate crystals through a long-term reduction of serum uric acid concentrations far beyond
the threshold for saturation of urate and provide prophylaxisto prevent acute flares [52]. In addition to the improvementin pain-relief and clinical effect, acupuncture therapy couldfurther decrease uric acid, compared with conventional west-ern pharmacological therapy. The underlying mechanismof this urate-lowering effect was still unclear, which needsto be further investigated. To analyze the possible sourceof heterogeneity within these studies, metaregression wasperformed.The type of acupuncture therapy was proved to besignificantly correlated with the heterogeneity; the evidencethus suggests that the urate-lowering effects of manual

10 Evidence-Based Complementary and Alternative Medicine
Study or subgroup
Baiyin 2014Hu et al. 2010Jin et al. 2012Li et al. 2013Liu et al. 2008Liu et al. 2014Liu 2014Ma 2002Ma 2004Wang 2013Wu et al. 2012Xi et al. 2006Xie et al. 2007Xie et al. 2007Xie et al. 2009Yan 2009Yin et al. 2005Yin et al. 2005Zhao 2007Zhao et al. 2009Zhou et al. 2012Zong et al. 2011Zou et al. 2006Zou et al. 2007
Total (95% CI)
Mean275.2
244.8581.7217
162.86220.16189.56148.1
149.1169.51
184.08330.788.6688.66
223.08206
221.98189.06109.82109.82
88.3134.82128.25119.26
SD59.47
102.4673.0762.2
46.4746.1
77.9261.3359.9949.68
108.84166.0464.1864.18
6184.6661.4454.5884.1884.1863.4284.54
8395.08
Total436830315644874842403466303030404030303080203030
1009
Mean165.2
202.9736.6
185.68126.5
162.53193.5763.1437.2128.34
148.92100.56
57.881.03176204
224.03224.0377.1780.1766.9
87.17136.8876.76
SD57.8690.0770.2
66.5947.4743.9372.9186.0585.7322.03
104.67180.8267.3264.0377.5479.7765.9965.9975.3975.3996.1174.6994.0862.95
Total446030294441873030203264303030203030303080203030
901
Weight
4.6%4.2%4.1%4.3%4.8%4.8%4.7%4.2%4.1%4.8%3.4%3.1%4.2%4.3%4.2%3.8%4.4%4.4%3.9%3.9%4.6%3.5%3.7%3.9%
100.0%
IV, random, 95% CI110.00 [85.34, 134.66]
41.88 [8.53, 75.23]45.10 [8.84, 81.36]
31.32 [−1.34, 63.98]36.36 [17.79, 54.93]57.63 [38.49, 76.77]−4.01 [−26.43, 18.41]84.96 [49.62, 120.30]
111.90 [76.26, 147.54]41.17 [23.00, 59.34]
35.16 [−16.35, 86.67]230.14 [170.41, 289.87]
30.86 [−2.42, 64.14]7.63 [−24.81, 40.07]47.08 [11.78, 82.38]2.00 [−41.71, 45.71]−2.05 [−32.38, 28.28]−34.97 [−65.61, −4.33]
32.65 [−7.79, 73.09]29.65 [−10.79, 70.09]21.40 [−3.83, 46.63]47.65 [−1.79, 97.09]−8.63 [−53.52, 36.26]
42.50 [1.70, 83.30]
41.30 [24.86, 57.74]
Acupuncture Western medicine Mean difference Mean difference
IV, random, 95% CI
−500 −250 0 250 500Favours control Favours acupuncture
Heterogeneity: 𝜏2 = 1367.30; 𝜒2 = 154.86, df = 23 (P < 0.00001); I2 = 85%
Test for overall effect: Z = 4.92 (P < 0.00001)
Figure 5: Forest plot of acupuncture therapy versus western medicine: uric acid.
acupuncture and electroacupuncture are somewhat different.No conclusions can be drawn as to which acupuncture typeis superior for patients with gouty arthritis.
A previous systematic review [13] consisting of tenRCTs reported that acupuncture alone was more effectivein the improvement of pain and uric acid when comparedwith standard western medicine. However, only ten studieswere identified to be eligible; only VAS score and uricacid were analyzed as outcome. No data about the safetyof acupuncture therapy was provided. In addition, tworecords listed in Figure 1A of the previous systematic reviewwere miscalculated, although this would not influence thefinal conclusion drawn by their work [13]. Based on fiverequired domains (study limitations, consistency, directness,precision, and publication bias), Shekelle and colleaguesassessed the strength of evidence for the conclusions drawnby the aforementioned systematic review [53]. The strengthof evidence for conclusions was judged to be insufficientto support or refute the effectiveness of acupuncture onsymptomatic outcomes, partially due to the unreportedpublication bias. Our meta-analysis managed to summarizeall published RCTs to compare the clinical effect and safety of
acupuncture with those of western medicine. 28 RCTs wereidentified; clinical effect, VAS score, uric acid, ESR, CRP, andadverse events were combined; risk of bias was independentlyassessed by two experienced reviewers using Cochrane’s tool.The results ofmetaregression showed a significant correlationbetween acupuncture type and heterogeneity in uric acid;publication bias assessment indicates no obvious publicationbias. Regarding the safety of acupuncture, which is an obviousadvantage of CAM therapies, the overall incidence of adverseevents in acupuncture groups was significantly lower thanthat in western medicine group.
There are several limitations in our study. First, themethodological qualities of included studies were judgedto be poor; details about allocation concealment were notdescribed by any study, which might limit the value ofconclusion about the clinical efficacy and safety of acupunc-ture. Second, all included studies utilized western medicineas control treatment, making the blinding of participantsimpossible. A sham acupuncture control is preferable, asopposed tomedication or no intervention. Also, the majorityof selected studies were written in Chinese, which limits thedissemination of scientific researches on acupuncture. Future

Evidence-Based Complementary and Alternative Medicine 11
Study or subgroup
Liu et al. 2014Wang 2013Wu et al. 2012Zhao 2007Zhou et al. 2012Zou et al. 2006Zou et al. 2007
Total (95% CI)
Mean4.434.826.646.696.466.576.56
SD1.420.581.371.511.6
1.511.55
Total44403430803030
288
Mean4.664.294.183.8
4.273.7
3.71
SD1.610.791.381.611.7
1.461.52
Total41203230803030
263
Weight
14.3%14.9%14.3%13.9%14.7%14.0%13.9%
100.0%
IV, random, 95% CI−0.23 [−0.88, 0.42]
0.53 [0.14, 0.92]2.46 [1.80, 3.12]2.89 [2.10, 3.68]2.19 [1.68, 2.70]2.87 [2.12, 3.62]2.85 [2.07, 3.63]
1.92 [0.96, 2.87]
Acupuncture Western medicine Mean difference Mean difference
IV, random, 95% CI
−10 −5 0 5 10Favours control Favours acupuncture
Heterogeneity: 𝜏2 = 1.54; 𝜒2 = 102.20, df = 6 (P < 0.00001); I2 = 94%
Test for overall effect: Z = 3.94 (P < 0.0001)
Figure 6: Forest plot of acupuncture therapy versus western medicine: pain intensity (VAS score).
Study or subgroup
Hu et al. 2010Liu 2014Wang 2013Wu et al. 2012Zhou et al. 2012
Total (95% CI)
Mean28.3
51.9711.0915.4527.7
SD14.0516.933.42
10.547.28
Total6887403480
309
Mean29
49.249.84
16.1623.8
SD16.0321.692.559.188.29
Total6087203280
279
Weight
8.6%7.2%
45.4%10.2%28.6%
100.0%
IV, random, 95% CI−0.70 [−5.95, 4.55]2.73 [−3.05, 8.51]1.25 [−0.29, 2.79]−0.71 [−5.47, 4.05]
3.90 [1.48, 6.32]
1.75 [0.11, 3.38]
Acupuncture Western medicine Mean difference Mean difference
IV, random, 95% CI
−10 −5 0 5 10Favours control Favours acupuncture
Heterogeneity: 𝜏2 = 0.91; 𝜒2 = 5.41, df = 4 (P = 0.25); I2 = 26%
Test for overall effect: Z = 2.09 (P = 0.04)
Figure 7: Forest plot of acupuncture therapy versus western medicine: ESR.
Study or subgroup
Hu et al. 2010Liu 2014Wang 2013Wu et al. 2012
Total (95% CI)
Mean15.4817.3822.943.63
SD13.086.646.21.2
Total68874034
229
Mean12.5118.0321.824.41
SD11.837.935.021.45
Total60872032
199
Weight
6.6%20.5%13.0%60.0%
100.0%
IV, random, 95% CI2.97 [−1.35, 7.29]−0.65 [−2.82, 1.52]1.12 [−1.80, 4.04]
−0.78 [−1.42, −0.14]
−0.26 [−1.42, 0.90]
Acupuncture Western medicine Mean difference Mean difference
IV, random, 95% CI
−10 −5 0 5 10Favours control Favours acupuncture
Heterogeneity: 𝜏2 = 0.47; 𝜒2 = 4.26, df = 3 (P = 0.23); I2 = 30%
Test for overall effect: Z = 0.44 (P = 0.66)
Figure 8: Forest plot of acupuncture therapy versus western medicine: CRP.
studies within western context are required. Third, financialconsiderations are important for consumers choosing CAMoptions as expensive treatments are generally avoided andcost is a frequent reason to stop treatment [54]. In Chineseculture, the safety and cost-effectiveness of acupuncturetherapy could assure the compliance of patients. Consideringparticipants’ opinions, cost-effectiveness of acupuncture alsomeant its efficacy. However, only ten studies recorded adverse
events associated with acupuncture and routine care; nostudy included cost-effectiveness assessment. Last, accordingto the ACR guideline, choice of pharmacologic agents shouldbe based upon number of joints involved and pain intensity;the established pharmacologic ULT should be continuedwithout interruption. However, some of our included stud-ies only administered first-line therapy options (NSAIDs,corticosteroids, and colchicine); ULT therapy during acute

12 Evidence-Based Complementary and Alternative Medicine
Study or subgroup
Gui and Chen 2014He et al. 2008Hu et al. 2010Jin et al. 2012Li et al. 2013Liu et al. 2014Liu 2014Wang 2013Xie et al. 2009Yan 2009
Total (95% CI)
Total events
Events1000001004
6
Total32306830314487403040
432
Events1513406268
142
70
Total28306030294187203020
375
Weight
14.0%9.4%9.2%
9.3%8.6%
13.9%9.3%9.5%
16.8%
100.0%
M-H, random, 95% CI0.03 [0.00, 0.23]0.02 [0.00, 0.38]0.09 [0.00, 1.74]Not estimable
0.06 [0.00, 1.07]0.18 [0.01, 3.81]0.16 [0.02, 1.33]0.02 [0.00, 0.34]0.02 [0.00, 0.33]1.00 [0.17, 5.98]
0.08 [0.03, 0.23]
Acupuncture Western medicine Odds ratio Odds ratio
M-H, random, 95% CI
0.001 0.1 1 10 1000Favours acupuncture Favours control
Heterogeneity: 𝜏2 = 0.87; 𝜒2 = 12.20, df = 8 (P = 0.14); I2 = 34%
Test for overall effect: Z = 4.68 (P < 0.00001)
Figure 9: Forest plot of acupuncture therapy versus western medicine: adverse events.
Table 3: Metaregression of basic characteristics of trials and improvement of uric acid and VAS score.
Outcome Number of RCTs Factor tested 𝑡 𝑃 Adjusted 𝑅2
Uric acid 22Acupuncture type 2.21 0.038 20.20%Combined therapy 0.35 0.730 −6.31%
Duration of treatment 1.58 0.127 7.67%
VAS score 7Acupuncture type −1.62 0.165 23.55%Combined therapy 1.32 0.243 12.20%
Duration of treatment −1.27 0.259 10.11%Note. RCT: randomized controlled trial; VAS: visual analogue scale.
0.02 0.1 1 10 50
0
0.5
1
1.5
2
OR
SE(lo
g[O
R])
Figure 10: Funnel plot of acupuncture therapy versus westernmedicine: clinical effect.
attack was stopped; some studies only used ULT, withoutusing first-line pharmacologic options. This would lead to anexaggeration of conclusions; thus, the effect of interventionshould be interpreted cautiously.
−500 −250 0 250 500
0
10
20
30
40
50
MD
SE(M
D)
Figure 11: Funnel plot of acupuncture therapy versus westernmedicine: uric acid.
In summary, the findings of our current study suggestthat acupuncture is better in improving clinical effectiverate, decreasing uric acid, and VAS score compared withwestern medicine. The overall incidence of adverse events in

Evidence-Based Complementary and Alternative Medicine 13
acupuncture group was lower than that in western medicinegroup. Due to the methodological deficiency of included tri-als, acupuncture therapy could not be guaranteed as standardCAM treatment. Additional RCTs with rigorous design andlarger sample size are encouraged.
Competing Interests
The authors have declared no conflict of interests.
References
[1] P. Richette and T. Bardin, “Gout,”The Lancet, vol. 375, no. 9711,pp. 318–328, 2010.
[2] R. L.Wortmann, “Gout and hyperuricemia,”Current Opinion inRheumatology, vol. 14, no. 3, pp. 281–286, 2002.
[3] P. Ghosh, M. Cho, G. Rawat, P. A. Simkin, and G. C. Gardner,“Treatment of acute gouty arthritis in complex hospitalizedpatients with anakinra,” Arthritis Care and Research, vol. 65, no.8, pp. 1381–1384, 2013.
[4] E. Arromdee, C. J. Michet, C. S. Crowson, W. M. O’Fallon, andS. E. Gabriel, “Epidemiology of gout: is the incidence rising?”Journal of Rheumatology, vol. 29, no. 11, pp. 2403–2406, 2002.
[5] P. P. Khanna, G. Nuki, T. Bardin et al., “Tophi and frequentgout flares are associated with impairments to quality of life,productivity, and increased healthcare resource use: resultsfrom a cross-sectional survey,” Health and Quality of LifeOutcomes, vol. 10, article 117, 2012.
[6] E. Pascual, “Persistence of monosodium urate crystals andlow-grade inflammation in the synovial fluid of patients withuntreated gout,” Arthritis & Rheumatism, vol. 34, no. 2, pp. 141–145, 1991.
[7] J. A. Singh and V. Strand, “Gout is associated with morecomorbidities, poorer health-related quality of life and higherhealthcare utilisation in US veterans,” Annals of the RheumaticDiseases, vol. 67, no. 9, pp. 1310–1316, 2008.
[8] B. F. Mandell, “Clinical manifestations of hyperuricemia andgout,” Cleveland Clinic Journal of Medicine, vol. 75, supplement5, pp. S5–S8, 2008.
[9] N. Dalbeth, B. Clark, K. Gregory et al., “Mechanisms of boneerosion in gout: a quantitative analysis using plain radiographyand computed tomography,” Annals of the Rheumatic Diseases,vol. 68, no. 8, pp. 1290–1295, 2009.
[10] M. Hamburger, H. S. B. Baraf, T. C. Adamson III et al., “2011Recommendations for the diagnosis and management of goutand hyperuricemia,” Postgraduate medicine, vol. 123, no. 6, pp.3–36, 2011.
[11] D. Khanna, P. P. Khanna, J. D. Fitzgerald et al., “2012 AmericanCollege of Rheumatology guidelines for management of gout.Part 2: therapy and antiinflammatory prophylaxis of acute goutyarthritis,” Arthritis Care & Research, vol. 64, no. 10, pp. 1447–1461, 2012.
[12] S. L. Kolasinski, “Food, drink, and herbs: alternative therapiesand gout,” Current Rheumatology Reports, vol. 16, no. 4, article409, 2014.
[13] W. B. Lee, S. H. Woo, B.-I. Min, and S.-H. Cho, “Acupuncturefor gouty arthritis: a concise report of a systematic and meta-analysis approach,” Rheumatology, vol. 52, no. 7, pp. 1225–1232,2013.
[14] D. Moher, A. Liberati, J. Tetzlaff, D. G. Altman, and P. Group,“Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement,” PLoS Medicine, vol. 6, no. 7,Article ID e1000097, 2009.
[15] S. L. Wallace, H. Robinson, A. T. Masi, J. L. Decker, D. J.McCarty, andT. F. Yu, “Preliminary criteria for the classificationof the acute arthritis of primary gout,” Arthritis & Rheumatism,vol. 20, no. 3, pp. 895–900, 1977.
[16] I. Pelaez-Ballestas, C. H. Cuevas, R. Burgos-Vargas et al.,“Diagnosis of chronic gout: evaluating the american college ofrheumatology proposal, European league against rheumatismrecommendations, and clinical judgment,” Journal of Rheuma-tology, vol. 37, no. 8, pp. 1743–1748, 2010.
[17] H. J. E. M. Janssens, J. Fransen, E. H. van de Lisdonk, P. L.C. M. van Riel, C. van Weel, and M. Janssen, “A diagnosticrule for acute gouty arthritis in primary care without joint fluidanalysis,”Archives of Internal Medicine, vol. 170, no. 13, pp. 1120–1126, 2010.
[18] S. A. O. T. C. Medicine, Standards for Diagnosis of Syndromesor Diseases of TCM and Evaluation of the Therapeutic Effect,Nanjing University Press, 1994.
[19] J. P. T. Higgins and S. Green, Cochrane Handbook for SystematicReviews of Interventions, Version 5.1.0, The Cochrane Collabo-ration, 2011.
[20] M. Baiyin, “Clinical observation on Mongolian medicine in thetreatment of gout,” Journal of North Pharmacy, vol. 11, no. 9, pp.36–37, 2014.
[21] M. Chenle, “Clinical observation on mongolian medicine com-bined with silver needle in the treatment of 25 cases of gout,”Journal of Medicine and Pharmacy of Chinese Minorities, no. 5,pp. 7–8, 2015.
[22] Y. Gong and M. Chen, “Clinical study of fire needling plusabdominal acupuncture in the treatment of acute gouty arthri-tis,” Hubei Journal of Traditional Chinese Medicine, vol. 36, no.12, p. 62, 2014.
[23] M. Gui and M. Chen, “Acupuncture combined with Chineseherbal medicine for 32 cases of acute gouty arthritis,” HunanJournal of Traditional Chinese Medicine, vol. 30, no. 12, pp. 74–75, 2014.
[24] Y. He, L. Gu, X. Li, and X. Yang, “Electroacupuncture plusacupoint injection for the treatment of acute gouty arthritis,”Modern Journal of Integrated Traditional Chinese and WesternMedicine, vol. 17, no. 3, pp. 383–384, 2008.
[25] Y. Hu, J. Li, K. Cao et al., “Clinical observation on acupuncturecombined with traditional Chinese medicine for treating acutegouty arthritis of 68 cases,” Journal of Sichuan of TraditionalChinese Medicine, vol. 28, no. 5, pp. 72–74, 2010.
[26] Z. Jin, S. Jiang, Y. Wang et al., “Therapeutic observation oncombined use of acupuncture and medication for acute goutyarthritis,” Shanghai Journal of Acupuncture and Moxibustion,vol. 31, no. 9, pp. 670–672, 2012.
[27] J. Li, T. He, X. Yan, and X. Du, “Combined use of acupunctureand medication for damp-heat with blood stasis acute goutyarthritis,”Asia-Pacific Traditional Medicine, vol. 9, no. 2, pp. 87–88, 2013.
[28] B. Liu, H.-M.Wang, and F.-Y.Wang, “Observation on therapeu-tic effect of electroacupuncture combined with local blockingtherapy on acute gouty arthritis,” Chinese Acupuncture andMoxibustion, vol. 28, no. 9, pp. 659–661, 2008.
[29] J. Liu, W. Xu, and X. Zhu, “Clinical observation on fireneedling plus external application of Chinese herbal medicine

14 Evidence-Based Complementary and Alternative Medicine
for the treatment of acute gouty arthritis,” Shanghai Journal ofAcupuncture and Moxibustion, vol. 33, no. 4, pp. 343–345, 2014.
[30] Z. Liu, “Combined use of acupunctureandmedication for acutegouty arthritis with retention of damp-heat,” Shanxi Journal ofTraditional Chinese Medicine, vol. 30, no. 4, pp. 27–28, 2014.
[31] X. Ma, “Acupuncture treatment of gouty arthritis and effect onserumuric acid,”Chinese Acupuncture andMoxibustion, vol. 22,no. 3, pp. 151–152, 2002.
[32] X. Ma, “Clinical analysis for the acupuncture treatment in casesof gouty renal damage,” Journal of Traditional Chinese Medicine,vol. 24, no. 3, pp. 185–187, 2004.
[33] H.Wang, “Clinical observation on acupuncture combined withfour wonderful decoction for acute gouty arthritis,” ChineseJournal of Basic Medicine in Traditional Chinese Medicine, vol.39, no. 6, pp. 688–689, 2013.
[34] Y. Wu, M. Xu, S. Zheng, J. Liao, C. Hu, andW. Zheng, “Clinicalresearch on electroacupuncture combined with blood-lettingtherapy by fire needling for treating acute gouty arthritis,”Liaoning Journal of Traditional Chinese Medicine, vol. 39, no. 7,pp. 1400–1402, 2012.
[35] Y. Xi, T. Zou, Z. Ai, Y. Liu, and Q. Zhang, “Clinical observationon acupuncture treatment of acute gouty arthritis in terms ofclearing heat eliminating dampness and stasis,” AcupunctureResearch, vol. 31, no. 6, pp. 362–364, 2006.
[36] J.-Y. Xie, L.Wang,Q.-X. Li, andX.-M. Li, “Study onmechanismsof electroacupuncture treatment of acute gouty arthritis,” Chi-nese Acupuncture and Moxibustion, vol. 27, no. 12, pp. 898–900,2007.
[37] X.-Q. Xie, Y.-X. Cao, F. Li, Y. Meng, and L. Deng, “Observationon therapeutic effect of surrounded needling therapy on acutegouty arthritis,” Chinese Acupuncture and Moxibustion, vol. 29,no. 5, pp. 375–377, 2009.
[38] B. Yan, “Observation on therapeutic effect of acupuncturecombined with blood-letting therapy on gout arthritis,” Journalof KunmingMedical University, vol. 30, no. 12, pp. 101–104, 2009.
[39] Y. Yin, H. Zhang, and T. Zhang, “Clinical observation onelectroacupuncture combined with medicine for treatment ofacute gouty arthritis,” Chinese Acupuncture and Moxibustion,vol. 25, no. 10, pp. 683–685, 2005.
[40] J. Zhang, “Observation on therapeutic effects of eye-acupuncture therapy for acute gouty arthritis,” LiaoningJournal of Traditional Chinese Medicine, vol. 37, no. 2, pp.334–335, 2010.
[41] H. Zhao, “Combined use of acupuncture andmedication for thetreatment of 60 cases of acute gouty arthritis,” Journal of ClinicalAcupuncture and Moxibustion, vol. 23, no. 9, pp. 26–27, 2007.
[42] Q.-W. Zhao, J. Liu, X.-D. Qu et al., “Observation on therapeuticeffect of electroacupuncture plus blood-letting puncture andcupping combined with diet intervention for treatment of acutegouty arthritis,” Chinese Acupuncture and Moxibustion, vol. 29,no. 9, pp. 711–713, 2009.
[43] L. Zhou, Q. Xu, and W. Zhang, “Comparative observationof therapeutic effects of acupuncture combined with infraredirradiation and western medicine on acute gouty arthritis,”World Journal of Acupuncture—Moxibustion, vol. 22, no. 1, pp.30–34, 2012.
[44] M. Zhou, “Combined use acupuncture andmedication for acutegouty arthritis of 20 cases,” Nei Mongol Journal of TraditionalChinese Medicine, no. 14, p. 44, 2014.
[45] J. Zong, Y. Gao, S.Wang, H. He, and J. Zheng, “40 cases of acutegouty arthritis treated bywarming needlemoxibustion,” Journal
of Sichuan of Traditional ChineseMedicine, vol. 29, no. 3, pp. 115–117, 2011.
[46] R. Zou, H.-X. Zhang, T.-F. Zhang, and Y. Xu, “Treatmentto acute gouty arthritis with electro-acupuncture at differentfrequencies versus medication,” Chinese Journal of ClinicalRehabilitation, vol. 10, no. 43, pp. 188–189, 2006.
[47] R. Zou, H.-X. Zhang, T.-F. Zhang, and Y. Xu, “Observationon therapeutic effect of electroacupuncture combined withacupoint-injection on acute gouty arthritis,” Chinese Acupunc-ture and Moxibustion, vol. 27, no. 1, pp. 15–17, 2007.
[48] Z. T. Lv, W. Song, J. Wu et al., “Efficacy of acupuncture inchildren with nocturnal enuresis: a systematic review andmeta-analysis of randomized controlled trials,” Evidence-BasedComplementary and Alternative Medicine, vol. 2015, Article ID320701, 12 pages, 2015.
[49] E. Ernst, “Complementary and alternativemedicine in rheuma-tology,” Best Practice and Research: Clinical Rheumatology, vol.14, no. 4, pp. 731–749, 2000.
[50] P. Katz and F. Lee, “Racial/ethnic differences in the use of com-plementary and alternative medicine in patients with arthritis,”Journal of Clinical Rheumatology, vol. 13, no. 1, pp. 3–11, 2007.
[51] N. Schlesinger, “Management of acute and chronic goutyarthritis: present state-of-the-art,” Drugs, vol. 64, no. 21, pp.2399–2416, 2004.
[52] N. Schlesinger, N. Dalbeth, and F. Perez-Ruiz, “Gout—what arethe treatment options?” Expert Opinion on Pharmacotherapy,vol. 10, no. 8, pp. 1319–1328, 2009.
[53] P. G. Shekelle, J. FitzGerald, S. J. Newberry et al., Managementof Gout, Agency for Healthcare Research andQuality, Rockville,Md, USA, 2016.
[54] J. K. Rao, K. Kroenke, K. A. Mihaliak, S. C. Grambow, andM.Weinberger, “Rheumatology patients’ use of complementarytherapies: results from a one-year longitudinal study,” ArthritisCare & Research, vol. 49, no. 5, pp. 619–625, 2003.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com