Embed Size (px)
Citation preview

Top Clin Nutr Vol 29 No 2 pp 98ndash112 Copyright c 2014 Wolters Kluwer Health | Lippincott Williams amp Wilkins
REVIEW
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient A Clinical Update
Kyle L Thompson MS RD CNSC
The increase of bariatric surgery patients implies that more of them will present to intensive care units with altered gastrointestinal anatomy Intensive care unit patients who have a history of recent or previous bariatric surgery comprise a unique population for conducting nutritional as-sessments and developing nutrition care plans An assumption that such patients can automatically be assigned to guidelines intended for critically ill obese patients is problematic Limited research exists to define appropriate nutrition support practice in the postbariatric population This review provides an overview of bariatric surgical procedures with an emphasis on the sequelae of altered gastrointestinal anatomy the evaluation of current evidence on providing nutrition support to critically ill patients who have a history of bariatric surgery and to update clinical guidelines for delivering nutrition support to these patients Key words bariatric surgery critical illness enteral nutrition nutrition support obesity parenteral nutrition
INCREASED numbers of bariatric surgical procedures imply that there will be more
patients entering intensive care units (ICU) with altered gastrointestinal (GI) anatomy1
The number of bariatric surgery procedures grew substantially every year from the mid-1990s until 2009 when they leveled off at about 220 000 per annum2 Intensive care unit patients who have a history of recent or previous bariatric surgery comprise a
Author Affiliation Department of Nutrition and Health Care Management College of Health Sciences Appalachian State University Boone North Carolina
The author has no significant relationships with or financial interest in any commercial companies per-taining to this article
Correspondence Kyle L Thompson MS RD CNSC Department of Nutrition and Health Care Manage-ment Appalachian State University Boone NC 28607 (thompsonklappstateedu)
DOI 10109701TIN0000445894751463f
unique population in terms of conducting a nutritional assessment and developing the nutrition care plan Some of these patients may be obese or morbidly obese and have complications from their surgery Others may be of normal weight with altered GI anatomy or underweight with malnutrition as a result of the new illness or excessive weight loss and nutrient deficiencies
A descriptive study of 467 nutrition support professionals in 2007 found that of those who responded to a survey 60 reported seeing 1 to 10 bariatric surgery patients with com-plications within the previous year Twenty percent of the respondents stated that they had seen more than 20 such patients in the same time frame1 Practitioners reported the perception that they were seeing greater num-bers of postbariatric patients1 Methods of nu-trition assessment and intervention for criti-cally ill postbariatric patients varied broadly among practitioners and depended on the in-dividual practitionerrsquos clinical judgment1
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
98
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 99
The postbariatric population is likely to present with obesity However for some patients with a distant history of bariatric surgery body mass index may be normal A subset of postbariatric patients may be underweight andor have developed malnu-trition For all patients with a history of bariatric surgery altered GI anatomy must be considered when providing nutritional care Bariatric surgery patients who have under-gone malabsorptive procedures retain a risk for nutrient deficiencies that may become severe Many of the long-term metabolic hormonal and physical effects of bariatric surgery remain unknown although long-term data are accumulating The purpose of this re-view is to provide an overview of bariatric surgical procedures to discuss sequelae of altered GI anatomy and to evaluate current evidence for critically ill patients who have undergone bariatric surgery
SEARCH STRATEGY
The search of databases included PubMed and CINAHL Inclusion criteria included ran-domized controlled trials clinical trials obser-vational studies descriptive studies system-atic reviews and meta-analyses published in English within the past 10 years however older studies were considered if deemed rel-evant to the review The population included adults 19 years of age or older with a distant or recent history of bariatric surgery Care set-tings were critical care and home care The nutrition intervention studied was nutrition support A total of 126 articles were identified initially through database searches Following a review of article abstracts 8 articles were found to address the topic directly One ad-ditional article was identified by a reviewer recommendation
While literature is available regarding com-plications of bariatric surgery and the criti-cally ill patient with obesity little research is focused on critical illness in patients with a distant or recent history of bariatric surgery No randomized controlled trials were located
that addressed this topic The identified ar-ticles include 1 retrospective cohort study 1 descriptive study 2 consensus documents and 5 narrative reviews Although this review is narrative every effort was made to select studies that reflect the current state of knowl-edge regarding the topic Table 1 lists studies identified via the literature search
BARIATRIC SURGERY UPDATE
Bariatric surgical procedures fall into 3 ma-jor categories (1) malabsorptive (2) restric-tive and (3) combination that is both re-strictive and malabsorptive3 Most bariatric surgical procedures are not considered exper-imental the history of GI surgery for the pur-poses of promoting weight loss now stretches back nearly 60 years4 Bariatric surgery is sup-ported by an increasing amount of long-term data regarding effectiveness and safety56
During the past decade efforts have increased to accumulate data for the purpose of defin-ing evidence-based guidelines and best clini-cal practices in bariatric surgery The Bariatric Outcomes Longitudinal Database is a propri-etary database that has existed since 2007 Es-tablished by the Surgical Review Corporation the Bariatric Outcomes Longitudinal Database currently houses data for more than 500 000 bariatric surgery patients worldwide7 The Bariatric Outcomes Longitudinal Database is used to establish quality benchmarks for bariatric surgical procedures and to establish standards by which surgical centers may be designated Bariatric Centers of Excellence8
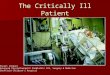
Four bariatric surgical methods are illus-trated in the Figure9 Worldwide the most common bariatric surgery is the laparoscop-ically placed adjustable gastric band (AGB) (see the Figure) A purely restrictive pro-cedure the AGB induces weight loss by limiting the size of the gastric pouch and thus reducing the amount of food that can be consumed3 The stomach and the lower GI tract remain intact and the pathway of food through the digestive system remains un-changed Repeated operations are common
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Tab
le 1
N
utr
itio
n S
up
po
rt P
ost
ndashBar
iatr
ic S
urg
ery
Tab
le o
f St
ud
ies
Iden
tifi
ed V
ia
Lite
ratu
re S
earc
h
Ty
pe
of
Stu
dy
M
eth
od
s C
on
clu
sio
ns
Ch
ob
an e
t al
49
Co
nse
nsu
s gu
idel
ines
Sy
stem
atic
rev
iew
of
Pro
vid
es g
uid
elin
es o
n t
he
bas
is o
f ava
ilab
le e
vid
ence
fo
r n
utr
itio
n c
are
evid
ence
o
f h
osp
ital
ized
ad
ult
s w
ith
ob
esit
y Fu
jioka
et
al14
N
arra
tive
rev
iew
N
A
Des
crib
es n
utr
itio
n p
rob
lem
s th
at m
ay o
ccu
r in
ho
spit
aliz
ed a
nd
cr
itic
ally
ill p
atie
nts
fo
llow
ing
bar
iatr
ic s
urg
ery
H
amilt
on
et
al63
R
etro
spec
tive
co
ho
rt
Ret
rosp
ecti
ve c
har
t H
ypo
calo
ric
TP
N m
ain
tain
ed n
utr
itio
nal
sta
tus
wh
ile p
rom
oti
ng
wei
ght
revi
ew
loss
in h
om
e ca
re p
atie
nts
wit
h c
om
plic
atio
ns
of
bar
iatr
ic s
urg
ery
K
um
pf
et a
l1 D
escr
ipti
ve
Qu
esti
on
nai
re
467
pra
ctit
ion
ers
ind
icat
ed w
idel
y va
ryin
g p
ract
ices
reg
ard
ing
the
adm
inis
tere
d t
o 4
73
pro
visi
on
of
nu
trit
ion
su
pp
ort
to
cri
tica
lly il
l m
orb
idly
ob
ese
nu
trit
ion
su
pp
ort
p
atie
nts
th
us
sup
po
rtin
g th
e n
eed
fo
r th
e d
evel
op
men
t o
f p
rofe
ssio
nal
s ev
iden
ce-b
ased
pra
ctic
e gu
idel
ines
M
arti
nd
ale
et a
l54
Nar
rati
ve r
evie
w
NA
P
rovi
des
su
gges
tio
ns
for
futu
re r
esea
rch
reg
ard
ing
crit
ical
ly il
l m
orb
idly
o
bes
e p
atie
nts
M
cCla
ve e
t al
15
Co
nse
nsu
s N
A
Pro
vid
es c
on
sen
sus
reco
mm
end
atio
ns
for
the
nu
trit
ion
car
e o
f cr
itic
ally
re
com
men
dat
ion
s ill
mo
rbid
ly o
bes
e p
atie
nts
Se
gara
n37
N
arra
tive
rev
iew
N
A
Dis
cuss
es is
sues
su
rro
un
din
g th
e p
rovi
sio
n o
f n
utr
itio
n s
up
po
rt t
o
ob
ese
cri
tica
lly il
l pat
ien
ts e
xp
erie
nci
ng
com
plic
atio
ns
follo
win
g b
aria
tric
su
rger
y
Shah
22
Nar
rati
ve r
evie
w
NA
D
iscu
sses
th
e p
rovi
sio
n o
f n
utr
ien
ts t
o p
atie
nts
wh
o b
eco
me
ill
po
stsu
rgic
ally
des
crib
es t
he
pro
visi
on
of
nu
trie
nts
th
rou
gh t
he
rem
nan
t st
om
ach
Z
iegl
er e
t al
62
Nar
rati
ve r
evie
w
NA
P
rovi
des
up
dat
e o
n lo
ng-
term
fo
llow
-up
of
nu
trit
ion
issu
es in
p
ost
ndashbar
iatr
ic p
atie
nts
100 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Ab
bre
viat
ion
s N
A n
ot
app
licab
le T
PN
to
tal p
aren
tera
l nu
trit
ion
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 101
Figure Altered gastrointestinal anatomy resulting from 4 methods of bariatric surgery Image courtesy of Walter Pories MD Reprinted with permission
since the gastric band may become dis-placed or eroded Typical weight losses re-sulting from successful AGB procedures aver-age about 35 of excess weight although a long-term failure rate of nearly 50 has been noted3 Failure may be related to band-related complications or to consumption of amounts of food andor nutrient-dense liquids large enough to stretch the stomach pouch
Popularly known as the ldquogastric bypassrdquo the Roux-en-Y surgery is the most common bariatric procedure used in the United States (see the Figure) In this combination pro-cedure the proximal and distal portions of the stomach are surgically separated and a stomach pouch of about 30 mL in volume is created10 A loop of the jejunum (the ldquoRoux limbrdquo) is attached to the stomach pouch and the biliopancreatic limb is attached to the Roux limb about 75 to 150 cm from the anas-tomosis of the stomach pouch and jejunum The portion of intestine remaining below the anastomosis created below the Roux junction is called the ldquocommon channelrdquo Weight loss is induced both by the reduced size of the stomach pouch and by the malabsorption re-
sulting from the intestinal resection356 Long-term results have been described as 49 to 62 excess weight loss maintained over 5 to 14 years in about 85 of patients35 Postsurgi-cal complications such as dumping syndrome and macro- and micronutrient deficiencies are common occurring in an estimated 70 of Roux-en-Y patients3 However in most cases these complications are manageable with the use of nutrient supplementation and nutri-tion education regarding appropriate eating practices11
ldquoGastric sleeverdquo surgery has gained popu-larity in recent years Gastric sleeve surgery is purely restrictive and involves removal of a substantial portion of the stomach leaving a greatly reduced pouch (the ldquosleeverdquo) for digestive purposes (see the Figure) Gastric sleeve surgery may be used as part of a surgical sequence for high-risk patients patients may receive the sleeve to promote initial weight loss and then receive a gastric bypass at a later time upon improvement of risk factors12
Short-term data indicate that the gastric sleeve surgery may provide greater weight loss results and fewer complications than the AGB
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
102 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
however unlike gastric banding the gastric sleeve surgery is not reversible Compared with the Roux-en-Y gastric bypass surgical complication rates are similar and there are fewer serious nutritional complications51314
The biliopancreatic diversion with duode-nal switch is a combination surgery that be-came popular in the 1990s and then quickly fell from favor (see the Figure) Although the surgery results in slightly greater weight loss than the Roux-en-Y bypass high rates of severe macro- and micronutrient deficien-cies surgical complications and deaths have prompted many bariatric surgeons to aban-don the procedure61516 Patients who have undergone biliopancreatic diversion with duodenal switch however may present with critical illness thus the clinician should be familiar with the anatomical alterations asso-ciated with the surgery
At the current time little is known regard-ing the long-term consequences of substan-tially altered GI anatomy and chronic malab-sorption of nutrients15 Data have indicated reductions in long-term mortality in patients receiving both gastric banding and gastric by-pass surgical procedures17 Short-term com-plication rates and weight loss results appear to be influenced by the skill of the bariatric surgeon with the best results obtained by surgeons and facilities performing high vol-umes of bariatric surgical procedures31618
As long-term data continue to accumulate it is expected that knowledge will increase re-garding outcomes of bariatric surgery over the life span
POSTOPERATIVE COMPLICATIONS OF BARIATRIC SURGERY
Nutrition-related
Common nutrition complications of bariat-ric surgery include both macro- and micronu-trient deficiencies The overall nutrition-related complication rate for patients under-going bariatric surgery appears to be about 30 with numbers substantially higher for malabsorptive surgical procedures19 Nutri-
tion complications may occur because of al-terations in the size and length of the stomach and the intestines reduction of surface area for nutrient absorption reduced numbers of metabolites necessary for nutrient absorption such as intrinsic factor or gastric acid andor alterations in dietary consumption patterns
Macronutrient deficiencies
Little is known regarding long-term pat-terns of dietary consumption following bariatric surgery20 However it seems appar-ent that a substantial decrease in total con-sumption of macronutrients occurs whether or not percentage intake of macronutrients is altered following surgery A systematic re-view of dietary intake following AGB surgery found that although proportional protein in-take as part of total dietary intake is main-tained or slightly increased total protein con-sumption in grams is decreased20 The same review reported the likelihood of a moder-ate decrease in percent fat intake and a con-current increase in percent carbohydrate in-take among the same population20 Moize et al21 studied a cohort of patients who had undergone either sleeve gastrectomy or Roux-en-Y gastric bypass and found no long-term changes in percent macronutrient intake for either group It should be noted that the pop-ulation was Spanish and macronutrient pro-portions were compared with those identi-fied for the general Spanish population21 The cohortrsquos total nutrient intake decreased sig-nificantly with total energy intake but not macronutrient distribution predicting percent weight loss21 Analysis of typical food con-sumption patterns is an important component of a complete nutrition assessment for post-bariatric patients although this information may be difficult to obtain in the critical care setting
Protein deficiency is the most com-mon macronutrient deficit following bariatric surgery and if severe can result in a diag-nosis of protein-energy malnutrition1922 Pos-sible causes of protein-energy malnutrition include reduced oral intake andor surgical complications resulting in too much or too
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 103
rapid weight loss The small stomach pouch remaining after a gastric resection may pro-duce insufficient stomach acid to promote normal protein digestion22 Enteral nutrition or reversal of the surgery may be required in
1922 extreme cases Bariatric surgery can result in fat malab-
sorption with resultant steatorrhea and other metabolic complications2324 One study of 9 patients before and after Roux-en-Y gastric by-pass surgery found a significant reduction in fat absorption (P lt 001) following bariatric surgery but no differences in fecal fat excre-tion pre- and postsurgery24 The degree of fat malabsorption in Roux-en-Y patients appears to be associated with the length of the com-mon channel below the anastomosis of the biliopancreatic and Roux limbs According to Fujioka et al19 a common channel length of 100 cm appears to be well tolerated in terms of postsurgical fat absorption capabilities If fat malabsorption is severe patients under-going bariatric surgery may develop essential fatty acid deficiency requiring parenteral ad-ministration of lipids or even reversal of the
19surgery Improvements in carbohydrate metabol-
ism including resolution of symptoms of di-abetes have been associated with bariatric surgery25 Similar improvements in β -cell function and insulin sensitivity have occurred in both gastric bypass and AGB patients suggesting that substantial weight loss is largely responsible for positive metabolic outcomes26 Odstrcil et al24 and Hammer and Hammer27 reported that indicators of carbo-hydrate absorption remained unchanged in a group of obese patients examined before and after Roux-en-Y gastric bypass surgery Prob-lems with carbohydrate-associated energy de-ficiency following surgery may be related to medical or surgical complications that pre-clude ingestion of adequate albeit reduced amounts of carbohydrates
Micronutrient deficiencies
Micronutrient deficiencies following bariat-ric surgery can exacerbate or complicate the course of critical illness15 Micronutrient
deficiencies may be related to the length of absorptive surface area remaining after surgery22 Depending on the specific portions of the digestive and absorptive surface areas that have been bypassed or reduced a variety of macro- or micronutrient deficiencies may occur
Moizacute found that dietary intake of e et al21
calcium magnesium phosphorus and iron did not meet recommendations in a cohort of postndashsleeve gastrectomy and postndashRoux-en-Y gastric bypass patients Other investigators have reported micronutrient deficiencies in-cluding the water-soluble vitamins thiamine B12 folate and C as well as the fat-soluble vita-mins D A and K28 Commonly reported min-eral deficiencies include iron zinc calcium and copper2829 however altered digestion and absorption of virtually any micronutrient may occur following surgery Physical and bio-chemical findings may indicate the presence of micronutrient deficiencies in postbariatric patients Investigators have described a vari-ety of nutritional aberrations including zinc deficiency associated with acrodermatitis30
iron deficiency associated with anemia31 and vitamin A deficiency associated with low serum prealbumin32 The mechanism underly-ing vitamin A deficiency and reduced levels of serum proteins such as prealbumin in bariatric patients remains poorly understood Explana-tions proposed have included reduced food intake reduced absorptive surface area in the small intestine and effects associated with prealbuminrsquos role as a transporter of retinol-binding protein32
Moize et al21 found 25-hydroxy vitamin D deficiency to be the most common micronu-trient deficiency within a study group of more than 300 postndashbariatric surgery patients Sim-ilar to several other micronutrients the pre-cise location where vitamin D is absorbed in the intestine remains unknown making the prediction of specific deficiencies in particu-lar patients difficult29 Thus patients with a history of bariatric surgery should be mon-itored at regular intervals for overall nutri-tional status including micronutrient status28
The possibility of atypical micronutrient
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
104 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
deficiencies should not be dismissed when performing nutrition assessment in the postndash bariatric surgery population
Dumping syndrome
Dumping syndrome is the most com-mon nutrition-related problem experienced by Roux-en-Y gastric bypass patients with ap-proximately 50 to 70 of patients experienc-ing this symptom22 The Roux-en-Y procedure promotes dumping syndrome by allowing for very rapid infusion of the reduced stomachrsquos contents into the jejunum with subsequent forceful osmotic effects33 During a dumping episode a quick fluid shift occurs between the intravascular space and the lumen of the intestine34 The early phase of dumping may include abdominal pain nausea cramping and diarrhea The late phase encompasses the effects of resultant hypoglycemia and may in-clude sweating palpitations weakness trem-bling and even syncope34
Avoidance of foods such as simple carbo-hydrates which may precipitate dumping may be associated with weight loss However Shah22 and Banerjee et al33 recently reported that long-term weight loss following a Roux-en-Y procedure is associated with reduced food intake rather than with dumping syn-drome Dumping syndrome in severe cases may serve as an etiological factor in identified macro- and micronutrient deficiencies or protein-energy malnutrition Dumping syn-drome can usually be managed effectively by providing appropriate nutrition education to bariatric surgical patients35 While dumping symptoms tend to lessen with the passage of time refractory dumping symptoms may require medical or surgical intervention Medical treatments may include the use of somatostatin analogs such as octreotide which has been demonstrated to be effec-tive in ameliorating dumping symptoms34
Surgical treatment may include anatomical revisions designed to slow down the speed of gastric emptying34 For patients who have received a Roux-en-Y procedure insertion of an additional length of jejunum between the stomach and the jejunal anastomosis may
relieve dumping symptoms34 Enteral feeding into the jejunum may be required if dumping symptoms cannot be resolved34
Nausea and vomiting
Nausea and vomiting in post-bariatric surgery patients may be associated with con-sumption of portions too large for the reduced gastric pouch or by the simultaneous con-sumption of solids and liquids Nausea and vomiting in the postbariatric surgery patient requires medical follow-up and further inves-tigation since this symptom may result from strictures or GI obstruction10 The majority of cases of nausea and vomiting can be resolved with appropriate nutrition education35
Mechanical causes of nausea and vomiting may require surgical treatment Although un-common in the critical care setting preg-nancy can be a cause of nausea and vomiting Postndashbariatric surgical patients who are preg-nant should be carefully monitored for nutri-ent deficiencies and supplemented as needed on an individual basis36
Surgery-related
Surgical complications appear in approxi-mately 10 to 16 of Roux-en-Y gastric by-pass patients2237 Correction of surgical com-plications often requires additional surgery and such patients may require care in an ICU for some period of time during their clinical course Until the complications are resolved patients may require nutrition support since intake of nutrients by the oral route may be contraindicated Surgical complications can include but are not limited to anastomotic leaks wound infections anastomotic stric-tures and incisional hernias
The most common surgical complication is the anastomotic leak affecting 2 to 5 of Roux-en-Y bypass patients137 Leaks occur most commonly at the gastrojejunal anasto-mosis with leaks also occurring at the je-junojejunostomy site or at the gastric sta-ple line3738 More severely obese patients tend to experience an increased number of complications39 In a prospective descrip-tive study of 3018 Roux-en-Y gastric bypass
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 105
patients Gonzalez et al38 found that 63 pa-tients developed anastomotic leaks Among these patients 58 reoperations were required with duration of nutrition support lasting from 2 to 12 weeks3738 Thirty percent of these patients were receiving some type of nutrition support at hospital discharge3738
Anastomotic strictures represent a com-mon surgical complication of bariatric surgery In many cases strictures can be cor-rected via single or repeated endoscopic di-latation procedures40 Some strictures require further surgery to achieve resolution40
NUTRITION SUPPORT OF CRITICALLY ILL POSTndashBARIATRIC SURGERY PATIENTS
Several authors have noted a dearth of research and thus a lack of evidence-based guidelines regarding nutrition sup-port for critically ill postndashbariatric surgery patients15223741 Little is known regarding nutrition assessment issues in this population Published definitions of hypocaloric high-protein feeding are not consistent and the degree to which weight status interacts with the effects of altered GI anatomy in critical illness is poorly understood
At the present time resources available to practitioners caring for such patients include a limited amount of literature consensus guide-lines for obese patients and clinical judgment For patients with a recent history of bariatric surgery some literature is available regarding treatment of various complications including nutrient deficiencies and nutrition impact se-quelae such as dumping syndrome
Nutrition support approaches will vary on the basis of the patientrsquos current weight status Although a large number of post-bariatric patients will present with obesity patients may be underweight overweight or normal weight Morbid obesity may be fully or partially resolved in individual patients and malnutrition may vary in degree and type Nutrition support professionals must be prepared to provide individualized care
to postndashbariatric surgical patients on the basis of each patientrsquos particular situation and clinical judgment based on practitioner experience assumes increased importance
Goals of nutrition support
According to the American Society for Parenteral and Enteral NutritionSociety of Critical Care Medicine (ASPENSCCM) guide-lines (McClave et al42) the goals for nutri-tion support in critically ill obese patients differ little from goals for normal weight pa-tients promotion of healing by modulating the stress response prevention of oxidative cell injury and optimization of the immune response42 Avoidance of poor metabolic out-comes which may include hyperglycemia hepatic injury due to excessive lipogenesis from overfeeding andor intravenous lipid delivery and excessive CO2 production as-sociated with overfeeding is also an ap-propriate goal for nutrition support in the critically ill population regardless of weight status37
For critically ill patients who are obese goals of nutrition support may include reduc-tion of fat mass with simultaneous preserva-tion of lean tissue15 Early enteral nutrition may be advantageous in promoting desired goals Enteral nutrition is recommended as the preferred feeding route whenever possi-ble However in the presence of contraindi-cations to enteral feeding parenteral nutri-tion may be used as the method of nutrient delivery4243
Nutrition assessment
Sedation and mechanical ventilation com-mon in the critical care setting may present barriers to history taking if the patient is unaccompanied by persons who can pro-vide information Consensus guidelines rec-ommend that all bariatric patients carry with them a written description of their surgery and its resultant GI anatomy15
Information regarding the magnitude and rate of the patientrsquos resultant weight loss should be gathered if possible15 In assessing
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 99
The postbariatric population is likely to present with obesity However for some patients with a distant history of bariatric surgery body mass index may be normal A subset of postbariatric patients may be underweight andor have developed malnu-trition For all patients with a history of bariatric surgery altered GI anatomy must be considered when providing nutritional care Bariatric surgery patients who have under-gone malabsorptive procedures retain a risk for nutrient deficiencies that may become severe Many of the long-term metabolic hormonal and physical effects of bariatric surgery remain unknown although long-term data are accumulating The purpose of this re-view is to provide an overview of bariatric surgical procedures to discuss sequelae of altered GI anatomy and to evaluate current evidence for critically ill patients who have undergone bariatric surgery
SEARCH STRATEGY
The search of databases included PubMed and CINAHL Inclusion criteria included ran-domized controlled trials clinical trials obser-vational studies descriptive studies system-atic reviews and meta-analyses published in English within the past 10 years however older studies were considered if deemed rel-evant to the review The population included adults 19 years of age or older with a distant or recent history of bariatric surgery Care set-tings were critical care and home care The nutrition intervention studied was nutrition support A total of 126 articles were identified initially through database searches Following a review of article abstracts 8 articles were found to address the topic directly One ad-ditional article was identified by a reviewer recommendation
While literature is available regarding com-plications of bariatric surgery and the criti-cally ill patient with obesity little research is focused on critical illness in patients with a distant or recent history of bariatric surgery No randomized controlled trials were located
that addressed this topic The identified ar-ticles include 1 retrospective cohort study 1 descriptive study 2 consensus documents and 5 narrative reviews Although this review is narrative every effort was made to select studies that reflect the current state of knowl-edge regarding the topic Table 1 lists studies identified via the literature search
BARIATRIC SURGERY UPDATE
Bariatric surgical procedures fall into 3 ma-jor categories (1) malabsorptive (2) restric-tive and (3) combination that is both re-strictive and malabsorptive3 Most bariatric surgical procedures are not considered exper-imental the history of GI surgery for the pur-poses of promoting weight loss now stretches back nearly 60 years4 Bariatric surgery is sup-ported by an increasing amount of long-term data regarding effectiveness and safety56
During the past decade efforts have increased to accumulate data for the purpose of defin-ing evidence-based guidelines and best clini-cal practices in bariatric surgery The Bariatric Outcomes Longitudinal Database is a propri-etary database that has existed since 2007 Es-tablished by the Surgical Review Corporation the Bariatric Outcomes Longitudinal Database currently houses data for more than 500 000 bariatric surgery patients worldwide7 The Bariatric Outcomes Longitudinal Database is used to establish quality benchmarks for bariatric surgical procedures and to establish standards by which surgical centers may be designated Bariatric Centers of Excellence8
Four bariatric surgical methods are illus-trated in the Figure9 Worldwide the most common bariatric surgery is the laparoscop-ically placed adjustable gastric band (AGB) (see the Figure) A purely restrictive pro-cedure the AGB induces weight loss by limiting the size of the gastric pouch and thus reducing the amount of food that can be consumed3 The stomach and the lower GI tract remain intact and the pathway of food through the digestive system remains un-changed Repeated operations are common
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Tab
le 1
N
utr
itio
n S
up
po
rt P
ost
ndashBar
iatr
ic S
urg
ery
Tab
le o
f St
ud
ies
Iden
tifi
ed V
ia
Lite
ratu
re S
earc
h
Ty
pe
of
Stu
dy
M
eth
od
s C
on
clu
sio
ns
Ch
ob
an e
t al
49
Co
nse
nsu
s gu
idel
ines
Sy
stem
atic
rev
iew
of
Pro
vid
es g
uid
elin
es o
n t
he
bas
is o
f ava
ilab
le e
vid
ence
fo
r n
utr
itio
n c
are
evid
ence
o
f h
osp
ital
ized
ad
ult
s w
ith
ob
esit
y Fu
jioka
et
al14
N
arra
tive
rev
iew
N
A
Des
crib
es n
utr
itio
n p
rob
lem
s th
at m
ay o
ccu
r in
ho
spit
aliz
ed a
nd
cr
itic
ally
ill p
atie
nts
fo
llow
ing
bar
iatr
ic s
urg
ery
H
amilt
on
et
al63
R
etro
spec
tive
co
ho
rt
Ret
rosp
ecti
ve c
har
t H
ypo
calo
ric
TP
N m
ain
tain
ed n
utr
itio
nal
sta
tus
wh
ile p
rom
oti
ng
wei
ght
revi
ew
loss
in h
om
e ca
re p
atie
nts
wit
h c
om
plic
atio
ns
of
bar
iatr
ic s
urg
ery
K
um
pf
et a
l1 D
escr
ipti
ve
Qu
esti
on
nai
re
467
pra
ctit
ion
ers
ind
icat
ed w
idel
y va
ryin
g p
ract
ices
reg
ard
ing
the
adm
inis
tere
d t
o 4
73
pro
visi
on
of
nu
trit
ion
su
pp
ort
to
cri
tica
lly il
l m
orb
idly
ob
ese
nu
trit
ion
su
pp
ort
p
atie
nts
th
us
sup
po
rtin
g th
e n
eed
fo
r th
e d
evel
op
men
t o
f p
rofe
ssio
nal
s ev
iden
ce-b
ased
pra
ctic
e gu
idel
ines
M
arti
nd
ale
et a
l54
Nar
rati
ve r
evie
w
NA
P
rovi
des
su
gges
tio
ns
for
futu
re r
esea
rch
reg
ard
ing
crit
ical
ly il
l m
orb
idly
o
bes
e p
atie
nts
M
cCla
ve e
t al
15
Co
nse
nsu
s N
A
Pro
vid
es c
on
sen
sus
reco
mm
end
atio
ns
for
the
nu
trit
ion
car
e o
f cr
itic
ally
re
com
men
dat
ion
s ill
mo
rbid
ly o
bes
e p
atie
nts
Se
gara
n37
N
arra
tive
rev
iew
N
A
Dis
cuss
es is
sues
su
rro
un
din
g th
e p
rovi
sio
n o
f n
utr
itio
n s
up
po
rt t
o
ob
ese
cri
tica
lly il
l pat
ien
ts e
xp
erie
nci
ng
com
plic
atio
ns
follo
win
g b
aria
tric
su
rger
y
Shah
22
Nar
rati
ve r
evie
w
NA
D
iscu
sses
th
e p
rovi
sio
n o
f n
utr
ien
ts t
o p
atie
nts
wh
o b
eco
me
ill
po
stsu
rgic
ally
des
crib
es t
he
pro
visi
on
of
nu
trie
nts
th
rou
gh t
he
rem
nan
t st
om
ach
Z
iegl
er e
t al
62
Nar
rati
ve r
evie
w
NA
P
rovi
des
up
dat
e o
n lo
ng-
term
fo
llow
-up
of
nu
trit
ion
issu
es in
p
ost
ndashbar
iatr
ic p
atie
nts
100 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Ab
bre
viat
ion
s N
A n
ot
app
licab
le T
PN
to
tal p
aren
tera
l nu
trit
ion
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 101
Figure Altered gastrointestinal anatomy resulting from 4 methods of bariatric surgery Image courtesy of Walter Pories MD Reprinted with permission
since the gastric band may become dis-placed or eroded Typical weight losses re-sulting from successful AGB procedures aver-age about 35 of excess weight although a long-term failure rate of nearly 50 has been noted3 Failure may be related to band-related complications or to consumption of amounts of food andor nutrient-dense liquids large enough to stretch the stomach pouch
Popularly known as the ldquogastric bypassrdquo the Roux-en-Y surgery is the most common bariatric procedure used in the United States (see the Figure) In this combination pro-cedure the proximal and distal portions of the stomach are surgically separated and a stomach pouch of about 30 mL in volume is created10 A loop of the jejunum (the ldquoRoux limbrdquo) is attached to the stomach pouch and the biliopancreatic limb is attached to the Roux limb about 75 to 150 cm from the anas-tomosis of the stomach pouch and jejunum The portion of intestine remaining below the anastomosis created below the Roux junction is called the ldquocommon channelrdquo Weight loss is induced both by the reduced size of the stomach pouch and by the malabsorption re-
sulting from the intestinal resection356 Long-term results have been described as 49 to 62 excess weight loss maintained over 5 to 14 years in about 85 of patients35 Postsurgi-cal complications such as dumping syndrome and macro- and micronutrient deficiencies are common occurring in an estimated 70 of Roux-en-Y patients3 However in most cases these complications are manageable with the use of nutrient supplementation and nutri-tion education regarding appropriate eating practices11
ldquoGastric sleeverdquo surgery has gained popu-larity in recent years Gastric sleeve surgery is purely restrictive and involves removal of a substantial portion of the stomach leaving a greatly reduced pouch (the ldquosleeverdquo) for digestive purposes (see the Figure) Gastric sleeve surgery may be used as part of a surgical sequence for high-risk patients patients may receive the sleeve to promote initial weight loss and then receive a gastric bypass at a later time upon improvement of risk factors12
Short-term data indicate that the gastric sleeve surgery may provide greater weight loss results and fewer complications than the AGB
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
102 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
however unlike gastric banding the gastric sleeve surgery is not reversible Compared with the Roux-en-Y gastric bypass surgical complication rates are similar and there are fewer serious nutritional complications51314
The biliopancreatic diversion with duode-nal switch is a combination surgery that be-came popular in the 1990s and then quickly fell from favor (see the Figure) Although the surgery results in slightly greater weight loss than the Roux-en-Y bypass high rates of severe macro- and micronutrient deficien-cies surgical complications and deaths have prompted many bariatric surgeons to aban-don the procedure61516 Patients who have undergone biliopancreatic diversion with duodenal switch however may present with critical illness thus the clinician should be familiar with the anatomical alterations asso-ciated with the surgery
At the current time little is known regard-ing the long-term consequences of substan-tially altered GI anatomy and chronic malab-sorption of nutrients15 Data have indicated reductions in long-term mortality in patients receiving both gastric banding and gastric by-pass surgical procedures17 Short-term com-plication rates and weight loss results appear to be influenced by the skill of the bariatric surgeon with the best results obtained by surgeons and facilities performing high vol-umes of bariatric surgical procedures31618
As long-term data continue to accumulate it is expected that knowledge will increase re-garding outcomes of bariatric surgery over the life span
POSTOPERATIVE COMPLICATIONS OF BARIATRIC SURGERY
Nutrition-related
Common nutrition complications of bariat-ric surgery include both macro- and micronu-trient deficiencies The overall nutrition-related complication rate for patients under-going bariatric surgery appears to be about 30 with numbers substantially higher for malabsorptive surgical procedures19 Nutri-
tion complications may occur because of al-terations in the size and length of the stomach and the intestines reduction of surface area for nutrient absorption reduced numbers of metabolites necessary for nutrient absorption such as intrinsic factor or gastric acid andor alterations in dietary consumption patterns
Macronutrient deficiencies
Little is known regarding long-term pat-terns of dietary consumption following bariatric surgery20 However it seems appar-ent that a substantial decrease in total con-sumption of macronutrients occurs whether or not percentage intake of macronutrients is altered following surgery A systematic re-view of dietary intake following AGB surgery found that although proportional protein in-take as part of total dietary intake is main-tained or slightly increased total protein con-sumption in grams is decreased20 The same review reported the likelihood of a moder-ate decrease in percent fat intake and a con-current increase in percent carbohydrate in-take among the same population20 Moize et al21 studied a cohort of patients who had undergone either sleeve gastrectomy or Roux-en-Y gastric bypass and found no long-term changes in percent macronutrient intake for either group It should be noted that the pop-ulation was Spanish and macronutrient pro-portions were compared with those identi-fied for the general Spanish population21 The cohortrsquos total nutrient intake decreased sig-nificantly with total energy intake but not macronutrient distribution predicting percent weight loss21 Analysis of typical food con-sumption patterns is an important component of a complete nutrition assessment for post-bariatric patients although this information may be difficult to obtain in the critical care setting
Protein deficiency is the most com-mon macronutrient deficit following bariatric surgery and if severe can result in a diag-nosis of protein-energy malnutrition1922 Pos-sible causes of protein-energy malnutrition include reduced oral intake andor surgical complications resulting in too much or too
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 103
rapid weight loss The small stomach pouch remaining after a gastric resection may pro-duce insufficient stomach acid to promote normal protein digestion22 Enteral nutrition or reversal of the surgery may be required in
1922 extreme cases Bariatric surgery can result in fat malab-
sorption with resultant steatorrhea and other metabolic complications2324 One study of 9 patients before and after Roux-en-Y gastric by-pass surgery found a significant reduction in fat absorption (P lt 001) following bariatric surgery but no differences in fecal fat excre-tion pre- and postsurgery24 The degree of fat malabsorption in Roux-en-Y patients appears to be associated with the length of the com-mon channel below the anastomosis of the biliopancreatic and Roux limbs According to Fujioka et al19 a common channel length of 100 cm appears to be well tolerated in terms of postsurgical fat absorption capabilities If fat malabsorption is severe patients under-going bariatric surgery may develop essential fatty acid deficiency requiring parenteral ad-ministration of lipids or even reversal of the
19surgery Improvements in carbohydrate metabol-
ism including resolution of symptoms of di-abetes have been associated with bariatric surgery25 Similar improvements in β -cell function and insulin sensitivity have occurred in both gastric bypass and AGB patients suggesting that substantial weight loss is largely responsible for positive metabolic outcomes26 Odstrcil et al24 and Hammer and Hammer27 reported that indicators of carbo-hydrate absorption remained unchanged in a group of obese patients examined before and after Roux-en-Y gastric bypass surgery Prob-lems with carbohydrate-associated energy de-ficiency following surgery may be related to medical or surgical complications that pre-clude ingestion of adequate albeit reduced amounts of carbohydrates
Micronutrient deficiencies
Micronutrient deficiencies following bariat-ric surgery can exacerbate or complicate the course of critical illness15 Micronutrient
deficiencies may be related to the length of absorptive surface area remaining after surgery22 Depending on the specific portions of the digestive and absorptive surface areas that have been bypassed or reduced a variety of macro- or micronutrient deficiencies may occur
Moizacute found that dietary intake of e et al21
calcium magnesium phosphorus and iron did not meet recommendations in a cohort of postndashsleeve gastrectomy and postndashRoux-en-Y gastric bypass patients Other investigators have reported micronutrient deficiencies in-cluding the water-soluble vitamins thiamine B12 folate and C as well as the fat-soluble vita-mins D A and K28 Commonly reported min-eral deficiencies include iron zinc calcium and copper2829 however altered digestion and absorption of virtually any micronutrient may occur following surgery Physical and bio-chemical findings may indicate the presence of micronutrient deficiencies in postbariatric patients Investigators have described a vari-ety of nutritional aberrations including zinc deficiency associated with acrodermatitis30
iron deficiency associated with anemia31 and vitamin A deficiency associated with low serum prealbumin32 The mechanism underly-ing vitamin A deficiency and reduced levels of serum proteins such as prealbumin in bariatric patients remains poorly understood Explana-tions proposed have included reduced food intake reduced absorptive surface area in the small intestine and effects associated with prealbuminrsquos role as a transporter of retinol-binding protein32
Moize et al21 found 25-hydroxy vitamin D deficiency to be the most common micronu-trient deficiency within a study group of more than 300 postndashbariatric surgery patients Sim-ilar to several other micronutrients the pre-cise location where vitamin D is absorbed in the intestine remains unknown making the prediction of specific deficiencies in particu-lar patients difficult29 Thus patients with a history of bariatric surgery should be mon-itored at regular intervals for overall nutri-tional status including micronutrient status28
The possibility of atypical micronutrient
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
104 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
deficiencies should not be dismissed when performing nutrition assessment in the postndash bariatric surgery population
Dumping syndrome
Dumping syndrome is the most com-mon nutrition-related problem experienced by Roux-en-Y gastric bypass patients with ap-proximately 50 to 70 of patients experienc-ing this symptom22 The Roux-en-Y procedure promotes dumping syndrome by allowing for very rapid infusion of the reduced stomachrsquos contents into the jejunum with subsequent forceful osmotic effects33 During a dumping episode a quick fluid shift occurs between the intravascular space and the lumen of the intestine34 The early phase of dumping may include abdominal pain nausea cramping and diarrhea The late phase encompasses the effects of resultant hypoglycemia and may in-clude sweating palpitations weakness trem-bling and even syncope34
Avoidance of foods such as simple carbo-hydrates which may precipitate dumping may be associated with weight loss However Shah22 and Banerjee et al33 recently reported that long-term weight loss following a Roux-en-Y procedure is associated with reduced food intake rather than with dumping syn-drome Dumping syndrome in severe cases may serve as an etiological factor in identified macro- and micronutrient deficiencies or protein-energy malnutrition Dumping syn-drome can usually be managed effectively by providing appropriate nutrition education to bariatric surgical patients35 While dumping symptoms tend to lessen with the passage of time refractory dumping symptoms may require medical or surgical intervention Medical treatments may include the use of somatostatin analogs such as octreotide which has been demonstrated to be effec-tive in ameliorating dumping symptoms34
Surgical treatment may include anatomical revisions designed to slow down the speed of gastric emptying34 For patients who have received a Roux-en-Y procedure insertion of an additional length of jejunum between the stomach and the jejunal anastomosis may
relieve dumping symptoms34 Enteral feeding into the jejunum may be required if dumping symptoms cannot be resolved34
Nausea and vomiting
Nausea and vomiting in post-bariatric surgery patients may be associated with con-sumption of portions too large for the reduced gastric pouch or by the simultaneous con-sumption of solids and liquids Nausea and vomiting in the postbariatric surgery patient requires medical follow-up and further inves-tigation since this symptom may result from strictures or GI obstruction10 The majority of cases of nausea and vomiting can be resolved with appropriate nutrition education35
Mechanical causes of nausea and vomiting may require surgical treatment Although un-common in the critical care setting preg-nancy can be a cause of nausea and vomiting Postndashbariatric surgical patients who are preg-nant should be carefully monitored for nutri-ent deficiencies and supplemented as needed on an individual basis36
Surgery-related
Surgical complications appear in approxi-mately 10 to 16 of Roux-en-Y gastric by-pass patients2237 Correction of surgical com-plications often requires additional surgery and such patients may require care in an ICU for some period of time during their clinical course Until the complications are resolved patients may require nutrition support since intake of nutrients by the oral route may be contraindicated Surgical complications can include but are not limited to anastomotic leaks wound infections anastomotic stric-tures and incisional hernias
The most common surgical complication is the anastomotic leak affecting 2 to 5 of Roux-en-Y bypass patients137 Leaks occur most commonly at the gastrojejunal anasto-mosis with leaks also occurring at the je-junojejunostomy site or at the gastric sta-ple line3738 More severely obese patients tend to experience an increased number of complications39 In a prospective descrip-tive study of 3018 Roux-en-Y gastric bypass
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 105
patients Gonzalez et al38 found that 63 pa-tients developed anastomotic leaks Among these patients 58 reoperations were required with duration of nutrition support lasting from 2 to 12 weeks3738 Thirty percent of these patients were receiving some type of nutrition support at hospital discharge3738
Anastomotic strictures represent a com-mon surgical complication of bariatric surgery In many cases strictures can be cor-rected via single or repeated endoscopic di-latation procedures40 Some strictures require further surgery to achieve resolution40
NUTRITION SUPPORT OF CRITICALLY ILL POSTndashBARIATRIC SURGERY PATIENTS
Several authors have noted a dearth of research and thus a lack of evidence-based guidelines regarding nutrition sup-port for critically ill postndashbariatric surgery patients15223741 Little is known regarding nutrition assessment issues in this population Published definitions of hypocaloric high-protein feeding are not consistent and the degree to which weight status interacts with the effects of altered GI anatomy in critical illness is poorly understood
At the present time resources available to practitioners caring for such patients include a limited amount of literature consensus guide-lines for obese patients and clinical judgment For patients with a recent history of bariatric surgery some literature is available regarding treatment of various complications including nutrient deficiencies and nutrition impact se-quelae such as dumping syndrome
Nutrition support approaches will vary on the basis of the patientrsquos current weight status Although a large number of post-bariatric patients will present with obesity patients may be underweight overweight or normal weight Morbid obesity may be fully or partially resolved in individual patients and malnutrition may vary in degree and type Nutrition support professionals must be prepared to provide individualized care
to postndashbariatric surgical patients on the basis of each patientrsquos particular situation and clinical judgment based on practitioner experience assumes increased importance
Goals of nutrition support
According to the American Society for Parenteral and Enteral NutritionSociety of Critical Care Medicine (ASPENSCCM) guide-lines (McClave et al42) the goals for nutri-tion support in critically ill obese patients differ little from goals for normal weight pa-tients promotion of healing by modulating the stress response prevention of oxidative cell injury and optimization of the immune response42 Avoidance of poor metabolic out-comes which may include hyperglycemia hepatic injury due to excessive lipogenesis from overfeeding andor intravenous lipid delivery and excessive CO2 production as-sociated with overfeeding is also an ap-propriate goal for nutrition support in the critically ill population regardless of weight status37
For critically ill patients who are obese goals of nutrition support may include reduc-tion of fat mass with simultaneous preserva-tion of lean tissue15 Early enteral nutrition may be advantageous in promoting desired goals Enteral nutrition is recommended as the preferred feeding route whenever possi-ble However in the presence of contraindi-cations to enteral feeding parenteral nutri-tion may be used as the method of nutrient delivery4243
Nutrition assessment
Sedation and mechanical ventilation com-mon in the critical care setting may present barriers to history taking if the patient is unaccompanied by persons who can pro-vide information Consensus guidelines rec-ommend that all bariatric patients carry with them a written description of their surgery and its resultant GI anatomy15
Information regarding the magnitude and rate of the patientrsquos resultant weight loss should be gathered if possible15 In assessing
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

Tab
le 1
N
utr
itio
n S
up
po
rt P
ost
ndashBar
iatr
ic S
urg
ery
Tab
le o
f St
ud
ies
Iden
tifi
ed V
ia
Lite
ratu
re S
earc
h
Ty
pe
of
Stu
dy
M
eth
od
s C
on
clu
sio
ns
Ch
ob
an e
t al
49
Co
nse
nsu
s gu
idel
ines
Sy
stem
atic
rev
iew
of
Pro
vid
es g
uid
elin
es o
n t
he
bas
is o
f ava
ilab
le e
vid
ence
fo
r n
utr
itio
n c
are
evid
ence
o
f h
osp
ital
ized
ad
ult
s w
ith
ob
esit
y Fu
jioka
et
al14
N
arra
tive
rev
iew
N
A
Des
crib
es n
utr
itio
n p
rob
lem
s th
at m
ay o
ccu
r in
ho
spit
aliz
ed a
nd
cr
itic
ally
ill p
atie
nts
fo
llow
ing
bar
iatr
ic s
urg
ery
H
amilt
on
et
al63
R
etro
spec
tive
co
ho
rt
Ret
rosp
ecti
ve c
har
t H
ypo
calo
ric
TP
N m
ain
tain
ed n
utr
itio
nal
sta
tus
wh
ile p
rom
oti
ng
wei
ght
revi
ew
loss
in h
om
e ca
re p
atie
nts
wit
h c
om
plic
atio
ns
of
bar
iatr
ic s
urg
ery
K
um
pf
et a
l1 D
escr
ipti
ve
Qu
esti
on
nai
re
467
pra
ctit
ion
ers
ind
icat
ed w
idel
y va
ryin
g p
ract
ices
reg
ard
ing
the
adm
inis
tere
d t
o 4
73
pro
visi
on
of
nu
trit
ion
su
pp
ort
to
cri
tica
lly il
l m
orb
idly
ob
ese
nu
trit
ion
su
pp
ort
p
atie
nts
th
us
sup
po
rtin
g th
e n
eed
fo
r th
e d
evel
op
men
t o
f p
rofe
ssio
nal
s ev
iden
ce-b
ased
pra
ctic
e gu
idel
ines
M
arti
nd
ale
et a
l54
Nar
rati
ve r
evie
w
NA
P
rovi
des
su
gges
tio
ns
for
futu
re r
esea
rch
reg
ard
ing
crit
ical
ly il
l m
orb
idly
o
bes
e p
atie
nts
M
cCla
ve e
t al
15
Co
nse
nsu
s N
A
Pro
vid
es c
on
sen
sus
reco
mm
end
atio
ns
for
the
nu
trit
ion
car
e o
f cr
itic
ally
re
com
men
dat
ion
s ill
mo
rbid
ly o
bes
e p
atie
nts
Se
gara
n37
N
arra
tive
rev
iew
N
A
Dis
cuss
es is
sues
su
rro
un
din
g th
e p
rovi
sio
n o
f n
utr
itio
n s
up
po
rt t
o
ob
ese
cri
tica
lly il
l pat
ien
ts e
xp
erie
nci
ng
com
plic
atio
ns
follo
win
g b
aria
tric
su
rger
y
Shah
22
Nar
rati
ve r
evie
w
NA
D
iscu
sses
th
e p
rovi
sio
n o
f n
utr
ien
ts t
o p
atie
nts
wh
o b
eco
me
ill
po
stsu
rgic
ally
des
crib
es t
he
pro
visi
on
of
nu
trie
nts
th
rou
gh t
he
rem
nan
t st
om
ach
Z
iegl
er e
t al
62
Nar
rati
ve r
evie
w
NA
P
rovi
des
up
dat
e o
n lo
ng-
term
fo
llow
-up
of
nu
trit
ion
issu
es in
p
ost
ndashbar
iatr
ic p
atie
nts
100 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Ab
bre
viat
ion
s N
A n
ot
app
licab
le T
PN
to
tal p
aren
tera
l nu
trit
ion
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 101
Figure Altered gastrointestinal anatomy resulting from 4 methods of bariatric surgery Image courtesy of Walter Pories MD Reprinted with permission
since the gastric band may become dis-placed or eroded Typical weight losses re-sulting from successful AGB procedures aver-age about 35 of excess weight although a long-term failure rate of nearly 50 has been noted3 Failure may be related to band-related complications or to consumption of amounts of food andor nutrient-dense liquids large enough to stretch the stomach pouch
Popularly known as the ldquogastric bypassrdquo the Roux-en-Y surgery is the most common bariatric procedure used in the United States (see the Figure) In this combination pro-cedure the proximal and distal portions of the stomach are surgically separated and a stomach pouch of about 30 mL in volume is created10 A loop of the jejunum (the ldquoRoux limbrdquo) is attached to the stomach pouch and the biliopancreatic limb is attached to the Roux limb about 75 to 150 cm from the anas-tomosis of the stomach pouch and jejunum The portion of intestine remaining below the anastomosis created below the Roux junction is called the ldquocommon channelrdquo Weight loss is induced both by the reduced size of the stomach pouch and by the malabsorption re-
sulting from the intestinal resection356 Long-term results have been described as 49 to 62 excess weight loss maintained over 5 to 14 years in about 85 of patients35 Postsurgi-cal complications such as dumping syndrome and macro- and micronutrient deficiencies are common occurring in an estimated 70 of Roux-en-Y patients3 However in most cases these complications are manageable with the use of nutrient supplementation and nutri-tion education regarding appropriate eating practices11
ldquoGastric sleeverdquo surgery has gained popu-larity in recent years Gastric sleeve surgery is purely restrictive and involves removal of a substantial portion of the stomach leaving a greatly reduced pouch (the ldquosleeverdquo) for digestive purposes (see the Figure) Gastric sleeve surgery may be used as part of a surgical sequence for high-risk patients patients may receive the sleeve to promote initial weight loss and then receive a gastric bypass at a later time upon improvement of risk factors12
Short-term data indicate that the gastric sleeve surgery may provide greater weight loss results and fewer complications than the AGB
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
102 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
however unlike gastric banding the gastric sleeve surgery is not reversible Compared with the Roux-en-Y gastric bypass surgical complication rates are similar and there are fewer serious nutritional complications51314
The biliopancreatic diversion with duode-nal switch is a combination surgery that be-came popular in the 1990s and then quickly fell from favor (see the Figure) Although the surgery results in slightly greater weight loss than the Roux-en-Y bypass high rates of severe macro- and micronutrient deficien-cies surgical complications and deaths have prompted many bariatric surgeons to aban-don the procedure61516 Patients who have undergone biliopancreatic diversion with duodenal switch however may present with critical illness thus the clinician should be familiar with the anatomical alterations asso-ciated with the surgery
At the current time little is known regard-ing the long-term consequences of substan-tially altered GI anatomy and chronic malab-sorption of nutrients15 Data have indicated reductions in long-term mortality in patients receiving both gastric banding and gastric by-pass surgical procedures17 Short-term com-plication rates and weight loss results appear to be influenced by the skill of the bariatric surgeon with the best results obtained by surgeons and facilities performing high vol-umes of bariatric surgical procedures31618
As long-term data continue to accumulate it is expected that knowledge will increase re-garding outcomes of bariatric surgery over the life span
POSTOPERATIVE COMPLICATIONS OF BARIATRIC SURGERY
Nutrition-related
Common nutrition complications of bariat-ric surgery include both macro- and micronu-trient deficiencies The overall nutrition-related complication rate for patients under-going bariatric surgery appears to be about 30 with numbers substantially higher for malabsorptive surgical procedures19 Nutri-
tion complications may occur because of al-terations in the size and length of the stomach and the intestines reduction of surface area for nutrient absorption reduced numbers of metabolites necessary for nutrient absorption such as intrinsic factor or gastric acid andor alterations in dietary consumption patterns
Macronutrient deficiencies
Little is known regarding long-term pat-terns of dietary consumption following bariatric surgery20 However it seems appar-ent that a substantial decrease in total con-sumption of macronutrients occurs whether or not percentage intake of macronutrients is altered following surgery A systematic re-view of dietary intake following AGB surgery found that although proportional protein in-take as part of total dietary intake is main-tained or slightly increased total protein con-sumption in grams is decreased20 The same review reported the likelihood of a moder-ate decrease in percent fat intake and a con-current increase in percent carbohydrate in-take among the same population20 Moize et al21 studied a cohort of patients who had undergone either sleeve gastrectomy or Roux-en-Y gastric bypass and found no long-term changes in percent macronutrient intake for either group It should be noted that the pop-ulation was Spanish and macronutrient pro-portions were compared with those identi-fied for the general Spanish population21 The cohortrsquos total nutrient intake decreased sig-nificantly with total energy intake but not macronutrient distribution predicting percent weight loss21 Analysis of typical food con-sumption patterns is an important component of a complete nutrition assessment for post-bariatric patients although this information may be difficult to obtain in the critical care setting
Protein deficiency is the most com-mon macronutrient deficit following bariatric surgery and if severe can result in a diag-nosis of protein-energy malnutrition1922 Pos-sible causes of protein-energy malnutrition include reduced oral intake andor surgical complications resulting in too much or too
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 103
rapid weight loss The small stomach pouch remaining after a gastric resection may pro-duce insufficient stomach acid to promote normal protein digestion22 Enteral nutrition or reversal of the surgery may be required in
1922 extreme cases Bariatric surgery can result in fat malab-
sorption with resultant steatorrhea and other metabolic complications2324 One study of 9 patients before and after Roux-en-Y gastric by-pass surgery found a significant reduction in fat absorption (P lt 001) following bariatric surgery but no differences in fecal fat excre-tion pre- and postsurgery24 The degree of fat malabsorption in Roux-en-Y patients appears to be associated with the length of the com-mon channel below the anastomosis of the biliopancreatic and Roux limbs According to Fujioka et al19 a common channel length of 100 cm appears to be well tolerated in terms of postsurgical fat absorption capabilities If fat malabsorption is severe patients under-going bariatric surgery may develop essential fatty acid deficiency requiring parenteral ad-ministration of lipids or even reversal of the
19surgery Improvements in carbohydrate metabol-
ism including resolution of symptoms of di-abetes have been associated with bariatric surgery25 Similar improvements in β -cell function and insulin sensitivity have occurred in both gastric bypass and AGB patients suggesting that substantial weight loss is largely responsible for positive metabolic outcomes26 Odstrcil et al24 and Hammer and Hammer27 reported that indicators of carbo-hydrate absorption remained unchanged in a group of obese patients examined before and after Roux-en-Y gastric bypass surgery Prob-lems with carbohydrate-associated energy de-ficiency following surgery may be related to medical or surgical complications that pre-clude ingestion of adequate albeit reduced amounts of carbohydrates
Micronutrient deficiencies
Micronutrient deficiencies following bariat-ric surgery can exacerbate or complicate the course of critical illness15 Micronutrient
deficiencies may be related to the length of absorptive surface area remaining after surgery22 Depending on the specific portions of the digestive and absorptive surface areas that have been bypassed or reduced a variety of macro- or micronutrient deficiencies may occur
Moizacute found that dietary intake of e et al21
calcium magnesium phosphorus and iron did not meet recommendations in a cohort of postndashsleeve gastrectomy and postndashRoux-en-Y gastric bypass patients Other investigators have reported micronutrient deficiencies in-cluding the water-soluble vitamins thiamine B12 folate and C as well as the fat-soluble vita-mins D A and K28 Commonly reported min-eral deficiencies include iron zinc calcium and copper2829 however altered digestion and absorption of virtually any micronutrient may occur following surgery Physical and bio-chemical findings may indicate the presence of micronutrient deficiencies in postbariatric patients Investigators have described a vari-ety of nutritional aberrations including zinc deficiency associated with acrodermatitis30
iron deficiency associated with anemia31 and vitamin A deficiency associated with low serum prealbumin32 The mechanism underly-ing vitamin A deficiency and reduced levels of serum proteins such as prealbumin in bariatric patients remains poorly understood Explana-tions proposed have included reduced food intake reduced absorptive surface area in the small intestine and effects associated with prealbuminrsquos role as a transporter of retinol-binding protein32
Moize et al21 found 25-hydroxy vitamin D deficiency to be the most common micronu-trient deficiency within a study group of more than 300 postndashbariatric surgery patients Sim-ilar to several other micronutrients the pre-cise location where vitamin D is absorbed in the intestine remains unknown making the prediction of specific deficiencies in particu-lar patients difficult29 Thus patients with a history of bariatric surgery should be mon-itored at regular intervals for overall nutri-tional status including micronutrient status28
The possibility of atypical micronutrient
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
104 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
deficiencies should not be dismissed when performing nutrition assessment in the postndash bariatric surgery population
Dumping syndrome
Dumping syndrome is the most com-mon nutrition-related problem experienced by Roux-en-Y gastric bypass patients with ap-proximately 50 to 70 of patients experienc-ing this symptom22 The Roux-en-Y procedure promotes dumping syndrome by allowing for very rapid infusion of the reduced stomachrsquos contents into the jejunum with subsequent forceful osmotic effects33 During a dumping episode a quick fluid shift occurs between the intravascular space and the lumen of the intestine34 The early phase of dumping may include abdominal pain nausea cramping and diarrhea The late phase encompasses the effects of resultant hypoglycemia and may in-clude sweating palpitations weakness trem-bling and even syncope34
Avoidance of foods such as simple carbo-hydrates which may precipitate dumping may be associated with weight loss However Shah22 and Banerjee et al33 recently reported that long-term weight loss following a Roux-en-Y procedure is associated with reduced food intake rather than with dumping syn-drome Dumping syndrome in severe cases may serve as an etiological factor in identified macro- and micronutrient deficiencies or protein-energy malnutrition Dumping syn-drome can usually be managed effectively by providing appropriate nutrition education to bariatric surgical patients35 While dumping symptoms tend to lessen with the passage of time refractory dumping symptoms may require medical or surgical intervention Medical treatments may include the use of somatostatin analogs such as octreotide which has been demonstrated to be effec-tive in ameliorating dumping symptoms34
Surgical treatment may include anatomical revisions designed to slow down the speed of gastric emptying34 For patients who have received a Roux-en-Y procedure insertion of an additional length of jejunum between the stomach and the jejunal anastomosis may
relieve dumping symptoms34 Enteral feeding into the jejunum may be required if dumping symptoms cannot be resolved34
Nausea and vomiting
Nausea and vomiting in post-bariatric surgery patients may be associated with con-sumption of portions too large for the reduced gastric pouch or by the simultaneous con-sumption of solids and liquids Nausea and vomiting in the postbariatric surgery patient requires medical follow-up and further inves-tigation since this symptom may result from strictures or GI obstruction10 The majority of cases of nausea and vomiting can be resolved with appropriate nutrition education35
Mechanical causes of nausea and vomiting may require surgical treatment Although un-common in the critical care setting preg-nancy can be a cause of nausea and vomiting Postndashbariatric surgical patients who are preg-nant should be carefully monitored for nutri-ent deficiencies and supplemented as needed on an individual basis36
Surgery-related
Surgical complications appear in approxi-mately 10 to 16 of Roux-en-Y gastric by-pass patients2237 Correction of surgical com-plications often requires additional surgery and such patients may require care in an ICU for some period of time during their clinical course Until the complications are resolved patients may require nutrition support since intake of nutrients by the oral route may be contraindicated Surgical complications can include but are not limited to anastomotic leaks wound infections anastomotic stric-tures and incisional hernias
The most common surgical complication is the anastomotic leak affecting 2 to 5 of Roux-en-Y bypass patients137 Leaks occur most commonly at the gastrojejunal anasto-mosis with leaks also occurring at the je-junojejunostomy site or at the gastric sta-ple line3738 More severely obese patients tend to experience an increased number of complications39 In a prospective descrip-tive study of 3018 Roux-en-Y gastric bypass
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 105
patients Gonzalez et al38 found that 63 pa-tients developed anastomotic leaks Among these patients 58 reoperations were required with duration of nutrition support lasting from 2 to 12 weeks3738 Thirty percent of these patients were receiving some type of nutrition support at hospital discharge3738
Anastomotic strictures represent a com-mon surgical complication of bariatric surgery In many cases strictures can be cor-rected via single or repeated endoscopic di-latation procedures40 Some strictures require further surgery to achieve resolution40
NUTRITION SUPPORT OF CRITICALLY ILL POSTndashBARIATRIC SURGERY PATIENTS
Several authors have noted a dearth of research and thus a lack of evidence-based guidelines regarding nutrition sup-port for critically ill postndashbariatric surgery patients15223741 Little is known regarding nutrition assessment issues in this population Published definitions of hypocaloric high-protein feeding are not consistent and the degree to which weight status interacts with the effects of altered GI anatomy in critical illness is poorly understood
At the present time resources available to practitioners caring for such patients include a limited amount of literature consensus guide-lines for obese patients and clinical judgment For patients with a recent history of bariatric surgery some literature is available regarding treatment of various complications including nutrient deficiencies and nutrition impact se-quelae such as dumping syndrome
Nutrition support approaches will vary on the basis of the patientrsquos current weight status Although a large number of post-bariatric patients will present with obesity patients may be underweight overweight or normal weight Morbid obesity may be fully or partially resolved in individual patients and malnutrition may vary in degree and type Nutrition support professionals must be prepared to provide individualized care
to postndashbariatric surgical patients on the basis of each patientrsquos particular situation and clinical judgment based on practitioner experience assumes increased importance
Goals of nutrition support
According to the American Society for Parenteral and Enteral NutritionSociety of Critical Care Medicine (ASPENSCCM) guide-lines (McClave et al42) the goals for nutri-tion support in critically ill obese patients differ little from goals for normal weight pa-tients promotion of healing by modulating the stress response prevention of oxidative cell injury and optimization of the immune response42 Avoidance of poor metabolic out-comes which may include hyperglycemia hepatic injury due to excessive lipogenesis from overfeeding andor intravenous lipid delivery and excessive CO2 production as-sociated with overfeeding is also an ap-propriate goal for nutrition support in the critically ill population regardless of weight status37
For critically ill patients who are obese goals of nutrition support may include reduc-tion of fat mass with simultaneous preserva-tion of lean tissue15 Early enteral nutrition may be advantageous in promoting desired goals Enteral nutrition is recommended as the preferred feeding route whenever possi-ble However in the presence of contraindi-cations to enteral feeding parenteral nutri-tion may be used as the method of nutrient delivery4243
Nutrition assessment
Sedation and mechanical ventilation com-mon in the critical care setting may present barriers to history taking if the patient is unaccompanied by persons who can pro-vide information Consensus guidelines rec-ommend that all bariatric patients carry with them a written description of their surgery and its resultant GI anatomy15
Information regarding the magnitude and rate of the patientrsquos resultant weight loss should be gathered if possible15 In assessing
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 101
Figure Altered gastrointestinal anatomy resulting from 4 methods of bariatric surgery Image courtesy of Walter Pories MD Reprinted with permission
since the gastric band may become dis-placed or eroded Typical weight losses re-sulting from successful AGB procedures aver-age about 35 of excess weight although a long-term failure rate of nearly 50 has been noted3 Failure may be related to band-related complications or to consumption of amounts of food andor nutrient-dense liquids large enough to stretch the stomach pouch
Popularly known as the ldquogastric bypassrdquo the Roux-en-Y surgery is the most common bariatric procedure used in the United States (see the Figure) In this combination pro-cedure the proximal and distal portions of the stomach are surgically separated and a stomach pouch of about 30 mL in volume is created10 A loop of the jejunum (the ldquoRoux limbrdquo) is attached to the stomach pouch and the biliopancreatic limb is attached to the Roux limb about 75 to 150 cm from the anas-tomosis of the stomach pouch and jejunum The portion of intestine remaining below the anastomosis created below the Roux junction is called the ldquocommon channelrdquo Weight loss is induced both by the reduced size of the stomach pouch and by the malabsorption re-
sulting from the intestinal resection356 Long-term results have been described as 49 to 62 excess weight loss maintained over 5 to 14 years in about 85 of patients35 Postsurgi-cal complications such as dumping syndrome and macro- and micronutrient deficiencies are common occurring in an estimated 70 of Roux-en-Y patients3 However in most cases these complications are manageable with the use of nutrient supplementation and nutri-tion education regarding appropriate eating practices11
ldquoGastric sleeverdquo surgery has gained popu-larity in recent years Gastric sleeve surgery is purely restrictive and involves removal of a substantial portion of the stomach leaving a greatly reduced pouch (the ldquosleeverdquo) for digestive purposes (see the Figure) Gastric sleeve surgery may be used as part of a surgical sequence for high-risk patients patients may receive the sleeve to promote initial weight loss and then receive a gastric bypass at a later time upon improvement of risk factors12
Short-term data indicate that the gastric sleeve surgery may provide greater weight loss results and fewer complications than the AGB
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
102 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
however unlike gastric banding the gastric sleeve surgery is not reversible Compared with the Roux-en-Y gastric bypass surgical complication rates are similar and there are fewer serious nutritional complications51314
The biliopancreatic diversion with duode-nal switch is a combination surgery that be-came popular in the 1990s and then quickly fell from favor (see the Figure) Although the surgery results in slightly greater weight loss than the Roux-en-Y bypass high rates of severe macro- and micronutrient deficien-cies surgical complications and deaths have prompted many bariatric surgeons to aban-don the procedure61516 Patients who have undergone biliopancreatic diversion with duodenal switch however may present with critical illness thus the clinician should be familiar with the anatomical alterations asso-ciated with the surgery
At the current time little is known regard-ing the long-term consequences of substan-tially altered GI anatomy and chronic malab-sorption of nutrients15 Data have indicated reductions in long-term mortality in patients receiving both gastric banding and gastric by-pass surgical procedures17 Short-term com-plication rates and weight loss results appear to be influenced by the skill of the bariatric surgeon with the best results obtained by surgeons and facilities performing high vol-umes of bariatric surgical procedures31618
As long-term data continue to accumulate it is expected that knowledge will increase re-garding outcomes of bariatric surgery over the life span
POSTOPERATIVE COMPLICATIONS OF BARIATRIC SURGERY
Nutrition-related
Common nutrition complications of bariat-ric surgery include both macro- and micronu-trient deficiencies The overall nutrition-related complication rate for patients under-going bariatric surgery appears to be about 30 with numbers substantially higher for malabsorptive surgical procedures19 Nutri-
tion complications may occur because of al-terations in the size and length of the stomach and the intestines reduction of surface area for nutrient absorption reduced numbers of metabolites necessary for nutrient absorption such as intrinsic factor or gastric acid andor alterations in dietary consumption patterns
Macronutrient deficiencies
Little is known regarding long-term pat-terns of dietary consumption following bariatric surgery20 However it seems appar-ent that a substantial decrease in total con-sumption of macronutrients occurs whether or not percentage intake of macronutrients is altered following surgery A systematic re-view of dietary intake following AGB surgery found that although proportional protein in-take as part of total dietary intake is main-tained or slightly increased total protein con-sumption in grams is decreased20 The same review reported the likelihood of a moder-ate decrease in percent fat intake and a con-current increase in percent carbohydrate in-take among the same population20 Moize et al21 studied a cohort of patients who had undergone either sleeve gastrectomy or Roux-en-Y gastric bypass and found no long-term changes in percent macronutrient intake for either group It should be noted that the pop-ulation was Spanish and macronutrient pro-portions were compared with those identi-fied for the general Spanish population21 The cohortrsquos total nutrient intake decreased sig-nificantly with total energy intake but not macronutrient distribution predicting percent weight loss21 Analysis of typical food con-sumption patterns is an important component of a complete nutrition assessment for post-bariatric patients although this information may be difficult to obtain in the critical care setting
Protein deficiency is the most com-mon macronutrient deficit following bariatric surgery and if severe can result in a diag-nosis of protein-energy malnutrition1922 Pos-sible causes of protein-energy malnutrition include reduced oral intake andor surgical complications resulting in too much or too
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 103
rapid weight loss The small stomach pouch remaining after a gastric resection may pro-duce insufficient stomach acid to promote normal protein digestion22 Enteral nutrition or reversal of the surgery may be required in
1922 extreme cases Bariatric surgery can result in fat malab-
sorption with resultant steatorrhea and other metabolic complications2324 One study of 9 patients before and after Roux-en-Y gastric by-pass surgery found a significant reduction in fat absorption (P lt 001) following bariatric surgery but no differences in fecal fat excre-tion pre- and postsurgery24 The degree of fat malabsorption in Roux-en-Y patients appears to be associated with the length of the com-mon channel below the anastomosis of the biliopancreatic and Roux limbs According to Fujioka et al19 a common channel length of 100 cm appears to be well tolerated in terms of postsurgical fat absorption capabilities If fat malabsorption is severe patients under-going bariatric surgery may develop essential fatty acid deficiency requiring parenteral ad-ministration of lipids or even reversal of the
19surgery Improvements in carbohydrate metabol-
ism including resolution of symptoms of di-abetes have been associated with bariatric surgery25 Similar improvements in β -cell function and insulin sensitivity have occurred in both gastric bypass and AGB patients suggesting that substantial weight loss is largely responsible for positive metabolic outcomes26 Odstrcil et al24 and Hammer and Hammer27 reported that indicators of carbo-hydrate absorption remained unchanged in a group of obese patients examined before and after Roux-en-Y gastric bypass surgery Prob-lems with carbohydrate-associated energy de-ficiency following surgery may be related to medical or surgical complications that pre-clude ingestion of adequate albeit reduced amounts of carbohydrates
Micronutrient deficiencies
Micronutrient deficiencies following bariat-ric surgery can exacerbate or complicate the course of critical illness15 Micronutrient
deficiencies may be related to the length of absorptive surface area remaining after surgery22 Depending on the specific portions of the digestive and absorptive surface areas that have been bypassed or reduced a variety of macro- or micronutrient deficiencies may occur
Moizacute found that dietary intake of e et al21
calcium magnesium phosphorus and iron did not meet recommendations in a cohort of postndashsleeve gastrectomy and postndashRoux-en-Y gastric bypass patients Other investigators have reported micronutrient deficiencies in-cluding the water-soluble vitamins thiamine B12 folate and C as well as the fat-soluble vita-mins D A and K28 Commonly reported min-eral deficiencies include iron zinc calcium and copper2829 however altered digestion and absorption of virtually any micronutrient may occur following surgery Physical and bio-chemical findings may indicate the presence of micronutrient deficiencies in postbariatric patients Investigators have described a vari-ety of nutritional aberrations including zinc deficiency associated with acrodermatitis30
iron deficiency associated with anemia31 and vitamin A deficiency associated with low serum prealbumin32 The mechanism underly-ing vitamin A deficiency and reduced levels of serum proteins such as prealbumin in bariatric patients remains poorly understood Explana-tions proposed have included reduced food intake reduced absorptive surface area in the small intestine and effects associated with prealbuminrsquos role as a transporter of retinol-binding protein32
Moize et al21 found 25-hydroxy vitamin D deficiency to be the most common micronu-trient deficiency within a study group of more than 300 postndashbariatric surgery patients Sim-ilar to several other micronutrients the pre-cise location where vitamin D is absorbed in the intestine remains unknown making the prediction of specific deficiencies in particu-lar patients difficult29 Thus patients with a history of bariatric surgery should be mon-itored at regular intervals for overall nutri-tional status including micronutrient status28
The possibility of atypical micronutrient
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
104 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
deficiencies should not be dismissed when performing nutrition assessment in the postndash bariatric surgery population
Dumping syndrome
Dumping syndrome is the most com-mon nutrition-related problem experienced by Roux-en-Y gastric bypass patients with ap-proximately 50 to 70 of patients experienc-ing this symptom22 The Roux-en-Y procedure promotes dumping syndrome by allowing for very rapid infusion of the reduced stomachrsquos contents into the jejunum with subsequent forceful osmotic effects33 During a dumping episode a quick fluid shift occurs between the intravascular space and the lumen of the intestine34 The early phase of dumping may include abdominal pain nausea cramping and diarrhea The late phase encompasses the effects of resultant hypoglycemia and may in-clude sweating palpitations weakness trem-bling and even syncope34
Avoidance of foods such as simple carbo-hydrates which may precipitate dumping may be associated with weight loss However Shah22 and Banerjee et al33 recently reported that long-term weight loss following a Roux-en-Y procedure is associated with reduced food intake rather than with dumping syn-drome Dumping syndrome in severe cases may serve as an etiological factor in identified macro- and micronutrient deficiencies or protein-energy malnutrition Dumping syn-drome can usually be managed effectively by providing appropriate nutrition education to bariatric surgical patients35 While dumping symptoms tend to lessen with the passage of time refractory dumping symptoms may require medical or surgical intervention Medical treatments may include the use of somatostatin analogs such as octreotide which has been demonstrated to be effec-tive in ameliorating dumping symptoms34
Surgical treatment may include anatomical revisions designed to slow down the speed of gastric emptying34 For patients who have received a Roux-en-Y procedure insertion of an additional length of jejunum between the stomach and the jejunal anastomosis may
relieve dumping symptoms34 Enteral feeding into the jejunum may be required if dumping symptoms cannot be resolved34
Nausea and vomiting
Nausea and vomiting in post-bariatric surgery patients may be associated with con-sumption of portions too large for the reduced gastric pouch or by the simultaneous con-sumption of solids and liquids Nausea and vomiting in the postbariatric surgery patient requires medical follow-up and further inves-tigation since this symptom may result from strictures or GI obstruction10 The majority of cases of nausea and vomiting can be resolved with appropriate nutrition education35
Mechanical causes of nausea and vomiting may require surgical treatment Although un-common in the critical care setting preg-nancy can be a cause of nausea and vomiting Postndashbariatric surgical patients who are preg-nant should be carefully monitored for nutri-ent deficiencies and supplemented as needed on an individual basis36
Surgery-related
Surgical complications appear in approxi-mately 10 to 16 of Roux-en-Y gastric by-pass patients2237 Correction of surgical com-plications often requires additional surgery and such patients may require care in an ICU for some period of time during their clinical course Until the complications are resolved patients may require nutrition support since intake of nutrients by the oral route may be contraindicated Surgical complications can include but are not limited to anastomotic leaks wound infections anastomotic stric-tures and incisional hernias
The most common surgical complication is the anastomotic leak affecting 2 to 5 of Roux-en-Y bypass patients137 Leaks occur most commonly at the gastrojejunal anasto-mosis with leaks also occurring at the je-junojejunostomy site or at the gastric sta-ple line3738 More severely obese patients tend to experience an increased number of complications39 In a prospective descrip-tive study of 3018 Roux-en-Y gastric bypass
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 105
patients Gonzalez et al38 found that 63 pa-tients developed anastomotic leaks Among these patients 58 reoperations were required with duration of nutrition support lasting from 2 to 12 weeks3738 Thirty percent of these patients were receiving some type of nutrition support at hospital discharge3738
Anastomotic strictures represent a com-mon surgical complication of bariatric surgery In many cases strictures can be cor-rected via single or repeated endoscopic di-latation procedures40 Some strictures require further surgery to achieve resolution40
NUTRITION SUPPORT OF CRITICALLY ILL POSTndashBARIATRIC SURGERY PATIENTS
Several authors have noted a dearth of research and thus a lack of evidence-based guidelines regarding nutrition sup-port for critically ill postndashbariatric surgery patients15223741 Little is known regarding nutrition assessment issues in this population Published definitions of hypocaloric high-protein feeding are not consistent and the degree to which weight status interacts with the effects of altered GI anatomy in critical illness is poorly understood
At the present time resources available to practitioners caring for such patients include a limited amount of literature consensus guide-lines for obese patients and clinical judgment For patients with a recent history of bariatric surgery some literature is available regarding treatment of various complications including nutrient deficiencies and nutrition impact se-quelae such as dumping syndrome
Nutrition support approaches will vary on the basis of the patientrsquos current weight status Although a large number of post-bariatric patients will present with obesity patients may be underweight overweight or normal weight Morbid obesity may be fully or partially resolved in individual patients and malnutrition may vary in degree and type Nutrition support professionals must be prepared to provide individualized care
to postndashbariatric surgical patients on the basis of each patientrsquos particular situation and clinical judgment based on practitioner experience assumes increased importance
Goals of nutrition support
According to the American Society for Parenteral and Enteral NutritionSociety of Critical Care Medicine (ASPENSCCM) guide-lines (McClave et al42) the goals for nutri-tion support in critically ill obese patients differ little from goals for normal weight pa-tients promotion of healing by modulating the stress response prevention of oxidative cell injury and optimization of the immune response42 Avoidance of poor metabolic out-comes which may include hyperglycemia hepatic injury due to excessive lipogenesis from overfeeding andor intravenous lipid delivery and excessive CO2 production as-sociated with overfeeding is also an ap-propriate goal for nutrition support in the critically ill population regardless of weight status37
For critically ill patients who are obese goals of nutrition support may include reduc-tion of fat mass with simultaneous preserva-tion of lean tissue15 Early enteral nutrition may be advantageous in promoting desired goals Enteral nutrition is recommended as the preferred feeding route whenever possi-ble However in the presence of contraindi-cations to enteral feeding parenteral nutri-tion may be used as the method of nutrient delivery4243
Nutrition assessment
Sedation and mechanical ventilation com-mon in the critical care setting may present barriers to history taking if the patient is unaccompanied by persons who can pro-vide information Consensus guidelines rec-ommend that all bariatric patients carry with them a written description of their surgery and its resultant GI anatomy15
Information regarding the magnitude and rate of the patientrsquos resultant weight loss should be gathered if possible15 In assessing
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

102 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
however unlike gastric banding the gastric sleeve surgery is not reversible Compared with the Roux-en-Y gastric bypass surgical complication rates are similar and there are fewer serious nutritional complications51314
The biliopancreatic diversion with duode-nal switch is a combination surgery that be-came popular in the 1990s and then quickly fell from favor (see the Figure) Although the surgery results in slightly greater weight loss than the Roux-en-Y bypass high rates of severe macro- and micronutrient deficien-cies surgical complications and deaths have prompted many bariatric surgeons to aban-don the procedure61516 Patients who have undergone biliopancreatic diversion with duodenal switch however may present with critical illness thus the clinician should be familiar with the anatomical alterations asso-ciated with the surgery
At the current time little is known regard-ing the long-term consequences of substan-tially altered GI anatomy and chronic malab-sorption of nutrients15 Data have indicated reductions in long-term mortality in patients receiving both gastric banding and gastric by-pass surgical procedures17 Short-term com-plication rates and weight loss results appear to be influenced by the skill of the bariatric surgeon with the best results obtained by surgeons and facilities performing high vol-umes of bariatric surgical procedures31618
As long-term data continue to accumulate it is expected that knowledge will increase re-garding outcomes of bariatric surgery over the life span
POSTOPERATIVE COMPLICATIONS OF BARIATRIC SURGERY
Nutrition-related
Common nutrition complications of bariat-ric surgery include both macro- and micronu-trient deficiencies The overall nutrition-related complication rate for patients under-going bariatric surgery appears to be about 30 with numbers substantially higher for malabsorptive surgical procedures19 Nutri-
tion complications may occur because of al-terations in the size and length of the stomach and the intestines reduction of surface area for nutrient absorption reduced numbers of metabolites necessary for nutrient absorption such as intrinsic factor or gastric acid andor alterations in dietary consumption patterns
Macronutrient deficiencies
Little is known regarding long-term pat-terns of dietary consumption following bariatric surgery20 However it seems appar-ent that a substantial decrease in total con-sumption of macronutrients occurs whether or not percentage intake of macronutrients is altered following surgery A systematic re-view of dietary intake following AGB surgery found that although proportional protein in-take as part of total dietary intake is main-tained or slightly increased total protein con-sumption in grams is decreased20 The same review reported the likelihood of a moder-ate decrease in percent fat intake and a con-current increase in percent carbohydrate in-take among the same population20 Moize et al21 studied a cohort of patients who had undergone either sleeve gastrectomy or Roux-en-Y gastric bypass and found no long-term changes in percent macronutrient intake for either group It should be noted that the pop-ulation was Spanish and macronutrient pro-portions were compared with those identi-fied for the general Spanish population21 The cohortrsquos total nutrient intake decreased sig-nificantly with total energy intake but not macronutrient distribution predicting percent weight loss21 Analysis of typical food con-sumption patterns is an important component of a complete nutrition assessment for post-bariatric patients although this information may be difficult to obtain in the critical care setting
Protein deficiency is the most com-mon macronutrient deficit following bariatric surgery and if severe can result in a diag-nosis of protein-energy malnutrition1922 Pos-sible causes of protein-energy malnutrition include reduced oral intake andor surgical complications resulting in too much or too
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 103
rapid weight loss The small stomach pouch remaining after a gastric resection may pro-duce insufficient stomach acid to promote normal protein digestion22 Enteral nutrition or reversal of the surgery may be required in
1922 extreme cases Bariatric surgery can result in fat malab-
sorption with resultant steatorrhea and other metabolic complications2324 One study of 9 patients before and after Roux-en-Y gastric by-pass surgery found a significant reduction in fat absorption (P lt 001) following bariatric surgery but no differences in fecal fat excre-tion pre- and postsurgery24 The degree of fat malabsorption in Roux-en-Y patients appears to be associated with the length of the com-mon channel below the anastomosis of the biliopancreatic and Roux limbs According to Fujioka et al19 a common channel length of 100 cm appears to be well tolerated in terms of postsurgical fat absorption capabilities If fat malabsorption is severe patients under-going bariatric surgery may develop essential fatty acid deficiency requiring parenteral ad-ministration of lipids or even reversal of the
19surgery Improvements in carbohydrate metabol-
ism including resolution of symptoms of di-abetes have been associated with bariatric surgery25 Similar improvements in β -cell function and insulin sensitivity have occurred in both gastric bypass and AGB patients suggesting that substantial weight loss is largely responsible for positive metabolic outcomes26 Odstrcil et al24 and Hammer and Hammer27 reported that indicators of carbo-hydrate absorption remained unchanged in a group of obese patients examined before and after Roux-en-Y gastric bypass surgery Prob-lems with carbohydrate-associated energy de-ficiency following surgery may be related to medical or surgical complications that pre-clude ingestion of adequate albeit reduced amounts of carbohydrates
Micronutrient deficiencies
Micronutrient deficiencies following bariat-ric surgery can exacerbate or complicate the course of critical illness15 Micronutrient
deficiencies may be related to the length of absorptive surface area remaining after surgery22 Depending on the specific portions of the digestive and absorptive surface areas that have been bypassed or reduced a variety of macro- or micronutrient deficiencies may occur
Moizacute found that dietary intake of e et al21
calcium magnesium phosphorus and iron did not meet recommendations in a cohort of postndashsleeve gastrectomy and postndashRoux-en-Y gastric bypass patients Other investigators have reported micronutrient deficiencies in-cluding the water-soluble vitamins thiamine B12 folate and C as well as the fat-soluble vita-mins D A and K28 Commonly reported min-eral deficiencies include iron zinc calcium and copper2829 however altered digestion and absorption of virtually any micronutrient may occur following surgery Physical and bio-chemical findings may indicate the presence of micronutrient deficiencies in postbariatric patients Investigators have described a vari-ety of nutritional aberrations including zinc deficiency associated with acrodermatitis30
iron deficiency associated with anemia31 and vitamin A deficiency associated with low serum prealbumin32 The mechanism underly-ing vitamin A deficiency and reduced levels of serum proteins such as prealbumin in bariatric patients remains poorly understood Explana-tions proposed have included reduced food intake reduced absorptive surface area in the small intestine and effects associated with prealbuminrsquos role as a transporter of retinol-binding protein32
Moize et al21 found 25-hydroxy vitamin D deficiency to be the most common micronu-trient deficiency within a study group of more than 300 postndashbariatric surgery patients Sim-ilar to several other micronutrients the pre-cise location where vitamin D is absorbed in the intestine remains unknown making the prediction of specific deficiencies in particu-lar patients difficult29 Thus patients with a history of bariatric surgery should be mon-itored at regular intervals for overall nutri-tional status including micronutrient status28
The possibility of atypical micronutrient
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
104 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
deficiencies should not be dismissed when performing nutrition assessment in the postndash bariatric surgery population
Dumping syndrome
Dumping syndrome is the most com-mon nutrition-related problem experienced by Roux-en-Y gastric bypass patients with ap-proximately 50 to 70 of patients experienc-ing this symptom22 The Roux-en-Y procedure promotes dumping syndrome by allowing for very rapid infusion of the reduced stomachrsquos contents into the jejunum with subsequent forceful osmotic effects33 During a dumping episode a quick fluid shift occurs between the intravascular space and the lumen of the intestine34 The early phase of dumping may include abdominal pain nausea cramping and diarrhea The late phase encompasses the effects of resultant hypoglycemia and may in-clude sweating palpitations weakness trem-bling and even syncope34
Avoidance of foods such as simple carbo-hydrates which may precipitate dumping may be associated with weight loss However Shah22 and Banerjee et al33 recently reported that long-term weight loss following a Roux-en-Y procedure is associated with reduced food intake rather than with dumping syn-drome Dumping syndrome in severe cases may serve as an etiological factor in identified macro- and micronutrient deficiencies or protein-energy malnutrition Dumping syn-drome can usually be managed effectively by providing appropriate nutrition education to bariatric surgical patients35 While dumping symptoms tend to lessen with the passage of time refractory dumping symptoms may require medical or surgical intervention Medical treatments may include the use of somatostatin analogs such as octreotide which has been demonstrated to be effec-tive in ameliorating dumping symptoms34
Surgical treatment may include anatomical revisions designed to slow down the speed of gastric emptying34 For patients who have received a Roux-en-Y procedure insertion of an additional length of jejunum between the stomach and the jejunal anastomosis may
relieve dumping symptoms34 Enteral feeding into the jejunum may be required if dumping symptoms cannot be resolved34
Nausea and vomiting
Nausea and vomiting in post-bariatric surgery patients may be associated with con-sumption of portions too large for the reduced gastric pouch or by the simultaneous con-sumption of solids and liquids Nausea and vomiting in the postbariatric surgery patient requires medical follow-up and further inves-tigation since this symptom may result from strictures or GI obstruction10 The majority of cases of nausea and vomiting can be resolved with appropriate nutrition education35
Mechanical causes of nausea and vomiting may require surgical treatment Although un-common in the critical care setting preg-nancy can be a cause of nausea and vomiting Postndashbariatric surgical patients who are preg-nant should be carefully monitored for nutri-ent deficiencies and supplemented as needed on an individual basis36
Surgery-related
Surgical complications appear in approxi-mately 10 to 16 of Roux-en-Y gastric by-pass patients2237 Correction of surgical com-plications often requires additional surgery and such patients may require care in an ICU for some period of time during their clinical course Until the complications are resolved patients may require nutrition support since intake of nutrients by the oral route may be contraindicated Surgical complications can include but are not limited to anastomotic leaks wound infections anastomotic stric-tures and incisional hernias
The most common surgical complication is the anastomotic leak affecting 2 to 5 of Roux-en-Y bypass patients137 Leaks occur most commonly at the gastrojejunal anasto-mosis with leaks also occurring at the je-junojejunostomy site or at the gastric sta-ple line3738 More severely obese patients tend to experience an increased number of complications39 In a prospective descrip-tive study of 3018 Roux-en-Y gastric bypass
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 105
patients Gonzalez et al38 found that 63 pa-tients developed anastomotic leaks Among these patients 58 reoperations were required with duration of nutrition support lasting from 2 to 12 weeks3738 Thirty percent of these patients were receiving some type of nutrition support at hospital discharge3738
Anastomotic strictures represent a com-mon surgical complication of bariatric surgery In many cases strictures can be cor-rected via single or repeated endoscopic di-latation procedures40 Some strictures require further surgery to achieve resolution40
NUTRITION SUPPORT OF CRITICALLY ILL POSTndashBARIATRIC SURGERY PATIENTS
Several authors have noted a dearth of research and thus a lack of evidence-based guidelines regarding nutrition sup-port for critically ill postndashbariatric surgery patients15223741 Little is known regarding nutrition assessment issues in this population Published definitions of hypocaloric high-protein feeding are not consistent and the degree to which weight status interacts with the effects of altered GI anatomy in critical illness is poorly understood
At the present time resources available to practitioners caring for such patients include a limited amount of literature consensus guide-lines for obese patients and clinical judgment For patients with a recent history of bariatric surgery some literature is available regarding treatment of various complications including nutrient deficiencies and nutrition impact se-quelae such as dumping syndrome
Nutrition support approaches will vary on the basis of the patientrsquos current weight status Although a large number of post-bariatric patients will present with obesity patients may be underweight overweight or normal weight Morbid obesity may be fully or partially resolved in individual patients and malnutrition may vary in degree and type Nutrition support professionals must be prepared to provide individualized care
to postndashbariatric surgical patients on the basis of each patientrsquos particular situation and clinical judgment based on practitioner experience assumes increased importance
Goals of nutrition support
According to the American Society for Parenteral and Enteral NutritionSociety of Critical Care Medicine (ASPENSCCM) guide-lines (McClave et al42) the goals for nutri-tion support in critically ill obese patients differ little from goals for normal weight pa-tients promotion of healing by modulating the stress response prevention of oxidative cell injury and optimization of the immune response42 Avoidance of poor metabolic out-comes which may include hyperglycemia hepatic injury due to excessive lipogenesis from overfeeding andor intravenous lipid delivery and excessive CO2 production as-sociated with overfeeding is also an ap-propriate goal for nutrition support in the critically ill population regardless of weight status37
For critically ill patients who are obese goals of nutrition support may include reduc-tion of fat mass with simultaneous preserva-tion of lean tissue15 Early enteral nutrition may be advantageous in promoting desired goals Enteral nutrition is recommended as the preferred feeding route whenever possi-ble However in the presence of contraindi-cations to enteral feeding parenteral nutri-tion may be used as the method of nutrient delivery4243
Nutrition assessment
Sedation and mechanical ventilation com-mon in the critical care setting may present barriers to history taking if the patient is unaccompanied by persons who can pro-vide information Consensus guidelines rec-ommend that all bariatric patients carry with them a written description of their surgery and its resultant GI anatomy15
Information regarding the magnitude and rate of the patientrsquos resultant weight loss should be gathered if possible15 In assessing
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 103
rapid weight loss The small stomach pouch remaining after a gastric resection may pro-duce insufficient stomach acid to promote normal protein digestion22 Enteral nutrition or reversal of the surgery may be required in
1922 extreme cases Bariatric surgery can result in fat malab-
sorption with resultant steatorrhea and other metabolic complications2324 One study of 9 patients before and after Roux-en-Y gastric by-pass surgery found a significant reduction in fat absorption (P lt 001) following bariatric surgery but no differences in fecal fat excre-tion pre- and postsurgery24 The degree of fat malabsorption in Roux-en-Y patients appears to be associated with the length of the com-mon channel below the anastomosis of the biliopancreatic and Roux limbs According to Fujioka et al19 a common channel length of 100 cm appears to be well tolerated in terms of postsurgical fat absorption capabilities If fat malabsorption is severe patients under-going bariatric surgery may develop essential fatty acid deficiency requiring parenteral ad-ministration of lipids or even reversal of the
19surgery Improvements in carbohydrate metabol-
ism including resolution of symptoms of di-abetes have been associated with bariatric surgery25 Similar improvements in β -cell function and insulin sensitivity have occurred in both gastric bypass and AGB patients suggesting that substantial weight loss is largely responsible for positive metabolic outcomes26 Odstrcil et al24 and Hammer and Hammer27 reported that indicators of carbo-hydrate absorption remained unchanged in a group of obese patients examined before and after Roux-en-Y gastric bypass surgery Prob-lems with carbohydrate-associated energy de-ficiency following surgery may be related to medical or surgical complications that pre-clude ingestion of adequate albeit reduced amounts of carbohydrates
Micronutrient deficiencies
Micronutrient deficiencies following bariat-ric surgery can exacerbate or complicate the course of critical illness15 Micronutrient
deficiencies may be related to the length of absorptive surface area remaining after surgery22 Depending on the specific portions of the digestive and absorptive surface areas that have been bypassed or reduced a variety of macro- or micronutrient deficiencies may occur
Moizacute found that dietary intake of e et al21
calcium magnesium phosphorus and iron did not meet recommendations in a cohort of postndashsleeve gastrectomy and postndashRoux-en-Y gastric bypass patients Other investigators have reported micronutrient deficiencies in-cluding the water-soluble vitamins thiamine B12 folate and C as well as the fat-soluble vita-mins D A and K28 Commonly reported min-eral deficiencies include iron zinc calcium and copper2829 however altered digestion and absorption of virtually any micronutrient may occur following surgery Physical and bio-chemical findings may indicate the presence of micronutrient deficiencies in postbariatric patients Investigators have described a vari-ety of nutritional aberrations including zinc deficiency associated with acrodermatitis30
iron deficiency associated with anemia31 and vitamin A deficiency associated with low serum prealbumin32 The mechanism underly-ing vitamin A deficiency and reduced levels of serum proteins such as prealbumin in bariatric patients remains poorly understood Explana-tions proposed have included reduced food intake reduced absorptive surface area in the small intestine and effects associated with prealbuminrsquos role as a transporter of retinol-binding protein32
Moize et al21 found 25-hydroxy vitamin D deficiency to be the most common micronu-trient deficiency within a study group of more than 300 postndashbariatric surgery patients Sim-ilar to several other micronutrients the pre-cise location where vitamin D is absorbed in the intestine remains unknown making the prediction of specific deficiencies in particu-lar patients difficult29 Thus patients with a history of bariatric surgery should be mon-itored at regular intervals for overall nutri-tional status including micronutrient status28
The possibility of atypical micronutrient
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
104 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
deficiencies should not be dismissed when performing nutrition assessment in the postndash bariatric surgery population
Dumping syndrome
Dumping syndrome is the most com-mon nutrition-related problem experienced by Roux-en-Y gastric bypass patients with ap-proximately 50 to 70 of patients experienc-ing this symptom22 The Roux-en-Y procedure promotes dumping syndrome by allowing for very rapid infusion of the reduced stomachrsquos contents into the jejunum with subsequent forceful osmotic effects33 During a dumping episode a quick fluid shift occurs between the intravascular space and the lumen of the intestine34 The early phase of dumping may include abdominal pain nausea cramping and diarrhea The late phase encompasses the effects of resultant hypoglycemia and may in-clude sweating palpitations weakness trem-bling and even syncope34
Avoidance of foods such as simple carbo-hydrates which may precipitate dumping may be associated with weight loss However Shah22 and Banerjee et al33 recently reported that long-term weight loss following a Roux-en-Y procedure is associated with reduced food intake rather than with dumping syn-drome Dumping syndrome in severe cases may serve as an etiological factor in identified macro- and micronutrient deficiencies or protein-energy malnutrition Dumping syn-drome can usually be managed effectively by providing appropriate nutrition education to bariatric surgical patients35 While dumping symptoms tend to lessen with the passage of time refractory dumping symptoms may require medical or surgical intervention Medical treatments may include the use of somatostatin analogs such as octreotide which has been demonstrated to be effec-tive in ameliorating dumping symptoms34
Surgical treatment may include anatomical revisions designed to slow down the speed of gastric emptying34 For patients who have received a Roux-en-Y procedure insertion of an additional length of jejunum between the stomach and the jejunal anastomosis may
relieve dumping symptoms34 Enteral feeding into the jejunum may be required if dumping symptoms cannot be resolved34
Nausea and vomiting
Nausea and vomiting in post-bariatric surgery patients may be associated with con-sumption of portions too large for the reduced gastric pouch or by the simultaneous con-sumption of solids and liquids Nausea and vomiting in the postbariatric surgery patient requires medical follow-up and further inves-tigation since this symptom may result from strictures or GI obstruction10 The majority of cases of nausea and vomiting can be resolved with appropriate nutrition education35
Mechanical causes of nausea and vomiting may require surgical treatment Although un-common in the critical care setting preg-nancy can be a cause of nausea and vomiting Postndashbariatric surgical patients who are preg-nant should be carefully monitored for nutri-ent deficiencies and supplemented as needed on an individual basis36
Surgery-related
Surgical complications appear in approxi-mately 10 to 16 of Roux-en-Y gastric by-pass patients2237 Correction of surgical com-plications often requires additional surgery and such patients may require care in an ICU for some period of time during their clinical course Until the complications are resolved patients may require nutrition support since intake of nutrients by the oral route may be contraindicated Surgical complications can include but are not limited to anastomotic leaks wound infections anastomotic stric-tures and incisional hernias
The most common surgical complication is the anastomotic leak affecting 2 to 5 of Roux-en-Y bypass patients137 Leaks occur most commonly at the gastrojejunal anasto-mosis with leaks also occurring at the je-junojejunostomy site or at the gastric sta-ple line3738 More severely obese patients tend to experience an increased number of complications39 In a prospective descrip-tive study of 3018 Roux-en-Y gastric bypass
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 105
patients Gonzalez et al38 found that 63 pa-tients developed anastomotic leaks Among these patients 58 reoperations were required with duration of nutrition support lasting from 2 to 12 weeks3738 Thirty percent of these patients were receiving some type of nutrition support at hospital discharge3738
Anastomotic strictures represent a com-mon surgical complication of bariatric surgery In many cases strictures can be cor-rected via single or repeated endoscopic di-latation procedures40 Some strictures require further surgery to achieve resolution40
NUTRITION SUPPORT OF CRITICALLY ILL POSTndashBARIATRIC SURGERY PATIENTS
Several authors have noted a dearth of research and thus a lack of evidence-based guidelines regarding nutrition sup-port for critically ill postndashbariatric surgery patients15223741 Little is known regarding nutrition assessment issues in this population Published definitions of hypocaloric high-protein feeding are not consistent and the degree to which weight status interacts with the effects of altered GI anatomy in critical illness is poorly understood
At the present time resources available to practitioners caring for such patients include a limited amount of literature consensus guide-lines for obese patients and clinical judgment For patients with a recent history of bariatric surgery some literature is available regarding treatment of various complications including nutrient deficiencies and nutrition impact se-quelae such as dumping syndrome
Nutrition support approaches will vary on the basis of the patientrsquos current weight status Although a large number of post-bariatric patients will present with obesity patients may be underweight overweight or normal weight Morbid obesity may be fully or partially resolved in individual patients and malnutrition may vary in degree and type Nutrition support professionals must be prepared to provide individualized care
to postndashbariatric surgical patients on the basis of each patientrsquos particular situation and clinical judgment based on practitioner experience assumes increased importance
Goals of nutrition support
According to the American Society for Parenteral and Enteral NutritionSociety of Critical Care Medicine (ASPENSCCM) guide-lines (McClave et al42) the goals for nutri-tion support in critically ill obese patients differ little from goals for normal weight pa-tients promotion of healing by modulating the stress response prevention of oxidative cell injury and optimization of the immune response42 Avoidance of poor metabolic out-comes which may include hyperglycemia hepatic injury due to excessive lipogenesis from overfeeding andor intravenous lipid delivery and excessive CO2 production as-sociated with overfeeding is also an ap-propriate goal for nutrition support in the critically ill population regardless of weight status37
For critically ill patients who are obese goals of nutrition support may include reduc-tion of fat mass with simultaneous preserva-tion of lean tissue15 Early enteral nutrition may be advantageous in promoting desired goals Enteral nutrition is recommended as the preferred feeding route whenever possi-ble However in the presence of contraindi-cations to enteral feeding parenteral nutri-tion may be used as the method of nutrient delivery4243
Nutrition assessment
Sedation and mechanical ventilation com-mon in the critical care setting may present barriers to history taking if the patient is unaccompanied by persons who can pro-vide information Consensus guidelines rec-ommend that all bariatric patients carry with them a written description of their surgery and its resultant GI anatomy15
Information regarding the magnitude and rate of the patientrsquos resultant weight loss should be gathered if possible15 In assessing
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

104 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
deficiencies should not be dismissed when performing nutrition assessment in the postndash bariatric surgery population
Dumping syndrome
Dumping syndrome is the most com-mon nutrition-related problem experienced by Roux-en-Y gastric bypass patients with ap-proximately 50 to 70 of patients experienc-ing this symptom22 The Roux-en-Y procedure promotes dumping syndrome by allowing for very rapid infusion of the reduced stomachrsquos contents into the jejunum with subsequent forceful osmotic effects33 During a dumping episode a quick fluid shift occurs between the intravascular space and the lumen of the intestine34 The early phase of dumping may include abdominal pain nausea cramping and diarrhea The late phase encompasses the effects of resultant hypoglycemia and may in-clude sweating palpitations weakness trem-bling and even syncope34
Avoidance of foods such as simple carbo-hydrates which may precipitate dumping may be associated with weight loss However Shah22 and Banerjee et al33 recently reported that long-term weight loss following a Roux-en-Y procedure is associated with reduced food intake rather than with dumping syn-drome Dumping syndrome in severe cases may serve as an etiological factor in identified macro- and micronutrient deficiencies or protein-energy malnutrition Dumping syn-drome can usually be managed effectively by providing appropriate nutrition education to bariatric surgical patients35 While dumping symptoms tend to lessen with the passage of time refractory dumping symptoms may require medical or surgical intervention Medical treatments may include the use of somatostatin analogs such as octreotide which has been demonstrated to be effec-tive in ameliorating dumping symptoms34
Surgical treatment may include anatomical revisions designed to slow down the speed of gastric emptying34 For patients who have received a Roux-en-Y procedure insertion of an additional length of jejunum between the stomach and the jejunal anastomosis may
relieve dumping symptoms34 Enteral feeding into the jejunum may be required if dumping symptoms cannot be resolved34
Nausea and vomiting
Nausea and vomiting in post-bariatric surgery patients may be associated with con-sumption of portions too large for the reduced gastric pouch or by the simultaneous con-sumption of solids and liquids Nausea and vomiting in the postbariatric surgery patient requires medical follow-up and further inves-tigation since this symptom may result from strictures or GI obstruction10 The majority of cases of nausea and vomiting can be resolved with appropriate nutrition education35
Mechanical causes of nausea and vomiting may require surgical treatment Although un-common in the critical care setting preg-nancy can be a cause of nausea and vomiting Postndashbariatric surgical patients who are preg-nant should be carefully monitored for nutri-ent deficiencies and supplemented as needed on an individual basis36
Surgery-related
Surgical complications appear in approxi-mately 10 to 16 of Roux-en-Y gastric by-pass patients2237 Correction of surgical com-plications often requires additional surgery and such patients may require care in an ICU for some period of time during their clinical course Until the complications are resolved patients may require nutrition support since intake of nutrients by the oral route may be contraindicated Surgical complications can include but are not limited to anastomotic leaks wound infections anastomotic stric-tures and incisional hernias
The most common surgical complication is the anastomotic leak affecting 2 to 5 of Roux-en-Y bypass patients137 Leaks occur most commonly at the gastrojejunal anasto-mosis with leaks also occurring at the je-junojejunostomy site or at the gastric sta-ple line3738 More severely obese patients tend to experience an increased number of complications39 In a prospective descrip-tive study of 3018 Roux-en-Y gastric bypass
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 105
patients Gonzalez et al38 found that 63 pa-tients developed anastomotic leaks Among these patients 58 reoperations were required with duration of nutrition support lasting from 2 to 12 weeks3738 Thirty percent of these patients were receiving some type of nutrition support at hospital discharge3738
Anastomotic strictures represent a com-mon surgical complication of bariatric surgery In many cases strictures can be cor-rected via single or repeated endoscopic di-latation procedures40 Some strictures require further surgery to achieve resolution40
NUTRITION SUPPORT OF CRITICALLY ILL POSTndashBARIATRIC SURGERY PATIENTS
Several authors have noted a dearth of research and thus a lack of evidence-based guidelines regarding nutrition sup-port for critically ill postndashbariatric surgery patients15223741 Little is known regarding nutrition assessment issues in this population Published definitions of hypocaloric high-protein feeding are not consistent and the degree to which weight status interacts with the effects of altered GI anatomy in critical illness is poorly understood
At the present time resources available to practitioners caring for such patients include a limited amount of literature consensus guide-lines for obese patients and clinical judgment For patients with a recent history of bariatric surgery some literature is available regarding treatment of various complications including nutrient deficiencies and nutrition impact se-quelae such as dumping syndrome
Nutrition support approaches will vary on the basis of the patientrsquos current weight status Although a large number of post-bariatric patients will present with obesity patients may be underweight overweight or normal weight Morbid obesity may be fully or partially resolved in individual patients and malnutrition may vary in degree and type Nutrition support professionals must be prepared to provide individualized care
to postndashbariatric surgical patients on the basis of each patientrsquos particular situation and clinical judgment based on practitioner experience assumes increased importance
Goals of nutrition support
According to the American Society for Parenteral and Enteral NutritionSociety of Critical Care Medicine (ASPENSCCM) guide-lines (McClave et al42) the goals for nutri-tion support in critically ill obese patients differ little from goals for normal weight pa-tients promotion of healing by modulating the stress response prevention of oxidative cell injury and optimization of the immune response42 Avoidance of poor metabolic out-comes which may include hyperglycemia hepatic injury due to excessive lipogenesis from overfeeding andor intravenous lipid delivery and excessive CO2 production as-sociated with overfeeding is also an ap-propriate goal for nutrition support in the critically ill population regardless of weight status37
For critically ill patients who are obese goals of nutrition support may include reduc-tion of fat mass with simultaneous preserva-tion of lean tissue15 Early enteral nutrition may be advantageous in promoting desired goals Enteral nutrition is recommended as the preferred feeding route whenever possi-ble However in the presence of contraindi-cations to enteral feeding parenteral nutri-tion may be used as the method of nutrient delivery4243
Nutrition assessment
Sedation and mechanical ventilation com-mon in the critical care setting may present barriers to history taking if the patient is unaccompanied by persons who can pro-vide information Consensus guidelines rec-ommend that all bariatric patients carry with them a written description of their surgery and its resultant GI anatomy15
Information regarding the magnitude and rate of the patientrsquos resultant weight loss should be gathered if possible15 In assessing
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 105
patients Gonzalez et al38 found that 63 pa-tients developed anastomotic leaks Among these patients 58 reoperations were required with duration of nutrition support lasting from 2 to 12 weeks3738 Thirty percent of these patients were receiving some type of nutrition support at hospital discharge3738
Anastomotic strictures represent a com-mon surgical complication of bariatric surgery In many cases strictures can be cor-rected via single or repeated endoscopic di-latation procedures40 Some strictures require further surgery to achieve resolution40
NUTRITION SUPPORT OF CRITICALLY ILL POSTndashBARIATRIC SURGERY PATIENTS
Several authors have noted a dearth of research and thus a lack of evidence-based guidelines regarding nutrition sup-port for critically ill postndashbariatric surgery patients15223741 Little is known regarding nutrition assessment issues in this population Published definitions of hypocaloric high-protein feeding are not consistent and the degree to which weight status interacts with the effects of altered GI anatomy in critical illness is poorly understood
At the present time resources available to practitioners caring for such patients include a limited amount of literature consensus guide-lines for obese patients and clinical judgment For patients with a recent history of bariatric surgery some literature is available regarding treatment of various complications including nutrient deficiencies and nutrition impact se-quelae such as dumping syndrome
Nutrition support approaches will vary on the basis of the patientrsquos current weight status Although a large number of post-bariatric patients will present with obesity patients may be underweight overweight or normal weight Morbid obesity may be fully or partially resolved in individual patients and malnutrition may vary in degree and type Nutrition support professionals must be prepared to provide individualized care
to postndashbariatric surgical patients on the basis of each patientrsquos particular situation and clinical judgment based on practitioner experience assumes increased importance
Goals of nutrition support
According to the American Society for Parenteral and Enteral NutritionSociety of Critical Care Medicine (ASPENSCCM) guide-lines (McClave et al42) the goals for nutri-tion support in critically ill obese patients differ little from goals for normal weight pa-tients promotion of healing by modulating the stress response prevention of oxidative cell injury and optimization of the immune response42 Avoidance of poor metabolic out-comes which may include hyperglycemia hepatic injury due to excessive lipogenesis from overfeeding andor intravenous lipid delivery and excessive CO2 production as-sociated with overfeeding is also an ap-propriate goal for nutrition support in the critically ill population regardless of weight status37
For critically ill patients who are obese goals of nutrition support may include reduc-tion of fat mass with simultaneous preserva-tion of lean tissue15 Early enteral nutrition may be advantageous in promoting desired goals Enteral nutrition is recommended as the preferred feeding route whenever possi-ble However in the presence of contraindi-cations to enteral feeding parenteral nutri-tion may be used as the method of nutrient delivery4243
Nutrition assessment
Sedation and mechanical ventilation com-mon in the critical care setting may present barriers to history taking if the patient is unaccompanied by persons who can pro-vide information Consensus guidelines rec-ommend that all bariatric patients carry with them a written description of their surgery and its resultant GI anatomy15
Information regarding the magnitude and rate of the patientrsquos resultant weight loss should be gathered if possible15 In assessing
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

106 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
postndashbariatric patients the nutrition practi-tioner should assume that apparently ran-dom or unrelated symptoms such as heart failure neurologic pathology or GI dis-tress could be associated with micronutrient deficiencies152237
Energy and protein needs
Ideally indirect calorimetry (IC) should be used to measure energy needs in the criti-cally ill post-bariatric surgery patient How-ever not every patient is a suitable candidate for IC and many hospitals lack equipment for performing IC In the absence of IC predic-tive equations must be used to estimate en-ergy needs Existing studies regarding energy needs in the critically ill obese patients do not account for altered GI anatomy resulting from bariatric surgery Little is known regard-ing the effects of higher weight ranges on en-ergy needs in critical illness Ireton-Jones44
in a classic article published in 1991 noted that the correlation between actual body weight and energy expenditure disappeared in patients with body mass index exceeding 60 kgm2 suggesting that the difficulty in de-termining appropriate energy provision in ex-tremely obese patients increases with body size
Alves et al45 found that although the Harris-Benedict equation using actual body weight and no stress factor provided the most ac-curate results in critically ill obese patients the range of variability of the results was un-acceptable Anderegg et al46 found that the Harris-Benedict equation using adjusted body weight and a stress factor provided results within 10 of measured needs in 50 of a group of 36 obese hospitalized adults Con-sensus guidelines prepared by participants in an Obesity in Critical Care workshop spon-sored by Nestle Healthcare Nutrition and pub-lished in the Journal of Parenteral and En-teral Nutrition recommend that energy be provided to critically ill obese adults at 11 to 14 kcalkg actual body weight or 22 to 25 kcalkg ideal body weight (IBW)15 How-ever no predictive equation or guideline
recommendation is specifically applicable to postndashbariatric patients1542
Frankenfield et al47 did a comparative study and evaluated the accuracy of 8 different predictive equations in 202 critically ill pa-tients The study evaluated 3 versions of the Penn State equation (PSU) and found that the PSU(m) equation was accurate within 10 of measured resting metabolic rate needs in 70 of young obese and 53 of elderly obese patients3747 More recently Frankenfield48
used an expanded sample to validate the PSU(m) in adults older than 60 years with body mass index greater than 30 finding accuracy within 10 of measured resting metabolic rate in 74 of patients In ASPEN clinical guidelines for hospitalized obese adult patients published in 2013 Choban et al49
recommended that the 2010 PSU equation be used to estimate energy needs in hospitalized obese patients and that the PSU(m) be used to estimate energy needs in hospitalized obese patients older than 60 years48 The recommen-dation for use of the PSUs is rated strong with high evidence49
Evidence of the appropriate amounts of protein to provide to the critically ill postndash bariatric surgery population is limited Inter-vention studies that have examined the ef-fects of exact amounts of protein tend to be small older and use the parenteral rather than enteral mode of feeding5051 Krieger et al52 found better preservation of lean body mass during energy restriction with the provision of at least 105 gkgd protein however this study was not conducted in crit-ically ill patients American Society for Par-enteral and Enteral NutritionSociety of Criti-cal Care Medicine guidelines recommend the provision of 15 to 20 gkg IBW protein to hospitalized obese patients42 Consensus guidelines for the severely obese critically ill patient recommend the provision of more than 20 gkg IBW to persons with classes I and II obesity and more than 25 gkg IBW to persons with class III obesity15 The con-sensus guidelines are not specific to postndash bariatric surgery patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 107
Enteral and parenteral nutrition
When a functional GI tract is available en-teral nutrition is the nutrition support method of choice However enteral nutrition may be contraindicated in obese critically ill postndash bariatric surgery patients on the basis of a non-functional GI tract increased intra-abdominal pressure promoting an unacceptable risk of reflux or aspiration or lack of ability to confirm correct nasogastric tube placement radiographically because of large body size or physical barriers such as an extremely large pannus154142 In the case of morbidly obese patients difficulty in reaching parts of the patientrsquos body to provide care may ne-cessitate the use of step stools or special lift teams and may hinder proper tube care and management41
Postndashpyloric tube placement into the je-junum may be considered and may present fewer obstacles to achievement of nutritional goals than a gastric tube15 Placement of a feeding tube into the remnant stomach has been successful in some postndashbariatric surgi-cal patients53 In this case food travels from the remnant stomach through the biliopan-creatic limb and into the common channel via the jejunojejunostomy located at the bil-iopancreatic limbRoux limb anastomosis53
If nutrition cannot be provided enterally par-enteral nutrition remains an option
Hypocaloric high-protein feeding
While a growing body of evidence indi-cates that the critically ill obese population may benefit from hypocaloric high-protein feedings there are no standard definitions or specific administration guidelines for such feedings43 Hypocaloric high-protein feed-ings allow for a calorie deficit while maintain-ing nitrogen balance and have been associ-ated with improved clinical outcomes such as reduced days on ventilator support fewer in-fections better glycemic control and reduced length of ICU stay15424350
The 2013 ASPEN clinical guidelines for nutrition support for hospitalized obese adult patients recommend a trial of hypocaloric
feeding at 50 to 70 estimated needs or less than 14 kcalkg in patients without serious renal or hepatic disease the strength of the recommendation is weak with low evidence49 The guidelines recommend the provision of protein at 12 gkg actual body weight or 2 to 25 gkg IBW with subsequent monitoring and adjustment of protein intake as indicated by nitrogen balance tests49
Consensus recommendations for energy provision to critically ill obese adults tend to approximate the recommended hypocaloric amount (11-14 kcalkg actual body weight or 22-25 kcalkg IBW)15
Enteral formula
No specific guidelines exist at the cur-rent time regarding the best enteral for-mula for critically ill postndashbariatric surgery patients1554 For the subset of critically ill postndashbariatric surgery patients who are obese McClave et al15 and Martindale et al54 have proposed the design of a formula specifically to minimize the metabolic derangements as-sociated with critical illness as an important topic for research Such a formula would be high-protein low-carbohydrate and would provide some marine fat content as an anti-inflammatory component54 Other nutrients have been proposed for inclusion as well including arginine glutamine selenium and zinc although evidence to support these pro-posals is weak and inconclusive1554
Micronutrient concerns
While a complete discussion of micronutri-ent needs for postndashbariatric surgery patients is outside the scope of this article it is impor-tant to remember that such deficiencies are common and may be present in a critically ill patient15192228 In the critically ill postndash bariatric surgery patient a strong possibility of surgically induced micronutrient deficiency should be assumed especially if the patient has a history of the biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass15 If possible the patient should be questioned regarding compliance with ongo-ing nutrient supplementation
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

108 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
Manzanares and Hardy55 reported that se-vere thiamin deficiency is common in the crit-ically ill population and is associated with as much as a 50 increase in overall mortality McClave et al15 recommends intravenous thi-amine administration in critically ill obese pa-tients before providing dextrose solutions to prevent cardiac malfunction Table 2 provides a list of symptomatic conditions along with possible related micronutrient deficiencies
Monitoring and refeeding syndrome
Usual monitors of nutritional status applied to ICU patients should be used in the critically ill obese population including postndashbariatric surgery patients15 For obese patients special attention may be paid to records of intake and output to ensure delivery of appropriate amounts of feeding Serial measures of IC may be taken to monitor changing energy needs as fat mass is reduced15 Monitors should also include micronutrient status glycemic indica-tors and measures of kidney function in view of high-protein feedings154245
Regardless of weight status the criti-cally ill postndashbariatric surgery population may present with significant malnutri-tion and an increased risk for refeeding syndrome5657 Refeeding syndrome is a po-tentially life-threatening complication most often associated with aggressive parenteral nutrition but the condition may occur with enteral and oral feedings as well58 Severe malnutrition is accompanied by suboptimal concentrations of intracellular electrolytes as
well as reduced secretion of insulin57 During the process of refeeding insulin secretion increases resulting in rapid shifts of glucose potassium phosphate magnesium and water toward the intracellular space Serum elec-trolyte abnormalities including hypokalemia hypophosphatemia and hypomagnesemia may precipitate severe sequelae such as cardiac arrhythmias respiratory difficulties and neurological aberrations57
Marik and Bedigian59 in a study of 62 crit-ically ill patients found that refeeding syn-drome occurred in 34 of patients and that the manifestations of refeeding syndrome can occur after as little as 48 hours of fasting In the study by Marik et al59 increased length of stay as well as increased time to respira-tor weaning was linked to the presence of refeeding syndrome as measured by serum phosphate levels Rio et al60 studied a cohort of 243 hospitalized subjects receiving nutri-tion support for the first time Rio et al60
found that risk factors associated with refeed-ing syndrome included poor dietary intake for more than 10 days weight loss greater than 15 prior to study initiation and baseline hypomagnesemia Hypomagnesemia at base-line was an independent predictor of refeed-ing syndrome (P lt 02) Of the cohort 133 presented with risk factors for refeeding syn-drome and 2 of patients developed severe metabolic aberrations Twenty-eight percent of patients died during hospitalization but none of the deaths was directly linked to refeeding syndrome60
Table 2 Conditions Associated With Micronutrient Deficiencies
Complication Possible Micronutrient Deficiencies
Anemia (macro- or Iron B12 folate Vitamin D copper zinc Vitamin A Vitamin E microcytic)192237
Bone pathology19 Calcium Vitamin D Heart failure15 Thiamin Neurological symptoms1522 Thiamin B12 Vitamin E copper Skin pathology19 Vitamin A zinc Vision problems19 Vitamin A thiamin Vitamin E Idiopathic symptoms15 Variable (nonspecific symptoms require further investigation)
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 109
In providing nutrition support to critically ill postndashbariatric surgery patients risk factors for refeeding syndrome should be assessed Slow initiation of feeding coupled with careful monitoring and correction of electrolyte ab-normalities during the refeeding process may prevent metabolic complications associated with the refeeding syndrome (Table 3)57-60
Little research exists regarding the process of transitioning critically ill patients with a his-tory of bariatric surgery from nutrition sup-port to oral feedings In practice it appears that patients are often returned either to the first phase of the postndashbariatric surgery diet (clear liquids) or to the type of diet the pa-tient was consuming prior to critical illness Benchmarks for oral intake before discontinu-ing nutrition support vary among institutions but it appears that many institutions consider an oral intake of 50 to 60 estimated needs to be sufficient for termination of nutrition support61
CONCLUSION
At the present time little evidence from sufficiently powered randomized controlled trials exists to inform the practice of nutrition support in critically ill patients with a recent
153762 or distant history of bariatric surgery An assumption that such patients can auto-matically be assigned to guidelines intended for critically ill obese patients is problem-atic Not all postndashbariatric surgery patients are obese The amount and absorptive capacity of unaltered GI surface area differs from pa-tient to patient The range of macro- and mi-cronutrient deficiencies that present in postndash bariatric surgery patients coupled with sub-stantial variations in postsurgical GI anatomy requires an individualized approach to each patientrsquos situation
Every aspect of nutrition support to critically ill postndashbariatric surgery patients requires further research to support the
Table 3 Suggestions for Providing Nutrition Support to Critically Ill PostndashBariatric Surgery Patients
When performing nutrition assessment Gather relevant information regarding the patientrsquos surgery15
Time elapsed since surgery Rate and magnitude of weight loss Weight history since surgery Nature of the patientrsquos altered GI anatomy Previous complications
Consider the possibility of nutrient deficiencies1922
Consider the possibility of refeeding syndrome in malnourished patients56
When determining energy requirements Measure by indirect calorimetry if possible374249
Predictive energy equations may be used if indirect calorimetry is not available3748
For obese patients younger than 60 years use the 2010 Penn State Equation48
For obese patients 60 years of age or older use the modified Penn State Equation48
When determining protein requirements BMI lt30 12-20 gkg actual body weight42
BMI ge 30 le 40 ge 20 gkg ideal body weight BMI gt 40 ge 25 gkg ideal body weight15
When considering hypocaloric high-protein feedings for obese patients Avoid in patients with significant renal or hepatic disease49
Provide energy at 50-70 estimated needs or lt14 kcalkg49
Provide protein at 12 gkg actual body weight or 20-25 gkg ideal body weight49
Abbreviations BMI body mass index GI gastrointestinal
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

110 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
development of evidence-based guidelines Research focused on critical illness in such patients is a vital component for increas-ing the knowledge base regarding long-term outcomes of bariatric surgery particularly as long-term data for various types of surgery continue to accrue
Areas for future research include but are not limited to optimal provision of energy and protein protocols for correction of
REFERENCES
nutrient deficiencies best practices for nu-trition support delivery selection of appro-priate enteral formulas and delineation of optimal parameters for hypocaloric high-protein feedings Increased numbers of postndash bariatric surgical patients ensure that issues for these patients in the critical care set-ting will remain an important component of daily practice for the nutrition support professional
1 Kumpf VJ Slocum K Binkley J Jensen G Com-plications after bariatric surgery survey evaluat-ing impact on the practice of specialized nutri-tion support Nutr Clin Pract 200722(6)673-678 doi1011770115426507022006673
2 Elliot V Bariatric surgery maintains doesnrsquot gain American Medical News American Medical As-sociation April 23 2012 httpwwwama-assn orgamednews20120423bisa0423htm Accessed October 19 2013
3 Madura JA DiBaise JK Quick fix or long-term cure Pros and cons of bariatric surgery F1000 Rep Med 20124(19)1-9
4 Gass M Beglinger C Peterli R Metabolic surgerymdash principles and current concepts Langenbecks Arch Surg 2011396(7)949-972 doi101007s00423-011-0834-35
5 Kopelman PG Grace C New thoughts on managing obesity Gut 200453(7)1044-1053 doi101136gut2003021816
6 Snow V Barry P Fitterman N Qaseem A Weiss K Pharmacologic and surgical management of obesity in primary care a clinical practice guideline from the American College of Physicians Ann Intern Med 2005142(7)525-587 doi1073260003-4819-142-7-200504050-00011
7 Surgical Review Corporation BOLD history http wwwsurgicalrevieworgboldhistory Published 2014 Accessed February 4 2014
8 Surgical Review Corporation Locate a center of ex-cellence or a surgeon of excellence httpwww surgicalrevieworglocate Published 2014 Acce-ssed February 4 2014
9 WIN Weight-control Information Network Bariatric surgery for severe obesity National Institute of Digestive and Diabetes and Kidney Diseases httpwinniddknihgovpublicationsgastrichtm Accessed October 18 2013
10 Karmali S Stoklossa CJ Sharma A et al Bariatric surgery Can Fam Phys 201056(9)873-879
11 Saltzman E Karl JP Nutrient deficiencies af-ter gastric bypass surgery Annu Rev Nutr
201333183-203 doi 101146annurev-nutr-071812-161225
12 Cleveland Clinic Foundation Weight Loss Surgery for Severely Obese Patients Information for Physicians from the Cleveland Clinic Bariatric and Metabolic Institute httpsweightloss clevelandclinicorgimagesfilePhysBrochure_FNL pdf Published 2008 Accessed October 18 2013
13 van Rutte PWJ Luyer MDP de Hingh IHJT Nien-huisj SW To sleeve or not to sleeve in bariatric surgery [published online ahead of print August 16 2012] ISRN Surg 20122012674042 doi 1054022012674042
14 El Chaar M Claros L Ezeji GC Miletics M Stoltz-fus J Improving outcome of bariatric surgery best practices in an accredited surgical center[published online ahead of print February 22 2014] Obes Surg doi 101007s11695-014-1209-y
15 McClave SA Kushner R Van Way CW et al Nutrition therapy of the severely obese critically ill patient summation of conclusions and recommen-dations JPEN J Parenter Enteral Nutr 201135(5 suppl)88S-96S doi1011770148607111415111
16 Schroeder R Garrison JM Johnson MS Treatment of adult obesity with bariatric surgery Am Fam Phys 201184(7)805-814
17 Pontiroli AE Morabito AA Long-term prevention of mortality in morbid obesity through bariatric surgery a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass Ann Surg 2011253(3)484-487 doi101097SLA0b013e31820d98cb
18 Kelly JJ Shikora S Jones DB et al Best prac-tice updates for surgical care in weight loss surgery Obesity (Silver Spring) 200917(5)863-870 doi101038oby2008570
19 Fujioka K DiBaise JK Martindale RG Nutri-tion and metabolic complications after bariatric surgery and their treatment JPEN J Par-enter Enteral Nutr 201135(5 suppl)52S-59S doi1011770148607111413600
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

Nutrition Support for the Critically Ill PostndashBariatric Surgery Patient 111
20 Dodsworth A Warren-Forward H Baines S A systematic review of dietary intake after la-paroscopic adjustable gastric banding J Hum Nutr Diet 201124(4)327-341 doi101111j1365-277X201101155x
21 Moize V Andreu A Flores L et al Long-term dietary intake and nutritional deficiencies fol-lowing sleeve gastrectomy or Roux-En-Y gastric bypass in a mediterranean population J Acad Nutr Diet 2013113(3)400-410 doi101016jjand 201211013
22 Shah MV Nutrition support in the complicated bariatric patient Support Line 200729(6)7-11
23 Kumar R Lieske JC Collazo-Clavell ML et al Fat malabsorption and increased intestinal ox-alate absorption are common after Roux-en-Y gas-tric bypass surgery Surgery 2011149(5)654-661 doi101016jsurg201011015
24 Odstrcil EA Martinez JG Santa Ana CA et al The contribution of malabsorption to the reduction in net energy absorption after long-limb Roux-en-Y gas-tric bypass Am J Clin Nutr 201092(4)704-713 doi103945ajcn201029870
25 Ikramuddin S Korner J Lee W et al Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes hypertension and hyperlipidemia the diabetes surgery study random-ized clinical trial JAMA 2013309(21)2240-2249 doi101001jama20135835
26 Raghow R Bariatric surgery-mediated weight loss and its metabolic consequences for type-2 diabetes World J Diabetes 20134(3)47-50 doi104239wjdv4i347
27 Hammer HF Hammer J Diarrhea caused by carbohy-drate malabsorption Gastroenterol Clin North Am 201241611-627 doi101016jgtc201206003
28 Shankar P Boylan M Sriram K Micronutri-ent deficiencies after bariatric surgery Nu-trition 201026(11-12)1031-1037 doi101016 jnut200912003
29 Dewey M Heuberger R Vitamin D and cal-cium status and appropriate recommenda-tions in bariatric surgery patients Gastroen-terol Nurs 201134(5)367-374 doi101097 SGA0b013e318229bcd0
30 Cunha SF Goncalves GA Marchini JS Roselino AM Acrodermatitis due to zinc deficiency after com-bined vertical gastroplasty with jejunoileal bypass case report Sao Paulo Med J 2012130330-335 doi101590S1516-31802012000500010
31 Chen MC Lee YC Lee WJ Liu HL Ser KH Diet behavior and low hemoglobin level after laparo-scopic mini-gastric bypass surgery Hepatogastroen-terology 201259(120)2530-2532
32 Zalesin KC Miller WM Franklin B et al Vita-min a deficiency after gastric bypass surgery an underreported postoperative complication J Obes 20112011 Article 760695
33 Banerjee A Ding Y Mikami D Needleman B The role of dumping syndrome in weight loss after gastric bypass surgery Surg Endosc 201227(5)1-6
34 Tack J Arts J Caenepeel P De Wulf D Biss-chops R Pathophysiology diagnosis and manage-ment of postoperative dumping syndrome Nat Rev Gastroenterol Hepatol 20096(10)583-590 doi101038nrgastro2009148
35 Nutrition Care Manual Academy of Nutrition and Dietetics http0-wwwnutritioncaremanualorg wnclnwnclnorgcontentcfmncm_content_id= 79355 Accessed October 11 2013
36 Magdaleno R Jr Pereira BG Chaim EA Turato ER Pregnancy after bariatric surgery a current view of maternal obstetrical and perinatal chal-lenges Arch Gynecol Obstet 2012285(3)559-566 doi101007s00404-011-2187-0
37 Segaran E Provision of nutritional support to those experiencing complications following bariatric surgery Proc Nutr Soc 201069536-542 doi101017S0029665110001965
38 Gonzalez R Sarr MG Smith CD et al Diag-nosis and contemporary management of anasto-motic leaks after gastric bypass for obesity J Am Coll Surg 2007204(1)47-55 doi101016 jjamcollsurg200609023
39 Benotti PN Wood GC Rodriguez H Carnevale N Liriano E Perioperative outcomes and risk factors in gastric surgery for morbid obesity a 9-year experience Surgery 2006139(3)340-346 doi101016jsurg200508017
40 Carrodeguas L Szomstein S Zundel N Lo Menzo E Rosenthal R Gastrojejunal anasto-motic strictures following laparoscopic Roux-en-Y gastric bypass surgery analysis of 1291 pa-tients Surg Obes Relat Dis 20062(2)92-97 doi101016jsoard200510014
41 McGinnis C Fischer J Larson G Nutrition support in the morbidly obese critically ill patient Nutr Clin Pract 200419(3)290-296 doi1011770115426504019003290
42 McClave SA Martindale RG Vanek VW et al Guide-lines for the provision and assessment of nutri-tion support therapy in the adult critically ill pa-tient Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutri-tion (ASPEN) JPEN J Parenter Enteral Nutr 200933(3)277-316
43 Choban PS Dickerson RN Morbid obesity and nutrition support is bigger different Nutr Clin Pract 200520(4)480-487 doi10 11770115426505020004480
44 Ireton-Jones CSTW Actual or ideal body weight which should be used to predict energy expenditure J Am Diet Assoc 199191(2)193-195
45 Alves VG da Rocha EE Gonzalez MC da Fon-seca RB Silva MH Chiesa CA Assessment of resting energy expenditure of obese patients
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited

112 TOPICS IN CLINICAL NUTRITIONAPRILndashJUNE 2014
comparison of indirect calorimetry with formu-lae Clin Nutr 200928(3)299-304 doi101016 jclnu200903011
46 Anderegg BA Worrall C Barbour E Simpson KN DeLegge M Comparison of resting energy expen-diture prediction methods with measured resting energy expenditure in obese hospitalized adults JPEN J Parenter Enteral Nutr 200833(2)168-175 doi1011770148607108327192
47 Frankenfield DC Coleman A Alam S Cooney RN Analysis of estimation methods for resting metabolic rate in critically ill adults JPEN J Parenter Enteral Nutr 200933(1)27-36
48 Frankenfield DC Validation of an equation for resting metabolic rate in older obese critically ill patients JPEN J Parenter Enteral Nutr 201135(2)264-269
49 Choban P Dickerson R Malone A et al ASPEN Clinical Guidelines nutrition support of hospitalized adult patients with obesity JPEN J Parenter Enteral Nutr 201337(6)714-744
50 Dickerson RN Optimal caloric intake for critically ill patients first do no harm Nutr Clin Pract 201126(1)48-54 doi1011770884533610393254
51 Choban PS Burge JC Scales D Flancbaum L Hy-poenergetic nutrition support in hospitalized obese patients a simplified method for clinical application Am J Clin Nutr 199766(3)546-550
52 Krieger JW Sitren HS Daniels MJ Langkamp-Henken B Effects of variation in protein and carbohydrate intake on body mass and composition during en-ergy restriction a meta-regression Am J Clin Nutr 200683(2)260-274
53 Goitein D Gagne DJ Papasavas PK et al Percu-taneous computed tomography-guided gastric rem-nant access after laparoscopic Roux-en-Y gastric bypass Surg Obes Relat Dis 20062(6)651-655 doi101016jsoard200609007
54 Martindale RG DeLegge M McClave S Mon-roe C Smith V Kiraly L Nutrition delivery for obese ICU patients delivery issues lack of guide-
lines and missed opportunities JPEN J Parenter Enteral Nutr 201135(5 suppl)80S-87S doi10 11770148607111415532
55 Manzanares W Hardy G Thiamine supplementation in the critically ill Curr Opin Clin Nutr Metab Care 201114(6)610-617
56 Hiesmayr M Nutrition risk assessment in the ICU Curr Opin Clin Nutr Metab Care 201215(2)174-180 doi101097MCO0b013e328350767e
57 Viana LA Burgos MG Silva RA Refeeding syndrome clinical and nutritional relevance Arq Bras Cir Dig 201225(1)56-59
58 Miller SJ Death resulting from overzealous to-tal parenteral nutrition the refeeding syndrome revisited Nutr Clin Pract 200823(2)166-171 doi1011770884533608314538
59 Marik PE Bedigian M Refeeding hypophosphatemia in critically ill patients in an intensive care unit a prospective study Arch Surg 1996131(10)1043-1047 doi101001archsurg199601430220037007
60 Rio A Whelan K Goff L Reidlinger DP Smee-ton N Occurrence of refeeding syndrome in adults started on artificial nutrition support prospective cohort study BMJ Open 20133(1)pii e002173
61 Grossman S Bautista C A transitional feeding protocol for critically ill patients Dimens Crit Care Nurs 200120(5)46-51 doi10109700003465-200109000-00014
62 Ziegler O Sirveaux MA Brunaud L Reibel N Quil-liot D Medical follow up after bariatric surgery nutritional and drug issues General recommenda-tions for the prevention and treatment of nutri-tional deficiencies Diabetes Metab 200935(6)544-557doi101016S1262-3636(09)73464-0
63 Hamilton C Dasari V Shatnawei A Lopez R Steiger E Seidner D Hypocaloric home parenteral nutri-tion and nutrition parameters in patients following bariatric surgery Nutr Clin Pract 200935(6 Pt 2) 544-557
Copyright copy 2014 Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited