Embed Size (px)
Citation preview

JMed Genet 1994;31:903-915
Review article
Recent advances in the gene map of inheritedeye disorders: primary hereditary diseases of theretina, choroid, and vitreous
Philip J Rosenfeld, Victor A McKusick, Joanna S Amberger, Thaddeus P Dryja
The diagnosis and basic understanding ofmanygenetic ocular disorders have been aided by theidentification of the disease causing chromo-somal loci. These chromosomal loci havebeen mapped using the candidate gene or thepositional cloning approaches. This review willfocus on genetic disorders that primarily affectocular function with emphasis on the mostrecent advances in the chromosomal mappingof these disorders. In particular, we will con-centrate on the genetic diseases affecting theposterior segment of the eye including the ret-ina, choroid, and vitreous. The success of link-age analysis has relied heavily on previousclinical classifications and there are numerousreports of distinct ocular diseases mapping tospecific chromosomal loci. However, there arealso many examples in which a well defineddisease maps to any of a number of chro-mosomal loci. This genetic phenomenon isknown as non-allelic or locus heterogeneityand can be viewed as reflecting the eye's limitedrepertoire of responses to a variety of geneticlesions. Another emerging pattern is that of"gene sharing" in which different mutationswithin the same gene can cause clinically dis-tinct ocular diseases. Mapping of mendeliangenetic disorders has helped refine the clinicalclassifications and has led to examples of both"lumping" and "splitting".
Ocular tumoursRETINOBLASTOMARetinoblastoma, an embryonic neoplasm oftheretina, is the most common primary intraocularmalignancy in infants and children. The av-erage annual incidence ofretinoblastoma in theUS population younger than 10 years old is10-9 per million.' The gene maps to chro-mosome 13q14, consists of 27 exons spanning180 to 388 bp of genomic DNA, produces a4-7 kb transcript, and encodes a nuclear phos-phoprotein consisting of 928 amino acids.The complete gene sequence is available.2 Theretinoblastoma (Rb) gene is a model for a classof recessive cancer genes where wild type alleleshave a tumour suppressor function. Retino-blastoma predisposition segregates as anautosomal dominant trait with 90% penet-
rance, but the mutations are actually recessiveat the cellular level since tumours arise only ifboth copies of the retinoblastoma gene areinactivated in a sensitive cell. These tumourinducing null mutations can arise by intragenicdeletion, insertion, or translocation, by singlenucleotide changes that affect coding or spli-cing sequences, or by epigenetic abnormalitiessuch as hypermethylation of the promoter re-gion.3-'3 Some retinoblastoma families showevidence of reduced or incomplete penetrance.The molecular basis of reduced penetrance hasbeen investigated in eight different families.""'7Two families with reduced penetrance havemutations in the promoter region of the re-tinoblastoma gene that decrease but do noteliminate the Rb gene product and three fam-ilies have a mutation that produces a mutantprotein with presumed diminished tumour sup-pressor activity. One of the families studiedactually has "pseudo-low penetrance" owing toindependently derived Rb mutations in distantrelatives. 7 In another two families, no commonintragenic haplotypes were identified in rel-atives with retinoblastoma and no mutationswere identified in the Rb genes.'6 These twofamilies could be other examples of "pseudo-low penetrance" with relatives having in-dependently derived Rb mutations.
Colour blindnessPROTAN AND DEUTAN SERIESThe red and green visual pigment genes havebeen cloned, sequenced, and mapped.'820Mutations in these genes are the molecularbasis for X linked colour vision abnor-malities.2'-23 Genes for the red and greenopsins lie on the long arm oftheX chromosomewithin Xq28. These genes are arranged in atandem array with one copy of the red pigmentgene at the 5' end and from one to five greenpigment genes located downstream in a headto tail configuration presumably arising fromunequal homologous recombination events.Only a single green pigment gene is expressedfrom this locus, probably the most proximalcopy.24 More than 95% of cases of red-greencolour blindness arise from mutant genotypesowing to unequal intra- and intergenic re-
Howe Laboratory,Departnent ofOphthalmology,Harvard MedicalSchool, MassachusettsEye and EarInfirmary, 243 CharlesStreet, Boston,Massachusetts 02114,USAP J RosenfeldT P Drya
Center for MedicalGenetics, The JohnsHopkins UniversitySchool of Medicine,Blalock Building,Room 1007, 600 NWolfe Street,Baltimore, Maryland,21287-4922, USAV A McKusickJ S Amberger
Correspondence toDr Rosenfeld.
903
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Rosenfeld, McKusick, Amberger, Dryja
combination events giving rise to deletions orhybrid genes within the tandem array of pig-ment genes.2' 25-28 These mutations are the gen-etic basis for protanopia (absence of red colourvision), protanomaly (anomalous red colourvision), deuteranopia (absence of green colourvision), and deuteranomaly (anomalous greencolour vision). A missense mutation within thehuman green visual pigment gene is anothercause of deuteranomaly.29 There is a directcorrelation between anomalous red/green vis-ion as detected by psychophysical experimentsand the shifts in the in vitro absorption maximaof hybrid pigments produced from clonedcDNAs when compared to normal cone pig-ments.30-32 In normal trichromats who displayperson to person variability in red colourmatching, two common alleles of the red pig-ment gene have been identified and the re-spective shifts in their absorption maxima canaccount for the differences in psychophysicaltesting.32-34 In general, persons with ab-normalities in red-green discrimination haveno other signs of retinal disease.The complete loss of red and green cone
function results in blue cone monochromacy,also known as incomplete achromotopsia.Males with this X linked trait use blue conesexclusively under photopic conditions and gen-erally have an acuity of only around 20/200.These persons are capable of limited huediscrimination but only at intermediate lightlevels.3536 Blue cone monochromats have re-arrangements within the red and green visualpigment gene cluster that result in the func-tional loss of both classes of opsin genes.3738These mutations fall into two classes. In oneclass, the loss of functional genes is mediatedby unequal homologous recombination andpoint mutations. A second class involves thedeletion of a locus control region upstream ofthe red and green pigment gene cluster. Theaffected upstream region can normally functionas an activator of cone specific gene expressionin transgenic mice.39
TRITANOPIATritanopia, the absence of blue colour vision,differs from the other colour vision disordersbecause it is inherited as an autosomal dom-inant trait with variable penetrance. The geneencoding the cone blue sensitive pigment hasbeen cloned, sequenced, and mapped to chro-mosome 7 at position 7q31.3-q32.'82'41 Pointmutations within the blue pigment gene havebeen associated with tritanopia.4 142
ROD MONOCHROMACYThe absence of functional cones is known astotal achromatopsia or rod monochromacy.This condition is inherited as an autosomalrecessive trait. Rod monochromatism is char-acterised by nystagmus in infancy that di-minishes with age. There is severe photophobiaand poor vision in ordinary lighting. Vision isimproved with dim light to 20/200 but there isa total absence of colour discrimination. Thefundus examination is normal but histo-
pathological studies of eyes from patients showabnormal or absent cones.43 There is evidencethat the genetic locus for rod monochromacyis on chromosome 14. In this report, a 20year old white woman with rod monochromacywas found to have a 14; 14 Robertsonian trans-location and shown to be isodisomic for thematernal chromosome 14. The responsiblelocus on chromosome 14 has not been iden-tified.
Congenital stationary night blindnessCongenital stationary night blindness (CSNB)is a group of genetically heterogeneous retinaldisorders characterised by non-progressivenight blindness. The disease can be inheritedas an autosomal dominant, autosomal re-cessive, or X linked trait, and there can bephenotypic heterogeneity even between fam-ilies with the same inheritance pattern. Elec-troretinographic evidence indicates an intactcone system but the rod system can be variablyaffected. The complete type has no detectablerod function, while the incomplete type hasreduced rod function. Reduced visual acuityand nystagmus are variable clinical features ofthis disease. Myopia is often associated with Xlinked and recessive forms. A dominant formof CSNB can be caused by certain missensemutations in the rhodopsin gene.45-4' Thesemutations are distinct from those responsiblefor retinitis pigmentosa, a progressive de-generation of both rods and cones. Dryja et al'6could not find a rhodopsin mutation in a subjectwith the Nougaret type of CSNB, perhaps themost thoroughly studied form of autosomaldominant CSNB. A type of CSNB usuallyassociated with myopia, nystagmus, and de-creased visual acuity has been designatedCSNB 1 and mapped to the short arm of theX chromosome at position Xp 11 .3.4851 Thefrequent occurrence of myopia in this disorderis believed to be a pleiotropic effect of theunidentified CSNB gene rather than the resultof a closely linked second gene.5' The gene forCSNB 1 might be allelic with unidentified genesresponsible for retinitis pigmentosa and ocularalbinism which have been assigned to the sameregion by linkage studies.52-56
Ocular albinismNettleship-Falls type ocular albinism or ocularalbinism type 1 (OA1) is inherited as an Xlinked recessive disorder. The fundamental ab-normality is believed to be defective mel-anogenesis within all pigment-containing cells,but the pigmentation appears grossly abnormalonly in the eye. Affected males present withdecreased visual acuity, nystagmus, and headnodding. Examination shows hypopig-mentation of the fundus, foveal hypoplasia,prominent choroidal vessels, iris translucency,posterior embryotoxon, and optic disc hypo-plasia.57 Visual evoked potentials show evi-dence of abnormal crossing of the optic nervesat the chiasm. Carrier females may show iristranslucency, pigment mottling at the fundusperiphery, and abnormal macromelanosomes
904
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Recent advances in the gene map of inherited eye disorders
on histological inspection of skin biopsies.Multipoint linkage analysis and comparativedeletion mapping have refined the location ofthe OA1 gene within Xp22.3.""6 Thissame region has been linked to a form of Xlinked recessive ocular albinism with late onsetprogressive sensorineural hearing loss.62 Bothforms of ocular albinism may be clinical ma-nifestations of different genes or the result ofallelic heterogeneity within the same gene.While the gene for OA1 has not yet beenidentified, it has been localised within a 200 kbregion that is contained within a 2-6 Mb yeastartificial chromosome contig.63
Forsius-Eriksson type ocular albinism orocular albinism type 2 (OA2) was originallydescribed in a family from the Aland Islandsin the Sea of Bothnia. This form of ocularalbinism is referred to as Aland Island eyedisease (AIED). OA2 or AIED is inherited asan X linked recessive disorder. This form ofocular albinism has the clinical characteristicsdescribed for OA1. In addition, affected maleswith OA2 often have progressive axial myopia,astigmatism, defective dark adaptation, andprotanomalous colour blindness. In contrast toOA1, the pigment containing cells in OA2appear normal and there is no evidence of opticnerve fibre misrouting at the chiasm. Based onelectrophysiological techniques, OA2 has beenconsidered by some to be a form of congenitalstationary night blindness with myopia(CSNB1).5664 The gene for OA2 was mappedby multilocus linkage analysis to the proximalregion of Xp (Xp 1 .3),"" the same regionimplicated in typical X linked congenital sta-tionary night blindness with myopia and a formof retinitis pigmentosa. The possibility existsthat OA2, congenital stationary night blind-ness, and retinitis pigmentosa are allelic. Thereis a discrepancy between mapping of OA2 toXpl 1.3 and the finding that a patient with theclinical characteristics of OA2 and Duchennemuscular dystrophy carries a deletion ofXp2 1.3-21.2.65 66 This finding would supportthe presence of an additional locus on the Xchromosome for ocular albinism that closelyresembles OA2.A third form of ocular albinism (OA3) is
inherited as an autosomal recessive disorder.This may be the genetic type found in mostisolated cases of females with ocular albinism.OA3 is phenotypically similar to OA2 exceptthat males and females are equally affected.Deletion analysis of one patient with OA3 haspermitted a tentative chromosomal assignmentto the ql3-ql5 region of chromosome 6.67
Retinitis pigmentosaRetinitis pigmentosa (RP) is a set of geneticdiseases that feature progressive photoreceptordegeneration. Tunnel vision caused by the earlyloss of peripheral photoreceptors is one hall-mark of this disease. As the disease progresses,central vision is lost as well. On examination,middle aged patients with RP classically havefundus changes that include peripheral in-traretinal pigmentation known as bone spic-ules, retinal vessel attenuation, and optic nerve
head pallor. Diagnosis often depends upon fullfield electroretinographic testing, dark ad-aptation threshold testing, and evaluation ofvisual fields. The disease is genetically het-erogeneous and can be inherited as an auto-somal dominant, autosomal recessive, or Xlinked trait. Affected subjects without a familyhistory of RP are designated as isolate or sim-plex cases. Most isolate cases are probablyrecessive cases although some may be X linkedcases or new dominant mutations. Populationsdiffer in the prevalence of each genetic type,but the recessive and isolate types usuallv ac-count for the majority of cases.68 Autosomalrecessive RP in association with hearing less isknown as Usher syndrome and will be discussedseparately. At least 11 chromosomal regionshave been implicated as containing genes caus-ing RP, and four of the genes have been iden-tified. The numerical designation for each locus(for example, RP-1, RP-2, etc) used by McKu-sick in Mendelian inheritance in man (1 1th edi-tion, 1994) and its online version (OMIM)has only categorical significance and does notcorrelate with disease severity, chronologicalorder of gene identification, or population pre-valence.69The first RP locus mapped was for an X
linked form ofthe disease.70 Subsequent linkageand heterogeneity analyses support the ex-istence ofat least two loci on theX chromosomethat are associated with RP.7' These un-identified loci have been designated RP-2 andRP-3. RP-2 was localised within Xpl 1.3-p1 1.22 by polymorphic microsatellite analysis,"2with the most likely position at Xpl 1.23.53The RP-3 locus was localised to Xp21.1 bymultipoint linkage analysis.727' Linkage datafrom a single family was suggestive of a thirdlocus at position Xp2l.3-p2l.2 and designatedRP-6.7' However, deletion mapping data donot support the location of this third locus.74Kaplan et al75 propose that RP-2 and RP-3 canbe distinguished clinically. Patients with RP-2are reported to have early onset night blindnessand severe myopia whereas RP-3 patients havelater onset night blindness and little if anymyopia." Other groups believe that the wideclinical variation in X linked RP makes geneticlocus identification on the basis of clinical fea-tures problematical."Using the candidate gene approach, Dryja et
al778 identified mutations in the rhodopsingene as a cause of autosomal dominant RP.Since these first reports of rhodopsin muta-tions, at least 60 different rhodopsin mutationshave been identified and rhodopsin mutationsare now known to account for about 25% ofautosomal dominant cases.79'-05 The rhodopsinlocus maps to chromosome 3q21-q24 and isdesignated as RP-4.Mutations within the peripherin/RDS gene
were also reported as a cause of autosomaldominant RP.82 1011 The peripherin/RDS genewas selected for screening because mutationsin the homologous mouse gene called rds causesa slow form of retinal degeneration in mice.To date, mutations in the peripherin/RDS geneare estimated to account for approximately3 to 5% of the autosomal dominant cases.
905
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Rosenfeld, McKusick, Amberger, Dryja
Interestingly, different mutations within theperipherin/RDS gene can cause a variety ofclinically distinct disorders including retinitispunctata albescens,"2 vitelliform macular dys-trophy,'08 macular dystrophy,'08 and patternpigment dystrophy of the fovea."3114 Thereis phenotypic variation even within a familysegregating a peripherin/RDS mutation, withaffected relatives in one pedigree having eitherretinitis pigmentosa, pattern dystrophy, orfundus flavimaculatus.'09 The peripherin/RDSgene maps to chromosome 6p21.1-cen"5116and is designated RP-7.A third locus for autosomal dominant RP
has been mapped to the pericentric region ofchromosome 8 between 8p 1 1 and 8q21 .117 Thislocus is designated RP-1 and the gene is notyet identified. Linkage analyses have implicatedunidentified loci on 7p (RP-9) and 7q (RP-10), each assignment based on one autosomaldominant pedigree to date."8 118A 119 A sixthdominant locus (RP-8) has been mapped tochromosome 19q13.4. 120 Linkage exclusion ofall the previously identified loci in one familywith autosomal dominant RP and hearing losssuggests the existence of at least one additionalgene for autosomal dominant RPJ.'2012'There are at least three loci where mutations
can cause autosomal recessive RP. The can-didate gene approach was used to identify thesemutations. Recessive RP can be caused by anull mutation in the rhodopsin gene and bymutations in the I subunit of the rod cGMPphosphodiesterase. 122-125 Additional recessivemutations have been identified in the gene forthe rod cGMP activated channel protein.'26
Retinitis pigmentosa and hearing lossUSHER SYNDROMESThe autosomal recessive forms of retinitis pig-mentosa associated with hearing loss are knownas the Usher syndrome. The Usher syndromeis phenotypically and genetically hetero-geneous. It accounts for about 15% to 20% ofpatients with retinitis pigmentosa and 50% ofpatients with combined deafness and blindness.Patients with Usher syndrome type I have ret-initis pigmentosa, profound congenital sen-sorineural deafness, and vestibular ataxia. Theretinitis pigmentosa usually becomes symp-tomatic within the first two decades of life.Usher syndrome type II is characterised byretinitis pigmentosa, partial acquired hearingimpairment, and no ataxia. The retinitis pig-mentosa usually becomes symptomatic in earlyadulthood. Not only is there non-allelic hetero-geneity between Usher syndrome types I andII, but there is non-allelic heterogeneitywithin each type of Usher syndrome. At leastfive different chromosomal loci have been in-ferred from linkage studies. One locus for Ushersyndrome type I is chromosome 14q32. 1-q32.3based on a study of 10 French families.'27 Thisgenetic form of Usher syndrome is designatedUSHIA. Two additional loci have beenmapped to chromosome 11.28-130 One locus isat position 1 lq13.5 (USH1B) and was foundamong British pedigrees. The other locus wasfound in French-Acadian families and localises
to the interval 1 lpl 5.2-pl4 (USH1C). Somebut not all Usher syndrome type II families arelinked to markers on chromosome 1 betweenlq42-qter (USH2A)."11-"14 A candidate genefor Usher syndrome type II was a cho-roideremia-like (CHML) gene that maps tochromosome 1q42-qter."` Single strand con-formation polymorphism analysis and directsequencing of the CHML gene in patients withUSH2A did not identify any disease specificmutations. The gene responsible for any formof Usher syndrome has not as yet been iden-tified.
Recently, the locus for another form of syn-dromic autosomal recessive RP, the Bardet-Biedl syndrome, was linked to the long armof chromosome 16 between regions q13 andq22.'35136 In addition to retinitis pigmentosa,this disorder is characterised by mental re-tardation, obesity, polydactyly, syndactyly, andhypogonadism. The chromosome 1 6q locuswas excluded from two additional unrelatedfamilies with Bardet-Biedl syndrome. This syn-drome provides yet another example of non-allelic heterogeneity in families with clinicallyindistinguishable diseases.
Retinal dystrophiesCONE DEGENERATIONSCone degenerations can be inherited as auto-somal dominant, autosomal recessive, or Xlinked disorders. The disorders are pheno-typically heterogeneous but usually presentwith decreased central visual acuity, fine nys-tagmus, defective colour vision, and photo-phobia. Unlike the retinitis pigmentosasyndromes, cone degenerations usually presentwith intact peripheral vision and night vision.Night blindness and peripheral field loss candevelop, especially in the cone-rod dystrophies.On examination, these patients may have nor-mal appearing fundi or they may have centralretinal pigment epithelial changes and an as-sociated macular lesion with the appearance ofa bull's eye. The diagnosis usually depends onfull field electroretinographic testing, colourtesting, and dark adaptation threshold testingto evaluate cone function. Using the candidategene approach, Reichel et al'37 identified thefirst genetic mutation responsible for a conedegeneration. In this X linked pedigree, affec-ted males and carrier females were found tohave a 6-5 kb deletion within the red pigmentgene at position Xq28. Another locus for Xlinked cone dysfunction was reportedly mappedby linkage analysis to the region Xp2 1-p11. 1.138 138A A possible locus for an autosomaldominant form ofcone dystrophy was proposedto be on chromosome 6 in the region q25-q26based on the identification of a translocation. 139Another photoreceptor dystrophy involvingboth cones and rods called cone-rod dystrophy(CRD) has been localised to chromosome1 8q2 1.1 -q2 1.3 by deletion mapping of men-tally retarded children with this disorder.'40More recently, Evans et al'4' mapped a locusfor autosomal dominant CRD to chromosome19q13.1-q1 3.2 in another family. A third locuson chromosome 17q has been proposed be-
906
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Recent advances in the gene map of inherited eye disorders
Genetic mapping ofprimary ocular diseases involving the retina, choroid, and vitreousCategory Disorder MIM Mode Location GenelproteinTumours Retinoblastoma 180200 AD 13ql4 RB1: retinoblastoma gene
Colour blindness
Night blindness, congenitalstationary (CSNB)
Ocular albinism (OA)
Retinitis pigmentosa (RP)
RP and congenital hearing loss
Retinal dystrophies
Chorioretinopathies
Vitreoretinopathies
ProtanopiaDeuteranopiaTritanopiaBlue cone monochromatismRod monochromacy, achromatopsiaCSNB, Rhodopsin type
CSNB PDEB type
CSNB with myopiaOA, type 1OA, type 2
OA, type 3RP-1RP-2RP-3RP-4RP-6RP-7-Human homologue of mouse rns
RP-8RP-9RP-10RP-Human homologue of mouse rd
RP-cGMP channel protein-i (CNGC)RP-digenic
Usher syndrome, type IAUsher syndrome, type 1BUsher syndrome, type 1 CUsher syndrome, type 2A*Cone dystrophy*, X linked
Cone dystrophy*, dominantCone-rod dystrophy*
North Carolina macular dystrophyMacular dystrophy, vitelliform, Best
disease*Macular dystrophy, atypical vitelliform typeMacular dystrophy*Patterned dystrophy of the RPE*
Butterfly shaped macular dystrophy*Retinitis punctata albescens*
Fundus flavimaculatus*Macular degeneration, juvenile*,
Stargardt disease (fundus flavimaculatus)
Sorsby's fundus dystrophyCystoid macular dystrophyChoroideremia
Gyrate atrophy of the choroid and retinaFamilial exudative vitreoretinopathy (FEVR)Neovascular inflammatory vitreoretinopathyFEVR, X linkedNorrie diseaseRetinal dysplasia, primaryRetinoschisis, juvenileStickler/Wagner syndromes*
303900303800190900303700216900180380.0031
180072.0005
310500300500300600
203310180100312600312610180380312612179605
180103180104180104180072
12382518072
276900276903276904276901304020
180020120970
XL-RXL-RADXL-RARAD
AD
XL-RXL-RXL-R
ARADXL-RXL-RAD/ARXL-RAD
ADADADAR
ARDigenic
ARARARARXL-R
ADAD
136550 AD153700 AD179605 AD153840 AD179605 AD179605. AD0009
179605. AD0005
179605 AD248200 AR
AD
136900 AD153880 AD303100 XL-R
258870133780193235310600310600312550312700120140
ARADADXL-RXL-RXL-RXL-RAD
Xq28Xq287q31.3-32Xq28143q21-q24
4p 16.3
Xpll.3Xp22.3Xp2l.3-p21.2 orXpl 1.3-p 11.236ql3-ql58p11 -q21Xpl 1.23Xp2 1.13q21-q24Xp2l.3-p21.26p21.1-cen
19q13.47pl5.1-pl37q4pl 6.3
4pl4-ql3llpl3/6p21.1-cen14q321 lq13.5llpl 5.2-pl41 q42-terXq28Xp2l-pll.l6q25-q2618q21-q22.219ql3.1-ql3.217q6ql4-q16.21lql36p21.1-cen8q246p21.1-cen6p21. 1-cen
6p21.1-cen
6p21.1-cenlp2l-pl313q346ql3-ql6.222ql3.1-qter7p2l-pl5Xq2 1.1 -q21.2
1Oq261 lql3.5-q221lql3Xpll.4Xpll.4XpllXp22.2-p22.112ql3.11-ql3
(plO5(Rb))Red cone opsinGreen cone opsinBlue cone opsinRed and green cone opsinsnkRhodopsin (rod opsin)Rod cGMP phosphodiesterase, 13subunitnknknk
nknknknkRhodopsin (rod opsin)nkPeripherin/retinaldegeneration slow (RDS)nknknkRod cGMPphosphodiesterase, ,B-subunitRod cGMP-channel proteinRDMI,Peripherin/RDSnknknknkRed cone opsinnknknknknknknkPeripherin/RDSnkPeripherin/RDSPeripherin/RDSPeripherin/RDS
Peripherin/RDSnknknknknkRAB geranylgeranyltransferase, component AOrnithine aminotransferasenknkNorrie disease proteinNorrie disease proteinnknkCollagen, type II, alpha-l-polypeptide
nk: not known, AD: autosomal dominant, AR: autosomal recessive, XL-R: X linked recessive, *non-allelic heterogeneity, MIM: Mendelian inheritance in man (1lthedition, 1994)
cause one case of CRD also had neuro-fibromatosis type 1.142
MACULAR DYSTROPHIESNorth Carolina macular dystrophy is an auto-somal dominant macular dystrophy with onsetduring infancy. The disease is usually non-progressive. The phenotype is completely pene-trant but the expressivity is highly variable.Generally, the macular lesions are bilateral andsymmetrical. The unidentified locus re-sponsible for this disorder designated MCDR1has been mapped to chromosome 6ql6.'43-'45A distinct macular dystrophy, Best disease
or vitelliform macular dystrophy, is char-acterised by the early onset ofa confluent yellowmass resembling an egg yolk within the macula.Over time, the vitelliform lesion becomes in-creasingly non-confluent and variably pig-
mented with accompanying atrophy of theretinal pigment epithelium. Funduscopicchanges precede visual impairment. Centralvisual loss is progressive. Electro-oculographycan be used to identify affected persons evenbefore the onset of fundus abnormalities. Theunidentified gene responsible for this disorderhas been mapped to chromosome 11qi3 bylinkage analysis.'46 A form of retinal dystrophyknown as atypical vitelliform macular dys-trophy involves the peripheral and peripapillaryretina more extensively than Best disease andthe yellow lesions tend to be smaller. Thisdisease was mapped by linkage analysis to chro-mosome 8q24. 147 A retinal dystrophy withmacular vitelliform lesions similar to Bestdisease has been associated with mutationsin the peripherin/RDS gene.'08113 Other auto-somal dominant retinal dystrophies asso-ciated with mutations in the peripherin/RDS
907
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Rosenfeld, McKusick, Amberger, Dryja
25
2-222
p16
1 13121111
112
14
q 21
2 22
24
3132
34
37
]Stargardt disease
]Usher syndrome, type 2A
25
221
p
141
124
2
2
Retinitis pigmentosa-4Congenital stationarynight blindness
3
Retinitis pigmentosa-7Retinitis pigmentosa, digenicFundus flavimaculatusMacular dystrophy, several typesRetinitis punctata albescens
I- Ocular albinism, type 3-Stargardt diseaseMacular dystrophy, North Carolina type
|}Cone dystrophy, dominant
2 21
p 15
11
1 11
2122
q 22
31
3-,
ThCystoid macular edema
Retinitis pigmentosa-9
Retinitis pigmentosa-10
Tritanopia
232 22
p121111
q 21
2 22
23
24
7
U-Retinitis pigmentosa-1
3]}Macular dystrophy,
atypical vitelliformtype
8
p I111
1214|
q 2 2
22311
34
p IiI
1
11 1
q 2<
31332e
liRetinoblastoma
-Stargardt disease
13
p 1 13
q 1 13}-Cone-rod dystrophy
Retinitis pigmentosa-8
19
)I- Usher syndrome, type 1A
14 Rod monochromacy
p I1 1
11q 1
13
20
36
34
3 32331
2 2221
1 13
1 12
21
2 232425
323241
4 42
44
C
1
222p221
1-1 5
q 21
222-
24
UU
U
Ui5
6
p I1 1=]1
1
q26
15
p 1 1
q2
21
908
I
3
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Recent advances in the gene map of inherited eye disorders
FIGURE 1
p
150 Mb.a
q
16
1 15
1<1321
226
28
31
32
35
4
15
P 11211
1 ia21
q 223
25
]}-Gyrate atrophy of thechoroid and retina
Retinitis pigmentosa,PDEB related
Congenital stationary night15
blindness, type3 P 1
13
-Retinitis pigmentosa,CNCG related
_ 1 13
14
q2_
31
3
~~~~~~~~~~~35
5
15
p 1 14
1
1 13
q223
2 23
10
] Usher syndrome, type 1CyRetinitis pigmentosa, digenic
FMacular dystrophy, Ivitelliform
Neovascular inflammatoryL vitreoretinopathy
sher syndrome, type 1 B~Familial exudative c
vitreoretinopathy
11
13_P 1_
1 1
q 2 -Cone-rod dystrophy
24
17
p ii12
11
13 Sorsby fundus dystrophy
22
p I11
11_
q 1_
y
12 -
q Cone-rod dystrophy
1822 C] Ocular albinism, type 1
2 Retinitis pigrnentosa-6p 21 Retinoschisis, juvenile
einitis pigmentosa-3I FEVR, X-linkedNorrie disease
1 13 LCongenital stationaryJ} nightblindness with myopia
21 " . Cone dystrophy, X-linkedq 1=1 Retinitis pigmentosa-2
2 Ocular albinism, type 2
-25Retinal dysplasia, primary
5 ChoroideremiaBlue cone monochromatism
28 C7 Cone dystrophy, X-linkedDeuteranopia
x Protanopia
THE HUMAN GENE MAP
Primary ocular diseases involvingthe retina, choroid, and vitreous
50 100a i
SCALE(in megabases)
2421
1_-U1 12
212-
2231
3434
9
U
IiUUU
13p 1 12
11
121 13
q 21
2=
13p 1
11 CI 11 z
q 12
24
12
16
I
909
Stickler syndromeI Wagner syndrom
I
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Rosenfeld, McKusick, Amberger, Dryja
gene include butterfly shaped patterndystrophy,'09 113 114 148 macular dystrophy,108 ret-initis punctata albescens,"2 and fundus fla-vimaculatus.'09 An autosomal recessive form offundus flavimaculatus with juvenile onset andsevere progressive visual loss known as Star-gardt disease has recently been mapped to theshort arm of chromosome 1.149150 Autosomaldominant forms of this disease have beenmapped to chromosome 13q34'5' and to thelong arm of chromosome 6 between lociD6S313 (6ql3-ql6.2) and D6S252 (6ql4-qi 6.2). '52 Linkage to the North Carolina mac-ular dystrophy gene on chromosome 6 wasexcluded in this family with autosomal dom-inant Stargardt-like disease.
ChorioretinopathiesCHOROIDEREMIAChoroideremia (CHM), an X linked recessivedisorder, causes constriction of peripheral vis-ion and reduction of night vision. There isprogressive loss of central vision leading toblindness usually in the fourth to fifth decadeof life owing to progressive degeneration of theretina, the retinal pigment epithelium, and thechoroid. While heterozygous women are usu-ally asymptomatic, they may have irregularlypigmented fundi and peripapillary chorioretinalatrophy. Rarely, they may also lose vision. Thedisease locus was mapped to band Xq21 byboth linkage analysis of pedigrees and cyto-genetic analysis ofpatients with detectable chro-mosomal translocations and deletions.153 154
Mutations in a gene encoded within thisregion, the CHM gene, have been identified infamilies with choroideremia. 153-158 The pre-dicted sequence of the putative CHM geneproduct was found to be homologous to abovine protein that inhibits the exchange ofGTP for bound GDP on Rab 3A, known asRab3A-GDP dissociation inhibitor (Rab3A-GDI).'59-'6 Subsequently, the CHM gene wasfound to be homologous to component A ofrat Rab geranylgeranyl transferase.'62 Furthersupport for the function of the CHM geneproduct was obtained by showing functionaldeficiency of Rab geranylgeranyl transferasecomponent A from lymphoblast extracts pre-pared from choroideremia patients.'63 Sup-plementation of these extracts with wild typecomponent A restored normal levels of ger-anylgeranyl transferase activity supporting theconclusion that the choroideremia gene en-codes at least one form of component A.
GYRATE ATROPHYGyrate atrophy is an autosomal recessive retinaldegeneration that is usually diagnosed in latechildhood. The characteristic fundus lesionsare sharply demarcated circular areas of cho-rioretinal atrophy in the periphery of the retina.Early peripapillary atrophy and myopia mayalso be evident. Other clinical findings includeconstricted visual fields, raised dark adaptationthresholds, and small or non-detectable elec-troretinographic responses. During the secondand third decades of life, the scalloped edges
of chorioretinal degeneration progress towardsthe posterior pole. One hallmark of this diseaseis hyperornithaemia which can be partially al-leviated in some patients by the administrationof pyridoxine (vitamin B6). A deficiency of themitochondrial enzyme ornithine aminotrans-ferase (OAT) in patients with gyrate atrophywas first identified by Valle et al. 164 This is oneof the few genetic eye disorders where thediscovery of a biochemical defect precededthe molecular genetic identification ofmutations.161 161 Using cDNA probes encodingOAT, Ramesh et al'67 and Barrett et al'68mapped the gene to chromosome 10q26 andfamily linkage data supported this locus asthe cause of gyrate atrophy.'69170 The OATstructural gene was shown to span 21 kilobasesand encode a 2-2 kilobase mRNA consistingof 11 exons.'7' Numerous mutations within thegyrate atrophy gene have been reported andextensive allelic heterogeneity exists in boththe vitamin B6 responsive and non-responsivephenotypes. 166 172-187 Unlike many hereditaryocular diseases where the defective genes areexpressed primarily in the affected tissues, OATis expressed throughout the body. The reasonsystemic defects in OAT lead specifically todegeneration of the choroid and retina is un-known.
VitreoretinopathiesFAMILIAL EXUDATIVE VITREORETINOPATHY,NEOVASCULAR INFLAMMATORYVITREORETINOPATHY, NORRIE DISEASE, ANDPRIMARY RETINAL DYSPLASIAFamilial exudative vitreoretinopathy (FEVR)can be inherited as an autosomal dominant orX linked recessive disease. The disease showsnearly 100% penetrance but variable ex-pressivity with onset any time from infancy tolate adulthood. FEVR closely resembles ret-inopathy of prematurity but there is no historyof premature birth or oxygen therapy. Thedisease is characterised by incomplete vas-cularisation of the peripheral retina with atyp-ical vessels lying adjacent to a more anterioravascular zone. Retinal exudation, neo-vascularisation, and fibrovascular proliferationdevelop at the periphery followed by tractionand exudative retinal detachments, falciformretinal folds, a "dragged disc" and macula,and vitreous haemorrhage. Patients with FEVRusually reach a stationary stage and total blind-ness is uncommon. A locus for autosomal dom-inant FEVR was mapped by linkage analysisto chromosome 1 1q13.5-q22.`88189 Autosomaldominant neovascular inflammatory vitreo-retinopathy (ADNIV) is another disease char-acterised by traction retinal detachment.Linkage analysis has mapped this disorder tochromosome 1 q 13, the same region as auto-somal dominant FEVR,'90 suggesting thatFEVR and ADNIV are allelic. If so, futureidentification of the locus will be necessary toexplain whyADNIV is a phenotypically distinctdisease characterised by developmentally nor-mal retinal vessels. Other clinical character-istics that distinguish ADNIV from FEVRinclude ocular inflammation, retinal and iris
910
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Recent advances in the gene map of inherited eye disorders
neovascularisation, cystoid macular oedema,fundus pigmentation, and a selective loss ofthe ERG B wave.When compared to autosomal dominant
FEVR, the X linked recessive form of FEVRusually has an earlier onset of symptoms. Theadult female gene carriers show no evidence ofdisease. Fullwood et all9" identified a familywith X linked FEVR and mapped the re-sponsible locus by linkage analysis to eitherXq21.3 or Xpll.4-11.3. The Xpll.4-11.3region also contains the Norrie disease genewhich has been cloned.'92193 Norrie disease isan X linked recessive disorder characterised byretinal dysplasia followed by retinal detachmentand blindness. Norrie disease is a neuro-developmental disorder associated with otherocular abnormalities such as microphthalmia,cataract, corneal opacities, congenital blind-ness, and bulbar atrophy. Extraocular mani-festations include progressive sensorineuralhearing loss and variable degrees of mentalretardation. The Norrie disease gene encodesa mucin-like protein with a tertiary structuresimilar to that of transforming growth factor194 and mutations within this gene have beenidentified in families with Norrie disease.19,5200Surprisingly, a point mutation within this Nor-rie disease gene was found to cosegregate in afamily with X linked FEVR studied by Chenet al.20'l This finding suggests that the genes forX linked FEVR and Norrie disease are allelic,and once again shows the phenomenon of"gene sharing" between phenotypically distinctdiseases. Another disease known as primaryretinal dysplasia also has a tight linkage re-lationship with the Norrie disease locus.202 LikeFEVR and Norrie disease, primary retinal dys-plasia is an X linked recessive disorder char-acterised by retinal detachment. The raisedretinal fold characteristic of primary retinaldysplasia arises from the optic disc and involvesthe macula as it extends to the temporal fundus.Mutations responsible for primary retinal dys-plasia have not as yet been reported.
JUVENILE RETINOSCHISISJuvenile retinoschisis (RS) is an X linked re-cessive disorder characterised by cystic de-generation of the peripheral and central retinaresulting in the splitting of the nerve fibre layer.A cystic maculopathy with a stellate appearanceis a characteristic finding in affected males.Phenotypic expression is highly variable butonset is usually during infancy and there is aslow deterioration throughout life with mildvisual impairment until after the age of 40. Thedisease progresses to retinal detachment, retinalatrophy, choroidal sclerosis, and possibly totalblindness. Vasculature abnormalities and vit-reous degeneration are associated features. Fe-male carriers of this disease are usuallyasymptomatic. Multipoint linkage analysis hasbeen used to map the gene responsible for thisdisease to within the Xp22.1-22.2 locus.20"208It is not known at this time if the variableexpressivity of this disease can be explained onthe basis of allelic heterogeneity, as the genehas not been identified.
WAGNER VITREORETINAL DEGENERATIONWagner syndrome is an autosomal dominantdisorder that has the same ocular features asStickler syndrome but none of the non-ocularmanifestations. Wagner syndrome is char-acterised by degeneration of the vitreous geland the retina. These patients appear to havean optically empty vitreous cavity on slit lampbiomicroscopy. Other associated ocular fea-tures include retinal detachment, myopia, andcataract. Stickler syndrome has the additionalfeatures of progressive arthropathy, cranio-oro-facial abnormalities, and deafness. It is unclearwhether the Wagner and Stickler syndromesshould be considered two distinct clinical dis-orders or whether they represent variable ex-pressivity of one disease. This debate has beencomplicated by the fact that Stickler syndromeis a genetically heterogeneous disease. Somefamilies with Stickler syndrome have defects inthe COL2A1 gene that encodes for type II aprocollagen.209214 However, about half of thefamilies reported so far with Stickler syndromedo not show cosegregation with the COL2A1locus.215-218 To confuse the issue further, onefamily with Wagner syndrome has been ex-cluded from the COL2A1 locus216 and anotherfamily has been linked to the COL2A1 locus.219Korkko et al219 proposed that premature ter-mination mutations within the COL2A1 genemay cause the more severe Stickler syndromewhile certain amino acid substitutions maycause a milder phenotype like Wagner syn-drome. The extent of the relationship betweenthe Stickler and Wagner syndromes remains tobe resolved.
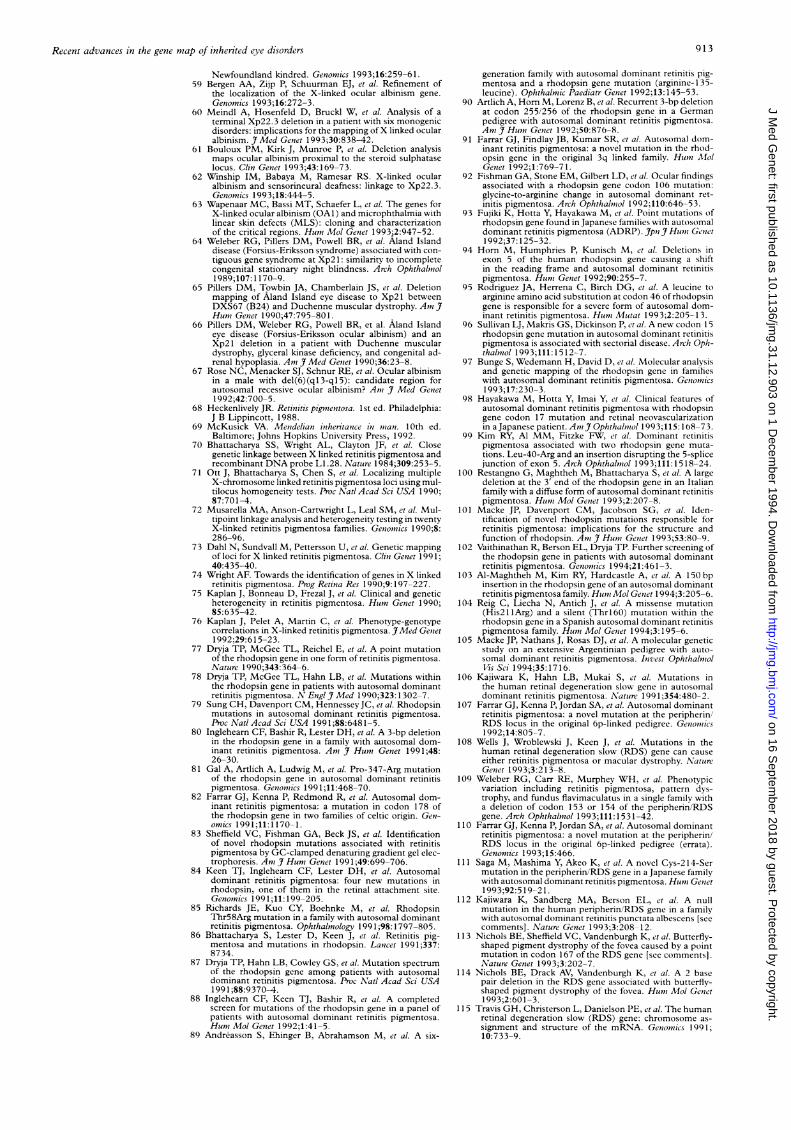
ConclusionThe primary genetic disorders of the retina,choroid, and vitreous discussed in this revieware summarised along with their MIM (Men-delian inheritance in man) number in the ac-companying table and idiograms. If a locus hasbeen identified as a cause for a disorder, theMIM number for that disease is assigned ac-cording to the identified disease gene. Thephenomenon of locus or non-allelic hetero-geneity can be appreciated in the table bythe different MIM numbers and genes that areassigned to the same clinical disorder. Theprevalence of "gene sharing" allelism betweenclinically distinct disorders is evident by therepeated reference to the same gene or MIMnumber for different diseases and the presenceof grouped disorders adjacent to a chro-mosomal location in the idiograms. Thissummary shows a genetic complexity to themapping ofocular disorders that could not havebeen appreciated by using clinical classificationschemes alone.
Note added in proofSince this review was submitted, several note-worthy chromosomal loci associated with pos-terior segment ocular disorders have beenpublished. A digenic form of retinitis pig-mentosa was reported in three unrelated fam-ilies.220 In these families, affected subjects weredouble heterozygotes with mutations in the
911
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Rosenfeld, McKusick, Aniberger, Dryja
unlinked peripherin/RDS and ROMI genes.
A heterozygous missense mutation in the rodcGMP phosphodiesterase P-subunit genes was
reported to cosegregate with autosomal dom-inant stationary night blindness in one family.22'The Bardet-Biedl syndrome was mapped to a
second locus on chromosome lq.222 An auto-somal dominant macular degeneration knownas Sorsby's fundus dystrophy was mapped tochromosome 22q13-qter.223 The locus forautosomal dominant cystoid macular dys-trophy was mapped to chromosome 7p 15-p2 1.224
1 Tramboli A, Marvin JP, Horm JW. The incidence of ret-inoblastoma in the United States: 1974 through 1985.Arch Ophthalmol 1990;108:128-32.
2 Toguchida J, McGee TL, Paterson JC, et al. Completegenomic sequence of the human retinoblastoma sus-ceptibility gene. Genonmics 1993;17:535-43.
3 Dunn JM, Phillips RA, Becker AJ, et al. Identification ofgermline and somatic mutations affecting the ret-inoblastoma gene. Scienice 1988;241:1797-800.
4 Dunn JM, Phillips RA, Zhu X, et al. Mutations in the RBIgene and their effects on transcription. Mol Cell Biol 1989;9:4596-604.
5 Yandell DW, Campbell TA, Dayton SH, et al. Oncogenicpoint mutations in the human retinoblastoma gene: theirapplication to genetic counseling. N Engl Y Med 1989;321:1689-95.
6 Sakai T, Toguchida J, Ohtani N, et al. Allele-specifichypermethylation of the retinoblastoma tumor-suppressorgene. Amn Y Hunm Genet 1991;48:880-8.
7 Hashimoto T, Takahashi R, Yandell DW, et al. Char-acterization of intragenic deletions in two sporadic ger-minal mutation cases of retinoblastoma resulting inabnormal gene expression. Oncogene 1991;6:463-9.
8 Kloss K, Wahrisch P, Greger V, et al. Characterization ofdeletions at the retinoblastoma locus in patients withbilateral retinoblastoma [see comments]. Amn YMed Genet199 1;39: 196-200.
9 Hogg A, Onadim Z, Baird PN, et al. Detection of hetero-zygous mutations in the RBI gene in retinoblastomapatients using single-strand conformation polymorphismanalysis and polymerase chain reaction sequencing. On-cogenie 1992;7:1445-51.
10 Lohmann D, Horsthemke B, Gillessen-Kaesbach G, et al.Detection of small RB 1 gene deletions in retinoblastomaby multiplex PCR and high-resolution gel electrophoresis.Huml Genet 1992;89:49-53.
11 Hogg A, Bia B, Onadim Z, et al. Molecular mechanismsof oncogenic mutations in tumors from patients withbilateral and unilateral retinoblastoma. Proc NatlAcad SciUSA 1993;90:7351-5.
12 Blanquet V, Turleau C, Gross MS, et al. Identification ofgermline mutations in the RB1 gene by denaturant gra-dient gel electrophoresis and polymerase chain reactiondirect sequencing. Hum Mol Genet 1993;2:975-9.
13 Janson M, Nordenskj6ld M. A constitutional mutationwithin the retinoblastoma gene detected by PFGE. ClinGeniet 1994;45:5-10.
14 Sakai T, Ohtani N, McGee TL, et al. Oncogenic germ-line mutations in Spl and ATF sites in the human retino-blastoma gene. Nature 1991 ;353:83-6.
15 Onadim Z, Hogg A, Baird PN, et al. Oncogenic pointmutations in exon 20 of the RB 1 gene in families showingincomplete penetrance and mild expression of the ret-inoblastoma phenotype. Proc Natl Acad Sci USA 1992;89:6177-81.
16 Munier FL, Wang MX, Spence A, et al. Pseudo lowpenetrance in retinoblastoma. Arch Ophthalmol 1993;111:1507-11.
17 Dryja TP, Rapaport J, McGee TL, et al. Molecular etiologyof low-penetrance retinoblastoma in two pedigrees. AnmY Humn Genet 1993;52:1122-8.
18 Nathans J, Thomas D, Hogness DS Molecular genetics ofhuman color vision: the genes encoding blue, green, andred pigments. Science 1986;232: 193-202.
19 Vollrath D, Nathans J, Davis R. Tandem array of humanvisual pigment genes at Xq28. Science 1988;240: 1669-72.
20 Feil R, Aubourg P, Helig R, et al. A 195-kb cosmid walkencompassing the human Xq28 color vision pigmentgenes. Genomics 1990;6:367-73.
21 Nathans J, Piantanida TP, Eddy RL, et al. Moleculargenetics of inherited variation in human color vision.Science 1986;232:203-10.
22 Nathans J, Merbs SL, Sung CH, et al. Molecular geneticsof human visual pigments. Annu Rev Genet 1992;26:403-24.
23 Winderickx J, Battisti L, Hibiya Y, et al. Haplotype diversityin the human red and green opsin genes: evidence for
sequence exchange in exon 3. Huml Mol Genet 1993;2:1413-21.
24 Winderickx J, Battisti L, Motulsky AG, et al. Selective
expression of human X chromosome-linked green opsingenes. Proc Natl Acad Sci USA, 1992;89:9710-4.
25 Drummond-Borg M, Deeb S, Motulsky AG. Molecularbasis of abnormal red-green color vision: a family with
three types of color vision defects. Amn_JHunm Geniet 1988;43:675-83.
26 Neitz M, Neitz J, Jacobs GH. Analysis of fusion gene andencoded photopigment of colour-blind humans. Nature1989;342:679-82.
27 Deeb SS, Lindsey DT, Hibiya Y, et al. Genotype-phenotyperelationships in human red/green color-vision defects:molecular and psychophysical studies. Ami _7 Hum11 Geniet1992;51:687-700.
28 Zhang Q, Mao W, Ma Q, et al. Molecular basis ofcongenitalcolor vision defects in Chinese patients. Jpn 7 Ophthal/mol1992;36:479-87.
29 Winderickx J, Sanocki E, Lindsey DT, et al. Defectivecolour vision associated with a missense mutation in thehuman green visual pigment gene. Nature Genet 1992;1:251-6.
30 Oprian DD, Asenjor AB, Lee N, et al. Design, chemicalsynthesis, and expression of genes for the three humancolor vision pigments. Biochempistry 1991 ;30: 11367-72.
31 Merbs SL, Nathans J. Absorption spectra of the hybridpigments responsible for anomalous color vision. Sci'ence1992;258:464-6.
32 Merbs SL, Nathans J. Absorption spectra of human conepigments. Nature 1992;356:433-5.
33 Winderickx J, Lindsey DT, Sanocki E, et al. Polymorphismin red photopigment underlies variation in colour match-ing. Nature 1992;356:431-3.
34 Neitz J, Neitz M, Jacobs GH. More than three differentcone pigments among people with normal color vision.VisionI Res 1993;33:117-22.
35 Hess RF, Mullen KT, Sharpe LT, et al. The photoreceptorsin atypical achromotopsia. I Phvsiol 1989;417:123-49.
36 Reitner A, Sharpe LT, Zrenner E. Is colour vision possiblewith only rods and blue sensitive cones? Nature 1991;352:798-800.
37 Nathans J, Davenport CM, Maumenee IH, et al. Moleculargenetics of human blue cone monochromacy. Scienice1989;245:831-8.
38 Nathans J, Maumenee IH, Zrenner E, et al. Genetic het-erogeneity among blue-cone monochromats. Am _7 HumiGeniet 1993;53:987-1000.
39 Wang Y, Macke JP, Merbs SL, et al. A locus control regionadjacent to the human red and green visual pigmentgenes. Neuroni 1992;9:429-40.
40 Fitzgibbon J, Appukuttan B, Gayther S, et al. Localisationof the human blue cone pigment gene to chromosomeband 7q31.3-32. Hunm Genet 1994;93:79-80.
41 Weitz CJ, Miyake Y, Shinzato K, et al. Human tritanopiaassociated with two amino acid substitutions in the blue-sensitive opsin. Am71 _ Huml Geniet 1992;50:498-507.
42 Weitz CJ, Went LN, Nathans J. Human tritanopia as-sociated with a third amino acid substitution in the blue-sensitive visual pigment. AmnJHunm Genet 1992;51:444-6.
43 Falls HF, Wolter JR, Alpern M. Typical total mono-chromacy - a historical and psychophysical study. ArchOphthalmol 1965;74:610-16.
44 Pentao L, Lewis RA, Ledbetter DH, et al. Maternal uni-parental isodisomy of chromosome 14: association withautosomal recessive rod monochromacy. Amin_J Humsl Genet1992;50:690-9.
45 Sieving PA, Richards JE, Bingham EL, et al. Dominantcongenital complete nystalopia and Gly9OAsp rhodopsinmutation. Inivest Ophthalnol Iis Sci 1992;33:1397.
46 Dryja TP, Berson EL, Rao VR, et al. Heterozygous missensemutation in the rhodopsin gene as a cause of congenitalstationary night blindness. Nature Genet 1993;4:280-3.
47 Rao VK, Cohen GB, Oprian DD. Rhodopsin mutationG90D and a molecular mechanism for congenital nightblindness. Nature 1994;367:639-42.
48 Musarella MA, Weleber RG, Murphey WH, et al. As-signment of the gene for complete X-linked congenitalstationary night blindness (CSNBI) to chromosomeXpll.3. Genomiics 1989;5:727-37.
49 Aldred MA, Dry KL, Sharp DM, et al. Linkage analysis inX-linked congenital stationary night blindness. Genonjics1992;14:99-104.
50 Bech-Hansen NT, Moore BJ, Pearce WG. Mapping oflocus for X-linked congenital stationary night blindness(CCNB1) proximal to DXS7. Genomics 1992;12:409-1 1.
51 Dry KL, Van DD, Aldred MA, et al. Linkage analysis ina family with complete type congenital stationary nightblindness with and without myopia. Clin Genet 1993;43:250-4.
52 Coleman M, Bhattacharya S, Lindsay S, et al. Localizationof the microsatellite probe DXS426 between DXS7 andDXS255 on Xp and linkage to X-linked retinitis pig-mentosa. Anm 7 Hunm Genet 1990;47:935-40.
53 Wright AF, Bhattacharya SS, Aldred MA, et al. Geneticlocalisation of the RP2 type of X linked retinitis pig-mentosa in a large kindred. _JMed Genet 199 1;28:453-7.
54 Schwartz M, Rosenberg T. Aland eye disease: linkage data.Genomtics 1991;10:327-32.
55 Alitalo T, Kruse TA, Forsius H, et al. Localization of theAland Island eye disease locus to the pericentromericregion of the X chromosome by linkage analysis. Am 7Hum Genet 1991;48:31-8.
56 Glass IA, Good P, Coleman MP, et al. Genetic mappingof a cone and rod dysfunction (Aland eye disease) to theproximal short arm of the human X chromosome. . MedGenet 1993;30:1044-50.
57 Charles SJ, Green JS, Grant JW, et al. Clinical featuresof affected males with X linked ocular albinism. Br _7Ophthalnol 1993;77:222-7.
58 Charles SJ, Green JS, Moore AT, et al. Genetic mappingof X-linked ocular albinism: linkage analysis in a large
912
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from
Recent advances in the gene map of inherited eye disorders
Newfoundland kindred. Genomics 1993;16:259-61.59 Bergen AA, Zijp P, Schuurman EJ, et al. Refinement of
the localization of the X-linked ocular albinism gene.Genomics 1993;16:272-3.
60 Meindl A, Hosenfeld D, Bruckl W, et al. Analysis of aterminal Xp22.3 deletion in a patient with six monogenicdisorders: implications for the mapping ofX linked ocularalbinism. .7 Med Genet 1993;30:838-42.
61 Bouloux PM, Kirk J, Munroe P, et al. Deletion analysismaps ocular albinism proximal to the steroid sulphataselocus. Clin Genet 1993;43:169-73.
62 Winship IM, Babaya M, Ramesar RS. X-linked ocularalbinism and sensorineural deafness: linkage to Xp22.3.Genonmics 1993;18:444-5.
63 Wapenaar MC, Bassi MT, Schaefer L, et al. The genes forX-linked ocular albinism (OA1) and microphthalmia withlinear skin defects (MLS): cloning and characterizationof the critical regions. Hun, Mol Genet 1993-2:947-52.
64 Weleber RG, Pillers DM, Powell BR, et al. Aland Islanddisease (Forsius-Eriksson syndrome) associated with con-tiguous gene syndrome at Xp2 1: similarity to incompletecongenital stationary night blindness. Arch Ophthatmol1989;107:1 170-9.
65 Pillers DM, Towbin JA, Chamberlain JS, et al. Deletionmapping of Aland Island eye disease to Xp21 betweenDXS67 (B24) and Duchenne muscular dystrophy. AnmHun, Genet 1990;47:795-801.
66 Pillers DM, Weleber RG, Powell BR, et al. Aland Islandeye disease (Forsius-Eriksson ocular albinism) and anXp21 deletion in a patient with Duchenne musculardystrophy, glyceral kinase deficiency, and congenital ad-renal hypoplasia. An, _7 Med Ge,,et 1990;36:23-8.
67 Rose NC, Menacker SJ, Schnur RE, et al. Ocular albinismin a male with del(6)(q13-ql5): candidate region forautosomal recessive ocular albinism? Ani _7 Med Genet1992;42:700-5.
68 Heckenlively JR. Retinitis piginentosa. 1st ed. Philadelphia:J B Lippincott, 1988.
69 McKusick VA. Metndelian inhenrtance in n,an. 10th ed.Baltimore; Johns Hopkins University Press, 1992.
70 Bhattacharya SS, Wright AL, Clayton JF, et al. Closegenetic linkage between X linked retinitis pigmentosa andrecombinant DNA probe L1.28. Nature 1984;309:253-5.
71 Ott J, Bhattacharya S, Chen S, et al. Localizing multipleX-chromosome linked retinitis pigmentosa loci using mul-tilocus homogeneity tests. Proc Natl Acad Sci USA 1990;87:701-4.
72 Musarella MA, Anson-Cartwright L, Leal SM, et al. Mul-tipoint linkage analysis and heterogeneity testing in twentyX-linked retinitis pigmentosa families. Genonmics 1990,8:286-96.
73 Dahl N, Sundvall M, Pettersson U, et al. Genetic mappingof loci for X linked retinitis pigmentosa. Clinl Geniet 1991;40:435-40.
74 Wright AF. Towards the identification of genes in X linkedretinitis pigmentosa. Prog Retina Res 1990;9:197-227.
75 Kaplan J, Bonneau D, Frezal J, et al. Clinical and geneticheterogeneity in retinitis pigmentosa. Humen Genet 1990;85:635-42.
76 Kaplan J, Pelet A, Martin C, et al. Phenotype-genotypecorrelations in X-linked retinitis pigmentosa. ]7Med Genet1992;29:615-23.
77 Dryja TP, McGee TL, Reichel E, et al. A point mutationof the rhodopsin gene in one form of retinitis pigmentosa.Nature 1990;343:364-6.
78 Dryja TP, McGee TL, Hahn LB, et al. Mutations withinthe rhodopsin gene in patients with autosomal dominantretinitis pigmentosa. N Engl t Med 1990;323: 1302-7.
79 Sung CH, Davenport CM, Hennessey JC, et al. Rhodopsinmutations in autosomal dominant retinitis pigmentosa.Proc Natl Acad Sci USA 1991;88:6481-5.
80 Ingleheam CF, Bashir R, Lester DH, et al. A 3-bp deletionin the rhodopsin gene in a family with autosomal dom-inant retinitis pigmentosa. Anm Hunm Genet 1991;48:26-30.
81 Gal A, Artlich A, Ludwig M, et al. Pro-347-Arg mutationof the rhodopsin gene in autosomal dominant retinitispigmentosa. Genon,ics 1991;11:468-70.
82 Farrar GJ, Kenna P, Redmond R, et al. Autosomal dom-inant retinitis pigmentosa: a mutation in codon 178 ofthe rhodopsin gene in two families of celtic origin. Gen-omics 1991;11:1170-1.
83 Sheffield VC, Fishman GA, Beck JS, et al. Identificationof novel rhodopsin mutations associated with retinitispigmentosa by GC-clamped denaturing gradient gel elec-trophoresis. Am Hun, Genet 199 1;49:699-706.
84 Keen TJ, Ingleheam CF, Lester DH, et al. Autosomaldominant retinitis pigmentosa: four new mutations inrhodopsin, one of them in the retinal attachment site.Genomnics 1991;11:199-205.
85 Richards JE, Kuo CY, Boehnke M, et al. RhodopsinThr58Arg mutation in a family with autosomal dominantretinitis pigmentosa. Ophthaltmology 1991 ;98: 1797-805.
86 Bhattacharya S, Lester D, Keen J, et al. Retinitis pig-mentosa and mutations in rhodopsin. Lancet 1991;337:8734.
87 Dryja TP, Hahn LB, Cowley GS, et al. Mutation spectrumof the rhodopsin gene among patients with autosomaldominant retinitis pigmentosa. Proc Nartl Acad Sci USA1991;88:9370-4.
88 Inglehearn CF, Keen TJ, Bashir R, et al. A completedscreen for mutations of the rhodopsin gene in a panel ofpatients with autosomal dominant retinitis pigmentosa.Hun, Mol Genet 1992;1:41-5.
89 Andreasson S, Ehinger B, Abrahamson M, et al. A six-
generation family with autosomal dominant retinitis pig-mentosa and a rhodopsin gene mutation (arginine-135-leucine). Ophthalnic Paediatr Genet 1992;13:145-53.
90 Artlich A, Hom M, Lorenz B, et al. Recurrent 3-bp deletionat codon 255/256 of the rhodopsin gene in a Germanpedigree with autosomal dominant retinitis pigmentosa.Anm_JHutmi Geniet 1992;50:876-8.
91 Farrar GJ, Findlay JB, Kumar SR, et al. Autosomal dom-inant retinitis pigmentosa: a novel mutation in the rhod-opsin gene in the original 3q linked family. Huin MfolGenet 1992;1:769-71.
92 Fishman GA, Stone EM, Gilbert LD, et al. Ocular findingsassociated with a rhodopsin gene codon 106 mutation:glycine-to-arginine change in autosomal dominant ret-initis pigmentosa. Arch Ophthaltnol 1992;110:646-53.
93 Fujiki K, Hotta Y, Hayakawa M, et al. Point mutations ofrhodopsin gene found in Japanese families with autosomaldominant retinitis pigmentosa (ADRP). Jpn _7 Hun,l Geiet1 992;37: 125-32.
94 Horn M, Humphries P, Kunisch M, et al. Deletions inexon 5 of the human rhodopsin gene causing a shiftin the reading frame and autosomal dominant retinitispigmentosa. Hunm Genet 1992;90:255-7.
95 Rodriguez JA, Herrena C, Birch DG, et al. A leucine toarginine amino acid substitution at codon 46 of rhodopsingene is responsible for a severe form of autosomal dom-inant retinitis pigmentosa. Humrz Mutat 1993;2:205-13.
96 Sullivan LJ, Makris GS, Dickinson P, et al. A new codon 15rhodopsin gene mutation in autosomal dominant retinitispigmentosa is associated with sectorial disease. Arch Oph-thaltiol 1993;111:1512-7.
97 Bunge S, Wedemann H, David D, et al. Molecular analysisand genetic mapping of the rhodopsin gene in famitieswith autosomal dominant retinitis pigmentosa. Getnon,ics1993;17:230-3.
98 Hayakawa M, Hotta Y, Imai Y, et al. Clinical features ofautosomal dominant retinitis pigmentosa with rhodopsingene codon 17 mutation and retinal neovascularizationin aJapanese patient. Am] Ophthaltmot 1993;115:168-73.
99 Kim RY, Al MM, Fitzke FW, et al. Dominant retinitispigmentosa associated with two rhodopsin gene muta-tions. Leu-40-Arg and an insertion disrupting the 5-splicejunction of exon 5. Arch Ophthaltmol 1993;lll:1518-24.
100 Restangno G, Maghtheh M, Bhattacharya S, et al. A largedeletion at the 3' end of the rhodopsin gene in an Italianfamily with a diffuse form of autosomal dominant retinitispigmentosa. Hum" Mol Genet 1993;2:207--8.
101 Macke JP, Davenport CM, Jacobson SG, et al. Iden-tification of novel rhodopsin mutations responsible forretinitis pigmentosa: implications for the structure andfunction of rhodopsin. Am]i_f Humii Getnet 1993;53:80-9.
102 Vaithinathan R, Berson EL, Dryja TP. Further screening ofthe rhodopsin gene in patients with autosomal dominantretinitis pigmentosa. Genomzlics 1994;21:461-3.
103 Al-Maghtheh M, Kim RY, Hardcastle A, et al. A 150 bpinsertion in the rhodopsin gene of an autosomal dominantretinitis pigmentosa family. Humn Mol Genzet 1994;3:205-6.
104 Reig C, Liecha N, Antich J, et al. A missense mutation(His2l IArg) and a silent (Thrl60) mutation within therhodopsin gene in a Spanish autosomal dominant retinitispigmentosa family. Humi Mol Geiet 1994;3:195-6.
105 Macke JP, Nathans J, Rosas DJ, et al. A molecular geneticstudy on an extensive Argentinian pedigree with auto-somal dominant retinitis pigmentosa. Invest OphthaltmolIis Sci 1994;35:17 16.
106 Kaiiwara K, Hahn LB, Mukai S, et al. Mutations inthe human retinal degeneration slow gene in autosomaldominant retinitis pigmentosa. Natiure 1991;354:480- 2.
107 Farrar GJ, Kenna P, Jordan SA, et al. Autosomal dominantretinitis pigmentosa: a novel mutation at the peripherin/RDS locus in the original 6p-linked pedigree. Genomics1 992;14:805-7.
108 Wells J, Wroblewski J, Keen J, et al. Mutations in thehuman retinal degeneration slow (RDS) gene can causeeither retinitis pigmentosa or macular dystrophy. NatureGenet 1993;3:213-8.
109 Weleber RG, Carr RE, Murphey WH, et al. Phenotypicvariation including retinitis pigmentosa, pattern dys-trophy, and fundus flavimaculatus in a single family witha deletion of codon 153 or 154 of the peripherin/RDSgene. Arch Ophthaltmol 1993;111:1531-42.
110 Farrar GJ, Kenna P, Jordan SA, et al. Autosomal dominantretinitis pigmentosa: a novel mutation at the peripherin/RDS locus in the original 6p-linked pedigree (errata).Genonzics 1993;15:466.
111 Saga M, Mashima Y, Akeo K, et al. A novel Cys-214-Sermutation in the peripherin/RDS gene in a Japanese familywith autosomal dominant retinitis pigmentosa. Humn Genet1993;92:5 19-2 1.
112 Kajiwara K, Sandberg MA, Berson EL, et al. A nullmutation in the human peripherin/RDS gene in a familywith autosomal dominant retinitis punctata albescens [seecomments]. Nature Genet 1993;3:208-12.
113 Nichols BE, Sheffield VC, Vandenburgh K, et al. Butterfly-shaped pigment dystrophy of the fovea caused by a pointmutation in codon 167 of the RDS gene [sec commentsj.Nature Genet 1993;3:202-7.
114 Nichols BE, Drack AV, Vandenburgh K, et al. A 2 basepair deletion in the RDS gene associated with butterflv-shaped pigment dystrophy of the fovea. Hum71Mol Genet1 993;2:60 1-3.
115 Travis GH, Christerson L, Danielson PE, etal. The humanretinal degeneration slow (RDS) gene: chromosome as-signment and structure of the mRNA. Genomics 1991;10:733-9.
913
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Rosenfeld, McKusick, Amberger, Dryja
116 Jordan SA, Farrar GJ, Kumar SR, et al. Autosomal dom-inant retinitis pigmentosa (adRP; RP6): cosegregation ofRP6 and the peripherin-RDS locus in a late-onset familyof Irish origin. Am J Hum Genet 1992;50:634-9.
117 Blanton SH, Heckenlively JR, Cottingham AW, et al. Link-age mapping of autosomal dominant retinitis pigmentosa(RP1) to the pericentric region of human chromosome8. Genomics 1991;11:857-69.
118 Inglehearn CF, Carter SA, Keen TF, et al. A new locus forautosomal dominant retinitis pigmentosa on chromosome7p Nature Genet 1993;4:51-3.
118A Inglehearn CF, Keen TJ, Al-Maghtheh M, et al. Furtherrefinement of the location for autosomal dominant ret-initis pigmentosa on chromosome 7p (RP9). Am J HumGenet 1994;54:675-80.
119 Jordan SA, Farrar GJ, Kenna P, et al. Localization of anautosomal dominant retinitis pigmentosa gene to chro-mosome 7q. Nature Genet 1993;4:54-8.
120 Al-Maghtheh M, Inglehearn CF, Keen TJ, et al. Iden-tification of a sixth locus for autosomal dominant retinitispigmentosa on chromosome 19. Hum Mol Genet 1994;3:351-4.
121 Kumar-Singh R, Farrar GJ, Mansergh F, et al. Exclusionof the involvement of all known retinitis pigmentosa lociin the disease present in a family of Irish origin providesevidence for a sixth autosomal dominant locus (RP8).Hum Mol Genet 1993;2:875-8.
122 Rosenfeld PJ, Cowley GS, McGee TL, et al. A Null muta-tion in the rhodosin gene causes rod photoreceptor dys-function and autosomal recessive retinitis pigmentosa.Nature Genet 1992;1:209-13.
123 McLaughlin ME, Sandberg MA, Berson EL, et al. Re-cessive mutations in the gene encoding the beta-subunitof rod phosphodiesterase in patients with retinitis pig-mentosa. Nature Genet 1993;4:130-4.
124 McLaughlin ME, Ehrhart TL, Sandberg MA, et al. Mut-ations in the beta subunit of rod phosphodiesterase inpatients with autosomal recessive retinitis pigmentosa.Invest Ophthalmol Vis Sci 1994;35:1718.
125 Rosenfeld PJ, Hahn LB, Miller S, et al. A rhodopsin splicesite mutation: recessive or dominant? Invest OphthalmolJ/s Sci 1994;35:1478.
126 McGee TL, Lin D, Berson EL, et al. Defects in therod cGMP-gated channel gene in patients with retinitispigmentosa. Invest Ophthalmol Vis Sci 1994;35: 1716.
127 Kaplan J, Gerber S, Bonneau D, et al. A gene for Ushersyndrome type I (USHIA) maps to chromosome 14q.Genomics 1992;14:979-87.
128 Smith RJH, Lee EC, Kimberling WJ, et al. Localization oftwo genes for Usher syndrome type I to chromosome 11.Genomics 1992;14:995-1002.
129 Kimberling WJ, Moller CG, Davenport S, et al. Linkageof Usher syndrome type I gene (USH 1 B) to the long armof chromosome 11. Genomics 1992;14:988-94.
130 Ayyagari R, Smith RJH, Polymeropoulos M, et al. Linkageand haplotype analysis and physical mapping of theUSHIC gene. Invest Ophthalmol 1is Sci 1994;35:2143.
131 Kimberling WJ, Weston MD, Moller C, et al. Localizationof Usher syndrome type II to chromosome lq. Genomics1990;7:245-9.
132 Lewis RA, Otterud B, Stauffer D, et al. Mapping recessiveophthalmic diseases: linkage of the locus for Usher syn-drome type II to a DNA marker on chromosome 1 q.Genomics 1990;7:250-6.
133 Bokhoven HV, Genderen CV, Molloy CM, et al. Mappingof the choroideremia-like (CHML) gene at lq42-qterand mutation analysis in patients with Usher syndrometype II. Genomics 1994;19:385-7.
134 Pieke Dahl S, Kimberling WJ, Gorin MB, et al. Geneticheterogeneity of Usher syndrome type II. 7 Med Genet1993;30:843-8.
135 Kwitek-Black AE, Carmi R, Duyk GM, et al. Linkage ofBardet-Biedl syndrome to chromosome 16q and evidencefor non-allelic heterogeneity. Nature Genet 1993;5:392-6.
136 Sheffield VC, Kwitek-Black A, Carmi R, et al. Homo-zygosity mapping of the gene for Bardet-Biedl syndromein large inbred families. Invest Ophthalmol 1is Sci 1994;35:1718.
137 Reichel E, Bruce AM, Sandberg MA, et al. An elec-troretinographic and molecular genetic study of X-linkedcone degeneration. Am 7 Ophthalmol 1989;108:540-7.
138 Bartley J, Gies C, Jacobsen D. Cone dystrophy (X-linked)(CODI) maps between DXS7(L1.28) and DXS206(XJl. l) and is linked to DXS84(754). Cytogenet Cell Genet1989;51:959.
138A Meire FM, Bergen AAB, De Rouck A, et al. X linkedprogressive cone dystrophy: localization of the gene locusto Xp2 1-p 11 .1 by linkage analysis. Br3'Ophthalmol 1994;78:103-8.
139 Tranebjaerg L, Sjo 0, Warburg M. Retinal cone dys-function and mental retardation associated with a de novobalanced translocation 1;6 (q44;q27). Ophthal PaediatrGenet 1986;7:167-73.
140 Warburg M, Sjo 0, Tranebjaerg L, et al. Deletion of aretinal cone-rod dystrophy: assignment to 18q21 1. Am JMed Genet 1991;39:288-93.
141 Evans K, Fryar A, Inglehearn C, et al. Genetic linkageof cone-rod retinal dystrophy to chromosome 19q andevidence for segregation distortion. Nature Genet 1994;6:210-13.
142 Kylstra JA, Aylsworth AS. Cone-rod retinal dystrophy ina patient with neurofibromatosis type I. Can3' Ophthalmol1 993;28:79-80.
143 Small KW, Weber JL, Roses A, et al. North Carolina
macular dystrophy is localized to 6ql4-q16.2. Am7HumGenet 1992;51(suppl):A34.
144 Small KW, Weber JL, Roses A, et al. North Carolinamacular dystrophy is assigned to chromosome 6. Genomics1992;13:681-5.
144A Small KW, Weber J, Roses A, et al. North Carolinamacular dystrophy (MCDRI). A review and refined map-ping to 6ql4-ql6.2. Ophthalmic Paediatr Genet 1993;14:141-2.
145 Small KW, Sanchez AR, Yelchits SV, et al. Physical map-ping of the MCDR1 (North Carolina macular dystrophy)locus. Invest Ophthalmol Vis Sci 1994;35:1717.
146 Stone EM, Nichols BE, Streb LM, et al. Genetic linkageof vitelliform macular degeneration (Best's disease) tochromosome 11q13. Nature Genet 1992;1:246-50.
147 Ferrell RE, Hittner HM, Antoszyk JH. Linkage of atypicalvitelliform macular dystrophy (VMD-1) to the solubleglutamate pyruvate transaminase (GPT1) locus. Am JHum Genet 1983;35:78-84.
148 Keen TJ, Inglehearn CF, Kim R, et al. Retinal patterndystrophy associated with a 4 bp insertion at codon 140in the RDS-peripherin gene. Hum Mol Genet 1994;3:367-8.
149 Kaplan J, Gerber S, Larget-Piet D, et al. A gene forStargardt's disease (fundus flavimaculatus) maps to theshort arm ofchromosome 1. Nature Genet 1993;5:308-1 1.
150 Kaplan J, Gerber S, Larget-Piet D, et al. A gene forStargardt's disease (fundus flavimaculatus) maps to theshort arm of chromosome 1 (correction). Nature Genet1994;6:214.
151 Zhang K, Bither PP, Park R, et al. A dominant Stargardt'smacular dystrophy locus maps to chromosome 13q34.Arch Ophthalmol 1994;112:759-64.
152 Stone EM, Nichols BE, Kimura AE, et al. Clinical featuresof a Stargardt-like dominant progressive macular dys-trophy with genetic linkage to chromosome 6q. ArchOphthalmol 1994;112:765-72.
153 Cremers PM, van de Pol DJR, Kerkhoff LPM, et al.Cloning of a gene that is rearranged in patients withchoroideremia. Nature 1990;347:674-7.
154 Merry DE, Janne PA, Landers JE, et al. Isolation of acandidate gene for choroideremia. Proc Natl Acad SciUSA 1992;89:2135-9.
155 van den Hurk JAJM, van de Pol TJR, Molloy CM, et al.Detection and characterization of point mutations in thechoroideremia candidate gene by PCR-SSCP analysisand direct DNA sequencing. Am J Hum Genet 1992;50:1195-202.
156 Sankila EM, Tolvanen R, van den Hurk JAJM, et al.Aberrant splicing of the CHM gene is a significant causeof choroideremia. Nature Genet 1992; 1: 109-13.
157 Schwartz M, Rosenberg T, van den Hurk JAJM, et al.Identification of mutations in Danish choroideremia fam-ilies. Hum Mutat 1993;2:43-7.
158 Pascal 0, Donnelly P, Fouanon C, et al. A new (old)deletion in the choroideremia gene. Hum Mol Genet 1993;1:1489.
159 Matsui Y, Kikuchi A, Araki S, et al. Molecular cloning andcharacterization of a novel type of regulatory protein(GDI) for smg p25A, a ras p21-like GTP-binding protein.Mol Cell Biol 1990;10:4116-22.
160 Fodor E, Lee RT, O'Donnell nI. Analysis ofchoroideraemiagene (letter). Nature 1991;351:614.
161 Cremers FP, Molloy CM, van de Pol DJR, et al. Anautosomal homologue of the choroideremia gene co-localizes with the Usher syndrome type II locus on thedistal part of chromosome lq. Hum Mol Genet 1992;1:71-5.
162 Seabra MC, Brown MS, Slaughter CA, et al. Purification ofcomponent A of Rab geranylgeranyl transferase: possibleidentity with the choroideremia gene product. Cell 1992;70:1049-57.
163 Seabra MC, Brown MS, Goldstein JL. Retinal de-generation in choroideremia: deficiency of Rab geranyl-geranyl transferase. Science 1993;259:377-81.
164 Valle D, Kaiser-Kupfer MI, Valle LAD. Gyrate atrophy ofthe choroid and retina: deficiency of ornithine amino-transferase in transformed lymphocytes. Proc Natl AcadSci USA 1977;74:5159-61.
165 Inana G, Hotta Y, Zintz C, et al. Molecular basis ofornithine aminotransferase defect in gyrate atrophy. ProgClin Biol Res 1991;362:191-219.
166 Ramesh V, Gusella JF, Shih VE. Molecular pathology ofgyrate atrophy of the choroid and retina due to omithineaminotransferase deficiency. MolBiolMed 199 1;8:81-93.
167 Ramesh V, Eddy R, Bruns GA, et al. Localization of theornithine aminotransferase gene and related sequenceson two human sequences. Hum Genet 1987;76:121-6.
168 Barrett DJ, Bateman JB, Sparkes RS, et al. Chromosomallocalization of human omithine aminotransferase genesequences to 10q26 and Xpll.2. Invest Ophthalmol VisSci 1987;28: 1037-42.
169 Wu J, Ramesh V, Kidd JR, et al. The ornithine am-inotransferase (OAT) locus is linked and distal to D 10S20on the long arm of chromosome 10. Cytogenet Cell Genet1988;48: 126-7.
170 Ramesh V, Benoit LA, Crawford P, et al. The ornithineaminotransferase (OAT) locus: analysis of RFLPs ingyrate atrophy. Am J Hum Genet 1988;42:365-72.
171 Mitchell GA, Looney JE, Brody LC, et al. Human or-nithine-delta aminotransferase: cDNA cloning and ana-lysis of the structural gene. Jf Biol Chem 1988;263:14288-95.
172 Mitchell G, Brody L, Looney J, et al. An initiator codonmutation in omithine-delta-aminotransferase causing
914
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from

Recent advances in the gene map of inherited eye disorders
gyrate atrophy of the choroid and retina. J Clin Invest1988;81:630-3.
173 Ramesh V, McClatchey Al, Ramesh N, et al. Molecularbasis of omithine aminotransferase deficiency in B-6-responsive and -nonresponsive forms of gyrate atrophy.Povc Natl Acad Sci USA 1988;85:3777-80.
174 Inana G, Hotta Y, Zintz C, et al. Expression defect ofornithine aminotransferase gene in gyrate atrophy. InvestOphthalmol Vis Sci 1988;29:1001-5.
175 Mitchell GA, Brody LC, Sipila I, et al. At least two mutantalleles of ornithine-delta-aminotransferase cause gyrateatrophy of the choroid and retina in Finns. Proc NatlAcadSci USA 1989;86:197-201.
176 Inana G, Chambers C, Hotta Y, et al. Point mutationaffecting processing of the omithine aminotransferaseprecursor protein in gyrate atrophy. J Biol Chem 1989;264:17432-6.
177 McClatchey AI, Kaufman DL, Berson E, et al. Splicingdefect at the omithine aminotransferase (OAT) locus ingyrate arophy. Am 7Hum Genet 1990;47:790-4.
178 Mitchell GA, Labuda D, Fontaine G, et al. Splice-mediatedinsertion of an Alu sequence inactivates ornithine delta-aminotransferase: a role for Alu elements in humanmutation. Proc NadAcad Sci USA 1991;88: 815-19.
179 Akaki Y, Hotta Y, Mashima Y, et al. A deletion in theornithine aminotransferase gene in gyrate atrophy. J BiolChem 1992;267: 12950-4.
180 Michaud J, Brody LC, Steel G, et al. Strand-separatingconformational polymorphism analysis: efficacy of de-tection of point mutations in the human ornithine delta-aminotransferase gene. Genomics 1992;13:389-94.
181 Mashima Y, Weleber RG, Kennaway NG, et al. A single-base change at a splice acceptor site in the ornithineaminotransferase gene causes abnormal RNA splicing ingyrate atrophy. Hum Genet 1992;90:305-7.
182 Mashima Y, Murakami A, Weleber RG, et al. Nonsense-codon mutations of the omithine aminotransferase genewith decreased levels ofmutant mRNA in gyrate atrophy.AmJHum Genet 1992;51:81-91.
183 Park JK, Herron BJ, O'Donnell JJ, et al. Three novelmutations of the ornithine aminotransferase (OAT) genein gyrate atrophy. Genomics 1992;14:553-4.
184 Park JK, O'Donnell JJ, Shih VE, et al. A 15-bp deletionin exon 5 of the ornithine aminotransferase (OAT) locusassociated with gyrate atrophy. Hum Mutat 1992;1:293-7.
185 Brody LC, Mitchell GA, Obie C, et al. Ornithine delta-aminotransferase mutations in gyrate atrophy: allelic het-erogeneity and functional consequences. J Biol Chem1992;267:3302-7.
186 Dietz HC, Valle D, Francomano CA, et al. The skipping ofconstitutive exons in vivo induced by nonsense mutations.Science 1993;259:680-3.
187 Inana G, Hotta Y, Mashima Y, et al. Molecular geneticbasis of gyrate atrophy. Invest Ophthalmol /s Sci 1994;35:1984.
188 Li Y, Muller B, Fuhrmann C, et al. The autosomal dom-inant familial exudative vitreoretinopathy locus maps onllq and is closely linked to D11S533. AmJHum Genet1992;51:749-54.
189 Li Y, Fuhrmann C, Schwinger E, et al. The gene forautosomal dominant familial exudative vitreoretinopathy(Criswick-Schepens) on the long arm of chromosome 11[letter]. Am J Ophthalmol 1992;113:712-3.
190 Stone EM, Kimura AE, Folk JC, et al. Genetic linkage ofautosomal dominant neovascular inflammatory vitreo-retinopathy to chromosome 11q13. Hum MolGenet 1992;1:685-9.
191 Fullwood P, Jones J, Bundey S, et al. X linked exudativevitreoretinopathy: clinical features and genetic linkageanalysis. BrJ Ophthalmol 1993;77:168-70.
192 Berger W, Meindl A, van de Pol, TJR, et al. Isolation of acandidate gene for Norrie disease by positional cloning.Nature Genet 1992;1:199-203.
193 Chen Z, Hendriks RW, Jobling MA, et al. Isolation andcharacterization of a candidate gene for Norrie disease.Nature Genet 1992;1:204-8.
194 Meitinger T, Meindl A, Bork P, et al. Molecular modellingof the Norrie disease protein predicts cystine knot growthfactor tertiary structure. Nature Genet 1993;5:376-80.
195 Berger W, van de Pol D, Warburg M, et al. Mutations inthe candidate gene for Norrie disease. Hum Mol Genet1992;1:461-5.
196 Meindl A, Berger W, Meitinger T, et al. Norrie disease iscaused by mutations in an extracellularprotein resemblingC-terminal globular domain of mucins. Nature Genet1992;2: 139-43.
197 Chen Z, Battinelli EM, Hendricks RW, et al. Norrie diseasegene: characterization of deletions and possible function.Genomics 1993;16:533-5.
198 Chen Z, Battinelli EM, WoodruffG, etal. Characterizationof a mutation within the NDP gene in a family with
a manifesting female carrier. Hum Mol Genet 1993;2:1727-9.
199 Wong F, Goldberg MF, Hao Y Identification of a nonsensemutation at codon 128 of the Norrie disease gene in amale infant. Arch Ophthalmol 1993;111:1553-7.
200 Zhu D, Maumenee IH. Mutation analysis of the Norriedisease gene in eleven families. Invest Ophthalmol Eis Sci1994;35: 1265.
201 Chen Z, Battinelli EM, Fielder A, et al. A mutation in theNorrie disease gene (NDP) associated with X-linkedfamilial exudative vitreoretinopathy. Nature Genet 1993;5:180-3.
202 Ravia Y, Braier-Goldstein 0, Bat-Miriam KM, et al. X-linked recessive primary retinal dysplasia is linked to theNorrie disease locus. Hum Mol Genet 1993;2:1295-7.
203 Sieving PA, Bingham E, Roth MS, et al. Linkage re-lationship of X-linked juvenile retinoschisis with Xp22. 1-p22.3 probes. Am J Hum Genet 1990;47:616-21.
204 Alitalo T, Kruse TA, de la Chapelle A. Refined localizationof the gene causing X-linked juvenile retinoschisis. Geno-mics 1991;9:505-10.
205 Alitalo T, Kruse TA, Ahrens P, et al. Genetic mapping of12 marker loci in the Xp22.3-21.2 region. Hum Genet1991 ;86:599-603.
206 Kaplan J, Pelet A, Hentati H, et al. Contribution to carrierdetection and genetic counselling in X linked retino-schisis. JfMed Genet 1991;28:383-8.
207 Oudet C, Weber C, Kaplan J, et al. Characterisation of ahighly polymorphic microsatellite at the DXS207 locus:confirmation of very close linkage to the retinoschisisdisease gene. J Med Genet 1992;30:300-3.
208 Bergen AA, van Schooneveld MJ, Orth U, et al. Multipointlinkage analysis in X-linked juvenile retinoschisis. ClinGenet 1993;43: 113-6.
209 Francomano C, Liberfarb RM, Hirose T, et al. The Sticklersyndrome: evidence for close linkage to the structuralgene for type II collagen. Genomics 1987;1:293-6.
210 Priestley L, Kumar D, Sykes B. Amplification of theCOL2A1 3-prime variable region used for segregationanalysis in a family with the Stickler syndrome. HumGenet 1990;85:525-6.
211 Ahmad NN, Ala-Kokko L, Knowlton RG, et al. Stopcodon in the procollagen II gene (COL2A1) in the familywith the Stickler syndrome (arthro-ophthalmopathy). ProcNad Acad Sci USA 1991;88:6624-7.
212 Brown DM, Nichols BE, Weingeist TA, et al. ProcollagenII gene mutation in Stickler syndrome. Arch Ophthalmol1992;11O: 1589-93.
213 Ahmad NN, McDonald-McGinn DM, Zackai EH, et al.A second mutation in the type II procollagen gene(COL2A1) causing the Stickler syndrome (arthro-oph-thalmopathy) is also a premature termination codon. AmJHum Genet 1993;52:39-45.
214 Brown DM, Vandenburgh K, Nichols BE, et al. Incidenceof frameshift mutations in the procollagen II gene inStickler syndrome and identification of four new muta-tions. Invest Ophthalmol Vis Sci 1994;35: 1717.
215 Knowlton RG, Weaver EJ, Struyk AF, et al. Genetic linkageanalysis of hereditary arthro-ophthalmopathy (Sticklersyndrome) and the type II procollagen gene. Am J HumGenet 1989;45:681-8.
216 Fryer AE, Upadhyaya M, Littler M, et al. Exclusion ofCOL2A1 as a candidate gene in a family with Wagner-Stickler syndrome. J Med Genet 1990;27:91-3.
217 Vmtiner GM, Temple K, Middleton-Price HR, et al. Gen-etic and clinical heterogeneity of Stickler syndrome. AmJ Med Genet 199 1;41:44-8.
218 Bonaventure J, Philippe C, Plessis G, et al. Linkage studyin a large pedigree with Stickler syndrome: exclusion ofCOL2A1 as the mutant gene. Hum Genet 1992;90:164-8.
219 Korkko J, Ritvaniemi P, Haataja L, et al. Mutation in typeII procollagen (COL2A1) that substitutes aspartate forglycine alpha 1-67 and that causes cataracts and retinaldetachment: evidence for molecular heterogeneity in theWagner syndrome and the Stickler syndrome (arthro-ophthalmopathy). Am J7 Hum Genet 1993;53:55-61.
220 Kajiwara K, Berson EL, Dryja TP. Digenic retinitis pig-mentosa due to mutations at the unlinked peripherin/RDS and ROMI loci. Science 1994;264:1604-8.
221 Gal A, Orth U, Baehr W, et al. Heterozygous missensemutation in the rod cGMP phosphodiesterase P-subunitgene in autosomal dominant stationary night blindness.Nature Genet 1994;7:64-8.
222 Leppert M, Baird L, Anderson KL, et al. Bardet-Biedlsyndrome is linked to DNA markers on chromosome 11qand is genetically heterogeneous. Nature Genet 1994;7:108-12.
223 Weber BHF, Vogt G, Wolz W, et al. Sorsby's fundusdystrophy is genetically linked to chromosome 22ql3-qter. Nature Genet 1994;7:158-61.
224 Kremer H, Pinckers A, van den Helm B, et al. Localizationof the gene for dominant cystoid macular dystrophy onchromosome 7p. Hum Mol Genet 1994;3:299-302.
915
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.12.903 on 1 D
ecember 1994. D
ownloaded from



![StVftHllf It THE iBBEVILLE PRESS AIED Mill, · 2017. 12. 17. · StVftHllf It THE iBBEVILLE PRESS AIED Mill, Abbeville S, C., November 155, 1869. ®jjt iprcss. ABBXIVVZiXj]]), S](https://img.dokumen.tips/doc/110x75/5ff5043876388e35ba4822e0/stvfthllf-it-the-ibbeville-press-aied-mill-2017-12-17-stvfthllf-it-the-ibbeville.jpg)

























