Embed Size (px)
DESCRIPTION
Rvisión de investigación cualitativa en afasias del año 2013
Citation preview

Aphasiology, 2013Vol. 27, No. 11, 1281–1301, http://dx.doi.org/10.1080/02687038.2013.818098
REVIEW
Qualitative research in aphasia: A review of the literature
Nina Simmons-Mackie and Karen E. Lynch
Southeastern Louisiana University, Communication Sciences and Disorders,Hammond, LA 70402 USA
Background: In the past decade, there has been a growing interest in qualitative researchin the field of aphasia. Knowledge of patterns and trends in this body of research wouldinform future research. However, there is little information about the characteristics orpatterns of qualitative research in aphasia.Aims: In order to describe qualitative research in aphasia, a review of the aphasia litera-ture from 1993 to 2013 was undertaken. Studies were identified using a variety of searchterms for the following electronic databases: PubMed, CINAHL, PsychINFO, Web ofScience and ComDisDome. A total of 78 articles that met the review criteria were iden-tified and data were extracted in the following areas: topic of study, participants, datacollection, research design and data analysis.Main Contribution: Publication of qualitative research in aphasia has increased since1993 and contributed to an important database regarding phenomena associated with lifewith aphasia. The most prevalent research topics relate to the experience of aphasia, activ-ities or participation of people with aphasia, perceptions of intervention or outcomes,perceived goals or needs and environmental factors. People with aphasia were the mostfrequent participants. A majority of studies employed generic qualitative methods inde-pendent of a traditional qualitative philosophy. Interview was the most prevalent datacollection method, and few studies reported methods of determining if the amount ofdata were sufficient to meet the study aims. The depth of interpretation (level of analysis)varied across studies from concrete category listings to higher-level explanatory themes.Conclusions: Despite the variation across studies, identified trends provided valuableinformation and raised interesting questions for debate. Questions are posed for futureconsideration such as “should aphasia researchers more frequently apply methods fromestablished qualitative traditions?” and “should aphasia research include a wider varietyof data collection methods?” Questions were raised regarding terminology (e.g., themesversus categories) and depth of interpretation in qualitative studies. The findings also pro-vide concrete direction; for example, qualitative researchers might improve the reportingof methods for determining data sufficiency.
Keywords: Aphasia; Qualitative research; Research design; Qualitative.
Address correspondence to: Nina Simmons-Mackie, Southeastern Louisiana University,Communication Sciences and Disorders, 580 Northwoods Dr., Abita Springs, LA 70420, USA. E-mail:[email protected]
© 2013 Taylor & Francis

1282 SIMMONS-MACKIE AND LYNCH
Qualitative research includes a variety of research traditions designed to provide a richdescription of a person, group, event or phenomenon and/or gain a deeper under-standing regarding an aspect of social life, experience or culture (e.g., Creswell, 2006;Lincoln & Guba, 1985; Wolcott, 1994). As such, qualitative research is particularlywell suited to exploring complex social phenomena such as communication and com-munication disorders. The umbrella term, qualitative research, encompasses a numberof philosophical and methodological approaches. For example, phenomenology,ethnography and grounded theory are well-known, established qualitative traditions(Creswell, 2006).
With the shift towards client-centred medicine and social model philosophies inhealth care, researchers and practitioners have been increasingly interested in theexperiences and insider perspectives of key stakeholders such as patients and healthcare providers (Hammell, 2001). This expansion of philosophy has been paralleledby a marked growth in qualitative research in health care fields (Bradely, Curry,& Devers, 2007; Sandelowski, 2004). The increase in qualitative research has beenapparent in aphasiology as well. Beginning almost 20 years ago, a series of arti-cles described potential applications of qualitative research in aphasia (Damico,Oelschlaeger, & Simmons-Mackie, 1999; Damico & Simmons-Mackie, 2003; Damico,Simmons-Mackie, Oelschlaeger, Elman, & Armstrong, 1999; Damico, Simmons-Mackie, & Schweitzer, 1995; Simmons-Mackie, 1994; Simmons-Mackie & Damico,1999, 2003). These articles discussed the key features of qualitative research and therequirements for systematic and rigorous qualitative study in aphasia. Since that time,aphasia researchers have increasingly employed qualitative methods to gather authen-tic data and access insider perspectives on various topics relevant to aphasia andaphasia intervention. However, little is known regarding the patterns of qualitativeinvestigation in the aphasia literature. In what topics of study has qualitative researchcontributed to the knowledge base in aphasia? What types of qualitative research haveprevailed? What types of data collection and analysis strategies have been used? Insightinto the patterns of qualitative research in aphasia can identify potential strengthsand weaknesses in current research practices and help researchers reflect on possi-ble changes in future research. Therefore, a project was initiated to review qualitativeresearch in the published aphasia literature in an effort to discover and describe trendsand issues that will inform future research. This review was not designed as a criti-cal review of the quality of each study. Rather, the goal of this review process was toidentify general patterns of qualitative research in aphasia.
METHODS
A search of the literature identified studies that employed qualitative research meth-ods to investigate issues relevant to aphasia. The following electronic databaseswere searched: PubMed, CINAHL, PsychINFO, Web of Science and ComDisDome.The search focused on aphasia and qualitative research published between January1993 and January 2013 using a variety of search terms (e.g., aphasia, qualita-tive research, qualitative, grounded theory, ethnography, narrative, phenomenology).A total of 925 articles were identified. Articles were eliminated from the review if theywere: (1) duplicates, (2) not published in a peer-reviewed journal, (3) not a report oforiginal research, (4) not a study of aphasia in adults, (5) not written in English, or(6) not qualitative research. Qualitative research studies were defined as those that

QUALITATIVE RESEARCH IN APHASIA 1283
were self-described as qualitative research, and/or the authors identified an estab-lished qualitative or interpretive tradition such as phenomenology or grounded theory.Descriptive case studies that were not described as qualitative research were notincluded. Articles reporting research using conversation analysis or discourse analysiswere excluded from this review since these constitute a distinct approach to qualitativeinvestigation using different methods and criteria.
A total of 78 studies met the criteria for inclusion in this review of qualitativeresearch in aphasia (see Appendix A). Each of the articles was reviewed, and rel-evant information was extracted. Data were extracted in the following areas: topicof study, reported research design or tradition, type of participants, data collection(including participant selection and method of determining data sufficiency) and dataanalysis (Appendix B). For topic, participants, design, type of data collection, sam-pling and data analysis method, the extracted data were initially analysed by groupingand labelling similar data into semantic categories (Spradley, 1980). This resulted incategories that were used to code the data across studies (see Appendix C). For exam-ple, data extracted to describe the topics of study were grouped into categories such as“experience of aphasia” or “intervention or program.” Once these coding categorieswere identified, the first author recycled through the extracted data and coded eacharticle. In order to ensure that data were coded reliably, a random sample of 15% ofthe identified articles were reviewed and coded independently by a second investigator.The resulting inter-rater agreement of 91% across studies and codes within categories(i.e., categories of topic, research design/tradition, type of participants, data collectionmethods, sampling, data sufficiency and data analysis) was deemed acceptable. Finally,frequency counts were computed to determine the number of articles represented foreach of the coded categories.
RESULTS
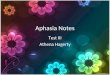
The number of qualitative research articles in aphasia that met the criteria for thisreview increased over the past 20 years (see Figure 1). Over four times as many quali-tative articles were published in the second half of the review period as in the first half,and a marked increase is apparent in the past 5 years.
68
19
45
0
10
20
30
40
50
60
70
1993–1997 1998–2002 2003–2007 2008–2012
Nu
mb
er o
f a
rtic
les
Year of publication
Figure 1. Number of qualitative research articles in aphasia from 1993 through 2012 that met reviewcriteria.

1284 SIMMONS-MACKIE AND LYNCH
Research topics
Topics of the research articles were grouped into broad categories reflecting the pri-mary focus of the article (see Table 1). The most prevalent topic related to perceptionsof the experience of aphasia (n = 20). These studies included experiences reportedfrom the perspective of people with aphasia (n = 13), family members or caregivers(n = 7) and speech-language pathologists (SLPs) (n = 2). A variety of subtopics fitwithin experience of aphasia such as the perspectives of people with aphasia and fam-ily members on living successfully with aphasia (e.g., Brown, Worrall, Davidson, &Howe, 2010), the meaning of quality of life with aphasia (Cruice, Worrall, & Hickson,2006) and perspectives on well-being, psychosocial adjustment and identity in aphasia(e.g., Bronken, Kirkevold, Martensen, & Kvigne, 2012). Seventeen studies addressedthe aspects of activities or participation for people with aphasia. Examples of thistopic included studies of communication activities of people with aphasia (e.g., havingconversations, reading, making phone calls) (Davidson, Worrall, & Hickson, 2003),participation in relationships (e.g., Davidson, Worrall, & Hickson, 2006; Northcott& Hilari, 2011) and participation in informed consent (Penn, Frankel, Watermeyer,& Muller, 2009). There were 16 articles reporting on specific interventions or servicesincluding services for people with aphasia (e.g., script training, computer-based ser-vices) and services for others (e.g., residential family program, training for health careproviders). Ten articles investigated perceived needs or goals of people with aphasia,family members or SLPs. There were seven studies on environmental factors affect-ing people with aphasia. These studies typically defined environmental barriers andfacilitators to participation for people with aphasia, including broad studies identi-fying environmental factors such as features in the community at large that impactpeople with aphasia (e.g., Howe, Worrall, & Hickson, 2008) and more focused studiessuch as environmental factors associated with public transport (Ashton et al., 2008)or acute health care (O’Halloran, Worrall, & Hickson, 2011). Four studies investi-gated the experience of discharge from speech-language therapy from the perspectiveof people with aphasia or others such as SLPs. Finally, two articles did not fit into theprevious topics and were designated as other.
Participants
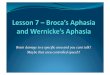
Various types of participants were included in the qualitative studies reviewed (seeFigure 2). Over two-thirds (54 out of 78) of the studies included people with aphasia as
TABLE 1Categories of topics addressed in qualitative research articles reviewed
Broad topic area Number of articles
The experience of aphasia 20Activities and participation 17Intervention or service 16Goals or needs 10Environmental factors 7Discharge from services 4Cultural or ethnic issues 2Other 2

QUALITATIVE RESEARCH IN APHASIA 1285
54
17
13 74
0
10
20
30
40
50
60
70
People with
aphasia
Family/carers SLPs Others Service
providers
Nu
mb
er o
f a
rtic
les
Types of participants
Figure 2. Number of articles involving specific types of participants in qualitative research articles reviewed.
research participants. Family members and significant others were included in 17 stud-ies; SLPs were included in 13 studies. Service providers such as stroke team membersand other people such as employers were included in 11 studies.
Research design
Historically qualitative research has been classified or characterised according to theresearch tradition or philosophical roots upon which the research is based. In fact,many definitions refer to qualitative research as a variety of traditions designed toexplicate social or cultural phenomena (e.g., Creswell, 2006). Each tradition reflectsan underlying philosophy or orientation that helps guide the research methods. Thus,the tradition helps determine the types of questions or topics that are suitable, thetypes of data that are allowable and the types of claims that can be made from theresults (e.g., Creswell, 2006).
Of the 78 articles included in the current review, 52 articles described the researcheither in very general terms such as “qualitative methods” (n = 47) or the authorsadopted a pragmatic or practical approach such as basic qualitative description(Sandelowski, 2000) (n = 5). Nonspecific or pragmatic qualitative approaches typi-cally employ qualitative methodology (e.g., open-ended interview, thematic analysis)independent of one of the traditional philosophical orientations (e.g., phenomenol-ogy, ethnography) (Sandelowski, 2000; Smith, Bekker & Cheater, 2011; Thomas,2006). The remaining 26 articles included reports of research conducted accordingto or adapted from one of the following established research traditions: phenomenol-ogy, grounded theory, narrative analysis or ethnography. Figure 3 demonstrates thedistribution of research traditions in the literature reviewed.
Data collection
The review included an analysis of several aspects of data collection including the sam-pling methods, method of data collection and the measures taken to ensure that thedata were sufficient to answer the research question. Results will be reported relativeto each of these aspects of data collection.

1286 SIMMONS-MACKIE AND LYNCH
52
11 58
2
0
Qualita
tive
Phenom
enolo
gy
Gro
unded theory
Narr
ative
Eth
nogra
pghy
10
20
30
40
50
60
70
Nu
mb
er o
f a
rtic
les
Qualitative research tradition
Figure 3. Qualitative research traditions or designs reported in qualitative articles reviewed.
It is standard practice for research articles to include information concerning sam-ple selection; that is, how the participants or events were selected for inclusion ina study. A majority of the articles reviewed (52 out of 78) reported using conve-nience samples to select participants or did not specifically label or describe samplingmethods. Two articles explicitly reported snowball sampling, where participants arenominated by others (e.g., the person with aphasia (PWA) nominates friends to partic-ipate in interviews) (Atkinson & Flint, 2001); however, snowball sampling was impliedin several additional articles. Purposeful sampling was explicitly reported in 13 arti-cles. Purposeful sampling requires that participants are deliberately selected with anexplicit purpose in mind that is consistent with the aims of the study (Marshall, 1996).Maximum variation sampling, a type of purposeful sampling, was reported in 9 arti-cles. Maximum variation sampling requires that participants are selected based ondiverse characteristics of particular interest (Patton, 2002). Two articles reported semi-random sampling. Two of the 13 articles employing observation reported that event ortime sampling was used to identify situations sampled for observation (Hammersley& Atkinson, 1995).
In addition to sampling methods, researchers must choose from a wide variety ofdata collection strategies applicable to qualitative research such as qualitative inter-views, focus groups, participant observation, artefact review, diaries and collection ofvideo or audio data (Creswell, 2006). Data collection methods are typically designedto suit the subject matter, the research question and/or the qualitative design of thestudy. Figure 4 shows the distribution of types of data collection methods employedacross the studies reviewed. Clearly, the overwhelming approach to qualitative datacollection in aphasia has been interviews, either one-on-one or in focus groups, withinterviews represented in 96% of the articles (75 out of 78). Interviews with peoplewith aphasia were conducted in 52 of these studies. Studies employing more than onedata collection strategy are represented recurrently. Only 18 studies employed morethan one data collection method (e.g., interviews & observations; interviews & video).
Data collection involves not only determination of the approach to sampling andthe method of collecting data (e.g., interview), but also involves consideration of theamount of data needed to address the research questions posed (e.g., Walker, 2012).Thus, another aspect of data collection is the method of determining the sufficiencyof data collected for a particular study. Some researchers consider a useful criterion

QUALITATIVE RESEARCH IN APHASIA 1287
75
14
83 5
0
10
20
30
40
50
60
70
80
Interviews/
focus group
Observation Recording Diary Artefacts
Nu
mb
er o
f a
rtic
les
Data collection method
Figure 4. Data collection methods employed in qualitative research articles reviewed.
in qualitative research is collecting data to saturation. Saturation is the collection ofdata in a study until redundancy occurs (Morse, 2005), and includes data satura-tion and theoretical saturation. Data saturation involves continual sampling within astudy until repetition of the data set has occurred and no new information is beingobtained (Bowen, 2008). Theoretical saturation occurs when no new categories orthemes are being identified in the data (Strauss & Corbin, 1990). Of the 78 stud-ies reviewed, 5 explicitly reported that saturation was a criterion in data collectionand 5 additional articles implied saturation criteria. One article described methods ofdetermining saturation. Although it is possible that researchers employed a criterionfor judging the amount of data required, 94% did not report or implicate a rationaleor method for determining that sufficient data were collected. It is notable that severalstudies involved relatively large participant pools, possibly with the expectation thatcollecting large numbers would ensure sufficient data.
Data analysis
Methods of analysing qualitative data abound in the literature and, although mostemploy some means of identifying and grouping content into units, categories orthemes, the specific data analysis approaches are highly varied and often complex.Therefore, for the purposes of this review, explicit labels and citations in articles wereused to classify the data analysis method. When nonspecific descriptions were given(e.g., coding, categorising), the data analysis method was identified as other/not speci-fied. Reflecting the literature in general, the qualitative research in aphasia includedvaried approaches to data analysis (see Table 2). Many of the qualitative articles(30%) did not report a specific analytic framework or cite a methodological refer-ence; rather, these articles provided general or vague descriptions of analysis methodssuch as “searching for themes in the data.” The most common labelled method ofanalysing data was qualitative content analysis (15 studies) (Graneheim & Lundman,2004). Content analysis involves identifying meaning or content units that containrelated concepts, labelling meaning units with a code, aggregating the data into cate-gories, then linking the categories into themes. The second most prevalent label usedto describe data analysis was thematic analysis (11 studies). Thematic analysis is often

1288 SIMMONS-MACKIE AND LYNCH
TABLE 2Methods of analysing qualitative data reported in reviewed articles
Reported data analysis method Number of articles
Qualitative content analysis 15Theme analysis 11Framework method 10Narrative analysis 6Qualitative software 5Open, axial & selective coding 3Constant comparison method 2Interpretive phenomenological analysis 2Other or not specified 24
used as a generic term to refer to a process of identifying themes in qualitative data.It requires identifying, analysing and reporting patterns within data (Braun & Clarke,2006). Typically, the analysis proceeds from description to interpretation. Thus, dataare initially “organized to reflect patterns in semantic content, and then these pat-terns are subjected to interpretive analysis in order to glean the significance of thepatterns and their broader meanings and implications” (Braun & Clarke, 2006, p. 13).Framework analysis is another method of identifying themes in qualitative data (e.g.,Richie & Spencer, 1994); this approach was reported in 10 studies. Framework analysisinvolves stages including immersing oneself in the data, listing key or recurrent ideas,sorting the ideas, labelling the ideas into manageable components or bites, rearrangingdata to try out different themes and finally interpreting the themes into a concep-tual framework (Richie & Spencer, 1994; Smith & Firth, 2011). Other approachesreported were narrative analysis, Interpretative Phenomenological Analysis (IPA),open, axial and selective coding and constant comparison. Narrative analysis repre-sents various approaches that focus on identifying patterns within stories or narratives.Riessman (1993) describes narrative analysis as a process of systematically interpret-ing the narrative interpretations of participants who tell their stories. IPA applies toa particular phenomenological orientation in qualitative research. Analysis often pro-ceeds from identifying or noting concepts in a core set of data (e.g., one transcript),labelling potential themes, clustering and ordering themes and then cycling throughadditional data sets to verify and interpret (Smith & Osborn, 2003). While this is sim-ilar to thematic analysis, IPA differs in that the guiding philosophy constrains theanalysis to focus on the meanings that particular experiences hold for participants(Smith & Osborn, 2003). Open, axial and selective coding, associated with groundedtheory, involves coding data, identifying connections between coded categories orsubcategories of data and finally developing a hypothesis to explain how core cate-gories interact to represent a theory or construct (Corbin & Strauss, 2008; Strauss &Corbin, 1990). The constant comparative method, also associated with grounded the-ory, entails continuously moving back and forth between emerging findings and thesource data to verify themes and hypotheses (Paul & Sanders, 2010).
In addition to the type of data analysis, the depth of data analysis varied acrossstudies. Qualitative investigation involves two slightly different outcomes of data anal-ysis: description and explanation (Ritchie & Lewis, 2003; Smith et al., 2011). Smithet al. (2011) describe description as a detailed, meaningful and relevant account of the

QUALITATIVE RESEARCH IN APHASIA 1289
topic under study. Thick description paints a picture for the reader to provide a senseof what the event, people or experience look, feel or sound like. To achieve adequatedescription, the researcher summarises and synthesises the data in a way that capturesthe key elements and represents the associations that tie the whole together. Finally,the description is carried to a higher level by extracting core concepts or descrip-tive categories that represent the topic of study (Smith et al., 2011). Some qualitativeresearch stops with description. Thus, the project focuses on developing a taxonomyor categorical description of a phenomenon, an event or a group.
A second goal of qualitative research is explanation (Smith et al., 2011).Explanation involves seeking patterns or associations across the data that relate to thecore concepts, relating these patterns to broader issues in life, society or culture, devel-oping hypotheses to explain these patterns, exploring the data and the wider literature,and finally developing higher-order interpretive themes that provide meanings and/orexplanations of the core concepts (Smith et al., 2011). In other words, deep inter-pretation requires moving away from listings or categories and towards higher-orderexplanations and/or interpretations of the phenomena.
An original plan for this review was to identify studies that were primarily descrip-tive versus studies that combined description and explanation. However, it proveddifficult to identify primarily descriptive versus explanatory approaches. The termscategory and theme were often used interchangeably, and the word interpretationappeared to mean different things to different researchers. Rather than a distinctionbetween description and explanation, the studies appeared to fall along a continuumfrom relatively concrete listings of categories to abstract, higher-order interpretations.Three studies that each reported themes derived from data analysis will be brieflydescribed in order to demonstrate the different qualitative outcomes of studies.
A qualitative study by Kerr, Hilari, and Litosseliti (2010) aimed to identify informa-tion needs of people with and without aphasia. The authors conducted focus groups,and from these data they used qualitative content analysis to arrive at 18 themes thatdefined the information needs of informants. The reported themes varied from veryspecific needs such as criteria for obtaining a disabled badge for the car to fairly broadtopics such as information about strokes. In other words, the authors reported a rela-tively concrete listing of categories representing a first-level sorting of qualitative data.There was little attempt to move beyond this to in-depth description or explanation.While the results are relatively concrete, the findings met the aim of the researcherswho wanted specific guidance on features to include on an information website.
A second study represents a higher level of description. Howe and colleagues(2008) interviewed people with aphasia in order to learn about the environmentalbarriers and facilitators to their participation in the community. The researchersemployed qualitative content analysis to analyse the interview data. The analysisresulted in seven themes that helped describe environmental influences on commu-nity participation including: other people’s awareness of aphasia, opportunities forparticipation, familiarity, availability of support, communication complexity, messageclarity and time available. These themes were distilled from a large volume of data inorder to represent the data in a descriptive way. In other words, Howe and colleaguescreated a taxonomy that helps others understand participation in the community asit relates to the environment. This descriptive taxonomy met the goal of identifyingenvironmental barriers and facilitators to participation for people with aphasia.
A third study provides an example of the highest level of interpretation in qualita-tive research. Parr (2007) used ethnographic investigation to explore life with severe

1290 SIMMONS-MACKIE AND LYNCH
aphasia. She observed and interviewed people with aphasia and others, and examinedrelevant artefacts such as notes taken by caregivers or written policies of organisations.Using framework methods to analyse the data, she identified four broad interactingcategories related to living with severe aphasia: infrastructure and resources, behaviourof other people, settings and environments, and personal identity and narrative. Theconstruction of these categories is similar to the themes reported by Howe and col-leagues; that is, the categories provide a condensed and informative description of thefactors that impact life with severe aphasia. However, Parr took the analysis a stepfurther to detail an overarching theme that cut across the results. Social exclusion wasa pervasive finding that permeated the lives of people with severe aphasia; this essenceof the study helped explain the experience of life with severe aphasia. In other words,the theme of social exclusion has explanatory power that goes beyond description.The reader begins to understand what it is like to have severe aphasia, what the impactof internal and external factors are and why people with severe aphasia tend to besocially isolated. Parr drew on social theory and the disability literature to explain themarginalisation associated with severe aphasia.
The three studies described above exemplify different levels of analysis from rela-tively concrete description to higher-order interpretation represented in the qualitativestudies reviewed.
DISCUSSION
Publication of qualitative research in aphasia has increased in the past 20 years and,as one might expect, the qualitative studies found in the aphasia literature reflect var-ied topics and methodologies. Despite the variability, several interesting findings andtrends warrant discussion, including a tendency for researchers to use a pragmaticapproach to qualitative research, prevalence of interviews in data collection, minimalattention to reporting data sufficiency criteria and variation in the depth or level ofdata analysis.
Research design or tradition
It is notable that 67% of the reviewed studies (52 out of 78) did not use a tra-ditional qualitative philosophy to guide the investigation. Rather, the trend was toemploy pragmatic or practical approaches that involve using qualitative methods (e.g.,theme analysis) detached from a broader philosophical tradition (e.g., phenomenol-ogy, ethnography). In fact, this tendency is not unique to aphasiology. There has beena trend, particularly in the nursing literature, to design qualitative studies withoutadhering to a specific guiding tradition. This approach has garnered several labelsincluding a pragmatic approach (Smith et al., 2011), a general inductive approach(Thomas, 2006) or a basic qualitative description (Sandelowski, 2000). Characteristicsof these pragmatic approaches to qualitative research are: (1) no traditional qualitativephilosophy is used to guide the study, (2) investigators select one or more qualitativedata collection and/or analysis strategies to fit the research question(s), and (3) inves-tigators are free to select aspects or criteria from any qualitative research paradigmthat they think will address the question or strengthen the study.
Proponents of the pragmatic approach to using qualitative methods indepen-dent of a driving qualitative philosophy argue that the approach is practical and

QUALITATIVE RESEARCH IN APHASIA 1291
straightforward, and avoids the complexities associated with the traditional qualita-tive philosophies (Sandelowski, 2000). Practical applications of qualitative methodsare useful for describing something in detail when the investigator is not interestedin higher-level interpretations related to social or cultural themes. Moreover, inves-tigators can pick and choose relevant methods that fit the question, and are notconstrained by the conventions associated with well-known traditions.
However, some consider that pragmatic approaches take the easy way out result-ing in a lower-quality, undisciplined product (Morse, Barrett, Mayen, Olson, &Spiers, 2002; Rolfe, 2006; Smythe, 2012). Since pragmatic approaches might encouragedescription of results in a relatively straightforward manner, then the method couldencourage superficial or oversimplified treatment of topics. Furthermore, pragmaticapproaches allow researchers to avoid a deeper understanding of the highly developedphilosophies that guide traditional qualitative paradigms (Braun & Clarke, 2006).Some critics suggest that qualitative research devoid of a theoretical framework mightresult in a lack of methodological coherence, which potentially affects a study’s valid-ity (Morse et al., 2002; Rolfe, 2006). An underlying philosophy or research traditionprovides guidance on the choice of questions, design and analysis; these are recognis-able and required elements (Smythe, 2012). Therefore, use of a guiding tradition mightaid the researcher and the consumer of research because they can identify missingelements and determine adherence to quality criteria.
During this review of qualitative research in aphasia, it was sometimes clear that theresearcher had made a conscious and informed decision to use a pragmatic approachthat suited the aims of the project. However, at other times, it was unclear if the use of aqualitative method independent of a guiding tradition was an explicit choice or simplya lack of experience or knowledge. Although there is often justification in employingpragmatic approaches, the high proportion of pragmatic studies in the aphasia litera-ture begs the question: does this represent best research practice? Aphasia researchersmight consider the relative benefits of pragmatic- versus philosophy-driven traditions.We might also wonder if the high occurrence rate of pragmatic qualitative research hasbeen self-perpetuating, with qualitative scientists imitating what they read. While thisreview does not suggest a right or wrong approach for future researchers, it raises theissue for further discussion and consideration.
Data collection
Another issue of interest is the prevalence of interviews in the reviewed research.Of 54 studies involving people with aphasia as participants, 51 studies includedinterviews with participants with aphasia. This finding suggests that, despite thecommunication disability, people with aphasia have been recruited to participate inqualitative interviews. It is encouraging that true insiders have been included in studiesrelated to aphasia. To facilitate participation of people with aphasia in interviews, sev-eral researchers used communication support methods. In fact, one of the qualitativestudies reviewed focused on the ability of people with aphasia to participate in inter-views when given sufficient support (Luck & Rose, 2007). The authors concluded that“Valuable data can be obtained from participants with aphasia when the interviewmethod is altered appropriately to meet their communicative needs” (p. 208).
Along with this positive finding that people with aphasia are being recruited to pro-vide their own perspectives, we might wonder about the preponderance of one datacollection strategy across qualitative studies in aphasia: 96% (75 out of 78) of the

1292 SIMMONS-MACKIE AND LYNCH
reviewed studies involved interviews, either one-on-one or in focus groups. Of these,60 studies used interview as the only data collection strategy. While qualitative inter-viewing is a powerful strategy for gathering insider information, interviews provideone perspective on a phenomenon—the informant’s perspective. This is appropriatewhen the aim of the study is to learn what people think or feel about some eventor phenomenon. However, what people believe, perceive or interpret does not alwaysreflect actual events. For example, in a study of aphasia therapy, Simmons-Mackie,Damico, and Damico (1999) reported that SLPs often acted in ways that did notmatch their stated goals for patients. For example, a therapist with a stated goal ofimproving gestures was observed to preferentially reinforce spoken productions dur-ing a gestural activity. Detailed observation provided a richer understanding of howSLPs crafted goals, and how other factors (e.g., cultural biases, habituated behaviours)altered the actual implementation of goals. Similarly, studies that aim to understandthe effects of aphasia on various aspects of daily life can include not only interviewsto determine how people with aphasia feel about or perceive experiences, but alsoinclude observations to determine what actually happens. The study of life with severeaphasia described above (Parr, 2007) would likely have achieved a different result ifonly interviews were obtained. For example, a PWA might report feeling uncomfort-able at a social event or report that friends no longer visit. Such an informant mightnot be aware of the myriad behavioural or environmental manifestations that createthese feelings. Direct observation would likely identify such factors that contribute tosocial isolation and help explain interview findings.
Given the potential to gain a richer understanding of phenomena, we might won-der why other data collection approaches such as observation and video recordinghave not been more widely used. There are a number of issues such as confidential-ity, liability and time that could be deterrents to various data collection approaches.Observation and video recording require the investigator to accompany a participantinto natural situations where unexpected events might occur. For example, confiden-tiality issues arise in a hospital setting where a participant observer might inadver-tently see other patients receiving treatments or overhear confidential doctor–patientdiscussions. Liability issues might arise when an investigator accompanies a partici-pant outside of an insured facility. Finally, observations might require additional timeand effort. However, if observation would contribute to deeper understanding andexpanded knowledge, then researchers might address the barriers to using this datacollection strategy.
Another finding regarding data collection was the minimal reporting of methodsfor determining that sufficient data had been collected to achieve the aims of theresearch. As noted, it is possible that data sufficiency was addressed in studies butwas not reported. However, the qualitative research literature suggests that there areprobably reasons that researchers have difficulty with criteria such as the saturationcriterion. First, the concept of saturation is vague with minimal information availableregarding how one demonstrates that saturation has been achieved (Francis et al.,2010; Walker, 2012). Second, researchers often need to specify the number of partici-pants, settings, events and time required a priori in order to satisfy funding sources orsupervisors. Given the time accountability standards in many work settings, it is dif-ficult to employ a procedure that does not allow the investigator to know in advancehow much time or resources will be required. However, since sufficient data are a req-uisite for trustworthy and valid findings, aphasia researchers might begin to addressthis gap in qualitative design and/or reporting.

QUALITATIVE RESEARCH IN APHASIA 1293
Data analysis: Description and explanation
The final issue that merits discussion is the wide variation in the level of descriptionand interpretation in qualitative research in aphasia. The three examples describedin the results section demonstrate studies that represent different levels of analysis.While different levels of analysis are typically designed to meet study goals, investiga-tors were often unclear regarding their level of interpretation or intended outcomes.For example, all three studies described above used the term theme to refer to theirfindings. In fact, the theme label was used to describe the results in the majority of theresearch reports. Yet, themes ranged from simple groupings or listings to higher-orderinterpretations. By conflating the labels in this way, it is sometimes difficult to deter-mine the depth of analysis that the researcher meant to achieve. Terminology such asmeaning units, core concepts, categories and themes are applied to different levels ofdata by different researchers. When researchers report first-level qualitative data (e.g.,concrete listings) as themes, it can be confusing to readers. Morse (2008), the editorof Qualitative Health Research, suggested that qualitative researchers should distin-guish qualitative themes from categories. She defines a category as “a collection ofsimilar data sorted into the same place, and this arrangement enables the researchersto identify and describe the characteristics of the category” (Morse, 2008, p. 727).Thus, categories are groupings of similar data that can be compared and contrasted.Categories help to describe the data. “A theme, on the other hand, is a meaning-ful “essence” that runs through the data. Just as a theme in opera occurs over andover again, sometimes in the foreground, sometimes in the background and some-times co-occurring with other tunes, so does the theme in our research” (Morse,2008, p. 727). The theme cuts across the descriptive categories and addresses morewide-reaching issues. While qualitative research often results in multiple descriptivecategories, usually the interpretive themes of a study are fewer in number. Futurereports of qualitative research in aphasia might more clearly define the levels of datareported with these definitions in mind.
Also related to a discussion of the level of interpretation, the majority of thestudies reviewed involved analysis of core concepts and description of meaningunits or categories. Very few studies involved higher-level explanatory interpreta-tion. In considering the level of interpretation in qualitative investigation, we mightliken qualitative analysis to cooking soup. The cook begins with a list of ingredients(chicken, onions, carrots, celery, salt, pepper). These ingredients are semantic con-cepts that can be grouped into descriptive categories (meats, vegetables, spices) or theycan be contrasted into larger categories (wet versus dry ingredients; main ingredi-ents versus seasonings). However, as the soup cooks, the flavours come together tocreate an essence that is more than the sum of the parts—a chicken soupness thatdefines the product and possibly evokes broader social or cultural meanings (e.g.,curative powers of chicken soup; memories of childhood). Like a soup, qualitativeresearch might involve consideration of the basic ingredients or core concepts of aphenomenon (as in Kerr et al., 2010), analysis of these into descriptive categories ortaxonomies (as in Howe et al., 2008) and extraction of the essence or themes thatcut across the categories and offer explanation (as in Parr, 2007). This delineationis not intended as a criticism since the aims of studies differ and require differentlevels of interpretation. Rather, the pattern of existing studies can raise awarenessand provoke consideration of potential areas of growth in qualitative investigation inaphasia.

1294 SIMMONS-MACKIE AND LYNCH
CONCLUSION
This review suggested that publication of qualitative research in aphasia has increasedover the past several years, contributing to a growing literature reflecting the per-spectives of key stakeholders such as people with aphasia and their family members.The findings provide both concrete direction (e.g., improve reporting of methodsfor determining data sufficiency) and also raise a variety of questions for debateand self-reflection (e.g., should more aphasia researchers apply methods from estab-lished qualitative traditions? Should aphasia research include more data collectionmethods? Should researchers strive to increase the depth of data analysis to achievehigher-order interpretations?) Additionally, the inclusion of people with aphasia asresearch informants has been a positive direction that reflects increasing sensitivity tothe importance of the insider perspective. Since the publication of qualitative researchin aphasia and efforts to understand the insider experience of aphasia appear to beincreasing, it is important to review our research methods and consider possibilitiesfor the future. This review revealed several trends and raised a number of questions toponder as qualitative researchers continue to contribute to knowledge and practice inaphasiology.
Manuscript received 26 February 2013Manuscript accepted 17 June 2013First published online 29 July 2013
REFERENCES
Ashton, C., Aziz, N. A., Barwood, C., French, R., Savina, E., & Worrall, L. (2008). Communicativelyaccessible public transport for people with aphasia: A pilot study. Aphasiology, 22(3), 305–320.
Atkinson, R., & Flint, J. (2001). Accessing hidden and hard-to-reach populations: Snowball research strate-gies. Social Research Update, 33. Retrieved March 15, 2013 from http://sru.soc.surrey.ac.uk/SRU33.html
Bowen, G. (2008). Naturalistic inquiry and the saturation concept: A research note. Qualitative Research,8(1), 137–152.
Bradely, E., Curry, L., & Devers, K. (2007). Qualitative data analysis for health services research:Developing taxonomy, themes, and theory. Health Services Research, 42(4), 1758–1772.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology,3, 77–101.
Bronken, B., Kirkevold, M., Martensen, R., & Kvigne, K. (2012). The aphasic storyteller: Co-constructingstories to promote psychosocial well-being after stroke. Qualitative Health Research, 22(10), 1303–1316.
Brown, K., Worrall, L., Davidson, B., & Howe, T. (2010). Snapshots of success: An insider perspective onliving successfully with aphasia. Aphasiology, 24(10), 1267–1295.
Corbin, J., & Strauss, A. (2008). Basics of qualitative research (3rd ed.). Thousand Oaks, CA: Sage.Creswell, J. (2006). Qualitative inquiry and research design: Choosing among five traditions (2nd ed.).
Thousand Oaks, CA: Sage.Cruice, M., Worrall, L., & Hickson, L. (2006). Perspectives of quality of life by people with aphasia and
their family: Suggestions for successful living. Topics in Stroke Rehabilitation, 13(1), 14–24.Damico, J. S., Oelschlaeger, M., & Simmons-Mackie, N. (1999). Qualitative methods in aphasia research:
Conversation analysis. Aphasiology, 13, 667–680.Damico, J. S., & Simmons-Mackie, N. (2003). Qualitative research and speech-language pathology: Impact
and promise in the clinical realm. American Journal of Speech-Language Pathology, 12, 131–143.Damico, J. S., Simmons-Mackie, N., Oelschlaeger, M., Elman, R., & Armstrong, E. (1999). Qualitative
methods in aphasia research: Basic issues. Aphasiology, 13, 651–666.Damico, J. S., Simmons-Mackie, N., & Schweitzer, L. (1995). Addressing the third law of gardening:
Methodological alternatives in aphasiology. Clinical Aphasiology, 23, 83–94.

QUALITATIVE RESEARCH IN APHASIA 1295
Davidson, B., Worrall, L., & Hickson, L. (2003). Identifying the communication activities of older peoplewith aphasia: Evidence from naturalistic observation. Aphasiology, 17(3), 243–264.
Davidson, B., Worrall, L., & Hickson, L. (2006). Social communication in older age: Lessons from peoplewith aphasia. Topics in Stroke Rehabilitation, 13(1), 1–13.
Francis, J., Johnston, M., Robertson, C., Glidewell, L., Entwistle, V., Eccles, M. P., & Grimshaw, J. (2010).What is an adequate sample size? Operationalising data saturation for theory-based interview studies.Psychology and Health, 25, 1229–1245.
Graneheim, U., & Lundman, B. (2004). Qualitative content analysis in nursing research: Concepts,procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), 105–112.
Hammell, K. (2001). Using qualitative research to inform the client-centred evidence-based practice ofoccupational therapy. The British Journal of Occupational Therapy, 64(5), 228–234.
Hammersley, M., & Atkinson, P. (1995). Ethnography: Principles in practice (2nd ed.). London: Routledge.Howe, T., Worrall, L., & Hickson, L. (2008). Interviews with people with aphasia: Environmental factors
that influence their community participation. Aphasiology, 22(10), 1092–1120.Kerr, J., Hilari, K., & Litosseliti, L. (2010). Information needs after stroke: What to include and how to
structure it on a website. A qualitative study using focus groups and card sorting. Aphasiology, 24(10),1170–1196.
Lincoln, Y., & Guba, E. (1985). Naturalistic inquiry. Beverly Hills, CA: Sage.Luck, A., & Rose, M. (2007). Interviewing people with aphasia: Insights into method adjustments from a
pilot study. Aphasiology, 21(2), 208–224.Marshall, M. (1996). Sampling for qualitative research. Family Practice, 13(6), 522–525.Morse, J. (2005). Strategies of intraproject sampling. In P.L. Munhall (Ed.), Nursing research: A qualitative
perspective (pp. 529–540). Sudbury, ON: Jones & Bartlett.Morse, J. (2008). Confusing categories and themes. Qualitative Health Research, 18, 727.Morse, J., Barrett, M., Mayen, M., Olson, K., & Spiers, J. (2002). Verification strategies for establishing
reliability and validity in qualitative research. International Journal of Qualitative Research, 1, 21–19.Northcott, S., & Hilari, K. (2011). Why do people lose their friends after a stroke? International Journal of
Language & Communication Disorders, 46(5), 524–534.O’Halloran, R., Worrall, L., & Hickson, L. (2011). Environmental factors that influence communication
between patients and their healthcare providers in acute hospital stroke units: An observational study.International Journal of Language and Communication Disorders, 46(1), 30–47.
Parr, S. (2007). Living with severe aphasia: Tracking social exclusion. Aphasiology, 21, 98–123.Patton, M. (2002). Qualitative research and evaluation methods (3rd ed.). London: Sage.Paul, N., & Sanders, G. (2010). Applying an ecological framework to education needs of communication
partners of individuals with aphasia. Aphasiology, 24(9), 1095–1112.Penn, C., Frankel, T., Watermeyer, J., & Muller, M. (2009). Informed consent and aphasia: Evidence of
pitfalls in the process. Aphasiology, 23(1), 3–32.Richie, J., & Spencer, L. (1994). Qualitative data analysis for applied policy research. In A. Bryman & R.
Burgess (Eds.), Analysing qualitative data (pp. 173–194). London: Routledge.Riessman, C. (1993). Narrative analysis. Newbury Park, CA: Sage.Ritchie, J. & Lewis, J. (Eds.). (2003). Qualitative research practice: A guide for social science students and
researchers. London: Sage.Rolfe, G. (2006). Validity, trustworthiness and rigour: Quality and the idea of qualitative research. Journal
of Advanced Nursing, 53, 304–310.Sandelowski, M. (2000). Whatever happened to qualitative description? Research in Nursing and Health, 23,
334–340.Sandelowski, M. (2004). Using qualitative research. Qualitative Health Research, 14(10), 1366–1386.Simmons-Mackie, N. (1994). Contributions of qualitative research to the study of functional communica-
tion and outcome in aphasia. ASHA Special Interest Division, 2(4), 14–18.Simmons-Mackie, N., & Damico, J. (1999). Qualitative methods in aphasia research: Ethnography.
Aphasiology, 13, 681–688.Simmons-Mackie, N., Damico, J., & Damico, H. (1999). A qualitative study of feedback in aphasia therapy.
American Journal of Speech-Language Pathology, 8, 218–230.Simmons-Mackie, N., & Damico, J. S. (2003). Contributions of qualitative research to the knowledge base
of normal communication. American Journal of Speech-Language Pathology, 12, 144–154.Smith, J., Bekker, H., & Cheater, F. (2011). Theoretical versus pragmatic design in qualitative research.
Nurse Researcher, 18, 39–51.

1296 SIMMONS-MACKIE AND LYNCH
Smith, J., & Firth, J. (2011). Qualitative data analysis: The framework approach. Nurse Researcher, 18(2),52–62.
Smith, J., & Osborn, M. (2003). Interpretive Phenomenological Anlysis. In J. Smith (Ed.), Qualitativepsychology (pp. 51–80). Thousand Oaks, CA: Sage.
Smythe, L. (2012). Discerning which qualitative approach fits best. New Zealand College of MidwivesJournal, 4, 5–12.
Spradley, J. (1980). Participant observation. New York, NY: Holt, Rinehart and Winston.Strauss, A., & Corbin, J. (1990). Basics of qualitative research: Grounded theory procedures and techniques.
Newbury Park, CA: Sage.Thomas, D. (2006). A general inductive approach for analyzing qualitative evaluation data. American
Journal of Evaluation, 27(2), 237–246.Walker, J. (2012). Use of saturation in qualitative research. Canadian Journal of Cardiovascular Nursing,
22(2), 37–41.Wolcott, H. (1994). Transforming qualitative data: Description, analysis and interpretation. Thousand Oaks,
CA: Sage.
APPENDIX AArticles included in the Review of Qualitative Research in AphasiaAndersson, S., & Fridlund, B. (2002).The aphasic person’s views of the encounter with other people: A
grounded theory analysis. Journal of Psychiatric & Mental Health Nursing, 9(3), 285–292.Armstrong, E., Hersh, D., Hayward, C., & Brown, M. (2012). Living with aphasia: Three Indigenous
Australian stories. International Journal of Speech-Language Pathology, 14(3), 271–280.Ashton, C., Aziz, N. A., Barwood, C., French, R., Savina, E., & Worrall, L. (2008). Communicatively
accessible public transport for people with aphasia: A pilot study. Aphasiology, 22(3), 305–320.Barrow, R. (2008). Listening to the voice of living life with aphasia: Anne’s story. International Journal of
Language & Communication Disorders, 43(Supplement 1), 30–46.Bronken, B., Kirkevold, M., Martensen, R., & Kvigne, K. (2012). The aphasic storyteller: Co-constructing
stories to promote psychosocial well-being after stroke. Qualitative Health Research, 22(10), 1303–1316.Brown, K., McGahan, L., Alkhaledi, M., Seah, D., Howe, T., & Worrall, L. (2006). Environmental factors
that influence the community participation of adults with aphasia: The perspective of service industryworkers. Aphasiology, 20(7), 595–615.
Brown, K., Worrall, L., Davidson, B., & Howe, T. (2010). Snapshots of success: An insider perspective onliving successfully with aphasia. Aphasiology, 24(10), 1267–1295.
Brown, K., Worrall, L., Davidson, B., & Howe, T. (2011). Exploring speech-language pathologists’ per-spectives about living successfully with aphasia. International Journal of Language & CommunicationDisorders, 46(3), 300–311.
Bruce, C., Parker, A., & Renfrew, L. (2006). ‘Helping or something’: Perceptions of students with aphasiaand tutors in further education. International Journal of Language & Communication Disorders, 41(2),137–154.
Cherney, L., Halper, A., & Kaye, R. (2011). Computer-based script training for aphasia: Emerging themesfrom post-treatment interviews. Journal of Communication Disorders, 44(4), 493–501.
Cruice, M., Hill, R., Worrall, L., & Hickson, L. (2010). Conceptualising quality of life for older people withaphasia. Aphasiology, 24(3), 327–347.
Cruice, M., Worrall, L., & Hickson, L. (2006). Perspectives of quality of life by people with aphasia andtheir family: Suggestions for successful living. Topics in Stroke Rehabilitation, 13(1), 14–24.
Dalemans, R., de Witte, L., Wade, D., & van den Heuvel, W. (2010). Social participation through the eyesof people with aphasia. International Journal of Language and Communication disorders, 45(5), 537–550.
Davidson, B., Howe, T., Worrall, L., Hickson, L. & Togher, L. (2008). Social participation for older peoplewith aphasia: the impact of communication disability on friendships. Topics in Stroke Rehabilitation,15(4), 325–340.
Davidson, B., Worrall, L., & Hickson, L. (2003). Identifying the communication activities of older peoplewith aphasia: Evidence from naturalistic observation. Aphasiology, 17(3), 243–264.
Davidson, B., Worrall, L., & Hickson, L. (2006). Social communication in older age: Lessons from peoplewith aphasia. Topics in Stroke Rehabilitation, 13(1), 1–13.
Davidson, B., Worrall, L., & Hickson, L. (2008). Exploring the interactional dimension of social communi-cation: A collective case study of older people with aphasia. Aphasiology, (3), 235–257.

QUALITATIVE RESEARCH IN APHASIA 1297
Elman, R. J., & Bernstein-Ellis, E. (1999). Psychosocial aspects of group communication treatment:Preliminary findings. Seminars in Speech & Language, 20(1), 65–72.
Ferguson, A., Duffield, G., & Worrall, L. (2010). Legal decision-making by people with aphasia: Criticalincidents for speech. International Journal of Language and Communication Disorders, 45(2), 244–258.
Fox, L., Poulsen, S., Bawden, K., & Packard, D. (2004). Critical elements and outcomes of a residential,family-based intervention for aphasia caregivers. Aphasiology, 18, 1177–1199.
Garcia, L., Barrette, J., & Laroche, C. (2000). Perceptions of the obstacles to work reintegration for personswith aphasia. Aphasiology, 14(3), 269–288.
Greig, C., Harper, R., Hirst, T., Howe, T., & Davidson, B. (2008). Barriers and facilitators to mobile phoneuse for people with aphasia. Topics in Stroke Rehabilitation, 15(4), 307–324.
Grohn, B., Worrall, L., Simmons-Mackie, N., & Brown, K. (2012). The first 3-months post-stroke: Whatfacilitates successfully living with aphasia? International Journal of Speech-Language Pathology, 14(4),390–400.
Hallé, M., Duhamel, F., & Le Dorze, G. (2011). The daughter-mother relationship in the presence ofaphasia: How daughters view changes over the first year poststroke. Qualitative Health Research, 21(4),549–562.
Hersh, D. (2003). Weaning clients from aphasia therapy: Speech pathologists’ strategies for discharge.Aphasiology, 17, 1007–1029.
Hersh, D. (2009). How do people with aphasia view their discharge from therapy? Aphasiology, 23(3):331–350.
Hersh, D. (2010). Aphasia therapists’ stories of ending the therapeutic relationship. Topics in StrokeRehabilitation, 17(1), 30–38.
Hersh, D., Sherratt, S., Howe, T., Worrall, L., Davidson, B., & Ferguson, A. (2012). An analysis of the“goal” in aphasia rehabilitation. Aphasiology, 26(8), 971–984.
Hinckley, J. (2005). The piano lesson: An autoethnography about changing clinical paradigms in aphasiapractice. Aphasiology, 19, 765–779.
Howe, T., Davidson, B., Worrall, L., Hersh, D., Ferguson, A., Sherratt, S., & Gilbert, J. (2012). ‘You neededto rehab... families as well’: Family members’ own goals for aphasia rehabilitation. International Journalof Language & Communication Disorders, 47(5), 511–521.
Howe, T., Worrall, L., & Hickson, L. (2008a). Interviews with people with aphasia: Environmental factorsthat influence their community participation. Aphasiology, 22(10), 1092–1120.
Howe, T., Worrall, L., & Hickson, L. (2008b). Observing people with aphasia: Environmental factors thatinfluence their community participation. Aphasiology, 22(6), 618–643.
Ireland, C., & Wotton, G. (1996). Time to talk: Counselling for people with dysphasia. Disability &Rehabilitation, 18(11), 585–591.
Johansson, M. B., Carlsson, M., Sonnander, K. (2012). Communication difficulties and the use of commu-nication strategies: From the perspective of individuals with aphasia. International Journal of Language& Communication Disorders, 47(2), 144–155.
Jones, F., Mandy, A., & Partridge, C. (2008). Reasons for recovery after stroke: A perspective based onpersonal experience. Disability & Rehabilitation, 30(7), 507–516.
Kardosh, B., & Damico, J. (2009). The contribution of language in shaping clinical culture: Palestinianaphasics and families living in Israel. Asia Pacific Journal of Speech, Language & Hearing, 12(3),243–252.
Kerr, J., Hilari, K., & Litosseliti, L. (2010). Information needs after stroke: What to include and how tostructure it on a website. A qualitative study using focus groups and card sorting. Aphasiology, 24(10),1170–1196.
Knight, K., Worrall, L., Rose, T., & Roth, E. (2006). The provision of health information to stroke patientswithin an acute hospital setting: What actually happens and how do patients feel about it? Topics inStroke Rehabilitation, 13(1), 78–97.
Larsson, I., & Thoren-Jonsson, A. (2007) The Swedish speech interpretation service: An exploratorystudy of a new communication support provided to people with aphasia. Augmentative and AlternativeCommunication, 23(4), 312–322.
Le Dorze, G., & Brassard, C. (1995). A description of the consequences of aphasia on aphasic persons andtheir relatives and friends, based on the WHO model of chronic diseases. Aphasiology, 9(3), 239–255.
Le Dorze, G., Brassard, C., Larfeuil, C., & Allaire, J. (1996). Auditory comprehension problems in aphasiafrom the perspective of aphasic persons and their families and friends. Disability & Rehabilitation,18(11), 550–558.

1298 SIMMONS-MACKIE AND LYNCH
Le Dorze, G., Julien, M., Brassard, C., Durocher, J., & Boivin, G. (1994). An analysis of the communicationof adult residents of a long-term care hospital as perceived by their caregivers. European Journal ofDisorders of Communication, 29(3), 241–268.
Le Dorze, G., & Signori, F. (2010). Needs, barriers and facilitators experienced by spouses of people withaphasia. Disability & Rehabilitation, 32(13), 1073–1087.
Le Dorze, G., Tremblay, V., & Croteau, C. (2009). A qualitative longitudinal case study of a daughter’sadaptation process to her father’s aphasia and stroke. Aphasiology, 23(4), 483–502.
Legg, L., Stott, D., Ellis, G., & Sellars, C. (2007). Volunteer stroke service (VSS) groups for patients withcommunication difficulties after stroke: A qualitative analysis of the value of groups to their users.Clinical Rehabilitation, 21(9), 794–804.
Luck, A., & Rose, M. (2007). Interviewing people with aphasia: Insights into method adjustments from apilot study. Aphasiology, 21(2), 208–224.
Lynch, K., Damico, J., Damico, H., Tetnowski, J., & Tetnowski, J. (2009). Reading skills in an individualwith aphasia: The usefulness of meaning-based clinical applications. Asia Pacific Journal of Speech,Language & Hearing, 12(3), 221–234.
Michallet, B., Le Dorze, G., & Tetreault, S. (2001). The needs of spouses caring for severely aphasic persons.Aphasiology, 15, 731–747.
Michallet, B., Tetreault, S., & Le Dorze, G. (2003). The consequences of severe aphasia on the spouses ofaphasic people: A description of the adaptation process. Aphasiology, 17, 835–859.
Mitchell, K., Skirton, H., & Monrouxe, L. (2011). Amelioration, regeneration, acquiescent and discordant:An exploration of narrative types and metaphor use in people with aphasia. Disability & Society, 26(3),321–335.
Mumby, K., & Whitworth, A. (2012). Evaluating the effectiveness of intervention in long-term aphasiapost-stroke: The experience from CHANT (Communication Hub for Aphasia in North Tyneside).International Journal of Language & Communication Disorders, 47(4), 398–412.
Nakano, E., & Hinckley, J. (2010). Therapy discharge becomes part of the life story. Topics in StrokeRehabilitation, 17(1), 39–46.
Nätterlund, B. (2010). A new life with aphasia: Everyday activities and social support. Scandinavian Journalof Occupational Therapy, 17, 117–129.
Nätterlund, B. (2010). Being a close relative of a person with aphasia. Scandinavian Journal of OccupationalTherapy, 17(1), 18–28.
Nordehn, G., Meredith, A., Bye, L., & Roth, E. (2006) A preliminary investigation of barriers to achievingpatient-centered communication with patients who have stroke-related communication disorders. Topicsin Stroke Rehabilitation, 13(1), 68–77.
Northcott, S., & Hilari, K. (2011). Why do people lose their friends after a stroke? International Journal ofLanguage & Communication Disorders, 46(5), 524–534.
O’Halloran, R., Worrall, L., & Hickson, L. (2011). Environmental factors that influence communicationbetween patients and their healthcare providers in acute hospital stroke units: An observational study.International Journal of Language and Communication Disorders, 46(1), 30–47.
Parr, S. (1994). Coping with aphasia: Conversations with 20 aphasic people. Aphasiology, 8(5), 457–466.Parr, S. (1995). Everyday reading and writing in aphasia: Role change and the influence of pre-morbid
literacy practice. Aphasiology, 9(3), 223–238.Parr, S. (2001). Psychosocial aspects of aphasia: Whose perspectives? Folia Phoniatrica et Logopaedica,
53(5), 266–288.Parr, S. (2007). Living with severe aphasia: Tracking social exclusion. Aphasiology, 21(1), 98–123.Paul, N., & Sanders, G. (2010). Applying an ecological framework to education needs of communication
partners of individuals with aphasia. Aphasiology, 24(9), 1095–1112.Pearl, G., Sage, K., & Young, A. (2011). Involvement in volunteering: An exploration of the personal
experience of people with aphasia. Disability & Rehabilitation, 33(19/20), 1805–1821.Penn, C., Frankel, T., Watermeyer, J., & Muller, M. (2009). Informed consent and aphasia: Evidence of
pitfalls in the process. Aphasiology, 23(1), 3–32.Pound, C., Parr, S., & Duchan, J. (2001), ‘Using partners’ autobiographical reports to develop, deliver, and
evaluate services in aphasia’. Aphasiology, 15(5), 477–493.Purves, B., Logan, H., & Marcella, S. (2011). Intersections of literal and metaphorical voices in aphasia.
Aphasiology, 25(6–7), 688–699.Rohde, A., Townley-O’Neill, K., Trendall, K., Worrall, L., & Cornwell, P. (2012). A comparison of client
and therapist goals for people with aphasia: A qualitative exploratory study Aphasiology, 26(10),1298–1315.

QUALITATIVE RESEARCH IN APHASIA 1299
Rose, T., Worrall, L., Hickson, L., & Hoffmann, T. (2011). Aphasia friendly written health information:Content and design characteristics. International Journal of Speech-Language Pathology, 13(4), 335–347.
Sherratt, S., Worrall, L., Pearson, C., Howe, T., Hersh, D., & Davidson, B. (2011). “Well it has to belanguage-related”: Speech-language pathologists’ goals for people with aphasia and their families.International Journal of Speech-Language Pathology, 13(4), 317–328.
Simmons-Mackie, N., Damico, J., & Damico, H. (1999). A qualitative study of feedback in aphasiatreatment. American Journal of Speech-Language Pathology, 8(3), 218–230.
Simmons-Mackie, N., Kagan, A., O’Neill-Christie, C., Huijbregts, M., McEwen, S., & Willems, J. (2007).Communicative access and decision making for people with aphasia: Implementing sustainable healthcare systems change. Aphasiology, 21(1), 39–66.
Sorin-Peters, R. (2004). The evaluation of a learner-centered training programme for spouses of adults withchronic aphasia using qualitative case study methodology. Aphasiology, 18(10), 951–975.
Sundin, K., Astrid, N., & Jansson, L. (2001). The meaning of skilled care providers’ relationships withstroke and aphasia patients. Qualitative Health Research, 11(3), 308–321.
True, G., Bartlett, M., Fink, R., Linebarger, M., & Schwartz, M. (2010). Perspectives of persons withaphasia towards SentenceShaper to Go: A qualitative study. Aphasiology, 24(9), 1032–1050.
van der Gaag, A., Smith, L., Davis, S., Moss, B., Cornelius, V., Laing, S., & Mowles, C. (2005). Therapy andsupport services for people with long-term stroke and aphasia and their relatives: A six-month follow-upstudy. Clinical Rehabilitation, 19(4), 372–380.
Wade, J., Mortley, J., & Enderby, P. (2003). Talk about IT: Views of people with aphasia and their partnerson receiving remotely monitored computer-based word finding therapy. Aphasiology, 17, 1031–1056.
Worrall, L., Sherratt, S., Rogers, P., Howe, T., Hersh, D., Ferguson, A., & Davidson, B. (2011). What peoplewith aphasia want: Their goals according to the ICF. Aphasiology, 25(3), 309–322.
Young, A., Gomersall, T., & Bowen, A. (2012). Trial participants’ experiences of early enhanced speechand language therapy after stroke compared with employed visitor support: A qualitative study nestedwithin a randomised controlled trial. Clinical Rehabilitation. Early online publication.
APPENDIX B
Information extracted for each article under review
(1) Topic: What is the broad topic of the investigation (e.g., early hospital experiencesof people with aphasia, life as a child of someone with aphasia)?
(2) Participants: Describe the type of participants (e.g., people with aphasia, familymembers, doctors).
(3) Research Tradition/Design: What is the “tradition” or design that guided thestudy (e.g., ethnography, phenomenology)? This should reflect the label explicitlyused to describe the tradition or design as stated in the article, not an inferenceabout the design based on reading the article. Enter the exact description that wasgiven in the article.
(4) Data Collection(A) Sampling method: What was the method of obtaining the sample (e.g., con-
venience, purposeful)? An explicit statement of the method is required; ifnot explicitly stated in the article, enter as “not stated.”
(B) Data collection method: What method of data collection was employed (e.g.,observation, interview, video recording)?
(C) Is there a statement regarding data sufficiency?! Yes or No: Is there an explicit mention of an attempt to determine datasufficiency or attempt to obtain saturation in the article? To meet thiscriterion, the authors need not describe how this was done, only refer toan effort to obtain sufficient data.
(D) Method of obtaining data sufficiency (saturation) is described

1300 SIMMONS-MACKIE AND LYNCH! Yes or No: The actual method of determining data sufficiency wasdescribed.
(5) Data Analysis(A) Data analysis methods: What was the stated method of analysing the data
(e.g., thematic analysis)? Enter the exact label used and the relevant citation.For generic descriptions, enter the language used to describe the analysis(e.g., categorising data)
(B) Level of analysis! Descriptive: the analysis provides a detailed, meaningful and relevantaccount of the topic under study; the project develops a descriptivetaxonomy or categorical description of a phenomenon, an event or agroup.! Explanatory: the analysis provides a deep interpretation that goesbeyond listings or categories and towards higher-order explanationsand/or interpretations of the phenomena, event or group.
APPENDIX C
Categories derived from a qualitative analysis of the extracted dataTopics of study derived from the extracted data! Investigates the experience of aphasia (for PWA, SLPs, Family, others) (e.g., qualityof life, living successfully with aphasia, what it is like for family members living withaphasia).! Investigates an intervention, treatment or program! Investigates discharge from intervention or program! Investigates or identifies goals or needs of PWA, family or others! Investigates issues associated with culture and aphasia! Investigates environmental factors or issues! Investigates activity or participation (e.g., what people do, communication activi-ties, relationships, work, leisure)! Other (does not fit in the above topics)
Types of participants derived from the extracted data! PWA! Family or Caregivers! SLPs! Other Service providers (e.g., nurses, attendants)! Others
Research Tradition or design derived from the extracted data! Qualitative study—nonspecific (used for articles where no explicit tradition is givenas in “qualitative methods” or “qualitative study” or when a pragmatic approach isreferenced as in “descriptive qualitative investigation”). Note the exact terminologyused in the article.! Phenomenology (used for any type of phenomenological investigation)! Grounded theory! Ethnography! Narrative

QUALITATIVE RESEARCH IN APHASIA 1301
Data collection method! Interview(s)! Focus group(s)! Observation! Diaries! Video or audio recording! Review of artefacts! Other
Sampling method! Convenience sample! Random or semi-random sampling! Snowball sampling! Purposeful sampling! Maximum variation sampling! Other! Not stated
Data analysis methods! Not stated or nonspecific analysis (e.g., qualitative analysis, sorting and coding,classifying, categorising)! Qualitative content analysis! Thematic analysis! Framework analysis! Open, axial and selective coding! NUD-IST (QSR International, Doncaster, Victoria, Australia) or other qualitativeanalysis software! Narrative analysis! Constant comparative method! Interpretive phenomenological analysis (IPA)! Other

Copyright of Aphasiology is the property of Psychology Press (UK) and its content may notbe copied or emailed to multiple sites or posted to a listserv without the copyright holder'sexpress written permission. However, users may print, download, or email articles forindividual use.