Embed Size (px)
Citation preview

Return to Work:
Why can’t we all be on the same team?
Kevin Bourke MD MRO CAME
2014 CAPA Conference

Ideal RTW Process
1.Got sick / injured.2.Off work for treatment &
recovery.3.Got all better.4.Got back to work.5.All within Presley-Reed
timeline!

Real World RTW• Not coordinated.• Attendings not exposed /
experienced.• Occurs by default / tradition
– E.g. - 42d off for Cesarean or tib-fib
• Default = laissez-faire.• Laissez-faire = longer off
work.• Longer off work = harder to
return.
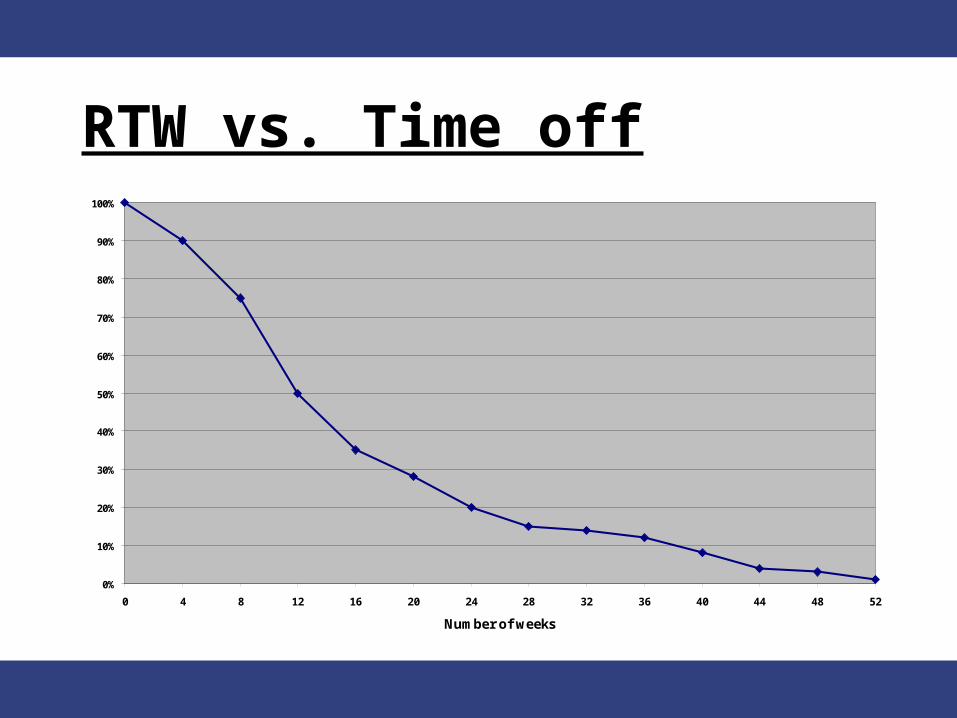
RTW vs. Time off
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Number of weeks

Approach:• “The RTW Space”
– Players/roles • “Company PA” vs. “Attending PA”
– Aim of RTW
• Concepts– Impairment vs. Disability– Employment Limitations– Tolerance

Approach (II):• RTW Challenges:
– Communication (Not!)– Guiding other roles– Silos
• Solutions / work-arounds– Teach ‘em!– FORMS! (Pitfalls and Pearls)

Roles:• Employee / worker• Attending clinician*• Employer
– Supervisor vs. corporate body• Third Party Insurer ?• You, the “Company PA”*

Employee / worker• Work = Good!
– $, stuff, esteem, self-worth– Positive benefits on health no
longer disputed– Another talk:
• Motivation, cultural issues (Sick Day banks, 42 days for hyst, etc.)
GP• “… to provide medical
treatment and guidance … to restore health; optimize social, psychological, and functional capabilities; and minimize the negative effects of injury.”1
1“Can you go back to work?” Can Fam Physician 2011;57:202-9
RTfW: Let’s Back up:• Why do people Return to (full) Work?
• Because they were “off sick” or restricted in their duties due to illness/injury.
• Received investigation / treatment for illness/injury
• GP/clinician identified the illness / injury / ”Sick” status...
• Illness / injury occurred.– 3 of these 4 involve the attending
physician(s)…… !!!!

Positions:
• Canadian Medical Association 2013 – “The Physician’s Role in Helping Patients Return to Work...”
• American Medical Assoc. 2004 – “Physician Guidelines for RTW”
• ACOEM 2008- “The Personal Physician’s Role in Helping Pts ... Stay at Work or Return to Work”

AMA Guide to RTW
• “The physician must communicate and support a reasonable (accurate??) clinical estimate of what the patient can do and can no longer do.”
• A Physician’s Guide to RTW – Talmage and Melhorn Eds. AMA Press 2005 …..Great read, and gift!
Clinicians‘ challenges:• Occ Med rare in curricula
– Dal / Irving establish Chair; before that?
• Work for their patient, not his/her boss– Goals broader, “the greater good”.
• GP ≠ disability decision-maker!– GPs often expand to fit role(s)... “can
do” attitude

Clinicians‘ challenges:• Haven’t been on the shop
floor!– Work described by patient:
• “gotta be 110% before I go back...”
• Work forms / liaison not “covered”.
• Goals broader, “the greater good”.

RTW Aim:• To safely resume previously
limited work duties, in a timely manner.
• WORK IS NOT DIGITAL,• HEALING IS NOT DIGITAL,• WHY SHOULD RTW BE ??

CONCEPTS• Impairment :
– loss of / loss of use of a body part, system, or function.
– Measureable / consistent
• Disability:– real-world impact of an
impairment.– varies between individuals

Employment Limitation(s)• Based upon IMPAIRMENT(s)• “Cannot do...” vs. “Should not
do...”• Shouldn't be a surprise to
employee• Means somebody is not paying attention
• Want clinician’s (neutral) assessment, not transcription of their pt’s opinion
• “Just the facts, Ma’am...”
Employment Limitation(s)
• KNOW THE JOB.– Establishes credibility– Reduces BS exposure

Know the job!

Employment Limitation(s)
• Detail specific task(s)– not the job, location, or boss– Suprvr gets to actually manage.
• Be inventive!– ANY return to workplace =
momentum

Example Limitation(s)
• “No lifting or push/pull over
25kg.”
• “Must be able to change
physical position (e.g.-
sit/stand) up to hourly.”
• No repetitive
bending/stooping.” • “Should not be employed in
supervisory role.”
Confidentiality
• EL’s are task-specific–Contain NO MEDICAL INFO
–Therefore not confidential.•Fit to file in HR.

TOLERANCE• Ability to continue
work/activity at a specific level.– Personal decision:
• Pros ($, other benefits)• Cons (shifts, commute, symptoms,
etc.)• Like EtOH, boredom thresholds...
highly variable
Getting the info you need:
• IMPAIRMENT(S)!– NOT placement / HR advice.– REALLY want to ask that fitness
question?– Can ask about Pt’s safety with
Dx/Tx
• YOU know JOB, attending knows Dx/Sx
• Yes/No questions = Yes/No answers
Modified work:
• No excuse in 2014 .... (maybe CEO)
• KNOW THE JOB / SHOP.– Be seen there by suprvr’s– Nurture RTW tasks
What are we (you) asking them?
• Yes/No questions get Yes/No answers....
• “Please indicate the nature of the illness....”???
• As a result of treatment, the patient/claimant’s condition has: □ Improved □ Deteriorated □ Remained the same □ Stabilized

Answers useful?
• Does GP understand what you want to know?
• Deduce their role from your questions?

SUM:• GP inherently involved in pt’s
“Sick Status”• Reporting and RTW
assessment added later• RTW / Occ Health not Med
School “required elements” • GPs work for their patient(s)
… “advocate”

Challenges:
• Yes, sometimes they won’t answer/rtn call.– MD<>MD can help.... got one? Hire
one?
• Delays in responding?– Explicit req fax... For right reasons,
and $delta
• Strays into HR/admin realm?– Thank 'em but re-ask the initial
question(s)

Challenges (cont’d):
• Teach old docs new tricks?– Maybe not… but clarify… hold
their feet to the fire, or get someone who can….
• Info seems incoherent with case– “quick look” by Occ Doc for
way fwd..?






























