Embed Size (px)
Citation preview

RESURFACING OF THE DAMAGED HAND BY THE PREFABRICATED FREE FLAP INCLUDING SERRATUS FASCIA: A CASE REPORT BORIS L. SHILOV, M.D.
MICROSURGERY 16S70-372 1995
T h e concept of free flap prefabrication is relatively new and has not received wide clinical application at this present time. However, prefabricated flaps have different advan- tages compared with the axial-pattern flaps and at the same time can be designed by the surgeon, who can combine the different tissues needed for reconstruction in one complex. Few case reports have been published and only two types of fascia (temporo-parietal and forearm) have been used as a vascular carrier in prefabricated flaps.’.2 This case report describes a hitherto undescribed free flap prefabrication em- ploying the serratus fascia.
CASE REPORT A 34-year-old white man presented with late radiation
damage to his left hand after he received an unknown dose of gamma-radiation, violating safety rules 5 years ago. The index and middle fingers were amputated soon after the accident due to severe damage. The skin of the palm and palmar surface of the ring and little fingers had signs of atrophic dermatitis with recurrent ulceration, and both of these fingers had flexion contractures (Fig. 1). An os- teoporotic process of the bones of the hand was present radiographically (Fig. 2). It was decided to resurface the palm partially as well as the ring and little fingers, thus releasing the contractures. The patient rejected a proposal to use radial and dorsal foot flaps, hence the selection of the flap prefabrication method. The serratus fascia and the per- imysium of the serratus anterior muscle in one complex was
From the Department of Plastic and Reconstructive Microsurgery, National Research Centre of Surgery, Moscow, Russia.
Acknowledgments: We thank Michael C. Bried, P.A., and ME. Nancy Harper (Section of Plastic and Maxillofacial Surgery, The Emory Clinic) for the prep- aration of this manuscript.
Address reprint requests to Dr. Boris L Shilov, Department of Plastic and Reconstructive Microsurgery, National Research Centre of Surgery, Abrikos- ovsky per. 2, 119874 Moscow, Russia.
Received for publication September 11, 1994; accepted February 1, 1995.
undermined with its vascular pedicle (Fig. 3). Through the same incision a subcutaneous “pocket” was prepared on the lateral surface of the thoracic wall and the fascia was transposed under the skin and fixed (Figure 4).
One month later, using the Doppler probe, the vascular pedicle and its main branches were delineated in the zone of prefabrication (Fig. 5). The whole fasciocutaneous complex was raised and transferred as a free flap to the hand, after the damaged skin was excised and the contractures released (Fig. 6). The microanastomoses were accomplished with an ulnar vascular bundle. The exteriorised fat pad on the dorsal surface between the ring and little fingers was covered with split skin graft (Figs. 7, 8).
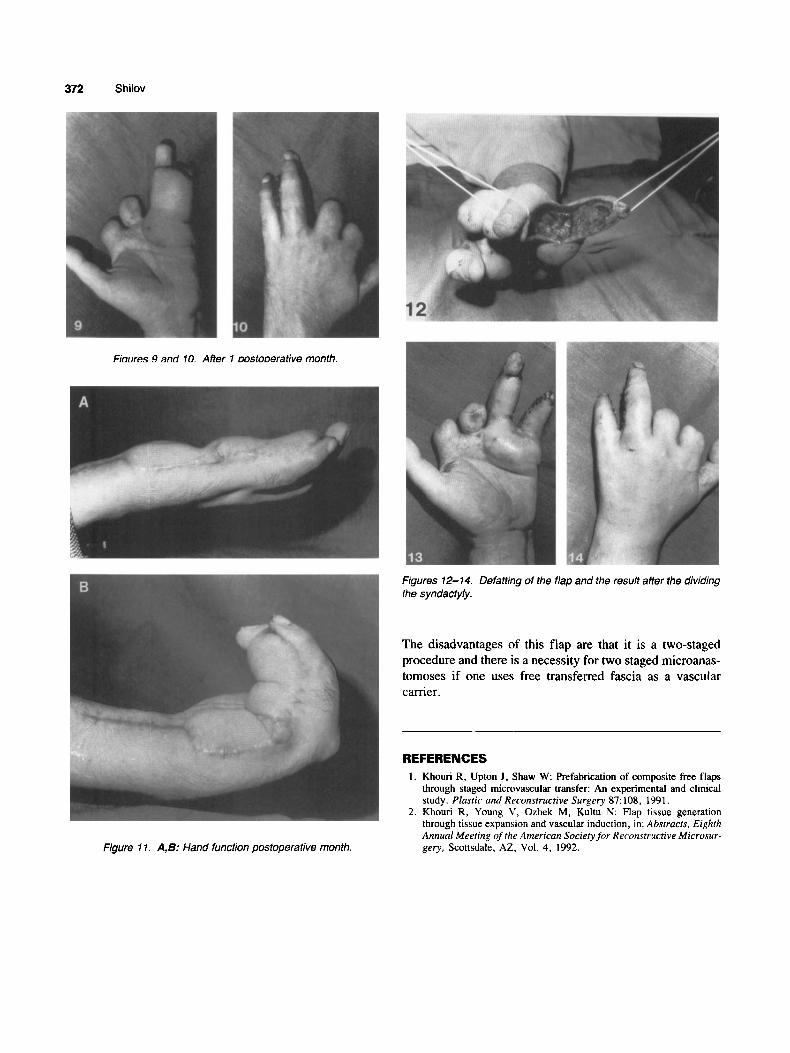
Complete and uneventful healing was observed within 1 month, (Figs. 9, lo), and hand function was also satisfac- tory in 1 month (Fig. 11). Two months post-operatively the flap was defatted and the syndactyly was divided (Figs. 12-14).
DISCUSSION Hand reconstruction procedures often demand thin, pli-
able, well-nourished flaps with long vascular pedicles. The most reliable flaps in these situations are the radial arm and the dorsal foot flaps. Unfortunately, they cause severe do- nor scars, are often associated with prolonged healing pe- riods, and sacrifice the the dominant hand artery. Prefabri- cated flaps can serve as alternatives in these cases. Prefabricated flaps have the following advantages:
1. The surgeon can determine the thickness and skin surface of the flap (e.g., thick, thin, with or without hairs).
2. The donor zone can be hidden if the surgeon uses the transposed serratus fascia (lateral aspect of the chest wall); also if the surgeon uses free transferred fascia the donor zone can be anywhere on the body surface.
3. The vascular pedicle is long and has a comparatively large vessel diameter.
4. The fascia as a deep layer of the flap has good tissue surface contact with tendons.
0 1995 Wiley-Liss, Inc.
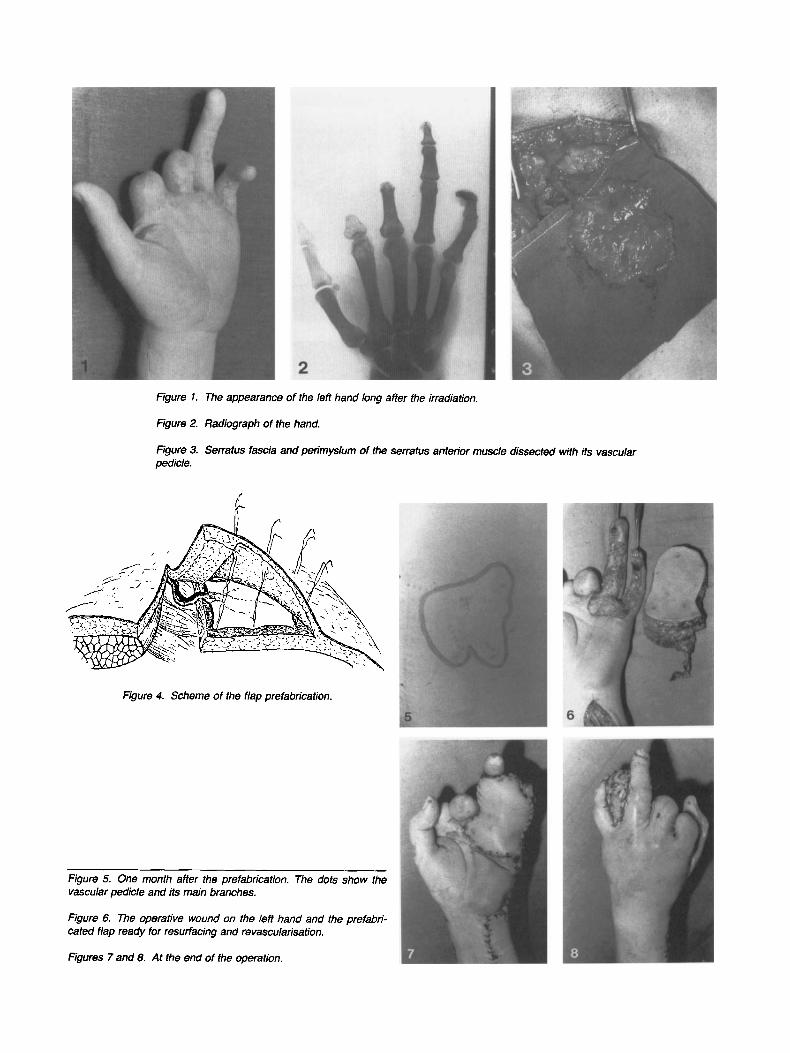
Figure 1. The appearance of the left hand long after the irradiation.
Figure 2. Radiograph of the hand.
Figure 3. Serratus fascia and perimysium of the serratus anterior muscle dissected with its vascular pedicle.
Figure 4. Scheme of the flap prefabrication.
Figure 5. One month after the prefabrication. The dots show the vascular pedicle and its main branches.
Figure 6. The operative wound on the left hand and the prefabri- cated flap ready for resurfacing and revascularisation.
Figures 7 and 8. At the end of the operation.
372 Shilov
Fioures 9 and 10. After 1 aostooerative month.
Figures 12-14. Defafting of the flap and the result after the dividing the syndacty/y.
The disadvantages of this flap are that it is a two-staged procedure and there is a necessity for two staged microanas- tomoses if one uses free transferred fascia as a vascular carrier.
Figure 1 1. A, B: Hand function postoperative month.
REFERENCES 1 . Khouri R, Upton J , Shaw W: Prefabrication of composite free flaps
through staged micmvascular transfer: An experimental and clinical study. Plastic and Reconstructive Surgery 87: 108, 1991.
2. Khouri R , Young V, Ozbek M, Kultu N: Flap tissue generation through tissue expansion and vascular induction, in: Abstracts, Eighth Annual Meeting of the American Society for Reconstructive Microsur- gery, Scottsdale, AZ, Vol. 4, 1992.


![[PPT]PREFABRICATED BUILDING - Wikispacescarlavl.wikispaces.com/file/view/PREFABRICATED+BUILDING.ppt · Web viewPREFABRICATED BUILDING Vargas, Valentina Vásquez, Carla CONTENT: Prefabricated](https://img.dokumen.tips/doc/110x75/5ada5d397f8b9a6d7e8ca107/pptprefabricated-building-buildingpptweb-viewprefabricated-building-vargas.jpg)


























