Embed Size (px)
Citation preview

Revue de chirurgie orthopédique et réparatrice de l’appareil moteur (2008) 94, e28—e34
Disponib le en l igne sur www.sc iencedi rec t .com
MÉMOIRE
Results of surgical treatment of congenital convexpes valgus (ten nonidiopathic feet)Résultats du traitement chirurgical du pied convexecongénital
K. Ayadi ∗, M. Trigui, F. Gdoura, W. Zribi, M. Zribi, M.H. Elleuch, H. Keskes
Service de chirurgie orthopédique et de traumatologie, CHU Habib Bourguiba, route El Aïn Km 0,5, 3000 Sfax, Tunisia
Accepted 5 December 2007
KEYWORDSVertical talus;Treatment;Surgery
SummaryPurpose of the study. — Congenital pes valgus is a rare and complex deformity of the foot raisingserious diagnostic and therapeutic challenges. The purpose of our work was to present thesurgical procedures used in our series and to analyze outcome.Material and methods. — Ten feet presenting congenital convex pes valgus treated surgicallyover a six-year period using the same operative technique were reviewed at minimum five yearsfollow-up. Idiopathic deformities were excluded from this series. Deformities were secondaryto arthrogryposis in five feet, multiple malformative syndrome in four, and diastematomyelia inone. The surgical technique used two approaches: a posteromedial incision to release the dorsalflexors, disinsert the tibialis posterior, open the talonavicular joint, release the Achilles tendonand release the posterior tibiotalar capsule; a lateral incision to lengthen the fibular tendonsand perform an osteotomy of the anterior process of the calcaneum. A talonavicular pin and acalcaneocuboid pin maintained the correction. The tibialis posterior tendon was reinserted onthe anterior aspect of the talonavicular capsule after incision of the dislocation chamber.Results. — Outcome was considered good in five cases and fair in five. Outcome was fair in thearthrogryposis feet. Undercorrection was observed in two feet and valgus flatfoot in three. Talarnecrosis occurred in one foot and navicular necrosis in two.Discussion. — Simultaneous correction of the different anomalies observed in the congenitalconvex foot was achieved in this series. The anatomic and functional results were satisfactory.
We recommend avoiding overly extensive release in order to decrease the risk of talar and navi-cular necrosis. It is also important to check the reduction radiographically during the operation.Patients should use an orthesis for several months postoperatively to avoid recurrence.© 2008 Elsevier Masson SAS. All rights reserved.DOI of original article:10.1016/j.rco.2007.12.001.∗ Corresponding author.
E-mail address: [email protected] (K. Ayadi).
0035-1040/$ – see front matter © 2008 Elsevier Masson SAS. All rights reserved.doi:10.1016/j.rco.2007.12.020

Results of surgical treatment of congenital convex pes valgus e29
MOTS CLÉSPied convexecongénital ;Traitement ;Chirurgie
Résumé Le pied convexe congénital est une malformation rare du pied qui pose plusieursproblèmes d’ordre diagnostique et thérapeutique. De nombreuses techniques de correctionchirurgicale ont été proposées. Nous rapportons dix cas de pied convexe congénital non idio-pathique, traités chirurgicalement selon la même technique opératoire sur une période de sixans avec un recul minimal de cinq ans. La malformation était secondaire à une arthrogryposedans cinq cas, à un syndrome polymalformatif dans quatre cas et à une diastématomyélie dansun cas. La technique chirurgicale comportait deux abords : un abord postéromédial permettantune libération des releveurs du pied, une désinsertion du tibial postérieur, une ouverture del’articulation talo-naviculaire et une libération du tendon d’Achille et de la capsule tibiota-lienne postérieure et un abord latéral permettant l’allongement des tendons fibulaires et uneostéotomie de l’apophyse antérieure du calcanéum. Les résultats ont été bons dans cinq caset moyens dans cinq cas. Les résultats moyens ont été observés dans les cas d’arthrogrypose.On a observé une hypocorrection dans deux cas et un aspect de pied plat valgus dans trois cas.Une nécrose du talus est survenue dans un cas et une nécrose du naviculaire dans deux cas. Latechnique utilisée a permis la correction simultanée des différentes anomalies du pied convexecongénital et a donné des résultats anatomiques et fonctionnels satisfaisants.© 2008 Elsevier Masson SAS. All rights reserved.
na
l
••
•
aan(stn
sCftoa
vflioyo
Introduction
Congenital pes valgus is a rare and complex deformity ofthe foot associating irreducible equinus of the hindfoot,irreducible talonavicular dislocation, and irreducible dorsalflexion of the forefoot at the transverse tarsal joint. Theseosteoarticular abnormalities were accompanied by a numberof ligament, tendon, and skin soft tissue anomalies [1,2], allof which made treatment of the vertical talus difficult. Thedifferent nonsurgical treatment methods available (rehabi-litation, casts, orthotic devices) give unsatisfactory resultseven if treatment is begun at birth [3]. Therefore, many sur-gical techniques have been reported in the literature. Theirgreat diversity shows how difficult surgical treatment is. Theresults are far from satisfactory, whatever the techniqueused.
The purpose of our work was to present the surgical pro-cedures used in our series and to analyze outcome.
Material and methods
Over a six-year period, 14 cases of congenital convex pes val-gus were operated on in our institution. Of these 14 feet, weretained ten feet operated on with the same surgical tech-nique with a minimum follow-up period of five years. Thisseries included seven children (four boys and three girls).The deformity was bilateral in three children. This anomalywas associated with other malformations in all cases: threechildren (five feet) had arthrogryposis, three children (fourfeet) had multiple malformative syndrome, and one child(one foot) had diastematomyelia (Table 1).
Arthrogryposis involved all four limbs in three childrenwith bilateral convex pes valgus. Two children were opera-ted on both sides and one child on a single side becausethe other was flexible. Two children also had unilateral hip
dysplasia, treated with a Salter osteotomy. The third child,who had severe arthrogryposis with substantial deformity inthe feet, was operated on at the age of 17 months, justbefore walking age. Nerve damage was severe; the childfi
st
ever walked and presented scoliosis in the oblique pelvisnd unilateral dislocation of the hip.
Three children had associated malformations in the fol-owing areas:
cleft palate with bilateral convex pes valgus;congenital talipes equinovarus on the opposite side of thevertical talus, in a child whose twin brother had died froma neurological problem with hydrencephalus;congenital myopathy with bilateral convex pes valgus. Weonly retained one foot that had been operated on at theage of six years for the study. The other side was treatedwith another surgical technique at the age of 15 months.
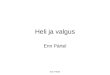
The diagnosis of convex pes valgus was both clinicalnd radiological. The clinical examination showed a convexppearance of the plantar side of the foot with talipes equi-ovarus of the hindfoot and dorsiflexion of the forefootFig. 1A). At the summit of this convexity and on the medialide of the foot, there was a bony ridge corresponding tohe head of the talus that no longer articulated with theavicular bone dislocated toward the top.
A: clinical aspect. B: preoperative radiological workuphowing that the talonavicular dislocation was irreducible.: clear improvement in the foot, which is maintained atollow-up after surgical correction. D: radiological aspect ofhe same child’s foot at follow-up showing a slight deformityf the talar dome, the navicular bone, and a reduction in themplitude of the ankle’s dorsal flexion.
In all cases, the radiological examination comprised threeiews: one frontal and two lateral, in dorsal and plantarexion (Fig. 1B). These different views demonstrated the
rreducible talonavicular dislocation. Before the appearancef the nucleus of the navicular bone, seen beginning at fourears of age, this dislocation was confirmed by the rupturef the line joining the axis of the talus and the axis of the
rst metatarsal.All of these children had had rehabilitation of their feetince birth. Successive corrective casts had been used inhree children. These nonsurgical treatments provided only

e30 K. Ayadi et al.
Table 1 Summary of patient data.
Etiology Age (months) Side Cast (weeks) Result X-ray atfollow-up
Follow-up (years)
Observation 1 Arthrogryposis 31 L 16 Good No necrosis 5Observation 2 Multiple
malformativesyndrome
17 R 16 Good No necrosis 8
30 L 16 Good No necrosis 7Observation 3 Multiple
malformativesyndrome
16 L 20 Good Navicularnecrosis, talusdeformity
8
Observation 4 Arthrogryposis 17 R 16 Fair Insufficientreduction
6
L 16 Fair Insufficientreduction
6
Observation 5 Diastematomyelia 46 L 16 Fair Naviculardeformity
9
Observation 6 Multiplemalformativesyndrome
72 L 16 Good Naviculardeformity
6
1616
at(
b
acsr
d
fisiawoi
Observation 7 Arthrogryposis 24 RL
slight clinical improvement in their feet. The age at theime of surgery varied between 16 months and six yearsTable 1).
The surgical technique used was broken down as descri-ed below.
The child was installed in the supine position onn ordinary operating table with a cushion under theontralateral buttock. The entire limb was prepared in a
terile stockinet with a pneumatic tourniquet at the limb’soot.First, a posteromedial incision was made to release theorsal flexors, with the surgeon on the plantar side of the
rta
Figure 1 Right convex pes va
Fair No necrosis 5Fair Talus deformity 5
oot and the first assistant on the opposite side. The incisions started next to the Achilles tendon, curves around in an Lhape behind the medial malleolus, then continues along thenternal edge of the foot at the junction of the dorsal skinnd the plantar skin. A dorsal cutaneous band is detachedith all of the subcutaneous fatty tissue up to the insertionf the tibialis anterior muscle. The posterior tibial pedicles repaired and isolated.
The anterior release begins with the excision of the ante-ior fibrosis retaining the forefoot in dorsal flexion, thenhe tibialis anterior tendon is lengthened and the extensorsre lengthened if necessary until transverse tarsal mobility
lgus in a 1.5-year-old boy.

s e31
Ft
ltmov
qaa
sflutmhTT
rp3
Results of surgical treatment of congenital convex pes valgu
is obtained. Lengthening the extensors was only deemednecessary in five cases.
Internal release reduces the talonavicular dislocation. Toexpose and reduce this dislocation, the superficial tibialisposterior tendon is identified and is disinserted from themedial and plantar side of the navicular bone by taking awide aponeurosis band to lengthen it. Then the talonavicu-lar joint is opened at its dorsal and medial side and thetalonavicular—first metatarsal reducibility and alignmentare checked.
Posterior release consists in lengthening the Achilles ten-don, excising the posterior aponeurosis of the leg, andcapsulotomy of the tibiotalar joint.
Next, lateral release is carried out, with the surgeonon the lateral side of the foot and the first assistant onthe opposite side. The incision is horizontal along the sub-malleolar lateral side. The fibularis longus and brevis areidentified before they are lengthened. We lengthened bothfibular tendons in seven cases and the fibularis brevis alonein three cases. Then the calcaneocuboid joint is identifiedand either dorsal and lateral capsular ligaments are releasedor a vertical osteotomy in the frontal plane of the calcaneum5 mm from the joint space, preserving a plantar hinge. Inthis series, capsuloligamentous release of the calcaneocu-boid joint was performed in three cases, whereas osteotomyof the calcaneum was done in seven cases.
The third stage is maintaining the reduction. A 1.8- or2-mm pin is pushed in from back to front following thelong axis of the talus. With one hand, the talus is broughtin dorsal flexion using the pin; with the other hand, thefoot is lowered in plantar flexion and adduction so as tobring the talonavicular joint surfaces into contact. The ver-ticality of the talus is reduced and pinning the navicular —first metatarsal is continued. If the alignment is satisfactory,the calcaneocuboid joint or the calcaneum osteotomy opensspontaneously on top and toward the outside. The osteo-tomy can be filled with a bone fragment harvested fromthe navicular, which extends laterally. The lateral arch ofthe foot is fixed using a pin from front to back through the
fifth metatarsal-cuboid-calcaneum. After the reduction ismaintained, the inferior dislocation chamber of the talus isuncovered with excess capsule (Fig. 2). Frontal and lateralX-rays verify the reduction.Figure 2 Operative view, showing inferior capsule distensionafter reduction of the talonavicular dislocation.
ugwpgynsltr1
R
Ts
(vp
igure 3 Convex insole prescribed after surgical correctiono prevent midfoot collapse.
At the end of the intervention, the extensor and the tibia-is anterior tendons are sutured, then a capsulorraphy of thealus dislocation chamber is done, and the procedure is ter-inated by suturing the tibialis posterior to the inferior side
f the capsule as a reinforcement to prevent recurrence ofertical talus.
The skin is closed on both approaches after the tourni-uet is released and hemostasis is established. Closing waslways possible and complete because of the excess skinfter release.
The foot is immobilized after surgery using a long legplint with the knee flexed and the foot in slight plantarexion. This splint is replaced with a circular long leg castsing general anesthesia after 1 week. The cast is made byhe same surgeon with the knee bent at 90◦ and the footolded with the forefoot lowered, valgus correction of the
indfoot, and a depression in the medial edge of the foot.his cast is replaced by a second one toward the 60th day.he pins are removed when the cast is changed.
The child is then cared for by a physical therapist forehabilitation and fitting night splints, concave insoles torevent the midfoot from collapsing (Fig. 3) and shoes for—4 years.
All the children were seen at the time of the study andnderwent a clinical examination with photographs, radio-raphic exams with a frontal dorsoplantar view of the footith load, a lateral view with load, and lateral views inlantar flexion and dorsal flexion. The results of the sur-ical treatment were analyzed with a mean follow-up of sixears (range, 5—8 years). We used the radiological and cli-ical Kodros and Dias score [4] to evaluate the results. Thiscore comprises 17 criteria: 11 clinical criteria and six radio-ogical criteria (Table 2). The result is obtained by addinghe points assigned for each criterion. The result is conside-ed excellent if the score is over 17, good at 14—16, fair at1—13, and poor if it is less than 11.
esults
here was no postoperative skin necrosis. A single case ofuperficial infection at the pins was noted.
The morphology of the foot was improved in all casesFig. 1A—C). We observed no cases of overcorrection. Howe-er, the surgical correction was deemed insufficient onostoperative x-ray in both feet of a girl who had arthro-

e32 K. Ayadi et al.
Table 2 Clinical criteria of the Kodros and Dias classifica-tion [4].
Clinical criteria Score: 1 Score: 0
Esthetic aspect ofthe foot
Acceptable Poor
Dorsal flexion ofthe foot
> 0◦ < 0◦
Plantar flexion ofthe foot
> 20◦ < 20◦
Mobility of thesubtalar bone
1 or 1/2 0
Abnormal boneprotrusion
Absent Present
Skin problems Absent PresentAspect of the
mediallongitudinalarch
Rectilinear Presence of break
Alignment of thehindfoot
Aligned Exaggerated valgus
Alignment of theforefoot
Aligned Nonaligned
gfaowsa
nits
tAgeipmphrccd
tootc
r
and functional results obtained at follow-up were identicalto those obtained at cast removal.
Overall, the results were judged to be good in five casesand fair in five cases based on the Kodros and Dias score(Tables 2 and 3).
Discussion
Several surgical techniques for treating congenital verticaltalus have been reported in the literature. The techniqueswith bone resection — talectomy [5] and naviculectomy[6—8] — are no longer done in first-line treatment today.The different techniques used currently can be divided intothree types:
• peritalar release [5], release and fixation of the subtalarand talonavicular joints using an anterolateral approach,followed a few weeks later by posterior release. This tech-nique exposes the patient to a high risk of talar necrosisand is consequently used less and less;
• dorsal release of the transverse tarsal joint [7,9—12],which uses an oblique-transversal dorsal approach. Thistechnique provides complete release of the dorsal retrac-tions but without inferior talonavicular capsulorraphy. Itis sometimes associated with simple posterior release;
• posterior, medial, and lateral releases: these techniquesuse different approaches;◦ three mini-approaches [13]: this technique consists of
a posterior approach to lengthen the Achilles tendonand release of the tibiotalar and subtalar joints. Then amedial approach reduces the talonavicular joint, shor-tening the tibialis posterior and transferring the tibialisanterior to the talus neck. Finally, a third, lateral,approach, makes it possible to lengthen the fibularisbrevis and longus tendons, the common extensor of thetoes, and the third fibularis tendon,
◦ two approaches: a posteromedial approach and a late-ral approach [14,15], with a technique similar to thatused in our series,
◦ a single approach: the transversal U-shaped Cincinnatiapproach [4] and [16]. This approach allows the surgeonto lengthen the Achilles tendon, release the tibiotalarand subtalar joints, lengthen the tibialis anterior andposterior tendons, then release the medial and dorsaltalonavicular capsule as well as the medial and late-ral subtalar capsule. The calcaneocuboid joint is notreleased systematically, nor is lengthening the fibulartendons systematic.
Table 3 Radiological criteria of the Kodros and Dias clas-sification [4].
Radiological criteria Score: 1 Score: 0
Front talocalcaneal angle Normal AbnormalFront talus—M1 angle Normal AbnormalLateral talocalcaneal angle Normal Abnormal
Special shoes No YesPain No Yes
ryposis (observation 4, Table 1). This aspect persisted atollow-up with satisfactory morphology of the feet. This wasctually a severe case of arthrogryposis in a girl operatedn at the age of 17 months. Progression was marked byorsening of the orthopedic deformities (hip dislocations,
tiffness in the upper limbs) and the neurological condition,nd the child had never walked.
A clinical aspect of residual valgus of the hindfoot, witho insufficient reduction showing up on the X-ray, was foundn three cases (two cases of arthrogryposis and one of dias-ematomyelia). This aspect was probably secondary to theoft tissue anomalies that go along with this deformity.
In addition to the improved morphology of the feet, func-ion was improved compared to the preoperative condition.ll the children were able to wear normal shoes after sur-ical correction. No troublesome residual pain was noted,ven at the last follow-up. A single patient described painn both feet after prolonged walking and another one com-lained of morning stiffness in the foot. The reduction inobility involved most particularly the tibiotalar joint, withersistence of equinus in the hindfoot in one child whoas arthrogryposis; however, the transverse tarsal joint hasemained mobile. Triceps insufficiency was observed in twohildren (two feet) who could not walk on their tiptoes. Aertain stiffness in the ankle probably explains why the footid not become pes calcaneus.
At follow-up, partial necrosis of the talus occurred inwo cases, with the only consequence being a deformityf the talar dome (Fig. 1D). Necrosis of the navicular wasbserved in three cases. It was partial in two cases and
otal in one case, but with no functional repercussions in allases.No surgical revision was deemed necessary and no recur-ence of the deformity occurred at follow-up. The anatomic
Lateral talus—M1 angle Normal AbnormalEquinus of the hindfoot Absent PresentTalonavicular subluxation No Yes

s
aewagsrtpcowioo
C
To5dogs
R
[
Results of surgical treatment of congenital convex pes valgu
The diversity of these techniques shows how difficult it isto treat congenital vertical talus surgically. All these tech-niques attempt to find a compromise between extensivereleases with the risk of necrosis of the talus or the navicularbone and economic releases with the risk of undercorrec-tion. We have listed what we believe to be the most highlyrecommended procedures: dorsal and medial release of thetalonavicular joint, posterior release of the tibiotalar joint,and dorsal and lateral release of the calcaneocuboid joint.Tendon lengthening depends on their retraction.
As for the release techniques, different procedures havebeen described to maintain the reduction. Most authors usea pin to maintain the talonavicular alignment [12,13,17].Like Seringe et al. [14], we use a second pin that maintainsthe calcaneocuboid alignment. Kodros and Dias [4] also usea second pin inserted through the sole of the foot throughthe calcaneum and the talus to maintain the subtalar joint.
Tendon transfer is also an active means to maintain thecorrection. Rombouts et al. [9], Duncan and Fixsen [13] prac-tice a tibialis anterior tendon transfer on the neck of thetalus. Aroojis et al. [17] transfer half of the tibialis ante-rior tendon. Osmond-Clarke [18] transfer the fibularis brevisto the neck of the talus. Mazzocca et al. [12] reserve thistransfer for children with a neuromuscular disease or myelo-meningoceles. Aroojis et al. [17] advise against these tendontransfers in cases of arthrogryposis. We did not use thesetendon transfer techniques, but we reinserted the tibialisposterior on the inferior side of the talonavicular capsuleafter having done a capsulorraphy of the dislocation cham-ber in this area.
In certain cases, Grice-type arthrodesis can be proposedat the same time or later to correct the foot’s valgus. Thisarthrodesis is particularly recommended in children whohave been operated on after three years of age or thosefor whom surgery was indicated after failure of orthopedictreatment [19]. Oppenheim et al. [20] obtained the bestresults in cases where they did a subtalar Grice arthrodesis.
The evaluation of vertical talus treatment is oftenrelatively subjective and the series are often small andheterogeneous: this makes comparison of the results ran-dom. Different scores have been proposed in the literature[6,10,21]. Mazzocca et al. [12] conducted a comparativestudy between 25 feet treated with posteromedial releaseand eight feet treated with dorsal release. They showed thatthe two techniques can satisfactorily reduce the differentanomalies of vertical talus feet, but release through thedorsal approach requires less time, provides better clinicalscores, and fewer complications appear after a three-yearfollow-up. They found no skin problems with this technique.Dodge et al. [19] state that no surgical technique givessignificantly better results than another. Independently ofthe surgical technique, Florensa et al. [22] consider thatcorrection of the idiopathic forms provides better results.However, when there is arthrogryposis or dysraphism, theresults are not as good and surgical indications must be dis-cussed with great caution. In these cases, our series showsthat surgical treatment improves the morphology of the foot
in all cases, but not necessarily function. Abstention fromsurgery is a legitimate response in children who cannot walkand in cases of flexible vertical talus.The complications observed after surgical correctionwere few in number. Some, such as a reduction in mobility
[
e33
nd undercorrection, were for the most part related to thetiology, particularly arthrogryposis. Triceps insufficiencyas frequent and should be sought after surgical treatment,s Seringe [1] emphasizes. It could give the impression of aood morphological correction of the foot. Avascular necro-is of the talus, very frequent in peritalar release, is mucharer in the technique that we use [1]. We only observedwo cases of talar dome deformity, probably secondary toartial necrosis of the talus. All the cases of talus and navi-ular deformity had no functional repercussions. Recurrencef the deformity, a possible complication after surgery [1],as not observed in our series because of the systematic
nferior talonavicular capsulorraphy, the prolonged periodf postoperative immobilization, and the systematic use ofrthotics.
onclusion
here is not a choice operative technique in the treatmentf congenital vertical talus. The technique used provided0% good results. Whatever the technique, it is recommen-ed to avoid overly extensive releases to reduce the riskf talar and navicular necrosis, to check reduction radiolo-ically during the operation, and to prescribe orthotics foreveral months to prevent recurrence.
eferences
[1] Seringe R., Le pied convexe congénital. Cahiersd’enseignement de la Sofcot no 70, Expansion ScientifiqueFrancaise, Paris (1999) p. 223—34.
[2] Specht EE. Congenital paralytic vertical talus. J Bone Joint Surg1975;57-A:842—7. View Record in Scopus | Cited By in Scopus(7).
[3] Lloyd-Roberts GC, Spence AJ. Congenital vertical talus. J BoneJoint Surg 1958;40B:33—41.
[4] Kodros SA, Dias LS. Single stage surgical correction of conge-nital vertical talus. J Pediatr Orthop 1999;19:42—8. Full Textvia CrossRef | View Record in Scopus | Cited By in Scopus(14).
[5] Rigault P, Badelon O, Pouliquen J.C. Le pied convexe congé-nital. Cahiers d’enseignement de la Sofcot no 23, ExpansionScientifique Francaise, Paris (1985) p. 23—43.
[6] Clark MW, D’Ambrosia RD, Ferguson AB. Congenital verticaltalus. Treatment by open reduction and navicular excision. JBone Joint Surg 1977;59-A:816—24. View Record in Scopus |Cited By in Scopus (12).
[7] Fitton JM, Nevelos AB. The treatment of congenital verticaltalus. J Bone Joint Surg Br 1979;61:481—3. View Record inScopus | Cited By in Scopus (7).
[8] Eyre-Brook A. Congenital vertical talus. J Bone Joint Surg1967;49-B:618—27. View Record in Scopus | Cited By in Scopus(13).
[9] Rombouts JJ, Durnez A, Locquet J, Vincent A. Le pied convexecongénital ; étude d’une série de 52 cas. Acta Orthop Belg1988;54:282—90. View Record in Scopus | Cited By in Scopus(2).
10] Seimon LP. Surgical correction of congenital vertical talus
under the age of 2 years. J Pediatr Orthop 1987;7:405—11. ViewRecord in Scopus | Cited By in Scopus (17).11] Stricker SJ, Rosen E. Early one-stage reconstruction of congeni-tal vertical talus. Foot Ankle Int 1997;18:535—43. View Recordin Scopus | Cited By in Scopus (11).

e
[
[
[
[
[
[
[
[
[
[21] Jacobsen ST, Crawford AH. Congenital vertical talus. J PediatrOrthop 1983;3:306—10. View Record in Scopus | Cited By in
34
12] Mazzocca AD, Thomson JD, Deluca PA, Romness MJ. Compa-rison of the posterior approach versus the dorsal approach inthe treatment of congenital vertical talus. J Pediatr Orthop2001;21:212—7. Full Text via CrossRef | View Record in Scopus| Cited By in Scopus (7).
13] Duncan RDD, Fixsen JA. Congenital convex pes valgus.J Bone Joint Surg Br 1999;81-B:250—4. Full Text viaCrossRef | View Record in Scopus | Cited By in Scopus(15).
14] Seringe R, Martin G, Katti E, Vaquier J. Le pied convexecongénital étude anatomique et déductions pratiques. Rev ChirOrthop 1990;76:234—44. View Record in Scopus | Cited By inScopus (3).
15] Daumas L, Filippe G, Carlioz H. Le pied convexe congenital.Technique et résultats de la correction opératoire en un seul
temps. Rev Chir Orthop 1995;81:527—37. View Record in Scopus| Cited By in Scopus (2).16] Drennan JC. Congenital vertical talus. J Bone Joint Surg1995;77-A:1916—23. View Record in Scopus | Cited By in Scopus(7).
[
K. Ayadi et al.
17] Aroojis AJ, King MM, Donohoe M, Riddle Ec, Kumar SJ. Conge-nital vertical talus in arthrogryposis and other contracturalsyndromes. Clin Orthop 2005;434:26—32. Full Text via CrossRef| View Record in Scopus | Cited By in Scopus (0).
18] Osmond-Clarke H. Congenital vertical talus. J Bone Joint Surg1956;38B:334—41.
19] Dodge LD, Kirklin Ashley R, Gilbert RJ. Treatment of the conge-nital vertical talus: a retrospective review of 36 feet withlong-term follow-up. Foot Ankle 1987;7:326—32. View Recordin Scopus | Cited By in Scopus (18).
20] Oppenheim W, Smith C, Christie W. Congenital vertical talus.Foot Ankle 1985;5:198—204. View Record in Scopus | Cited Byin Scopus (8).
Scopus (19).22] Florensa G, Dimeglio A, Mercier M, Dimeglio E. Le pied convexe
congénital. Ann Readapt Med Phys 1991;34.