Embed Size (px)
Citation preview

Hindawi Publishing CorporationBioMed Research InternationalVolume 2013 Article ID 158621 7 pageshttpdxdoiorg1011552013158621
Research ArticleVentricular Dyssynchrony and Function Improve followingCatheter Ablation of Nonseptal Accessory Pathways in Children
Sylvia Abadir12 Anne Fournier1 Marc Dubuc2 Georgia Sarquella-Brugada1
Patrick Garceau2 and Paul Khairy12
1 Department of Pediatric Cardiology Sainte-Justine Hospital Universite de Montreal Montreal QC Canada H3T 1C52Department of Cardiology Montreal Heart Institute Universite de Montreal Montreal QC Canada H1T 1C8
Correspondence should be addressed to Paul Khairy paulkhairyumontrealca
Received 8 April 2013 Accepted 9 June 2013
Academic Editor Stamatios Lerakis
Copyright copy 2013 Sylvia Abadir et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Introduction Paradoxical or hypokinetic interventricular septal motion has been described in patients with septal or paraseptalaccessory pathways Data regarding nonseptal pathways is limitedMethods andResultsWe quantified left ventricular dyssynchronyand function in 16 consecutive children 142 plusmn 37 years weighing 53 plusmn 17 kg prior to and following catheter ablation ofbidirectional septal (119873 = 6) and nonseptal (119873 = 10) accessory pathways Following ablation the left ventricular ejection fractionincreased by 49 plusmn 21 (119875 = 0038) from a baseline value of 570 plusmn 78 By tissue Doppler imaging the interval betweenQRS onset and peak systolic velocity (Ts) decreased from a median of 330ms to 180ms (119875 = 0013) The left ventricular ejectionfraction increased to a greater extent following catheter ablation of nonseptal (59 plusmn 26 119875 = 0023) versus septal (25 plusmn 41119875 = 0461) pathways The four patients with an ejection fraction lt50 two of whom had left lateral pathways improved to gt50after ablation Similarly the improvement in dyssynchrony was more marked in patients with nonseptal versus septal pathways(difference between septal and lateral wall motion delay before and after ablation 206 plusmn 71ms (119875 = 0015) versus 14 plusmn 114ms(119875 = 0655)) Conclusion Left ventricular systolic function and dyssynchrony improve after ablation of antegrade-conductingaccessory pathways in children with more pronounced changes noted for nonseptal pathways
1 Introduction
Manifest atrioventricular accessory pathways in the so-called Wolff-Parkinson-White syndrome result in electricaland mechanical preexcitation of ventricular myocardiumat their site of insertion Earlier echocardiographic studiesdemonstrated that left posteroseptal accessory pathways areassociated with abnormal left ventricular posterior wallmotion [1ndash3] and that right anterior or right posteroseptalpathways produce abnormal interventricular septal motion[2 4ndash6] Since these studies predated the era of catheterablation localization of accessory pathways was based solelyon electrocardiographic criteria [7] More recent reportsunderscored the potential for right-sided and septal path-ways [8 9] to result in left ventricular dysfunction thatimproves following catheter ablation [10ndash12] However itis generally believed that left lateral accessory pathwaysproduce a lesser degree of ventricular dyssynchrony and
dysfunction by virtue of their location and relative distanceaway from the normal conduction system There is a paucityof data regarding potential deleterious effects of nonseptalpathways on inter- and intraventricular dyssynchrony Wetherefore sought to characterize and compare the degree ofleft ventricular dyssynchrony systolic and diastolic functionsby detailed echocardiographic analyses with tissue Dopplerimaging prior to and following catheter ablation of septal andnonseptal accessory pathways
2 Materials and Methods
21 Study Population We enrolled consecutive children (le18years of age) with a diagnosis of Wolff-Parkinson-Whitesyndrome (ie manifest ventricular preexcitation associatedwith palpitations) referred for catheter ablation at Sainte-Justine Hospital over a 2-year period We excluded patientswith a congenital heart defect (other than an isolated bicuspid
2 BioMed Research International
aortic valve) and those in whom transthoracic echocardio-grams could not be performed for logistical reasons priorto or following catheter ablation The protocol was approvedby the local institutional review board and written informedinformed consent was obtained from all patients
22 Electrocardiograms and Transthoracic Echocardiogra-phy Electrocardiograms were performed prior to and aftercatheter ablation in all patients PR intervals were mea-sured by computed analyses The accessory pathway loca-tion was initially classified by an established electrocardio-graphic algorithm in children [13] and subsequently refinedaccording to the site of successful catheter ablation Two-dimensional transthoracic echocardiography was performedusing standard parasternal long axis apical 4-chamberand subcostal views prior to and within 24 hours aftercatheter ablation Cardiac function valve regurgitation anddyssynchrony parameters were assessed For each parameterthree consecutive cardiac cycles were recorded and the threevalues averaged Two independent reviewers analyzed offlinetransthoracic echocardiographic data
Cardiac dyssynchrony was assessed by the followingcriteria (Figures 1 2 3 and 4)
(i) aortic preejection delay (APD) using M-mode andpulsed Doppler modes measured from the onset ofthe QRS complex to the beginning of aortic ejection(abnormal if ge140ms) [14]
(ii) interventricular mechanical delay (IVMD) using thepulsed Doppler mode defined as the differencebetween aortic and pulmonary preejection delay(abnormal if ge40ms) [14]
(iii) septal-to-posterior wall motion delay (SPWMD)using M-mode imaging (abnormal if ge130ms) [15]
(iv) delay between time to peak systolic velocity at basalseptal and basal lateral segments using tissue Dopplerimaging (abnormal if ge60ms) [16] This measurewas first performed using pulsed tissue Doppler andthen confirmed using color-coded tissue Doppler andtime-velocity curves (from left ventricular septal andlateral wall sample points selected in an apical long-axis view)
The left ventricular ejection fraction was quantified usingthe Simpson method [17] in the apical view and consideredabnormal if le55 Aortic and mitral valve regurgitation wasassessed semiquantitatively by 2D color Doppler imagingand classified as discrete mild moderate or severe [18]Diastolic parameters were assessed using the pulsed Dopplermode tissue Doppler imaging (E wave velocity E wavedeceleration time (EDT) and the EE1015840 ratio at basal septaland basal lateral left ventricular segments) Diastolic functionwas considered abnormal if the EDT was lt150 or gt220msand if EE1015840 gt 15 [19ndash21] Complications such as pericardialeffusion and increased valvular insufficiency were assessed bythe postprocedural transthoracic echocardiogram
23 Catheter Ablation Procedure All catheter ablation pro-cedures were performed under general anaesthesia Threequadripolar catheters were advanced to the high right atriumHis position and right ventricular apex A decapolar catheterwas placed in the coronary sinus An initial electrophysi-ological study was performed to assess baseline intervalsatrial atrioventricular nodal accessory pathway ventricu-lar refractory periods Wenckebach physiology retrogradeconduction and inducible supraventricular tachycardia Theatrial insertion of the accessory pathway was identified asthe earliest atrial signal during retrograde accessory pathwayconduction The ventricular insertion was assessed duringmaximum preexcitation as the site of earliest ventriculardepolarization Accessory pathways were ablated using tran-scatheter cryoenergy for septal and radiofrequency energyfor lateral pathways (left or right) Coexisting arrhythmiassuch as atrioventricular nodal reentrant tachycardia wereablated during the same intervention Catheter ablation wasconsidered successful if after 30 minutes of observationthere was no evidence of antegrade or retrograde conductionacross an accessory pathway and no inducible supraventric-ular tachycardia with and without an isoproterenol infusion(002 120583gkgmin) Barring any complication patients weredischarged the following day
24 Statistical Analysis Continuous variables are summa-rized bymean plusmn standard deviation ormedian and interquar-tile range (IQR 25th 75th percentiles) depending on normal-ity of distribution Categorical variables are represented byfrequencies and percentages Intrapatient comparisons priorto and following ablation were assessed by paired Studentrsquost-tests or Wilcoxon signed-rank tests Two-tailed 119875 valueslt005 were considered statistically significant Analyses wereperformed with SAS software Version 92 (SAS InstituteCary NC USA)
3 Results
31 Patient and Procedural Characteristics Overall 16 chil-dren (5 females) age 142 plusmn 37 years weight 53 plusmn 17 kgwere systematically assessed All hadWolff-Parkinson-Whitesyndrome structurally normal hearts and evidence of sus-tained supraventricular tachycardia by Holter monitoring orexternal event loop recorders Patient and procedural char-acteristics are summarized in Table 1 Septal or paraseptalpathways were present in 6 (375) patients and nonseptalpathways in 10 (625) The nonseptal pathways consistedof left lateral (119873 = 5) right lateralanterolateral (119873 = 3) andleft posterior (119873 = 2) connections All patients underwentsuccessful catheter ablation Cryoenergy was employed in 4patients and radiofrequency energy in 12
32 Echocardiographic Parameters Prior to ablation nodifferences in left ventricular ejection fraction or indicesof left ventricular dyssynchrony were observed in patientswith septal versus nonseptal accessory pathways Table 2and Figure 5 summarize the echocardiographic parametersprior to and following catheter ablation Prior to ablation
BioMed Research International 3
(a) (b)
Figure 1 Determination of interventricular mechanical delay (IVMD) using pulsed Doppler mode corresponding to the difference betweenaortic (a) and pulmonary (b) preejection delay No significant delay in left ventricular contraction is observed
Table 1 Baseline and procedural characteristics
Patient Age at ablation(years) Weight (kg) Body surface
area (m2) Energy source Location of AP Delta-HVinterval (ms)
FU after ablation(months)
1 167 587 18 RF LL 77 2772 194 730 19 RF RPS 53 2083 150 586 17 RF RPS 40 2084 189 620 17 RF RPS 10 2155 149 560 16 RF RPL 45 2646 137 540 16 RF LPS 18 047 165 770 19 RF LP 81 398 130 390 13 Cryo RA 23 409 141 710 18 RF LL 21 4010 97 300 11 RF LL 17 4111 76 230 09 Cryo RAS NA 4212 68 220 09 Cryo RA 40 5913 171 600 17 RF LL 24 6514 164 700 18 RF RL 39 9315 153 580 16 RF LL 19 15116 118 400 13 Cryo RPS 44 185Summary 142 plusmn 37 533 plusmn 175 15 plusmn 03 RF 12 Cryo 6 6 septal 10 nonseptal 367 plusmn 214 121 plusmn 92AP denotes accessory pathway FU followup RF radiofrequency Cryo cryoenergy LL left lateral RPS right posteroseptal RPL right posterolateral LPSleft posteroseptal LP left posterior RAS right anteroseptal RAL right anterolateral RA right anterior RL right lateral NA not available
6 patients had a left ventricular ejection fraction lt55 and4 lt50 Following ablation the ejection fraction increasedby 49 plusmn 21 (119875 = 0038) from a baseline value of 570 plusmn78This was accompanied by a significant reduction in thedifference between aortic and pulmonary preejection times(110 plusmn 33ms 119875 = 0017) The left ventricular ejectionfraction increased to a greater extent following ablation ofnonseptal (59 plusmn 26 119875 = 0023) versus septal (25 plusmn 41119875 = 0461) pathways The 4 patients with a left ventricularejection fraction lt50 prior to ablation 2 of whom had leftlateral pathways improved to gt50 after ablation By tissueDoppler imaging the time to peak systolic velocity decreasedfrom 330ms (IQR 200 480) to 180ms (IQR 50 240)119875 = 0013 No significant change in septal-to-posterior wallmotion delay or diastolic parameters was noted
Similar to changes in left ventricular ejection fraction themagnitude of improvement in left ventricular dyssynchronywas more marked in patients with nonseptal versus septalpathways The difference between septal and lateral wallmotion delay before and after ablation was 206 plusmn 71ms(119875 = 0015) versus 14 plusmn 114ms (119875 = 0655) for nonseptalversus septal pathways respectively
4 Discussion
A possible pathophysiological link between accessory path-ways and ventricular dysfunction has been proposed inthe absence of tachycardia-induced cardiomyopathy [9 1222] Most prior reports investigating this association havefocused on septal pathways [9ndash12] In our study whichincorporated detailed echocardiographic assessment prior
4 BioMed Research International
Table 2 Echocardiographic parameters prior to and following catheter ablation
Patient Location of AP LV ejection fraction () SPWMD (ms) ESD septal (ms) ESD lateral (ms) Delta ESD septal-lateral (ms)PRE POST PRE POST PRE POST PRE POST PRE POST
1 LL 48 58 101 100 256 143 240 120 16 232 RPS 72 68 47 64 164 147 147 120 17 273 RPS 55 NA 58 40 NA NA NA NA NA NA4 RPS 61 57 30 33 211 154 NA NA NA NA5 RPL 50 76 53 47 200 110 167 110 33 06 LPS 60 63 50 87 157 112 122 92 35 207 LP 61 61 5 64 175 135 146 117 29 188 RA 48 53 31 40 184 188 280 271 96 839 LL 62 59 33 63 125 124 112 122 13 210 LL 65 68 44 61 162 180 96 175 66 511 RAS 49 62 76 78 293 195 183 NA 110 NA12 RA 52 55 99 10 192 170 133 155 59 1513 LL 68 77 15 115 140 127 110 103 30 2414 RL 55 62 80 61 155 NA 280 NA 125 NA15 LL 49 50 100 72 133 108 110 96 23 1216 RPS NA 62 77 75 NA NA NA NA NA NAMean plusmn SD mdash 57 plusmn 8 62 plusmn 8 56 plusmn 30 63 plusmn 26 182 plusmn 47 145 plusmn 30 164 plusmn 64 135 plusmn 52 50 plusmn 38 21 plusmn 23LVdenotes left ventricle SPWMD septal-to-posterior wallmotion delay ESD electrosystolic delay (or time-to-peak systolic velocity) PRE preablation POSTpostablation LL left lateral RPS right posteroseptal RPL right posterolateral LPS left posteroseptal LP left posterior RAS right anteroseptal RAL rightanterolateral RA right anterior RL right lateral NA not available
Figure 2 Assessment of septal-to-posterior wall motion delay(SPWMD) using M-mode imaging Normal SPWMD (lt130ms) isdemonstrated
to and following catheter ablation of accessory pathwaysthe following salient features were noted (1) left ventriculardyssynchrony and dysfunction were observed in patientswith septal and nonseptal pathways (2) dyssynchrony anddysfunction were reversible following successful ablation ofthe accessory pathway (3) improvements were more markedin patients with nonseptal pathways and (4) left ventriculardiastolic function parameters prior to ablation (ie meanlateral and septal EE1015840 values of 56 and 71 resp) werecomparable to a cohort of 325 healthy children [23] andunchanged following ablation
Tomaske et al retrospectively reported a series of 34children (mean age 142 years) with Wolff-Parkinson-Whitesyndrome who underwent successful radiofrequency abla-tion of right septal or posteroseptal accessory pathways
[12] Prior to ablation 56 of patients had a left ventric-ular ejection fraction lt55 It improved significantly aftercatheter ablation from a mean of 50 to 56 Classicdyssynchrony parameters were studied Whereas SPWMDdecreased significantly after ablation no change in IVMDwasobserved Five patients underwent two-dimensional strainanalysis which showed a reduction in the difference betweenthe earliest and latest negative strain after ablation Our studyextends these findings to include an analysis of tissueDopplerimaging to children with manifest ventricular preexcitationregardless of its location
In another series of 63 children with Wolff-Parkinson-White syndrome (mean age at diagnosis 59 years) leftventricular dysfunctionwas reported only in associationwithseptal accessory pathways [11] The mean left ventricularejection fraction was 53 in patients with septal accessorypathways (119873 = 15) compared to 62 for all other locationsMoreover septal dyskinesia was identified in 6 patients withright septal accessory pathways and was the only factorsignificantly associated with a reduction in left ventricularejection fraction After ablation the left ventricular ejectionfraction significantly improved in these 6 patients from 42 plusmn5 to 55plusmn7 TissueDoppler imagingwas not systematicallyperformed
The relationship between dyskinetic segments and leftventricular dysfunction is also supported by the pacemakerliterature which suggests that right ventricular apical pacingmay have a detrimental effect on left ventricular function[24ndash26] Restoration of cardiac synchrony by cardiac resyn-chronization therapy is a well-established intervention thatimproves all-cause mortality [27 28] Animal experiments
BioMed Research International 5
(a) (b)
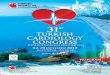
Figure 3 Determination of the delay between time-to-peak systolic velocity at basal septal (a) and basal lateral (b) segments using tissueDoppler imaging A significant delay is demonstrated in this patient (no 10)
Figure 4 Determination of time-velocity curves using color-codedtissue Doppler and Q-analyses (from left ventricular septal andlateral wall sample points selected in an apical long-axis view) Inthis example (patient no 6) no significant delay is demonstratedbetween septal and lateral left ventricular walls following catheterablation
have shown that asynchronous electrical activation inducedby ventricular pacing results in asymmetrical hypertro-phy and ventricular dilation due to regional differences inworkload [29] A pathophysiological link between nonseptalaccessory pathways and ventricular dyssynchrony is sup-ported by such preclinical experiments which demonstratedthat early activation of the left ventricular free wall inpaced dogs resulted in significant thinning of left ventricularmyocardium and thickening of the late-activated septumDyskinetic segments may function much like aneurysmsand induce adverse remodelling with progressive dilatation[9 10] Hemodynamic changes with altered blood flowpatterns may ensue producing endomyocardial fibroelasticthickening [10]
It may therefore be hypothesized that ventricular preex-citation can result in remodelling changes similar to ventric-ular pacing with segmental dyskinesia leading to thinningdyssynchrony ventricular dilation and ultimately ventricu-lar dysfunction Such a patternmay be produced fromany siteof ventricular activation remote from the normal conductionsystem Our results are consistent with the hypothesis thatdyssynchrony induced by nonseptal pathways may be asdeleterious and sometimes more so than septal pathways
020406080
100120140160180200
LVEF ()
After ablationBefore ablation
SPWMD(ms)
ESD septal(ms)
ESD lateral(ms)
Delta ESD septal-lateral
(ms)
Figure 5 Echocardiographic parameters prior to and followingcatheter ablation LVEF denotes left ventricular ejection fractionSPWMD septal-to-posteriorwallmotion delay ESD electrosystolicdelay (or time-to-peak systolic velocity)
Further studies are required to confirm these findings andto assess the relevance of targeting accessory pathways basedsolely on hemodynamic effects of preexcitation [30]
Limitations As is often the case with pediatric case seriesthe study was limited by the small number of patientsNevertheless to minimize selection bias all consecutivechildren referred for catheter ablation of Wolff-Parkinson-White syndrome were enrolled over a 2-year period Indetermining dyssynchrony echocardiographic assessmentwas limited to basal septal and lateral segments by means oftissue Doppler imaging The comparative value of samplingadditional segments or the use of potentially complementaryimaging techniques such as strain and strain rate could notbe assessed
5 Conclusion
In a series of pediatric patients with Wolff-Parkinson-White syndrome and absence of structural heart diseaseleft ventricular systolic function and dyssynchrony improved
6 BioMed Research International
after successful ablation of antegrade-conducting accessorypathways The more pronounced changes were observed inpatients with nonseptal pathways
Conflict of Interests
The authors do not have any conflict of interests with thecontent of the paper
References
[1] KHina TMurakami S Kusachi et al ldquoDecreased amplitude ofleft ventricular posterior wall motion with notch movement todetermine the left posterior septal accessory pathway in Wolff-Parkinson-White syndromerdquo Heart vol 82 no 6 pp 731ndash7391999
[2] H Hishida I Sotobata and Y Koike ldquoEchocardiographic pat-terns of ventricular contraction in the Wolff-Parkinson-Whitesyndromerdquo Circulation vol 54 no 4 pp 567ndash570 1976
[3] A N DeMaria Z Vera A Neumann and D TMason ldquoAltera-tions in ventricular contraction pattern in theWolff-Parkinson-White syndrome Detection by echocardiographyrdquo Circulationvol 53 no 2 pp 249ndash257 1976
[4] A R Ticzon A N Damato A R Caracta G Russo J R Fosterand S H Lau ldquoInterventricular septal motion during preexci-tation and normal conduction in Wolff-Parkinson-White syn-drome Echocardiographic and electrophysiologic correlationrdquoThe American Journal of Cardiology vol 37 no 6 pp 840ndash8471976
[5] G S Francis PTheroux R AOrsquoRourke ADHagan andADJohnson ldquoAn echocardiographic study of interventricular septalmotion in the Wolff-Parkinson-White syndromerdquo Circulationvol 54 no 2 pp 174ndash178 1976
[6] L Sasse and H A del Puerto ldquoEchocardiography of ventric-ular septal movement in Wolff-Parkinson-White syndromerdquoArchivos del Instituto de Cardiologia de Mexico vol 46 no 4pp 445ndash450 1976
[7] J P Boineau J F Moore and W C Sealy ldquoBasis of clinicalECG variations in right and left ventricular pre-excitation Aunitary concept of WPWrdquo in Cardiac Arrhythmias The 25thHahnemann Symposium Grune and Stratton New York NYUSA 1973
[8] F E A U ten Cate M A Kruessell K Wagner et al ldquoDilatedcardiomyopathy in children with ventricular preexcitationthe location of the accessory pathway is predictive of thisassociationrdquo Journal of Electrocardiology vol 43 no 2 pp 146ndash154 2010
[9] G Fazio M Mongiovi L Sutera G Novo S Novo and SPipitone ldquoSegmental dyskinesia inWolff-Parkinson-White syn-drome a possible cause of dilatative cardiomyopathyrdquo Interna-tional Journal of Cardiology vol 123 no 2 pp e31ndashe34 2008
[10] J Cadrin-Tourigny A Fournier G Andelfinger and P KhairyldquoSevere left ventricular dysfunction in infants with ventricularpreexcitationrdquo Heart Rhythm vol 5 no 9 pp 1320ndash1322 2008
[11] B S Kwon E J Bae G B Kim C I Noh J Y Choi and YS Yun ldquoSeptal dyskinesia and global left ventricular dysfunc-tion in pediatric Wolff-Parkinson-White syndrome with septalaccessory pathwayrdquo Journal of Cardiovascular Electrophysiologyvol 21 no 3 pp 290ndash295 2010
[12] M Tomaske J Janousek V Razek et al ldquoAdverse effects ofWolff-Parkinson-White syndrome with right septal or pos-teroseptal accessory pathways on cardiac functionrdquo Europacevol 10 no 2 pp 181ndash189 2008
[13] L V A Boersma E Garcıa-Moran L Mont and J BrugadaldquoAccessory pathway localization by QRS polarity in childrenwith Wolff-Parkinson-White syndromerdquo Journal of Cardiovas-cular Electrophysiology vol 13 no 12 pp 1222ndash1226 2002
[14] S Cazeau P Bordachar G Jauvert et al ldquoEchocardiographicmodeling of cardiac dyssynchrony before and during multisitestimulation a prospective studyrdquo Pacing and Clinical Electro-physiology vol 26 no 1 pp 137ndash143 2003
[15] M V Pitzalis M Iacoviello R Romito G Luzzi M Anaclerioand C Forleo ldquoRole of septal to posterior wall motion delayin cardiac resynchronization therapyrdquo Journal of the AmericanCollege of Cardiology vol 48 no 3 pp 596ndash597 2006
[16] J J Bax T H Marwick S G Molhoek et al ldquoLeft ventriculardyssynchrony predicts benefit of cardiac resynchronizationtherapy in patients with end-stage heart failure before pace-maker implantationrdquo The American Journal of Cardiology vol92 no 10 pp 1238ndash1240 2003
[17] N B Schiller ldquoTwo-dimensional echocardiographic determi-nation of left ventricular volume systolic function and massSummary and discussion of the 1989 recommendations of theAmerican society of echocardiographyrdquo Circulation vol 84 no3 pp I280ndashI287 1991
[18] WA ZoghbiM Enriquez-Sarano E Foster et al ldquoRecommen-dations for evaluation of the severity of native valvular regur-gitation with two-dimensional and doppler echocardiographyrdquoJournal of the American Society of Echocardiography vol 16 no7 pp 777ndash802 2003
[19] E Abergel ldquoEchocardiographic indices of diastolic function putto the practical testrdquo Archives des Maladies du Coeur et desVaisseaux vol 98 no 4 pp 325ndash330 2005
[20] C J McMahon S F Nagueh R H Pignatelli et al ldquoCharac-terization of left ventricular diastolic function by tissue dopplerimaging and clinical status in children with hypertrophic car-diomyopathyrdquo Circulation vol 109 no 14 pp 1756ndash1762 2004
[21] P Rumeau P Acar S Paranon et al ldquoEvaluation of left ventric-ular diastolic function in children by doppler tissue imagingrdquoArchives des Maladies du Coeur et des Vaisseaux vol 100 no 5pp 405ndash410 2007
[22] M Emmel S Balaji andN Sreeram ldquoVentricular preexcitationassociated with dilated cardiomyopathy a causal relationshiprdquoCardiology in the Young vol 14 no 6 pp 594ndash599 2004
[23] B W Eidem C J McMahon R R Cohen et al ldquoImpactof cardiac growth on doppler tissue imaging velocities astudy in healthy childrenrdquo Journal of the American Society ofEchocardiography vol 17 no 3 pp 212ndash221 2004
[24] P P Karpawich ldquoChronic right ventricular pacing and cardiacperformance The pediatric perspectiverdquo Pacing and ClinicalElectrophysiology vol 27 no 6 pp 844ndash849 2004
[25] A S Manolis ldquoThe deleterious consequences of right ventricu-lar apical pacing time to seek alternate site pacingrdquo Pacing andClinical Electrophysiology vol 29 no 3 pp 298ndash315 2006
[26] M V T Tantengco R L Thomas and P P Karpawich ldquoLeftventricular dysfunction after long-term right ventricular apicalpacing in the youngrdquo Journal of the American College ofCardiology vol 37 no 8 pp 2093ndash2100 2001
BioMed Research International 7
[27] M R Bristow L A Saxon J Boehmer et al ldquoCardiac-resyn-chronization therapy with or without an implantable defibrilla-tor in advanced chronic heart failurerdquoTheNew England Journalof Medicine vol 350 no 21 pp 2140ndash2150 2004
[28] J G F Cleland J Daubert E Erdmann et al ldquoThe effect ofcardiac resynchronization on morbidity and mortality in heartfailurerdquo The New England Journal of Medicine vol 352 no 15pp 1539ndash1549 2005
[29] F W Prinzen E C Cheriex T Delhaas et al ldquoAsymmetricthickness of the left ventricular wall resulting from asyn-chronous electric activation a study in dogs with ventricularpacing and in patients with left bundle branch blockrdquo TheAmerican Heart Journal vol 130 no 5 pp 1045ndash1053 1995
[30] M I Cohen J K Triedman B C Cannon et al ldquoPACESHRSexpert consensus statement on the management of the asymp-tomatic young patient with a Wolff-Parkinson-White (WPWventricular preexcitation) electrocardiographic patternrdquo HeartRhythm vol 9 no 6 pp 1006ndash1024 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
aortic valve) and those in whom transthoracic echocardio-grams could not be performed for logistical reasons priorto or following catheter ablation The protocol was approvedby the local institutional review board and written informedinformed consent was obtained from all patients
22 Electrocardiograms and Transthoracic Echocardiogra-phy Electrocardiograms were performed prior to and aftercatheter ablation in all patients PR intervals were mea-sured by computed analyses The accessory pathway loca-tion was initially classified by an established electrocardio-graphic algorithm in children [13] and subsequently refinedaccording to the site of successful catheter ablation Two-dimensional transthoracic echocardiography was performedusing standard parasternal long axis apical 4-chamberand subcostal views prior to and within 24 hours aftercatheter ablation Cardiac function valve regurgitation anddyssynchrony parameters were assessed For each parameterthree consecutive cardiac cycles were recorded and the threevalues averaged Two independent reviewers analyzed offlinetransthoracic echocardiographic data
Cardiac dyssynchrony was assessed by the followingcriteria (Figures 1 2 3 and 4)
(i) aortic preejection delay (APD) using M-mode andpulsed Doppler modes measured from the onset ofthe QRS complex to the beginning of aortic ejection(abnormal if ge140ms) [14]
(ii) interventricular mechanical delay (IVMD) using thepulsed Doppler mode defined as the differencebetween aortic and pulmonary preejection delay(abnormal if ge40ms) [14]
(iii) septal-to-posterior wall motion delay (SPWMD)using M-mode imaging (abnormal if ge130ms) [15]
(iv) delay between time to peak systolic velocity at basalseptal and basal lateral segments using tissue Dopplerimaging (abnormal if ge60ms) [16] This measurewas first performed using pulsed tissue Doppler andthen confirmed using color-coded tissue Doppler andtime-velocity curves (from left ventricular septal andlateral wall sample points selected in an apical long-axis view)
The left ventricular ejection fraction was quantified usingthe Simpson method [17] in the apical view and consideredabnormal if le55 Aortic and mitral valve regurgitation wasassessed semiquantitatively by 2D color Doppler imagingand classified as discrete mild moderate or severe [18]Diastolic parameters were assessed using the pulsed Dopplermode tissue Doppler imaging (E wave velocity E wavedeceleration time (EDT) and the EE1015840 ratio at basal septaland basal lateral left ventricular segments) Diastolic functionwas considered abnormal if the EDT was lt150 or gt220msand if EE1015840 gt 15 [19ndash21] Complications such as pericardialeffusion and increased valvular insufficiency were assessed bythe postprocedural transthoracic echocardiogram
23 Catheter Ablation Procedure All catheter ablation pro-cedures were performed under general anaesthesia Threequadripolar catheters were advanced to the high right atriumHis position and right ventricular apex A decapolar catheterwas placed in the coronary sinus An initial electrophysi-ological study was performed to assess baseline intervalsatrial atrioventricular nodal accessory pathway ventricu-lar refractory periods Wenckebach physiology retrogradeconduction and inducible supraventricular tachycardia Theatrial insertion of the accessory pathway was identified asthe earliest atrial signal during retrograde accessory pathwayconduction The ventricular insertion was assessed duringmaximum preexcitation as the site of earliest ventriculardepolarization Accessory pathways were ablated using tran-scatheter cryoenergy for septal and radiofrequency energyfor lateral pathways (left or right) Coexisting arrhythmiassuch as atrioventricular nodal reentrant tachycardia wereablated during the same intervention Catheter ablation wasconsidered successful if after 30 minutes of observationthere was no evidence of antegrade or retrograde conductionacross an accessory pathway and no inducible supraventric-ular tachycardia with and without an isoproterenol infusion(002 120583gkgmin) Barring any complication patients weredischarged the following day
24 Statistical Analysis Continuous variables are summa-rized bymean plusmn standard deviation ormedian and interquar-tile range (IQR 25th 75th percentiles) depending on normal-ity of distribution Categorical variables are represented byfrequencies and percentages Intrapatient comparisons priorto and following ablation were assessed by paired Studentrsquost-tests or Wilcoxon signed-rank tests Two-tailed 119875 valueslt005 were considered statistically significant Analyses wereperformed with SAS software Version 92 (SAS InstituteCary NC USA)
3 Results
31 Patient and Procedural Characteristics Overall 16 chil-dren (5 females) age 142 plusmn 37 years weight 53 plusmn 17 kgwere systematically assessed All hadWolff-Parkinson-Whitesyndrome structurally normal hearts and evidence of sus-tained supraventricular tachycardia by Holter monitoring orexternal event loop recorders Patient and procedural char-acteristics are summarized in Table 1 Septal or paraseptalpathways were present in 6 (375) patients and nonseptalpathways in 10 (625) The nonseptal pathways consistedof left lateral (119873 = 5) right lateralanterolateral (119873 = 3) andleft posterior (119873 = 2) connections All patients underwentsuccessful catheter ablation Cryoenergy was employed in 4patients and radiofrequency energy in 12
32 Echocardiographic Parameters Prior to ablation nodifferences in left ventricular ejection fraction or indicesof left ventricular dyssynchrony were observed in patientswith septal versus nonseptal accessory pathways Table 2and Figure 5 summarize the echocardiographic parametersprior to and following catheter ablation Prior to ablation
BioMed Research International 3
(a) (b)
Figure 1 Determination of interventricular mechanical delay (IVMD) using pulsed Doppler mode corresponding to the difference betweenaortic (a) and pulmonary (b) preejection delay No significant delay in left ventricular contraction is observed
Table 1 Baseline and procedural characteristics
Patient Age at ablation(years) Weight (kg) Body surface
area (m2) Energy source Location of AP Delta-HVinterval (ms)
FU after ablation(months)
1 167 587 18 RF LL 77 2772 194 730 19 RF RPS 53 2083 150 586 17 RF RPS 40 2084 189 620 17 RF RPS 10 2155 149 560 16 RF RPL 45 2646 137 540 16 RF LPS 18 047 165 770 19 RF LP 81 398 130 390 13 Cryo RA 23 409 141 710 18 RF LL 21 4010 97 300 11 RF LL 17 4111 76 230 09 Cryo RAS NA 4212 68 220 09 Cryo RA 40 5913 171 600 17 RF LL 24 6514 164 700 18 RF RL 39 9315 153 580 16 RF LL 19 15116 118 400 13 Cryo RPS 44 185Summary 142 plusmn 37 533 plusmn 175 15 plusmn 03 RF 12 Cryo 6 6 septal 10 nonseptal 367 plusmn 214 121 plusmn 92AP denotes accessory pathway FU followup RF radiofrequency Cryo cryoenergy LL left lateral RPS right posteroseptal RPL right posterolateral LPSleft posteroseptal LP left posterior RAS right anteroseptal RAL right anterolateral RA right anterior RL right lateral NA not available
6 patients had a left ventricular ejection fraction lt55 and4 lt50 Following ablation the ejection fraction increasedby 49 plusmn 21 (119875 = 0038) from a baseline value of 570 plusmn78This was accompanied by a significant reduction in thedifference between aortic and pulmonary preejection times(110 plusmn 33ms 119875 = 0017) The left ventricular ejectionfraction increased to a greater extent following ablation ofnonseptal (59 plusmn 26 119875 = 0023) versus septal (25 plusmn 41119875 = 0461) pathways The 4 patients with a left ventricularejection fraction lt50 prior to ablation 2 of whom had leftlateral pathways improved to gt50 after ablation By tissueDoppler imaging the time to peak systolic velocity decreasedfrom 330ms (IQR 200 480) to 180ms (IQR 50 240)119875 = 0013 No significant change in septal-to-posterior wallmotion delay or diastolic parameters was noted
Similar to changes in left ventricular ejection fraction themagnitude of improvement in left ventricular dyssynchronywas more marked in patients with nonseptal versus septalpathways The difference between septal and lateral wallmotion delay before and after ablation was 206 plusmn 71ms(119875 = 0015) versus 14 plusmn 114ms (119875 = 0655) for nonseptalversus septal pathways respectively
4 Discussion
A possible pathophysiological link between accessory path-ways and ventricular dysfunction has been proposed inthe absence of tachycardia-induced cardiomyopathy [9 1222] Most prior reports investigating this association havefocused on septal pathways [9ndash12] In our study whichincorporated detailed echocardiographic assessment prior
4 BioMed Research International
Table 2 Echocardiographic parameters prior to and following catheter ablation
Patient Location of AP LV ejection fraction () SPWMD (ms) ESD septal (ms) ESD lateral (ms) Delta ESD septal-lateral (ms)PRE POST PRE POST PRE POST PRE POST PRE POST
1 LL 48 58 101 100 256 143 240 120 16 232 RPS 72 68 47 64 164 147 147 120 17 273 RPS 55 NA 58 40 NA NA NA NA NA NA4 RPS 61 57 30 33 211 154 NA NA NA NA5 RPL 50 76 53 47 200 110 167 110 33 06 LPS 60 63 50 87 157 112 122 92 35 207 LP 61 61 5 64 175 135 146 117 29 188 RA 48 53 31 40 184 188 280 271 96 839 LL 62 59 33 63 125 124 112 122 13 210 LL 65 68 44 61 162 180 96 175 66 511 RAS 49 62 76 78 293 195 183 NA 110 NA12 RA 52 55 99 10 192 170 133 155 59 1513 LL 68 77 15 115 140 127 110 103 30 2414 RL 55 62 80 61 155 NA 280 NA 125 NA15 LL 49 50 100 72 133 108 110 96 23 1216 RPS NA 62 77 75 NA NA NA NA NA NAMean plusmn SD mdash 57 plusmn 8 62 plusmn 8 56 plusmn 30 63 plusmn 26 182 plusmn 47 145 plusmn 30 164 plusmn 64 135 plusmn 52 50 plusmn 38 21 plusmn 23LVdenotes left ventricle SPWMD septal-to-posterior wallmotion delay ESD electrosystolic delay (or time-to-peak systolic velocity) PRE preablation POSTpostablation LL left lateral RPS right posteroseptal RPL right posterolateral LPS left posteroseptal LP left posterior RAS right anteroseptal RAL rightanterolateral RA right anterior RL right lateral NA not available
Figure 2 Assessment of septal-to-posterior wall motion delay(SPWMD) using M-mode imaging Normal SPWMD (lt130ms) isdemonstrated
to and following catheter ablation of accessory pathwaysthe following salient features were noted (1) left ventriculardyssynchrony and dysfunction were observed in patientswith septal and nonseptal pathways (2) dyssynchrony anddysfunction were reversible following successful ablation ofthe accessory pathway (3) improvements were more markedin patients with nonseptal pathways and (4) left ventriculardiastolic function parameters prior to ablation (ie meanlateral and septal EE1015840 values of 56 and 71 resp) werecomparable to a cohort of 325 healthy children [23] andunchanged following ablation
Tomaske et al retrospectively reported a series of 34children (mean age 142 years) with Wolff-Parkinson-Whitesyndrome who underwent successful radiofrequency abla-tion of right septal or posteroseptal accessory pathways
[12] Prior to ablation 56 of patients had a left ventric-ular ejection fraction lt55 It improved significantly aftercatheter ablation from a mean of 50 to 56 Classicdyssynchrony parameters were studied Whereas SPWMDdecreased significantly after ablation no change in IVMDwasobserved Five patients underwent two-dimensional strainanalysis which showed a reduction in the difference betweenthe earliest and latest negative strain after ablation Our studyextends these findings to include an analysis of tissueDopplerimaging to children with manifest ventricular preexcitationregardless of its location
In another series of 63 children with Wolff-Parkinson-White syndrome (mean age at diagnosis 59 years) leftventricular dysfunctionwas reported only in associationwithseptal accessory pathways [11] The mean left ventricularejection fraction was 53 in patients with septal accessorypathways (119873 = 15) compared to 62 for all other locationsMoreover septal dyskinesia was identified in 6 patients withright septal accessory pathways and was the only factorsignificantly associated with a reduction in left ventricularejection fraction After ablation the left ventricular ejectionfraction significantly improved in these 6 patients from 42 plusmn5 to 55plusmn7 TissueDoppler imagingwas not systematicallyperformed
The relationship between dyskinetic segments and leftventricular dysfunction is also supported by the pacemakerliterature which suggests that right ventricular apical pacingmay have a detrimental effect on left ventricular function[24ndash26] Restoration of cardiac synchrony by cardiac resyn-chronization therapy is a well-established intervention thatimproves all-cause mortality [27 28] Animal experiments
BioMed Research International 5
(a) (b)
Figure 3 Determination of the delay between time-to-peak systolic velocity at basal septal (a) and basal lateral (b) segments using tissueDoppler imaging A significant delay is demonstrated in this patient (no 10)
Figure 4 Determination of time-velocity curves using color-codedtissue Doppler and Q-analyses (from left ventricular septal andlateral wall sample points selected in an apical long-axis view) Inthis example (patient no 6) no significant delay is demonstratedbetween septal and lateral left ventricular walls following catheterablation
have shown that asynchronous electrical activation inducedby ventricular pacing results in asymmetrical hypertro-phy and ventricular dilation due to regional differences inworkload [29] A pathophysiological link between nonseptalaccessory pathways and ventricular dyssynchrony is sup-ported by such preclinical experiments which demonstratedthat early activation of the left ventricular free wall inpaced dogs resulted in significant thinning of left ventricularmyocardium and thickening of the late-activated septumDyskinetic segments may function much like aneurysmsand induce adverse remodelling with progressive dilatation[9 10] Hemodynamic changes with altered blood flowpatterns may ensue producing endomyocardial fibroelasticthickening [10]
It may therefore be hypothesized that ventricular preex-citation can result in remodelling changes similar to ventric-ular pacing with segmental dyskinesia leading to thinningdyssynchrony ventricular dilation and ultimately ventricu-lar dysfunction Such a patternmay be produced fromany siteof ventricular activation remote from the normal conductionsystem Our results are consistent with the hypothesis thatdyssynchrony induced by nonseptal pathways may be asdeleterious and sometimes more so than septal pathways
020406080
100120140160180200
LVEF ()
After ablationBefore ablation
SPWMD(ms)
ESD septal(ms)
ESD lateral(ms)
Delta ESD septal-lateral
(ms)
Figure 5 Echocardiographic parameters prior to and followingcatheter ablation LVEF denotes left ventricular ejection fractionSPWMD septal-to-posteriorwallmotion delay ESD electrosystolicdelay (or time-to-peak systolic velocity)
Further studies are required to confirm these findings andto assess the relevance of targeting accessory pathways basedsolely on hemodynamic effects of preexcitation [30]
Limitations As is often the case with pediatric case seriesthe study was limited by the small number of patientsNevertheless to minimize selection bias all consecutivechildren referred for catheter ablation of Wolff-Parkinson-White syndrome were enrolled over a 2-year period Indetermining dyssynchrony echocardiographic assessmentwas limited to basal septal and lateral segments by means oftissue Doppler imaging The comparative value of samplingadditional segments or the use of potentially complementaryimaging techniques such as strain and strain rate could notbe assessed
5 Conclusion
In a series of pediatric patients with Wolff-Parkinson-White syndrome and absence of structural heart diseaseleft ventricular systolic function and dyssynchrony improved
6 BioMed Research International
after successful ablation of antegrade-conducting accessorypathways The more pronounced changes were observed inpatients with nonseptal pathways
Conflict of Interests
The authors do not have any conflict of interests with thecontent of the paper
References
[1] KHina TMurakami S Kusachi et al ldquoDecreased amplitude ofleft ventricular posterior wall motion with notch movement todetermine the left posterior septal accessory pathway in Wolff-Parkinson-White syndromerdquo Heart vol 82 no 6 pp 731ndash7391999
[2] H Hishida I Sotobata and Y Koike ldquoEchocardiographic pat-terns of ventricular contraction in the Wolff-Parkinson-Whitesyndromerdquo Circulation vol 54 no 4 pp 567ndash570 1976
[3] A N DeMaria Z Vera A Neumann and D TMason ldquoAltera-tions in ventricular contraction pattern in theWolff-Parkinson-White syndrome Detection by echocardiographyrdquo Circulationvol 53 no 2 pp 249ndash257 1976
[4] A R Ticzon A N Damato A R Caracta G Russo J R Fosterand S H Lau ldquoInterventricular septal motion during preexci-tation and normal conduction in Wolff-Parkinson-White syn-drome Echocardiographic and electrophysiologic correlationrdquoThe American Journal of Cardiology vol 37 no 6 pp 840ndash8471976
[5] G S Francis PTheroux R AOrsquoRourke ADHagan andADJohnson ldquoAn echocardiographic study of interventricular septalmotion in the Wolff-Parkinson-White syndromerdquo Circulationvol 54 no 2 pp 174ndash178 1976
[6] L Sasse and H A del Puerto ldquoEchocardiography of ventric-ular septal movement in Wolff-Parkinson-White syndromerdquoArchivos del Instituto de Cardiologia de Mexico vol 46 no 4pp 445ndash450 1976
[7] J P Boineau J F Moore and W C Sealy ldquoBasis of clinicalECG variations in right and left ventricular pre-excitation Aunitary concept of WPWrdquo in Cardiac Arrhythmias The 25thHahnemann Symposium Grune and Stratton New York NYUSA 1973
[8] F E A U ten Cate M A Kruessell K Wagner et al ldquoDilatedcardiomyopathy in children with ventricular preexcitationthe location of the accessory pathway is predictive of thisassociationrdquo Journal of Electrocardiology vol 43 no 2 pp 146ndash154 2010
[9] G Fazio M Mongiovi L Sutera G Novo S Novo and SPipitone ldquoSegmental dyskinesia inWolff-Parkinson-White syn-drome a possible cause of dilatative cardiomyopathyrdquo Interna-tional Journal of Cardiology vol 123 no 2 pp e31ndashe34 2008
[10] J Cadrin-Tourigny A Fournier G Andelfinger and P KhairyldquoSevere left ventricular dysfunction in infants with ventricularpreexcitationrdquo Heart Rhythm vol 5 no 9 pp 1320ndash1322 2008
[11] B S Kwon E J Bae G B Kim C I Noh J Y Choi and YS Yun ldquoSeptal dyskinesia and global left ventricular dysfunc-tion in pediatric Wolff-Parkinson-White syndrome with septalaccessory pathwayrdquo Journal of Cardiovascular Electrophysiologyvol 21 no 3 pp 290ndash295 2010
[12] M Tomaske J Janousek V Razek et al ldquoAdverse effects ofWolff-Parkinson-White syndrome with right septal or pos-teroseptal accessory pathways on cardiac functionrdquo Europacevol 10 no 2 pp 181ndash189 2008
[13] L V A Boersma E Garcıa-Moran L Mont and J BrugadaldquoAccessory pathway localization by QRS polarity in childrenwith Wolff-Parkinson-White syndromerdquo Journal of Cardiovas-cular Electrophysiology vol 13 no 12 pp 1222ndash1226 2002
[14] S Cazeau P Bordachar G Jauvert et al ldquoEchocardiographicmodeling of cardiac dyssynchrony before and during multisitestimulation a prospective studyrdquo Pacing and Clinical Electro-physiology vol 26 no 1 pp 137ndash143 2003
[15] M V Pitzalis M Iacoviello R Romito G Luzzi M Anaclerioand C Forleo ldquoRole of septal to posterior wall motion delayin cardiac resynchronization therapyrdquo Journal of the AmericanCollege of Cardiology vol 48 no 3 pp 596ndash597 2006
[16] J J Bax T H Marwick S G Molhoek et al ldquoLeft ventriculardyssynchrony predicts benefit of cardiac resynchronizationtherapy in patients with end-stage heart failure before pace-maker implantationrdquo The American Journal of Cardiology vol92 no 10 pp 1238ndash1240 2003
[17] N B Schiller ldquoTwo-dimensional echocardiographic determi-nation of left ventricular volume systolic function and massSummary and discussion of the 1989 recommendations of theAmerican society of echocardiographyrdquo Circulation vol 84 no3 pp I280ndashI287 1991
[18] WA ZoghbiM Enriquez-Sarano E Foster et al ldquoRecommen-dations for evaluation of the severity of native valvular regur-gitation with two-dimensional and doppler echocardiographyrdquoJournal of the American Society of Echocardiography vol 16 no7 pp 777ndash802 2003
[19] E Abergel ldquoEchocardiographic indices of diastolic function putto the practical testrdquo Archives des Maladies du Coeur et desVaisseaux vol 98 no 4 pp 325ndash330 2005
[20] C J McMahon S F Nagueh R H Pignatelli et al ldquoCharac-terization of left ventricular diastolic function by tissue dopplerimaging and clinical status in children with hypertrophic car-diomyopathyrdquo Circulation vol 109 no 14 pp 1756ndash1762 2004
[21] P Rumeau P Acar S Paranon et al ldquoEvaluation of left ventric-ular diastolic function in children by doppler tissue imagingrdquoArchives des Maladies du Coeur et des Vaisseaux vol 100 no 5pp 405ndash410 2007
[22] M Emmel S Balaji andN Sreeram ldquoVentricular preexcitationassociated with dilated cardiomyopathy a causal relationshiprdquoCardiology in the Young vol 14 no 6 pp 594ndash599 2004
[23] B W Eidem C J McMahon R R Cohen et al ldquoImpactof cardiac growth on doppler tissue imaging velocities astudy in healthy childrenrdquo Journal of the American Society ofEchocardiography vol 17 no 3 pp 212ndash221 2004
[24] P P Karpawich ldquoChronic right ventricular pacing and cardiacperformance The pediatric perspectiverdquo Pacing and ClinicalElectrophysiology vol 27 no 6 pp 844ndash849 2004
[25] A S Manolis ldquoThe deleterious consequences of right ventricu-lar apical pacing time to seek alternate site pacingrdquo Pacing andClinical Electrophysiology vol 29 no 3 pp 298ndash315 2006
[26] M V T Tantengco R L Thomas and P P Karpawich ldquoLeftventricular dysfunction after long-term right ventricular apicalpacing in the youngrdquo Journal of the American College ofCardiology vol 37 no 8 pp 2093ndash2100 2001
BioMed Research International 7
[27] M R Bristow L A Saxon J Boehmer et al ldquoCardiac-resyn-chronization therapy with or without an implantable defibrilla-tor in advanced chronic heart failurerdquoTheNew England Journalof Medicine vol 350 no 21 pp 2140ndash2150 2004
[28] J G F Cleland J Daubert E Erdmann et al ldquoThe effect ofcardiac resynchronization on morbidity and mortality in heartfailurerdquo The New England Journal of Medicine vol 352 no 15pp 1539ndash1549 2005
[29] F W Prinzen E C Cheriex T Delhaas et al ldquoAsymmetricthickness of the left ventricular wall resulting from asyn-chronous electric activation a study in dogs with ventricularpacing and in patients with left bundle branch blockrdquo TheAmerican Heart Journal vol 130 no 5 pp 1045ndash1053 1995
[30] M I Cohen J K Triedman B C Cannon et al ldquoPACESHRSexpert consensus statement on the management of the asymp-tomatic young patient with a Wolff-Parkinson-White (WPWventricular preexcitation) electrocardiographic patternrdquo HeartRhythm vol 9 no 6 pp 1006ndash1024 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
(a) (b)
Figure 1 Determination of interventricular mechanical delay (IVMD) using pulsed Doppler mode corresponding to the difference betweenaortic (a) and pulmonary (b) preejection delay No significant delay in left ventricular contraction is observed
Table 1 Baseline and procedural characteristics
Patient Age at ablation(years) Weight (kg) Body surface
area (m2) Energy source Location of AP Delta-HVinterval (ms)
FU after ablation(months)
1 167 587 18 RF LL 77 2772 194 730 19 RF RPS 53 2083 150 586 17 RF RPS 40 2084 189 620 17 RF RPS 10 2155 149 560 16 RF RPL 45 2646 137 540 16 RF LPS 18 047 165 770 19 RF LP 81 398 130 390 13 Cryo RA 23 409 141 710 18 RF LL 21 4010 97 300 11 RF LL 17 4111 76 230 09 Cryo RAS NA 4212 68 220 09 Cryo RA 40 5913 171 600 17 RF LL 24 6514 164 700 18 RF RL 39 9315 153 580 16 RF LL 19 15116 118 400 13 Cryo RPS 44 185Summary 142 plusmn 37 533 plusmn 175 15 plusmn 03 RF 12 Cryo 6 6 septal 10 nonseptal 367 plusmn 214 121 plusmn 92AP denotes accessory pathway FU followup RF radiofrequency Cryo cryoenergy LL left lateral RPS right posteroseptal RPL right posterolateral LPSleft posteroseptal LP left posterior RAS right anteroseptal RAL right anterolateral RA right anterior RL right lateral NA not available
6 patients had a left ventricular ejection fraction lt55 and4 lt50 Following ablation the ejection fraction increasedby 49 plusmn 21 (119875 = 0038) from a baseline value of 570 plusmn78This was accompanied by a significant reduction in thedifference between aortic and pulmonary preejection times(110 plusmn 33ms 119875 = 0017) The left ventricular ejectionfraction increased to a greater extent following ablation ofnonseptal (59 plusmn 26 119875 = 0023) versus septal (25 plusmn 41119875 = 0461) pathways The 4 patients with a left ventricularejection fraction lt50 prior to ablation 2 of whom had leftlateral pathways improved to gt50 after ablation By tissueDoppler imaging the time to peak systolic velocity decreasedfrom 330ms (IQR 200 480) to 180ms (IQR 50 240)119875 = 0013 No significant change in septal-to-posterior wallmotion delay or diastolic parameters was noted
Similar to changes in left ventricular ejection fraction themagnitude of improvement in left ventricular dyssynchronywas more marked in patients with nonseptal versus septalpathways The difference between septal and lateral wallmotion delay before and after ablation was 206 plusmn 71ms(119875 = 0015) versus 14 plusmn 114ms (119875 = 0655) for nonseptalversus septal pathways respectively
4 Discussion
A possible pathophysiological link between accessory path-ways and ventricular dysfunction has been proposed inthe absence of tachycardia-induced cardiomyopathy [9 1222] Most prior reports investigating this association havefocused on septal pathways [9ndash12] In our study whichincorporated detailed echocardiographic assessment prior
4 BioMed Research International
Table 2 Echocardiographic parameters prior to and following catheter ablation
Patient Location of AP LV ejection fraction () SPWMD (ms) ESD septal (ms) ESD lateral (ms) Delta ESD septal-lateral (ms)PRE POST PRE POST PRE POST PRE POST PRE POST
1 LL 48 58 101 100 256 143 240 120 16 232 RPS 72 68 47 64 164 147 147 120 17 273 RPS 55 NA 58 40 NA NA NA NA NA NA4 RPS 61 57 30 33 211 154 NA NA NA NA5 RPL 50 76 53 47 200 110 167 110 33 06 LPS 60 63 50 87 157 112 122 92 35 207 LP 61 61 5 64 175 135 146 117 29 188 RA 48 53 31 40 184 188 280 271 96 839 LL 62 59 33 63 125 124 112 122 13 210 LL 65 68 44 61 162 180 96 175 66 511 RAS 49 62 76 78 293 195 183 NA 110 NA12 RA 52 55 99 10 192 170 133 155 59 1513 LL 68 77 15 115 140 127 110 103 30 2414 RL 55 62 80 61 155 NA 280 NA 125 NA15 LL 49 50 100 72 133 108 110 96 23 1216 RPS NA 62 77 75 NA NA NA NA NA NAMean plusmn SD mdash 57 plusmn 8 62 plusmn 8 56 plusmn 30 63 plusmn 26 182 plusmn 47 145 plusmn 30 164 plusmn 64 135 plusmn 52 50 plusmn 38 21 plusmn 23LVdenotes left ventricle SPWMD septal-to-posterior wallmotion delay ESD electrosystolic delay (or time-to-peak systolic velocity) PRE preablation POSTpostablation LL left lateral RPS right posteroseptal RPL right posterolateral LPS left posteroseptal LP left posterior RAS right anteroseptal RAL rightanterolateral RA right anterior RL right lateral NA not available
Figure 2 Assessment of septal-to-posterior wall motion delay(SPWMD) using M-mode imaging Normal SPWMD (lt130ms) isdemonstrated
to and following catheter ablation of accessory pathwaysthe following salient features were noted (1) left ventriculardyssynchrony and dysfunction were observed in patientswith septal and nonseptal pathways (2) dyssynchrony anddysfunction were reversible following successful ablation ofthe accessory pathway (3) improvements were more markedin patients with nonseptal pathways and (4) left ventriculardiastolic function parameters prior to ablation (ie meanlateral and septal EE1015840 values of 56 and 71 resp) werecomparable to a cohort of 325 healthy children [23] andunchanged following ablation
Tomaske et al retrospectively reported a series of 34children (mean age 142 years) with Wolff-Parkinson-Whitesyndrome who underwent successful radiofrequency abla-tion of right septal or posteroseptal accessory pathways
[12] Prior to ablation 56 of patients had a left ventric-ular ejection fraction lt55 It improved significantly aftercatheter ablation from a mean of 50 to 56 Classicdyssynchrony parameters were studied Whereas SPWMDdecreased significantly after ablation no change in IVMDwasobserved Five patients underwent two-dimensional strainanalysis which showed a reduction in the difference betweenthe earliest and latest negative strain after ablation Our studyextends these findings to include an analysis of tissueDopplerimaging to children with manifest ventricular preexcitationregardless of its location
In another series of 63 children with Wolff-Parkinson-White syndrome (mean age at diagnosis 59 years) leftventricular dysfunctionwas reported only in associationwithseptal accessory pathways [11] The mean left ventricularejection fraction was 53 in patients with septal accessorypathways (119873 = 15) compared to 62 for all other locationsMoreover septal dyskinesia was identified in 6 patients withright septal accessory pathways and was the only factorsignificantly associated with a reduction in left ventricularejection fraction After ablation the left ventricular ejectionfraction significantly improved in these 6 patients from 42 plusmn5 to 55plusmn7 TissueDoppler imagingwas not systematicallyperformed
The relationship between dyskinetic segments and leftventricular dysfunction is also supported by the pacemakerliterature which suggests that right ventricular apical pacingmay have a detrimental effect on left ventricular function[24ndash26] Restoration of cardiac synchrony by cardiac resyn-chronization therapy is a well-established intervention thatimproves all-cause mortality [27 28] Animal experiments
BioMed Research International 5
(a) (b)
Figure 3 Determination of the delay between time-to-peak systolic velocity at basal septal (a) and basal lateral (b) segments using tissueDoppler imaging A significant delay is demonstrated in this patient (no 10)
Figure 4 Determination of time-velocity curves using color-codedtissue Doppler and Q-analyses (from left ventricular septal andlateral wall sample points selected in an apical long-axis view) Inthis example (patient no 6) no significant delay is demonstratedbetween septal and lateral left ventricular walls following catheterablation
have shown that asynchronous electrical activation inducedby ventricular pacing results in asymmetrical hypertro-phy and ventricular dilation due to regional differences inworkload [29] A pathophysiological link between nonseptalaccessory pathways and ventricular dyssynchrony is sup-ported by such preclinical experiments which demonstratedthat early activation of the left ventricular free wall inpaced dogs resulted in significant thinning of left ventricularmyocardium and thickening of the late-activated septumDyskinetic segments may function much like aneurysmsand induce adverse remodelling with progressive dilatation[9 10] Hemodynamic changes with altered blood flowpatterns may ensue producing endomyocardial fibroelasticthickening [10]
It may therefore be hypothesized that ventricular preex-citation can result in remodelling changes similar to ventric-ular pacing with segmental dyskinesia leading to thinningdyssynchrony ventricular dilation and ultimately ventricu-lar dysfunction Such a patternmay be produced fromany siteof ventricular activation remote from the normal conductionsystem Our results are consistent with the hypothesis thatdyssynchrony induced by nonseptal pathways may be asdeleterious and sometimes more so than septal pathways
020406080
100120140160180200
LVEF ()
After ablationBefore ablation
SPWMD(ms)
ESD septal(ms)
ESD lateral(ms)
Delta ESD septal-lateral
(ms)
Figure 5 Echocardiographic parameters prior to and followingcatheter ablation LVEF denotes left ventricular ejection fractionSPWMD septal-to-posteriorwallmotion delay ESD electrosystolicdelay (or time-to-peak systolic velocity)
Further studies are required to confirm these findings andto assess the relevance of targeting accessory pathways basedsolely on hemodynamic effects of preexcitation [30]
Limitations As is often the case with pediatric case seriesthe study was limited by the small number of patientsNevertheless to minimize selection bias all consecutivechildren referred for catheter ablation of Wolff-Parkinson-White syndrome were enrolled over a 2-year period Indetermining dyssynchrony echocardiographic assessmentwas limited to basal septal and lateral segments by means oftissue Doppler imaging The comparative value of samplingadditional segments or the use of potentially complementaryimaging techniques such as strain and strain rate could notbe assessed
5 Conclusion
In a series of pediatric patients with Wolff-Parkinson-White syndrome and absence of structural heart diseaseleft ventricular systolic function and dyssynchrony improved
6 BioMed Research International
after successful ablation of antegrade-conducting accessorypathways The more pronounced changes were observed inpatients with nonseptal pathways
Conflict of Interests
The authors do not have any conflict of interests with thecontent of the paper
References
[1] KHina TMurakami S Kusachi et al ldquoDecreased amplitude ofleft ventricular posterior wall motion with notch movement todetermine the left posterior septal accessory pathway in Wolff-Parkinson-White syndromerdquo Heart vol 82 no 6 pp 731ndash7391999
[2] H Hishida I Sotobata and Y Koike ldquoEchocardiographic pat-terns of ventricular contraction in the Wolff-Parkinson-Whitesyndromerdquo Circulation vol 54 no 4 pp 567ndash570 1976
[3] A N DeMaria Z Vera A Neumann and D TMason ldquoAltera-tions in ventricular contraction pattern in theWolff-Parkinson-White syndrome Detection by echocardiographyrdquo Circulationvol 53 no 2 pp 249ndash257 1976
[4] A R Ticzon A N Damato A R Caracta G Russo J R Fosterand S H Lau ldquoInterventricular septal motion during preexci-tation and normal conduction in Wolff-Parkinson-White syn-drome Echocardiographic and electrophysiologic correlationrdquoThe American Journal of Cardiology vol 37 no 6 pp 840ndash8471976
[5] G S Francis PTheroux R AOrsquoRourke ADHagan andADJohnson ldquoAn echocardiographic study of interventricular septalmotion in the Wolff-Parkinson-White syndromerdquo Circulationvol 54 no 2 pp 174ndash178 1976
[6] L Sasse and H A del Puerto ldquoEchocardiography of ventric-ular septal movement in Wolff-Parkinson-White syndromerdquoArchivos del Instituto de Cardiologia de Mexico vol 46 no 4pp 445ndash450 1976
[7] J P Boineau J F Moore and W C Sealy ldquoBasis of clinicalECG variations in right and left ventricular pre-excitation Aunitary concept of WPWrdquo in Cardiac Arrhythmias The 25thHahnemann Symposium Grune and Stratton New York NYUSA 1973
[8] F E A U ten Cate M A Kruessell K Wagner et al ldquoDilatedcardiomyopathy in children with ventricular preexcitationthe location of the accessory pathway is predictive of thisassociationrdquo Journal of Electrocardiology vol 43 no 2 pp 146ndash154 2010
[9] G Fazio M Mongiovi L Sutera G Novo S Novo and SPipitone ldquoSegmental dyskinesia inWolff-Parkinson-White syn-drome a possible cause of dilatative cardiomyopathyrdquo Interna-tional Journal of Cardiology vol 123 no 2 pp e31ndashe34 2008
[10] J Cadrin-Tourigny A Fournier G Andelfinger and P KhairyldquoSevere left ventricular dysfunction in infants with ventricularpreexcitationrdquo Heart Rhythm vol 5 no 9 pp 1320ndash1322 2008
[11] B S Kwon E J Bae G B Kim C I Noh J Y Choi and YS Yun ldquoSeptal dyskinesia and global left ventricular dysfunc-tion in pediatric Wolff-Parkinson-White syndrome with septalaccessory pathwayrdquo Journal of Cardiovascular Electrophysiologyvol 21 no 3 pp 290ndash295 2010
[12] M Tomaske J Janousek V Razek et al ldquoAdverse effects ofWolff-Parkinson-White syndrome with right septal or pos-teroseptal accessory pathways on cardiac functionrdquo Europacevol 10 no 2 pp 181ndash189 2008
[13] L V A Boersma E Garcıa-Moran L Mont and J BrugadaldquoAccessory pathway localization by QRS polarity in childrenwith Wolff-Parkinson-White syndromerdquo Journal of Cardiovas-cular Electrophysiology vol 13 no 12 pp 1222ndash1226 2002
[14] S Cazeau P Bordachar G Jauvert et al ldquoEchocardiographicmodeling of cardiac dyssynchrony before and during multisitestimulation a prospective studyrdquo Pacing and Clinical Electro-physiology vol 26 no 1 pp 137ndash143 2003
[15] M V Pitzalis M Iacoviello R Romito G Luzzi M Anaclerioand C Forleo ldquoRole of septal to posterior wall motion delayin cardiac resynchronization therapyrdquo Journal of the AmericanCollege of Cardiology vol 48 no 3 pp 596ndash597 2006
[16] J J Bax T H Marwick S G Molhoek et al ldquoLeft ventriculardyssynchrony predicts benefit of cardiac resynchronizationtherapy in patients with end-stage heart failure before pace-maker implantationrdquo The American Journal of Cardiology vol92 no 10 pp 1238ndash1240 2003
[17] N B Schiller ldquoTwo-dimensional echocardiographic determi-nation of left ventricular volume systolic function and massSummary and discussion of the 1989 recommendations of theAmerican society of echocardiographyrdquo Circulation vol 84 no3 pp I280ndashI287 1991
[18] WA ZoghbiM Enriquez-Sarano E Foster et al ldquoRecommen-dations for evaluation of the severity of native valvular regur-gitation with two-dimensional and doppler echocardiographyrdquoJournal of the American Society of Echocardiography vol 16 no7 pp 777ndash802 2003
[19] E Abergel ldquoEchocardiographic indices of diastolic function putto the practical testrdquo Archives des Maladies du Coeur et desVaisseaux vol 98 no 4 pp 325ndash330 2005
[20] C J McMahon S F Nagueh R H Pignatelli et al ldquoCharac-terization of left ventricular diastolic function by tissue dopplerimaging and clinical status in children with hypertrophic car-diomyopathyrdquo Circulation vol 109 no 14 pp 1756ndash1762 2004
[21] P Rumeau P Acar S Paranon et al ldquoEvaluation of left ventric-ular diastolic function in children by doppler tissue imagingrdquoArchives des Maladies du Coeur et des Vaisseaux vol 100 no 5pp 405ndash410 2007
[22] M Emmel S Balaji andN Sreeram ldquoVentricular preexcitationassociated with dilated cardiomyopathy a causal relationshiprdquoCardiology in the Young vol 14 no 6 pp 594ndash599 2004
[23] B W Eidem C J McMahon R R Cohen et al ldquoImpactof cardiac growth on doppler tissue imaging velocities astudy in healthy childrenrdquo Journal of the American Society ofEchocardiography vol 17 no 3 pp 212ndash221 2004
[24] P P Karpawich ldquoChronic right ventricular pacing and cardiacperformance The pediatric perspectiverdquo Pacing and ClinicalElectrophysiology vol 27 no 6 pp 844ndash849 2004
[25] A S Manolis ldquoThe deleterious consequences of right ventricu-lar apical pacing time to seek alternate site pacingrdquo Pacing andClinical Electrophysiology vol 29 no 3 pp 298ndash315 2006
[26] M V T Tantengco R L Thomas and P P Karpawich ldquoLeftventricular dysfunction after long-term right ventricular apicalpacing in the youngrdquo Journal of the American College ofCardiology vol 37 no 8 pp 2093ndash2100 2001
BioMed Research International 7
[27] M R Bristow L A Saxon J Boehmer et al ldquoCardiac-resyn-chronization therapy with or without an implantable defibrilla-tor in advanced chronic heart failurerdquoTheNew England Journalof Medicine vol 350 no 21 pp 2140ndash2150 2004
[28] J G F Cleland J Daubert E Erdmann et al ldquoThe effect ofcardiac resynchronization on morbidity and mortality in heartfailurerdquo The New England Journal of Medicine vol 352 no 15pp 1539ndash1549 2005
[29] F W Prinzen E C Cheriex T Delhaas et al ldquoAsymmetricthickness of the left ventricular wall resulting from asyn-chronous electric activation a study in dogs with ventricularpacing and in patients with left bundle branch blockrdquo TheAmerican Heart Journal vol 130 no 5 pp 1045ndash1053 1995
[30] M I Cohen J K Triedman B C Cannon et al ldquoPACESHRSexpert consensus statement on the management of the asymp-tomatic young patient with a Wolff-Parkinson-White (WPWventricular preexcitation) electrocardiographic patternrdquo HeartRhythm vol 9 no 6 pp 1006ndash1024 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
Table 2 Echocardiographic parameters prior to and following catheter ablation
Patient Location of AP LV ejection fraction () SPWMD (ms) ESD septal (ms) ESD lateral (ms) Delta ESD septal-lateral (ms)PRE POST PRE POST PRE POST PRE POST PRE POST
1 LL 48 58 101 100 256 143 240 120 16 232 RPS 72 68 47 64 164 147 147 120 17 273 RPS 55 NA 58 40 NA NA NA NA NA NA4 RPS 61 57 30 33 211 154 NA NA NA NA5 RPL 50 76 53 47 200 110 167 110 33 06 LPS 60 63 50 87 157 112 122 92 35 207 LP 61 61 5 64 175 135 146 117 29 188 RA 48 53 31 40 184 188 280 271 96 839 LL 62 59 33 63 125 124 112 122 13 210 LL 65 68 44 61 162 180 96 175 66 511 RAS 49 62 76 78 293 195 183 NA 110 NA12 RA 52 55 99 10 192 170 133 155 59 1513 LL 68 77 15 115 140 127 110 103 30 2414 RL 55 62 80 61 155 NA 280 NA 125 NA15 LL 49 50 100 72 133 108 110 96 23 1216 RPS NA 62 77 75 NA NA NA NA NA NAMean plusmn SD mdash 57 plusmn 8 62 plusmn 8 56 plusmn 30 63 plusmn 26 182 plusmn 47 145 plusmn 30 164 plusmn 64 135 plusmn 52 50 plusmn 38 21 plusmn 23LVdenotes left ventricle SPWMD septal-to-posterior wallmotion delay ESD electrosystolic delay (or time-to-peak systolic velocity) PRE preablation POSTpostablation LL left lateral RPS right posteroseptal RPL right posterolateral LPS left posteroseptal LP left posterior RAS right anteroseptal RAL rightanterolateral RA right anterior RL right lateral NA not available
Figure 2 Assessment of septal-to-posterior wall motion delay(SPWMD) using M-mode imaging Normal SPWMD (lt130ms) isdemonstrated
to and following catheter ablation of accessory pathwaysthe following salient features were noted (1) left ventriculardyssynchrony and dysfunction were observed in patientswith septal and nonseptal pathways (2) dyssynchrony anddysfunction were reversible following successful ablation ofthe accessory pathway (3) improvements were more markedin patients with nonseptal pathways and (4) left ventriculardiastolic function parameters prior to ablation (ie meanlateral and septal EE1015840 values of 56 and 71 resp) werecomparable to a cohort of 325 healthy children [23] andunchanged following ablation
Tomaske et al retrospectively reported a series of 34children (mean age 142 years) with Wolff-Parkinson-Whitesyndrome who underwent successful radiofrequency abla-tion of right septal or posteroseptal accessory pathways
[12] Prior to ablation 56 of patients had a left ventric-ular ejection fraction lt55 It improved significantly aftercatheter ablation from a mean of 50 to 56 Classicdyssynchrony parameters were studied Whereas SPWMDdecreased significantly after ablation no change in IVMDwasobserved Five patients underwent two-dimensional strainanalysis which showed a reduction in the difference betweenthe earliest and latest negative strain after ablation Our studyextends these findings to include an analysis of tissueDopplerimaging to children with manifest ventricular preexcitationregardless of its location
In another series of 63 children with Wolff-Parkinson-White syndrome (mean age at diagnosis 59 years) leftventricular dysfunctionwas reported only in associationwithseptal accessory pathways [11] The mean left ventricularejection fraction was 53 in patients with septal accessorypathways (119873 = 15) compared to 62 for all other locationsMoreover septal dyskinesia was identified in 6 patients withright septal accessory pathways and was the only factorsignificantly associated with a reduction in left ventricularejection fraction After ablation the left ventricular ejectionfraction significantly improved in these 6 patients from 42 plusmn5 to 55plusmn7 TissueDoppler imagingwas not systematicallyperformed
The relationship between dyskinetic segments and leftventricular dysfunction is also supported by the pacemakerliterature which suggests that right ventricular apical pacingmay have a detrimental effect on left ventricular function[24ndash26] Restoration of cardiac synchrony by cardiac resyn-chronization therapy is a well-established intervention thatimproves all-cause mortality [27 28] Animal experiments
BioMed Research International 5
(a) (b)
Figure 3 Determination of the delay between time-to-peak systolic velocity at basal septal (a) and basal lateral (b) segments using tissueDoppler imaging A significant delay is demonstrated in this patient (no 10)
Figure 4 Determination of time-velocity curves using color-codedtissue Doppler and Q-analyses (from left ventricular septal andlateral wall sample points selected in an apical long-axis view) Inthis example (patient no 6) no significant delay is demonstratedbetween septal and lateral left ventricular walls following catheterablation
have shown that asynchronous electrical activation inducedby ventricular pacing results in asymmetrical hypertro-phy and ventricular dilation due to regional differences inworkload [29] A pathophysiological link between nonseptalaccessory pathways and ventricular dyssynchrony is sup-ported by such preclinical experiments which demonstratedthat early activation of the left ventricular free wall inpaced dogs resulted in significant thinning of left ventricularmyocardium and thickening of the late-activated septumDyskinetic segments may function much like aneurysmsand induce adverse remodelling with progressive dilatation[9 10] Hemodynamic changes with altered blood flowpatterns may ensue producing endomyocardial fibroelasticthickening [10]
It may therefore be hypothesized that ventricular preex-citation can result in remodelling changes similar to ventric-ular pacing with segmental dyskinesia leading to thinningdyssynchrony ventricular dilation and ultimately ventricu-lar dysfunction Such a patternmay be produced fromany siteof ventricular activation remote from the normal conductionsystem Our results are consistent with the hypothesis thatdyssynchrony induced by nonseptal pathways may be asdeleterious and sometimes more so than septal pathways
020406080
100120140160180200
LVEF ()
After ablationBefore ablation
SPWMD(ms)
ESD septal(ms)
ESD lateral(ms)
Delta ESD septal-lateral
(ms)
Figure 5 Echocardiographic parameters prior to and followingcatheter ablation LVEF denotes left ventricular ejection fractionSPWMD septal-to-posteriorwallmotion delay ESD electrosystolicdelay (or time-to-peak systolic velocity)
Further studies are required to confirm these findings andto assess the relevance of targeting accessory pathways basedsolely on hemodynamic effects of preexcitation [30]
Limitations As is often the case with pediatric case seriesthe study was limited by the small number of patientsNevertheless to minimize selection bias all consecutivechildren referred for catheter ablation of Wolff-Parkinson-White syndrome were enrolled over a 2-year period Indetermining dyssynchrony echocardiographic assessmentwas limited to basal septal and lateral segments by means oftissue Doppler imaging The comparative value of samplingadditional segments or the use of potentially complementaryimaging techniques such as strain and strain rate could notbe assessed
5 Conclusion
In a series of pediatric patients with Wolff-Parkinson-White syndrome and absence of structural heart diseaseleft ventricular systolic function and dyssynchrony improved
6 BioMed Research International
after successful ablation of antegrade-conducting accessorypathways The more pronounced changes were observed inpatients with nonseptal pathways
Conflict of Interests
The authors do not have any conflict of interests with thecontent of the paper
References
[1] KHina TMurakami S Kusachi et al ldquoDecreased amplitude ofleft ventricular posterior wall motion with notch movement todetermine the left posterior septal accessory pathway in Wolff-Parkinson-White syndromerdquo Heart vol 82 no 6 pp 731ndash7391999
[2] H Hishida I Sotobata and Y Koike ldquoEchocardiographic pat-terns of ventricular contraction in the Wolff-Parkinson-Whitesyndromerdquo Circulation vol 54 no 4 pp 567ndash570 1976
[3] A N DeMaria Z Vera A Neumann and D TMason ldquoAltera-tions in ventricular contraction pattern in theWolff-Parkinson-White syndrome Detection by echocardiographyrdquo Circulationvol 53 no 2 pp 249ndash257 1976
[4] A R Ticzon A N Damato A R Caracta G Russo J R Fosterand S H Lau ldquoInterventricular septal motion during preexci-tation and normal conduction in Wolff-Parkinson-White syn-drome Echocardiographic and electrophysiologic correlationrdquoThe American Journal of Cardiology vol 37 no 6 pp 840ndash8471976
[5] G S Francis PTheroux R AOrsquoRourke ADHagan andADJohnson ldquoAn echocardiographic study of interventricular septalmotion in the Wolff-Parkinson-White syndromerdquo Circulationvol 54 no 2 pp 174ndash178 1976
[6] L Sasse and H A del Puerto ldquoEchocardiography of ventric-ular septal movement in Wolff-Parkinson-White syndromerdquoArchivos del Instituto de Cardiologia de Mexico vol 46 no 4pp 445ndash450 1976
[7] J P Boineau J F Moore and W C Sealy ldquoBasis of clinicalECG variations in right and left ventricular pre-excitation Aunitary concept of WPWrdquo in Cardiac Arrhythmias The 25thHahnemann Symposium Grune and Stratton New York NYUSA 1973
[8] F E A U ten Cate M A Kruessell K Wagner et al ldquoDilatedcardiomyopathy in children with ventricular preexcitationthe location of the accessory pathway is predictive of thisassociationrdquo Journal of Electrocardiology vol 43 no 2 pp 146ndash154 2010
[9] G Fazio M Mongiovi L Sutera G Novo S Novo and SPipitone ldquoSegmental dyskinesia inWolff-Parkinson-White syn-drome a possible cause of dilatative cardiomyopathyrdquo Interna-tional Journal of Cardiology vol 123 no 2 pp e31ndashe34 2008
[10] J Cadrin-Tourigny A Fournier G Andelfinger and P KhairyldquoSevere left ventricular dysfunction in infants with ventricularpreexcitationrdquo Heart Rhythm vol 5 no 9 pp 1320ndash1322 2008
[11] B S Kwon E J Bae G B Kim C I Noh J Y Choi and YS Yun ldquoSeptal dyskinesia and global left ventricular dysfunc-tion in pediatric Wolff-Parkinson-White syndrome with septalaccessory pathwayrdquo Journal of Cardiovascular Electrophysiologyvol 21 no 3 pp 290ndash295 2010
[12] M Tomaske J Janousek V Razek et al ldquoAdverse effects ofWolff-Parkinson-White syndrome with right septal or pos-teroseptal accessory pathways on cardiac functionrdquo Europacevol 10 no 2 pp 181ndash189 2008
[13] L V A Boersma E Garcıa-Moran L Mont and J BrugadaldquoAccessory pathway localization by QRS polarity in childrenwith Wolff-Parkinson-White syndromerdquo Journal of Cardiovas-cular Electrophysiology vol 13 no 12 pp 1222ndash1226 2002
[14] S Cazeau P Bordachar G Jauvert et al ldquoEchocardiographicmodeling of cardiac dyssynchrony before and during multisitestimulation a prospective studyrdquo Pacing and Clinical Electro-physiology vol 26 no 1 pp 137ndash143 2003
[15] M V Pitzalis M Iacoviello R Romito G Luzzi M Anaclerioand C Forleo ldquoRole of septal to posterior wall motion delayin cardiac resynchronization therapyrdquo Journal of the AmericanCollege of Cardiology vol 48 no 3 pp 596ndash597 2006
[16] J J Bax T H Marwick S G Molhoek et al ldquoLeft ventriculardyssynchrony predicts benefit of cardiac resynchronizationtherapy in patients with end-stage heart failure before pace-maker implantationrdquo The American Journal of Cardiology vol92 no 10 pp 1238ndash1240 2003
[17] N B Schiller ldquoTwo-dimensional echocardiographic determi-nation of left ventricular volume systolic function and massSummary and discussion of the 1989 recommendations of theAmerican society of echocardiographyrdquo Circulation vol 84 no3 pp I280ndashI287 1991
[18] WA ZoghbiM Enriquez-Sarano E Foster et al ldquoRecommen-dations for evaluation of the severity of native valvular regur-gitation with two-dimensional and doppler echocardiographyrdquoJournal of the American Society of Echocardiography vol 16 no7 pp 777ndash802 2003
[19] E Abergel ldquoEchocardiographic indices of diastolic function putto the practical testrdquo Archives des Maladies du Coeur et desVaisseaux vol 98 no 4 pp 325ndash330 2005
[20] C J McMahon S F Nagueh R H Pignatelli et al ldquoCharac-terization of left ventricular diastolic function by tissue dopplerimaging and clinical status in children with hypertrophic car-diomyopathyrdquo Circulation vol 109 no 14 pp 1756ndash1762 2004
[21] P Rumeau P Acar S Paranon et al ldquoEvaluation of left ventric-ular diastolic function in children by doppler tissue imagingrdquoArchives des Maladies du Coeur et des Vaisseaux vol 100 no 5pp 405ndash410 2007
[22] M Emmel S Balaji andN Sreeram ldquoVentricular preexcitationassociated with dilated cardiomyopathy a causal relationshiprdquoCardiology in the Young vol 14 no 6 pp 594ndash599 2004
[23] B W Eidem C J McMahon R R Cohen et al ldquoImpactof cardiac growth on doppler tissue imaging velocities astudy in healthy childrenrdquo Journal of the American Society ofEchocardiography vol 17 no 3 pp 212ndash221 2004
[24] P P Karpawich ldquoChronic right ventricular pacing and cardiacperformance The pediatric perspectiverdquo Pacing and ClinicalElectrophysiology vol 27 no 6 pp 844ndash849 2004
[25] A S Manolis ldquoThe deleterious consequences of right ventricu-lar apical pacing time to seek alternate site pacingrdquo Pacing andClinical Electrophysiology vol 29 no 3 pp 298ndash315 2006
[26] M V T Tantengco R L Thomas and P P Karpawich ldquoLeftventricular dysfunction after long-term right ventricular apicalpacing in the youngrdquo Journal of the American College ofCardiology vol 37 no 8 pp 2093ndash2100 2001
BioMed Research International 7
[27] M R Bristow L A Saxon J Boehmer et al ldquoCardiac-resyn-chronization therapy with or without an implantable defibrilla-tor in advanced chronic heart failurerdquoTheNew England Journalof Medicine vol 350 no 21 pp 2140ndash2150 2004
[28] J G F Cleland J Daubert E Erdmann et al ldquoThe effect ofcardiac resynchronization on morbidity and mortality in heartfailurerdquo The New England Journal of Medicine vol 352 no 15pp 1539ndash1549 2005
[29] F W Prinzen E C Cheriex T Delhaas et al ldquoAsymmetricthickness of the left ventricular wall resulting from asyn-chronous electric activation a study in dogs with ventricularpacing and in patients with left bundle branch blockrdquo TheAmerican Heart Journal vol 130 no 5 pp 1045ndash1053 1995
[30] M I Cohen J K Triedman B C Cannon et al ldquoPACESHRSexpert consensus statement on the management of the asymp-tomatic young patient with a Wolff-Parkinson-White (WPWventricular preexcitation) electrocardiographic patternrdquo HeartRhythm vol 9 no 6 pp 1006ndash1024 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
(a) (b)
Figure 3 Determination of the delay between time-to-peak systolic velocity at basal septal (a) and basal lateral (b) segments using tissueDoppler imaging A significant delay is demonstrated in this patient (no 10)
Figure 4 Determination of time-velocity curves using color-codedtissue Doppler and Q-analyses (from left ventricular septal andlateral wall sample points selected in an apical long-axis view) Inthis example (patient no 6) no significant delay is demonstratedbetween septal and lateral left ventricular walls following catheterablation
have shown that asynchronous electrical activation inducedby ventricular pacing results in asymmetrical hypertro-phy and ventricular dilation due to regional differences inworkload [29] A pathophysiological link between nonseptalaccessory pathways and ventricular dyssynchrony is sup-ported by such preclinical experiments which demonstratedthat early activation of the left ventricular free wall inpaced dogs resulted in significant thinning of left ventricularmyocardium and thickening of the late-activated septumDyskinetic segments may function much like aneurysmsand induce adverse remodelling with progressive dilatation[9 10] Hemodynamic changes with altered blood flowpatterns may ensue producing endomyocardial fibroelasticthickening [10]
It may therefore be hypothesized that ventricular preex-citation can result in remodelling changes similar to ventric-ular pacing with segmental dyskinesia leading to thinningdyssynchrony ventricular dilation and ultimately ventricu-lar dysfunction Such a patternmay be produced fromany siteof ventricular activation remote from the normal conductionsystem Our results are consistent with the hypothesis thatdyssynchrony induced by nonseptal pathways may be asdeleterious and sometimes more so than septal pathways
020406080
100120140160180200
LVEF ()
After ablationBefore ablation
SPWMD(ms)
ESD septal(ms)
ESD lateral(ms)
Delta ESD septal-lateral
(ms)
Figure 5 Echocardiographic parameters prior to and followingcatheter ablation LVEF denotes left ventricular ejection fractionSPWMD septal-to-posteriorwallmotion delay ESD electrosystolicdelay (or time-to-peak systolic velocity)
Further studies are required to confirm these findings andto assess the relevance of targeting accessory pathways basedsolely on hemodynamic effects of preexcitation [30]
Limitations As is often the case with pediatric case seriesthe study was limited by the small number of patientsNevertheless to minimize selection bias all consecutivechildren referred for catheter ablation of Wolff-Parkinson-White syndrome were enrolled over a 2-year period Indetermining dyssynchrony echocardiographic assessmentwas limited to basal septal and lateral segments by means oftissue Doppler imaging The comparative value of samplingadditional segments or the use of potentially complementaryimaging techniques such as strain and strain rate could notbe assessed
5 Conclusion
In a series of pediatric patients with Wolff-Parkinson-White syndrome and absence of structural heart diseaseleft ventricular systolic function and dyssynchrony improved
6 BioMed Research International
after successful ablation of antegrade-conducting accessorypathways The more pronounced changes were observed inpatients with nonseptal pathways
Conflict of Interests
The authors do not have any conflict of interests with thecontent of the paper
References
[1] KHina TMurakami S Kusachi et al ldquoDecreased amplitude ofleft ventricular posterior wall motion with notch movement todetermine the left posterior septal accessory pathway in Wolff-Parkinson-White syndromerdquo Heart vol 82 no 6 pp 731ndash7391999
[2] H Hishida I Sotobata and Y Koike ldquoEchocardiographic pat-terns of ventricular contraction in the Wolff-Parkinson-Whitesyndromerdquo Circulation vol 54 no 4 pp 567ndash570 1976
[3] A N DeMaria Z Vera A Neumann and D TMason ldquoAltera-tions in ventricular contraction pattern in theWolff-Parkinson-White syndrome Detection by echocardiographyrdquo Circulationvol 53 no 2 pp 249ndash257 1976
[4] A R Ticzon A N Damato A R Caracta G Russo J R Fosterand S H Lau ldquoInterventricular septal motion during preexci-tation and normal conduction in Wolff-Parkinson-White syn-drome Echocardiographic and electrophysiologic correlationrdquoThe American Journal of Cardiology vol 37 no 6 pp 840ndash8471976
[5] G S Francis PTheroux R AOrsquoRourke ADHagan andADJohnson ldquoAn echocardiographic study of interventricular septalmotion in the Wolff-Parkinson-White syndromerdquo Circulationvol 54 no 2 pp 174ndash178 1976
[6] L Sasse and H A del Puerto ldquoEchocardiography of ventric-ular septal movement in Wolff-Parkinson-White syndromerdquoArchivos del Instituto de Cardiologia de Mexico vol 46 no 4pp 445ndash450 1976
[7] J P Boineau J F Moore and W C Sealy ldquoBasis of clinicalECG variations in right and left ventricular pre-excitation Aunitary concept of WPWrdquo in Cardiac Arrhythmias The 25thHahnemann Symposium Grune and Stratton New York NYUSA 1973
[8] F E A U ten Cate M A Kruessell K Wagner et al ldquoDilatedcardiomyopathy in children with ventricular preexcitationthe location of the accessory pathway is predictive of thisassociationrdquo Journal of Electrocardiology vol 43 no 2 pp 146ndash154 2010
[9] G Fazio M Mongiovi L Sutera G Novo S Novo and SPipitone ldquoSegmental dyskinesia inWolff-Parkinson-White syn-drome a possible cause of dilatative cardiomyopathyrdquo Interna-tional Journal of Cardiology vol 123 no 2 pp e31ndashe34 2008
[10] J Cadrin-Tourigny A Fournier G Andelfinger and P KhairyldquoSevere left ventricular dysfunction in infants with ventricularpreexcitationrdquo Heart Rhythm vol 5 no 9 pp 1320ndash1322 2008
[11] B S Kwon E J Bae G B Kim C I Noh J Y Choi and YS Yun ldquoSeptal dyskinesia and global left ventricular dysfunc-tion in pediatric Wolff-Parkinson-White syndrome with septalaccessory pathwayrdquo Journal of Cardiovascular Electrophysiologyvol 21 no 3 pp 290ndash295 2010
[12] M Tomaske J Janousek V Razek et al ldquoAdverse effects ofWolff-Parkinson-White syndrome with right septal or pos-teroseptal accessory pathways on cardiac functionrdquo Europacevol 10 no 2 pp 181ndash189 2008
[13] L V A Boersma E Garcıa-Moran L Mont and J BrugadaldquoAccessory pathway localization by QRS polarity in childrenwith Wolff-Parkinson-White syndromerdquo Journal of Cardiovas-cular Electrophysiology vol 13 no 12 pp 1222ndash1226 2002
[14] S Cazeau P Bordachar G Jauvert et al ldquoEchocardiographicmodeling of cardiac dyssynchrony before and during multisitestimulation a prospective studyrdquo Pacing and Clinical Electro-physiology vol 26 no 1 pp 137ndash143 2003
[15] M V Pitzalis M Iacoviello R Romito G Luzzi M Anaclerioand C Forleo ldquoRole of septal to posterior wall motion delayin cardiac resynchronization therapyrdquo Journal of the AmericanCollege of Cardiology vol 48 no 3 pp 596ndash597 2006
[16] J J Bax T H Marwick S G Molhoek et al ldquoLeft ventriculardyssynchrony predicts benefit of cardiac resynchronizationtherapy in patients with end-stage heart failure before pace-maker implantationrdquo The American Journal of Cardiology vol92 no 10 pp 1238ndash1240 2003
[17] N B Schiller ldquoTwo-dimensional echocardiographic determi-nation of left ventricular volume systolic function and massSummary and discussion of the 1989 recommendations of theAmerican society of echocardiographyrdquo Circulation vol 84 no3 pp I280ndashI287 1991
[18] WA ZoghbiM Enriquez-Sarano E Foster et al ldquoRecommen-dations for evaluation of the severity of native valvular regur-gitation with two-dimensional and doppler echocardiographyrdquoJournal of the American Society of Echocardiography vol 16 no7 pp 777ndash802 2003
[19] E Abergel ldquoEchocardiographic indices of diastolic function putto the practical testrdquo Archives des Maladies du Coeur et desVaisseaux vol 98 no 4 pp 325ndash330 2005
[20] C J McMahon S F Nagueh R H Pignatelli et al ldquoCharac-terization of left ventricular diastolic function by tissue dopplerimaging and clinical status in children with hypertrophic car-diomyopathyrdquo Circulation vol 109 no 14 pp 1756ndash1762 2004
[21] P Rumeau P Acar S Paranon et al ldquoEvaluation of left ventric-ular diastolic function in children by doppler tissue imagingrdquoArchives des Maladies du Coeur et des Vaisseaux vol 100 no 5pp 405ndash410 2007
[22] M Emmel S Balaji andN Sreeram ldquoVentricular preexcitationassociated with dilated cardiomyopathy a causal relationshiprdquoCardiology in the Young vol 14 no 6 pp 594ndash599 2004
[23] B W Eidem C J McMahon R R Cohen et al ldquoImpactof cardiac growth on doppler tissue imaging velocities astudy in healthy childrenrdquo Journal of the American Society ofEchocardiography vol 17 no 3 pp 212ndash221 2004
[24] P P Karpawich ldquoChronic right ventricular pacing and cardiacperformance The pediatric perspectiverdquo Pacing and ClinicalElectrophysiology vol 27 no 6 pp 844ndash849 2004
[25] A S Manolis ldquoThe deleterious consequences of right ventricu-lar apical pacing time to seek alternate site pacingrdquo Pacing andClinical Electrophysiology vol 29 no 3 pp 298ndash315 2006
[26] M V T Tantengco R L Thomas and P P Karpawich ldquoLeftventricular dysfunction after long-term right ventricular apicalpacing in the youngrdquo Journal of the American College ofCardiology vol 37 no 8 pp 2093ndash2100 2001
BioMed Research International 7
[27] M R Bristow L A Saxon J Boehmer et al ldquoCardiac-resyn-chronization therapy with or without an implantable defibrilla-tor in advanced chronic heart failurerdquoTheNew England Journalof Medicine vol 350 no 21 pp 2140ndash2150 2004
[28] J G F Cleland J Daubert E Erdmann et al ldquoThe effect ofcardiac resynchronization on morbidity and mortality in heartfailurerdquo The New England Journal of Medicine vol 352 no 15pp 1539ndash1549 2005
[29] F W Prinzen E C Cheriex T Delhaas et al ldquoAsymmetricthickness of the left ventricular wall resulting from asyn-chronous electric activation a study in dogs with ventricularpacing and in patients with left bundle branch blockrdquo TheAmerican Heart Journal vol 130 no 5 pp 1045ndash1053 1995
[30] M I Cohen J K Triedman B C Cannon et al ldquoPACESHRSexpert consensus statement on the management of the asymp-tomatic young patient with a Wolff-Parkinson-White (WPWventricular preexcitation) electrocardiographic patternrdquo HeartRhythm vol 9 no 6 pp 1006ndash1024 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
after successful ablation of antegrade-conducting accessorypathways The more pronounced changes were observed inpatients with nonseptal pathways
Conflict of Interests
The authors do not have any conflict of interests with thecontent of the paper
References
[1] KHina TMurakami S Kusachi et al ldquoDecreased amplitude ofleft ventricular posterior wall motion with notch movement todetermine the left posterior septal accessory pathway in Wolff-Parkinson-White syndromerdquo Heart vol 82 no 6 pp 731ndash7391999
[2] H Hishida I Sotobata and Y Koike ldquoEchocardiographic pat-terns of ventricular contraction in the Wolff-Parkinson-Whitesyndromerdquo Circulation vol 54 no 4 pp 567ndash570 1976
[3] A N DeMaria Z Vera A Neumann and D TMason ldquoAltera-tions in ventricular contraction pattern in theWolff-Parkinson-White syndrome Detection by echocardiographyrdquo Circulationvol 53 no 2 pp 249ndash257 1976
[4] A R Ticzon A N Damato A R Caracta G Russo J R Fosterand S H Lau ldquoInterventricular septal motion during preexci-tation and normal conduction in Wolff-Parkinson-White syn-drome Echocardiographic and electrophysiologic correlationrdquoThe American Journal of Cardiology vol 37 no 6 pp 840ndash8471976
[5] G S Francis PTheroux R AOrsquoRourke ADHagan andADJohnson ldquoAn echocardiographic study of interventricular septalmotion in the Wolff-Parkinson-White syndromerdquo Circulationvol 54 no 2 pp 174ndash178 1976
[6] L Sasse and H A del Puerto ldquoEchocardiography of ventric-ular septal movement in Wolff-Parkinson-White syndromerdquoArchivos del Instituto de Cardiologia de Mexico vol 46 no 4pp 445ndash450 1976
[7] J P Boineau J F Moore and W C Sealy ldquoBasis of clinicalECG variations in right and left ventricular pre-excitation Aunitary concept of WPWrdquo in Cardiac Arrhythmias The 25thHahnemann Symposium Grune and Stratton New York NYUSA 1973
[8] F E A U ten Cate M A Kruessell K Wagner et al ldquoDilatedcardiomyopathy in children with ventricular preexcitationthe location of the accessory pathway is predictive of thisassociationrdquo Journal of Electrocardiology vol 43 no 2 pp 146ndash154 2010
[9] G Fazio M Mongiovi L Sutera G Novo S Novo and SPipitone ldquoSegmental dyskinesia inWolff-Parkinson-White syn-drome a possible cause of dilatative cardiomyopathyrdquo Interna-tional Journal of Cardiology vol 123 no 2 pp e31ndashe34 2008
[10] J Cadrin-Tourigny A Fournier G Andelfinger and P KhairyldquoSevere left ventricular dysfunction in infants with ventricularpreexcitationrdquo Heart Rhythm vol 5 no 9 pp 1320ndash1322 2008
[11] B S Kwon E J Bae G B Kim C I Noh J Y Choi and YS Yun ldquoSeptal dyskinesia and global left ventricular dysfunc-tion in pediatric Wolff-Parkinson-White syndrome with septalaccessory pathwayrdquo Journal of Cardiovascular Electrophysiologyvol 21 no 3 pp 290ndash295 2010
[12] M Tomaske J Janousek V Razek et al ldquoAdverse effects ofWolff-Parkinson-White syndrome with right septal or pos-teroseptal accessory pathways on cardiac functionrdquo Europacevol 10 no 2 pp 181ndash189 2008
[13] L V A Boersma E Garcıa-Moran L Mont and J BrugadaldquoAccessory pathway localization by QRS polarity in childrenwith Wolff-Parkinson-White syndromerdquo Journal of Cardiovas-cular Electrophysiology vol 13 no 12 pp 1222ndash1226 2002
[14] S Cazeau P Bordachar G Jauvert et al ldquoEchocardiographicmodeling of cardiac dyssynchrony before and during multisitestimulation a prospective studyrdquo Pacing and Clinical Electro-physiology vol 26 no 1 pp 137ndash143 2003
[15] M V Pitzalis M Iacoviello R Romito G Luzzi M Anaclerioand C Forleo ldquoRole of septal to posterior wall motion delayin cardiac resynchronization therapyrdquo Journal of the AmericanCollege of Cardiology vol 48 no 3 pp 596ndash597 2006
[16] J J Bax T H Marwick S G Molhoek et al ldquoLeft ventriculardyssynchrony predicts benefit of cardiac resynchronizationtherapy in patients with end-stage heart failure before pace-maker implantationrdquo The American Journal of Cardiology vol92 no 10 pp 1238ndash1240 2003
[17] N B Schiller ldquoTwo-dimensional echocardiographic determi-nation of left ventricular volume systolic function and massSummary and discussion of the 1989 recommendations of theAmerican society of echocardiographyrdquo Circulation vol 84 no3 pp I280ndashI287 1991
[18] WA ZoghbiM Enriquez-Sarano E Foster et al ldquoRecommen-dations for evaluation of the severity of native valvular regur-gitation with two-dimensional and doppler echocardiographyrdquoJournal of the American Society of Echocardiography vol 16 no7 pp 777ndash802 2003
[19] E Abergel ldquoEchocardiographic indices of diastolic function putto the practical testrdquo Archives des Maladies du Coeur et desVaisseaux vol 98 no 4 pp 325ndash330 2005
[20] C J McMahon S F Nagueh R H Pignatelli et al ldquoCharac-terization of left ventricular diastolic function by tissue dopplerimaging and clinical status in children with hypertrophic car-diomyopathyrdquo Circulation vol 109 no 14 pp 1756ndash1762 2004
[21] P Rumeau P Acar S Paranon et al ldquoEvaluation of left ventric-ular diastolic function in children by doppler tissue imagingrdquoArchives des Maladies du Coeur et des Vaisseaux vol 100 no 5pp 405ndash410 2007
[22] M Emmel S Balaji andN Sreeram ldquoVentricular preexcitationassociated with dilated cardiomyopathy a causal relationshiprdquoCardiology in the Young vol 14 no 6 pp 594ndash599 2004
[23] B W Eidem C J McMahon R R Cohen et al ldquoImpactof cardiac growth on doppler tissue imaging velocities astudy in healthy childrenrdquo Journal of the American Society ofEchocardiography vol 17 no 3 pp 212ndash221 2004
[24] P P Karpawich ldquoChronic right ventricular pacing and cardiacperformance The pediatric perspectiverdquo Pacing and ClinicalElectrophysiology vol 27 no 6 pp 844ndash849 2004
[25] A S Manolis ldquoThe deleterious consequences of right ventricu-lar apical pacing time to seek alternate site pacingrdquo Pacing andClinical Electrophysiology vol 29 no 3 pp 298ndash315 2006
[26] M V T Tantengco R L Thomas and P P Karpawich ldquoLeftventricular dysfunction after long-term right ventricular apicalpacing in the youngrdquo Journal of the American College ofCardiology vol 37 no 8 pp 2093ndash2100 2001
BioMed Research International 7
[27] M R Bristow L A Saxon J Boehmer et al ldquoCardiac-resyn-chronization therapy with or without an implantable defibrilla-tor in advanced chronic heart failurerdquoTheNew England Journalof Medicine vol 350 no 21 pp 2140ndash2150 2004
[28] J G F Cleland J Daubert E Erdmann et al ldquoThe effect ofcardiac resynchronization on morbidity and mortality in heartfailurerdquo The New England Journal of Medicine vol 352 no 15pp 1539ndash1549 2005
[29] F W Prinzen E C Cheriex T Delhaas et al ldquoAsymmetricthickness of the left ventricular wall resulting from asyn-chronous electric activation a study in dogs with ventricularpacing and in patients with left bundle branch blockrdquo TheAmerican Heart Journal vol 130 no 5 pp 1045ndash1053 1995
[30] M I Cohen J K Triedman B C Cannon et al ldquoPACESHRSexpert consensus statement on the management of the asymp-tomatic young patient with a Wolff-Parkinson-White (WPWventricular preexcitation) electrocardiographic patternrdquo HeartRhythm vol 9 no 6 pp 1006ndash1024 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 7
[27] M R Bristow L A Saxon J Boehmer et al ldquoCardiac-resyn-chronization therapy with or without an implantable defibrilla-tor in advanced chronic heart failurerdquoTheNew England Journalof Medicine vol 350 no 21 pp 2140ndash2150 2004
[28] J G F Cleland J Daubert E Erdmann et al ldquoThe effect ofcardiac resynchronization on morbidity and mortality in heartfailurerdquo The New England Journal of Medicine vol 352 no 15pp 1539ndash1549 2005
[29] F W Prinzen E C Cheriex T Delhaas et al ldquoAsymmetricthickness of the left ventricular wall resulting from asyn-chronous electric activation a study in dogs with ventricularpacing and in patients with left bundle branch blockrdquo TheAmerican Heart Journal vol 130 no 5 pp 1045ndash1053 1995
[30] M I Cohen J K Triedman B C Cannon et al ldquoPACESHRSexpert consensus statement on the management of the asymp-tomatic young patient with a Wolff-Parkinson-White (WPWventricular preexcitation) electrocardiographic patternrdquo HeartRhythm vol 9 no 6 pp 1006ndash1024 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom