Embed Size (px)
Citation preview

Research ArticleBlindness Registers as Epidemiological Tools for Public HealthPlanning: A Case Study in Belize
Sally L. Baxter,1 Richard P. Wormald,2 Joan M. Musa,3 and Daksha Patel2
1Department of Ophthalmology, the University of California San Diego Shiley Eye Center (MC 0946), 9415 Campus Point Drive,La Jolla, CA 92093, USA2International Centre for Eye Health, London School of Hygiene and Tropical Medicine, London WC1E 7HT, UK3Belize Council for the Visually Impaired, Belize City, Belize
Correspondence should be addressed to Sally L. Baxter; [email protected]
Received 23 August 2014; Revised 18 November 2014; Accepted 18 November 2014; Published 3 December 2014
Academic Editor: Leo J. Schouten
Copyright © 2014 Sally L. Baxter et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
For public eye health programs, blindness registers can be an important tool for informing service planning. This study examineshow the Belize Council for the Visually Impaired (BCVI) used its blindness register data to drive several public health interventions.Cross-sectional analysis was performed for all active registrants (𝑛 = 1194) to determine the distribution of causes of registrationaccording to age, sex, and geographical district. Cataract was the leading cause of registration (39.6%), followed by glaucoma(20.8%), diabetic retinopathy (10.2%), and childhood blindness (9.4%). The distribution of the causes of registration was fairlysimilar between men and women and across the various districts. However, in Stann Creek, whose population is largely of Africandescent, glaucoma exceeded cataract. For most causes, the majority of registrants were registered at age 50 or older. Follow-up wasconducted four years later. Several interventions had been initiated, most notably bolstering cataract surgical services and creatingscreening programs for glaucoma and diabetic retinopathy. The register itself was also improved to maximize its utility for futureuse. While standardized surveys may be the most appropriate method of estimating population-based measures such as prevalenceor incidence, the blindness register is still a valuable source of data for public health planning.
1. Introduction
Disease registers have widespread applications in medicineand public health. Traditionally they have been designedto collect clinical information on a single topic and trackpatient outcomes longitudinally over time [1]. They have alsobeen used as data sources for population-based research. Forinstance, several studies have employed blindness registers toestimate the prevalence and incidence of blindness and visualimpairment in various regions around the world, includingAustralia [2, 3], Israel [4], Singapore [5], Taiwan [6], Canada[7], Ireland [8], and England [9]. Notably, these studieshave largely been conducted in developed nations. Diseaseregisters may also drive quality improvement initiatives. Inpublic eye health, prominent examples of this include theimplementation of an eye-related indicator based on theCertificate of Vision Impairment (CVI) form by the National
Health Service in the United Kingdom, as well as the recentlyunveiled Intelligent Research in Sight (IRIS) registry by theAmerican Academy of Ophthalmology. Finally, registers canalso provide an entry point for nonmedical purposes, such asqualifying visual status to receive rehabilitation and supportservices, as well as possible financial and social benefits [9].
The World Health Organization’s (WHO) VISION 2020initiative has engendered increasing awareness of avoidableblindness, particularly in developing countries where there isa greater burden of visual impairment. This study describeshow one nonprofit organization, the Belize Council for theVisually Impaired (BCVI), used epidemiological findingsfrom a national low vision and blindness register in Belizeto inform the planning of its public eye health services.Prior to this analysis, there were virtually no publisheddata concerning the epidemiology of blindness and visualimpairment in Belize.
Hindawi Publishing CorporationEpidemiology Research InternationalVolume 2014, Article ID 659717, 8 pageshttp://dx.doi.org/10.1155/2014/659717

2 Epidemiology Research International
Belize is a small nation (population 333,200) consistingof a diverse mix of ethnic groups [10], with about one-third of the population living in poverty [11]. Eye care is notincluded in the government-sponsored healthcare system,and private ophthalmologists are unaffordable formost of thepopulation. BCVI addresses this access issue by providingaffordable primary and secondary eye care to about 12,000–15,000 patients per year in both urban and rural settings,as well as offering rehabilitation services and promoting eyehealth education and awareness, and has been recognized asan example for sustainable eye care in Latin America andthe Caribbean [12]. Since 1988, BCVI has operated a registerof patients who qualify for its rehabilitation services. Herewe analyze the BCVI register based on cause of registration,age, sex, and geographical district. These epidemiologicalfindings were then used to generate recommendations forthe organization to improve its delivery of services. Over thecourse of several years, the organization implemented severalof these recommendationswith promising results, illustratingthe role of the blindness register as a critical public healthplanning tool in eye programs.
2. Materials and Methods
The BCVI register includes patients who qualified for reha-bilitation services based on best-corrected visual acuity(BCVA) of 20/200 or less in both eyes and determinationby the referring ophthalmologist to gain no benefit fromfurther medical treatment or surgery. This analysis includespatients who were registered from 1988 until December 31,2009. The register was compiled and managed by the BCVIRehabilitation Coordinator, a role which was filled by thesame individual throughout this whole period, based onmonthly reports from the examining ophthalmologist, whovaried considerably over the years. This dataset was sentelectronically to the London School of Hygiene and TropicalMedicine (LSHTM), where the analysis was performed.
For each registered patient, data used included sex, age,district of residence, visual acuity in each eye, level of visualimpairment (see Table 1), extent of rehabilitation needed, andprimary cause of registration. Causes of registration were cat-egorized into the WHO’s priority disease categories of visualimpairment: cataract, glaucoma, diabetic retinopathy, age-related macular degeneration (AMD), childhood blindness,and uncorrected refractive error. Causes of registration thatdid not fall into one of these categories were designated as“other.” For patient confidentiality, names and addresses wereremoved from the dataset, and the file was given passwordprotection. This study received ethical approval from theethical review committee at LSHTM and was performedin compliance with the Declaration of Helsinki. Univariateanalyses were performed examining causes of registration byage, sex, and district using STATA 11.
Based on the results of these analyses, recommendationswere generated to help BCVI optimize service delivery.Follow-up with the organization was conducted approx-imately four years after the original analysis to evaluatewhat interventions had been performed and assess how
Table 1: WHO levels of visual impairment.
Category Worse than Equal to or betterthan
Mild or no visualimpairment
6/183/10 (0.3)20/70
Moderate visualimpairment
6/18 6/603/10 (0.3) 1/10 (0.1)20/70 20/200
Severe visualimpairment
6/60 3/601/10 (0.1) 1/20 (0.05)20/200 20/400
Blindness3/60
No light perception1/20 (0.05)20/400
Categories of visual impairment were defined according to the WorldHealth Organization (WHO) International Classification of Diseases (ICD-10) based on presenting distance visual acuity in the better eye.
the epidemiological findings gleaned from the blindness reg-ister had influenced the organization’s public health impact.
3. Results and Discussion
As of December 31, 2009, 1194 persons were listed on theBCVI register. Characteristics of the study population arepresented in Table 2. The registrants were about equally splitbetween men (48.9%) and women (51.1%). Most (62.3%) metthe WHO criterion for blindness. The majority (64.4%) were50 years old or older at the time of registration. The highestproportion of registrants (35.8%) claimed Belize district astheir district of residence.
Cataract was by far the leading cause of registration,accounting for 39.6% of all registrants, followed by glau-coma, which accounted for 20.8% (see Table 2). Other majorcauses of registration for blindness and visual impairmentwere diabetic retinopathy (10.2%) and childhood blindness(9.4%), a categorywhich included retinopathy of prematurity,congenital cataracts, congenital glaucoma, and any cornealor retinal pathology in individuals under the age of 15. Age-related macular degeneration (AMD) accounted for 1.2%of the register and refractive error only 0.6%. Causes ofblindness in the register that did not fall under one of theWHO’s priority disease categories were grouped under a sep-arate category designated as “other” causes. Taken together,these accounted for 18.2% of the register. The most commondiagnosis within this category was trauma, representing 2.3%of the entire register, while other conditions included tumorsand retinal pathologies such as retinitis pigmentosa. Besidestrauma, none of the other individual causeswithin the “other”category exceeded 0.5% of the register.
The registration patterns for men and for women weresimilar (Table 2). The majority of individuals were registeredat the age of 50 or older for most causes, reflecting the age-related pathophysiology of many eye diseases. Cataract and

Epidemiology Research International 3
Table 2: Causes of registration for blindness and low vision rehabilitation by the Belize Council for the Visually Impaired (BCVI) based ondata from all actively registered individuals (𝑛 = 1194) as of December 31, 2009.
CataractNumber(%)
GlaucomaNumber(%)
DiabeticretinopathyNumber (%)
ChildhoodblindnessaNumber (%)
Age-relatedmacular
degenerationNumber (%)
Uncorrectedrefractiveerror
Number (%)
OtherbNumber (%)
TotalcNumber (%)
Overall 472 (39.6) 248 (20.8) 121 (10.2) 112 (9.4) 14 (1.2) 7 (0.6) 217 (18.2) 1191 (100)Gender
Male 232 (39.9) 135 (23.2) 36 (6.2) 58 (10.0) 4 (0.7) 2 (0.3) 115 (19.8) 582 (100)Female 240 (39.4) 113 (18.6) 85 (14.0) 54 (8.9) 10 (1.6) 5 (0.8) 102 (16.8) 610 (100)
Age atregistration
0–4 4 (4.1) 10 (10.2) 0 (0) 64 (65.3) 0 (0) 0 (0) 20 (20.4) 98 (100)5–15 8 (8.8) 9 (9.9) 2 (2.2) 41 (45.1) 1 (1.1) 4 (4.4) 26 (28.6) 91 (100)16–39 18 (16.4) 15 (13.6) 15 (13.6) 6 (5.5) 0 (0) 2 (1.8) 54 (49.1) 110 (100)40–49 44 (35.5) 34 (27.4) 18 (14.5) 0 (0) 1 (0.8) 0 (0) 27 (21.8) 124 (100)50+ 398 (51.9) 180 (23.5) 85 (11.1) 1 (0.1) 12 (1.6) 1 (0.1) 90 (11.7) 767 (100)
District ofresidence
Belize 142 (33.3) 120 (28.2) 50 (11.7) 35 (8.2) 9 (2.1) 1 (0.2) 69 (16.2) 426 (100)Cayo 80 (41.0) 31 (15.9) 18 (9.2) 19 (9.7) 0 (0) 0 (0) 47 (24.1) 195 (100)Corozal 67 (51.9) 15 (11.6) 18 (14.0) 13 (10.1) 0 (0) 0 (0) 16 (12.4) 129 (100)Orange Walk 69 (39.2) 37 (21.0) 16 (9.1) 15 (8.5) 1 (0.6) 4 (2.3) 34 (19.3) 176 (100)Stann Creek 23 (19.8) 30 (25.9) 17 (14.7) 15 (12.9) 2 (1.7) 2 (1.7) 27 (23.3) 116 (100)Toledo 91 (61.1) 15 (10.1) 2 (1.3) 15 (10.1) 2 (1.3) 0 (0) 24 (16.1) 149 (100)
a“Childhood blindness” includes congenital cataract, congenital glaucoma, retinopathy of prematurity, and any entity designed as “corneal” or “retinal” in thoseunder the age of 15.bThe “other” designation includes trauma, tumor, uveitis, retinal detachment, retinitis pigmentosa, and other corneal and retinal pathologies in individualsover the age of 15.cTotals do not match the overall total study population number due to missing data.
glaucomawere the two leading causes of registration for indi-viduals over the age of 40. Most of those listed with glaucomawere in their late 40s and above. Similarly, registrations fordiabetic retinopathy occurred for individuals predominantlyover the age of 50. These are chronic conditions that arebest managed with early detection, suggesting that a goalof earlier registration would be appropriate. For the 15-year-olds and under group, childhood blindness was the maincause of registration, with 57% aged 0 to 4 years at the timeof registration. Children on the register should ideally getappropriate support and rehabilitation, and the earlier this ispossible the better.
The causes of registration were fairly consistent across thedifferent districts. Cataract was most commonly listed as thecause of registration in all districts except Stann Creek, thedistrict of Belize with the highest proportion of populationof African descent, where glaucoma was the leading cause.Childhood blindness comprised approximately 10% of theregistrations within each district.
Based on these results, we proposed several recommen-dations to BCVI, regarding both the distribution of diseaseburden (Table 3) and how to improve the register itself(Table 4).
In response to these recommendations, BCVI beganseveral significant interventions within only four years. A fewkey interventions will be highlighted here.
3.1. Cataract. Cataract was the leading cause of registration atall levels of visual impairment. In theory, cataract should notbe listed as a cause of permanent blindness at all because it is atreatable condition. However, the fact that it is identified hereas themost commonly listed cause of registration emphasizesthe ongoing burden of cataract which outstrips the avail-ability and access to services. Cataract therefore remains apressing public health challenge, particularly in a nation withlimited resources and equity in service provision across allsocioeconomic groups, such as Belize. Because it is typicallycorrectable by surgery, its prominence among those individ-uals qualifying for rehabilitation services suggests that theremay be limited availability of eye services and specificallysurgical services. BCVI recognized the inadequacy of cataractsurgical services in Belize early on; that recognition was whatsparked the creation of their cataract surgery program in2000. Since the analysis of the register, they have recruitedmore personnel. In addition to an ophthalmologist from theUS who has been operating 4-5 months annually for many

4 Epidemiology Research International
Table 3: Key results based on data from the current BCVI register, their implications, and subsequent recommendations.
Result Implication(s) Recommendation(s)
Large disease burdenin the over-50 agegroup
Improved case detection andservice provision for olderindividuals are needed
(i) Publicize awareness of BCVI services among the community, generalpractitioners and other healthcare professionals, and nursing homes or elderlycare centers(ii) Establish strong referral networks for all districts
Cataract is the leadingcause of registrationfor low vision andblindness
May potentially be due toinadequate cataract surgicalcoverage
(i) Recruit more ophthalmologists to join BCVI if possible or increase surgicalrates of current ophthalmologists(ii) Monitor cataract surgical rates and outcomes(iii) Provide outreach services to all districts on a regular and sustainable basis(iv) Provide early and easier access to cataract surgical services
Relatively lateregistration fordiabetic retinopathy,glaucoma, andchildhood blindness
More effective early detectionand improved referral systemsare needed since these aremanageable conditions
(i) Institute screening programs for diabetic retinopathy and glaucoma andcoordinate with general practitioners treating high risk patients(ii) Collaborate with pediatricians, nurseries, preschools, and elementaryschools to promote early detection of childhood blindness and improve schoolvision health programs
years, they recently recruited an additional ophthalmologistfrom Cuba who works on a part-time basis throughout theyear. Additionally, several ophthalmologists volunteer on ashort-term basis, including two cataract teams from the USwho operate for about 1 week each annually.
In Belize, there are no ophthalmology residency train-ing programs in the country. Therefore the country cur-rently depends on recruiting ophthalmologists who havebeen trained elsewhere. Based on a study on the globalophthalmology workforce conducted by the InternationalCouncil of Ophthalmology [13], in 2010 there were 10practicing ophthalmologists in Belize, equivalent to about32 ophthalmologists per million population. There were noophthalmology residents in training. By comparison, duringthat same year in the UK there were 52 ophthalmologists permillion with 700 residents in training, while in the US therewere 81 ophthalmologists per million with 1350 residentsin training. However, Belize’s workforce slightly exceeds theglobal average of 31 ophthalmologists permillion.The issue ofan adequate ophthalmology workforce is a widespread issueamong numerous developing nations. Belize benefits fromgeographical proximity to theUS andCaribbean nationswitha greater supply of medical training programs, as well asfrom historical ties to the United Kingdom. However, in theabsence of resources to establish comprehensive postgraduateophthalmology training programs, the focus has been onrecruiting talent from abroad and on maximizing the use ofancillary staff such as optometrists, ophthalmic technicians,visual rehabilitation specialists, and administrative assistants.
Besides increasing personnel to address surgical vol-ume, BCVI has also reduced the visual acuity criterionfor cataract extraction from 20/100 to 20/30 and maintainsactive lists (separate from the register) to keep track ofpatients who need cataract surgery so they are not incorrectlylisted on the blindness register for rehabilitation. Startingin 2013, they have also begun measuring preoperative andpostoperative visual acuity to gauge the clinical outcomesof their cataract surgery program. In addition, they haveimplemented outreach services through their primary eyecare clinics via a surgical coordinator to provide easier access
to surgical services andmeet patient needs at the district level.These changes signify progress toward addressing avoidableblindness caused by untreated cataract in this country.
3.2. Glaucoma. Stann Creek was the only district in whichglaucoma exceeded cataract as the top cause of registration.Garifunas, people of African descent, make up the highestproportion of this district’s population [10]. The increasedrisk of primary open-angle glaucoma among those of Africandescent is well documented [14–17]. Because of the morerapid progression [18] and earlier appearance of glaucoma inthose of African descent [19], screening should be initiatedearlier than in other populations. Ethnicity was not recordedon the register by BCVI. In theory this information wouldhave helped illuminate how causes of registration may havevaried by ethnic group and identify high risk individuals.However, in practice BCVI found it was very difficult tocollect this information because so many of their patientscome from mixed ethnic backgrounds and could not clearlyidentify themselves with any one single ethnic group.
Nevertheless, in response to this finding BCVI began acommunity awareness program in the Stann Creek district,going to each village with an educational video, conductingcommunity meetings, and then conducting clinics to identifyhigh risk individuals for earlier glaucoma assessment. Whilenot enough time has elapsed to tell whether these communityengagement activities will actually translate into decreasedincidence of blindness due to end-stage uncontrolled glau-coma, they are definitely a step in the right direction.
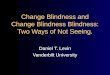
3.3. Diabetic Retinopathy. Because the register had alertedBCVI to diabetic retinopathy as an increasingly commoncomplication over time (Figure 1), in the subsequent yearsafter this analysis, BCVI has taken steps to initiate anew national diabetic retinopathy screening program. Withfunding from Project Alliance International and the LionsClub International Foundation, they have purchased threeportable fundus cameras to be placed at different clinicsites throughout the country. They have also employed twoadditional ophthalmic assistants to take the photos and grade

Epidemiology Research International 5
Table4:Po
tentialareas
ofim
provem
entfor
theB
elize
Cou
ncilforthe
VisuallyIm
paire
d(BCV
I)registe
r.
Gap
Descriptio
nRe
commendatio
n(s)
Organization/staffi
ngRe
spon
sibilitiesfor
ther
egister
ares
plitbetweenmultip
lesta
ffpo
sitions,and
person
nelh
avem
anyotherd
emands
thattake
precedence
over
ther
egister
(i)Inclu
deregiste
rmaintenance
andup
datin
gin
descrip
tions
ofstaff
positions
andcontracts
(ii)D
evelo
paformalandexplicitsyste
mforh
owther
espo
nsibilitie
sfor
ther
egister
will
bedividedandpu
taccou
ntabilitychecks
inplace
(iii)Trainperson
neltocarryou
tregular
datacle
aningchecks
Registe
rmaintenance
Errorsandinconsistencies
indataentryandlack
offollow-upon
patie
ntstatus
(i.e.,
ifreferred
totre
atmento
rsurgery)
(i)Develo
paformalfollo
w-upprocessfor
updatin
gther
egister
with
settim
elines
(ii)C
onsid
erlin
king
ther
egister
with
othersou
rces
ofinform
ation(i.e.,
clinics,the
patie
ntrecordsd
atabase,theB
elizeH
ealth
Inform
ationSyste
m,m
ortalityrecords,etc.)
Incompletec
overage
ofthep
opulation
Theregister
may
potentially
miss
manyind
ividualssufferin
gfro
mlowvisio
nandblindn
ess,inclu
ding
thosew
house
privated
octorsandthoseinremotea
reas
ofthec
ountry
(i)Prom
otea
warenesso
fBCV
Iand
registratio
nin
thec
ommun
ity(clin
ics,grocerysto
res,
churches,and
scho
ols)to
boostreferrals
(ii)B
uild
morer
elationships
with
privateo
phthalmologiststobo
osttheirreferrals
(iii)Con
ductmoreo
utreachclinics
toreachremote/marginalized
commun
ities
(iv)P
rovide
professio
naltrainingforo
phthalmologistso
nho
wto
completethe
registe
rusingcle
ardefin
ition
sand
criteria
Collectingrelevant
varia
bles
Somek
eyvaria
bles
regardingthes
ociald
eterminantsof
health
arem
issing
(i)Collectinform
ationon
ethn
icity,socioecon
omicstatus,and
resid
ence
with
inan
urbanor
ruralsettin
gfora
llnewregistrants
Cod
ing
Cod
ingof
somev
ariables
isno
talignedwith
categorie
sthat
arew
idely
inusee
lsewhere
(i)Cod
ethe
levelofvisu
alim
pairm
entand
thec
ause
ofregistratio
naccordingto
criteria
set
bytheW
orld
Health
Organization(W
HO)inordertoallowfore
asierc
ross-com
paris
onandcontextualanalysisin
thefuture
Registr
ationprocess
Individu
alsw
ithavoidableb
lindn
essa
relistedon
the
registe
rfor
rehabilitationandsupp
ortservicesw
henthey
shou
ldbe
referred
totre
atmentinstead
(i)Ev
aluatepatientso
nthec
urrent
registe
rand
referthem
totre
atmentifapp
licable(i.e.,
for
cataract);ifalltreatmentfails,
then
keep
them
onther
egister
forrehabilitatio
n
Publicizingresults
Repo
rtsfrom
BCVId
atag
oto
fund
ersb
utaren
otinclu
ded
inthep
ublic
domain,
andresults
aren
otwidely
dissem
inated
(i)Ad
vocateforthe
inclu
sionof
datafro
mther
egister
inBe
lize’s
compilatio
nof
natio
nal
health
statistics
(ii)S
endresults
from
analyses
ofregiste
rdatatotheW
HOandtheP
anAmerican
Health
Organization(PAHO)sothatdatafro
mBe
lizew
illbe
inclu
dedin
theirreports

6 Epidemiology Research International
Year of registration
0
5
10
15
20
25
30
35
40
45
50
Num
ber o
f peo
ple r
egist
ered
with
dia
betic
retin
opat
hy
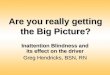
1988–1989 1990–1994 1995–1999 2000–2004 2005–2009
Figure 1: Trends in registration of blindness and low vision due todiabetic retinopathy in Belize.
them to determine whether the screened individual requiresfollow-up with an ophthalmologist. At the time of this report,the program is not yet fully operational but a training sessionhas already been scheduled with faculty from Brighton andSussex University Hospital in the United Kingdom. The goalof this program is to detect patients with diabetic retinopathyand initiate treatment at an earlier stage, thereby reducingavoidable blindness and ideally decreasing the number ofpeople listed on the blindness register with this disease in thecoming years.
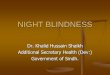
3.4. Retinopathy of Prematurity (ROP). This analysis deter-mined that childhood blindness was an important cause ofblindness in Belize, and upon further investigation BCVIfound that there was a markedly increased incidence ofbilateral blindness secondary to ROP between 2007 and 2009(Figure 2). Each case was followed up by BCVI’s Rehabilita-tion Field Officers, and the suspected cause was unmonitoredexcess oxygenation in preterm infants. Once this cluster ofcases was identified, the lead BCVI ophthalmologist alertedthe staff at the one referral pediatric neonatal intensive careunit (NICU) located at the Karl Heusner Memorial Hospitalin Belize City, the only NICU in the country. Two trainingsessions, one in 2009 and one in 2011, were conducted withneonatologists, pediatricians, and NICU nurses focusing onoxygen usage, monitoring of premature infants, and ROPprevention. Subsequently, between 2010 and 2012, BCVIreported that only one case of ROP had been registered.While it would be difficult to prove that the decrease inincidence was caused by this intervention, nevertheless itis an illustration of how data provided in the register wereused to drive a public health intervention and an educationalcampaign aimed not at treatment but at prevention of adebilitating disease.
3.5. Improvements to the Low Vision and Blindness Register.BCVI also made several changes to the register itself inline with these recommendations in order to improve theirservices. One issue was potential ambiguity surrounding
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Year of registration
0
2
4
6
8
10
12
14
Num
ber o
f chi
ldre
n re
giste
red
with
retin
opat
hy o
f pre
mat
urity
Figure 2: Trends in registration of blindness and low vision due toretinopathy of prematurity in Belize.
the exact diagnosis causing blindness. This was particularlytrue if the patient suffered from multiple eye conditions. Forexample, upon review of themedical charts, BCVI found thatseveral individuals were listed as “cataract” in the registerbecause that was the first diagnosis on their problem listat the most recent clinic visit, when in reality they hadsubsequently had the cataract removed and were actuallyblind from another cause such as glaucoma or diabeticretinopathy. This may have overestimated the amount ofblindness caused by cataract and underestimated the amountof blindness caused by glaucoma and diabetic retinopathy.This reemphasizes the need for accurate registration sincecataract is operable, but glaucoma and diabetic retinopathycause visual impairment that is potentially avoidable withearly detection and management but is irreversible if allowedto progress. In addition, BCVI changed their coding practicesso that instead of haphazard entry of diagnoses they arenow using the WHO ICD-10 codes. They have gone back totheir clinic records to update much of the register and assignaccurate diagnoses. This will help streamline future analysesand will be conducive to ongoing monitoring and evaluation.
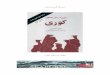
Looking at the number of new registrations longitudinally(Figure 3), the overall trend indicates a gradual increaseover time, although there were substantial variations. Thesteepest increase occurred after 2006, with the largest singleincrease in the number of new registrations occurring in2009. Starting in 2009, BCVI began making special effortsto increase awareness of the register among the clinics tofacilitate identification and registration of new patients whoqualified for rehabilitation services. In addition, numerousefforts were made to follow up on individuals who werealready registered and update the register by removingpatients who had received vision-restoring treatment, movedout of Belize, or died. In the years since this analysis wasperformed, BCVI has continued to work aggressively tomaximize the register’s coverage of the population and ensureit is as updated as possible. This will improve data accuracyand better inform public health interventions in the future.
3.6. Challenges and Limitations. Thedata used to describe thedistribution of causes of blindness and visual impairment in

Epidemiology Research International 7
1977
1991
1996
2001
2006
Year
0
50
100
150
200
250
300
350
Num
ber o
f new
regi
strat
ions
Figure 3: Longitudinal trends in the number of new registrationsfor blindness and low vision in Belize.
this study were not generated from a planned research studywith unbiased sampling procedures and standardized proce-dures and protocols. They were drawn from a community-based source capturing only those patients who interfacedwith their clinics, thereby introducing potential bias inrepresenting the country’s population as a whole. Given thelack of accurate information regarding population coverage,an accurate estimate of country-wide prevalence or incidencebased on the BCVI register would be difficult to achieve.Population-based studies using standardized data collectionmethods would be helpful in the future for generating theseestimates.
While in some respects this lack of epidemiological rigormay be a limitation, in other respects this is a more accuraterepresentation of “real” public health practice, especially in adeveloping setting with limited or scarce resources. Further-more, the process of identifying some of the shortcomingsin the data collection process itself is a useful exercise tofuel ongoing improvement for the future. While the specificfindings may be local in scope, the overall principles can beapplied on a national scale, and this case study illustrates howdata fromblindness registers, even if not themost precise, canstill drive significant public health interventions.
4. Conclusions
This study illustrates the value of blindness registers not onlyfor day-to-day operational or management purposes (e.g.,tracking of patients requiring rehabilitation services), but alsofor providing data on local disease patterns that can informquality improvement initiatives in the long termplanning anddelivery of healthcare services. Avoidable blindness, that is,blindness that is theoretically curable (such as cataract andrefractive errors) or at least manageable with early detection(such as glaucoma and diabetic retinopathy), remains animportant issue in Belize as well as in Latin America and theCaribbean in general, a finding that has been highlighted byseveral other surveys in this region [12, 20–23].
Cataract is the leading cause of registration, emphasizingthe ongoing need to bolster surgical services in this region.
Globally, cataract remains the leading cause of visual impair-ment in all regions of the world, except in themost developedcountries [24]. Glaucoma and diabetic retinopathy are alsocommon causes of blindness, illustrating the need for robustearly detection programs that may help mitigate some ofthe visual impairment caused by these diseases when theyprogress untreated.This study also highlights the importanceof accurate coding, regular updates and maintenance, andworking toward maximal population coverage when operat-ing a disease register to maximize its utility. Despite some oftheir limitations in data quality, blindness registers can stillserve as incredibly useful tools in informing public healthplanning.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
Acknowledgments
The authors’ gratitude goes to the Marshall Commission forresearch and travel funding for the purposes of completingthis project. This study has been presented at the 9th GeneralAssembly of the International Agency for the Prevention ofBlindness, the 22nd Congress of the International Societyfor Geographical and Epidemiological Ophthalmology, theChildren’s Hospital of Philadelphia 4th Annual PediatricGlobal Health Symposium, and the 2012 Unite for SightGlobal Health and Innovation Conference.
References
[1] J. Goldberg, H. M. Gelfand, and P. S. Levy, “Registry evaluationmethods: a review and case study,” Epidemiologic Reviews, vol.2, pp. 210–220, 1980.
[2] R. L. Cooper, “Blind registrations in Western Australia: a five-year study,”Australian and New Zealand Journal of Ophthalmol-ogy, vol. 18, no. 4, pp. 421–426, 1990.
[3] V. K. Yong, W. H. Morgan, R. L. Cooper et al., “Trends inregistered blindness and its causes over 19 years in WesternAustralia,” Ophthalmic Epidemiology, vol. 13, no. 1, pp. 35–42,2006.
[4] M. D. Farber, “National registry for the blind in Israel: Estima-tion of prevalence and incidence rates and causes of blindness,”Ophthalmic Epidemiology, vol. 10, no. 4, pp. 267–277, 2003.
[5] K.H. Lim, “Registration of newblindness in Singapore for 1985–1995,” SingaporeMedical Journal, vol. 39, no. 3, pp. 104–106, 1998.
[6] I. L. Tsai, L. C. Woung, C. Y. Tsai et al., “Trends in blind andlow vision registrations in Taipei City,” European Journal ofOphthalmology, vol. 18, no. 1, pp. 118–124, 2008.
[7] A. E. Macdonald, “Causes of blindness in Canada: an analysisof 24,605 cases registered with the Canadian National Institutefor the Blind,”CanadianMedical Association journal, vol. 92, pp.264–279, 1965.
[8] C. Kelliher, D. Kenny, and C. O’Brien, “Trends in blind regis-tration in the adult population of the Republic of Ireland 1996–2003,” British Journal of Ophthalmology, vol. 90, no. 3, pp. 367–371, 2006.

8 Epidemiology Research International
[9] M. E. Brennan and E. G. Knox, “An investigation into thepurposes, accuracy, and effective uses of the Blind Register inEngland,” British Journal of Preventive and Social Medicine, vol.27, no. 3, pp. 154–159, 1973.
[10] Statistical Institute of Belize, Abstract of Statistics, StatisticalInstitute of Belize, Belmopan, Belize, 2009.
[11] 2009 Country Poverty Assessment, Committee NHDA, 2010.[12] J. C. Silva, J. B. Bateman, and F. Contreras, “Eye disease and care
in Latin America and the Caribbean,” Survey of Ophthalmology,vol. 47, no. 3, pp. 267–274, 2002.
[13] S. Resnikoff,W. Felch, T.-M. Gauthier, and B. Spivey, “The num-ber of ophthalmologists in practice and training worldwide: agrowing gap despite more than 200,000 practitioners,” BritishJournal of Ophthalmology, vol. 96, no. 6, pp. 783–787, 2012.
[14] A. Sommer, J. M. Tielsch, J. Katz et al., “Racial differences in thecause-specific prevalence of blindness in East Baltimore,” TheNew England Journal of Medicine, vol. 325, no. 20, pp. 1412–1417,1991.
[15] C. A. Girkin, “Primary open-angle glaucoma in African Amer-icans,” International Ophthalmology Clinics, vol. 44, no. 2, pp.43–60, 2004.
[16] L. Racette, M. R. Wilson, L. M. Zangwill, R. N. Weinreb, and P.A. Sample, “Primary open-angle glaucoma in blacks: a review,”Survey of Ophthalmology, vol. 48, no. 3, pp. 295–313, 2003.
[17] J. M. Tielsch, A. Sommer, J. Katz, R. M. Royall, H. A. Quigley,and J. Javitt, “Racial variations in the prevalence of primaryopen-angle glaucoma. The Baltimore eye survey,” Journal of theAmericanMedical Association, vol. 266, no. 3, pp. 369–374, 1991.
[18] H. A. Quigley, “Number of people with glaucoma worldwide,”British Journal of Ophthalmology, vol. 80, no. 5, pp. 389–393,1996.
[19] R. Wilson, T. M. Richardson, E. Hertzmark, and W. M. Grant,“Race as a risk factor for progressive glaucomatous damage,”Annals of Ophthalmology, vol. 17, no. 10, pp. 653–659, 1985.
[20] B. Munoz and S. K. West, “Blindness and visual impairment intheAmericas and theCaribbean,”British Journal ofOphthalmol-ogy, vol. 86, no. 5, pp. 498–504, 2002.
[21] Pan American Health Organization and WHO, Strategic Planfor Vision 2020: The Right to Sight—Caribbean Region. Wash-ington, D.C. and Barbados, 2002.
[22] H. Limburg, F. B. Von-Bischhoffshausen, P. Gomez, J. C.Silva, and A. Foster, “Review of recent surveys on blindnessand visual impairment in Latin America,” British Journal ofOphthalmology, vol. 92, no. 3, pp. 315–319, 2008.
[23] J. M. Furtado, V. C. Lansingh, M. J. Carter et al., “Causes ofblindness and visual impairment in Latin America,” Survey ofOphthalmology, vol. 57, no. 2, pp. 149–177, 2012.
[24] S. Resnikoff, D. Pascolini, D. Etya’ale et al., “Global data onvisual impairment in the year 2002,”Bulletin of theWorldHealthOrganization, vol. 82, no. 11, pp. 844–851, 2004.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com