Embed Size (px)
Citation preview
Journal of Plastic, Reconstructive & Aesthetic Surgery (2009) 62, 800e805
Reconstruction of skin defects after resection ofsevere gluteal hidradenitis suppurativa withfasciocutaneous flaps
Kazuo Kishi a,*, Hideo Nakajima a, Nobuaki Imanishi b
a Department of Plastic and Reconstructive Surgery, Keio University School of Medicine, 35 Shinanomachi,Shinjuku-ku, Tokyo 160-8582, Japanb Department of Anatomy, Keio University School of Medicine, 35 Shinanomachi, Shinjuku-ku, Tokyo 160-8582, Japan
Received 15 March 2007; accepted 19 September 2007
KEYWORDSHidradenitissuppurativa;Fasciocutaneous flap;Gluteal
* Corresponding author. Tel.: þ81 31054.
E-mail address: [email protected].
1748-6815/$-seefrontmatterª2008Bridoi:10.1016/j.bjps.2007.09.063
Summary Background: Although skin grafting after resection of the hidradenitis suppurativais frequently used, the contour after skin grafting is unsatisfactory. We studied four patientswho suffered from severe gluteal hidradenitis suppurativa and needed total skin resectionof the affected lesion.Methods: Reconstruction after total skin resection was performed with fasciocutaneous (FC)flaps of three different designs based on an arterial anatomical study: an island V-Y advance-ment flap based on the descending branch of the inferior gluteal artery; a rotation V-Y ad-vancement flap based on the first perforator of the deep femoral artery and the descendingbranch of the inferior gluteal artery; and, a bilobed flap at each lobe containing either the des-cending branch or medial branch of the inferior gluteal artery. The flap designs were decidedfrom the size and the location of the skin defect.Results: The contours after reconstruction were satisfactory and did not experience any recur-rence of hidradenitis suppurativa for at least 1 year after operation.Conclusion: We showed three different designs of FC flaps to cover the gluteal skin defectsbased on the anatomical study. FC flaps may be chosen for reconstruction after resection ofperianal hidradenitis suppurativa.ª 2008 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Publishedby Elsevier Ltd. All rights reserved.
5363 3814; fax: þ81 3 3352
ac.jp (K. Kishi).
tishAssociationofPlastic,Reconstruc
Hidradenitis suppurativa is a recurrent, chronic inflamma-tory disease with complications such as abscesses, sinustract formations, fistulisation, and scarring.1 Although theetiology of hidradenitis suppurativa is still unknown, occlu-sions of apocrine glands are observed histologically. Also,the skin where apocrine glands do not exist does not usually
tiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

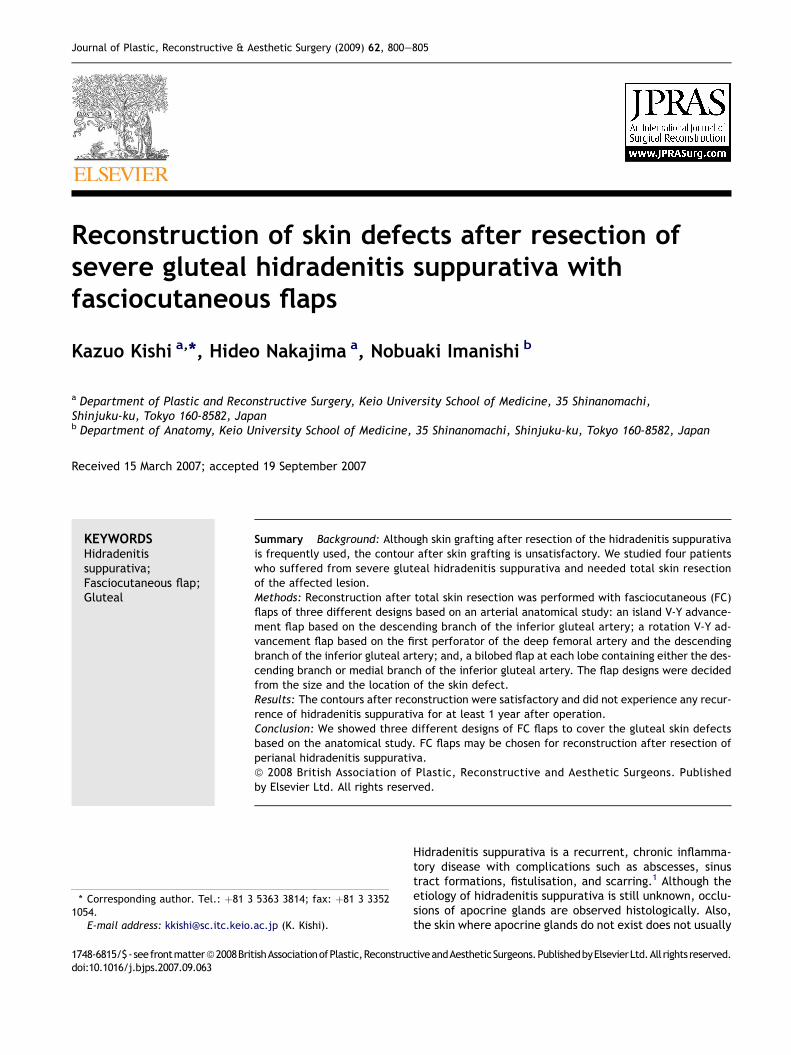
Figure 1 Descending branch of inferior gluteal artery runsbeneath gluteal maximus and fascia lata (arrowheads). Themedial branch was observed in the lower part of the glutealmaximus (open arrowheads). The first perforating branch is ob-served in the lateral lower part of the gluteus maximus(arrow).
Reconstruction of skin defects 801
become the original lesion of the hidradenitis suppurativa.Resection of chronically infected skin is the most oftenused effective treatment. After resection, a skin graft is of-ten performed.2e4 The contours after skin grafting are,however, unsatisfactory. Also, if the treatment of hidrade-nitis suppurativa is based on skin grafting, resection ofchronically inflamed skin will sometimes be insufficient topreserve fat tissue as a cushion. In the present study, weshow four patients who required reconstruction of defectsafter resection of perianal hidradenitis suppurativa withvarious designs of fasciocutaneous (FC) flaps based on thearterial anatomy.
Patients and methods
Patients
Four patients, having severe chronic inflammatory skin withhydradenitis suppurativa, were treated with follow-upperiods of at least 1 year. All of the patients were male,and age at operation ranged from 24 to 64 years old. Thesizes of the skin defects after total skin resection rangedfrom 170 cm2 to 460 cm2. All patients had been treatedwith antibiotics before operation, but the lesion had grad-ually become larger.
Anatomical study
Ten cadavers were systemically injected with a lead oxide-gelatin mixture as previously described.5 The buttock andthe posterior thigh region were dissected beneath deep fas-cia, and were X-rayed to observe the arterial anatomy.
Results
Anatomy
As reported previously, the descending branch of theinferior gluteal artery passes beneath gluteal maximus,and runs in the central part of the thigh along with theposterior femoral cutaneous nerve. From our observations,we found that several branches separate from the descend-ing branch of the inferior gluteal artery, and run medially inthe upper part of the thigh. The first perforating branch isobserved in the lateral lower part of the gluteous maximus(Figure 1). Based on these anatomical observations, threedifferent types of FC flap can be designated to cover theskin defects of the buttock: 1) island V-Y advancementflap based on the descending branch of inferior gluteal ar-tery (gluteal thigh flap)6; 2) rotation V-Y advancement flapbased on the first perforator of the deep femoral artery andthe descending branch of the inferior gluteal artery; and 3)a bilobed flap at each lobe containing either descendingbranch or medial branch of the inferior gluteal artery(Figure 2).
Surgical procedure
All patients were operated upon under general anaesthesia,and the patients were in a prone position. The existence ofeach artery was checked with Doppler before operation.
Design 1Two sides were operated upon with an island V-Y advance-ment flap based on the descending branch of the inferiorgluteal artery. The skin portion was designed so that thedescending branch of the inferior gluteal artery wassituated centrally. The incision was made at the distalside of the flap including fascia lata. The descending branchof the inferior gluteal artery was easily found beneath thefascia lata semitendinosus muscle medially and bicepsfemoris muscle laterally. The distal portion of the descend-ing branch of the inferior gluteal artery was dissected. Theflap was raised centrally until it easily reached the skindefect. If movement of the flap was disrupted by thegluteus maximus, the muscle could be partially bisected torelease the pedicle. Donor sites were primarily sutured.
Design 2Three sides were reconstructed with a rotation V-Y ad-vancement flap based on the first perforator of the deepfemoral artery and the descending branch of the inferiorgluteal artery. The design of the flap is similar to design 1except that the partial skin is connected to the lateral partof the thigh. The skin incision is made at the peripheralside, as is the case with the gluteal thigh flap, to identifythe descending branch of the inferior gluteal artery. Thereason why the lateral side of the flap is kept connected isto provide a sufficient blood supply to the flap with the firstperforating artery. This flap not only includes the descend-ing branch of the inferior gluteal artery, but also thecutaneous branch of the first perforating artery. The bloodsupply of the first perforating branch to the flap is assumedto come from the lateral undivided skin. Thus, the flapincludes both characteristics of V-Y advancement flap androtation flap. The flap is raised beneath fascia lata androtated toward the skin defects. Donor sites are primarilysutured.

Figure 2 Three different designs for covering perianal skin defects. (Design 1) V-Y advancement flap based on descending branchof the inferior gluteal artery (gluteal thigh flap). (Design 2) Rotation V-Y advancement flap based on first perforator of deep femoralartery and descending branch of inferior gluteal artery. (Design 3) Bilobed flap each lobe containing either descending branch ormedial branch of the inferior gluteal artery.
Figure 3 64-year-male with perianal hidradenitis suppura-tiva on his left buttock. (a) Flap design; (b) Resection of in-flamed skin resulted in 15� 12 cm skin defects; Island glutealthigh flap was moved by V-Y advancement. (c) Immediately af-ter operation; (d) 1 year after operation.
802 K. Kishi et al.
Design 3One side is reconstructed with a bilobed flap at each lobecontaining either descending branch or medial branch ofinferior gluteal artery. This flap is used to cover theperianal area only. The perianal skin defect is coveredwith the lobe including the medial branch, and the defectafter elevating this lobe is covered with the lobe includingthe descending branch.
Case reports
Case 1A 64-year-old male patient was resected on his left buttockbecause of perianal hidradenitis suppurativa, resulting in15� 12 cm skin defects. An island gluteal thigh flap was de-signed, as in design 1, on the left thigh, and reconstructedwith V-Y advancement. The size of the flap was 12� 18 cmand the flap took completely. The skin defect and the donorsite were closed primarily, and did not need skin grafting.Three years after operation, no recurrence was observed(Figure 3).
Case 2A 40-year-old male patient suffering from bilateral perianalhidradenitis suppurativa had a resection of buttock skin17� 12 cm to the left, and 18� 15 cm to the right. His leftbuttock was reconstructed with an island gluteal thigh flap.
The right side was reconstructed with design 2, a rotationV-Y advancement flap based on the first perforator of thedeep femoral artery and descending branch of the inferiorgluteal artery because the defect was larger than the leftside. Both flaps took well, and all of the defects and thedonor sites were closed primarily. Three years afteroperation, no recurrence was observed (Figure 4).
Case 3A 36-year-old man was suffering from bilateral perianalhidradenitis suppurativa. After resection, 15� 20 cm and10� 17 cm skin defects appeared, and both sides were cov-ered with a rotation V-Y advancement flap based on the

Figure 4 (a) A 40-year-old male patient suffered from bilateral hidradenitis suppurativa. (b) Skin defects were 17� 12 cm to theleft, and 18� 15 cm to the right. (c) Flaps were transferred. (d,e) Immediately after operation. (f) At 3 months after operation, norecurrence was observed.
Reconstruction of skin defects 803
first perforator of the deep femoral artery and descendingbranch of the inferior gluteal artery (design 2). In the pres-ent case, the lowermost muscle berry of the gluteus maxi-mus muscle was dissected around the descending branch2 cm in width to ease movement of the flap. One year afterreconstruction, no recurrence was observed (Figure 5).
Case 4A 24-year-old man was suffering from wide perianal hidra-denitis suppurativa on the left side. In the present case,because the skin defect occupied almost the entire leftbuttock, it was impossible to cover the entire skin defectwith a FC flap. Thus, we covered only the perianal skin witha bilobed flap (design 3), as a skin graft around the anus issusceptible to bacterial infection. Each lobe containedeither descending branch or medial branch of inferior glutealartery. The remainder of the skin defects were covered withcollagen sponge and a meshed skin graft 2 weeks later. Theflap took well without any infection (Figure 6).
The results are summarised in Table 1.
Discussion
Squamous cell carcinoma can grow from the hidradenitissuppurativa.7e9 Also, when the affected area is large,
patients may die from severe infection.10 Thus, it is rec-ommended to resect all of the inflamed skin when treatinghidradenitis suppurativa.10e13 There are various reportson treatments for gluteal hidradenitis suppurativa, mostof which are based on skin grafting.14 The contours andthe function of the cushion after meshed skin grafting,however, were unsatisfactory. As it was reported that hi-dradenitis suppurativa frequently recurred because ofdeep situated fistulas, leaving fat tissues to preserve ac-ceptable contour and cushion effects will cause a higherrecurrence rate. An advantage of reconstructing a skin de-fect with FC flaps after resecting hidradenitis suppurativais that complete resection of chronically inflamed skin in-cluding fat tissue is possible.15e17 As we resected allchronically inflamed skin and subcutaneous tissue includ-ing fat tissue, we did not experience recurrence of hidra-denitis suppurativa where FC flaps were moved. Wepreviously used an extended gluteus maximus mc flapwith the lower half of the gluteus maximus muscle cover-ing the skin defect after a similar resection. The advan-tages of using a mc flap to cover the skin defectsfollowing resection of hidradenitis suppurativa have alsobeen shown by another group.12 Although the reconstruc-tion method with a gluteus maximus mc flap is also easyand reliable, the flap sometimes becomes bulky,

Figure 5 (a) A 36-year-old man suffered from bilateral perianal hidradenitis suppurativa; After resection,15� 20 cm and10� 17 cm skin defects appeared. Both sides were covered with a rotation V-Y advancement flap. Gluteus maximus muscle waspartially bisected around the descending branch 2 cm in width to make movement of the flap easy. (b) 6 months afterreconstruction.
804 K. Kishi et al.
especially when the upper side of the buttock needs to bereconstructed. Moreover, the stress to the patients andfunctional loss are unneglectable with a mc flap ratherthan with a FC flap. As the thigh skin has fairly good
Figure 6 (a) A 24-year-old man suffered from wide perianal hidflamed skin, the skin defect covered almost all of the left hip; (the anus; (d) Flap elevation; (e) 1 week after operation, the bilobhad partial necrosis.
volume, the donor sides of five of the patients six sideswere also sutured primarily without skin grafting.
We used three different types of FC flap based on thearterial anatomy on the buttock and thigh. It is taken for
radenitis suppurativa on the left hip; (b) After resection of in-c) A bilobed flap was designed to cover only the area arounded flap took completely although the tip of the dissected skin

Table 1 Summary of the patients
Patientnumber
Age Gender Defectsize (cm)
Flap dimension(cm)
Type offlap
Operativetime
Postoperativecomplication
1 64 male 15� 12 12� 18 design 1 2 h 30 m no2 right 40 male 18� 15 14� 17 design 2 4 h 10 m no2 left 17� 12 15� 18 design 1 no3 right 36 male 10� 17 16� 18 design 2 3 h 20 m no3 left 15� 20 17� 22 design 2 no4 24 male 23� 20 15� 10 design 3 2 h 50 m local necrosis of
the dissected skin
Reconstruction of skin defects 805
granted that the more vessels a flap has, the more reliablethat flap is. Based on this theory, we assume that therotation V-Y advancement flap based on first perforator ofthe deep femoral artery and the descending branch ofinferior gluteal artery is the most reliable of the three FCflaps shown in the present paper. Thus, the largest flap willbe raised among the three flaps, although the maximalreliable size to be raised is not known at present. However,as the rotation arc of the flap was restricted by skin or firstperforator, an island gluteal thigh flap might be suitable forcases that need to move the flap further. In order to coverthe medial side, including perianal site, design 3 is easy toreconstruct. As there is a rich vascular network from thedescending branch toward the medial thigh, large FC flapcan be elevated as far as the fascia lata and surroundingvascular networks are included in the flap.
Other FC flaps such as medial thigh flap or superomedialthigh flap cover the perianal and lower parts of the glutealregion. These flaps, however, are based on the branches offemoral arteries, and it is difficult to reach the upper partof the gluteal region. Also, a positional change afterresection is needed.
In summary, when the skin defect is large and is mainlylocated at the lower part of the buttock, design 2 is the firstchoice. When the skin defect includes the upper side of thebuttock, design 1 should be chosen. Design 3 is suitable forcovering the perianal or lower part of the buttock.
References
1. Brown TJ, Rosen T, Orengo IF. Hidradenitis suppurativa. SouthMed J 1998;91:1107e14.
2. Kuo HW, Ohara K. Surgical treatment of chronic gluteal hidra-denitis suppurativa: reused skin graft technique. DermatolSurg 2003;29:173e8.
3. Yamada N, Matsuo A, Masuda R, et al. Ideal skin grafting forpyodermia chronica. Br J Plast Surg 2002;55:358e61.
4. Matsushita S, Ishihara T, Masuguchi S, et al. The histopatholog-ical basis for employing the reused skin graft technique forchronic perianal pyoderma. Plast Reconstr Surg 2004;114:833e5.
5. Nakajima H, Imanishi N, Aiso S. Arterial anatomy of the nipple-areola complex. Plast Reconstr Surg 1995;96:843e5.
6. Hurwitz DJ, Swartz WM, Mathes SJ. The gluteal thigh flap: a re-liable, sensate flap for the closure of buttock andperinealwounds. Plast Reconstr Surg 1981;68:521e32.
7. Altunay IK, Gokdemir G, Kurt A, et al. Hidradenitis suppurativaand squamous cell carcinoma. Dermatol Surg 2002;28:88e90.
8. Lapins J, Ye W, Nyren O, et al. Incidence of cancer among pa-tients with hidradenitis suppurativa. Arch Dermatol 2001;137:730e4.
9. Shukla VK, Hughes LE. A case of squamous cell carcinoma com-plicating hidradenitis suppurativa. Eur J Surg Oncol 1995;21:106e9.
10. Endo Y, Tamura A, Ishikawa O, et al. Perianal hidradenitis sup-purativa: early surgical treatment gives good results in chronicor recurrent cases. Br J Dermatol 1998;139:906e10.
11. Mendonca H, Rebelo C, Fernandes A, et al. Squamous cell car-cinoma arising in hidradenitis suppurativa. J Dermatol Surg On-col 1991;17:830e2.
12. Ritz JP, Runkel N, Haier J, et al. Extent of surgery and recur-rence rate of hidradenitis suppurativa. Int J Colorectal Dis1998;13:164e8.
13. Rompel R, Petres J. Long-term results of wide surgical excisionin 106 patients with hidradenitis suppurativa. Dermatol Surg2000;26:638e43.
14. Bohn J, Svensson H. Surgical treatment of hidradenitis suppu-rativa. Scand J Plast Reconstr Surg Hand Surg 2001;35:305e9.
15. Geh JL, Niranjan NS. Perforator-based fasciocutaneous islandflaps for the reconstruction of axillary defects following excisionof hidradenitis suppurativa. Br J Plast Surg 2002;55:124e8.
16. Elliot D, Kangesu L, Bainbridge C, et al. Reconstruction of theaxilla with a posterior arm fasciocutaneous flap. Br J Plast Surg1992;45:101e4.
17. Tanaka A, Hatoko M, Tada H, et al. Experience with surgicaltreatment of hidradenitis suppurativa. Ann Plast Surg 2001;47:636e42.