Embed Size (px)
Citation preview

RCPA-QAP
HP-2016 REVIEW
ANNE GILBERT
ICPMR, WESTMEAD HOSPITAL
WESTMEAD, NSW
AUSTRALIA

RCPA-QAP HP- BACKGROUND
Compulsory surveys for Australian and New Zealand laboratories
performing Haemoglobinopathy testing
(National Accreditation Testing Authority NATA)
Running since 1976
Current committee of 3 –
Anne Gilbert, ICPMR, Westmead Hospital, NSW, Australia
Kerryn Weekes, Monash Medical Centre, Melbourne, Vic, Australia
George Chan, Labplus, Auckland Hospital, New Zealand

RCPA-QAP HP PARTICIPANTS -102
COUNTRY NUMBER OF LABS
AUSTRALIA 34
NEW ZEALAND 8
MALAYSIA 29
HONG KONG 13
SINGAPORE 5
SOUTH AFRICA 6
INDIA 2
PHILLIPINES 1
MACAU 1
FRANCE 1
GERMANY 1
OMAN 1

RCPA-QAP HP- BACKGROUND
4 surveys pa
Freeze dried haemolysate, patient history and blood film (digital)
Evaluate Hb A2, Hb F, Hb variant (if present)
Diagnosis
Assessed on all of these parameters

HP 2016 SURVEY SAMPLES
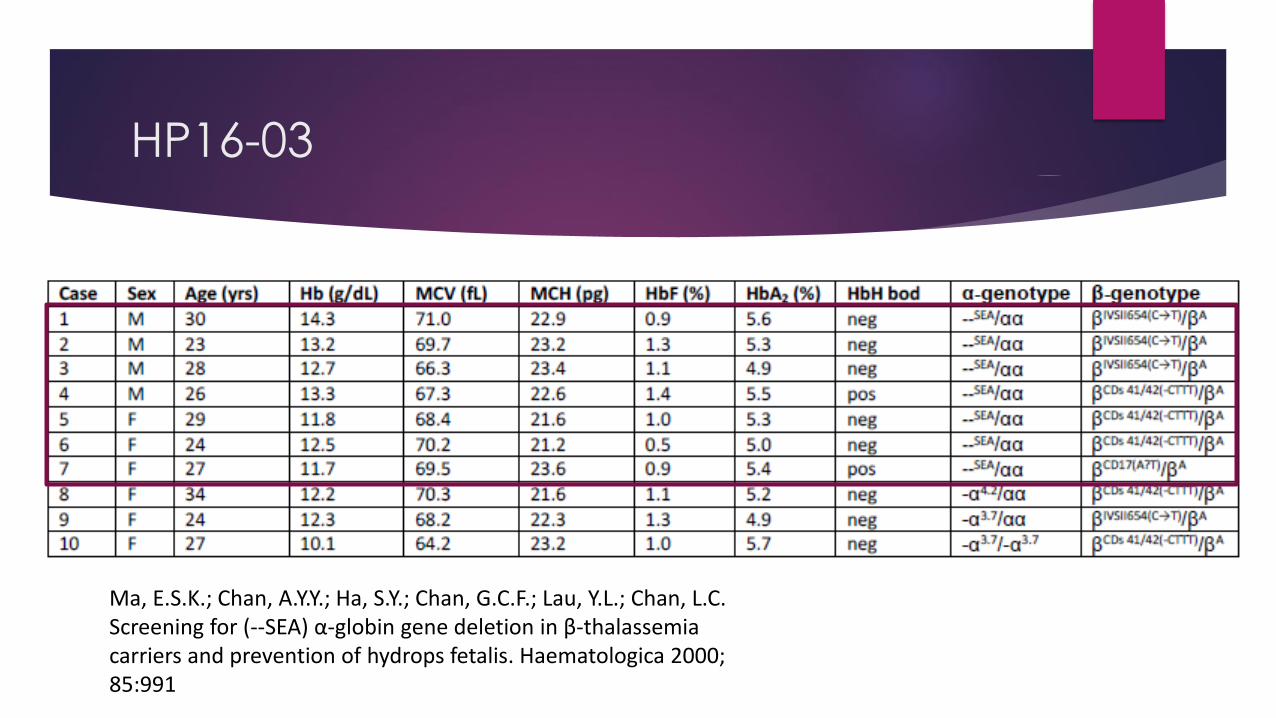
HP16-03 Heterozygous beta thalassaemia- alpha thal not excluded.
HP16-05 Hb Etobicoke [alpha 84(F5) Ser>Arg].
HP16-08 Hb J-Baltimore [beta 16(A13) Gly>Asp].
HP16-10 Low Hb A2, microcytic

HP16-03 HISTORY
Insert
28 year old pregnant Chinese female
RCC 5.4
Hb 109
MCV 64
MCH 20

HP16-03 BLOOD FILM

HP16-03 EXPECTED FINDINGS
METHOD EXPECTED RESULT
HPLC (Bio-Rad VII) Elevated Hb A2
Cap EPG (Sebia) Elevated Hb A2
Alk EPG Increased Hb A2 band

HP16-03 BIO-RAD VII HPLC

HP16-03 SEBIA CAP EPG

Hb A2

HP16-03: Hb A2
METHOD CLASSIFICATION MEDIAN MEAN SD CV Number
Biorad Variant II 4.6 4.6 0.1 2.9 58
Biorad D10 4.9 4.9 0.3 5.0 11
Sebia Capillarys/ Minicap 5.1 5.1 0.1 1.8 28
ALL RESULTS 4.7 4.8 0.3 6.5 106

HP16-03: Hb F
Mostly <1%
Mostly normal interpretation.

HP16-03 DX CODES

HP16-03
Chinese have high incidence of both beta thalassaemia and alpha 0 thalassaemia.
For all beta thal patients from an alpha 0 endemic region – SEA, Greece must
mention that alpha thalassaemia cannot be excluded
Cannot presume that reduced globin chain imbalance will normalise indices.
15% (2008) to 22% (2011) to 37% in 2016 indicated that alpha thal can’t be excluded
in beta thal heteroztgotes. Still 63% don’t.
HP16-03
Ma, E.S.K.; Chan, A.Y.Y.; Ha, S.Y.; Chan, G.C.F.; Lau, Y.L.; Chan, L.C.Screening for (--SEA) α-globin gene deletion in β-thalassemia carriers and prevention of hydrops fetalis. Haematologica 2000; 85:991

HP16-05 HISTORY
Insert
24 yo pregnant female
RCC 5.0
Hb 145
MCV 88
MCH 29

HP16-05 FILM

HP16-05 EXPECTED FINDINGS
METHOD EXPECTED RESULT
HPLC (Bio-Rad VII) Hb variant elutes in the D window
Cap EPG (Sebia) Hb variant separates in the D zone
Alk EPG Hb variant with mobility of Hb S/D
Acid EPG Hb variant does not separate.

HP16-05 BIO-RAD VII HPLC
D window
Minor peak S window
Reduced Hb A2

16-05 CAP EPG
D window
Minor peak Z1
Reduced Hb A2

HP16-05: Hb A2
METHOD CLASSIFICATION MEDIAN MEAN SD CV Number
Biorad Variant II 1.8 1.8 0.1 7.1 65
Biorad D10 2.0 2.2 0.5 21.6 11
Sebia Capillarys/Minicap 2.0 2.0 0.2 7.9 33
ALL RESULTS 1.1 1.8 0.2 9.0 107

HP16-05: Hb F
All <1%
All normal

HP16-05 DX CODES

HP16-05 Hb ETOBICOKE (a84(F5)Ser>Arg)
Serine (neutral)
Arginine (basic)

Hb Etobicoke a84(F5)Ser>Arg site
a84(F5) faces into
haem group

HP16-05 Hb ETOBICOKE (a84(F5)Ser>Arg
Rare variant – participants not expected to identify it.
F helix important in oxygenation/deoxygenation and for stabilisation of the globin chain.
Hb Etibicoke is slightly unstable with increased oxygen affinity.
This is not evident in vivo – probably due to low level of alpha variants.
b mutations at this site result in erythrocytosis and a high oxygen affinity phenotype.

HP16-08 HISTORY
36 year old female
RCC 4.4
Hb 123
MCV 89
MCH 28
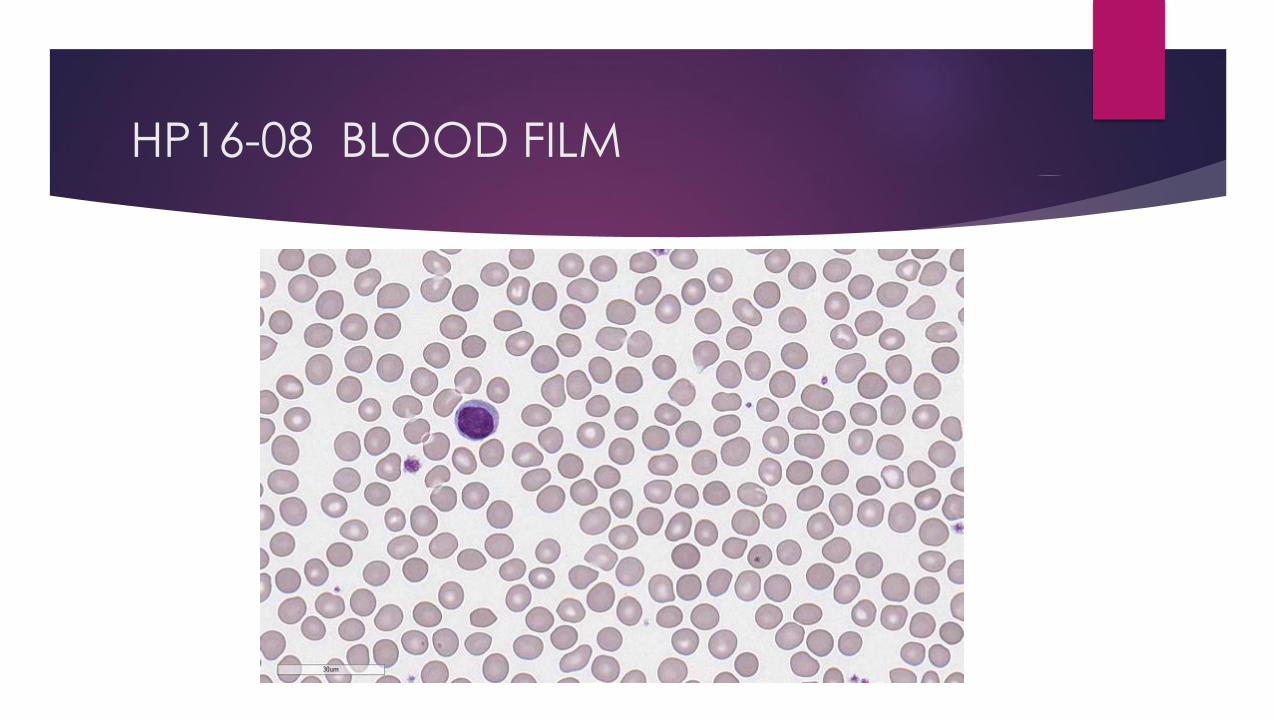
HP16-08 BLOOD FILM

HP16-08 EXPECTED FINDINGS
METHOD EXPECTED RESULT
HPLC (Bio-Rad VII) Hb variant elutes in the P3 window
Cap EPG (Sebia) Hb variant separates in the Z12 zone
Alk EPG Hb variant with mobility of Hb J
Acid EPG Hb variant does not separate.

HP16-08 BIO-RAD VII HPLC
P3 window
Hb X1c co-elutes with Hb F
Hb F inaccurate

HP16-08 SEBIA CAP EPG
Hb F <1%

HP16-08: Hb F
METHOD CLASSIFICATION MEDIAN MEAN SD CV Number
Biorad Variant II 2.3 2.8 0.2 6.4 62
Biorad D10 3.2 3.0 0.8 28.3 11
Sebia Capillarys/Minicap 0 0.1 0.2 161.3 32
ALL RESULTS 2.2 1.7 1.1 64.3 111

HP16-08: Hb F
Data skewed

HP16-08 Hb VARIANT
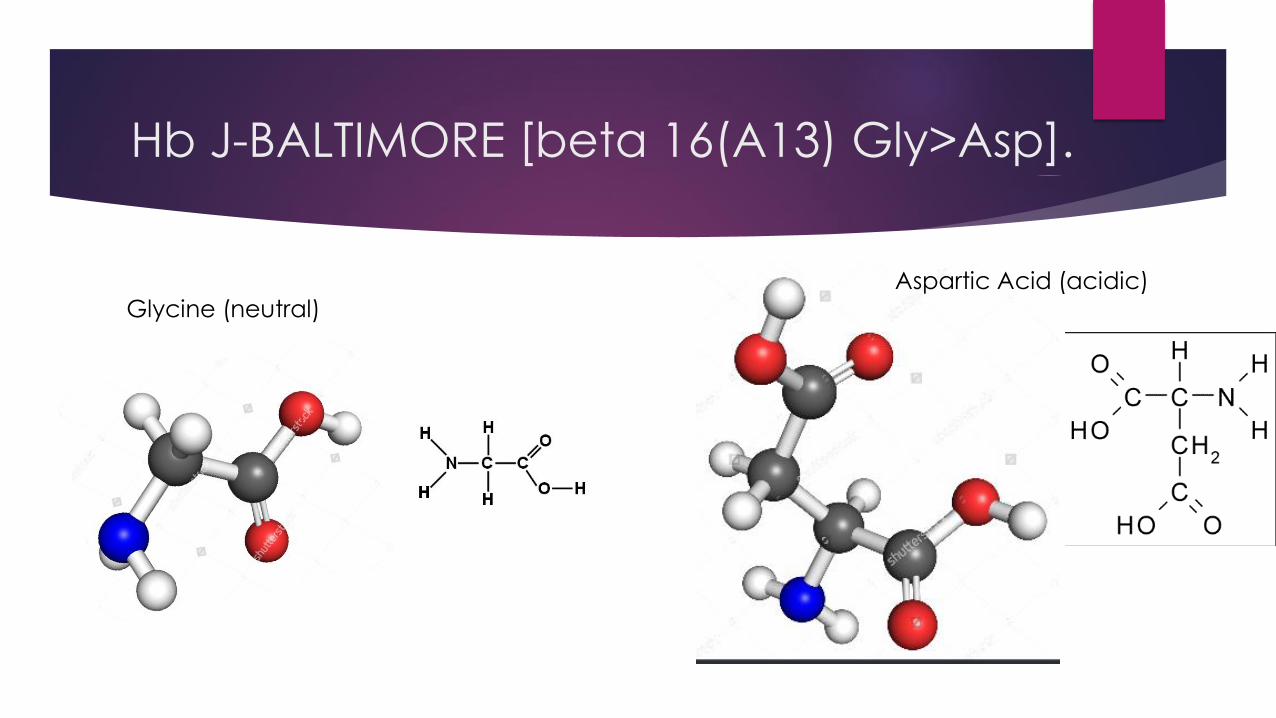
Hb J-BALTIMORE [beta 16(A13) Gly>Asp].
Glycine (neutral) Aspartic Acid (acidic)

Hb J-Baltimore [beta 16(A13) Gly>Asp] site
A13 external.
Can cope with big changes

Hb J-BALTIMORE [beta 16(A13) Gly>Asp].
Rare variant – participants not expected to identify it.
Interferes with Hb A1c quantitation
Haematologically normal.

HP16-10 HISTORY
70 year old Italian male
RCC 5.4
Hb 116
MCV 68
MCH 21

HP16-10 BLOOD FILM

HP16-10 EXPECTED FINDINGS
METHOD EXPECTED RESULT
HPLC (Bio-Rad VII) Reduced Hb A2
Cap EPG (Sebia) Reduced Hb A2

HP16-10 BIO-RAD VII HPLC

HP16-10 SEBIA CAP EPG

HP16-10: Hb A2
METHOD CLASSIFICATION MEDIAN MEAN SD CV Number
Biorad Variant II 1.8 1.8 0.1 5.6 64
Biorad D10 1.9 1.9 0.1 4.7 11
Sebia Capillarys/Minicap 1.7 1.7 0.1 4.7 35
ALL RESULTS 1.8 1.8 0.1 6.2 111

HP16-10: Hb F
Mostly <1%
Mostly normal

HP16-10 DX CODES

HP16-10 COMMENTS
DD alpha thal + delta thal +/or irondeficiency – code created.
Many participant RRs did not indicate reduced Hb A2
Delta thal common in Italians and Greeks –as is beta thal
Beta thal with co-inherited delta thal may mask Hb A2 elevation.
The committee has suggested that laboratories review their reference ranges , which should be calculated based on normal patient population.
Instruments such as Bio-Rad HPLC and Sebia Capillary Electrophoresis: the lower limit for Hb A2 should not be below 2.0 and the upper limit should be less than 3.5.
Currently, only about 30% participants have reference ranges that fall within these limits, which has significant implications for diagnostic decisions.





























