Embed Size (px)
Citation preview

Case 3Rayos, K.- Rodas, F.

Case 3 21 year old student CC: Loss of vision OS and
eye aches associated with movement.
PMH: Similar episode in the OD three years ago with spontaneous resolution. Also, a history of right sided numbness made better with ‘hilot’.
Vision: Right 20/20-2Left 20/40-1
IOP: OU 15mm Hg (Normal IOP: 15.5 mmHg
with fluctuations of 2.75)

What is your working diagnosis?
Hypertensive Retinopathy

Hypertensive Retinopathy
Characterized by a variety of retinal vascular signs in individuals with elevated BP
Causes blurring of vision Bilateral, symmetrical End organ manifestation

Hypertensive Retinopathy Funduscopic findings:
o Focal attentuation of a major retinal arteriole
o Broadening of the arteriolar light reflex
o Arteriovenous crossing changes
o Hemorrhageso Retinal infarcts (Cotton-wool
spots)o Choroidal infarcts
(Elschnig’s spots)o Serous dettachment of the
retinao Severe disk edema

Arteriosclerotic Changes
– Arteriolar narrowing that is almost always bilateral • Grade I - 3/4 normal caliber • Grade II - 1/2 normal caliber • Grade III - 1/3 normal caliber • Grade IV - thread-like or invisible
– Arterio-venous crossing changes (aka “AV nicking") with venous constriction and banking
– Arteriolar color changes • Copper wire arterioles are those arterioles in which the
central light reflex occupies most of the width of the arteriole.
• Silver wire arterioles are those arterioles in which the central light reflex occupies all of the width of the arteriole.

Stages of Hypertensive Retinopathy
• Grade 1 – general narrowing of arterioles• Grade 2- Narrowing of arterioles plus arteriolar
spasm• Grade 3 – Grade 2 changes plus hemorrhage
and exudates- Flame-shaped (splinter hemorrhages)- seen in the nerve fiber layer
- Cotton wool spots – result of microinfarction of NFL which produces aggregates of Cytoid bodies- Hard waxy exudates may be seen (lipophilic exudates located in Outer plexiform Inner Nuclear layer)

Stages of Hypertensive RetinopathyGrade 4- All grade 3 changes with
optic disc edema, necrosis, thinning, clumping and proliferation of Retinal pigment epithelium May also occur as a result of obliterative
changes in the choriocapillary in malignant hypertension .

Vascular Changes
Arteriolar narrowing o A:V- 2:3
AV crossing changes
Gradingo I- Leakageo II- Blood and
hemorrhageo III- Cotton wool
spotso IV- Optic disc
swelling, subretinal exudates

What are your differentials?
Other retinopathies that are known complications of high blood pressure are called:
Diabetic retinopathy Ischemic optic neuropathy Retinal artery occlusion Retinal emboli Retinal vein occlusion

Diabetic RetinopathyNon-proliferative Type Capillaries develop:
o Microaneurysmso Thickening of the BMo Dec # of pericytes
Classification based on severity:o Mild
o Atleast 1 microaneurysmo Moderate
o Extensive microaneurysmo Intraretinal hemorrhageso Venous beadingo Cotton wool spots
o Severeo Cotton wool spotso Venous beadingo Intraretinal microvascular
abnormalities (IRMA)

Diabetic RetinopathyProliferative Type
Presence of neovascularization on optic disk
Bleeding of vessels
Massive vitreous hemorrhageo Sudden visual loss

Ischemic Optic Neuropathy• Age: older age groups– Nonarteritic: late 40s and older– Arteritic: >50 y/o
• Gender predilection: F>M• History: painless visual loss upon
awakening– Early: malaise, weight loss, fever, vague
abdominal or GI pains, and anorexia– Late: abdominal aortic aneurysm
• Clinical Findings: – Nonarteritic: visual loss and field loss,
small cup disc ratio, sectorial disc edema, pale and swollen optic disc
– Arteritic: chalky white, pale, and swollen optic disc; quite prominent, ropey, and tender temporal arteries; oral, tongue, or scalp ulcer

Retinal Artery Occlusion• Age: Mean: early in the 7th decade• Gender predilection: M>F• History: Acute persistent painless loss
of vision, complete/sectional visual field defect, history of hypertension or diabetes mellitus, other medical problems (atrial fibrillation), prolonged direct pressure or drug-induced
• Clinical Findings: – Fundoscopy: afferent pupillary defect,
cherry red spot and a ground-glass retina, emboli, whitening of the retina and Boxcar segmentation (BRAO)
– PE: can have murmurs, carotid bruits, or other signs of cardiovascular disease

Retinal Emboli
Most commonly arise from carotid artery disease
In patients younger than 40, a cardiac origin such as atrial fibrillation, mitral valve prolapse or subacute endocarditis is considered
Three types:1. Cholesterol emboli• Also called Hollenhorst plaques• Usually arise from an atheromatous
plaque in the carotid artery and consist of cholesterol and fibrin
• Lodge at the bifurcation of the retinal arterioles, are refractile and appear larger than the vessel that contains them

Retinal Emboli
2. Calcific emboli▪ Originates from damaged cardiac valves
producing complete occlusion and infarction of the distal retina
▪ Solid and calcified and usually occur in younger patients
3. Platelet fibrin emboli▪ Account for most cases of amaurosis
fugax▪ Due to the transit of platelet aggregates
through the retinal and choroidal circulations
▪ May be reduced by drugs that reduce platelet aggregation like aspirin

Central Retinal Vein Occlusion Increased incidence in smokers,
hypertension, diabetes mellitus, hyperlipidemia,collagen-vascular disease, chronic renal failure and hyperviscosity syndromes• Fundoscopy shows
– Dilated tortuous veins with retinal and macular edema
– Hemorrhages all over the posterior pole
– Cotton wool spots

Diagnostic Examinations
Get patient’s Blood Pressure Ophthalmoscopy Flourescein angiography

Sphygmomanometry
Used to monitor the blood pressure of the patient
Blood Pressure Classification
Blood Pressure Classification
Systolic, mmHg
Diastolic, mmHg
Normal <120 and <80 Prehypertension 120–139 or 80–89
Stage 1 hypertension 140–159 or 90–99
Stage 2 hypertension 160 or 100 Isolated systolic hypertension
140 and <90 Source: Table 241-1. Harrison’s Principles of Internal Medicine 17th ed.

Ophthalmoscopy
• Ophthalmoscope has long been regarded as part of the standard evaluation of persons with hypertension
• Ophthalmoscope has been shown to have high rates of interobserver variability (20 to 42 percent) and intraobserver variability (10 to 33 percent) when used in persons with mild hypertension
• few studies have demonstrated associations between hypertensive retinopathy and specific cardiovascular outcomes (e.g., incident stroke and coronary heart disease) or have adequately controlled for relevant confounding factors (e.g., hyperlipidemia and cigarette smoking)
http://content.nejm.org/cgi/content/full/351/22/2310

Mild Hypertensive Retinopathy – Opthalmoscopy
Figure 1. Examples of Mild Hypertensive Retinopathy. Panel A shows arteriovenous nicking (black arrow) and focal narrowing (white arrow).
Panel B shows arteriovenous nicking (black arrows) and widening or accentuation ("copper wiring") of the central light reflex of the arterioles (white arrows).
Mild Hypertensive Retinopathy – Opthalmoscopy
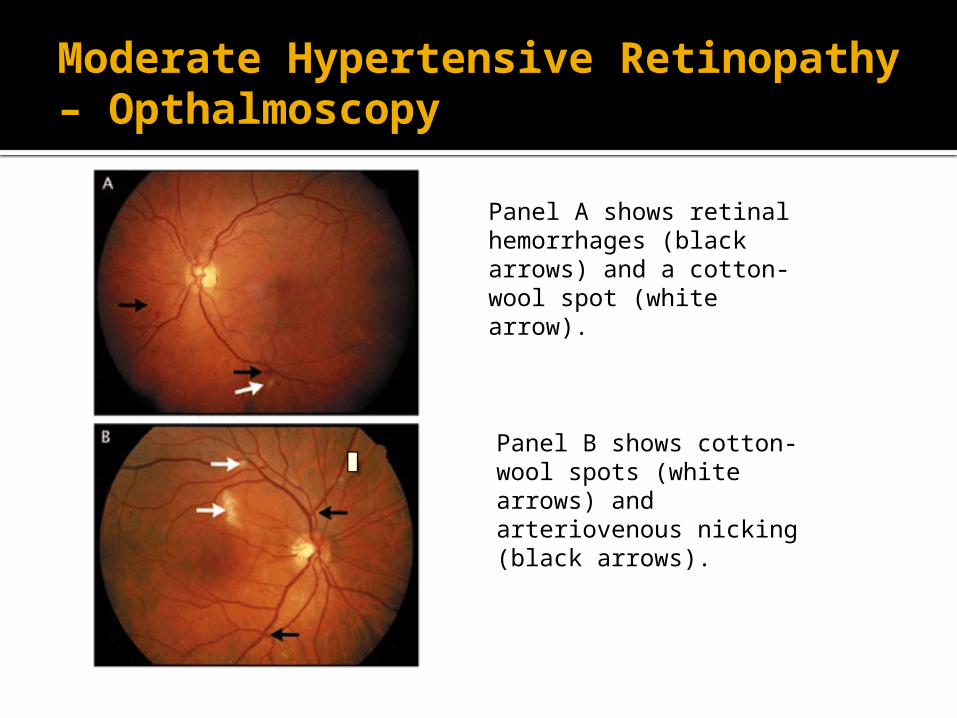
Moderate Hypertensive Retinopathy – Opthalmoscopy
Panel A shows retinal hemorrhages (black arrows) and a cotton-wool spot (white arrow).
Panel B shows cotton-wool spots (white arrows) and arteriovenous nicking (black arrows).

Multiple cotton-wool spots (white arrows), retinal hemorrhages (black arrows), and swelling of the optic disk are visible
Moderate Hypertensive Retinopathy – Opthalmoscopy


Fluorescein angiography
Technique for examining the circulation of the retina using the dye tracing method
Involves injection of sodium fluorescein into the systemic circulation, and then an angiogram is obtained by photographing the fluorescence emitted after illumination of the retina with blue light at a wavelength of 490 nanometers
Can detect diabetic retinopathy, vein occlusions, retinal artery occlusions, edema of the optic disc, and tumors.

CAUSES OF HYPERFLUORESCENCE:
leaking defects (i.e. capillary leakage, aneurysm, neovascularization) pooling defects staining transmission (filling) defects abnormal vasculature
CAUSES OF HYPOFLUORESCENCE:
blocking defect (i.e. blood) filling defect (capillary blockage)

Treatment
Control hypertension Other vision- threatening conditions should also
be controlled Laser Intravitreal injection of corticosteroids Anti-vascular endothelial growth factor drugs
monoclonal antibodies such as bevacizumab (Avastin), antibody derivatives such as ranibizumab (Lucentis),
or orally-available small molecules that inhibit the
tyrosine kinases stimulated by VEGF: ▪ lapatinib (Tykerb), sunitinib (Sutent), sorafenib (Nexavar),
axitinib, and pazopanibMerck manual online medical library

http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=cardio&part=A379&rendertype=table&id=A433

THANK YOU!





























