-
8/14/2019 Radiological Screening for Breast Cancer
1/34
-
8/14/2019 Radiological Screening for Breast Cancer
2/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Why screen for breast cancer?Why screen for breast cancer? Does
screening reduce breast cancer mortality?Does screening reduce
breast cancer mortality?
How should average risk women be screened?How should average
risk women be screened? When do we start screening?When do we start
screening? Is there a difference between digital and filmIs there a
difference between digital and film
mammography?mammography?
When is breast MR appropriate?When is breast MR appropriate? Is
there a role for MRI to screen the contralateralIs there a role for
MRI to screen the contralateral
breast in patients with a new diagnosis of breastbreast in
patients with a new diagnosis of breastcancer?cancer?
Is breast MRI better for screening high risk women?Is breast MRI
better for screening high risk women?
Our patient: 54F presents for screeningOur patient: 54F presents
for screening
mammographymammography
-
8/14/2019 Radiological Screening for Breast Cancer
3/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Screening CriteriaScreening Criteria The ConditionThe
Condition
Must be important health problem.Must be important health
problem. Epidemiology and natural history of the disease should be
adequately understood.Epidemiology and natural history of the
disease should be adequately understood. Must have a detectable
risk factor, disease marker, latent period or early symptomaticMust
have a detectable risk factor, disease marker, latent period or
early symptomatic
stage.stage. The TestThe Test
Simple, safe, precise and validated screening test.Simple, safe,
precise and validated screening test.
Acceptable to the populationAcceptable to the population
TreatmentTreatment
The treatment/intervention for patients identified through
screening must be effectiveThe treatment/intervention for patients
identified through screening must be effectiveand early treatment
must improve outcomes compared to late treatment.and early
treatment must improve outcomes compared to late treatment.
Agreed policy on who to treat.Agreed policy on who to treat.
Screening programScreening program
RCT must demonstrate that screening reduced morbidity and
mortality.RCT must demonstrate that screening reduced morbidity and
mortality. The benefit of screening must outweigh the risks/side
effects from the screening.The benefit of screening must outweigh
the risks/side effects from the screening. Facilities for diagnosis
and treatment should be available.Facilities for diagnosis and
treatment should be available. The total cost of finding a case
should be economically balanced in relation to medicalThe total
cost of finding a case should be economically balanced in relation
to medical
expenditure as a whole.expenditure as a whole. Case-finding
should be a continuous process.Case-finding should be a continuous
process.
Wilson and Jungner1968
-
8/14/2019 Radiological Screening for Breast Cancer
4/34
-
8/14/2019 Radiological Screening for Breast Cancer
5/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Early evidence for screeningEarly evidence for screening
The decision to embark on national screeningThe decision to
embark on national screeningprograms in the US and UK were based on
the RRprograms in the US and UK were based on the RRreduction in
breast cancer specific mortality ofreduction in breast cancer
specific mortality ofthese two early trials.these two early
trials.
Trial Location Year Age N= Median
follow-up
RRreduction
Absolute riskreduction
HIP* New York 1963 40-64 31,000 pairs 16 years 21% 0.14%
TwoCountry
Sweden 1977 40-74 77,000 Study
56,000 Control
17 years 32% 0.18%
*Health Insurance Plan
*Health Insurance Plan
Gotzsche and Nielsen. Cochrane Review. 20Gotzsche and Nielsen.
Cochrane Review. 20Humphrey et al. Ann Intern Med. 2002.Humphrey et
al. Ann Intern Med. 2002.
-
8/14/2019 Radiological Screening for Breast Cancer
6/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Current evidence for screeningCurrent evidence for
screeningHumphrey et al. Ann Intern Med. 2002.Humphrey et al. Ann
Intern Med. 2002.
Meta-analyses of seven RCT (Edinburgh excluded)Meta-analyses of
seven RCT (Edinburgh excluded)concluded mammography reduces breast
cancerconcluded mammography reduces breast cancermortality rates in
women age 40-74mortality rates in women age 40-74
-
8/14/2019 Radiological Screening for Breast Cancer
7/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Relative vs. Absolute RiskRelative vs. Absolute Risk
Example: A patient with cancer is trying to decide whether
toExample: A patient with cancer is trying to decide whether
toundergo radiation treatment (XRT) to reduce their risk of
aundergo radiation treatment (XRT) to reduce their risk of
arecurrence. Besides the side effects of treatment, XRT
isrecurrence. Besides the side effects of treatment, XRT
iscumbersome requiring treatments 5 days a week for 6 weeks.
XRTcumbersome requiring treatments 5 days a week for 6 weeks.
XRTreduces the risk of recurrence by 75%!!reduces the risk of
recurrence by 75%!!
A relative risk reduction of 75% is relative to the risk of
recurrence.A relative risk reduction of 75% is relative to the risk
of recurrence.
If the risk of recurrence without XRT is 20%:If the risk of
recurrence without XRT is 20%: Risk of recurrence with XRT = 20% -
20% * 0.75 = 5%Risk of recurrence with XRT = 20% - 20% * 0.75 =
5%
Absolute risk reduction of XRT = 20% - 5% = 15%Absolute risk
reduction of XRT = 20% - 5% = 15%
If the risk of recurrence without XRT is 4%:If the risk of
recurrence without XRT is 4%: Risk of recurrence with XRT = 4% - 4%
* 0.75 = 1%Risk of recurrence with XRT = 4% - 4% * 0.75 = 1%
Absolute risk reduction of XRT = 4% - 1% = 3%Absolute risk
reduction of XRT = 4% - 1% = 3%
-
8/14/2019 Radiological Screening for Breast Cancer
8/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Mammography vs. AdjuvantMammography vs. Adjuvant
ChemotherapyChemotherapyBerry et al. NEJM. 2007.Berry et al.
NEJM. 2007.
Since the variability between the models was greaterSince the
variability between the models was greaterfor screening than
treatment, there is greaterfor screening than treatment, there is
greateruncertainty when estimating the benefit of
screening.uncertainty when estimating the benefit of screening.
-
8/14/2019 Radiological Screening for Breast Cancer
9/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Screening only has a benefit if followed by adjuvant
treatmentScreening only has a benefit if followed by adjuvant
treatment
Mammography vs. AdjuvantMammography vs. Adjuvant
ChemotherapyChemotherapyBerry et al. NEJM. 2007.Berry et al.
NEJM. 2007.
Reductionin
mortalitywith
adjuvant tx
alone
Noreductionin
mortalitywith
screeningalone
-
8/14/2019 Radiological Screening for Breast Cancer
10/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Screening QuestionedScreening QuestionedGotzsche and Nielsen.
Cochrane Review. 2006Gotzsche and Nielsen. Cochrane Review.
2006
Meta-analysis of the seven RCTs (same Humphrey)Meta-analysis of
the seven RCTs (same Humphrey) The Edinburgh trial was excludedThe
Edinburgh trial was excluded Two trials were adequately randomized
(best)Two trials were adequately randomized (best) Four trials were
suboptimally randomizedFour trials were suboptimally randomized
Overall RR reduction = 20%Overall RR reduction = 20% For the
best trials:For the best trials:
RR reduction = 15%RR reduction = 15% Absolute risk reduction is
0.05%Absolute risk reduction is 0.05%
Screening leads to overdiagnosis andScreening leads to
overdiagnosis andovertreatment:overtreatment: RR increase = 30%RR
increase = 30% Absolute risk increase = 0.5%Absolute risk increase
= 0.5%
-
8/14/2019 Radiological Screening for Breast Cancer
11/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Screening QuestionedScreening QuestionedGotzsche and Nielsen.
Cochrane Review. 2006Gotzsche and Nielsen. Cochrane Review.
2006
Conclusion:Conclusion: For every 2000 women screened over 10For
every 2000 women screened over 10
years, one will have her life prolonged and 10years, one will
have her life prolonged and 10healthy women will be diagnosed with
breasthealthy women will be diagnosed with breastcancer and treated
unnecessarily.cancer and treated unnecessarily.
It is not clear whether screening does moreIt is not clear
whether screening does moregood than harm.good than harm.
-
8/14/2019 Radiological Screening for Breast Cancer
12/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Guidelines for screeningGuidelines for screening
For average risk women with lifetime risk 70: screen with
mammography if life expectancy isscreen with mammography if life
expectancy is
>10 yrs>10 yrs
For high risk women with lifetime risk >20-25%:For high risk
women with lifetime risk >20-25%: Includes BRCA1/BRCA2
mutations, women with a strong FHxIncludes BRCA1/BRCA2 mutations,
women with a strong FHx
of breast or ovarian cancer, and women who were treatedof breast
or ovarian cancer, and women who were treatedwith mantle radiation
for Hodgkins lymphomawith mantle radiation for Hodgkins
lymphoma
Screen with MRI as adjunct to mammography starting at ageScreen
with MRI as adjunct to mammography starting at age40 or 10 years
before the diagnosis of a first degree relative40 or 10 years
before the diagnosis of a first degree relative
Saslow et al. CA Cancer J Clin. 2007.
-
8/14/2019 Radiological Screening for Breast Cancer
13/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Cost-effectiveness of screeningCost-effectiveness of
screening
AgeAge Cost per year of life savedCost per year of life saved
40-4940-49 $105,000$105,000
50-6950-69 $21,400$21,400 >65 to 75 or 80>65 to 75 or 80
$34,000-$88,000$34,000-$88,000
For the 40-49 and the 50-69 age group,For the 40-49 and the
50-69 age group,
screening is cost-effectivescreening is cost-effective Screening
is cost-effective in the oldestScreening is cost-effective in the
oldest
age group if the women are healthy.age group if the women are
healthy.
Salzmann et al. Ann Intern Med. 1997Mandelblatt et al. Ann
Intern Med. 200
-
8/14/2019 Radiological Screening for Breast Cancer
14/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
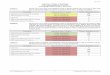
Digital vs. Film MammographyDigital vs. Film MammographyPisano
et al. NEJM. 2005.Pisano et al. NEJM. 2005.
Study Design:Study Design: Prospective study: 49,528
asymptomatic women underwentProspective study: 49,528 asymptomatic
women underwent
both digital and film screening mammographyboth digital and film
screening mammography
Methods:Methods: Mammograms were interpreted by using the BIRADS
systemMammograms were interpreted by using the BIRADS system
and malignancy scaleand malignancy scale Breast cancer status
was ascertained by breast biopsy or by f/uBreast cancer status was
ascertained by breast biopsy or by f/u
mammography at > 10 m.mammography at > 10 m. Sensitivity
and specificity was calculated at 365 and 455 days.Sensitivity and
specificity was calculated at 365 and 455 days. For malignancy
scale, ROC analysis was performed.For malignancy scale, ROC
analysis was performed.
Results/Conclusion:Results/Conclusion: The accuracy of digital
mammography was significantly higherThe accuracy of digital
mammography was significantly higher
than film for women < 50 yo, women with dense breasts onthan
film for women < 50 yo, women with dense breasts onmammography
andmammography andpre- and perimenopausal womenpre- and
perimenopausal women
B itt L HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
15/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Our patient: 54F presents for screeningOur patient: 54F presents
for screening
mammographymammography Her risk factors for breast cancer:Her
risk factors for breast cancer: Gender and ethnicityGender and
ethnicity Estrogen exposure:Estrogen exposure:
Menarche at age 11Menarche at age 11
P2G2 with first pregnancy at age 34P2G2 with first pregnancy at
age 34 PremenopausalPremenopausal
No personal history of breast cancerNo personal history of
breast cancer Family history of post-menopausal breast cancerFamily
history of post-menopausal breast cancer
in mother and paternal aunt, not Ashkenaziin mother and paternal
aunt, not Ashkenaziethnicityethnicity
By the Gail Model, her lifetime risk of BC isBy the Gail Model,
her lifetime risk of BC is
17.6%17.6% Case courtesy of Dr. Valerie Fein-Zachary
B i L HMS IVB itt L HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
16/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Is mammography appropriateIs mammography appropriate
screening for this patient?screening for this patient?
Yes, her lifetime risk is
-
8/14/2019 Radiological Screening for Breast Cancer
17/34
B itt L HMS IVB itt L HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
18/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
BI-RADS mammography categoriesBI-RADS mammography categories
0: Need additional imaging0: Need additional imaging 1:
Negative, routine follow-up1: Negative, routine follow-up 2:
Benign, routine follow-up2: Benign, routine follow-up 3: Probably
benign finding3: Probably benign finding
Follow-up with diagnostic view of the suspicious lesion in
sixFollow-up with diagnostic view of the suspicious lesion in
six
monthsmonths Probability of malignancy is 2 percentProbability
of malignancy is 2 percent
4: Suspicious4: Suspicious Core-needle biopsy or needle
localization biopsy as soon asCore-needle biopsy or needle
localization biopsy as soon as
possiblepossible >2 to 95 percent risk of malignancy>2 to
95 percent risk of malignancy Stratified further as:Stratified
further as:
(a) Low-risk(a) Low-risk (b) Intermediate-risk(b)
Intermediate-risk (c) Moderate to high-risk(c) Moderate to
high-risk
5: Highly suggestive of malignancy5: Highly suggestive of
malignancy Core-needle biopsy or needle localization biopsy as soon
asCore-needle biopsy or needle localization biopsy as soon as
possiblepossible >95 percent risk of malignancy>95 percent
risk of malignancy
6: Biopsy-proven carcinoma6: Biopsy-proven carcinoma
B itt L HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
19/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Fletcher.UpToDate. 2007.
Brittan Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
20/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
4 m later, she palpates a mass in her left4 m later, she
palpates a mass in her left
breastbreast Mammography is repeated:Mammography is
repeated:
Brittany Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
21/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
4 m later, she palpates a mass in her left4 m later, she
palpates a mass in her left
breastbreast Mammography is repeated:Mammography is
repeated:
BI-RADS 4c
Brittany Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
22/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
DDx of a breast massDDx of a breast mass
Carcinoma of theCarcinoma of thebreastbreast
Phyllodes tumorPhyllodes tumor
FibroadenomaFibroadenoma
Adenoma of the nippleAdenoma of the nipple Intraductal
papillomaIntraductal papilloma
Carcinoma of the breastCarcinoma of the breast
Benign calcifications in:Benign calcifications in: SkinSkin
ArteriesArteries CystsCysts
Fibroadenoma with denseFibroadenoma with densepopcorn-like
calcificationspopcorn-like calcifications
Foreign body post-traumaForeign body post-trauma
DDx of a calcifications
on mammography
Brittany Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
23/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
An ultrasound guided core biopsy reveals ainfiltrating ductal
carcinoma and DCIS
Brittany Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
24/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Use of MRI to screen the contralateralUse of MRI to screen the
contralateral
breast after an initial BC diagnosisbreast after an initial BC
diagnosisLehman et al. NEJM. 2007.Lehman et al. NEJM. 2007. Study
design:Study design:
Prospective study of 969 women with a recent diagnosis
ofProspective study of 969 women with a recent diagnosis
ofunilateral breast cancer, who had no abnormalities onunilateral
breast cancer, who had no abnormalities onclinical exam or
mammography in the contralateral breast,clinical exam or
mammography in the contralateral breast,
underwent breast MRunderwent breast MR Results:Results:
12.5% had positive MRI findings12.5% had positive MRI findings
25% with a positive MRI were positive for cancer25% with a positive
MRI were positive for cancer 3.1% had contralateral BC detected by
MRI3.1% had contralateral BC detected by MRI
Conclusion:Conclusion: MRI can detect clinically and
mammographically occult BCMRI can detect clinically and
mammographically occult BC
in the contralateral breast after a new diagnosis of breastin
the contralateral breast after a new diagnosis of
breastcancer.cancer.
Brittany Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
25/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Breast MRI techniqueBreast MRI technique
Without contrast: Density, architecture,Without contrast:
Density, architecture,fluid-filled structures and
implantsfluid-filled structures and implants
Contrast, gadolinium, is used toContrast, gadolinium, is used
tomaximize cancer detection.maximize cancer detection.
Contrast agents improve detection sinceContrast agents improve
detection since
malignant tumors are hypervascular andmalignant tumors are
hypervascular andenhance early (before normal breastenhance early
(before normal breasttissue) after contrast is given.tissue) after
contrast is given.
Brittany Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
26/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
http://www.qcif.edu.au/industry/QldXRay.html
Brittany Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
27/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Benign breast findings on MRIBenign breast findings on MRI
Fibroadenoma Lactating breast Implant with bubbleT2
Post-contrast T1 No contrast T1 Post-contrast
www.mrsc.ucsf.edu/breast/picts_of_breast_mri.ht
Brittany Lee HMS IVBrittany Lee HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
28/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Malignant findings on MRIMalignant findings on MRI
T1 Pre-contrast IDC T1 Post-contrast IDC
T1 Pre-contrast DCIS T1 Post-contrast DCIS
www.mrsc.ucsf.edu/breast/picts_of_breast_mri.ht
Brittany Lee HMS IVBrittany Lee, HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
29/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Our patients breast MRIOur patients breast MRI
Right Breast Left Breast
Brittany Lee, HMS IVBrittany Lee, HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
30/34
Brittany Lee, HMS IVBrittany Lee, HMS IV
Dr. Gillian LiebermanDr. Gillian Lieberman
Breast MRI is better for screening high riskBreast MRI is better
for screening high risk
womenwomen Multiple studies demonstrate that breast MR is
moreMultiple studies demonstrate that breast MR is more
sensitive than mammography for high risk women*sensitive than
mammography for high risk women*
Kriege et al. NEJM 2004:Kriege et al. NEJM 2004: 1909 women with
lifetime risk >15% were screened every 61909 women with lifetime
risk >15% were screened every 6
month with clinical breast exam (CBE) and every year withmonth
with clinical breast exam (CBE) and every year withmammography (M)
and MRImammography (M) and MRI
Median f/u of 2.9 yearsMedian f/u of 2.9 years
Results:Results:
Sensitivity was 79.5% MRI, 33.3% M and 17.9% CBESensitivity was
79.5% MRI, 33.3% M and 17.9% CBE
Specificity was 89.8% MRI, 95% M and 98.1% CBESpecificity was
89.8% MRI, 95% M and 98.1% CBE Conclusion:Conclusion:MRI is more
sensitive than mammography inMRI is more sensitive than mammography
in
detecting tumors in women with an inherited
susceptibilitydetecting tumors in women with an inherited
susceptibilityto breast cancer.to breast cancer.
*Leach et al. Lancet. 2005.
Lehman et al. Radiology. 2007.
Kriege et al. NEJM. 2004.
Kuhl et al. J Clin Oncol. 2005.
Brittany Lee, HMS IVBrittany Lee, HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
31/34
Brittany Lee, HMS IVy ,
Dr. Gillian LiebermanDr. Gillian Lieberman
Our patient: SummaryOur patient: Summary 54F with average risk
for breast cancer had a benign findings on a54F with average risk
for breast cancer had a benign findings on a
screening mammogramscreening mammogram 4 months later, she p/w a
left breast mass4 months later, she p/w a left breast mass U/S
guided bx of the L lesion revealed IDC and DCISU/S guided bx of the
L lesion revealed IDC and DCIS Breast MRI of the contralateral
breast showed a suspicious lesionBreast MRI of the contralateral
breast showed a suspicious lesion
in the right posterior breastin the right posterior breast
MR-guided bx the R lesion revealed IDC and DCISMR-guided bx the R
lesion revealed IDC and DCIS No evidence of metastatic disease was
seen on full-body CT andNo evidence of metastatic disease was seen
on full-body CT and
bone scanbone scan Underwent bilateral mastectomy:Underwent
bilateral mastectomy:
Right total mastectomy with sentinel node biopsyRight total
mastectomy with sentinel node biopsy Left modified radical
mastectomy since grossly positive axillary nodesLeft modified
radical mastectomy since grossly positive axillary nodes
were found intraoperativelywere found intraoperatively
Pathology:Pathology: Right: IDC 0.9 cm, grade I with LVI
positive and 1:1 sentinel nodesRight: IDC 0.9 cm, grade I with LVI
positive and 1:1 sentinel nodes
positive. Histology was ER/PR+ and HER-2/neu negative.positive.
Histology was ER/PR+ and HER-2/neu negative. Left: IDC >7 cm,
grade 3 with LVI positive and 5:9 axillary nodesLeft: IDC >7 cm,
grade 3 with LVI positive and 5:9 axillary nodes
positive.positive.
Histology was ER/PR+ and HER-2/neu positive.Histology was ER/PR+
and HER-2/neu positive.
Case courtesy of Dr. Valerie Fein-Zachary
Brittany Lee, HMS IVBrittany Lee, HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
32/34
y ,y ,
Dr. Gillian LiebermanDr. Gillian Lieberman
ConclusionConclusion Does screening reduce breast cancer
mortality?Does screening reduce breast cancer mortality?
Uncertain since although 7 RCTs show that screening reduces
theUncertain since although 7 RCTs show that screening reduces
therelative risk of breast cancer mortality by 15-20%, not all of
these trialsrelative risk of breast cancer mortality by 15-20%, not
all of these trialswere randomized well and the absolute risk
reduction was only 0.05-were randomized well and the absolute risk
reduction was only 0.05-0.1%0.1%
How should average risk women be screened?How should average
risk women be screened? Guidelines suggest to consider mammography
screening at age 40 andGuidelines suggest to consider mammography
screening at age 40 and
recommends to start everyone at age 50.recommends to start
everyone at age 50. Digital mammography is more accurate at
detecting breast cancer thanDigital mammography is more accurate at
detecting breast cancer than
filmfilm
When do I use breast MRI?When do I use breast MRI? Screening for
women >20% lifetime risk of breast cancerScreening for women
>20% lifetime risk of breast cancer Evaluation of the
ipsilateral breast for synchronous lesions in a womenEvaluation of
the ipsilateral breast for synchronous lesions in a women
with a newly diagnosed breast cancer that is believed to be
morewith a newly diagnosed breast cancer that is believed to be
moreextensive than seen on standard imagingextensive than seen on
standard imaging
Evaluation of the contralateral breast for occult disease in
women withEvaluation of the contralateral breast for occult disease
in women witha unilateral breast cancer that had no clinical or
mammographica unilateral breast cancer that had no clinical or
mammographicabnormalities on the opposite sideabnormalities on the
opposite side
Women with mammographically occult primary disease with anWomen
with mammographically occult primary disease with anadenocarcinoma
of unknown primary site in the axillary nodesadenocarcinoma of
unknown primary site in the axillary nodes
Brittany Lee, HMS IVBrittany Lee, HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
33/34
y ,y ,
Dr. Gillian LiebermanDr. Gillian Lieberman
ReferencesReferences
Berry DA, et al. Effect of screening and adjuvant therapy on
mortality from breast cancer. NEJM. 2005. 353;Berry DA, et al.
Effect of screening and adjuvant therapy on mortality from breast
cancer. NEJM. 2005. 353;17: 1784-92.17: 1784-92. Boyd NF, et al.
Mammographic density and the risk and Detection of Breast Cancer.
NEJM. 2007. 356; 3:Boyd NF, et al. Mammographic density and the
risk and Detection of Breast Cancer. NEJM. 2007. 356; 3:
227-36.227-36. Fletcher SW. Report of the International Workshop
on Screening for Breast Cancer. J Natl Cancer Inst. 1993.Fletcher
SW. Report of the International Workshop on Screening for Breast
Cancer. J Natl Cancer Inst. 1993.
85; 20: 1644-56.85; 20: 1644-56. Fletcher SW. Screening average
risk women for breast cancer. 2007. UptoDate.Fletcher SW. Screening
average risk women for breast cancer. 2007. UptoDate. Glass AG, et
al. Breast cancer incidence, 1980-2006: combined roles of
menopausal hormone therapy,Glass AG, et al. Breast cancer
incidence, 1980-2006: combined roles of menopausal hormone
therapy,
screening mammography, and estrogen receptor status. J Natl
Cancer Inst. 2007. 99; 15: 1152-61.screening mammography, and
estrogen receptor status. J Natl Cancer Inst. 2007. 99; 15:
1152-61. Gotzsche PC and Nielsen M. Screening for breast cancer
with mammography. Cochrane Database ofGotzsche PC and Nielsen M.
Screening for breast cancer with mammography. Cochrane Database
of
Systematic Review. 2006. 4.Systematic Review. 2006. 4. Humphrey
LL, et al. Breast cancer screening: a summary of the evidence for
the U.S. Preventive ServicesHumphrey LL, et al. Breast cancer
screening: a summary of the evidence for the U.S. Preventive
ServicesTask Force. Ann Intern Med. 2002. 137; 5 Part 1:
347-60.Task Force. Ann Intern Med. 2002. 137; 5 Part 1: 347-60.
Jemal A, et al. Cancer statistics from SEER, CA Cancer J Clin.
2007. 55; 1: 43-66.Jemal A, et al. Cancer statistics from SEER, CA
Cancer J Clin. 2007. 55; 1: 43-66. Kriege M, et al. Efficacy of MRI
and mammography for breast-cancer screening in women with a
familial orKriege M, et al. Efficacy of MRI and mammography for
breast-cancer screening in women with a familial or
genetic predisposition. NEJM. 2004. 35; 5:427-37.genetic
predisposition. NEJM. 2004. 35; 5:427-37. Lehman CD, et al. MRI
Evaluation of the contralateral breast in women with recently
diagnosed breastLehman CD, et al. MRI Evaluation of the
contralateral breast in women with recently diagnosed breast
cancer. NEJM. 2007. 356; 13: 1295-1303.cancer. NEJM. 2007. 356;
13: 1295-1303. Mandelblatt J, et al. The cost-effectiveness of
screening mammography beyond age 65. Ann Intern Med.Mandelblatt J,
et al. The cost-effectiveness of screening mammography beyond age
65. Ann Intern Med.
2003. 139:835.2003. 139:835. Macura KJ, et al. Patterns of
Enhancement on Breast MR Images: Interpretation and Imaging
Pitfalls.Macura KJ, et al. Patterns of Enhancement on Breast MR
Images: Interpretation and Imaging Pitfalls.
Radiographics. 2006. 26:1719-34.Radiographics. 2006. 26:1719-34.
Pisano ED, et al. Diagnostic performance of digital vs. film
mammography for breast-cancer screening.Pisano ED, et al.
Diagnostic performance of digital vs. film mammography for
breast-cancer screening.
NEJM. 2005. 353; 17: 1773-83.NEJM. 2005. 353; 17: 1773-83.
Ravdin PM, et al. The decrease in breast-cancer incidence in 2003
in the United States. NEJM. 2007. 356;Ravdin PM, et al. The
decrease in breast-cancer incidence in 2003 in the United States.
NEJM. 2007. 356;
16: 1670-74.16: 1670-74. Salzmann P, et al. Cost-effectiveness
of extending screening mammography guidelines to include
womenSalzmann P, et al. Cost-effectiveness of extending screening
mammography guidelines to include women
40-49 years of age. Ann Intern Med. 1997. 127:955.40-49 years of
age. Ann Intern Med. 1997. 127:955. Saslow D, et al. American
cancer society guidelines for breast screening with MRI as an
adjunct toSaslow D, et al. American cancer society guidelines for
breast screening with MRI as an adjunct to
mammography. CA Cancer J Clin. 2007. 57; 2: 75-89.mammography.
CA Cancer J Clin. 2007. 57; 2: 75-89.
Brittany Lee, HMS IVBrittany Lee, HMS IV
-
8/14/2019 Radiological Screening for Breast Cancer
34/34
y ,y
Dr. Gillian LiebermanDr. Gillian Lieberman
AcknowledgementsAcknowledgements
Residents:Residents: Katie KrajewskiKatie Krajewski
Anne KimAnne Kim Senthil PalaniappunSenthil Palaniappun Andrew
BennettAndrew Bennett
Dr. Valerie Fein-ZacharyDr. Valerie Fein-Zachary Dr. Gillian
LiebermanDr. Gillian Lieberman Maria LevantakisMaria Levantakis