-
40 • Equine Health Update •
Indications• Investigation of pain causing lameness localised to
the fetlock region by clinical signs and/or diagnostic analgesia.•
Investigation of traumatic/penetrating wounds to the fetlock
region.• May be requested as part of a pre-purchase examination.•
Assessment of angular limb deformities.• Monitoring and
re-evaluation of pathology.
Patient preparation• Ensure the hair coat is clean as debris
will appear radiopaque on radiographs and may mimic or mask
abnormalities.• Radiography of this region is usually
well-tolerated. However, sedation will usually aid the acquisition
of well
positioned and good quality radiographs and reduce procedure
time, number of repeated acquisitions and risk to personnel and
equipment.
• The horse should be weight-bearing evenly on the forelimbs
with the metacarpus of the limb to be radiographed as vertical as
possible in both planes (i.e. when viewed from both the front and
the side). The same principles of positioning apply when
radiographing the hindlimb fetlock.
Radiographic views• There are four standard views of the fetlock
joint:
- Lateromedial - Dorsopalmar(/plantar) -
Dorsolateral-palmaro(/plantaro)medial oblique -
Dorsomedial-palmaro(/plantaro)lateral oblique
• There are various other additional views for identifying
specific lesions or visualising specific areas.• The technique for
radiography of metacarpophalangeal joint (forelimb) is described
below, however the same
principles apply for radiography of the metatarsophalangeal
joint (hindlimb).
Radiography of the Equine Fetlock Joint
IMVi Clinical teamLaura Quiney BVSc MRCVS
Holly Johnson BVSc Cert AVP MRCVS
-
41• Volume 21 Issue 2 | May 2019 •
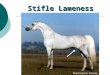
Lateromedial (LM)• The X-ray beam should be horizontal.• For a
true lateromedial the beam must be perpendicular to the
dorsopalmar axis of the leg at the level of the fetlock joint.
Palpating the medial and lateral epicondyles of the third
metacarpal bones may aid determination of the correct angle.
• Centre at the level of the distal condyles of the third
metacarpal bone.• Collimate to include the distal one third of the
metacarpus and at least the
proximal one half of the proximal phalanx in the image.
For a true lateromedial radiograph (left image), the sagittal
ridge of the third metacarpal bone (arrow) should be visible and
the condyles should be superimposed (arrowhead), allowing clear
visualisation of the joint space. If the radiograph is oblique
(right image) then sagittal ridge cannot be evaluated and
realignment of the beam relative to the fetlock is necessary to
achieve adequate diagnostic quality.
-
42 • Equine Health Update •
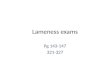
Flexed lateromedial• Compared with the weight-bearing
lateromedial, the flexed
lateromedial view offers better visualisation of the sagittal
ridge (arrow) of the third metacarpal bone and the dorsal surfaces
of the proximal sesamoid bones (arrowheads).
• To flex the fetlock, either rest the foot on a raised wooden
block or hold the toe with a lead gloved hand.
• To acquire a true lateromedial first ensure that the limb is
vertical and not rotated by viewing the position of the limb from
the front. The X-ray beam should be perpendicular to the
dorsopalmar direction of the fetlock.
• Acquire the radiograph by centering and collimating as for the
weight-bearing view (above).
For a flexed lateromedial radiograph to be of good diagnostic
quality the limb must first be assessed from the front to ensure
that the limb is both vertical and not rotated (left image).
A good quality flexed lateromedial radiograpgh allows the distal
aspect of the sagittal ridge (arrowhead) to be visualised.
-
43• Volume 21 Issue 2 | May 2019 •
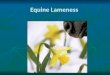
Dorsopalmar (DP) • Angle the X-ray beam 10° distally i.e.
dorso10°proximal-palmarodistal oblique.• Ensure the beam is
parallel to the dorsopalmar direction of the limb.• Centre at the
level of the condyles of the third metacarpal bone and
collimate.
N.B. A steeper distal angle of at least 15° is usually required
for the metatarsophalangeal joint (hindlimbs), i.e. dorso
15°proximal-plantarodistal oblique.
A horizontal X-ray beam will lead to superimposition of the
proximal sesamoid bones over the metacarpophalangeal joint which
will hinder evaluation (left image).
By angling 10° distally, the proximal sesamoid bones will be
superimposed proximal to the joint space, allowing improved
evaluation of the joint margins (right image).
-
44 • Equine Health Update •
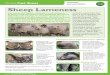
Dorsolateral-palmaromedial oblique (DLPMO)• Skylines the
dorsomedial and palmarolateral aspects of the fetlock joint, and
the
lateral proximal sesamoid bone.• The X-ray beam should be
horizontal, and at a 45° angle to the dorsopalmar axis
of the leg, aiming from a dorsolateral position towards a
palmaromedial position.• Centre at the level of the condyles of the
third metacarpal bone and collimate.
A marker to identify the limb being images should be placed, by
convention, to either the dorsal or lateral aspect of the limb.
This is essential not only to help identify which limb has been
imaged, but also to identify which are the medial and lateral
aspects of the limb and therefore which view has been acquired. In
this DLPMO image, the L marker is on the plantarolateral side of
the fetlock.
-
45• Volume 21 Issue 2 | May 2019 •
Dorsomedial-palmarolateral oblique (DMPLO)• Skylines the
dorsolateral and palmaromedial aspects of the fetlock
joint, and the medial proximal sesamoid bone.• Acquire as for
the DLPMO image, but from a dorsomedial position
aiming towards a palmarolateral position. Alternatively, to
avoid crossing the horse aiming from the palmarolateral position
towards a dorsomedial position will produce the same image.
In this DMPLO image, the L marker is on the dorsolateral side of
the fetlock. If this image was not labelled as a DMPLO view, it
could be easily identified as such because of the location of the
marker.
-
46 • Equine Health Update •
Additional radiographic views
Angled-down obliques (DPrM-PaDiLO and DPrL-PaDiMO)
• Useful for assessment of the palmar aspects of the medial or
lateral condyles of the third metacarpal bone because the proximal
sesamoid bones will be superimposed proximally to them (arrow).
• Acquisition is not as complex as it first seems- use the same
principles as for the comparable oblique view, but rather than
using a horizontal beam, angle down by 45°.
• The cassette should be positioned perpendicular to the
direction of the X-ray beam to minimise distortion.
Flexed dorsopalmar
• Used to further assess different aspects of the sagittal ridge
of the third metacarpal bone or the joint surface, for example if a
fracture is suspected.
• Acquire several tangential dorsopalmar views using different
proximal or distal angles to skyline different aspects of the joint
surface. The cassette should be positioned perpendicular to the
beam to minimise distortion.
-
47• Volume 21 Issue 2 | May 2019 •
Flexing the limb by resting the toe on a block can aid
acquisition of dorsodistal-palmaroproximal oblique views (example
of one tangential view, left image). The metacarpus should be
vertical. Flexed dorsopalmar radiographic image of a fetlock with a
sagittal fracture of the proximal phalanx.
Skyline of the metacarpophalangeal joint
• Dorsoproximal- dorsodistal oblique image
• Skylines the distal articular surface (sagittal ridge and
condyles) of the third metacarpal bone
• The limb should be flexed with the metacarpus vertical.
Position the cassette horizontally and angle the beam distally by
40-70°, depending on which area of the dorsal joint surface is to
be assessed.
-
48 • Equine Health Update •
1. Which radiographic view is best for visualisation of the
palmar aspect of the medial condyle of the third metacarpal
bone?
a. DPrM-PaDiLOb. Lateromedialc. DM-PaLOd. Flexed lateromediale.
DL-PaMO
2. Which of these statements regarding acquisition of a
dorsoplantar radiograph is usually correct?
a. The x-ray beam should be horizontalb. The x-ray beam should
be angled distally by 10°
(D10Pr-PlDiO)c. The x-ray beam should be angled proximally by
10°
(D10DiPlPrO)d. The x-ray beam should be angled distally by
15°
(D15Pr-PlDiO) e. The x-ray beam should be parallel with the
surface
the horse is standing on
3. Which of these lateromedial radiographs (right) is of
adequate diagnostic quality?
a. Image 01b. Image 02 c. Image 03 d. Image 04 e. Image 05
CPD QuestionsRadiography of the Equine Fetlock Joint
01 02 03
04 05
4. The marker (L) was placed to the lateral side of this left
fetlock. Which view is this?
a. DL-PaMOb. DPrL-PaDiMOc. DM-PaLOd. DPrM-PaDiLOe.
Lateromedial
AC/2119/19TO ANSWER: Download the Vet360 App or go
tocpdsolutions co.za/?re=onlinevets
-
49• Volume 21 Issue 2 | May 2019 •
5. Which of these statements is correct?
a. Using sedation for radiography is virtually never
required
b. Sedation will make fetlock radiography more difficult to
perform
c. Sedation will often help with the acquisition of good quality
radiographs in a shorter period of time
d. Sedation is likely to increase the number of repeated
acquisitions required
e. Sedation never helps with acquisition of well positioned
radiographs
6. Which of these radiographic views will offer the best
visualisation of the dorsal surfaces of the proximal sesamoid
bones?
a. DPb. Flexed DPc. LMd. Flexed LMe. DPrM-PaDiLO
7. In what instance would a flexed DP be particularly
useful?
a. Further assessment of the proximal sesamoid bones
b. Further assessment of the dorsal aspect of the condyles of
the third metacarpal bones
c. Further assessment of the sagittal ridge of the third
metacarpal bone
d. All of the abovee. None of the above
8. Why is collimation important for all views?
a. To reduce scatter and optimise exposure factors to achieve
optimum image quality
b. To prevent unwanted anatomy included in the radiographic
image
c. To optimise radiation safety for personnel performing
radiography
d. All of the above e. None of the above
9. When placing a marker in an image where does convention
require the marker to be placed in relation to the anatomy being
imaged?
a. Mediallyb. Distallyc. Proximally and medially d. Laterally e.
Proximally
10. What is the most important reason for the horse to be stood
standing squarely and weight bearing evenly through the limbs when
performing fetlock radiography?
a. If the horse is sedated, it will always be unsteady and may
fall over
b. Uneven weight bearing is likely to result in obliquity of the
anatomy relative to x-ray beam in the radiograph resulting in a
less diagnostic image
c. When the horse is not standing squarely it is difficult to
get both limbs in the same radiograph
d. When the horse is standing unevenly it is difficult to take a
full set of radiographs of the joint
e. Uneven weight bearing will always result in motion artefact
in your radiograph
-
50 • Equine Health Update •
Biography - Laura Quiney BVSc MRCVS
Laura qualified from the University of Bristol and subsequently
completed an equine orthopaedic internship at the Animal Health
Trust (AHT). Following a period working in ambulatory equine
practice she returned to the AHT as a Junior Clinician, focussing
on diagnostic imaging, lameness investigation and clinical
research. She is currently a Clinical Manager at IMV Imaging where
she develops educational content and provides CPD in diagnostic
imaging to veterinary surgeons throughout the UK.
Biography – Holly Johnson BVSc Cert AVP MRCVS
Holly graduated from Liverpool Veterinary school, UK in 2007.
She completed an equine internship at The Liphook Equine Hospital
in Hampshire, UK, before moving to Australia to work as a primary
stud vet in the Hunter Valley for Scone Equine Hospital. Her
passion for internal medicine and diagnostic imaging, particularly
ultrasound, led her to complete an RCVS Cert AVP when she returned
to the UK. Holly currently works as one of the in house clinical
team vets at IMV Imaging combining her love of ultrasound with
teaching, delivering a wide variety of ultrasound training to
veterinary clinicians in the UK and internationally.