Embed Size (px)
Citation preview

Radiation Safety in the Operation of Fluoroscopic X-ray Systems
Michael C. Talmadge Radiation Safety Officer
Lahey Hospital & Medical Center
September 2013
This document is intended to provide training pursuant to 105 CMR 120.405 (K) for Physicians’ that are not Board Certified in Radiology and operate fluoroscopic systems.

1
TABLE OF CONTENTS
Introduction ........................................................................................................... 2
Ionizing Radiation Fundamentals
Ionizing Radiation ............................................................................................... 2
Biological Effects .................................................................................................. 3
Fluoroscopic X-rays Systems
Fluoroscopic Systems ........................................................................................... 5
Techniques Factors ............................................................................................... 6
Automatic Brightness Control ........................................................................... 7
Boost/High Level Control ................................................................................... 8
Viewing Conditions ............................................................................................. 8
Mobile Units .......................................................................................................... 8
CT Fluoroscopy ..................................................................................................... 8
Operators ................................................................................................................ 9
Features
Magnification ........................................................................................................ 9
Pulsed Operation .................................................................................................. 10
Anti-scatter Grid ................................................................................................... 11
Last Image Hold .................................................................................................... 12
Virtual Collimation .............................................................................................. 12
Fluorography: High Quality, Recorded Fluoroscopy .................................... 12
Radiation Safety
Radiation Dose Indicators .................................................................................. 13
Radiation Safety: Occupational Exposure (Staff) ........................................... 17
Dose Reduction Guidelines ............................................................................... 21
References .............................................................................................................. 22

2
INTRODUCTION Fluoroscopy is an invaluable tool in the hands of a qualified practitioner; however, it also presents concerns with regard to radiation safety for patients and personnel. Additionally there a many applicable regulatory requirements, for which non-compliance cannot be tolerated. Compliance as well as the safety of patients and staff depends heavily on the competency of the fluoroscopy operator. IONIZING RADIATION FUNDAMENTALS Ionizing Radiation Radiation exists in many forms including visible light, microwaves, radio waves and x-rays. Ionizing radiation, such as x-rays, is that which is sufficiently energetic so that is capable of removing orbital electrons from molecules that it interacts with. The ionization of molecule produces a chemical change, such as the breaking of chemical bonds, which in turn can lead to biological effect, such as damage to cellular DNA. For this reason, ionizing radiation presents unique biological effects apart from other forms of radiation and necessitates special safety considerations.
H20 OH- + H+
Hydrolysis of a water molecule as a result of ionization. The production of ions or free radicals within a cell can lead to cellular damage.
Three quantities used to describe ionizing radiation are defined below along with common units. Exposure Roentgen (R) This quantity is generally used to express the results of a measurement of a radiation field in air. Exposure is often used to express the results of physics survey performed on a fluoroscopy system. Absorbed Dose Gray (Gy) or rad (1 Gy = 100 rad) This quantity is proportional to the amount energy deposited by radiation in a material or tissue per unit mass. Generally, the absorbed dose is the quantity of interest in determining whether or not a radiation-induced injury may occur. Absorbed Dose Equivalent Sievert (Sv) or rem (1 Sv = 100 rem) This quantity is proportional to the absorbed dose but is adjusted to reflect the relative health risk posed by a radiation exposure, specifically carcinogenic risk. Generally, this quantity is used for low levels of radiation exposure, such as occupational exposures. For occupational x-ray exposures, the absorbed dose equivalent is generally equal to the absorbed dose.

3
These three quantities are often referred to collectively as “exposure” or “dose” although it is important to understand that they are separate quantities that can be related to one another. The fluoroscopist will commonly encounter exposure quantities [R] and have the need to convert this value to absorbed dose [rad or Gy]. While there is no simple conversion, in many situations a rough estimate of 1 R = 1 rad or 1 R = 0.01 Gy can be used. Biological Effects Ionizing radiation can produce a wide range of biological effects dependent upon the magnitude of the radiation exposure and the type of tissues irradiated. These effects can be placed in one of two categories: Deterministic and Stochastic effects. Deterministic effects produce clinically observable changes for which causality can generally be clearly established. These effects generally occur with hours to months following a relatively large exposure and can vary in severity and latency depending on the magnitude of the exposure. The effects can be specific to tissues and organs involved or can manifest themselves systemically in the case an exposure to the whole body. Most importantly, a deterministic effect does not occur unless the radiation exposure exceeds certain thresholds for a given tissue, organ or organ system. In fluoroscopy the skin is considered to be the tissue for which the risk of a radiation-induced injury is the greatest. These injuries range from the relatively mild and temporary to the very severe and permanent. The threshold for an observable skin injury is commonly accepted to occur for an area of skin that receives an absorbed dose of approximately 2 Gy. Above this level, the type of injury escalates with exposure and can be expected at the threshold doses listed below:
Radiation-Induced Skin Injuries
Effect Threshold (mGy) Latency
Early Transient Erythema 2,000 Hours Temporary Epilation 3,000 3 Weeks Main Erythema 6,000 10 Days Permanent Epilation 7,000 3 Weeks Dry Desquamation 10,000 4 Weeks Invasive Fibrosis 10,000 Dermal Atrophy 11,000 >14 Weeks Telangiectasis 12,000 >52 Weeks Moist Desquamation 15,000 4 Weeks Late Erythema 15,000 6-10 Days Dermal Necrosis 18,000 >10 Weeks Secondary Ulceration 20,000 >6 Weeks
Adopted From: FDA, Avoidance of Serious X-ray Induced Skin Injuries to Patients during Fluoroscopically-Guided Procedures. 1994.

4
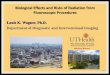
6-8 Weeks 16-21 Weeks 18-21 Months
Radiation-induced Skin Injuries from Fluoroscopy.
Skin-injury progression following an extended procedure involving coronary angiography, angioplasty and artery bypass-graft all within the same day. The dose to the affected skin area
was estimated to be above 20,000 mGy. (FDA) In fluoroscopy the area or areas of skin through which the x-ray beam enters the body is generally the tissue at the greatest risk of injury because these are the skin locations that will be maximally exposed. The injury thresholds listed above do not apply to the skin as a whole, rather it is the radiation dose received by a particular skin area that will determine if that skin area will be injured. Furthermore, radiation doses to the same skin areas during the past several months can also increases the radiosensitivity and susceptibility to injury. While biological repair processes following irradiation of the skin are considered to be underway for about two months following exposure, it is recommended that consideration be given to all significant skin exposures that have occurred within the past six to twelve months when assessing a patient’s potential for radiation induced skin injury. The Joint Commission considers a dose to a single area of skin exceeding 15 Gy from fluoroscopic procedures in a six to twelve month period to be reviewable sentinel event. Stochastic effects, on the other hand, generally refer to effects that are not unique to radiation exposure but exhibit an increase in occurrence with exposure to radiation. The nature of these effects is probabilistic, in which the magnitude of the exposure increases the probability of occurrence. Namely these effects are an increased risk of cancer and hereditary effects. While hereditary effects have only been observed in animal studies, it is well known that high levels of radiation exposure increases the likelihood of many cancers within an individual’s lifetime. The latent period between a given radiation exposure and the formation of a diagnosable cancer tends to be on the order of 5 to 20 years. While the evidence regarding carcinogenic effects is only conclusive for large exposures to radiation, the risk has been extrapolated to lower levels of radiation exposures in order to provide a conservative approach toward managing radiation exposure. The adoption of this assumption has been widespread and has led to the

5
paradigm that all radiation exposures should be minimized within reason and should be assess from a risk-benefit stand-point. This concept is embodied in the ALARA philosophy (As Low As Reasonably Achievable), which has been applied to occupational exposures to personnel as well as medical exposures to patients. FLUOROSCOPIC X-RAY SYSTEMS Fluoroscopic Systems X-rays are a form of ionizing radiation that are produced by a device, such as fluoroscopic system. An x-ray can be thought of as an individual packet of energy traveling through space: In this way an x-ray is characterized by its energy, commonly expressed in terms of kilo-electron-volt (keV). The x-ray generating component of a fluoroscopy system is referred to as an x-ray tube or x-ray source. This consists of a vacuum sealed vessel in which electrons are accelerated toward a positively charged metallic target. When these electrons strike the target a series of interactions occurs that stops the electrons and produces an x-ray spectrum of varying energy (keV). This x-ray spectrum is defined in terms of the accelerating voltage potential used and is commonly expressed as the kV or kVp. The tube housing, in which x-rays are produced, is shielded in such a way so that x-rays are only permitted to escape in one direction. The shielding also collimates the x-rays to form a useful x-ray beam directed at the image receptor. As the beam is emerging from the collimator it also passes through metallic filtration, the purpose of which is to remove low energy x-rays from the beam that will not contribute meaningfully to the formation of the image. Note that the beam, though collimated, diverges as a function of distance from the x-ray tube, as illustrated below.
The image receptor receives the x-ray beam, stopping it while capturing information about the incoming x-rays. Essentially the image receptor counts the number of x-rays that impinge upon its surface as a function of location, providing information describing the spatial distribution of the x-ray beam’s intensity. In this way, the image receptor can

6
be thought of as camera sensitive to x-rays. This information is then used to generate an image where the gray-scale of each displayed pixel is related to the number of x-rays that struck the corresponding point on the image receptor. When the x-ray beam traverses through the body different tissues, contrast media, or foreign objects attenuate the beam to varying degrees and thus the emerging x-ray beam conveys anatomical information. The image receptor is generally in the form of one of two technologies: an image intensifier or a flat-panel detector. These devices although different technologically serve the same purpose and are similar in clinical operation. The geometrical configuration of a fluoroscopy system is critical to both image quality and patient dose. The distance between the x-ray tube and the image receptor is referred to as Source-to-Image Distance (SID) while the distance between the x-ray tube and the surface of the patient is referred to as the Source-to-Skin Distance (SSD). Some systems, such as portable C-arms, generally have a fixed a SID (100cm) whereas others, such as an immobile C-arm found in a dedicated interventional area, may have variable SID. While both of these systems allow the SSD to be varied, other systems, such as those employing an under-the-table x-ray tube, may have a fixed SSD but variable SID. For most applications, it is advantageous from both an image quality and patient dose stand-point to maximize the SSD. Note that on a fixed-SID C-arm gantry system maximization of the SSD is achieved by positioning the image receptor as close to the patient as practically possible. Regulations prohibit an SSD of less than 38cm on stationary systems and 30cm on mobile systems. On most C-arms a spacer is affixed to the x-ray tube to prohibit an SSD less that 30cm. For fluoroscopy systems that are intended for specific surgical applications requiring an SSD less than 30cm the regulations provide a provision for use of an SSD of no less than 20cm. Mini C-arms, defined as having as SID of less than 45cm, are permitted to use an SSD of no less than 19cm for extremity imaging while an SSD of no less than 10cm for specific surgical applications is provisionally allowed for specific surgical applications. Techniques Factors The tube current expressed in mA (milli-amperes) and tube potential expressed in kVp or kV (kilovolt potential) are the fundamental operating parameters that govern the output of the x-ray tube. Tube current is often expressed in terms to mAs (milliampere-seconds) to express the current integrated over time. The tube current modulates the rate at which x-rays are produced (beam intensity) while the tube potential modulates both the rate at which x-rays are produced as well as the energy spectrum (also referred to as the beam quality) of the emitted x-rays. Both the beam quality and beam intensity affect the quality of the image produced as well as the radiation dose received by the patient. An increase in the tube potential (kV) tends to reduce patient dose at the expense of a decrease in image contrast; whereas an increase in tube current (mA) tends to improve the visibility of low-contrast objects at the expense of an increase in patient dose.

7
In many cases, an improvement in image quality generally comes at the cost of increased dose to the patient. Therefore, the output of the x-ray tube must be carefully managed so as to produce an image that will provide the required visual information while minimizing the dose to the patient. Automatic Brightness Control In most modern fluoroscopy systems the x-ray output is automatically adjusted in real-time through the use of Automatic Brightness Control (ABC) or Automatic Exposure Rate Control (AERC) features. During imaging this feedback-type system monitors the output of the image receptor and then adjusts the x-ray tube output based on an optimization algorithm in an attempt to achieve a given level of image quality. While some systems are also be capable of modifying other operational parameters such as pulse width and filtration, the modulation of the tube current (mA) and tube potential (kVp) are typically the primary means of adjusting the x-ray tube output. The ABC/AERC features will automatically adjust tube output based upon the composition and thickness of the part of the subject being imaged. For example, if a posterior-anterior view is being used and then the C-arm gantry is reposition to perform a lateral or oblique view the tube output will increase due to the increase in tissue thickness that the beam will have to travel through before reaching the image receptor. The tube potential and/or current will change in order to achieve this depending upon how the ABC/AERC feature is attempting to balance image quality versus patient dose. The ABC/AERC systems use algorithms to make such adjustments and in some cases will allow the user to indicate a preference toward dose reduction or image quality though the use of operational modes. When operating using ABC/AERC it is important to ensure that nothing unnecessary is left in the field of view as this provides additional beam attenuation and the x-ray source output will be automatically increased in an attempt to maintain image quality. This is especially true of dense or metallic items, such as lead aprons, that tend to attenuate x-ray very effectively. In situations where there are concerns about limiting the dose to an organ that does not need to imaged, such as the gonads, these organs should be outside the field of view, by field placement or use of collimation. While these areas could also be shielded, using a lead apron for example, care must be taken to ensure that the shielding material is not in the field of view as this will degrade image quality and increase the x-ray source output. It should also be noted that the placement of shielding over patient anatomy that is not in the field of view is generally unlikely to significantly impact the radiation dose to those areas. Patient extremities should also be repositioned whenever possible so that they are not in the field of view, unless the extremity itself needs to be imaged. This is of particular concern during lateral and oblique imaging of the chest. Image quality is generally measured in terms of image contrast and brightness and for the purposes of an ABC/AERC system is specified by the operational mode. This refers to the user-selected settings, such as normal, low dose, or boost/high level control

8
mode. While the availability of dose setting options varies depending on the fluoroscopy system being used, these options are used to indicate the level of image quality desired by the operator, which is inversely related to the dose received by the patient. For example, boost or high level control modes of operation will provide brighter images but the dose rate experienced by the patient may more than double while the low dose modes available on some fluoroscopy systems will spare the patient dose but will also reduce image brightness. Boost/High Level Control Boost/high level control mode of operation is generally operated using a separate foot pedal and is accompanied by an audible alarm due to fact that regulations permit the entrance skin dose to be twice the allowable limit for normal operation. Boost/high level control mode should be used sparingly and is generally only needed when imaging a very thick patient. Viewing Conditions Fluoroscopy images should be viewed under low ambient light conditions to maximize the operator’s visual perception. In fact, poor viewing conditions during the course of a procedure can lead the operator to increase x-ray output or result in increased radiation exposure to the patient and staff. Mobile Units Mobile fluoroscopy units can be used in areas, such as patient rooms and critical care units, when it is not practical to transport the patient to a procedural area. In these situations all uninvolved patients, staff and other persons should vacate the area during imaging. If an uninvolved patient cannot be moved then they should be positioned at least two meters away from the primary x-ray beam or protected by an apron or other shield of at least 0.25mm lead equivalence. CT Fluoroscopy CT fluoroscopy is dynamic three-dimensional imaging generally used in interventional procedures in which cross-sectional visualization or increased image contrast is desirable. In CT fluoroscopy the x-ray source rotates around the long axis of the patient in order to create a three-dimensional data set of the region of interest. While this is often performed using a diagnostic CT scanner, the procedure differs from a diagnostic exam in that the same region is imaged repeatedly, as needed. CT fluoroscopy is typically performed using reduced mA relative to diagnostic scans in order to reduce patient and staff exposures. However, staff exposure rates are typically higher as compared to two-dimensional fluoroscopy. Patient’s undergoing CT fluoroscopy are exposed to a highly collimated beam that rotates around them. Doses to the skin can in some cases approach the skin-injury thresholds, but the area of skin maximally exposed will form a band around the patient’s circumference. In all cases the number of scans should be minimized and the scan protocol should be specifically intended for CT fluoroscopy.

9
The use of CT fluoroscopy in which scanning may be performed repeatedly on the same region warrants an evaluation of the potential risks of injurious exposures. In situations where such a risk exists, dosimetric indicators should be developed in order to monitor patient doses in real-time. Low dose techniques, such as reduced mA, are also recommended. The O-arm is a specialized unit that allows for two-dimensional fluoroscopic operation as well as three-dimensional imaging capabilities. However, the three-dimensional imaging modality is not typically used in a repeated fluoroscopic-fashion; instead it is generally performed as a pre-planned scan. Operators Per Massachusetts regulations, the following personnel may operate fluoroscopic equipment under the conditions and limitations listed:
• Board-Certified Radiologists • Licensed Radiologic Technologists: For positioning purposes only. • Non-Radiology Physicians Annual radiation safety training required. Attending Physicians must have active fluoroscopy credentials through the Medical Staff Office. • Licensed Physician Assistants Additional training requirements, examination, practice agreement and supervision requirements, limited scope, active fluoroscopy credentials through the Medical Staff Office. (See RSO) • Nurse Practitioners May act as first assistant during cardiac catheterization procedures in accordance with 105 CMR 130.900 and Board of Registration in Nursing Advisory Ruling Number 0201 provided that the primary operator is a qualified Physician as defined above. Active fluoroscopy credentials through the Medical Staff Office required. (See RSO)
Personnel who are not listed above, such as nursing staff, are not permitted to operate fluoroscopic systems and should not engage in any activity that could be interpreted as such. FEATURES Magnification Many fluoroscopy systems are also capable of producing magnified images by either geometric or electronic means. Geometric magnification is achieved by increasing the distance between the image receptor and the patient, which for many systems requires

10
one to decrease the SSD, thereby using the divergence of the x-ray beam to create an enlarged projection of the subject. More commonly on modern systems, magnification is achieved electronically without the need to modify the SSD. Using either means, magnification nearly always increases the dose rate being experienced by the patient. Under electronic magnification the ABC/AERC system automatically increases x-ray tube output in order to produce an image of acceptable brightness, whereas in geometric magnification the reduction in SSD reduces the cross-sectional area of the beam at the point where it enters the patient, concentrating the deposition of energy into a smaller area of skin resulting in a higher dose to that area.
Geometric Magnification Electronic Magnification The table below presents measurements of the entrance skin dose for various modes of operation and magnification for a GE portable C-Arm. Note the trend of increasing dose rate with magnification and the effect of the three operational modes.
Entrance Skin Exposure Measurements GE OEC 9800+GSP C-Arm
Magnification Operational Mode
Tube Potential kVp
Current mA
Dose Rate mGy/min
None Low Dose 81 1.0 3.4
Normal 78 2.8 8.6 High Level 77 5.4 16.0
Mag. View One
Low Dose 83 1.5 5.0 Normal 80 4.2 13.5
High Level 80 8.8 28.4
Mag. View Two
Low Dose 81 2.0 6.4 Normal 80 6.0 18.5
High Level 81 14.0 42.3 Pulsed Operation Originally fluoroscopy systems produced a continuous output of x-rays and used a frame rate of 30 frames per second for display. Most modern systems use pulses of x-rays and will default to 30 pulses per second, analogous to the continuous operation of earlier units but with the advantage of reducing image blur. However, in doing this the

11
tube current (mA) had to be increased in order to provide sufficient image brightness as the x-ray output had been compressed into a pulsed wave form. Consequently, the advent of pulsed fluoroscopy itself did not, in general, lead to a reduction in patient dose. This concept is important to understand as it has implications on the use of variable pulsed fluoroscopy that is now available and often considered to be a dose reduction feature.
Pulse Height Modulation Pulse Width Modulation
Many modern fluoroscopic systems allow the operator to modulate the pulse rate used to perform imaging. As discussed above, the use of reduced pulse rates may appear to be a simple and reliable way to reduce the dose to the patient but this cannot always be assumed. While reducing the pulse rate can certainly reduce the dose to the patient, there are a few issues that one must be aware of when considering modulation of the pulse rate. As described above, a decrease in pulse rate often requires an increase in pulse height, which defines the tube current (mA) in order to maintain image quality. Additionally, some systems also allow for pulse width modulation, which defines the duration of each pulse. Indeed, many fluoroscopy systems are designed so that these adjustments of pulse height and possibly pulse width are made automatically when the pulse rate is changed. Both parameters can have the affect of increasing the dose to the patient, counteracting the dose reduction achieved by a lower pulse rate. Furthermore, some dynamic applications may not be well suited for lower pulse rates and may then require longer beam-on time to complete the procedure. These factors can potentially negate the dose savings that one hopes to achieve by using lower pulse rates and for this reason the fluoroscopist must ensure that a reduction in pulse rate is actually reducing the dose to the patient. This determination may be specific to the procedure, fluoroscopy system, patient and can be easily made on a unit equipped with DAP-based monitoring system, as discussed in more detail below. Anti-scatter Grid A grid placed in front of the face of the image receptor is used to enhance image quality by blocking scattered radiation and in some systems this grid is removable. The removal of the grid when imaging smaller patients, as in pediatrics, or thin anatomy can be an effective means to reduce patient dose with little to no appreciable degradation in image quality.

12
Last Image Hold Last Image hold refers to the modern fluoroscopy systems ability to continue to display the last captured image after the exposure is complete. This simple feature allows the operator to view an image without having to continuously expose the patient, encouraging the operator to make shorter exposures (i.e. less time on the pedal). Many systems also allow the operator to save images retrospectively using this feature. Virtual Collimation Some fluoroscopy systems allow the operator to collimate the x-ray beam at their discretion enabling them to limit the field of view to the anatomical region of interest. This is generally achieved by using the last image hold feature to position collimation that will be superimposed on the image. Not be confused with magnification, which provides a more detailed view of a smaller area, collimation simply limits the size of the x-ray beam reducing the extent of the patient being exposed. While this is valuable dose reduction technique, it is unlikely to have a significant effect on the peak skin dose to the skin area remaining in the field of view. The use of collimation to limit the field of view to the area of interest also tends to improve image quality and reduce staff doses. Fluorography: High Quality, Recorded Fluoroscopy Some systems are capable of recording a series of high quality images in succession. Such equipment is generally intended for a particular specialty, such as cardiac or neurological angiography, with features tailored for the intended application. These images are generally acquired using increased tube output to improve image quality with a single run consisting of many images. Cineangiography or, simply, cine is one such type of fluorography whereas digital subtraction angiography (DSA) is another technique in which images are digitally combined before and after the injection of contrast media in such a way that the background tissues are removed, improving the visualization of vascular structures. DSA, in turn, has led to the development of techniques, such as road mapping, in which an image produced using DSA can be used to overlay a map of the vasculature over live images to aid in intravascular navigation. Cone-beam computed tomography (CBCT) is also used on some systems to produce three dimensional angiographic data sets. Generally the use of fluorography comes at the expense of significantly increased patient (and staff) doses. While regulations limit the skin entrance exposure rates that can be produced during fluoroscopy, there are no such limitations on that produced during fluorographic operation. The dose rate experienced by the patient during fluorography has been reported to be up to ten to sixty times that experienced during normal fluoroscopy. As a result, the use of fluorography should only be used as needed and the quality of the images must be balanced against the resultant increase in dose. The frame rate used in fluorography is also an important parameter with respect the usefulness of the images and the dose. Cardiac angiography tends to require higher frame rates due to the motion of the heart, generally between 10 and 60 frames per second, whereas DSA of static structures can typically be achieved using lower rates from 0.5 to 4 frames per

13
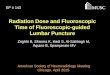
second. If possible, personnel should vacate the procedural area temporarily during fluorographic operation. RADIATION SAFETY Radiation Dose Indicators While it often difficult and impractical to make an accurate evaluation of patient doses received from fluoroscopy, there are practical dose indicators that can be used by the fluoroscopist to assess patient dose. Due to the fact that the skin area where the x-ray beam enters the patient is the region of maximum dose and is at the greatest risk of injury, the peak skin dose experienced by that skin area or areas is the quantity of greatest concern for the prevention of radiation-induced injury. In order to better understand the connection between radiation dose indicators and the risk of skin injury it is important to understand the following dosimetric quantities particular to fluoroscopy: Air Kerma at a Reference Point Gray (Gy) This quantity can be thought of as the absorbed dose to air, not including backscattered x-rays, that can be calculated for a reference point at a given distance from the x-ray source focal spot. This value is commonly displayed by fluoroscopy systems equipped with a dose-area-product (DAP) monitoring system. Entrance-Surface Absorbed Dose Gray (Gy) This is the calculated absorbed dose to the skin at the point where the x-ray beam enters the patient, including backscattered x-rays, assuming that the x-ray beam entry point on the patient does not change. This quantity can be estimated from the Air Kerma at a reference point. Peak Skin Dose Gray (Gy) The absorbed dose, including backscatter x-rays, to the area or areas of skin that are maximally exposed. This quantity depends on the amount of beam motion that occurs during the course of a procedure and ultimately determines the likelihood of a radiation-induced injury to that area of skin. It is very difficult to accurately determine and is not provided by any fluoroscopy system. The simplest indicator of patient dose is often the beam-on time. Modern systems display the cumulative beam-on time as well as provide an audible alarm that sounds every five minutes of accumulated beam-on time and must be manually reset by the operator. The beam-on time can be used to provide an estimate of entrance-surface absorbed dose using measurements that are taken during the annual physics survey. A summary of the results of this survey appears on a label attached to each fluoroscopy system. This label indicates the typical and maximum exposure rates that occur using ABC/AERC under normal mode of operation (excluding Boost/High Level Control) for a representative set of technique factors (mA and kV) and a reference SSD that is

14
intended to correlate to a typical clinical SSD. The reference point for these measurements is 30cm from the front of the image receptor on a C-arm system, per FDA and Massachusetts regulatory requirements, and does not include contributions from backscattered x-rays.
Sample Physics Survey Machine Label The exposure rates listed on this label are Air Kerma rates at the specified reference point. The Entrance-Surface Absorbed Dose rate can then be approximated from these quantities using the following equation (NCRP Report No. 168, 2010): Entrance-Surface Exposure Absorbed Dose Rate = Rate X 11.4 [mGy/min] [R/min] Using the information on the sample physics survey label above and this equation, it can be shown that the Entrance-Surface Absorbed Dose Rates at the reference point are typically 11.4 mGy/min and maximally 69.5 mGy/min. Given these values one could conclude that if fluoroscopy is performed without any beam motion (constant beam entry point on patient) then the threshold for skin injury of 2,000 mGy could be reached for beam-on times ranging from 28 minutes to 175 minutes. The fluoroscopist could narrow this range down by monitoring the ABC/AERC adjusted technique factors and comparing them to the values listed on the physics survey label. For example, if a fluoroscopist observed that a given procedure performed using ABC/AERC under normal fluoroscopy was generally imaging using 80kV and 3mA then they could conclude that the entrance skin dose rate was likely closer to that given by the typical value of 1.0 R/min (11.4 mGy/min). Alternatively, for a large patient or lateral/oblique view one could expect that the technique factors may approach those values associated with the maximum exposure rate, indicating that the entrance skin dose rate was moving closer to 6.1 R/min (69.5 mGy/min). One must bear in mind, however, that the accuracy of such estimates depends heavily on how well the actual SSD correlates to the SSD of reference point used in the physics survey measurements. While beam-on times combined with information provided from the annual physics survey can be a useful indicator, many modern systems are equipped with Dose-Area-Product (DAP) based monitoring systems, which are used to provide a more direct estimate of the Entrance-Surface Absorbed Dose. The DAP meter itself is an ionization
System: OEC 9800 Date Tested: 7/9/2013 Typical Exposure Rate: 1.0 R/min Technique: kV: 78 mA: 2.8 Maximum Exposure Rate: 6.1 R/min Technique: kV: 120 mA: 6.3

15
chamber located just outside the x-ray collimator that can effectively measure the dose rate as the beam exits the collimator. However, due to the divergence of the x-ray beam the dose decreases with increasing distance from the x-ray source focal spot. Intuitively, this can be explained by considering the effect of the divergence as the spreading of the same amount of radiation across greater cross-sectional area, thus reducing the dose (dose = energy/mass). In fact, the dose rate is inversely proportional to the square of the distance from the x-ray focal spot, as illustrated below. For this reason, it is preferable from a dose-savings stand-point to maximize the distance from the x-ray tube to the patient.
X-ray beam divergence causes the dose rate to decrease with increasing
distance from the x-ray source focal spot. A DAP based monitoring system essentially measures the dose experienced by the DAP meter and then provides a calculated Air Kerma to a given reference point, known as the Air Kerma reference point, that is intended to represent the point at which the beam will enter a patient. For isocentric C-arm systems, this reference point is typically located 15 cm away from the isocenter in the direction of the x-ray source. The isocenter of a C-arm is typically between 75cm and 80cm away from the x-ray source, placing the air kerma reference point between 60cm and 65cm from the x-ray source. These units typically display the cumulative Air Kerma at this reference point in mGy. The Entrance-Surface Absorbed Dose rate can then be approximated using the following equation (NCRP Report No. 168, 2010):

16
Entrance-Surface Cumulative Absorbed Dose = Air Kerma X 1.3 [mGy] [mGy] It is important to understand that the information from the annual physics survey, which is summarized on a label on each unit, and the information that is displayed by a system equipped with a DAP-based monitoring system correspond to two different reference points, that are unlikely to be equidistant from the x-ray source focal spot. Given that the dose rate varies considerably with distance, the location of this reference point and how well it corresponds to the actual point at which the beam enters the patient is critical. The figure below illustrates the location of the two reference points.
Dosimetric Reference Points: The regulatory compliance point is used during the annual physics survey (label) and is defined as 30 cm from the image receptor. Whereas the air kerma reference point used by
DAP meter-equipped system is defined as 15 cm from the isocenter in the direction of the x-ray source. For systems with adjustable SID, only the regulatory compliance point changes.
If a unit is equipped with DAP-based monitoring system then it is generally advisable to use the information it provides since it is based on the measured x-ray output. The cumulative Air Kerma value displayed by such a system can then be used to estimate the Entrance-Surface Absorbed Dose. If a system is not equipped a DAP-based monitoring system then the beam-on time in conjunction with the information from the physics survey should be used. Based on the technique factors being used (kV and mA) the fluoroscopist must compare them to that used in the physics survey to estimate a representative exposure rate. The estimated exposure rate can then be multiplied by the beam-on time to determine the cumulative exposure from which the Entrance-Surface Absorbed Dose can be calculated. Using either method, the accuracy of the estimation of Entrance-Surface Absorbed Dose depends heavily on how well the actual patient SSD correlates to that of the applicable reference point.

17
In theory, the Entrance-Surface Absorbed Dose can provide an estimate of the total dose delivered to the area of skin where the x-ray beam enters the patient if the beam entry point does not change which of course is not the typical scenario encountered in many fluoroscopically guided procedures. Consequently, the fluoroscopist must instead consider the peak skin dose, which is the dose to any single skin area. In practice, estimating this quantity is impractical in most cases and generally unnecessary. However, an understanding of the concept of peak skin dose and mindfulness towards minimizing it so as to reduce the risk of skin injury is imperative, especially in procedures where the Entrance-Surface Absorbed Dose may approach the 2,000 mGy skin injury threshold. Regulations require that a record of the absorbed dose to a patient’s skin be included in the medical record for each patient undergoing fluoroscopy. The estimates that can be provided by a DAP-based system can be used for this purpose. If a DAP-based estimate is not available, as on some older units, the information on the physics survey label should used to make an estimation of the skin dose using the method discussed earlier in this section. Additionally, the patient dose record should also identify the skin area or areas that were exposed. Furthermore, if there is reason to believe that a patient may have received an absorbed dose to an area or areas of skin equal to or greater than 2 Gy then a report must be made to the Radiation Safety Officer and the patient should receive follow-up instructions regarding skin care. Procedural areas in which these doses are expected have processes in place that fulfill these requirements; however, a fluoroscopist should contact the Radiation Safety Officer should there be questions as to reporting or patient follow-up requirements. Radiation Safety: Occupational Exposure (Staff) Fluoroscopic procedures are generally the largest source of occupational exposure in the medical setting. Unlike many other radiological procedures, fluoroscopy is dynamic imaging performed on-demand at the discretion of the operator and generally requires some staff to be in close proximity during imaging. While fluoroscopy is widely used in medicine and thus tends to involve large numbers or personnel from a variety of specialties, many of the procedures are limited in terms of their exposure potential to both the patient and staff. Certain interventional procedures, such Cardiac Catheterization and Angiography, are associated with a much larger exposure potential and are generally performed in dedicated fluoroscopy suites with permanent imaging installations. However, in all areas where fluoroscopy is performed attentiveness toward radiation safety is essential. The primary source of staff exposure involved in fluoroscopic procedures is the scattered x-rays that originate from the part of the patient being imaged. These x-rays interact with the tissue through which they are traveling in such a way that they are re-directed, leaving the primary x-ray beam. While scattered x-rays can be re-directed in any direction there is a tendency for them to be backscattered, meaning that they are redirected more than 90º from the original direction of travel. Consequently, the

18
intensity of scattered x-rays tends to be largest on the side of the patient nearest to the x-ray tube. For this reason, it is preferable to have the x-ray tube oriented beneath the patient when possible as this allows for the use of leaded drapes that can be hung off the table so as to protect staff. Overhead fluoroscopy, in which the x-ray source is positioned above the patient, can result in up to a three-fold increase in staff exposures in the absence of drapes or other shielding. Although there are some systems that specifically intended for overhead operation and may have overhead drapes, for most C-arm systems it is advisable to minimize overhead fluoroscopy from a staff exposure standpoint.
Beam Orientation has a significant impact of staff exposures. On most C-arm systems, it is preferable to orientate the gantry such that the x-ray source is beneath the patient where drapes can often be used to
effectively block backscattered and leakage x-rays. This reduces staff exposure to the backscattered radiation and, to a lesser extent, x-ray source leakage.
During imaging, there is also a small amount of radiation not in the primary x-ray beam originating from the x-ray tube itself (leakage) as well as from the backside of the image receptor as it stops the x-ray beam. Both of these sources of exposure are limited by regulation and are of secondary significance to the scattered radiation originating from the patient. Protective equipment, such as lead drapes and aprons, are highly effective in attenuating scattered x-rays encountered during fluoroscopy. Lead aprons should be worn by all personnel that will be present in the room during fluoroscopy and will shield 90-95% of the incoming scattered x-rays. Additional shielding in the form of thyroid collars, ceiling-mounted transparent shields and mobile shields can also be used as appropriate. Protective apparel, such as aprons, should be of 0.50mm lead equivalence and tested annually to ensure effectiveness. This apparel should be stored on sturdy hangers to avoid damaging the shielding material inside.

19
Recently the use of protective leaded eyewear has received increased attention out of concern for the radiosensitivity of the lens of eyes, specifically radiation-induced cataract formation, and in 2012 the use of such eyewear became a regulatory requirement in Massachusetts for personnel that are located directly at the patient table during imaging. This would generally apply to the physician and first assistant although may be advisable for other staff as well. Eyewear should be of at least 0.50mm lead equivalence, comfortable, and should provide side-shields or have close fitting curved frames so as to provide lateral protection. Eyewear of 0.75mm lead equivalence with a design that provides lateral shielding has been shown to reduce the exposure to the lens of the eye by up to approximately 90%, tending to be most effective when the wearer is facing the part of the patient being imaged. For some it may be worthwhile to obtain prescription leaded eyewear while others may prefer to use eyewear that will accommodate prescription lens worn underneath. Personnel radiation exposures are required to be as low as reasonably achievable (ALARA). This requires an ongoing vigilance and attention to radiation safety that allows personnel to take reasonable steps to reduce radiation exposure. The use of personnel protective equipment, such as lead aprons, provides substantial protection; however, personnel should also be mindful of their location with respect to the useful fluoroscopy beam and attempt to maximize the distance within reason between themselves and the x-ray beam. Substantial dose savings to staff can be achieved simply by backing away from the patient table during imaging or avoiding the area near the x-ray tube during lateral or oblique imaging. It is also in important to limit the personnel that will be present during fluoroscopic imaging to only those that have a justifiable need to be in the room. In some procedural areas, observation can be achieved from a control room and should be used when appropriate as an alternative to direct in-room observation. In general, it is not appropriate to allow individuals under the age of 18 to be present during fluoroscopy due to the radiation exposure, unless the individual is the patient. Occupational Dose Limits are annual regulatory limits that have been established to ensure that radiation exposure to personnel is limited to levels such that radiation exposure is comparable to other occupational hazards in safe workplace settings. Occupational dose limits are limited to work-related exposure and do not apply to patients. These annual limits are as follows in millirem (mrem): Deep Dose Equivalent (DDE) 5,000 mrem Shallow Dose Equivalent (SDE) 50,000 mrem Lens Dose Equivalent (LDE) 15,000 mrem The average person in the United States is estimated to receive approximately 310 mrem annually (DDE) from naturally occurring radiation originating from natural radioactivity and solar/cosmic radiation.

20
The developing fetus is particularly sensitive to radiation exposure and for this reason careful consideration must be given to pregnant personnel (and patients) that may be exposed to radiation. Pregnant personnel have the option to declare the pregnancy in writing to the radiation safety office, at which point a special fetal dose limit of 500 mrem for the entire gestation with a recommended monthly limit of 50 mrem. In response to a declaration of pregnancy, radiation exposure history is evaluated and changes to monitoring may be needed. Although most personnel would not require any restriction in their duties in order to ensure compliance with fetal dose limits, some colleagues may need to modify case-load or coverage accordingly. Declarations of pregnancy are optional as well as revocable and communications with the radiation safety office regarding pregnancy are confidential. Occupational radiation exposure is measured using personnel monitors. Generally these consist of “radiation badges” which are worn by personnel and are used to estimate the exposure received by the wearer. Such monitors must be exchanged regularly (quarterly or monthly depending on the procedural area) so that the old monitors can be sent back to the vendor for analysis. An electronic dosimetry system that allows for immediate assignment and analysis is also in use for short-term monitoring needs in some areas. All personnel that are present during fluoroscopy should be wearing appropriate radiation monitoring. Most personnel are monitored using a single monitor which should be worn on the outside of the leaded apparel at the collar-level. Some personnel in procedural areas where longer interventional procedures are routinely performed are monitored using two monitors, in which the second monitor is worn inside the leaded apparel at the waist level. The two badge system is used in these areas because it allows for a more accurate estimation of the deep dose equivalent to the whole body. Some fluoroscopy operators perform procedures that require them to have their hands in close proximity to the x-ray beam during imaging. These operators should request an extremity monitor in the form of a “ring badge.” If an operator’s hand or any other body part is exposed to the primary x-ray beam (in the field of view) then gloves or other shielding of at least 0.5mm lead equivalence must be used per regulation. However, it should be noted that the presence of this shielding material in the field of view will tend to increase the x-ray output on most modern units operating under ABC/AERC control increasing patient and staff exposure. It is therefore recommended that beam positioning and collimation be used whenever possible to ensure that an operator’s hands remain outside of the field of view. The personnel radiation monitoring program is managed by the radiation safety office and overseen by the radiation safety committee. All results are regularly reviewed and individuals with elevated or unusual results are contacted. Each procedural area has a badge coordinator that helps to facilitate the process of obtaining and exchanging monitors as well as posting results.

21
Dose Reduction Guidelines In general, the fluoroscopist seeks to minimize the radiation exposure to patient and to staff while maintaining adequate image quality for the procedure at hand. Patient dose reduction consists of two distinct considerations: The overall radiation exposure to the patient should be minimized, but more importantly in preventing skin injury, the peak skin dose to those skin areas that are beam entry points must also be carefully managed. For example, minimizing beam-on time can reduce the dose to the patient overall and reduce the peak skin dose whereas using collimation to limit the field of view likely decreases the overall dose to the patient but is not likely to produce appreciable reductions to the peak skin dose for the area still in the field of view. Some strategies and techniques simultaneously can further each of these goals while others have both costs and benefits. With respect to radiation dose management in fluoroscopy, it is generally prudent to make the avoidance of peak skin doses that may produce skin-injuries the top priority. The following table provides a list of techniques and strategies and summarizes the effects of each.
Technique / Strategy Effects Patient Dose Staff Dose Image Quality
Minimize Beam-on Time Decrease Decrease N/A Maximize SSD Decrease N/A Improve
Dose Spreading (Multiple Beam entry points)
Decreases Peak Skin doses N/A N/A
Minimize Overhead Fluoroscopy N/A Decrease N/A
Minimize Lateral/Oblique Views Decrease Decrease N/A
Use of Pulsed Mode (Decreasing the frame rate)
Potential Decrease (Must be verified)
Potential Decrease
May reduce temporal resolution
Use of Low Dose Mode Decrease Decrease Ay reduce image quality.
Minimize use of Magnification Decrease Decrease N/A
Use of beam collimation to limit the field of view
Decreases area of skin exposed and total exposure to patient. Does not
significantly reduce the peak skin dose in the field of view.
Decrease (less scatter)
May improve image quality.
Minimize use of Fluorography (Cine, DSA) Decrease Decrease N/A
Low Light Viewing Potential Decrease Potential Decrease
Improved Viewing

22
References American Association of Physicists in Medicine. Report No. 58, Managing the Use of Fluoroscopy in Medical Institutions. October 1998. FDA, Avoidance of Serious X-ray-Induced Skin Injuries To Patients During Fluoroscopically-Guided Procedures. September 9, 1994. Mahadevappa, M. Fluoroscopy: Patient Radiation Exposure Issues. July 2001 RadioGraphics, 21, 1033-1045. National Council on Radiation Protection & Measurements. Report No. 168, Radiation Dose Management For Fluoroscopically-Guided Interventional Medical Procedures. July 21, 2010. Pooley, R.A. et al. The AAPM/RSNA Physics Tutorial for Residents – Digital Fluoroscopy. RadioGraphics 2001; 21:521-534. Wagner L.K. et al. Minimizing Risks from Fluoroscopic X-Rays. Partners in Radiation Management, Fourth Edition, LTD. 2004.