Embed Size (px)
Citation preview

Quick fixation of skin grafts
Frederick Kaempffe, MD, and Clayton A. Peimer, MD, BufSalo, N.Y.
Rigid fixation of a skin graft to its recipient bed is an essential step in achieving survival during the first week until vascularization and union are relatively ad- equate. ‘3 * Numbers of techniques and modifications of the original British “stent” have been described to at- tempt to produce firm, even, and secure pressure on the graft site. 2-7 We have found that all are not uniformly predictable, nor simple; this led us to search for a method that would be rapidly precise and effective for most circumstances.
Technique
Split- or full-thickness skin graft is harvested and applied to the prepared recipient bed, and the edges are
From the Department of Orthopaedic Surgery, State University of New York at Buffalo, School of Medicine, Buffalo, N.Y.
Received for publication May 22, 1989; accepted in revised form April 30, 1990.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Reprint requests: Clayton A. Peimer, MD, Millard Fillmore Hospital, 3 Gates Circle, Buffalo, NY 14209.
3/l/22391
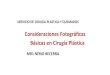
secured with a few skin staples (or sutures, as the sur- geon prefers). On convex recipient sites (e.g., finger- tips, dorsum of hand), a stent is rapidly made by sta- pling Adaptic (Johnson & Johnson Products Inc., New Brunswick, N.J.) gauze a few millimeters back from one edge of the graft, pulling tightly, then laying it across the graft, and securing it to the other edge by stapling it into normal skin (Fig. 1). This lubricated open mesh allows passage of fluid from the graft site.
For concave surfaces (e.g., the midpalm), the stent is made as an Adaptic-cotton sandwich: two sheets of Adaptic are stapled together as a single unit to normal skin along one edge of the graft (as previously). The bottom piece of gauze is gently placed onto the graft and allowed to contour into the concavity (it is not pulled, stretched, or tented). Next, cotton balls (or sheets) previously soaked in mineral oil and wrung out are placed onto the bottom layer of gauze (Fig. 2). Finally, the top sheet of gauze is pulled tightly over the cotton balls (which have now given the site a convex contour) and stapled to the opposite edge of the graft, resulting in even pressure on the bed beneath. Addi- tional dressings or splints are completed in the usual manner, as appropriate for the anatomic region and diagnosis.
Fig. 1. Skin graft secured to fingertip with skin staples. On this convex surface, Adaptic is next stapled tightly across the graft to stent it in place.
THE JOURNAL OF HAND SURGERY 761

762 KaempfSe and Peimer
The Journal of
HAND SURGERY
** <-
Cotton fluff
/--- /
Top layer Adaptic*
Bottom layer Adaptic’
concave surface
Fig. 2. For concave surfaces, a layer of Adaptic is stapled to one edge and placed lightly onto the graft (not pulled tightly); cotton sheets (or balls) previously soaked in mineral oil serve as stents, over which a second layer of Adaptic is then tightly stapled.
Discussion
The use of this sturdy, open weave nonadherent
gauze permits passage of fluid from the graft bed. The
stent is both rapidly applied and quite secure, a fact that protects the graft even in the most young and vig- orous, or careless, patients. When outer dressings and splints are removed, there is stiI1 no chance of inad- vertently dislodging the skin graft until the staples are
removed. Indeed, stent removal is also simple and be- nign, providing the surgeon has not gotten carried away with the stapler. To eliminate the need for staple re-
moval in a young child, (e.g., congenital syndactyly) we substitute 5-O plain catgut sutures; and let the parents
soak-off the stent, when used on a convex surface with- out a cotton sandwich. The minor variation in technique for convex and concave surfaces assures firm, even
pressure for either to give uniform apposition of the graft to its bed.
Our technique is not new and may represent merely a modem extension of Bunnell’s purported method of securing skin grafts to convex recipient surfaces by over-suturing silk butterfly netting onto the bed-a
story told by the late Richard J. Smith, MD, when he
taught his own modifications of that technique, which forms the basis for this method.
We thank John A. Nyquist, associate medical illustrator, University of Buffalo, for his assistance.
1.
2.
3.
4.
5.
6.
7.
REFERENCES
Rudolph R. Healing processes in skin grafts. Surg Gynecol Obstet 1973;136:641-54. Rudolph R. Skin grafting. In: Goldwyn RM, ed. The unfavorable result in plastic surgery. 2nd ed. Boston: Little Brown & Company, 1984: 143-9. Bunnell S. Skin and flexion contractures. In: Surgery of
the hand. Philadelphia: JB Lippincott, 1944: 159-60. Daniller A. Skin grafts. In: Chapman MW, ed. Operative orthopaedics. Philadelphia: JB Lippincott, 1988: 1952.
Freeman B. The use of the pocket stapler in surgery. Plast Reconstr Surg 1962;30(2):289-91.
Marble H. Open injuries and their management. In: The hand: A manual and atlas for the general surgeon. Phil- adelphia: WB Saunders, 1960:148. Shively RE, Northington JW, Williamson GB, Bum RA. A simple skin graft dressing following early graft inspec- tion. Ann Plast Surg 1981;7(4):334-5.









![Immunological challenges associated with artificial skin …...Transplanting autologous skin grafts [4, 5] is the therapeutic approach of choice that successively reform the skin,](https://img.dokumen.tips/doc/110x75/610d210bde142e0c054be240/immunological-challenges-associated-with-artificial-skin-transplanting-autologous.jpg)