Embed Size (px)
Citation preview

Queensland University of Technology
School of Nursing
Centre for Nursing Research
Family outcomes following patient transfer from
Intensive Care: an educational intervention
Marion Lucy Mitchell
RN, RM, CHN, BN (Hon), GCert (Higher Education).
This dissertation is submitted to fulfil the requirement for the award of
Doctor of Philosophy at Queensland University of Technology.
2003

ii
KEYWORDS
Family members Intensive Care Transfer Anxiety ‘Uncertainty in illness’ Satisfaction Pre-transfer education General System Theory Adult Learning Theory

iii
ABSTRACT
Introduction
The purpose of this study was to improve family members’ transfer from Intensive
Care. A structured pre-transfer educational method of patient transfer was
introduced and evaluated.
Background of the study
Many studies have documented the needs of family members whilst in intensive
care units (ICU) but few have evaluated interventions to support meeting these
needs. No studies have documented ‘uncertainty in illness’ levels of family
members around transfer from ICU or the relationship between uncertainty and
anxiety.
Method
The study used a quasi-experimental pre-test, post-test non-equivalent control
group design based on the General System Theory (von Bertalanffy, 1972). There
were four phases to the study with the intervention grounded in Knowles’ Adult
Learning Theory (1980).
Family members of patients in an ICU were purposively allocated to a control
(n = 80) and intervention group (n = 82). A pre-test, post-test strategy was used
with data from the control group collected first and once completed, the
intervention was introduced into the ICU. The intervention group data were then
collected using the same data collection tools. The intervention group

iv
experienced a transfer method designed to improve communication with the bed-
side nurse in ICU whereas the control group received existing ad hoc transfer
methods.
Participants were surveyed before and after transfer using Spielberger et al.’s state
anxiety inventory and Mishel’s ‘uncertainty in illness’ scale. Demographic data
were collected for both patients and family members together with family
members’ satisfaction with the transfer process they experienced. At the
completion of the study, intensive care nurses (n = 40) were surveyed to assess
their perception of the efficacy of the intervention.
Results
Three factors were found to significantly affect levels of ‘uncertainty in illness’
and these included state anxiety scores (F = 50.9, p < .000), the relationship of the
family member to the patient (F = 2.9, p = .022), and the unexpected nature of the
admission (F = 23.09, p < .000). These factors accounted for 33% of the variance
of ‘uncertainty in illness’ scores.
State anxiety levels were significantly affected by the degree of family social
support (F = 10.0, p = .002) and uncertainty as previously mentioned. State
anxiety reduced significantly following transfer for both groups and ‘uncertainty
in illness’ reduced significantly for the intervention group (t = 2.21, p = .03).
When controlled for pre-transfer levels, however, there was no significant
reduction in the intervention group when compared with the control group.

v
‘Uncertainty in illness’ for the intervention group reduced, however, whereas
scores for the control group did not.
The intervention group experienced significantly higher levels of satisfaction with
transfer (Z = -2.43, p = .015) and felt significantly better prepared for transfer
(Z = -3.26, p = .001) than did the control group. The vast majority of ICU nurses
(90.6%) thought the intervention provided a useful framework for discussing the
patient’s condition with family members and 94% thought it should be introduced
for all transfers from ICU.
Conclusions
Uncertainty is significantly related to state anxiety in this sample. Previous
research suggests that individual’s coping ability is affected by both anxiety and
‘uncertainty in illness’ which limit their adaptation to the new ward situation.
This results in relationship disturbances and psychological distress (Mishel, 1981)
at a time when patients rely on family support. The intervention reduced
uncertainty and improved family members’ satisfaction with the transfer process
by improved communication between family members and ICU nurses. The
intervention was fully endorsed and supported by ICU nurses who recommended
its introduction for all future transfers.

vi
TABLE OF CONTENTS
KEYWORDS.......................................................................................................................................I
ABSTRACT......................................................................................................................................III
LIST OF TABLES...........................................................................................................................XI
LIST OF FIGURES......................................................................................................................XIII
STATEMENT OF ORIGINAL AUTHORSHIP ......................................................................XIV
DECLARATION OF ENROLMENT......................................................................................... XV
ACKNOWLEDGEMENTS.........................................................................................................XVI
CHAPTER 1: INTRODUCTION.................................................................................................... 1 1.1 CLINICAL RESEARCH PROBLEM........................................................................................... 2 1.2 PROJECT SUMMARY ............................................................................................................. 4
1.2.1 Assumptions ................................................................................................................ 5 1.2.2 Research Questions .................................................................................................... 5 1.2.3 Research Aims and Objectives................................................................................... 6
1.3 STRUCTURE OF THE THESIS.................................................................................................. 7
CHAPTER 2: LITERATURE REVIEW........................................................................................ 9 2.0 INTRODUCTION..................................................................................................................... 9 2.1 GENERAL SYSTEM THEORY IN CONTEXT .......................................................................... 11 2.2 CRITICAL ILLNESS .............................................................................................................. 17 2.3 ‘UNCERTAINTY IN ILLNESS’............................................................................................... 20 2.4 ANXIETY............................................................................................................................. 25 2.5 NEEDS OF FAMILIES ........................................................................................................... 29 2.6 TRANSFER FROM INTENSIVE CARE .................................................................................... 35 2.7 KNOWLES’ ADULT LEARNING THEORY............................................................................. 43 2.8 SUMMARY OF LITERATURE ................................................................................................ 45 2.9 CONCEPTUAL FRAMEWORK ............................................................................................... 47
CHAPTER 3: METHODOLOGY................................................................................................. 51 3.0 INTRODUCTION................................................................................................................... 51 3.1 STUDY DESIGN ................................................................................................................... 52 3.2 RESEARCH STRATEGY........................................................................................................ 52 3.3 PHASE ONE......................................................................................................................... 55
3.3.1 Research Design ....................................................................................................... 55 3.3.1.1 Expert panel ......................................................................................................... 55 3.3.1.2 Family member.................................................................................................... 60
3.3.2 Sampling Framework............................................................................................... 61 3.3.2.1 Population ............................................................................................................ 61

vii
3.3.3.2 Sample .................................................................................................................. 63 3.3.3.3 Inclusion criteria ................................................................................................. 64
3.3.4 Data Collection and Analysis .................................................................................. 64 3.4 PHASE TWO: BROCHURE DEVELOPMENT .......................................................................... 66
3.4.1 Sample....................................................................................................................... 67 3.4.2 Inclusion Criteria ..................................................................................................... 68 3.4.3 Data Collection and Analysis .................................................................................. 68
3.5 PHASE THREE..................................................................................................................... 69 3.5.1 Research Design....................................................................................................... 69
3.5.1.1 Pilot ....................................................................................................................... 71 3.5.1.2 Control Group ..................................................................................................... 72 3.5.1.3 Intervention Phase Preparation ........................................................................ 75
3.5.2 The Intervention....................................................................................................... 76 3.5.2.1 Recruitment of ICU nurses ................................................................................ 79 3.5.2.2 The Intervention Phase....................................................................................... 82
3.5.3 Sampling Framework............................................................................................... 83 3.5.3.1 Control Group ..................................................................................................... 83
Population.......................................................................................................................... 83 Sample ........................................................................................................................... 83
3.5.3.2 Intervention Group ............................................................................................. 84 Population.......................................................................................................................... 84 Sample ........................................................................................................................... 84
3.5.3.3 Inclusion criteria for control and intervention groups ................................... 85 3.5.4 Variables ................................................................................................................... 85 3.5.5 Procedure for data collection .................................................................................. 86 3.5.6 Instruments ............................................................................................................... 88
3.5.6.1 Acute Physiology, Age, Chronic Health Evaluation III (APACHE III) ....... 88 3.5.6.2 State Trait Anxiety Inventory for Adults (STAI)............................................ 89 3.5.6.3 Parent’s Perception Uncertainty Scale – Family (PPUS-FM) ...................... 93 3.5.6.4 Rand and Medical Outcomes Study - Social Support Survey ....................... 96 3.5.6.5 Family Members’ Degree of Satisfaction ........................................................ 97
3.6 PHASE FOUR....................................................................................................................... 99 3.6.1 Research Design....................................................................................................... 99 3.6.2 Sampling Framework............................................................................................. 100
3.6.2.1 Population .......................................................................................................... 100 Sample ......................................................................................................................... 100
3.6.2.2 Inclusion Criteria .............................................................................................. 100 3.6.3 Procedure for Data Collection............................................................................... 101 3.6.4 Data Analyses ......................................................................................................... 101
3.7 ANALYTICAL PROCEDURES FOR THE STUDY ................................................................... 102

viii
3.7.1 Sample and the questionnaire ............................................................................... 103 3.7.2 Demographic Variables.......................................................................................... 103
3.8 RESEARCH QUESTIONS STATISTICAL TESTS.................................................................... 104 3.8.1 Question 1. .............................................................................................................. 104 3.8.2 Question 2 ............................................................................................................... 105 3.8.3 Question 3 ............................................................................................................... 107 3.8.4 Question 4 ............................................................................................................... 108 3.8.5 Question 5 ............................................................................................................... 111
3.9 ETHICAL CONSIDERATIONS.............................................................................................. 112 3.9.1 Potential Risks ........................................................................................................ 113
3.10 CHAPTER SUMMARY......................................................................................................... 114
CHAPTER 4: DESIGNING THE INTERVENTION............................................................... 115 4.0 INTRODUCTION................................................................................................................. 115 4.1 PHASE ONE- EXPERT PANEL OF CRITICAL CARE NURSES................................................. 115
4.1.1 Questionnaire ......................................................................................................... 115 4.1.1.1 Transfer Plans.................................................................................................... 119 4.1.1.2 Ward Orientation .............................................................................................. 119 4.1.1.3 Staff Orientation................................................................................................ 119 4.1.1.4 Ward Expectations ............................................................................................ 120 4.1.1.5 Reassurance and Support................................................................................. 120 4.1.1.6 Summary of expert panel questionnaire ........................................................ 121
4.1.2 Expert panel’s focus group discussion.................................................................. 122 4.1.2.1 Summary of expert panel focus group discussion ......................................... 125
4.2 PHASE ONE: FAMILY MEMBERS’ DATA COLLECTION ...................................................... 125 4.2.1 Summary of family member data .......................................................................... 127
4.3 PHASE TWO ...................................................................................................................... 128 4.3.1 Teachers .................................................................................................................. 128 4.3.2 Senior Nursing Personnel...................................................................................... 129
4.4 SUMMARY OF INTERVENTION DESIGN.............................................................................. 129
CHAPTER 5: DESCRIPTION OF THE SAMPLE .................................................................. 131 5.0 INTRODUCTION................................................................................................................. 131 5.1 FAMILY MEMBER DEMOGRAPHICS .................................................................................. 132
5.1.1 Age of family members........................................................................................... 132 5.1.2 Gender of family members..................................................................................... 133 5.1.3 Educational level of family members .................................................................... 133 5.1.4 Relationship to patient ........................................................................................... 134 5.1.5 Previous admission or visit to an ICU................................................................... 134 5.1.6 Nationality of family members............................................................................... 135
5.2 PATIENT DEMOGRAPHICS................................................................................................. 136 5.2.1 Age of patients ........................................................................................................ 136

ix
5.2.2 Gender of patients .................................................................................................. 137 5.2.3 Expected or unexpected admission to ICU........................................................... 137 5.2.4 Degree of illness of patients................................................................................... 138 5.2.5 Reason for admission to ICU................................................................................. 139 5.2.6 Length of patient stay in ICU ................................................................................ 140
5.3 SUMMARY OF SAMPLE...................................................................................................... 140
CHAPTER 6: RESULTS.............................................................................................................. 142 6.0 INTRODUCTION................................................................................................................. 142 6.1 QUESTION 1- LEVEL OF UNCERTAINTY ........................................................................... 142 6.2 QUESTION 2 - UNCERTAINTY AND ANXIETY.................................................................... 143
6.2.1 Question 2.1 ............................................................................................................ 143 6.2.2 Question 2.2 ............................................................................................................ 145 6.2.3 Question 2.3 ............................................................................................................ 149 6.2.4 Summary of Question 2 ........................................................................................ 151
6.3 QUESTION 3: INTERVENTION’S EFFECT ON UNCERTAINTY AND ANXIETY ....................... 152 6.3.1 Summary of Question 3 ......................................................................................... 158
6.4 QUESTION 4: FAMILY MEMBERS’ PERCEPTION OF TRANSFER.......................................... 158 6.4.1 Question 4.1 ............................................................................................................ 158 6.4.2 Question 4.2 ............................................................................................................ 160 6.4.3 Question 4.3 ............................................................................................................ 161 6.4.4 Question 4.4 ............................................................................................................ 162 6.4.5 Question 4.5 ............................................................................................................ 166 6.4.6 Summary of Question 4 ......................................................................................... 168
6.5 QUESTION 5 - ICU NURSES’ PERCEPTION OF INTERVENTION .......................................... 169 6.5.1 Question 5.1 ............................................................................................................ 169 6.5.2 Question 5.2 ............................................................................................................ 170 6.5.3 Question 5.3 ............................................................................................................ 170 6.5.4 Summary of Question 5 ......................................................................................... 173
6.6 SUMMARY OF RESULTS .................................................................................................... 173
CHAPTER 7: DISCUSSION........................................................................................................ 176 7.0 INTRODUCTION................................................................................................................. 176 7.1 PHASE ONE....................................................................................................................... 177 7.2 PHASE TWO ...................................................................................................................... 181 7.3 QUESTION 1...................................................................................................................... 182 7.4 QUESTION 2...................................................................................................................... 186
7.4.1 Question 2.1 ............................................................................................................ 186 7.4.2 Question 2.2 ............................................................................................................ 189 7.4.3 Question 2.3 ............................................................................................................ 190
7.5 QUESTION 3...................................................................................................................... 191 7.6 QUESTION 4...................................................................................................................... 197

x
7.6.1 Question 4.1 ............................................................................................................ 197 7.6.2 Question 4.2 ............................................................................................................ 198 7.6.3 Question 4.3 ............................................................................................................ 200 7.6.4 Question 4.4 ............................................................................................................ 201 7.6.5 Question 4.5 ............................................................................................................ 203
7.7 QUESTION 5...................................................................................................................... 205 7.7.1 Question 5.1 ............................................................................................................ 205 7.7.2 Question 5.2 ............................................................................................................ 206 7.7.3 Question 5.3 ............................................................................................................ 206
7.8 STUDY’S FINDINGS IN RELATION TO CONCEPTUAL FRAMEWORK ................................... 207 7.9 LIMITATIONS .................................................................................................................... 208
CHAPTER 8: CONCLUSIONS................................................................................................... 210 8.0 INTRODUCTION................................................................................................................. 210 8.1 RESEARCH QUESTIONS ..................................................................................................... 212
8.1.1 Question 1 ............................................................................................................... 213 8.1.2 Question 2 ............................................................................................................... 213 8.1.3 Question 3. .............................................................................................................. 215 8.1.4 Question 4 ............................................................................................................... 216 8.1.5 Question 5 ............................................................................................................... 218
8.2 FUTURE DIRECTION .......................................................................................................... 219 8.2.1 Recommendations for practice .............................................................................. 219 8.2.2 Recommendations for education ........................................................................... 220 8.2.3 Recommendations for research ............................................................................. 222
8.3 SUMMARY ........................................................................................................................ 223 APPENDICES.................................................................................................................................. 225
Appendix A – Expert Panel Information and Consent Form.............................................. 225 Appendix B: Expert Panel Questionnaire............................................................................. 230 Appendix C: Phase One Information for Family Members. ............................................... 232 Appendix D: Phase One Family Members’ Questionnaire ................................................. 234 Appendix E: Pre-Transfer Brochure..................................................................................... 236 Appendix F: Phase Two - Information for Teachers.......................................................... 238 Appendix G: Two – Teachers’ Feedback Sheet.................................................................... 240 Appendix H: Phase Three – Information and Consent Form for Family Members. ....... 241 Appendix I: Phase Three and Four- Information and Consent Form for Nurses. .......... 245 Appendix J: Phase Three Family Members’ Questionnaire before Transfer.................... 250 Appendix K: Phase Three – Family Members’ Questionnaire after Transfer................... 256 Appendix L: Phase Four ICU Nurses’ Questionnaire........................................................ 264
REFERENCES................................................................................................................................. 265

xi
LIST OF TABLES
TABLE 4.1: Expert panel questionnaire responses ............................................ 118
TABLE 4.2: Phase One: family members’ relationship to patient ...............................125
TABLE 4.3: Factors important to family members in Phase One .................................127
TABLE 5.1: Age of family members ............................................................................132
TABLE 5.2: Gender of family members .......................................................................133
TABLE 5.3: Years of education ....................................................................................134
TABLE 5.4: Relationship of family members to patients .............................................134
TABLE 5.5: Family members’ ICU experience ............................................................135
TABLE 5.6: Nationality of family members .................................................................135
TABLE 5.7: Age of patients ..........................................................................................136
TABLE 5.8: Gender of patients .....................................................................................137
TABLE 5.9: Patients’ admission type ...........................................................................138
TABLE 5.10: Patients’ APACHE III scores..................................................................139
TABLE 5.11: Reason for admission to ICU..................................................................139
TABLE 5.12: Length of patient stay in days .................................................................140
TABLE 6.1: PPUS-FM before transfer .........................................................................143
TABLE 6.2: State anxiety before transfer .....................................................................144
TABLE 6.3: Correlational analysis of PPUS-FM before transfer and demographic
factors ............................................................................................................................145
TABLE 6.4: Relationship groups’ PPUS-FM ...............................................................147
TABLE 6.5: One way analysis of variance of PPUS-FM before transfer and
selected factors...............................................................................................................147
TABLE 6.6: Multiple regression of PPUS-FM and selected factors .............................149
TABLE 6.7: Correlational analysis of state anxiety before transfer and selected
factors ............................................................................................................................150 TABLE 6.8: One way analysis of variance of state anxiety before transfer and
selected factors...............................................................................................................151 TABLE 6.9: State anxiety before and after transfer ......................................................153
TABLE 6.10: PPUS-FM before and after transfer ........................................................153
TABLE 6.11: PPUS-FM and state anxiety after transfer...............................................155
TABLE 6.12: ANCOVA – PPUS-FM and state anxiety after transfer for control and
intervention groups ........................................................................................................156
TABLE 6.13: Family members’ transfer results............................................................161
TABLE 6.14: Areas of worry for family members........................................................163
TABLE 6.15: Information family members wanted......................................................166

xii
TABLE 6.16: Importance of transfer process for family members............................... 170 TABLE 6.17: Times Rns used intervention .................................................................. 171
TABLE 6.18: Helpfullness of intervention as a framework for discussion................... 171
TABLE 6.19: Discussion promoted by intervention ..................................................... 172
TABLE 6.20: Future use of intervention....................................................................... 173

xiii
LIST OF FIGURES
FIGURE 2.1: Conceptual framework ............................................................................48
FIGURE 4.1: Four phases of study................................................................................54
FIGURE 6.1: Graph of state anxiety before and after transfer with estimated marginal
means for post-transfer scores .......................................................................................156
FIGURE 6.2: Graph of PPUS-FM before and after transfer with estimated marginal
means for post-transfer scores .......................................................................................157

xiv
STATEMENT OF ORIGINAL AUTHORSHIP
The work contained in this thesis has not been previously submitted for a degree
or diploma at any other higher education institution. To the best of my knowledge
and belief, the thesis contains no material previously published or written by
another person except where due reference is made.
Signed _____________________ Date ____________

xv
DECLARATION OF ENROLMENT
I, Marion Mitchell, a candidate for the degree of Doctor of Philosophy at
Queensland University of Technology, have not been enrolled for another tertiary
award during the term of my PhD candidature without the knowledge and
approval of the University’s Research Degrees Committee.
Candidature’s Signature
___________________________
Date: / /

xvi
ACKNOWLEDGEMENTS
There are a number of individuals and groups I would like to acknowledge. These
include:
• the families in my study who so willingly gave of their time in what was a
critical period of illness for their family – thank you.
• my supervisors, Professor Mary Courtney and Mrs Fiona Coyer. Thank
you sincerely for your invaluable guidance, constructive criticism and
encouragement provided so willingly to me.
• the Queensland Nursing Council, Royal College of Nursing, Australia, the
Centaur Memorial Fund for Nurses and Griffith University who have
financially, or in kind, supported my project - my grateful thanks.
• my friends and colleagues who individually have encouraged and
supported me throughout – my sincere thanks.
• my husband, Brian and sons - Stuart and James, for their understanding,
patience and love which supported me enormously throughout this study –
thank you. My thanks also to my Father, Mac whose never-ending love
and interest give me strength and a sense of achievement.
I wish to dedicate this work to my Mother, Ruth Crombie who died before I
started this project but whose memory has constantly supported me – she would
have been such a good editor!

1
CHAPTER 1: INTRODUCTION
1.0 Introduction
This thesis is concerned with families and their experience of transfer from
Intensive Care Units (ICU). This interventional study examines the relationship
between family members’ anxiety and uncertainty during the transfer process and
the efficacy of the intervention. There is a growing acknowledgement of the
relationship among anxiety, uncertainty, and the ability for family members to
cope with illness situations but no research has occurred in the area of ICU.
Transfer from ICU has been chosen as the focus for this research as it is
frequently seen by families and patients to be a negative outcome when in fact it is
proof that the illness is improving. When an event is perceived to have negative
connotations by family members, their ability to cope is compromised (Mishel,
1983). It is postulated that the basis behind family member and patient reluctance
to move to a general ward is that they are not prepared well for the move thus
making adjustment difficult. Previous research has indicated that critical care
nurses do not see discharge planning as part of their role (Thompson, 1985) which
is of great concern as they are cited by family members as the best provider of
information to meet their needs (Quinn, Redmond, & Begley, 1996). The role of
transferring patients and family members from ICU is important and nurses need
to have a structured method to support the transfer (Chaboyer, Foster, Kendall, &
James, 2002). This research will therefore evaluate an intervention designed to
improve the transfer process by supporting ICU nurses in communicating with
family members about imminent patient transfer.

2
1.1 Clinical Research Problem A critical illness significantly affects the entire family unit as they try to come to
terms with the situation in which they find themselves. This often unexpected
illness frequently requires extensive and complicated nursing and medical
treatments only available in ICUs. To the uninitiated visitor, this highly technical
area may initially be frightening or alarming particularly when a family member is
the patient who requires the treatment modalities and care which accompany the
setting. Primarily, family members communicate with the bedside nurse about
aspects of patient care and treatment and relationship subsequently develop. The
close monitoring of patients is often comforting, reassuring and supportive for
family members who experience anxiety as a result of the critical illness (Curry,
1995).
Rehabilitation and recovery programs, together with high demands for ICU beds,
see a reduction in patient length of stay (LOS) in ICU and an acceleration in
patient transfer to the general ward. This subsequent transfer from the highly
technical and generally one on one nursing in ICU is reported as a stressor for
family members (Leith, 1999) who have developed a relationship with the ICU
health care team and frequently feel the patient is not yet ready for transfer.
Family members’ stress and anxiety at the time of transfer may reduce their ability
to play the key role in patient recovery (Leske, 1992; McShane, 1991) which
extends far beyond the time in ICU.
In the general ward an entirely new health care team takes over the ongoing care
for patients. This demands the development of new relationships between patients,
3
family members and staff who have different methods of care to that practised in
ICU. Discussions regarding the seriousness and prognosis of the illness, an
unfamiliarity with what to expect next and continuing intricate treatments, can
lead to family members’ experiencing uncertainty about the illness (Mishel,
1981). Feelings of uncertainty may impair family members’ adaptation leading to
the perception that transfer is seen as a negative experience which limits family
members’ coping strategies (Mishel, 1988). This is at a time when family
members are the one continuing feature, or constant, in patients’ ongoing care.
High levels of uncertainty related to the illness and transfer from ICU to a general
ward may be associated with a reduced ability for family members to manage or
cope with the illness situation.
Consequently, family members need preparation for transfer from ICUs to general
wards to assist them in the transition and better prepare them for their ongoing
role as carer. Communication about proposed changes in treatment, such as an
imminent move to a general ward, is reported as an important need by family
members (Leske, 1991). Although most nurses acknowledge the importance of
good communication with family members, in ICU there are actual and perceived
barriers to achieving this. Many institutions have no formal procedures to assist
nurses and family members in this process. In some instances, patient demands
and time restrictions may prevent nurses from interacting and communicating
fully with family members (Curry, 1995) or alternatively, nurses may choose to
distance themselves from family members as they perceive they are not well
equipped to assist family members with their needs (Scullion, 1994). Those nurses
who feel under-prepared require assistance and support in this vital
4
communication role to empower them to interact confidently with patients’
families to give them the information they need (Chaboyer et al., 2002). This
support for nurses is even more necessary in a busy, highly demanding ICU
environment if nurses are to meet both patient and families’ needs efficiently.
Their role includes supporting and promoting a positive continuum of care
beyond an ICU environment and this can be achieved by improving
communication with family members.
Educational strategies directed to improving and supporting ICU nurses’
communication with family members is an initiative worthy of investigation as it
not only facilitates positive two-way interaction but potentially reduces family
members’ anxiety and uncertainty which may accompany the transfer out of ICU
to a general ward. Nurses who lack the confidence or knowledge to
independently engage with family members may benefit professionally by
utilising educational strategies which prepare them for a task they have previously
approached with trepidation.
1.2 Project Summary The purpose of this study was to improve the experience of transfer from ICU for
family members and ICU nurses. A structured pre-transfer educational process to
individualise and improve communication between nurses and family members
was developed and evaluated. There were a number of assumptions underlying
this study and they include the following.

5
1.2.1 Assumptions 1. Family members play a significant part in the rehabilitation and ongoing care
of critically ill patients.
2. Anxiety adversely affects family members’ ability to cope with the crisis
situation of a critical illness.
3. Information regarding the transfer process is an important need for family
members of ICU patients.
1.2.2 Research Questions The following research questions were developed from the literature.
Question 1 What was the level of ‘uncertainty in illness’ in family members
before transfer from ICU as measured by Mishel’s Parents’
Perception of Uncertainty Scale –Family (PPUS-FM) Scale?
Question 2.1 Was there a relationship between family members’ ‘uncertainty in
illness’ as measured by PPUS-FM (Mishel, 1997) and anxiety levels
as measured by State Trait Anxiety Inventory – State (STAI)
(Spielberger, Gorsuch, & Lushene, 1983)?
2.2 Were patient and family member’ factors significantly related to
PPUS-FM?
2.3 Were patient and family member’ factors significantly related to
STAI – state scores?
Question 3 Has the introduction of the intervention led to a reduction in the
‘uncertainty in illness’ and state anxiety levels?
Question 4.1 Has the introduction of the intervention led to an improvement in
family members’ satisfaction with regard to their information
needs?

6
4.2 Has the introduction of the intervention led to an improvement in
ICU nursing staff communication with family members ?
4.3 Has the introduction of the intervention led to an improvement in the
overall preparedness of family members for transfer?
4.4 Were family members worried or frightened by information given to
them and what was the information that caused this concern?
4.5 What information did family members wish they had been told?
Question 5.1 What was the ICU nurses’ perception of their unit’s attitude to
families and how important family members were to patients’
recovery?
5.2 What was the ICU nurses’ perception of the level of importance of
the process of transfer from ICU for families?
5.3 Has the intervention provide a useful means to improve discussion
with family members from ICU nurses’ perspective and would they
recommend its use?
1.2.3 Research Aims and Objectives The following research aims and objectives were developed in conjunction with
the research questions.
1. To collaborate with family members and nurses to determine relevant transfer
information requirements.
2. To examine the concept of ‘uncertainty in illness’ for family members as it
related to the transfer period from ICU.

7
3. To produce a patient and family focused educational brochure, which
supported and facilitated improved nurse/family communication about
transfer.
4. To determine the efficacy of the intervention in reducing family anxiety and
uncertainty following transfer.
5. To measure family members’ level of satisfaction with the transfer process.
6. To evaluate the benefits of the structured pre-transfer process as perceived by
ICU nurses.
1.3 Structure of the Thesis This thesis begins with a discussion of background information pertaining to
family and patient transfer from ICU. The clinical research problem and
significance to nursing practice are outlined. The research questions and aims and
objectives for the study are enumerated. The second chapter reviews current
literature on this topic. The dearth of research evaluating intervention studies in
this area in ICU are highlighted with studies from other nursing specialities
examined in relation to an ICU cohort. These existing studies have predominantly
described and identified anxiety and uncertainty in patients or families. In
contrast to this approach, this study developed a Conceptual Framework grounded
in emerging theoretical and empirical evidence to evaluate an intervention.
Chapter 3 outlines the methodology employed for the four phases of the study.
The sample size in this study allowed for a range of statistical analyses to answer
the five research questions.

8
Chapter 4 presents the analysis of results for Phase One and Phase Two of the
study which aimed at determining relevant information necessary for inclusion
within the intervention. Chapter 5 compares and contrasts the characteristics of the
primary research sample of family members and patients within the control and
intervention groups. Chapter 6 presents further results in relation to the aims of
the study and the five research questions. These results are discussed in Chapter 7
in relation to existing research. Limitations of the current study are also outlined
in Chapter 7.
The final chapter for this thesis contains the conclusions from the study. It also
highlights the implications for clinical practice, future research, and nursing
education.

9
CHAPTER 2: LITERATURE REVIEW
2.0 Introduction The literature review examines seven areas of research in connection with family
members of critically ill patients. The first section explores the General System
Theory and suggests that this is an appropriate theoretical basis for focusing upon
family members of patients who are critically ill. It supports the assumption that
ongoing support from family members is integral to the wellbeing and
improvement of critically ill patients.
The second section investigates the experience of critical illness from the
perspective of the family. Family members’ cognitive appraisal of the illness
event is very different to patients’ perception and therefore requires individual
nursing interventions. The manner in which family members manage the acute
experience of a critical illness and are supported and prepared for the
rehabilitation phase is dependent upon the balance between family members’
internal and external resource (Halm et al., 1993) which in part, are contingent
upon the care they receive in ICU.
The third section explores the concept of ‘uncertainty in illness’, first described by
Mishel in 1981, to see if facets of this paradigm are identifiable in the study
sample of family members of patients transferring from ICU to the ward. Current
literature regarding ‘uncertainty in illness’ suggests that those with high levels of
uncertainty have a reduced ability to apply adequate coping mechanisms during

10
the illness situation. This has the capacity to impact significantly upon patient
outcomes.
The fourth area in the literature review analyses the potential impact anxiety has
on family members who experience the critical illness of a family member. High
levels of anxiety are not only an antecedent to possible physiological changes in
those experiencing it, but are also thought to impair their ability to positively
influence the critically ill family member’s recovery (Liddle, 1989; McSahne,
1991). This outcome has significant ramifications for nurses who, when
embracing holistic care, need to also consider the needs of families in addition to
the needs of the patient. Literature in the area of family member’s needs is
reported upon in section five.
The sixth section of the literature review highlights findings from studies
examining factors which influence family members’ perception of the transfer of a
previously critically ill family member from ICU to a general ward area. Authors
consider that moving from a secure environment to one which is unknown to
family members forms a basis for anxiety surrounding the illness/recovery process
which, in most instances, is a positive and progressive step. The documentation
that transfer anxiety exists as a phenomenon pays credence to the reality of the
need for nurses to, not only be aware of it, but also be knowledgeable about ways
to reduce its occurrence.
The final section of the literature review examines Knowles’ Adult Learning
Theory which is suggested as a way to understand how adults interpret and

11
understand reality (1980). This understanding gives insight into how to approach
methods aimed at improving comprehension and recall, both of which can be
problematic in high anxiety situations. This chapter will conclude with the
development of the Conceptual Framework emanating from the literature
2.1 General System Theory in Context The greatest social institution which influences individuals in our society is
considered to be the family unit (Friedman, 1998). A definition of ‘family’ needs
to reflect society’s beliefs and attitudes and therefore is subject to change based
upon contemporary thinking. Australia’s cultural diversity supports a definition
which encompasses all types of family groups and is defined by Wright who
suggests that “the family is who they say they are” (Wright & Leahey, 1994,
p. 40). This definition has broadened the concept of family to potentially include
any combination of family members as defined by its participants and has been
incorporated into research within Australian studies (Walters, 1995).
Leske’s 1991 study categorised the make-up of families of critically ill patients
using data from 27 researchers over a period of a decade. There were 905 family
members in the combined studies and Leske found that the composition of
families comprised spouse (38%); child (27%); parent (20%); sibling (5%);
extended family (4%) and significant other (5%). Interestingly, in a 1998 North
American study with admittedly, much fewer participants (n = 52) of critically
patients, 18 or 37% of the family members were significant others and not blood
relationships (Mendonca & Warren, 1998). This may indicate a societal trend over
the past two decades since the commencement of Leske’s study, where a broader
definition of family is now relevant as indicated by the increased percent within

12
the significant other category. The small numbers in the 1998 (Mendonca &
Warren) study necessitate caution when drawing conclusions from the data.
It appears that a broad definition of family has been embraced by nursing
researchers and writers who frequently refer to the term ‘significant other’ when
studying family situations where shared relationships exist between patients and
others (Benner, Hooper-Kyriakidis, & Stannard, 1999; Chavez & Faber, 1987;
Jacono, Hicks, Antonioni, O’Brien, & Rasi, 1990; Raleigh, Lepczyk, & Rowley,
1990; Spatt, Ganas, Hying, Hirsch, & Koch, 1986). Collectively, they recognise
that one’s family and significant others, can be instrumental in promoting the
recovery and rehabilitation of the patient and for this study a broad definition such
as Wright’s and Leahey’s will be used (1994, p. 40). In view of the significance of
family to individual wellbeing, the family, in its broad context, therefore needs to
be the focus of care rather than the sick patient in isolation (Farvis, 2002; Nettle et
al., 1993; Plowright, 1996; Russell, 1999; Wright & Leahey, 1994).
The family’s role has been recognised since the inception of modern day nursing,
as an integral component of an individual’s health. Florence Nightingale
considered family care was important to the wellbeing of the individual and
advocated home based services (Dossey, 2000). This strong family focus within
nursing continued to be encouraged into the 20th Century. Whall (1993) reviewed
the position of family within nursing during the 1900s by examining both
literature and nursing curricula. The evidence suggests that the theme of family,
as a unit of care, has featured in most nursing curricula and was a significant
element in standards of practice (Whall, 1993). Nurses modified their practice to

13
involve family members, who prior to World War Two, cared for their sick in the
home (Wright & Leahey, 1994). After 1945, sick people were cared for more
frequently in hospitals where family participation in caring for the loved one was
discouraged (Craven & Sharp, 1972). This trend to restrict family participation
and visitation is now recognised as potentially detrimental to the recovery of sick
people (Scullion, 1994; Spatt et al., 1986). Family visits are thought to provide a
significant degree of connection to the outside world for the patient at a time when
everything surrounding them is foreign and unfamiliar (Dyer, 1995). This link
with their home environment provides a degree of orientation to ill patients who
otherwise are exposed solely to an environment which could be viewed as highly
medicalised and clinical with the focus on illness processes.
The importance of one’s family can be explained by von Bertalanffy’s General
System Theory (von Bertalanffy, 1973). Von Bertalanffy (1973) commenced
development on the General System Theory in the 1930s in response to the
developing complexities of the scientific era and further developed the theory over
the next three decades in view of modern technology with its connection to
computer, behavioural and social sciences. General System Theory goes further
than examining the elements making up the parts of the system but also
investigates their interrelations. These interrelations, von Bertalanffy suggests can
not be isolated into causal chains and requires an interpretation of “..man with his
biology, culture and linguistic endowment” (1973, p. xxi) to understand the
manner in which one deals with a situation.

14
The fundamental principle of the General System Theory is that systems are open
and not closed and are therefore influenced by a multitude of external factors (von
Bertalanffy, 1973). The General System Theory has a conceptual framework
based upon five tenets, which lends support to a broad definition of family. The
first belief is that the family interacts on two levels. Firstly within the broader
community such as one’s neighbourhood, church group or social organisation and
secondly within relationships such as a parent-child or parent-parent. That is, a
family unit is a social system dependent upon its environment, interrelationships
and organisation (Friedman, 1998).
The second belief within the General System Theory is that the family as a whole
is greater than the sum of its parts (von Bertalanffy, 1973). This acknowledges
the complexity and significance of interrelated relationships and interdependence
(Friedman, 1998) within a family group. The third component of the theory
suggests that a change or alteration in one family member causes an effect on
other family members (Wright & Leahey, 1994). This theory acknowledges the
inevitability of change for individuals within a family which then responds or
adapts to manage the change. The manner in which a family responds is
contingent upon individual and family perceptions and the resources upon which
they draw in response to the new demand (Friedman, 1998). In the case of
sickness the change experienced may be profound and unexpected, affecting an
overwhelming response in family members. Without effective family coping
strategies and problem solving efforts, a family is unable to function adequately
(Friedman, 1998) and attain a state of equilibrium.

15
The fourth principle suggests the family is capable of balancing change and
stability (Wright & Leahey, 1994). With predictable life events, such as children
becoming increasingly independent, a family has time to accept and adapt to the
reduced need for parental direction. This slow maturation process is frequently
welcomed and enjoyed as the family celebrates various rights of passage in the
expected growth of the children. In this example, the family members gradually
identify the changing needs of their offspring and all members alter their
behaviour accordingly to maintain a healthy functioning family unit, however
with unexpected, unpredictable family changes, the family does not have the
benefit of preparation and slow introduction to the changed situation. For
example, in the case of an acute illness, the immense and frequently unplanned
change may see the family unable to balance internal and external resources to
provide stability in the situation. A family’s understanding of the situation
influences the manner in which it is interpreted and acted upon (Friedman, 1998).
That is, a similar incident experienced by two families may be interpreted
anywhere along a continuum from a minor disruption to a critical situation
depending upon the family’s perception of the event.
Finally, von Bertalanffy suggests that family members’ behaviour occurs in a
circular rather than linear framework (Wright & Leahey, 1994). That is, one
member’s actions will affect another’s who in turn reciprocates in response to the
initial behaviour. The responses one receives, therefore, need to be considered
within the context of the entire interaction with considerable importance attributed
to the initial behaviour. The internal dynamics of a family are therefore complex

16
and to be understood need to be considered in its entirety and not as isolated
communications and incidents.
The General System Theory succeeds in conceptualising the complex notion of
family and is not only used within nursing scholarship but also is accepted and at
times, adapted in the areas of information technology, business (Wright & Leahey,
1994), tourism (La Lopa & Marecki, 1999), and behavioural and physical sciences
(Snow, 2002; von Bertalanffy, 1973). Wellard (1997) suggests that within nursing,
the General System Theory as it applies to families, fails to acknowledge power
base issues and societal influences on the family. She recommends caution in the
application of the theory and suggests that nurses recognise the potential impact of
an authority differential both within and outside the family unit and to plan
nursing interventions accordingly. Constructive family-centred nursing
interventions require considerable assessment and evaluation and a General
System Theory provides a framework within which nurses can appraise the needs
of the family being mindful of the broad issues of equity and class, as suggested
by Wellard (1997).
The theory proposes that relationships and individual wellness play a significant
role in the attainment of family homeostasis and equilibrium. “Family systems
generally seek to maintain a steady state, yet must accommodate growth and
development, i.e. change” (Wright & Leahey, 1994, p. 8). Growth and
developmental change occur over a period of time and allow family members a
period of adaptation and understanding which facilitates family homeostasis. This
does not occur, however, in the case of a critical illness in one member of the

17
family unit as generally, critical illness is unplanned and impacts upon the family
resources in a profound and unpredictable manner. The ensuing impact on both
the collective family, and individual family members, can be understood and
explained by the General System Theory, which sees family members
endeavouring to adapt to a rapidly different family situation. Family needs centre
on their requirements for the tools and skills to adapt to the current situation,
which in this study, is a critical illness.
2.2 Critical Illness Critical illness is one where the patient’s state of being is precarious and recovery
is contingent upon their internal and external resources. This illness situation, as
with other significant family problems, affects the entire family unit. McClowry
(1992) suggests that a General System Theory approach explains family member’s
reactions to the critical illness as they respond to the physical insult on their loved
one. They experience an inability to balance change and maintain stability in an
environment which is unfamiliar and frequently frightening (Millar, 1991). Their
loved one is at risk of dying (Coulter, 1989) or suffering ongoing deficits, and
together with family roles being forced to undergo unplanned change (Halm,
1990; McClowry, 1992), a precarious family situation evolves.
The critical episode may be part of a continuum with the family’s involvement far
exceeding the time the patient spends in ICU (Compton, 1990; McClowry, 1992)
which at times represents only the preliminary phase of the illness (Millar, 1991).
The manner in which family members manage the acute experience and are
supported and prepared for the rehabilitation phase is dependent upon the

18
patient’s illness state, the balance between the family member’s internal and
external resource and their cognitive appraisal of the event (Halm et al., 1993).
The cognitive appraisal of the event from family members’ perspective is very
different to that of patients who may be too ill to fully comprehend the severity of
the situation or alternatively, appraise the situation as less severe than others.
This clinical observation is supported by Compton (1990) who reports that
critically ill patients are, at times, more concerned about the welfare of their
family members and how they are coping with them in ICU than by their own
health state. Although patients in this study (Compton, 1990) were described by
staff and family to be critically ill, the patients did not describe themselves in that
way. Rather, they reported feeling safe and not under threat of death. This altered
sense of reality on the part of the patient may intensify the sense of responsibility
experienced by the family members who are frequently called upon to make
treatment decisions on behalf of their critically ill family member.
Halm et al. (1993) utilised a conceptual framework based upon the patient’s
illness state, the balance between the family member’s internal and external
resource and their cognitive appraisal of the event to evaluate family members’
coping strategies and how they evolve over time. In this explorative study within
five ICUs in a large tertiary referral centre, 52 adult family members’ behavioural
responses were measured by the Iowa ICU Family Scale, developed by the
researchers. Content validity was established by the researchers. The self-
reporting qualitative and quantitative questions explored five areas: sleep
behaviours; eating pattern; support systems; family roles and activity behaviour.

19
Respondents were asked to score on a day-by-day basis, how the critical illness
affected the five particular behaviours when compared to the previous day or
week. Not surprisingly, the study identified that family members experience
changes in routine behaviour including reduced sleep and nutritional intake which
makes them more susceptible to physical illness (Halm et al., 1993). Reduced
nutritional intake and inadequate sleep may lead to demonstrated behaviours such
as emotional eruptions (Hickey & Leske, 1992) and irritability, reduced cognitive
ability such as an inability to retain information, poor concentration and impaired
decision making (Cagan, 1988; Halm et al., 1993). These are significant findings
when one considers that families are integral to the recovery of patients (Hickey
& Leske, 1992; Spatt et al., 1986), who by the very nature of their critical illness,
are reliant upon those caring for them to make crucial decisions on their behalf.
Nursing staff who undertake an early and progressive family assessment are able
to detect deficits in coping behaviours (McClowry, 1992) and assist family
members in the development of management strategies. These include enlisting
assistance from pre-existing support systems (Halm, 1990), active participation in
the physical care of patients (Cagan, 1988; Coulter, 1989), and providing
information to family members about the situation (Molter, 1979). Research
suggests that at this initial phase in the critical illness the family member’s
primary consideration is for the needs of their sick loved one rather than personal
needs (Curry, 1995; Molter, 1979). However, fulfilment of personal needs are at
risk as assistance from family support systems may be diminished due to reduced
contact when family members provide a bed-side vigil in the acute phases of the
illness (Halm, 1990). Direct communication amongst supporting family members
20
during this period often proves difficult as ICU protocols at times, do not allow
phone calls from family members. This is at a time when support from family
members is crucial as the outcome of the critical illness is so uncertain (Coulter,
1989). Although nursing research acknowledges the need for providing adequate
support systems for family members in critical illness situations, ICU protocols
are not always conducive to nurses fulfilling their role in holistic nursing.
2.3 ‘Uncertainty in Illness’ For family members, uncertainty regarding the illness outcome could be a
common feature of many critical illness situations due to the precarious nature of
the illness process. An American nursing researcher, Merle Mishel, has
extensively explored the concept of uncertainty since the early 1980s in relation to
illness situations. She defines ‘uncertainty in illness’ as “..the inability to
determine the meaning of illness related events. It is the cognitive state created
when the person cannot adequately structure or categorise an event because of the
lack of sufficient cues” (Mishel, 1988, p. 225). Mishel hypothesises that this may
be the result of receiving mixed messages relating to the illness, multiple intricate
treatments, and inadequate knowledge regarding the seriousness and prognosis of
the illness (Mishel, 1988).
Symptom pattern without form or consistency promotes uncertainty by giving a
confusing picture of the illness. That is, individual symptoms need to be
distinguishable to allow for their inclusion in a pattern of symptoms for family
members (Mishel & Braden, 1988). Consistency of symptoms permits pattern
recognition, which is predicable and congruent with the illness situation. This

21
expectation or predicability of symptoms related to an illness reduces uncertainty
and enhances individuals’ coping mechanisms (Mishel, 1988). Unfamiliarity with
illness symptoms is common in critical illness and may promote the feeling of
uncertainty on the part of the family member of the critically ill patient and hence
reduce the effectiveness of their coping strategies.
Consistent information and education from a credible authority reduces
uncertainty by assisting one to interpret the pattern of symptoms, to understand
and predict treatment situations as, or before, they arise (Mishel & Braden, 1988).
Having faith and trust in the providers of the information is crucial to reducing
uncertainty feelings. It has been found that social support assists with decreasing
ambiguity related to mixed messages, concerning the state of the illness, by
providing the opportunity to compare with each other, ideas and information
concerns (Mishel & Braden, 1987). Social support provides a network where the
family member can draw on others’ thoughts to confirm beliefs in a preferred
interpretation of the uncertainty event (Mishel & Braden, 1988) and so adjust to
the situation (Mishel & Braden, 1987).
Experiencing uncertainty restricts one’s ability to decipher and interpret the
situation (Mishel, 1981). This reduced ability to make sense of the situation,
Mishel (1988) considers may impair adaptation leading to the perception that the
positive illness events are appraised as a negative outcome which limits coping
strategies. In the case of a critical illness, it is frequently the family who
experience uncertainty about their loved one’s condition who may not consider
the situation as critical as others perceive it. The family’s adaptation and coping
22
strategies may prove to be inadequate in managing the illness situation, which
persists far beyond the ICU environment. As family members frequently
contribute significantly to after-hospital care for patients, their ability to cope
effectively with the illness state is crucial to the subsequent success of
rehabilitation or management of illness progression.
‘Uncertainty in illness’ has been reported in a number of study population
including adults, children, care-givers, parents and spouses in both acute
(myocardial infarction) and long term conditions (diabetes mellitis, rheumatoid
arthritis, recurrent cancer, cardiovascular disease, and lupus) (Mishel, 1983;
Mishel, 1995). There are however, no reported studies which have examined
uncertainty in a cohort of ICU family members thus limiting discussion and
understanding in this area.
In the area of chronic illness, however, research indicates that in a subject sample
with rheumatoid arthritis, higher levels of uncertainty are associated with an
increased perception of the severity of their illness (Braden, 1990). Braden (1990)
suggests that in this population, interventions directed towards reducing
uncertainty, together with increasing independence, may positively influence
problem solving and belief in one’s self to be able to better deal with the situation
(Mishel & Sorenson, 1991). These ways of coping may incorporate requesting
information to reappraise the situation in a more positive light (Mishel, 1988;
Deane & Degner, 1998) and in so doing, reduce the uncertainty (Mast, 1995) and
anxiety experienced (Wong & Bramwell, 1992). Nurses are well placed in their
24 hours of care in ICU to provide information about the patient condition (Dyer,

23
1991) and are suggested as reliable sources of information as indicated by the
studies by Molter (1979) and Mendonca and Warren (1998).
Uncertainty was further examined by Andersson-Segesten (1991) in patients with
chest pain in two coronary care units using Mishel’s Uncertainty in Illness Scale
(MUIS) (Mishel, 1981). This was an intervention study where the introduced
variables were the style of nursing care operational within each unit and the
physical environment. One unit was newly built whereas the other was neither
new nor redecorated. Unit A (the new unit) functioned on a primary nursing
system where each patient was allocated to one nurse whose responsibility it was
to care for the patient. This style of nursing is designed to limit the number of
nurses caring for a patient in an attempt to promote better outcomes from
improved continuity of care (Keen & Weir, 1995). Unit B (the old unit), however,
had a team nursing approach where registered nurses worked in conjunction with
a nurse’s aide and a task-orientated practice focus was operational. A task
focussed approach to patient care changes the nursing focus away from a patient
centred approach and is thought to reduce the ability of the nurses to meet
individual patient needs (Keen & Weir, 1995).
Interestingly, there was no significant difference in the level of uncertainty
between the two cohorts of 30 patients. There was, however, a significant
correlation between Factor One on the MUIS tool, ambiguity, and the length of
time since a previous admission (Andersson-Segesten, 1991), with higher levels of
ambiguity (and uncertainty) occurring in participants who had a shorter time
between admission. Within the cardiac care context, this association between

24
increased ambiguity and recent readmission to the unit is perhaps predictable as
patients try to make sense of their unstable illness situation. As Mishel’s (1988)
theory explains, symptoms which do not fit a pattern can increase the ambiguity
associated with the illness and may be the cause for readmission as the patient
grapples with the meaning behind the symptomatology.
Andersson-Segesten (1991) suggests that the styles of nursing and patients’
environment does make a difference but she fails to demonstrate statistically that
the difference lies in the area of reduction of uncertainty. Non-participant
observation may have documented similar levels of communication, information
sharing and reassurance in the two groups, regardless of the mode of nursing.
These are thought to be closely associated with reducing uncertainty in illness
(Mishel, 1981) and may account for the results. The small sample and effect size
may also have contributed to the non-significant result. The majority of
participants in this study were unsure of their diagnosis and potential disease
progression which is a variable in a number of studies examining uncertainty
(Gaskins & Brown, 1992; Hilton, 1989) and may account for the levels of
uncertainty. Andersson-Segesten (1991) further suggests that participants with
coronary pain awaiting diagnosis will experience high levels of uncertainty
irrespective of nursing interventions.
Uncertainty in the above study would be seen in Mishel’s model (1988) as a
negative coping strategy or danger, as opposed to being seen as an opportunity
which promotes positive coping strategies. Uncertainty perceived as a danger has
been associated with anxiety (Wong & Bramwell, 1992) when there is a perceived
25
threat of malignancy diagnosis (Deane & Degner, 1998), fear of recurrence of
breast cancer (Mast, 1998) or the possibility of deterioration in a family member’s
critical condition (Coulter, 1989).
Mishel and other researchers are adding to the knowledge of the phenomenon of
‘uncertainty in illness’ in a broad band of recipients of health care, thus adding to
the assertion that the concept is significant and detectable across most clinical
practice settings. As mentioned previously, no described studies have measured
uncertainty in ICU family members thus indicating there is a deficit in the
knowledge concerning this psychological phenomenon. Further understanding of
the phenomenon will continue to expands nursing knowledge and promote the
development of evidence based interventions directed to identifying precipitating
factors and improving outcomes for recipients of health care.
2.4 Anxiety ‘Uncertainty in illness’ has been linked, or associated with, participant anxiety
(Wong & Bramwell, 1992). Anxiety can be described as “a feeling of
apprehension caused by a threat to a person or his values. Some describe it as an
exaggerated feeling of impending doom, dread, or uneasiness” (Robb, 1997, p.
56). It is suggested that anxiety is comprised of two components. Spielberger and
his colleagues (Spielberger et al., 1983) contend that one facet of anxiety includes
an individual’s reaction to a particular situation, which alters as the situation and
their methods of managing it alters (Chavez & Faber, 1987). It is a transient
emotion that varies over time and is termed state anxiety (Spielberger et al.,1983).
An individual’s state anxiety has the capacity to alter with each situation

26
depending upon the feelings the situation arouses. One situation may result in very
high levels of state anxiety whereas, another may not trigger a state anxiety
response at all. The other facet is considered to be one’s trait anxiety. This is a
relatively constant individual characteristic which predisposes one to respond in a
particular manner (Spielberger et al., 1983). Spielberger et al.’s (1983) definition
suggests that an individual during a number of different situations will record a
similar level of trait anxiety irrespective of the situations, as it is an innate
characteristic.
The level of anxiety experienced influences the manner in which an individual
functions. During a critical illness, anxiety is experienced by family members
(Artinian, 1991; Caine, 1989; Chen, 1990; Halm, 1990; Hayes, 1990; McClowry,
1992; Mendonca & Warren, 1998; Rukholm, Bailey, Coutu-Wakulczyk, & Bailey,
1991) with the extent being determined by the individual’s level of state and trait
anxiety. A family member’s anxiety affects their ability to operate within and
outside the hospital environment and it is suggested that high anxiety levels inhibit
family members’ capacity to enhance patient recovery (Liddle, 1989; Lynn-
McHale & Smith, 1993; McShane, 1991) and contribute to patient care (Lynn-
McHale & Smith). In reality, family members may try to manage their anxiety by
remaining by the patient’s bedside, trying to find support and hope in the situation
(Chartier & Coutu-Wakulczyk, 1989) while they maintain a vigil.
Authors Benner et al., (1999) suggest that anxiety contributes to a lack of
understanding and perception about the illness situation which Broome (1985)
suggests may lead to repeated questioning by family members around a previously

27
discussed topic. This anxiety-related lack of comprehension is not always
recognised by ICU nurses who may misinterpret the reasons for family members’
repeated questioning. Family members with high anxiety levels as a result of a
crisis situation (Robb, 1997) may therefore have altered information needs which
nurses need to understand and recognise. The use of language which is spoken in
plain English (Wooley, 1990) with no medical jargon (Breu & Dracup, 1978; Ley,
1979; Scriven & Tucker, 1997) will assist in family members’ comprehension.
When nurses communicate with family members they need to consider repeating
important information due to the effects of high anxiety.
Family members perceive they are given inadequate patient related information
which they describe as an additional stressor (Benzer, Mutz, & Pauser, 1983;
Jones & O’Donnell, 1994). In a Canadian study (Chartier & Coutu-Wakulczyk,
1989) of 207 family members of patients in an ICU, 24% of the variation of state
anxiety of family members was attributed to lack of knowledge about the
situation. It needs to be highlighted, however, that a study reported upon in 1989
may well document aspects of society’s health-care expectations which no longer
apply. That is, it could be argued that social norms regarding moral rights to
information concerning critical illness, may have changed over the last decade of
ICU nursing where paternalistic attitudes by health care providers may have been
more prevalent than is the case today.
Alternatively, deficits in the receipt of information may originate, not from health
care providers’ failure to fully inform family members and patients, but from
family members’ unwillingness to ask questions about the critical illness situation.

28
McClowry (1992) suggests that family members may choose not to question the
staff as a coping strategy to lessen the impact of the situation. Their reduced
understanding allows them to have a false sense of the reality of the condition
where they, perhaps inaccurately, anticipate a complete recovery (McClowry,
1992). This potentially unreal picture reduces families’ ability to adapt to the
current situation as they deny aspects of the illness and consequently diminish
their positive contribution to patients’ recovery (Quinn et al., 1996).
Nurses are well placed in their 24 hours of contact with patients to provide current
information to family members (Dyer, 1991) and to assist in their understanding
of the patient experience (Whire, 1997). It could be suggested that family
members are equally interested and concerned by what their sick family member
is experiencing along with the names or number of current treatment modalities.
ICU nurses need to not only be skilled, but also available to relate to family
members the current patient status.
Another aspect of ICU nurse interaction with family members is that it
“humanises the ICU environment” (Marsden, 1992, p. 116) where high levels of
technical expertise and complicated treatments take precedence over other
activities. Effective communication between family members and nurses (Farvis,
2002; Holden, Harrison, & Johnson, 2002), however, is vital to the understanding
of the situation and promotes compassion amidst the technological environment
(Walters, 1995). Nurses’ body language and inferences are important aspects of
the communication process (Cohen, Craft, & Titler, 1988) and written information
alone will not allay anxiety (Teasdale, 1993). Nurses’ diligent sharing of

29
consistent information with family members (Titler, Bombei, & Schutte, 1995)
can in itself, reduce their anxiety and increase energy reserves (McClowry, 1992)
which are expended at an accelerated rate in high anxiety situations (Friedman,
1998).
When anxiety levels are reduced there is an additional benefit according to Lynn-
McHale and Smith (1993) who suggest that when family members’ anxiety levels
are consistently at a low level, they are less demanding of nurses. This may well
allow the nurse to concentrate on other aspects of the critical illness situation and
supports the notion that by reducing anxiety levels and meeting the needs of
family members (Lynn-McHale & Smith, 1993), ICU nurses can best support the
recovery of patients (Liddle, 1989; McShane, 1991; Wilkinson, 1995).
2.5 Needs of Families When an adult family member suffers a critical illness, it removes them from their
pre-illness role within their family. The subsequent role and relationship changes
for family members, heightens their anxiety (Titler, Cohen, & Craft, 1991) as they
endeavour to adjust to the new situation. Their ability to cope is reliant upon
family relationships and the way they are able to draw on resources and support
systems (Leske, 1986; Lynn-McHale & Bellinger, 1988) as a mean of reducing
their anxiety levels (Freichels, 1991) in an effort to adapt and problem solve. The
reduction of anxiety is important, not only for the wellbeing of the family member
but also from the perspective of the patient as family members’ anxiety reaction
can affect patient recovery (Mendonca & Warren, 1998). Consequently, meeting
the individual needs of family members (Quinn et al., 1996) is a critical and

30
fundamental component of caring for patients (Kleinpell & Powers, 1992;
McShane, 1991; Mendonca & Warren, 1998).
Researchers have recognised that examination of the needs of family members in
ICUs is warranted and the interest and sheer number of research projects over the
past two decades legitimises families as recipients of care in an holistic ICU
nursing model (Artinian, 1991; Fowlie, Frances, & Russell, 2000; Hayes, 1990;
Kleinpell & Powers, 1992; Molter, 1979; Quinn et al., 1996). Molter’s seminal
study in 1979 provided foundation research into the needs of family members, an
area previously not the focus of study. Although Molter’s sample of family
members was not large (n = 40), she was able to document a ranking of the
importance, or otherwise, of 45 needs during a structured interview process. This
initial research led to the development of a tool, the Critical Care Family Needs
Inventory (CCFNI) by Molter and Leske in 1983 and thus provided a quantitative
research instrument of 40 items. This has been used extensively by researchers
interested in the needs of families in an ICU environment (Leske, 1991).
Additional research by Quinn et al. (1996) cautions that nurses in their study
perceived family members’ needs differently to the way the family member
perceived them in 20 out of the 30 listed needs. This lack of congruence between
the nurse and family members’ perception highlights the worth of such research,
which can provide direction for family focused interventions.
The primary needs for family members in the study (Quinn et al., 1996) related to
reassurance and information about their family members’ condition whereas

31
nurses rated family members’ need to talk about their feelings as a primary need.
These are quite diverging perceptions and therefore noteworthy. In light of the
General System Theory, the unexpected nature of the critical illness presents
challenges to the adaptive ability of the family who need to draw on all its internal
and external resources to obtain a degree of stability in the situation to be able to
function. The understanding of information about the critical event is an important
aspect of this process of adaptation. That is, it is considered that an understanding
of the critical illness situation is vital to a family’s adjustment, therefore its need
for information is a high priority particularly in the early days after admission
(Freichels, 1991) and when significant changes occur or are predicted. The part
anxiety plays in their adaptive response gives credence to improved sharing of
meaningful information in a manner the family members are able to comprehend.
Nurses who by necessity are constantly by the patient’s bedside in ICU, have the
opportunity to get to know the family during its visits and are thus able to develop
a rapport and provide information in a way it can understand.
Studies however, indicate that commonly, patient demands and time restrictions
preclude nurses from including family members in their care (Cohen et al., 1988;
Curry, 1995; Fox & Jeffrey, 1997; Hickey & Leske, 1992; Millar, 1991; Quinn et
al., 1996). Alternatively, nurses elect to withdraw from family members and
family dynamics as they find involvement stressful (Dunkell & Eisendrath, 1983;
Scullion, 1994; Fox & Jeffrey, 1997; Benner et al., 1999). This coupled with a
perception of being ill-prepared for assisting families in a crisis situation (Curry,
1995; Hickey & Leske, 1992; Hickey & Lewandowski, 1988; Scullion, 1994)
suggests nurses prefer to concentrate their time and effort on the highly technical

32
aspects of their role (Fox & Jeffrey, 1997). These strategies fail to acknowledge
the crucial part family members play in the recovery of the patient together with
the need for professional development to better equip ICU nurses for these
situations.
In order for the family to provide the support to the patient, a number of primary
needs have to be met. Leske (1991) reviewed raw data over a period of a decade
from 27 researchers, all using the same instrument, the CCFNI. The sample
comprised 905 family members of 668 critically ill patients. Analysis of the
accumulated data categorised family needs into three areas: (1) the need for
assurance; (2) the need for proximity; and (3) the need for information (Leske,
1991). These are not ranked in order of importance but rather for convenience.
Under the category of assurance, families wanted their questions answered
honestly, to feel there is hope, and to feel confident that those caring for their
family member cared for them (Leske, 1991). The need to be physically close to
their family member rated highly and falls into the category of proximity. The
ability to visit frequently and have fewer limits on visiting times is seen as a way
to promote closeness and emotional support (Leske, 1991) which contributes to
the reduction of patients’ feelings of isolation (Ballard, 1981). Physical separation
is a constant reminder to the family that the critical illness is accompanied by a
danger to the integrity of their family unit (Leske, 1991). This perception of
danger has been linked to ‘anticipatory grief’ where family members experience a
sense of loss due to the potential death of the patient (Breu & Dracup, 1978;
Wooley, 1990). Nurses can be proactive in this situational crisis by promoting

33
family member visitation and their involvement in patient care together with the
provision of relevant information about the patient’s condition and treatment
(Breu & Dracup, 1978; Wooley, 1990).
The requirement for information is the third category from Leske’s (1991)
analysis of data. As referred to earlier, information needs are not ranked after
assurance and proximity needs as in fact, information needs constitute seven out
of the top ten needs in both Leske’s study of combined data (1991) and Freichel’s
study (1991). To know the patient’s prognosis, details on treatment, progress and
plans for transfer are all identified as primary needs for information (Molter,
1979). Effective communication is paramount with family members identifying a
need to talk to doctors every day about the patient’s condition. Furthermore,
family members request being called at home should the patient’s condition
deteriorate (Leske, 1991; Molter, 1979).
Medical practitioners have been criticised for giving inadequate information and
explanation (Jones, Hoggart, Withey, Donaghue, & Ellis, 1979) and in practice,
information is frequently supplied by bed-side nurses. The amount and depth of
information required is individual and nurses need to assess family understanding
(Coulter, 1989) and needs as information overload can be problematic.
Additionally, nurses frequently interpret for family members, information given
by medical staff (Coulter, 1989; Koller, 1991; Meyer, 1992) and how it may
impact upon the patient (White, 1997). Families’ heightened anxiety state may
require the information to be repeated simply and free of jargon (Broome, 1985;
Robb, 1997; Wooley, 1990).

34
Studies examining family needs have explored who the participating family
members considered meet their needs (Mendonca & Warren, 1998; Molter, 1979).
In Molter’s study (1979) of 40 family members, nurses met 20 out of the 35
needs. Although this may be seen to place an onus of responsibility on nurses,
Mendonca and Warren (1998) found in their study of 52 family members of
critically ill patients, information, proximity and assurance needs were in fact met.
Molter’s study (1979) only documents needs met less than 50% of the time in her
study cohort. The four needs met less than 50% of the time can be grouped within
the category of support with the one exception of needing to talk to the doctor at
least once a day. This information need was considered to be very important or
important, by more than half the study cohort. Molter’s results indicate that all
other needs are met more than 50% of the time.
It is interesting, but not unexpected, that a number of studies indicate that family
members of critically ill patients rate their personal support needs low on the list
of 45 items of needs (Foss & Tenholder, 1993; Leske, 1991; Mendonca & Warren,
1998; Molter, 1979). Personal comfort is similarly rated at the lowest end of the
list (Hayes, 1990) as family members state “...they do not expect the health care
personnel to be concerned about them, ...the family members saw the staff as
being responsible only for the care of the patient and not his family” (Molter,
1979, p. 338). Perhaps family members indicate or imply to nurses that personal
needs are not uppermost in their requirements and nurses consequently direct their
efforts to other family need areas.

35
It is argued, however, that ICUs in recent times which promote a family friendly
approach (Benner et al., 1999), assist ICU nurses to individualise patient care
through communication with their family members (Dunkel & Eisendrath, 1983).
ICU nurses who are confident and comfortable with a family orientated process of
nursing, communicate to family members the important part they play in the on-
going health care of the patient. By facilitating interaction and communication
with family friendly policies, nurses can help prepare family members for patient
discharge from ICUs before it occurs and potentially reduce their anxiety of
leaving the security of the unit (Leske, 1991).
2.6 Transfer from Intensive Care Knowing about transfer plans as they are being made is consistently rated as a
primary information need by family members in ICU (Daley, 1984; Leske, 1992;
Molter, 1979; Quinn et al., 1996) to a greater extent than those with family
members in general ward areas (Foss & Tenholder, 1993). Although transfer is
seen as a positive step by many families (Cutler & Garner, 1995; Toth, 1980), it
can invoke anxiety for both patients (Leith, 1999; Lethbridge, Somboon & Shea,
1976; Roberts, 1976; Saarmann, 1993; Schwartz & Brenner, 1979) and family
members (Cagan, 1988; Leske, 1992; Toth, 1980).
Bouvé, Rozmus and Giordano (1999) suggest that parental anxiety at time of
discharge from a Paediatric Intensive Care Unit (PICU) is closely related to the
changed environment, uncertainty of continuing treatment regime, need to adapt
to new staff, and a reduction in monitoring equipment. Poe (1982) suggests that
this anxiety, which Roberts (1976) defines as transfer anxiety, could stem from a

36
“fear of the unknown” (Poe, 1982, p. 364). Roberts (1976) suggests that transfer
anxiety consists of:
… anxiety experienced by an individual when he moves from a familiar, somewhat secure environment to an environment that is unfamiliar. In ICU units it involves separation from the close surveillance of monitors and machines. It also results from interpersonal separation from those nurses and doctors who maintain personal surveillance. ( p. 227-8).
It is interesting that this definition was coined in the mid 1970s when technology
in ICUs was elementary when compared with the technology used today. Modern
day society, by way of popular media and other exposure, develops a perception
of how current technology is part of critical illness and thus leads to different
expectations than families of the 1970s experienced. Although the technological
parameters have changed, other facets that contribute to transfer anxiety persist
today.
Saarmann (1993) and others (Coyle, 2001; Streater et al., 2001) suggest that
transfer anxiety is a type of separation anxiety which is ably explained within
Robert’s (1976) definition. Saarmann (1993) suggests that this type of anxiety can
be reduced by early and adequate preparation for transfer (Bouvé et al., 1999;
Choate & Stewart, 2002) which can occur unexpectedly due to demands on ICU
beds. Nurses who establish successful communication strategies with family
members can introduce the notion of discharge to a general ward early in the
relationship in such a way that it is perceived as a natural and desirable occurrence
(Russell, 2000).
Whilst in ICU, patients are completely dependent upon nursing staff where a high
patient:nurse staffing ratio supports this level of care. In general wards, however,

37
a much lower ratio of nurses to patients occurs. This places a higher expectation
upon the patient to be more self reliant and independent (Lethbridge et al., 1976;
Schactman, 1989). This degree of independence is reinforced and confirmed by a
reduction in the monitoring equipment (Cagan, 1988; McKinney & Melby, 2002),
and the number and frequency of nursing observations (Leith, 1999; Roberts,
1976). This, together with the general ward layout which restricts the visibility of
patients by nursing staff (Lethbridge et al., 1976) forms a very different situation
for the patient and their family. The altered surroundings, changed nursing
expectations, and different health care team creates a foreign environment to
which the patient and family need to adjust.
Leith (1999) interviewed patients and family members on their perceptions of
transfer from ICU to general ward areas and found that a proportion of family
members did not adjust well to the move. This qualitative study reported that
some family members suffered from insomnia, were angry, tearful, and generally
unhappy about their family member’s transfer. A contributing factor may have
been that family members were not well prepared for the transfer of their family
member’s next phase of care along the rehabilitation continuum.
Preparing for transfer to the ward forms a component of discharge planning and
should be commenced when the patient arrives in ICU (Thompson, 1985). This
does not always appear to occur, sometimes due to the unforseen admissions of
emergency cases, whilst in other instances, nurses do not consider discharge
planning is part of their role (Thompson, 1985). This is in spite of the fact that
research consistently states that families want to be informed as transfer is being
38
considered and planned (Foss & Tenholder, 1993; Leske, 1992; Molter, 1979;
Quinn et al., 1996) which perhaps allows for a period of adjustment and
reorganisation of ways of thinking on the part of family members.
Predicted progression and improvement does not always occur in critical illness
thus affecting plans for transfer. Communication with families is therefore
essential as knowing about transfer ahead of time facilitates the opportunity for
family members to meet their needs regarding information on future treatments
and the projected prognosis for their ill family member. Information can be
shared by a variety of methods. In an ICU setting, Bokinskie (1992) suggests
family conferencing, which, in Bokinskie’s case involved a meeting with the
family, the ward nurse and the ICU nurse. At the meeting, Bokinskie (1992)
suggests that the new ward layout could be discussed together with the
expectations of the general ward staff. Family and patient needs could also be
addressed and family centred goals could be established. This tripartite
conference may reduce family anxiety by way of promoting communication and
continuity of care.
The promotion of continuity of care is supported by good communication between
the ICU and ward registered nurse, and the family (Barbetti & Choate, 2003;
Russell, 1999b; Schwartz & Brenner, 1979). Barbetti and Choate (2003) go
further to suggest that the family has a role to play in the actual transfer event
when family members can be physically close to, and support their family
member. This proximity of a supportive family member is considered to be a
component in reducing stress in the transferred patients (Schwartz & Brenner,

39
1979). One could surmise that the family member would also be better orientated
to the new environment and future treatments and so feel less anxious about the
transfer as they are intimately involved with the transfer process. Schwartz and
Brenner’s (1979) proposal places limitation upon the times when patients can be
transferred, that is, when their family members are present, and this could be
problematic and unrealistic as transfers frequently occur all through the day and
night depending on individual circumstances.
Shannon (1973) suggests that family members should be telephoned to be told of
any impending transfer out of the unit. At this time, the ICU nurse could discuss
with the family member the differences to expect in the new ward. This
communication could be made considerably easier for the family member if prior
discussion has occurred by way of preparation for transfer. Although a phone
call to absent family members presents one opportunity to communicate with
family members about transfer to the general ward, Provine (1986) advocates that
nurses should take every opportunity to increase patient and family knowledge
about the situation by explaining therapies and proposed plans such as transfer.
These education sessions can be on an ad hoc basis (Provine, 1986) or be
presented as a structured pre-transfer session (Saarmann, 1993).
Poe (1982) concurs with the concept of a structured pre-transfer session as her
study recorded a reduction in patient’s perception of risk associated with their
transfer from ICU to a general ward. Poe (1982) utilised an individually
structured pre-transfer teaching program for a small study (n = 16) where the
experimental group experienced a teaching program and the control group

40
experienced the usual transfer preparation by the ICU nurses. Poe (1982)
speculated (but did not test) that the experimental group’s greater level of
preparedness may have fostered the development of coping mechanisms to reduce
their anxiety.
Other forms of preparing patients and families for ICU situations have been
utilised as seen with Ziemer (1983) who produced tape recordings containing
varying levels of information to instruct ICU patients pre-operatively about their
impending procedure. The study revealed no significance in the patient’s ability to
cope post-operatively irrespective of their level of pre-operative taped
information. This study relied on patients listening to the information without a
nurse in attendance or scheduled to answer questions and perhaps highlights the
limitations of one-way methods of learning.
Written information about transfer has the benefit of providing patients and
families with a record of information to which they can subsequently refer
(Cagan, 1988). Lange (1989) further suggests that printed matter is beneficial as it
provides material which can be shared in a controlled manner to suit participants’
needs. That is, it is versatile in the time when it can be read, and the amount of
information can be limited or repeated depending on participants’ retention
capabilities. As patients frequently are thought to forget sizeable amounts of what
occurs in ICUs (Odell, 2000; Russell, 1999a), it is imperative to include family
members in all education procedures including pre-transfer teaching sessions.

41
Written material in the form of booklets has been extensively used as a method to
convey information to family members and/or patients in ICUs (Cutler & Garner,
1995; Derham, 1991; Hayes, 1990; Henneman & Cardin, 1992; Maillet, Pata, &
Grossman, 1993; Parrinello, 1984; Raleigh et al., 1990; Watts & Brooks, 1997).
Few studies, however, have evaluated the effectiveness of the brochures they have
used. An exception to this is a study by Waitkoff and Imburgia (1990) who
evaluated a booklet designed to inform patients and their families about the
activity and rehabilitation following cardiac surgery. Ninety percent of the 165
participants deemed the brochure helpful in answering their questions. Similarly,
the small study by Spatt et al., (1986) developed a brochure on their ICU which
they found to be helpful to family members but noted that only 11 out of the 25
participants in fact received the brochure which was meant to be given to all
family members. This non-compliance with an introduced information
intervention may indicate staff’s negativity or reduced perception of the
worthiness of the brochure. Scriven and Tucker (1997) emphasize the need to
have high quality information brochures which use graphic artists and high quality
material to assist with the production of aesthetically pleasing material for best
effects.
One may surmise that if family members in Spatt et al.’s study (1986) found the
brochure helpful, it meets some of their needs. Anxiety reduction has been
identified as a primary need by family members of ICU patients (Molter, 1979)
and Teasdale (1993) supports the notion that the written word is insufficient in
reducing anxiety. Teasdale (1993) conjectures that the inferences, body language
and ability to ask questions, which are facilitated with face-to-face communication

42
has the capacity to reduce anxiety. Direct communication allows information to
be specific and relevant to the individual situation (Teasdale, 1993) and the
printed version, written in plain language (Macey & Bouman, 1991; Maillet et al.,
1993; Parrinello, 1983) serves as a record for future reference.
Bouvé et al. (1999) conducted a randomised control trial to compare the
effectiveness of utilising a “transfer-preparation letter along with a verbal
explanation” (p. 114) and no formal transfer planning, in reducing parent’s level
of anxiety at discharge of their child from a PICU. Lazarus’s Stress and Coping
Model provided the framework for Bouvé et al.’s study where anxiety was
perceived as being a result of individual and environmental determinants.
Lazarus’s model suggests that stress and anxiety can be reduced with an increase
in information and the transfer-preparation letter, in conjunction with nurse
explanations, constituted the intervention.
A convenience sample of 31 parents formed the experimental group and 19 the
control group. The unequal numbers were a result of the randomisation process
and somewhat limited the ability to compare the two cohorts. Spielberger’s State-
Trait Anxiety Inventory (STAI) was administered 24 to 48 hours prior to transfer.
The intervention group then received the letter and talk by the nurse who spoke of
the positive aspects of the transfer and the changed expectations in the general
ward. The control group was not prepared for transfer.
The experimental group had significantly lower levels of anxiety post transfer
than did the control group. The authors acknowledge that there is the possibility

43
of tainting the data with information meant only for the experimental group being
received by the control group. It is easy to imagine ICU nurses inadvertedly
informing parents on some aspects of the general ward. Ethically they may have
felt the need not to disadvantage members of the control group by preparing them
informally for transfer. A more definite separation of the two groups would have
prevented this. A study utilising two sites or two ICUs would provide this
separation. Alternatively, a times-series study would allow for separation of the
two cohorts and provide valid data (Polit & Hungler, 1997). Finally, the small
numbers for this study conducted in a PICU limit the generalisability of the
results.
2.7 Knowles’ Adult Learning Theory A criticism common to these research projects based on educational interventions
is that researchers do not state if their material is based upon educational
principles or grounded in a learning theory. That is, the information contained
within the interventions may not be presented in a way to facilitate learning.
According to Merriam (1996) all adult learning theories need to consider the
learner, the learning process and the context. Without due consideration to these
features designed material or programs may not succeed in enhancing knowledge
acquisition.
There are a number of learning theories which are grouped in a variety of ways.
One such grouping sees four distinct orientations: the behaviourist, the cognitive,
the humanist and social learning orientations. Although all four orientations offer
purposeful understanding of ways to explain and implement strategies for
learning, the humanist approach ably recognises the adult learner as an

44
autonomous and self-directed learner who aims for learning as “.. a function of
motivation and involves choice and responsibility” (Merriam & Caffarella, 1991,
p.137). Merriam and Caffarella (1991) suggest that the humanist approach
understands learning to encompass more than thought processes and behavioural
change as it emphasises how human emotions can have an effect on learning.
Knowles’s Adult Learning Theory fits within the humanist orientation with its
focus on self-directed learning which involves teaching adults how to take
responsibility and be in control of their learning (Caffarella, 1993).
Knowles’ Adult Learning Theory bases its andragogical model, or the art and
science of helping adults learn, on six principles (1980). These principles include:
• a need to know,
• a responsible for their own learning,
• the role of experience as a resource in one’s learning,
• a readiness or applicability of the information to their life situation,
• motivation to learn, and
• problem centred learning with real life problems (Knowles, 1980).
Individual adults will not always possess all these principles particularly when
faced with a new area of learning (McAllister, 1997) such as in an ICU
environment hearing about their relative’s critical illness. Adult education
however, could be described as aiming to nurture these attributes and is dependent
upon the teacher (in this case the bed-side nurses) who may need to develop an
understanding of the learner and give considerable direction initially (McAllister,
1997). Knowles (1980) agrees with this notion and suggests that adults move
towards self-directedness at different rates depending on life events and support in

45
understanding to learn may be required. Brookfield (1986) concurs with Knowles’
principles and highlights the varied learning styles exhibited by adult learners who
use different strategies for coding and retaining information. Brookfield (1986)
suggests that individuals learn at a varying pace but need the information to be
meaningful to their life situation. Educational interventions which incorporate
these features into their model are therefore more likely to positively affect
learning outcomes (McAllister, 1997) and are thus recommended.
2.8 Summary of Literature Families of critically ill patients in ICU form a crucial link in the health care
continuum as they provide both physical and emotional support to patients in the
acute crisis and subsequent care. A broad definition of family is adopted for this
study and as Wright states “a family is who they say they are” (Wright & Leahey,
1994, p. 40). This all-embracing definition permits the recognition of any mix for
family members.
The General System Theory (von Bertalanffy, 1973) assists in explaining the
profound effects of the critical illness upon the family and explains the need for
the family to find a balance, or degree of equilibrium, in order to cope with the
situation (Robb, 1997). The critical illness generally permits little or no time to
adapt to the new situation and this impacts significantly on the family by reducing
their ability to cope with the situation. The unplanned situation forces role
changes (Halm, 1990) and adaptation is contingent upon their internal and
external resources. The theory encourages the adoption of the family unit as the
recipient of care rather than the patient in isolation to best improve outcomes for
the patient as it sees the family as an important part of patient care. ICU nursing

46
which embraces family centred care is able to support the family as it cares for the
critically ill patient.
Family members’ cognitive appraisal of the situation and on-going care is
dependent, in part, upon their understanding of events. High levels of anxiety are
frequently experienced by family members of critically ill patients (McClowry,
1992; Mendonca & Warren, 1998) and this impacts upon their degree of
understanding and perception about the illness (Benner et al., 1999). ICU nurses
require an understanding that family members’ information needs are greater due
to their heightened anxiety state and the possible presence of uncertainty about the
illness.
Uncertainty about the illness situation is thought to reduce family members’
ability to interpret illness events (Mishel, 1988) and has the capacity to further
reduce, or limit, the coping ability of family members (Mishel, 1983). Mishel
(1988) postulates that it is a result of mixed messages, multiple intricate
treatments and an inadequate knowledge regarding the seriousness and prognosis
of the illness. It is easy to expect that high levels of uncertainty exist in critical
illness situations where anxiety may reduce families’ ability to retain and interpret
information. Uncertainty has not previously been examined in this cohort and
thus further research in this area is required.
Family members’ needs during a critical illness have been examined and fall into
three categories: (1) need for assurance (2) need for proximity (3) and the need for
information (Leske, 1991). Individual information needs rank in seven out of the

47
top ten needs (Freichels, 1991) which demands that significant importance be
placed on effective communication strategies in ICU situations with families.
Studies suggest that the transfer out of ICU is a significant anxiety producing
event for families (Leith, 1999) who request to be informed as transfer plans are
being made (Leske, 1991). ICU nurses are well placed to prepare family members
for transfer which should be part of discussion as soon as the patient arrives in the
unit (Thompson, 1985). Structured pre-transfer information sharing sessions
based upon sound adult learning principles (Knowles, 1986) is advocated as a way
to prepare family members (Poe, 1982) for the different environment and
expectations in the general ward. Both written and face-to-face communication is
suggested as the best method as it allows nurses to individualise information and
gauge understanding. It also facilitates the opportunity for questioning by family
members. Although a number of interventions to improve communication around
transfer have been developed, there is a scarcity of meaningful evaluation
associated with these interventions. Research evidence is required before
interventions should be incorporated into ICU nursing practice which is a dynamic
and ever changing milieu.
2.9 Conceptual Framework Having completed the review of literature, a Conceptual Framework was
developed to visually represent the key concepts and suggest factors which impact
upon family members at the time of transfer of their relative from ICU (Figure
2.1).

48
Figure 2.1 Conceptual Framework
Transferred with structured pre-transfer communication
Transferred without structured pre-transfer communication
Family Background Factors
• Previous ICU admissions
• Illness related factors
• Social factors
• Demographics
G e n e r a l S y s t e m T h e o r y
Anxiety
Family Outcomes
Uncertainty
Satisfaction
Anxiety
Family Outcomes
Uncertainty
Satisfaction
Family
Anxiety
Uncertainty
The overarching philosophy for this study is von Bertalanffy’s General System
Theory. General System Theory ably explains and recognises the importance and
support family members provide to each other in a critical illness situation.
Continuity of care demonstrated by family members, is the one constant during
the illness period, including transfer from ICU, and is therefore depicted under the
umbrella of General System Theory in the conceptual model. The process of being
informed about transfer from ICU to a general ward is described as an important
need by family members (Leske, 1991) who are striving to understand the
implications of moving from the highly technical, closely monitored ICU.
For each family member, background factors will impact on their ability to
manage in crisis situations. These factors may include: patient illness related

49
factors (such as, the degree of illness) (Ogden, 1996); social factors such as
support systems (Sherbourne & Stewart, 1991); demographic details (age and
gender); and previous exposure to ICU admissions (Bouvé et al., 1999).
Heightened levels of anxiety (McDowell & Newell, 1996), together with the
presence of high levels of ‘uncertainty in illness’ (Mishel & Braden,1987) have
been identified in family members of sick people. Both ‘uncertainty in illness’
and anxiety can reduce a family member’s coping ability (Leske, 1992; McShane,
1991; Mishel, 1988) at a time of illness. Inadequate or inappropriate coping
strategies can adversely affect the outcomes for the critically ill patient when
decisions need to be made quickly (Ogden, 1996).
Although not previously reported, high levels of ‘uncertainty in illness’ may
feature for family members around the time of transfer from ICU as the illness
progression is frequently difficult to predict or understand. A lack of
understanding about the illness situation is suggested as a precursor to increased
uncertainty (Mishel, 1988) and, at the time of transfer from ICU, there are
frequently vast changes in treatments and medication modalities. The possibility
of a relationship between high uncertainty and anxiety levels is suggested and this
study proposes to analyse this.
It is suggested that improved family member understanding of the situation will
occur with better communication and information sharing around transfer and thus
reduce ‘uncertainty in illness’ and anxiety. A structured pre-transfer education
session between the nurse and family members is proposed to facilitate this

50
communication and understanding. Reduced uncertainty, according to Mishel’s
theory (1983), will permit family members to draw on their internal and external
resources more effectively and better cope with the acute situation as they view
the transfer from ICU in a more positive light (Mishel, 1988).
It is suggested that the structured pre-transfer education session will also improve
family member’s satisfaction with the transfer process as a consequence of their
increased understanding of the new ward environment and the altered patient
expectations which accompany the general ward. Von Bertalanffy’s (1973)
General System Theory informs the methodology for this study as it assists
scientific understanding of inter-relationships and endeavours to explain causal
factors. The following chapter describes the methodology which guided the study.

51
CHAPTER 3: METHODOLOGY
3.0 Introduction This chapter outlines the study design and strategy with each phase’s sampling
framework and data collection methods. Data collection tools are explained with
justification for their inclusion. Analytical procedures are outlined in relation to
each of the five research questions. Ethical considerations and potential risks are
identified at the end of the chapter.
The review of the literature identified several methodological weaknesses of other
studies in the area of anxiety and ‘uncertainty in illness’. One methodological
weakness was the fact that no previous studies have reported on these factors with
a sample of family members in ICU much less evaluated an intervention to reduce
its level of occurrence. Non representative samples in a number of studies was
problematic (Bouvé et al., 1999; Toth, 1980; Wong & Bramwell, 1992) with
samples as small as nine participants being reported within a quantitative
methodology (Bokinski, 1992). The timing of administration of measures was
not always reported and therefore presented problems when considering the
interpretation of results (Chartier & Coutu-Wakulczyk, 1989). Educational
brochures used as an intervention were frequently not evaluated for their efficacy
nor were they stated to be based on educational principles on the way people learn
(Bradenburg & Gifford, 1997; Cutler & Garner, 1995) and therefore are limited in
regards to the research basis for their study. A number of principles were
therefore considered important in the design of this study to ensure enhanced
methodological rigour in addressing the research questions of the study.

52
These principles included:
• the examination of the factor ‘uncertainty in illness’ in a cohort of ICU
family members,
• ensuring a large enough sample to ensure sufficient power to detect
clinically significant alterations in the factors under examination,
• the timing of the administration of the measures was standardised for
ready comparison between a control and intervention group, and
• the intervention was grounded in a theoretical framework suited to adults.
3.1 Study Design The quantitative quasi-experimental pre-test, post-test non-equivalent control
group design for the study was guided by von Bertalanffy’s (1973) General
System Theory. Multiple collection points before and after the introduction of the
intervention allowed the researcher, to cautiously attribute the results post
intervention to the introduction of the intervention (Polit & Hungler, 1997) - in
this case, the structured pre-transfer educational method of transfer.
3.2 Research Strategy A research site was identified and ethical approval received from the hospital and
university ethics committees. This followed discussion with the divisional
Director of Nursing, Nurse Care Practitioner of ICU and the ICU clinical research
projects’ officer. The study was conducted in both the ICU and general wards of a
large metropolitan tertiary referral hospital. The ICU had 24 beds with a varied
case-mix of elective surgery, emergency admissions, and inter and intra hospital
transfers requiring intensive therapy. During data collection in 2001, the number
of admissions to this unit was 1460.

53
The study was conducted in four phases (Figure 4.1). The purpose of Phase One
was to gather information about important factors involved with the transfer
process from an ICU to general ward area from the perspective of family
members. Family members of patients who have been transferred from the site’s
ICU were surveyed. Additionally, an expert nursing panel was formed to obtain a
nursing perspective regarding information thought to be important to family
members during the transfer of their relative. This, together with nursing research
literature on the transfer needs of families with critically ill relatives, combined to
form the foundation for Phase Two.
Phase Two involved the development of a brochure based upon the data from
Phase One. Draft brochures were developed and reviewed by senior hospital
nursing personnel before the final brochure was commercially printed.
Phase Three had a pre-test, post-test design which evaluated the impact of a
structured pre-transfer educational method on family members with relatives
transferred from ICU to a general ward. Outcome data were gathered on eligible
family members, initially experiencing existing transfer procedures, then
following the introduction of the structured pre-transfer educational method. The
pre-test, post-test design with a prolonged period of pre and post transfer data
collection creates its own ‘control’ period (Polit & Hungler, 1997). This allows
the researcher with a carefully planned study to exclude alternative explanations
for changes in outcome data once the intervention has been introduced (Bowling,
1997).

54
Phase Four of the study evaluated the critical care nurses’ perception of the utility
of the structured pre-transfer educational method in supporting the transfer
process. A survey questionnaire was developed by the researcher to capture the
opinions of the critical care nurses who had used the structured pre-transfer
educational method to transfer patients.
Figure 4.1: Four Phases of Study.
Phase One 1. Expert panel survey & focus group discussion 2. Post ICU family members.
Phase Two Development of Educational Package from Phase One data.
Phase Three 1. Survey families - pre & post-test with current transfer method 2. Implementation of intervention3. Survey families - pre & post-test following intervention
Phase Four ICU RNs’ evaluation of intervention

55
3.3 Phase One
3.3.1 Research Design An exploratory descriptive design was used to gather information from relatives
and a panel of critical care nurses to develop an educational brochure. This
formed the basis for the structured pre-transfer educational intervention. Research
in the area of families’ needs around the time of transfer was also used to inform
the content for the educational package and the questionnaires.
3.3.1.1 Expert panel The expert group were members of the ICU professional body’s Education
Advisory Panel (n = 8). In addition, the site’s ICU educator and the facility’s
general ward educator were members of what will be referred to as the ‘expert
panel’. This totalled a sample for the expert panel of ten nurses.
Each member of the Education Advisory Panel and the hospital educators was
contacted firstly by telephone when the researcher introduced herself and the
project. Each participant was given a brief overview of the project and the aims to
improve the transfer process for family members following the discharge of a
relative from an intensive care unit to a general ward. They were each invited to
consider participating in the study and were sent an information package, a
consent form (Appendix A) and questionnaire (Appendix B) for further
consideration. In two instances, the potential participant was unable to be
contacted by telephone and email communication was used as a way of
introduction prior to sending out the written information.

56
The written invitation and information letter guaranteed participant confidentiality
and outlined the purpose of the study stating that there were two components to
the expert nurse participation. The questionnaire asked them to consider
information which they thought important to family members prior to the transfer
of their relative from ICU to a general ward. In addition, they were asked their
perceptions and attitudes to current practice involving care of the family in the
critical care area. It was important that the researcher explained and stressed the
need for confidentiality on the part of all participants to ensure any who worked at
the study site did not discuss issues raised and inadvertedly alter current patient
and family transfer practices in the site’s ICU. Return pre-paid envelopes were
included to facilitate the successful return of completed questionnaires. All
surveys were coded to provide the researcher with identifying data should a
survey not be returned. One follow up phone call and/or email was made to act as
a reminder and assist any participants who may have had difficulty with a
question. No further phone calls were made, as non-reply after the follow up
period was viewed as a wish not to participate.
The second component to the data collection with the expert panel was an
invitation to participate in a focus group discussion. Focus group discussions are
considered to be an effective way to collect data from participants on a topic of
interest to them (Kruger & Casey, 2000). The fundamental tenet underpinning the
use of focus groups is that group interaction reveals additional data other methods
would not elicit (Webb & Kevern, 2001). Around eight participants have been
suggested as optimum in allowing the opportunity for each participant to give

57
their point of view, comment and build upon others’ contributions (Kruger &
Casey, 2000).
Prior to the focus group meeting, the researcher collated the returned participants’
responses to the closed questions and wrote out in full, their open-ended
responses. The meeting was timed to coincide with the annual critical care
conference, where a majority of the participants were delegates. A face-to-face
meeting at another time presented difficulties as members of the expert panel live
in all Australian states. Having spoken with the chairperson of the Educational
Advisory Panel, time was allocated at the end of their scheduled meeting for the
focus discussion. As all members in attendance had agreed to participate and had
responded to the survey they were aware of the project and its aims. The
researcher was invited to sit in on the meeting and to speak at the close of official
business.
Expert panel participants were welcomed by the researcher and thanked for their
participation in this aspect of the project. Hospitality was extended to the
participants by way of refreshments provided by the researcher in an effort to
make them feel comfortable and appreciated. This was a group of peers who
already knew each other and were all members of the Education Advisory panel.
This facilitated an easy introduction to the discussion as it was not necessary for
participants to get to know each other. During the preceding meeting the
researcher had witnessed each participant contribute to discussion with respect for
others. These are both important facets of successful focus group discussions
(Flick, 2002).
58
The discussion occurred around a table in a private room. The purpose of the
meeting was explained to them and additional reassurance that any information
they provided would not be linked individually to them in any report or
publication. This confidentially was important as they needed to feel assured they
could speak freely about issues they saw as important. During the focus group
discussion, the researcher, acting as moderator encouraged expert panel discussion
on the issues raised by participants’ responses to the questionnaire. At this time,
participants were asked to prioritise the information to be contained in the
educational brochure which by its very nature was limited in space. It was
therefore important to have a concise representation of the expert panel’s opinions
as to the hierarchical listing of the issues and information. The researcher wanted
to be confident that the chosen topics within the brochure were considered to be
the most important by the expert panel.
After distributing the collated survey data, the researcher asked participants to
discuss the results and in particular the open-ended question responses as it was
this question which provided a broad diversity of comments. After allowing for
perusal time, the researcher asked for group discussion where items could be
deleted, altered or added to. Considerable discussion ensued with some items
being deleted following discussion. Other items required clarification, some were
grouped together and still others were added. The opportunity for the group to
discuss suggestions was productive and at the completion of each category under
discussion the points were summarised and verified by the participants as an
accurate representation of discussion. Face validity of the data is important and

59
was achieved thus by the moderator outlining identified issues to the participants
for clarification and verification (Kidd & Parshall, 2000).
At the completion of the discussion, the group was asked if they considered the
five categories named by the researcher to be appropriate. They concurred that
they were appropriate. At the completion of the focus group discussion, the
researcher thanked the participants for their time and thoughtful contribution to
the discussion.
Following this meeting, the researcher collated the material from the focus group
discussion in a written document. This was electronically mailed to those who
participated in the focus group discussion. They were asked to respond by email if
they considered any point inaccurate or incomplete. Additional comments were
welcomed. As no emails were received, the researcher considered this to be a
positive affirmation of the summary of events and outcomes.
The researcher subsequently organised to meet with the site’s ICU and general
ward educators to have a similar meeting as was held at the focus group
discussion. This was agreed to but only the site’s ICU educator was able to attend.
The general ward educator communicated on the day that she had resigned from
the hospital and would be leaving that week and preferred not to participate in the
group discussion. Therefore the researcher discussed the participants' survey
forms responses only with the ICU educator. This was very rewarding as some of
the issues mentioned by the focus group members depended on ward practices and

60
hospital protocols. The site’s educator responded to these items with knowledge
and experience of the research site.
Regarding a general ward educator’s contribution, the researcher decided to forgo
this aspect of feedback and involvement. It was considered of limited value to
wait for another educator to be appointed to the position as it would be some time
for them to be able to contribute by giving a specific facility perspective. The
researcher did have the incumbent’s survey response to the written questionnaire
so was able to include this written information from the present general ward
educator’s perspective.
3.3.1.2 Family member The second component of Phase One was to survey family members whose
relative had been transferred from the site’s ICU to a general ward. A
questionnaire developed by the researcher (Appendix D) asked consenting
relatives to contribute information important to them around the time of transfer
from ICU to the ward. They were asked to reflect on their own recent experience.
No names appeared on any surveys to ensure confidentiality for the participants.
There were 12 questions in the survey, 11 were closed with a five-point scale and
the final question was open-ended asking participants if they wanted to comment
further.
Recruitment commenced in December 2001. The researcher went to the ICU and
checked the names of the patients who had been transferred to a general ward that
morning or the previous afternoon/evening. The researcher would visit the

61
transferred patients and if they had a visitor the researcher would approach them
and introduce herself and the study first checking if they met the selection criteria.
An information sheet (Appendix C) was provided and any questions answered.
Following time for discussion and the answering of any questions, verbal consent
to participate was requested and they were invited to complete the questionnaire.
The questionnaire took about five minutes to complete. The researcher noted their
relationship to the patient.
As the questionnaire had not been previously tested, content validity was checked
with six participants. Following normal recruitment and completion of the survey,
the researcher asked if the questions were clear and easy to follow. All responded
that it was clear and easy to follow the meaning of the questions. The conclusion
was made that the questionnaire required no changes for subsequent participants
and their data were included for analysis. Once 20 questionnaires were completed,
recruitment ceased. The data were collated for use in Phase Two where the
brochure was developed.
3.3.2 Sampling Framework
3.3.2.1 Population
An expert panel of nurses was formed. All members of the Australian College of
Critical Care Nurses (ACCCN) Education Advisory Panel were invited to
participate along with the study site’s ICU nurse educator, and a nurse educator
from the general wards. ACCCN is the professional body for critical care nurses
and would therefore be able to contribute significantly to discussion on issues
related to ICUs. The Educational Advisory Panel provided the researcher with a

62
finite group innately interested in issues in the critical care arena. Their
involvement pays testament to their commitment and interest in professional
development in the area of critical care nursing education and perhaps research.
Others on the expert panel included educators from both the participating ICU and
general wards. It is suggested that they add another dimension to the discussion
as they work within the study site environment and their educative role provided
them with an intimate knowledge of current procedure and understanding of
patients’ needs. In addition, they provided educational support to staff in this
study and therefore their knowledge of the research project could see them act as
informal support persons for the nurses. In particular, this may occur in the ICU
environment where the intervention was introduced in Phase Three of the project.
The selection of two educators as opposed to clinicians was an attempt by the
researcher to provide distance between the Phase One study participants [nurse
educators] and subsequent patient transfer and data collection from participating
families. Educators do not provide continuing client care and therefore are not
responsible for family and patient transfer from ICU to the ward.
As outlined previously, information was also collected from family members. The
participants constituted a second population for this section of Phase One data
collection – family members whose relative had been transferred from ICU to a
general ward.

63
3.3.3.2 Sample (1) Expert panel consisting of:
• Consenting registered nurses from the ACCCN Education Advisory Panel,
• ICU nurse educator, and
• General ward nurse educator.
(2) Family members: The sample size for family members in Phase One of the
study was set at 20 participants. This was justified on the basis that the
information obtained from this cohort represented just one of three
components of the total information to be used for Phase Two. The other
components included information from research literature and from the expert
panel. As the expert panel was a finite number of ten participants, comparison
between family member and expert panel did not require large numbers.
The convenience sample consisted of those consenting family members who
fulfilled the inclusion criteria set out below. Individuals within this sample
did not form part of other phases of the study. Following discussion with the
ICU nurse managers, potential participants who met the selection criteria,
were approached by the researcher in the general ward. Both oral and written
information explaining guaranteed confidentiality and the purpose of the
questionnaire occurred. All family members visiting in the general ward were
approached and the final sample was determined by the voluntary response of
the family members and the sample size for this component of the research
project. Only one family member per patient was able to complete the
questionnaire.

64
3.3.3.3 Inclusion criteria (1) Expert Panel: currently either a member of the ACCCN Education Advisory
Panel or an educator in ICU or a general ward area at the study site.
(2) For family member:
[a] had a relative in ICU for a period of at least ten hours before being
transferred to a general ward;
[b] patient was not extremely unstable or dying;
[c] family member could understand, speak and read English;
[d] visited patient in ICU.
The exclusion of family members of patients who were extremely unstable or
dying was based on humanitarian grounds of not wanting to distress them further.
3.3.4 Data Collection and Analysis The researcher collated data from the expert panel’s responses to the
questionnaire. Of the ten questions, nine were closed questions with a five point
scale. Frequencies were calculated with these questions. One question was open-
ended and participants’ responses were transcribed in full. The researcher
distributed the collated data from the questionnaire the participants had previously
completed together with the open-ended question responses. For the open-ended
question, the researcher examined the data and coded the responses by searching
for differences and similarities between comments written by the participants.
This open coding method is suggested to be an effective way to group, or
categorises qualitative data (Rice & Ezzy, 1999) and further coding methods into
sub categories and core categories was not necessary as the data readily grouped
into five main categories based upon clearly evolving concepts (Flick, 2002).

65
The collated responses formed the topic for discussed at the focus group meeting.
Large pieces of paper easily read by all participants were used to group and list
the issues raised by the participants’ questionnaire responses. These same sheets
were used to document the prioritisation given to each issue within the categories
by the expert panel. The participants in the focus group had the opportunity to see
the researcher’s interpretation of the discussion prior to the meeting’s conclusion.
At this time each participant had the opportunity to verify that the researcher had a
true interpretation of the group’s decisions.
Following the focus group meeting, the researcher shared the collective results
with members of the expert panel who were unable to attend the focus group. The
participant had the opportunity to make comment upon the outcomes from the
focus group meeting and their thoughts were included into the final version for the
draft brochure.
The second aspect of data collection in Phase One related to information gathered
from family members whose relative had transferred from the ICU to a general
ward. The questionnaires from the family members were collected by the
researcher at the time of completion as all participants chose to complete the
questionnaire at the patient’s bed-side.
The researcher collated participants’ questionnaire data with frequencies
calculated for all 11 closed questions and the open-ended responses were
transcribed in full. A similar method of coding was used to that described for the
expert panel qualitative data. The combined data from the expert panel and the

66
family surveys were organized to form the basis for the information contained in
the brochure.
3.4 Phase Two: Brochure Development During Phase Two, a brochure was developed and commercially produced
(Appendix E). Lange (1989) recommends the use of a tool such as a brochure to
help direct conversation, present individualised information, and provide a written
record for future reference. The material to be used within the brochure was
collected in a manner to ensure it complied with the principles of Knowles’ Adult
Learning Theory (1980) in that the information was problem centred and was
directly applicable to family members in their real life situation with a critically ill
relative about to be transferred out of ICU.
To facilitate broadband usage of the information, it is suggested that the language
level of the brochure should be between the literary level of fifth grade (Maillet et
al., 1993) and ninth grade (Macey & Bouman, 1991). Based upon this, the
researcher chose an eighth grade level of literacy for the written brochure content.
An A4 piece of paper with two equal columns containing general introductory
and directed prompt questions, or statements, was developed by the researcher
from Phase One data. This was sent to three grade eight teachers with a feedback
sheet for comment. There were six questions on the feedback sheet. The first
asked if in their opinion the brochure was clearly written for an eighth grade
audience. They reviewed the brochure content to ensure the level of literacy was
maintained. It was important that the brochure was clear and easy to read. Their
comments and suggestions were incorporated into the next draft of the brochure.

67
This was taken to senior nursing personnel within the research site to request
further suggestions for improvement of the brochure. These personnel included:
• ICU educator
• Assistant Director of Nursing (Medicine)
• Assistant Director of Nursing (Surgery -General wards)
• Assistant Director of Nursing (Surgery - including ICU)
Where possible, their feedback was incorporated into the next Draft Brochure. A
visually appealing document would support the brochure’s use and a graphic artist
was enlisted to assist with the provision of a product which was both engaging and
professional in appearance.
The researcher chose not to seek feedback from the critical care nurses in ICU as
Phase Four of the study requested feedback from the ICU nurses on the efficacy of
the brochure and the pre-transfer educational method. Critical care nurses’
involvement in the production of the brochure, it is suggested, may have affected
their response on its efficacy and therefore influence data results.
3.4.1 Sample A convenience sample of three teachers who regularly teach eighth grade students
provided the sample for Phase Two. The researcher approached male and female
teachers to ensure there would not be a gender bias. Teachers from both
government and non-government sectors were chosen to ensure literacy levels
from both sectors were considered. This is not to infer that one sector is different
to the other but rather as a demonstration of completeness in the research method.
Following communication about the project and the information contained in the

68
draft brochure, an invitation and information letter (Appendix F) was sent to the
teachers who were known to the researcher.
3.4.2 Inclusion Criteria (1) currently teaching eighth grade students
(2) male and female teachers within sample
(3) representation from government and non-government schools
3.4.3 Data Collection and Analysis The participants were sent a form on which they were to respond to the material
contained within the draft brochure. This teacher feedback sheet simplified and
formalised the teachers’ responses. Reply paid envelopes were provided to the
participants for the return of their feedback sheets (Appendix G). The researcher
collated the comments from the two male and one female teachers. As non-
nurses, the teachers were naive readers and thus provided important feedback to
the researcher from the perspective of potential family members. The researcher
was very close to the subject content and at times made assumptions regarding the
clarity of information. The suggestions were incorporated into the next draft of the
brochure.
The appointed hospital photographer, under direction of the researcher, took a
number of photos in and around the ICU for potential use in the brochure. In
accordance with usual hospital protocol, no photos were taken where it might be
possible to identify a patient. One serendipitous photo of a patient and their
family member leaving the unit to a general ward was taken. As the
69
accompanying nurse and family member’s face may have been discernible,
although at a distance, the researcher sought consent for its potential use. The
nurse’s consent was obtained and the photographer developed the coloured photo
to A4 size to allow the researcher to show the family member the photo before
asking for its potential use in the brochure. This consent was readily given to the
researcher in the presence of a witness, a registered nurse from ICU. The final
version of the brochure was given to a graphic artist who designed the brochure in
association with the researcher. This was commercially printed. The Assistant
Director of Nursing (Surgical – including ICU) reviewed the final colour version
and gave written endorsement for its use. Copies of the final brochure were
printed at the expense of the researcher with copies sent to the Assistant Directors
of Nursing and the hospital and university ethics committees for their records.
3.5 Phase Three 3.5.1 Research Design A pre-test, post-test design was used to evaluate the impact of a structured pre-
transfer educational method of transfer upon the family members’ ‘uncertainty in
illness’, level of anxiety, and satisfaction with the transfer procedure. Outcome
data were gathered for the control and intervention groups, before and after
transfer from ICU. The control group participants experienced the existing
transfer procedure which was operational in the study site ICU. There was no set
method of transfer in the unit and nurses transferred patients based upon
individual methods.
Daily during the data collection period, the researcher ascertained those patients
likely to be transferred that day and as family members visited in ICU the

70
researcher approached them and following an introduction, informed them of the
aims of the project. Following time for questions, an invitation and information
sheet were given to the family member. This was followed by the consent form
which required a witness signature (Appendix H). Once consent was obtained, the
questionnaire was given to them. The researcher remained nearby should they
have any questions on the self-administered survey. Generally, however,
participants requested the researcher to read and mark the questionnaire for them.
The researcher ensured that the participant at all times was able to see the
responses being made on the participant’s behalf on the form. Only one survey per
patient was permitted. This was to ensure the results would not be skewed by
many responses from a few patients’ many family members.
The first questionnaire in the pre-transfer period for both the control and
intervention groups, was distributed while the patient was in ICU, prior to the
nurse’s transfer preparation. Following completion of the 78 question survey,
which took approximately 15 minutes, the researcher organised a time the
following day when the family member planned to visit the patient in the general
ward. The next day, the researcher met with the same family member and gave
them the second questionnaire (80 questions) in the post-transfer period. These
questionnaires were all completed within 48 hours following transfer as suggests
by Simpson, Armstrong and Mitchell (1989). Outside this timeframe, family
members may have a reduced recall about transfer which could impact upon their
responses.

71
3.5.1.1 Pilot A pilot period with a sample of ten participants was conducted. The entire
questionnaire in both the ICU and general ward was used for three reasons.
Firstly, the researcher wanted to ensure the time taken by participants was not
excessive. Secondly, parts of the questionnaire, although extensively tested to
ensure content validity and reliability, were designed in the United States of
America and the researcher wanted to ensure that minor language nuances did not
impair understanding by the participants. Finally, the researcher developed part of
the questionnaire and the pilot period provided feedback on the clarity and content
validity.
The ten participants were each asked if the questions were confusing or if the
questionnaires were too long or difficult to understand in any way (Appendices J
& K). They were also asked if they had any overall comments about the
questionnaire. All responded that the questions were easy to follow and as the
questionnaire took between 12 and 15 minutes each, the questionnaires’ length
were not stated to be problematic for participants. No changes were suggested by
the sample.
At the completion of the pilot period, two typographical changes to Post-Transfer
questionnaire were made. No changes were made to the pre-transfer questionnaire.
The researcher observed that some participants in answering Question 51
appeared confused by the presence of two boxes into which to place their answer.
Instead of adding together the number of close friends and relatives they have and
putting this number in the boxes, they were putting in for example, six and seven

72
in each box. This could be interpreted that they have 67 close relatives and friends
but in reality they had six close friends and seven close relatives. As the
researcher was with each of the participants during the completion of the
questionnaire, a check of their true intention was possible. After the pilot period,
all questionnaires had only one box for the answer to this question and this change
resolved this potential difficulty. The second change was a spelling error which
was corrected for the subsequent questionnaire. The pilot period proved
satisfactory and met the aims by being completed in a reasonable time frame, was
readily understood and was clear in its intent. Therefore, the pilot data were
included in the subsequent analysis.
3.5.1.2 Control Group Data collection for Phase 3 of the study commenced in January, 2002. The
researcher was present at the hospital daily in order to identify potential patients
for transfer and invite participation by family members when they visited in ICU.
Generally, visiting hours for the ICU were from 11am to 8pm during which time
the researcher remained in the unit for recruitment purposes. The researcher
approached either the nurse in-charge of the shift, a doctor, or the individual bed-
side nurse to ask if any patient was potentially for transfer to a general ward that
day. Inclusion criteria were also checked at this time. For some of the elective
surgery patients it was routine that patients remained in the unit only overnight
and so for these the researcher could anticipate their transfer plans.
When the transferring patient’s family member arrived to visit, the researcher,
after a period of time, would approach the bed-side and introduce herself and the

73
study. The researcher invited the family member’s participation and went through
the Information Sheets and Consent Form with them. The Consent Form required
their signature to be witnessed and this was provided by nurses, other family
members, or ancillary staff. The researcher was careful not to speak with the
nurses about the project other than to say the research was interested in family
members around the time of transfer. This was undertaken in order to prevent any
nurse changing present transfer practices and thus tainting the data.
The researcher gave the participant the questionnaire which was coded to ensure
confidentiality. Some participants choose to stay by their family member’s bed-
side whilst others preferred to go to the waiting room outside ICU to complete the
questionnaire. A few of the participants discussed some of the questions with
other family members and collectively decided on their response. The only time
this was discouraged was for the anxiety component of the scale. It was important
in this section that whoever signed the consent form and was to complete the
second questionnaire, completed the anxiety component alone as the scale
measures one’s state anxiety which is an individual rating of anxiety. The data
before and after transfer were compared, therefore the same person was required
to completed this. Following completion of the first questionnaire the researcher
asked the participants if they knew when they would be visiting the patient the
following day and tried to make a time to meet for the second questionnaire.
The second questionnaire, coded the same way as the first survey for each
participant, was completed once the patient had been moved to the general ward
and had been visited in the ward by the family member. Once again, generally the
74
participants wanted the researcher to read the questions and fill out the
questionnaire for them, however, an increased number did self-administer this
questionnaire. A number of the questions in both questionnaires were the same
and perhaps they now felt they had an idea of what was involved and could
complete it by themselves.
A small number of family members did not know when they would be visiting
next and the researcher gave them a pager number and asked them to ring to
organise a meeting. This proved successful each time it was used. Another small
group, who did not know when they would be returning, asked to be given the
post-transfer questionnaire for them to complete after they visited in the ward. The
researcher instructed these participants that it needed to be completed within 48
hour following transfer and assurance was given that this would occur. The
second questionnaire was given to them in a self-adhesive envelope with a biro
enclosed. Each participant’s second questionnaire was coded beforehand to
ensure the matching of participant’s responses for data entry purposes. The
participant was asked to hand the completed questionnaire to a nurse in its
envelope. The envelope was addressed to the researcher in ICU. The site’s internal
mailing system returned these to the researcher. The researcher was able to check
that the 48 hour time-frame was adhered to by keeping details of transfer times
and questionnaire return times.
During the period of data collection, there was a small proportion of patients
readmitted to the unit. These patients and their family members were only

75
recruited once to the study. The control group (n = 80) was recruited over seven
weeks.
3.5.1.3 Intervention Phase Preparation Following completion of the control data collection, the intervention phase of the
study, the structured pre-transfer method of transfer, was introduced to the ICU
nurses. It was now opportune to disclose the aims and objectives of the project to
the ICU nurses. To this end, a number of strategies were implemented. Firstly,
after speaking with the ADON for ICU, the researcher wrote an article for the ICU
newsletter (“Critical Edge”). This in-house ICU newsletter invites contributions
from all staff members and often reviews a clinical issue. The project’s article
gave a brief overview of the project and invited participation for the intervention
phase. In the same issue, the ADON gave support to the project and its possible
contribution to ICU nursing.
Secondly, the researcher produced a summary poster of the project including the
intervention phase and this was placed on the Research Noticeboard within the
unit. All current projects were displayed on this noticeboard which was positioned
near the staff-room.
Thirdly, at the Nurse Practice Coordinator’s (NPC) invitation, the researcher
spoke about the study at a senior staff meeting. Four consultant doctors, ICU
Medical Director, NPC, ICU educator and the research coordinator were present.
A brief outline of the study was given and copies of the material contained within
the structured pre-transfer brochure were distributed for comment and discussion.
One participant highlighted that consent to speak with the family member about

76
the patient’s condition may need to be obtained from the patient prior to
discussion with the relative. The researcher agreed that registered nurses and
doctors would continue to ascertain this consent in the same manner as they
currently practise. No other queries were made regarding the material to be
included in the structured pre-transfer educational method. The researcher
considered it was important to be inclusive with the introduction of the
intervention phase as, in this case, the doctors may find themselves required to
speak with relatives about a patient’s condition in response to the structured pre-
transfer education session. It was also important to share research goals in a
collegial manner particularly in a close working relationship which occurs in an
ICU. During the pre-test period, the researcher by necessity had to be cautious
with information concerning the project but following that period open disclosure
would only serve to enhance the cooperation from those in the unit.
3.5.2 The Intervention The intervention for this study was called a structured pre-transfer educational
method for transfer. It involved the ICU nurse using a brochure to discuss with
family members information concerning the imminent transfer of the patient. The
nurses were educated about the methods to employ and this will be discussed
later. The intervention was grounded in Knowles’ Adult Learning Theory (1980)
and to ensure the intervention assisted family members in their understanding and
knowledge retention, the principles of the theory governed the manner in which
the intervention was implemented. In general terms this involved nurses giving
information directed towards real life problems which may arise as a result of the
imminent transfer from ICU. By engaging with family members, nurses could

77
gauge their readiness to learn about patient problems and in some cases, defer
discussion or speak in added depth to fulfill family members’ needs. The content
of the brochure will now be outlined.
At the beginning of the brochure there was an introduction which stated the
importance of family members to patient’s recovery and the natural progression of
transfer to a general ward. The ICU nurse would progress through the material
contained within the brochure sequentially to discuss the patient’s condition
(Appendix E).
The brochure was designed to be individualised for each family and had spaces
for the patient’s name to be entered along with the projected time of transfer,
ward, doctor and NPC’s name in the new ward. The brochure contained sentences
which acted as prompts for the nurse and covered five areas. The five area
included: transfer plans, ward information, staff information, expectations in the
general ward, and support services for family members.
The first was the area of planning for transfer. The nurse would ask “Do you
know the plan of care for…?” Depending on the answer to this, the nurse would
inform the family member of relevant information based upon the family
member’s current knowledge and understanding and include the plan and timing
for transfer. Treatment could be discussed under this heading and expected length
of stay discussed or they would be referred to the ward nurse for this information
This area of discussion was at times extensive and may have involved other health
care team members such as the intensivist or social worker.
78
The second section on the brochure led the nurse to explain information on the
new ward. Its name, location, visiting hours, phone number and how to get there
was explained. Any special information pertinent to that ward was highlighted,
for example, in the Infectious Diseases Ward, no flowers were allowed and some
wards restricted visitors to two at a time. The speciality of the ward was
explained, for example, it may have been the post-operative cardiac surgery ward.
The research site had a policy whereby all ICU patients were transferred to their
optimal ward and they were not transferred to other wards. This was
advantageous as at this point in the transfer discussion, the ICU nurse could
reassure family members that the new ward staff specialized in caring for people
with the patient’s condition.
The third area gave information regarding the staff in the new ward. The ICU
nurse explained that a new medical and nursing team would be caring for the
patient and the names of the doctor and nurse in charge were written on the
brochure for future reference. Family members were told that the models of
nursing would be different and that the patient’s condition now allowed for a
nurse to care for a number of patients. It was highlighted that this indicated the
patient was requiring less extensive nursing which was a positive outcome.
Should the patient continue to require allied health professionals, it was explained
that the new ward had their own team.
The fourth area for discussion was the different patient expectations in the general
ward. Issues specific to the patient were highlighted and may have included
information on the patient becoming more independent (but this was dependent

79
upon individual patient condition and thus was dependent upon each case).
Family members were informed that daily ward rounds occurred in the general
ward and that they should ask the nurse when these occurred and how to arrange
to speak with the doctor or other team members. The fact that ICU style
monitoring equipment would no longer be necessary was highlighted as a positive
indicator of their improved condition.
The final area included support for family members. It gave the ward nurse as the
first point of contact should the family member have any concerns about the
patient or should they want to speak with a social worker or chaplain. The length
of discussion involved in this transfer planning procedure varied in response to
family members’ questions or comments. The personalised brochure was given to
the family member to take with them for future reference.
3.5.2.1 Recruitment of ICU nurses
The researcher needed to recruit ICU registered nurses who, in their usual
working day, transferred patients and family members to the ward. Without
registered nurses’ cooperation, the intervention phase would not be possible.
Obtaining their interest, involvement and ultimate consent was vital to the success
of the project.
As only those nurses transferring patients were eligible for the intervention phase,
the unit managers, educators and other off-line nurses were not able to be
included, as their role did not include direct patient care. A list of nurses working

80
in the unit was printed and those eligible to participate were highlighted for the
researcher. There were 120 nurses who constituted the potential sample.
A ward meeting was used as one forum to invite participation. The researcher
provided chocolates which were handed around during the overview and
subsequent discussion about the project. Once the researcher had spoken and
answered questions, she left the room asking them to read the information sheets
and sign the Consent Form if wishing to participate (Appendix I). The Consent
Form required a witness signature. The manner in which the researcher, who was
not an employee of the hospital, left the room ensured no pressure was placed on
potential participants.
This ward meeting yielded 11 nurses’ signed Consent Forms from the possible 14
who were present. As with all critical care areas, it was difficult to speak with
large numbers of staff at any one time due to patient care needs. In the ICU
environment where hand-over was at the bed-side on a one-to-one basis, there was
not the opportunity to speak at the daily shift changes which were often available
in general wards. Thus, the researcher proceeded to speak with ICU registered
nurses at the bed-side on a one-to-one basis to inform them of the project and to
invite their participation. The researcher was assisted in this by the ICU research
coordinator who also spoke with nurses about the project and invited their
participation.
The recruitment period extended over a two-week period, including weekends. It
was important to ensure recruitment extended to the weekend period as a number

81
of part-time ICU nurses only work on the weekend. As the researcher intended
collection data from family members on all days of the week, weekend nurses
constituted an important component of the sample.
Following the recruitment phase, an educational phase was implemented. Two in-
service education sessions were used to discuss with the nurses the project and the
content of the structured pre-transfer educational brochure. A strong emphasis on
the importance of a consistent process for transfer was made in all the educational
sessions so that all nurses followed the outlined structured procedure. Overheads
were used for one session and a power-point presentation for the other. This was
in response to the equipment available in the room. After a brief overview of the
project and methodology being used, the researcher highlighted the exclusion
criteria for family members. The intervention was the primary focus for the half-
hour sessions with the commercially printed brochures distributed for perusal.
This permitted those present to individually view the developed material which
was to act as a prompt for their transfer communication session with family
members. Questions were answered by the researcher who once again provided
chocolates for those present. Discussion ensued around the general topic area but
no nurse indicated concerns about the content or process to be followed.
Fourteen RNs attended the first in-service and eight, the second. An added bonus
was that four additional consents were received following these sessions. The
nurses had either been on night-duty during the recruitment period or on leave.
For those nurses not at the in-service sessions, the researcher decided to give one-
on-one instruction about the brochure’s content. A record was kept on each nurse

82
to ensure an educational session was given to all consenting nurses before the
introduction of the intervention phase data collection commenced.
The researcher spoke during the orientation period with all new nurses who
moved to work in ICU after completion of the recruitment period and within the
data collection period. They were informed about the project and invited to
participate. The invitation, information and consent form were provided and to
those consenting nurses, one-on-one instructions followed regarding the structured
pre-transfer educational method.
3.5.2.2 The Intervention Phase Following the ICU nurses recruitment period the intervention phase commenced.
That is, all consenting nurses transferred patients and family members from the
unit following the structured pre-transfer educational method for transfer. Data
were then collected from consenting family members of patients who were to be
transferred from the ICU to the general ward area in what was now the
intervention group.
Potential participating family members were approached by the researcher in the
same way as with the control group. This time however, the researcher had to
ensure the nurse caring for the patient was participating in the study. Only those
who were participating could be approached by the researcher who carried a list of
participating nurses. Agency nurses and nurses pooled from elsewhere were not
included in the study. As with the control group, the first questionnaire was
completed in ICU before the nurse had commenced the structured pre-transfer

83
education. The researcher would then fill in some details on the brochure to
individualise the information for the relative. For example, the researcher would
add the patient’s name, the name of the general ward, the consultant, and the nurse
in charge of the ward. The researcher then gave this brochure to the nurse at the
bed-side in ICU telling her/him that the family member was participating in the
study and required the transfer information as outlined in the brochure. The nurse
would go through the content of the brochure with specific reference to the
patient. Frequently this stimulated conversation and questions. On more than one
occasion a doctor was asked to speak with the relatives as they indicated they had
very little (if any) knowledge of the plan of care for their relative. The family
member was given the filled in brochure to keep following the structured pre-
transfer discussion with the nurse. After transfer to a general ward, the same data
collection method was used by the researcher to collect the post transfer
questionnaire as for the control cohort.
3.5.3 Sampling Framework 3.5.3.1 Control Group
Population
All family members who had a relative in ICU constituted the population.
Sample
A convenience sample of 80 participants was selected from the total adult
population of family members visiting an ICU patient prior to transfer. Following
informed consent, all eligible family members were surveyed. Only one family
member per patient was permitted to participate. The sample size for Phase Three
of the study was determined by power analysis (Talbot, 1995) which indicates the

84
ability of the study to detect changes or associations within the population (Burns
& Grove, 1995). There are four components to power analysis – level of
significance, sample size, size of the effect, and the power (Talbot, 1995). The
level of significance was set at 0.05 to reduce Type 1 error, and the power was set
at 0.8 to reduce Type II error. The effect size was calculated to detect changes of
five units for anxiety, based on previous study results (Bouvé et al., 1999; Wong
& Bramwell, 1992) and eight units for ‘uncertainty in illness’. The desired sample
size per cohort for an alpha of 0.05 and power of 0.8 was 50 per group. In
recognition that the above power analysis can be affected by a number of factors,
it was decided to increase the desired sample size to 80 sets of completed
questionnaires to ensure an adequate power. Attrition occurs in all research and
therefore needed to be factored into the sampling framework. As data collection
for the post-transfer period generally was the day after the first questionnaire, the
researcher was able to quickly assess retention rate and ensure the correct sample
size for both cohorts.
3.5.3.2 Intervention Group Population All family members of patients in ICU constituted the population.
Sample A convenience sample of 82 participants was selected from the total adult
population of family members visiting an ICU patient prior to, and after, patient
transfer to a general ward. Following informed consent, all eligible family
members were surveyed before the critical care nurses gave transfer information.
The optimal sample size for the study had been set as the same for the control and
intervention groups to permit comparison of the groups.

85
3.5.3.3 Inclusion criteria for control and intervention groups
Inclusion criteria for family members were determined from clinical experience
and the literature:
(1) Patient was in ICU more than 10 hours
(2) Family member was over the age of 18 years
(3) Family member was able to understand, read and write English
(4) Reason for transfer was not for palliative care
It was considered that a patient stay of less than ten hours in ICU may be
insufficient to attribute any affect following transfer to their period in ICU. As this
unit accepted daily, routine post-operative cases who generally were transferred to
the general ward the following day, it was considered important to include this
group. An inability to understand and write English was considered a reason for
exclusion as the tools were designed to be self-administered and nuances in the
language may cause misinterpretation. The researcher acknowledges that relatives
who are of non-English speaking background will also potentially experience the
phenomena under investigation but the tool may not be sensitive and provide a
true reflection of their anxiety and uncertainty. Finally, the researcher did not
want to impose on already stricken relatives who have been informed that the ICU
has no further treatment options to offer their relative. There was also a potential
difference in their experience of transfer which would definitely not be positive.
3.5.4 Variables The dependent variables include factors potentially influencing family members:
• Level of state anxiety,
• Level of ‘uncertainty in illness’, and

86
• Degree of satisfaction with transfer.
Additional variables measured were selected in response to literature in the area of
anxiety and ‘uncertainty in illness’ which suggests the factors below may
influence the dependent variables. These variables included:
• Gender of family member and patient,
• Age of patient and family member,
• Family members’ relationship to patient,
• Educational level of family member, and
• Social support available to family member.
As there was no previous published studies in the ICU area for ‘uncertainty in
illness’, the following variables were considered by the researcher to potentially
affect this phenomenon and hence the following data were also collected:
• Previous admissions or visits to ICU for family member,
• Patient length of stay (LOS) in ICU,
• Patient’s risk of morbidity (APACHE III score),
• Reason for ICU admission,
• Expected or unexpected nature of the admission, and
• Nationality of family member.
3.5.5 Procedure for data collection The control and intervention groups pre-transfer questionnaire contained 76 items
(Appendix J) which included questions relating to participants’ socio-
demographic details (age, gender, nationality, education, social support,
relationship to patient) and previous admissions or visits to an ICU. The
questionnaire also included two other self-reporting scales - the State Trait

87
Anxiety Inventory (STAI), and Mishel’s (1983) Parent Perception of Uncertainty
Scale - Family (PPUS-FM). The patients’ LOS and APACHE III score were
obtained from ICU records.
Control and intervention groups after transfer questionnaire consisted of 80 items
(Appendix K). They included the State portion of the STAI, the PCUS-FM, the
MOS SSS (Sherbourne & Stewart, 1991), and ten questions relating to family
members’ satisfaction with the transfer process. Two final items were open-ended
questions allowing participants the opportunity to make individual comments
regarding the overall process of transfer. This was designed to provide family
members with the opportunity to comment on an issue important to them or one
not raised by the researcher.
The researcher remained with the subject during completion of the questionnaire
to clarify any points and promote questionnaire return. There were however,
alternative methods for questionnaire return. A sealed internal envelope addressed
to the researcher via ICU was provided to relatives requesting them.
Descriptive statistics have been used for socio-demographic data including
frequencies, means and standard deviations. The reason for the patient admission
was grouped in categories to permit comparison of the control and intervention
groups. Family members’ and patients’ age was also grouped to more readily
compare groups. Chi square and t-tests have been used to compare differences in
demographic data results between the control and intervention to check for
homogeneity of the two samples. The data collection tools will now be discussed.

88
3.5.6 Instruments
3.5.6.1 Acute Physiology, Age, Chronic Health Evaluation III (APACHE III) The purpose of the APACHE III is to accurately predict the hospital mortality risk
for critically ill patients within 78 major medical and surgical risk categories
(Cooper, Sirio, Rotondi, Shepardson, & Rosenthal, 1999). The APACHE III scale
(0 –299) attributes scores to the patient’s age, severity and type of disease, and
comorbidities (Knaus et al., 1991) with the higher number indicating a higher risk
of mortality. This calculation of severity of illness scale contains three parts:
physiological data, a rating assignment for age and a rating for chronic illness
(Higgins, 1999). Knaus et al. (1991) reported with their prospective study of
17,440 ICU clients in 40 hospitals that for 95% of admission the APACHE III
score of risk of hospital death within 24 hours of admission was within 3% of
what in reality occurred. This high level of accuracy allows for objective analysis
of the patient’s predicted outcome with the limitation that after the initial 24 hour
period, an updated score may be needed to predict individual time related risk
(Knaus et al., 1991). The APACHE III rating scale allows the researcher to
reliably measure the patient’s outcome of illness as a dependent variable in the
study with the reliability and validity tested (Knaus et al., 1991). Comparison of
differences between the control and intervention groups’ APACHE III score were
made by using independent t-test analysis. An advantage of the APACHE III tool
is that it is sensitive to illness progression and provides a daily score of severity of
illness whereas the APACHE II score assigns only one score per patient at the
time of admission (Knaus et al., 1991). The APACHE III score acknowledges that
a patient may be admitted for routine post-operative management and hence have
a relatively low Day One score (that is, APACHE II score). If the patient,

89
however, experiences acute complications with haemodynamic impairment, the
APACHE III score takes into account this information on a daily basis and thus
gives a true reflection of the patient status over their period in ICU. It is
suggested in this study, the degree of severity of illness throughout the ICU period
may impact on family members’ anxiety and uncertainty around the transfer
period and therefore the highest APACHE III score was used for analysis. The
site ICU staff routinely collect APACHE III scores on all patients.
3.5.6.2 State Trait Anxiety Inventory for Adults (STAI) Designed by Spielberger in 1968, the STAI measures the psychological
parameters of both the state and trait anxiety levels. The state or situational
anxiety level, refers to the temporary feelings of anxiety perceived by a person in
a particular situation (Spielberger et al., 1983), whereas, trait anxiety refers to the
innate tendency to feelings of anxiety. The instrument consists of 40 items, 20
relate to how a person currently feels and the remaining 20 ask how a person
generally feels (Spielberger et al., 1983). The instrument has undergone extensive
psychometric testing and was found to be a valid and reliable tool to measure
anxiety (Spielberger et al., 1983). Although both state and trait anxiety were
collected from the sample, the state version has been used for analysis as it
accurately detects altered anxiety levels in differing sets of circumstances as one
experiences in ICU and then a general ward area. STAI-state has been extensively
used in the critical care area to examine the anxiety experienced by family
members and patients and is thus suggested as an appropriate instrument (Poe
1982; Raleigh et al.,1990; Rukholm et al., 1991; Lynn-McHale et al., 1997). The
alpha coefficients for the state version ranges from .83 to .92. The test-retest

90
reliability varies in response to an individual’s circumstances, and as expected, is
low (.40) (Spielberger et al., 1983).
A self-reporting Likert-type scale with four points, 1 = not at all to 4 = very much,
is used. The scoring procedure as outlined by Spielberger et al. (1983) has a rating
of 4 which indicates the presence of high anxiety for the ten state anxiety items
(for example, “I feel frightened”). A rating of 4 for the remaining ten items (for
example, “I feel calm”) indicate the absence of anxiety. The raw scores for all
items were entered unchanged and the scores for the absent anxiety items were
reversed, so responses of 4 were changed to 1 and so on. The total state anxiety
scores were added by the Statistical Package for Social Sciences (SPSS Version
10, graduate package). Total scores vary from 20 to a maximum of 80. Scores of
less than 33 equate to low anxiety, between 33 and 43 are medium anxiety scores
and between 43 and 55 are high anxiety scores (Spielberger, 1983). For
participants who omitted one or two items, the pro-rated scale score was obtained
as suggested by Spielberger et al. (1983). One question was inadvertedly omitted
from the questionnaire and to permit comparison with published norms, a new
score was calculated based on the individual mean score for each participant. This
strategy permitted a complete score with the additional item added reflecting
individual anxiety levels. Questionnaires with three or more missing scores were
excluded as their validity may be questioned.
Comparisons in state anxiety levels between the control and intervention groups
before and after transfer were made. The relationship between patient and family
member factors and STAI scores were also examined. A detailed description of

91
the analysis involved is presented later in this chapter where each research
question is discussed in relation to the statistical tests performed.
The STAI has been used by a number of studies within the ICU environment.
Lynn-McHale et al. (1997) evaluated the anxiety levels of both relatives and
patients following a peri-operative education program by using both the STAI and
a Visual Analogue Scale (VAS). Two non-randomised convenience samples were
formed. One group received standard pre-operative teaching while the
intervention group received the standard education plus an ICU tour. Family
members’ anxiety levels were significantly (p<0.05) higher than those of the
patient group. Results indicated that overall anxiety levels reduced following the
teaching sessions, however, there was no significance between the anxiety levels
of the control and intervention groups. That is, the ICU tour had no significant
effect on the anxiety levels of either the patient or family cohort (Lynn-McHale et
al., 1997). The study sample was made up of cardiac surgical patients and their
families and the study’s results suggest that both families and patients
understandably, are anxious about more than the ICU environment prior to cardiac
surgery.
Raleigh et al. (1990) also studied pre cardiac surgery education preparation for
relatives and patients. They used the STAI-state survey (Spielberger et al., 1983)
together with a questionnaire evaluating participants’ level of knowledge
following an education session. Relatives and patients prior to class, after class,
and the evening before surgery completed the State Anxiety Inventory. The
family members’ mean anxiety levels were significantly higher than those of the

92
patients and neither group’s anxiety reduced significantly following education.
The authors comment that had they measured fear rather than anxiety they may
have shown a significant result (Raleigh et al., 1990). Once again, this supports
the observation that the impending surgery was the overriding concern and
education did not reduce the anxiety it created.
Rukholm et al.’s Canadian study (1991) examined the needs, situational and trait
anxiety levels of relatives of critically ill patients in three ICUs in relation to three
variables. These included, spiritual needs, worries about the ICU environment and
knowledge of the ICU environment gained through previous experience or pre-
admission orientation. Results showed that both trait and state anxiety levels were
higher than reported by Spielberger et al.’s normative data (1983) suggesting that
participants experience anxiety in an ICU environment. Older subjects had
reduced situational anxiety compared with their younger counterparts in this study
(Rukholm et al.,1991).
Poe (1982) utilised the STAI to evaluate the effectiveness of pre-transfer teaching
for myocardial infarct patients upon transfer to a general ward. There was a
significant difference between the two groups (one received pre-transfer teaching
and the other group did not) with those having pre-transfer structured teaching
having significantly less anxiety. This article, however, has limited information on
the data collection methods used and the method of analysis which limits a full
evaluation or replication of the study.

93
Wong and Bramwell (1992) also used the STAI as an evaluation tool in the study
where the relationship between uncertainty and anxiety in 24 women after
mastectomy following breast cancer was examined. The state portion of the scale
was administered to participants one to two days (Time One) prior to hospital
discharge and one to two weeks (Time Two) following discharge. The trait
anxiety scale was administered at Time One. The Mishel’s ‘Uncertainty in illness’
scale (1981) was used to measure their uncertainty in regard to the illness in
addition to semi-structured interviews at both Times One and Two. Two tailed
paired t-test indicated that uncertainty and anxiety were higher before discharge
than after, but the result was not significant at the 0.05 level. There was however,
a correlation between anxiety and uncertainty at the Time Two assessment and the
higher the uncertainty the higher the anxiety level for the sample. The relationship
described supports the concept that psychological evaluation of a personal
situation which results in uncertainty also see the subject experiencing anxiety
(Wong & Bramwell, 1992). No significant relationship was discovered between
the demographic variables, anxiety and uncertainty.
3.5.6.3 Parent’s Perception Uncertainty Scale – Family (PPUS-FM) PPUS-FM was developed by Mishel for family member as an adaptation of the
Mishel ‘Uncertainty in Illness’ Scale for adults (MUIS) developed in 1981 to
measure a patient’s level of uncertainty during an illness. Following the
development of the MUIS, which measures ‘uncertainty in’ illness for adult
hospitalised patients, Mishel modified the tool to measure other groups influenced
by ‘uncertainty in illness’. These groups include parents’ and families’ responses
to their child’s or relative’s hospitalization and illness, and individuals cared for in

94
the community (Mishel, 1983). The MUIS measures a personal evaluation of self
in regard to uncertainty whereas the Parent’s Perception of Uncertainty in Illness
tool (PPUS) and the PPUS-FM measure a parent or family member’s perception
of their uncertainty in relation to their child or family member’s illness. The scale
examining family member’s perception of ‘uncertainty in illness’ is called the
Parent’s Perception of Uncertainty in Illness – Family (PPUS-FM) scale and has
31 items (Mishel, 1997). A condition of use of the scale is that researchers need
to ask additional demographic and patient related questions. These include age,
gender and years of education of the family member, and the reason the patient is
receiving treatment.
There are four factors measured by the scale: (1) ambiguity, (2) complexity, (3)
inconsistency, and (4) unpredictability (Mishel, 1983). Ambiguity relates to the
perception by the subject that cues given to them about the illness are obscure or
unclear. Complexity, takes into account multiple treatment modalities and
elaborate processes of care required by the patient. Inconsistency, refers to a
disparity in the information given to the subject concerning an aspect of the
illness. Finally, the factor, unpredicability, examines the probability of illness
outcomes versus treatment modalities (Mishel, 1997). Mishel advocates, however,
that for the PPUS-FM tool, a combined four-factor score should be used as the
reliability coefficients for the subsamples were generally low for one factor
(Mishel, 1997). Support for the scale using different measurements and similar
concepts has been documented and test re-test studies support the reliability of the
instrument (Mishel, 1997).

95
Each item represents aspects of uncertainty on a five point Likert scale ranging
from strongly agree to strongly disagree. The larger the score, the larger the
amount of uncertainty experienced. The raw scores for all items were entered
unchanged and the scores for the absent uncertainty items (11 in total – for
example, “The purpose of each treatment for my relative is clear to me”) were
reversed, so responses of 5 were changed to 1, 4 to 2 and so on. The total
uncertainty scores were added by SPSS. Total scores vary from 35 to a maximum
of 155. The PPUS-FM administration directions instruct any questions deemed to
be ‘not applicable’ to the participant be assigned a “0” for that item (Mishel,
1997). These instructions were complied with.
Authors have used the PPUS-FM to determine spouses’ perception of uncertainty
in relation to their wife’s illness (Northouse, Laten, & Reddy, 1995) but no
published studies have been located on family members’ uncertainty in the area of
illness requiring ICU nursing. Thus the validity of the tool with this cohort is not
confirmed. Mishel (1997) reports the PPUS-FM tool’s reliability ranges between
0.81 to 0.92 across 15 data sets of family members having relatives with, for
example, alzheimers’ disease, cancer, multiple sclerosis, renal disease and
myocardial infarction.
Comparisons in PPUS-FM levels between the control and intervention groups
before and after transfer were made in the current study. The relationship between
patient and family member factors and PPUS-FM scores were also examined. A
detailed description of the analysis involved is presented later in this chapter

96
where each research question is discussed in relation to the statistical tests
performed.
3.5.6.4 Rand and Medical Outcomes Study - Social Support Survey The Rand and Medical Outcomes Study team has developed a 19 item survey
which measures social functioning as a measure of social support. Social support
refers to the ability to develop and maintain primary social relationships. As both
tangible and emotional support is thought to assist people in coping with stress
and illness (McDowell & Newell, 1996), it was an important variable to examine
with this study cohort.
The social support survey was developed for patients with chronic illnesses and
has been designed to be simple, brief, self-administered and multi-dimensional
(Sherbourne & Stewart, 1991). “Although the scale was designed for use in a
study of chronically ill patients, the items are universally applicable” (McDowell
& Newell, 1996, p.140) and have been chosen for this study for its multi-
dimensional approach and clarity of intent. Due to the lack of previous research
with this cohort however, the validity of this tool is not confirmed.
Sherbourne and Stewart (1991) suggest it is easy to administer as each item is
brief and limited to only one idea – for example, “How often do you have
someone to help you if you were confined to bed?” There are four possible sub-
scales: tangible support (four items); affection (three items); positive social
interaction (four items); and emotional or informational support (eight items). An
additional item, the number of close relatives and friends, represents a structural

97
support item (Ogden, 1996) and is the first item in the scale. Responses are
recorded on a five point answer scale with the score of one indicating the
participant has the support “none of the time” to the score of five where the
participant has the support “all of the time”. The scale has been extensively tested
with 2,987 participants for validity and the tool was found to be reliable with an
internal consistency for the entire scale of 0.97 (Sherbourne & Stewart, 1991). Its
validity has been confirmed by factor analysis and correlation with, amongst
others, loneliness, marital and family functioning, and mental health (McDowell
& Newell, 1996). Factor analysis suggests that the 19 items can be grouped for an
overall index that combines the 19 items’ scores (Sherbourne & Stewart, 1991). In
addition to the 19 items, there is one structural support item which asks “About
how many close friends and close relatives do you have (people you feel at ease
with and can talk about what is on your mind)?”
The raw scores for the 19 items were entered unchanged into SPSS and added
together to obtain an overall index for social support. The scoring system is
unidirectional for all 19 items with a higher score indicating more support. Total
scores vary from 19 to 95. The score for the additional item asking the number of
close relatives and friends was entered unchanged. Levels of social support for
the control and intervention groups were compared and will be explained within
the research question analysis section to follow.
3.5.6.5 Family Members’ Degree of Satisfaction
Ten items were developed by the researcher to examine family members’ degree
of satisfaction with transfer and formed part of the post-transfer questionnaire.

98
The items are based upon the literature which suggests that seven out of the ten
top needs of family members in ICU are in the area of information needs (Leske
1999, Molter, 1979). Although there is extensive literature on the needs of the
family, no scale was found which evaluated satisfaction with transfer.
Four items were designed to measure family member’s satisfaction with the
information regarding transfer (for example, “How satisfied were you with
information about the transfer of your relative regarding having your questions
answered honestly?”). Responses on the five-point scale ranged from “very
satisfied” to “very dissatisfied”. Five items related to the method of
communication used, for example, “Was the information given to you easy to
understand?” A mix of open-ended and fixed response options was used for these
items. The open-ended questions allowed participants the opportunity to comment
further on an aspect of transfer or to highlight an area not obvious to the
researcher. The final item asked respondents for an overall assessment of how
well prepared they were for transfer and possible responses ranged from “not at all
prepared” to “well prepared”. These items were tested in the pilot period together
with all other items of the questionnaire and were found by participants to be easy
to understand and clear in their intent, however, further research will be necessary
for validity and reliability testing.
The raw scores were entered into SPSS unchanged. The four information items
were tallied with a higher score indicating greater satisfaction with information.
The two communication items were also tallied. The third communication item
(“Was there anything that worried or frightened you?”) was examined in

99
association with the following open-ended question where the participant was
asked to comment on their response. The two open-ended responses were
transcribed in full and grouped according to categories or shared topic areas. Rice
and Ezzi (1999) suggest that this method of open coding is an effective method for
organising qualitative data using comparison and reduction.
Mean values for satisfaction and communication were compared between the
control and intervention groups and will be discussed within the research question
of this chapter. The qualitative data from the questionnaires have been transcribed
in full, grouped and reported under categories.
One researcher, not employed by the health facility, collected all the data. All
participants were informed of the independence of the researcher. Confidentiality
of data was assured to the participants and visible coding on the survey forms was
manifestation of one aspect of confidentially evident to participants.
3.6 Phase Four
3.6.1 Research Design An explorative descriptive study was used with a questionnaire developed by the
researcher to evaluate the critical care nurses’ perception of the usefulness of the
structured pre-transfer educational method together with their attitudes about
family members. Nine items requested feedback on aspects of the transfer process
and the nurses’ perception of the importance, or otherwise, of family to critically
ill patients. The questionnaire was piloted with five non-participating critical care
nurses to check for clarity and intent. As suggested, a reordering of two items

100
occurred to promote logical sequencing. These changes were made before the
questionnaire was used in the main study (Appendix L) and the pilot participants
did not participate in the main study.
3.6.2 Sampling Framework 3.6.2.1 Population All critical care registered nurses in the ICU constituted the study population.
Sample
The sample for the questionnaire included all consenting critical care nurses who
participated in the intervention. It was important to evaluate the intervention from
the critical care nurses’ perspective and those who had experienced using the pre-
transfer educational method were able to make informed comment based on
personal experience. The first question in the questionnaire asked how many times
the critical care nurse has used the structured pre-transfer method.
3.6.2.2 Inclusion Criteria
• critical care registered nurses in ICU
• utilised the structured pre-transfer educational method to facilitate the
transfer of a patient where the family member was part of the study

101
3.6.3 Procedure for Data Collection During Phase Three, ICU nurses were invited to participate in the study and the
information letter and discussion highlighted that the second component of
participation involved completing a small questionnaire at the completion of the
structured pre-transfer educational method data collection period. The consent
form for the intervention phase included consent for this phase of data collection.
Within the intervention period, the researcher noted all ICU nurses who
transferred patients and their consenting family members to a general ward using
the structured pre-transfer educational method. Following completion of the
intervention phase of the study, the researcher placed a questionnaire in each
eligible participating nurse’s pigeonhole in the staff-room. Each questionnaire was
coded to provide confidentiality and a method for accurate follow-up. Sealable
self-addressed envelopes were provided for the return of the completed
questionnaire.
A reminder note was placed in the pigeonhole of those nurses who had not
returned their questionnaire after a two-week period. A second reminder was
given to the remaining few outstanding participants a week later but no further
follow-up occurred. It was important to achieve as higher a rate of return as
possible to gain an accurate assessment of the efficacy of the transfer method from
the ICU nurses’ viewpoint but still allow participants the right to withdraw.
3.6.4 Data Analyses The first question quantifies how many times the participant used the structured
pre-transfer educational method. A further six quantitative questions were used to
obtain a measurable representation of participants’ opinions (for example, “Was it

102
helpful providing a framework for your discussion with the relative?”). In
addition, two open-ended questions allowed participants the opportunity to
comment on aspects that the researcher has not foreseen.
The raw data were entered into SPSS unchanged. Questions two and three were
re-coded to allow the numeric score to represent the discussion with the relative.
In both instances “not at all” and “not sure” were re-coded as zero and “minimal”
and “helpful at times” re-coded as one, in questions one and two respectively.
“Some discussion” and “quite helpful” were re-coded as two and “very helpful”
and “yes, a great deal” were re-coded as three. Re-coded questions two and three
were tallied to gain a score for the communication with the family member. The
other items were kept discrete and are reported individually either as descriptive
statistics or categories as required with the open-ended questions. These responses
were transcribed in full and grouped according to common topics.
3.7 Analytical Procedures for the Study As stated previously, the data were analyses using the Statistical Package for
Social Sciences (SPSS) Version 10.0, (1999) student computer version. Accuracy
of data entry was assured by a systematic review of every fifth questionnaire
(20%) checked against the computerised version. Data were re-entered in the few
cases (error rate .05%) where discrepancies occurred. Collected data were
reviewed for completeness and missing data were checked against original
questionnaires and where appropriate, sample means were used for isolated single
missing values (Spielberger et al., 1983). A visual check was performed on all
variables for range and logic of values. The distribution of variables was visually

103
found to be of normal distribution. Only those participants who completed both
before and after transfer questionnaires were retained. The remaining incomplete
data sets were deleted from the database.
The design and aims of the study directed the data analysis methods. Before each
statistical test was used, their underlying assumptions were examined. Statistical
significance is reported at an alpha level of .05. All t-tests were two-tailed in
nature.
3.7.1 Sample and the questionnaire
The reliability of the psychometric properties of the STAI – State portion, PPUS-
FM and MOS -SSS were assessed on the sample using Cronbach’s alpha. The
Cronbach’s alpha for STAI – State version ranged from .93 to .96 and for the
PPUS-FM it ranged from .88 to .92 across four assessment points. The MOS SSS
alpha ranged from .96 to .97 at two assessment points. The Cronbach’s alpha for
the sub-scale of family members’ satisfaction with regard to transfer information
recorded a score of .87 and .86 across two collection points. These alpha values
are high indicating the scales have demonstrated internal consistency. The alpha
for the nurses’ communication with family members’ sub-scale was quite low at
.55 and .45 so as there was insufficient overlap in the items to form a sub-scale,
each item was treated separately.
3.7.2 Demographic Variables Descriptive statistics were used to examine family members’ and patients’
demographic variables. Continuous variables including patient and family
members’ age, educational level, APACHE III score, and LOS in ICU were

104
described with frequencies, means and standard deviation, or median scores for
each cohort. Categorical or dichotomous data including the nature of admission
(expected or unexpected), patient and family members’ gender, nationality,
relationship to patient, reason for admission and previous admission or visits to an
ICU were described with frequencies and percentages.
Following the description of the above variables, the control and intervention
groups’ means were compared to detect significant differences. The categorical or
dichotomous data were analysed using Chi square analysis having first complied
with the underlying assumptions. Two sample t-tests were performed on the
interval and ratio data to compare means of the control and intervention groups.
When the underlying assumptions were not met a Mann-Whitney U test was
performed. The following section outlines the statistical tests for each of the five
research questions.
3.8 Research Questions Statistical Tests 3.8.1 Question 1. What is the level of ‘uncertainty in illness’ in family members before transfer
from ICU as measured by Mishel’s PPUS-FM scale?
The control and intervention group PPUS-FM scores were tallied from the before
and after transfer questionnaires. Descriptive statistics with minimum, maximum,
mean, and standard deviation were conducted. The distribution according to the
histogram was visually determined. Comparison of the control and intervention
groups’ means were analysed using independent t-tests, having established a
normal distribution existed. Another underlying assumption is that there are equal
105
variances and as this assumption was not met, the non-parametric Mann-Whitney
U test was used for analysis.
3.8.2 Question 2
Question 2.1 Was there a relationship between family members’ ‘uncertainty in
illness’ as measured by PPUS-FM (Mishel, 1997) and anxiety
levels as measured by STAI – state (Spielberger et al., 1983)?
‘Uncertainty in illness’ and state anxiety scores were collected and tallied for both
the control and intervention groups. The researcher wanted to ascertain if this
data could be combined for analysis of factors which may account for the variance
of these variables or if the samples needed to be treated separately. If combined,
the sample size doubled and would therefore increase the reliability of the results.
As with Question 1 and the levels of PPUS-FM scores, descriptive statistics with
minimum, maximum, mean, and standard deviation were calculated for STAI –
state scores for both cohorts. Distribution was visually checked. Independent t-
tests examining significant differences in the two groups’ mean scores were
performed. As these analyses indicated the control and intervention groups were
not significantly different in regard to PPUS-FM and STAI-state scores, the pre
transfer data sets were combined to detect relationships between the two
dependent variables. The relationship between STAI-state and PPUS-FM was
analysed using Pearson product-moment correlation analysis having first
examined the underlying assumptions.

106
Question 2.2 Were patient and family member’ factors significantly related to
PPUS-FM scores?
Question 2.3 Were patient and family member’ factors significantly related to
STAI – state scores?
Similar statistical tests were used for both these questions and they will be
described here together. A series of Pearson product-moment correlations were
performed using PPUS-FM scores and STAI –state scores before transfer and
factors with continuous data scores (age, APACHE III, education level, LOS, and
social support). One-way analysis of variance (ANOVA) was used for the
categorical data (gender, relationship to patient, ICU experience, APACHE III
score, and the nature of the admission) and PPUS-FM scores and STAI-state
scores. This test is used for a dependent variable (for example, PPUS-FM)
measured on an interval or ratio scale and when the independent variable is a
nominal or categorical scale (Polit, 1996). Post-hoc analysis with a Tukey test was
performed for the category, “relationship to patient” to detect which group had
different mean scores when compared with all other groups.
Nationality was not analysed as it did not meet the assumptions underlying
statistical tests due to the small and nonexistent numbers in some cells. It was
inappropriate to recategorize or collapse categories down as results would have
been meaningless.
Those factors which were significantly related to either PPUS-FM or STAI-state
scores were analysed using a multiple regression model. As one factor was
categorical in nature, dummy coding was necessary to create a series of
107
dichotomous dummy variables that contrast members in one category with all
others (Polit, 1996).
3.8.3 Question 3
Has the introduction of the intervention led to a reduction in the ‘uncertainty in
illness’ and state anxiety levels?
‘Uncertainty in illness’ and state anxiety levels were compared using the before
and after transfer period scores for the control and intervention groups to examine
any change. Control and intervention groups were examined as separate data sets
for both variables and paired t-test (two tailed) analyses were performed for both
the anxiety and ‘uncertainty in illness’ mean scores after examining the
underlying assumptions. Means, standard deviation and levels of significance
were calculated.
Following the paired t-test, an Analysis of Covariance (ANCOVA) was performed
as random assignment of the sample was not possible in this quasi-experimental
design (Polit & Hungler, 1999). Although the independent t-test of the pre-transfer
scores indicates a significant difference, pre-transfer scores could still influence
results (Polit & Hungler, 1999). An ANCOVA permits post-hoc statistical control
of the extraneous variables (pre-transfer STAI-state and PPUS-FM scores) and
thus reduce systematic bias as well as within-groups error (Coakes & Steed,
2001). Once underlying assumptions were checked, pre transfer scores (PPUS-
FM, STAI –state scores) were entered as the covariate and the post transfer PPUS-
FM and STAI-state scores as the dependent variable. Estimated marginal means
were calculated in the post-transfer period accounting for pre-transfer levels of

108
PPUS-FM and STAI –state scores for the two groups. The F value, degrees of
freedom, partial eta squared and significance level were calculated. A graph was
prepared for PPUS-FM and STAI-state scores to allow a visual representation of
the before and after transfer estimated marginal mean changes for the control and
intervention groups. The following section outlines the analysis associated with
Question 4.
3.8.4 Question 4 There are five parts to this question all of which relate to how family members
perceive components of their transfer from ICU. The five parts to the question are
now outlined.
Question 4.1 Has the introduction of the intervention led to an improvement in
family members’ satisfaction with regard to their information
needs?
Satisfaction with information was measured by four questions in the after transfer
questionnaire. The Cronbach alpha coefficient was found to be .87 and .86 for the
control and intervention groups respectively. With internal consistency adequate,
the scores for the four questions were tallied with the median scores calculated for
both groups. The difference between the two groups was compared having first
checked statistical assumptions. The histogram for both groups was skewed and
therefore an independent t-test was inappropriate. The non-parametric Mann-
Whitney U test was employed to analyse the differences between the two groups
scores. The Z value and level of significance were calculated.
109
Question 4.2 Has the introduction of the intervention led to an improvement in
ICU nursing staff communication with family members?
The second component of Question 4 examined how family members perceive the
communication by the ICU nurses about patient transfer plans. Two questions on
the after transfer questionnaire examined this attribute. As the Cronbach alpha
coefficient was quite low at .55 and 45 for the control and intervention groups
data, there was insufficient overlap in the items to form a sub-scale.
Consequently, the two questions were analysed individually.
Mean and standard deviation scores from the first question were calculated for the
two groups. To compare these results, an independent t-test analysis was
performed after examination of the underlying assumptions. The t value, degrees
of freedom and level of significance were calculated.
The analysis was repeated for the second question, however an underlying
assumption of the independent t-test was not complied with as variances were
unequal. Consequently, a Mann-Whitney U test was performed to examine
significant differences in the control and intervention groups’ mean scores.
Question 4.3 Has the introduction of the intervention led to an improvement in
the overall preparedness of family members for transfer?
The third part of Question 4 examined the perception of the family member on
how well prepared they felt for transfer to a general ward. This constituted one
question in the after transfer survey with a five-point scale from “not at all
prepared” to “well prepared”. Examination of the histograms showing negative

110
skewing towards being better prepared required the use of a Mann-Whitney U test
to examine differences in the control and intervention groups’ mean and standard
deviation scores. Z scores and level of significance were calculated.
Question 4.4 Were family members’ worried or frightened by information given
to them and what was the information that caused this concern?
There were two components to this part of the question which had both
quantitative and qualitative questions. The first question asked family members to
quantify on a three-point scale the concerns they experienced as a result of the
information given to them by the ICU nurse. Frequencies, percentages, mean and
standard deviations were calculated for both groups. Statistical comparison of the
two groups’ means did not permit the use of a two-sample t-test due to unequal
variances, hence a Mann-Whitney U test was performed. The level of
significance and Z score were calculated.
The second part to this question was an open-ended question allowing participants
to comment on what worried or frightened them. Responses to this question were
transcribed in full. Following examination of the data the researcher coded the
responses by searching for differences and similarities between comments written
by the participants. This open coding method is suggested to be an effective way
to group, or categorises qualitative data (Rice & Ezzy, 1999). Further coding
methods into sub categories and core categories was not necessary as the data
readily grouped into major categories based upon clearly evolving concepts
(Flick, 2002). Frequencies and percentages of responses within each category
were calculated for the control and intervention groups. Examples from each

111
category were reported verbatim to demonstrate the types of comments made by
participants.
Question 4.5 What information did family members wish they had been told?
An open-ended question asked participants for the information they would have
liked prior to transfer. This data was treated similarly to the previous question’s
qualitative data in that participants’ comments were transcribed in full and
examined for categories fitting the comment. Frequencies and percentages were
calculated for each group and each category. An example of the verbatim
comments for each category are reported. The following section outlines the
analyses applied to Question 5 data.
3.8.5 Question 5 Question 5.1 What was the ICU nurses’ perception of their unit’s attitude to
families and how important were family members to patients’
recovery?
Nurses were asked their unit’s attitude to family members by way of a five point
scale in the questionnaire given to those nurse who had used the intervention.
Frequencies and percentages were calculated. Participants were also asked the
level of importance of family members to patients’ recovery. Frequencies and
percentages were similarly calculated for data from this question.

112
Question 5.2 What was the ICU nurses’ perception of the level of importance of
the process of transfer from ICU for families?
This one question asked participants to record on a five-point scale how important
they thought the transfer process was for family members. Frequencies and
percentages were calculated.
Question 5.3 Has the intervention provide a useful means to improve discussion
with family members from ICU nurses’ perspective and would they
recommend its use?
Participants were firstly asked to record how many times they had used the
intervention with a selection of four choices from once to more than ten.
Frequencies and percentages were calculated. Two questions related to the
discussion which occurred as a result of the intervention. One asked if the
intervention provided a framework for discussion and the other asked if it resulted
in discussion with the family member about the patient. Responses to these
questions were described using frequencies and percentages. The final part of this
question asked participants if they would recommend the introduction of the
intervention into their workplace. They were given four choices from “no” to
“definitely”. Their responses are described using frequencies and percentages.
That completes the report on the analyses performed for all five research questions
and the ethical considerations for this study will follow.
3.9 Ethical Considerations The research was approved by the hospital and Queensland University of
Technology Human and Research Ethics Committees. All potential participants

113
were given verbal and written information sheets about the study and informed of
their right not to participate. The researcher made very clear to all potential
participants that she was not an employee of the study site or affiliated with it in
any way. Participants were assured that they could withdraw at any time without
explanation and not answer any question as they chose. Opportunities were
provided for participants to ask questions at any stage. Consent was obtained prior
to enrolment in the study. No names appeared on any questionnaires or feedback
sheet and a coding system known only to the researcher was employed thus
ensuring confidentiality for all participants. All data has been kept in a locked
cabinet and will be for a period of seven years after which it will be destroyed in
accordance with the National Health and Medical Research Council guidelines.
3.9.1 Potential Risks
The researcher who has extensive critical care nursing experience collected all
data for the study. There were no foreseeable or known actual physical or
psychological risks to participants in this study. The study did not challenge the
participant nurses in any way and as the researcher was not an employee of the
facility they should not have felt threatened professionally. Family members had
data collected with existing or new transfer procedures and neither method
challenged family members but rather provided information. Potential
psychological risks stemmed from the intrusion on family members’ time visiting
the patient in ICU and the ward. When a family member appeared to become
distressed, questions would be asked as to the availability of immediate and on-
going support. Strategies for support and counselling were in place with letters of
support from the hospital chaplain and counselling services.

114
3.10 Chapter summary
This chapter outlined the rationale for the study design and the research strategy
with each phase’s sampling framework and data collection methods. Data
collection tools were explained and reliability coefficients reported. Analytical
procedures were outlined in relation to each of the five research questions. Ethical
considerations and potential risks completed the chapter. The following chapter
outlines the characteristics of the sample.

115
CHAPTER 4: DESIGNING THE INTERVENTION
4.0 Introduction
The previous Methodology Chapter describes the study design and analytical
procedures performed in each of the four phases of the study. Ethical
considerations and potential risks were outlined. This chapter presents the results
of Phase One and Phase Two. Results of the two phases informed the content for
the development of the educational brochure which occurred in Phase Two.
Phase One and Phase Two of the study were investigative and informed the
development of the educational brochure used within Phase Three of the study.
The aim of Phase One was to acquire important and relevant material for the
content of the brochure. The second section of this chapter outlines the results of
Phase Two of the study. This phase involved teachers of eight grade students
reviewing the draft brochure developed from information collected in Phase One.
The aim of this phase was to ensure the content of the brochure was clear, easy to
read and had a literacy level congruent with that of a 12 year old child.
4.1 Phase One- Expert panel of critical care nurses 4.1.1 Questionnaire The panel of ten nurses who constituted the critical care professional body’s
Educational Advisory Panel were sent a questionnaire with ten closed and one
open-ended question. The questions related to their perception of family
members’ transfer needs.

116
Nine out of the ten questionnaires were returned completed (90% response rate)
with the tenth not returned. On a five-point scale, four participants reported that
family members were “hardly ever” included in transfer plans as they were being
made (Table 4.1). Five participants answered that “sometimes” family members
were included in planning the transfer from ICU. When asked to reflect on their
own ICU, they were asked how they would rate the current transfer procedure.
Five indicated the process was “not very good”, one was “not sure” and three
indicated it was “quite good”. All respondents rated their hospital’s attitude to
family members as “quite good” (Table 4.1).
When asked on the importance of family members to critically ill patients’
recovery, all participants thought family members were either “important” or
“very important” to the recovery process. When asked if family members
physically accompany the patient at the time of transfer, seven of the sample
indicated that family members “sometimes” accompany the patient upon transfer
to general wards. One respondent indicated that family members “always”
accompany patients and another that family members “seldom” accompany the
patient during transfer (Table 4.1).
When asked about their perception of family members’ needs in relation to
general wards the following responses were recorded. Six participants thought it
was “important” or “very important” for family members to know the number of
patients per room and all thought it was “important” or “very important” for
family members to have access to telephones in the general wards. Eight of the
sample thought it was “important” or “very important” for family members to

117
know the nurse: patient ratio in the ward with one respondent “not sure”. Seven
participants indicated that knowing the expectations of the nurses in the general
ward was “important” or “very important”. Two respondents indicated that they
were “not sure” in relation to this question (Table 4.1).
When asked if family members were made aware that a different health care team
would be caring for the patient in the general ward, three indicated that family
members “always” knew, whereas three others said that “sometimes” they knew.
The last three of the sample indicated that family members “seldom” knew a new
team would be found in the general ward (Table 4.1).

118
Table 4.1: Expert panel questionnaire responses.
Question Always Sometimes Not sure Hardly ever Never Families included in transfer plans
0 5 0 4 0
Do families go with patient at transfer
1 7 0 1 0
Families know about new health care team
3 3 0 3 0
Question Excellent Quite good Not sure Not very
good Poor
Rate current transfer
0 3 1 5 0
Hospital attitude to families
0 9 0 0 0
Question Not
important Slightly important
Not sure Important Very important
Families to patients’ recovery
0 0 0 3 6
Number of patients per room
0 2 1 3 3
Phone access in ward
0 0 0 5 4
Nurse: patient ratio
0 0 1 6 2
Ward expectations
0 0 2 3 4
Responses to the open-ended question asking what information they considered
important for family members before transfer were transcribed in full. Categories
were developed in response to common features of participants’ comments. This
open coding method is suggested to be an effective way to group, or categorises
qualitative data (Rice & Ezzy, 1999) and further coding methods into sub
categories and core categories was not necessary as the data readily grouped into
five main categories based upon clearly evolving concepts (Flick, 2002).

119
The categories included:
• transfer plans,
• ward orientation,
• staffing orientation,
• ward expectations, and
• reassurance and support.
4.1.1.1 Transfer Plans Responses in this area included comments such as family members needing to
know why the patient was leaving ICU. Reasons for delays in transfer,
progression of health status, potential that the patient may be transferred earlier
and the need for a predicted LOS were also considered important information
needs of the family members in the area of “transfer plans”.
4.1.1.2 Ward Orientation In this category participants thought family members should be told information
specific to the ward in the form of a ward orientation. The suggestions included
the ward location, type of ward (for example, respiratory or cardiac), ward layout,
ward telephone number, number of patients per room, visiting hours, limitation on
the ward (no flowers or only two visitors at a time) and differences in equipment.
4.1.1.3 Staff Orientation The expert panel members thought that family members should be orientated to
the staff in the general ward and hence the category of “staff orientation”.
Suggestions included that family members should be told that the ICU nurses did
not care for patients in the general ward and that a new medical team (including
nursing staff) take over the care. The name of the new consultant and the charge

120
nurse was thought to be information family members needed along with the
expertise of the nurses in the new ward should be reinforced. If a liaison nurse
existed within the hospital then information regrading this role could be explained.
The fact that members of the expert panel all worked or were affiliated with
different ICUs and wrote according to procedures within their unit was evident
throughout. For example, one respondent wrote that “the ICU nurse will undertake
a follow-up visit (for patients who have had an extended stay in ICU, greater than
five days generally) to make sure [the] patient and family [are] OK”.
4.1.1.4 Ward Expectations The fourth category of responses centred upon what to expect in the general ward.
Participants suggested that information regarding different expectations of patients
and family members by general ward staff were important information for family
members before transfer. This information included the need for patients to
understand that, where possible, they would be expected to assume a greater
degree of independence. The plan of care in the general ward may be quite
different to that experienced in ICU and therefore the family needed this
explained.
4.1.1.5 Reassurance and Support The last category was the need for the family to experience “reassurance and
support” around the plan of transfer from ICU. The expert panel suggested the
various physical facilities available to families should be outlined such as
bathroom and kitchen facilities, chapel location, close affordable accommodation
and the need to care for oneself. Assurance that following transfer there was often
a period of readjustment required on the part of the patient and the family who

121
may sometimes feel abandoned which could cause anxiety. Information as to
whom the family approached should they have any concerns was thought to be
important. A participant thought it was important to reassure that there was
“someone close-by and that [the] ICU nurse will provide explanation and hand-
over to staff”. Another participant considered that a “patient with any degree of
disability in terms of communication, for example, a tracheostomy, then their
anxiety is increased.” The participant did not, however, write as to how to deal
with this situation.
4.1.1.6 Summary of expert panel questionnaire In summary, the expert panel of nurses reported considerable amounts of
information were required by family members before transfer from ICU. This
information was grouped into five categories including an understanding of
transfer plans, ward orientation, staffing orientation, ward expectations, and
reassurance and support. There was a degree of congruence amongst participants
who considered family members play an important role in critically ill patients’
recovery. Although all of the sample thought their hospital had a “quite good”
attitude to family members, only five indicated that “sometimes” family members
were involved in transfer plans with the remaining four saying that family
members were “hardly ever” involved. The expert panel considered information
sharing to be important in preparation for transfer and this was reflected in their
responses regarding how they rated their current transfer procedure with five
suggesting their procedure was “not very good”.
122
4.1.2 Expert panel’s focus group discussion The focus discussion group meeting involved seven members of the expert panel.
The remaining three were unable to attend. A summary of the closed question
results and verbatim recording from the open-ended question on the questionnaire
were distributed to the focus group members. Discussion ensued and the group
collectively agreed with the five categories from the open-ended question as
nominated by the researcher. Each of theses categories was discussed and items
within were ranked with the most important information listed first and so on. It
was at this time that certain information was deleted as members considered it was
too specific to be included. For example, the time of shift change-over was
considered too difficult for inclusion in a generic brochure for all general ward
areas. The participants also commented that a number of comments could be
grouped together under the one topic. For example, one written response was that
the family member needed information relating to “discharge planning” and
another wrote that family should be told “why they leaving ICU, reason for
transfer, such as progression of health status, cessation of pharmacological therapy
etc.” Also the comment relating to LOS could be incorporated under the same
topic of discharge planning.
The participants considered information about the number of other patients
sharing the room may well be additional unnecessary information. They
cautioned against writing specific information on the brochure which may have
legal ramifications. One example was where initially participants considered
having in the brochure the nurse:patient ratio to expect in the general ward.
During discussion, however, this was considered unwise as if the brochure stated

123
the nurse: patient ratio will be 1: 6 and the actual ratio is 1: 8 then issues may
ensue. The suggestion was a phrase such as “your nurse will be caring for a group
of patients”. Another suggestion was that phrases such as there will be the
“expectation of patient regaining more independence” could be replaced by a less
specific term such as “issues relating to care” will be discussed. This then
incorporated those patients who would not become more independent and allowed
the nurse to individualise the information given.
Within the category of “reassurance and support”, the group suggested adding the
general ward social worker’s contact details. They reasoned the family may not
have needed the social worker while in ICU but may require their services in the
general ward when the illness outcome is perhaps clearer.
Participants’ overall comments about the brochure reinforced that the information
should be kept simple. They considered it important to individualise the brochure
with a place for the family member’s name. They cautioned if the brochure
contained sensitive information, it needed to be managed responsibly. Patient
confidentiality was an issue highlighted and the nurse therefore needed to
ascertain the patient’s consent for discussing with family members, issues relating
to the patient’s illness and treatments. Participants also suggested a space at the
back for additional information while in the ward, such as out-patients’
appointments.
The recorded notes from the focus group discussion were later forwarded to those
in attendance at the focus group discussion for their review of the document. They

124
were requested to highlight to the researcher the need for alterations or
information which was incorrect. The researcher did not receive feedback
suggesting changes were necessary.
There were three participants not present at the focus group discussion. Two had
completed the questionnaire and a meeting was organised to gather additional data
from them. One participant attended this meeting with the second unable to attend
as she had resigned from the hospital. The third member was not included as they
had indicated a preference to not be involved by non-return of the questionnaire.
The meeting therefore occurred with one participant who was the ICU educator at
the research site and was therefore able to provide vital information specific to the
unit where data collection occurred. She gave information about the procedure for
transferring patients from ICU and how this may impact upon family members.
For example, she was able to tell the researcher the hospital had a policy outlining
all transfers from ICU had preferential treatment and were moved to ward areas
specialising in the patient’s condition. A less ill patient may well need to be
moved from the general ward to allow them to accept the ICU patient. She
commented that a different physiotherapist, speech therapist and occupational
therapist would be caring for the patient after transfer and that this needed to be
highlighted along with the changes in the nursing and medical staff. The
participant suggested that the first point of contact for relatives in the general ward
would be the NPC should they have any issues. Finally the participant
commented that for some patients the ICU intensivist would provide follow-up
care but that this was not universal.

125
4.1.2.1 Summary of expert panel focus group discussion To summarise, the expert panel of critical care nurses discussed and prioritised
information to be contained in the information brochure which would act as a
prompt for discussion by the nurse. The site ICU educator gave specific
information relevant to the data collection site to ensure the brochure was
pertinent to the study site. Having completed the data collection from the expert
panel, family members following transfer from ICU were surveyed and the results
will now be presented.
4.2 Phase One: Family members’ data collection Family members visiting patients following transfer from ICU formed the sample
for this aspect of Phase One. The sample size was 20. The only demographic
data collected on these participants were their relationship to the patient. The
major relationship groups were wives or husbands of the patient and the remaining
sample represented other expected groups as indicated in Table 4.2.
Table 4.2: Phase One: family members’ relationship to patient.
Relationship n = 20 Wife 7 Husband 6 Sister 1 Father 1 Mother 1 Grandmother 1 Daughter 2 Friend 1
The 20 family members completed a 12 question survey with 11 closed and one
open-ended question. The first nine questions related to how important it was for

126
them to know certain things before patient transfer from ICU. For example, the
first question asked “How important is it for the family to know the ward name
and its location before transfer?” As seen in Table 4.3 nine participants (45%)
considered it was “very important” and three (15%) thought it was “important”.
They were asked about the importance of knowing the ward phone number, the
nurse: patient ratio, the visiting hours, the name of the doctor, and the number of
patients per room. For all questions except information about the number of
patients per room, the majority of participants thought the information to be
“important” or “very important”. Seven participants (35%), however, thought it
was “not important” knowing the number of patients each nurse cared for in the
general ward whereas 12 (60%) considered it was “important” or “very important”
(Table 4.3). Questions relating to the importance of knowing information
regarding patient transfer plans, the outcome of the illness and proposed
treatments were also asked. Most family members thought these were “important”
or “very important” pieces of information (Table 4.3).
Participants were asked “If in their experience families were considered important
in that hospital?” Fifteen (75%) indicated that they were either “important” or
“very important”. According to 18 participants (90%), staff use everyday
language when speaking about patients either “all the time” or “sometimes”. The
final question asked participants what information they considered important prior
to the patient leaving ICU. This open-ended question elicited only one written
comment of “update and general overview.” Others commented verbally
indicating that everything had been covered in the survey.

127
Table 4.3: Factors important to family members in Phase One.
Factor Not important
n (%)
Slightly important
n (%)
Not sure
n (%)
Important
n (%)
Very important
n (%) Outcome of illness 1 (5%) 2 (10%) 1 (5%) 4 (20%) 12 (60%)
Dr’s name
2 (10%) 0 1 (5%) 7 (35%) 10 (50%)
Proposed treatments
2 (10%) 3 (15%) 0 5 (25%) 10 (50%)
Name and location of ward
4 (20%) 3 (15%) 1 (5%) 3 (15%) 9 (45%)
Ward phone number
2 (10%) 2 (10%) 1 (5%) 6 (30%) 9 (45%)
Hospital importance of families
1 (5%) 0 4 (20%) 6 (30%) 9 (45%)
Included in planning transfer being made
4 (20%) 2 (10%) 0 9 (45%) 5 (25%)
Visiting hours
1 (5%) 2 (10%) 0 12 (60%) 5 (25%)
Nurse:patient ratio
7 (35%) 1 (5%) 0 10 (50%) 2 (10%)
Patients per room
12 (60%) 2 (10%) 0 6 (30%) 0
4.2.1 Summary of family member data In summary, the family members visiting patients following transfer from ICU
thought there was a lot of information which was important for them to receive
before moving from ICU. This included information on geographical aspects of
the ward, contact details for the ward and the names of the general ward staff
caring for their relative. They did not seem to need to know the number of
patients sharing the room with their relative. This is congruent with comments by
the expert panel of critical care nurses. Almost universally the participants thought
information about prognosis and treatment were important facts they wanted to
know before leaving ICU. The hospital rated well as participants thought the
hospital considered families to be important. Similarly, a high rating occurred
regarding the level of language used in communicating about patients’ conditions.

128
The results of the data collection from the participants of family members and the
expert panel of critical care nurses formed the basis for the development of a draft
brochure containing information about transfer from ICU. The process of the
development and publication of the brochure will now be reported as Phase Two
of the study.
4.3 Phase Two 4.3.1 Teachers An A4 piece of paper with two equal columns containing general introductory
and directed prompt questions, or statements, was developed by the researcher
from Phase One data. This was sent to the three grade eight teachers with a
feedback sheet for comment. There were six questions on the feedback sheet. The
first asked if in their opinion the brochure was clearly written for an eighth grade
audience. All responded that it was, however, many suggestions to alter sentence
construction and syntax were given. They thought the brochure was not too long
or too short. They responded that the language level was not too complex for
eighth grade literacy level but once again, suggestions were made in word choice.
They were asked for additional comments and all made notations directly on the
brochure.
The researcher had used the word “orientation” and one participant suggested
changing this to “information” in view of the level of literacy desired. In some
instances the suggestion was one of rewording to improve the flow, for example:
the brochure read, “Once your relative moves to the ward, staff caring for him/her
will be different.” The suggested change was “The staff in the general ward may
be new to you. The following information will be of use to you”. All suggestions

129
improved the clarity and flow of the wording and these changes were incorporated
into the next draft of the brochure which was shown to senior nursing personnel
for comment.
4.3.2 Senior Nursing Personnel The four Assistant Directors of Nursing (ADON) each made suggestions. The
ADONs’ ideas were incorporated into the next draft of the brochure. Following
this extensive process of consultation, the final brochure (draft six) was
commercially produced with assistance from graphic designers.
4.4 Summary of intervention design This chapter has presented the results of both Phase One and Phase Two data
collection. Phase One data were obtained from family members of patients
discharged from ICU and from a panel of expert critical care nurses. The expert
panel considered that family members should be given information regarding the
intended plans for transfer together with information about the new ward and its
different staff. The expert panel also considered information on the different
expectations in the general ward was important for family members to have
explained to them. Finally, they considered information relating to the support
systems available to family members needed to be highlighted with contact details
written down.
The family members surveyed wanted information on the geographical location of
the ward, contact details of the general ward and the names of the doctors caring
for the patient. Details about the future treatment and prognosis were very
important to them.

130
The data from Phase One informed the content for the development of the
educational brochure which comprised Phase Two of the study. Three teachers
provided feedback to ensure the language and level of literacy were congruent
with an eighth grade student level. Senior hospital personnel reviewed the draft
brochures before final production of the brochure. The following chapter
presents the results from Phase Three and Phase Four of the study with regard to
the sample including family member and patient factors.

131
CHAPTER 5: DESCRIPTION OF THE SAMPLE
5.0 Introduction The previous chapter presented results from the data collected within Phase One
and Phase Two of the study. Results from Phase Three and Phase Four of the
study with regard to the sample including family member and patient factors will
now be reported. A description is given of participants and comparison made
between the control and intervention groups within Phase Three of the study.
The sample size in the control group was 91 with 80 participants completing the
two questionnaires. This represents a retention rate for the control group of 88%.
The intervention group recruitment sample size was 86 participants with 82
remaining in the study (retention rate 95%). Participants did not complete the
study for one of two reasons. The first reason was that patients unexpectedly
deteriorated and hence was not transferred as planned (n = 5), therefore, the
participant did not meet the selection criteria for the post-transfer survey. The
second reason for non-completion was that the researcher was unable to time a
meeting with the family member in the ward to complete the questionnaire (n =
10). Although meeting times were always arranged, situations change for family
members and planned visit times consequently altered.
In addition to family members data, patient data were also collected. These are
presented following the family members’ demographic details.

132
5.1 Family Member Demographics
5.1.1 Age of family members The mean age of the participants (family members) in the control group was 49.91
years (range of 25 to 79 years, SD = 12.03) and in the intervention group the mean
age was 48.56 years (range of 18 to 80 years, SD = 14.11). Table 5.1 outlines the
age of participants in the control and intervention sample in four age categories.
There was a slight increase in the number of family members in the 36 – 45 and a
slight decrease in the number of family members in the less than 36 year age
groups for the control sample. Overall there was a general consistency between
the mean age of the participants in the control and intervention sample population.
Statistical comparison of the two groups using a two-sample t-test analysis was
performed having first examined the following assumptions underlying the test:
1. Data should be interval or ratio level of measurement,
2. The scores should be randomly sampled from the population of interest, and
3. Scores should be normally distributed (Polit & Hungler, 1996).
The scores were normally distributed and analysis showed the control and
intervention groups did not significantly differ in regard to their age (t = .655, df =
160, p = .51.
Table 5.1: Age of family members.
Age group in years Control (n = 80) % (n )
Intervention (n = 82) % (n )
< 36 13.8% (11) 19.5% (16) 36 – 45 25.0% (20) 19.5% (16) 46 – 60 43.7% (35) 45.1% (37) > 60 17.5% (14) 15.9% (13)

133
5.1.2 Gender of family members The control and intervention groups had similar numbers and percentages of both
male and female (Table 5.2). A Chi square analysis was performed as the
variables were categorical in nature. The assumptions underlying a Chi square
analysis include:
1. Sample is randomly sampled from the population,
2. Observations are from different subjects and no subject is counted twice, and
3. Size of expected frequencies is not less than five (Croakes & Steed, 2001).
With all assumptions examined, the test showed that the proportion of each gender
for the two groups was not significantly different (χ2 = .199, df = 1, p = .656).
Table 5.2: Gender of family members.
Gender Control % (n)
Intervention % (n)
Males 31.3% (25) 28.0% (23) Females 68.8% (55) 72.0% (59)
5.1.3 Educational level of family members The years of education of the participants in the control and intervention sample,
were similar (Table 5.3). Two sample t-tests were performed having met the
assumptions outlined previously. The two groups did not significantly differ
(t = -.069, df = 160, p = .945).
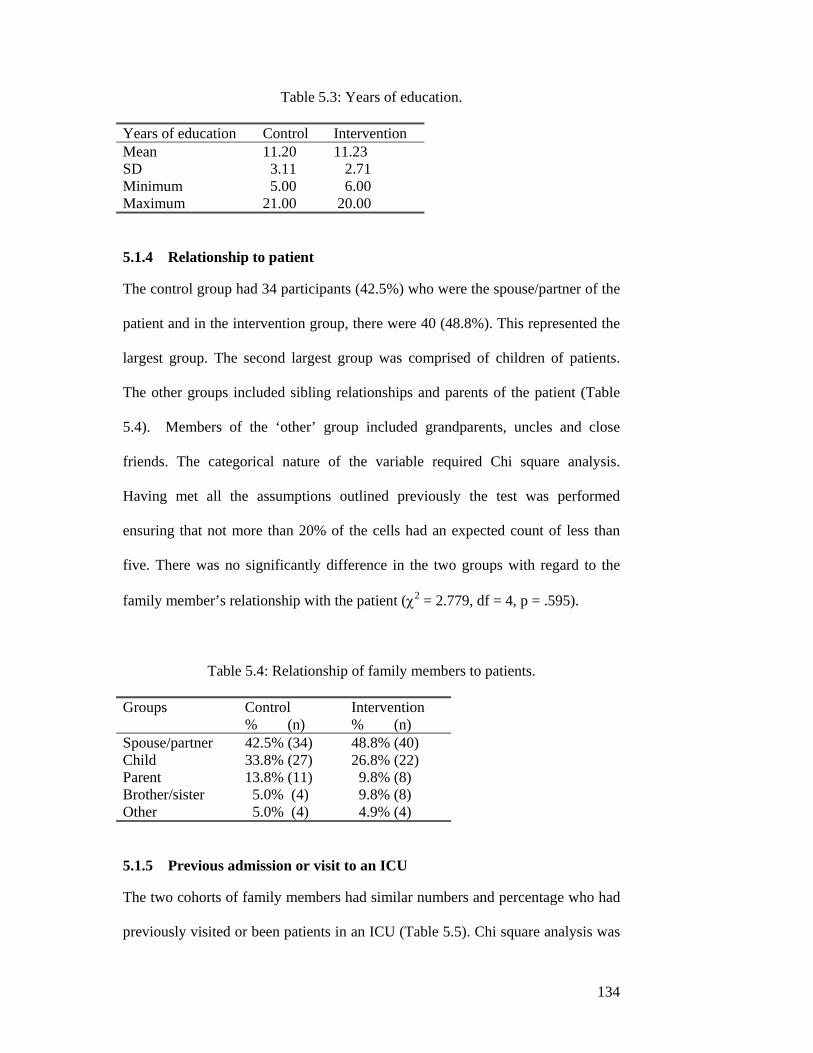
134
Table 5.3: Years of education.
Years of education Control Intervention Mean 11.20 11.23 SD 3.11 2.71 Minimum 5.00 6.00 Maximum 21.00 20.00
5.1.4 Relationship to patient The control group had 34 participants (42.5%) who were the spouse/partner of the
patient and in the intervention group, there were 40 (48.8%). This represented the
largest group. The second largest group was comprised of children of patients.
The other groups included sibling relationships and parents of the patient (Table
5.4). Members of the ‘other’ group included grandparents, uncles and close
friends. The categorical nature of the variable required Chi square analysis.
Having met all the assumptions outlined previously the test was performed
ensuring that not more than 20% of the cells had an expected count of less than
five. There was no significantly difference in the two groups with regard to the
family member’s relationship with the patient (χ2 = 2.779, df = 4, p = .595).
Table 5.4: Relationship of family members to patients.
Groups Control % (n)
Intervention % (n)
Spouse/partner 42.5% (34) 48.8% (40) Child 33.8% (27) 26.8% (22) Parent 13.8% (11) 9.8% (8) Brother/sister 5.0% (4) 9.8% (8) Other 5.0% (4) 4.9% (4)
5.1.5 Previous admission or visit to an ICU The two cohorts of family members had similar numbers and percentage who had
previously visited or been patients in an ICU (Table 5.5). Chi square analysis was

135
used for this categorical variable having first examined and met the underlying
assumptions. There was no significant difference in the two samples (χ2 = .12,
df = 1, p = .729).
Table 5.5: Family members’ ICU experience.
ICU experience Control % (n)
Intervention % (n)
Previous ICU experience 60.0% (48) 57.3% (47) No previous ICU experience 40.0% (32) 42.7% (35)
5.1.6 Nationality of family members Both the control and intervention sample had similar numbers for the five
categories of nationality as outlined in Table 5.6. An overwhelming percentage of
participants from both the control and intervention sample were Australian. Few
participants in both samples were in the remaining groups as outlined in Table 5.6.
The nationalities which featured in the ‘other’ group included, amongst others,
participants from New Zealand, Tonga and India. When statistical tests were run,
the underlying assumptions were broken due to the small or nonexistent numbers
in some categories, however, examination of the table clearly shows there is no
difference in the two groups in the area of nationality.
Table 5.6: Nationality of family members.
Nationality Control % (n)
Intervention % (n)
Australian 83.9% (67) 81.7% (67) Indigenous Australian 2.5% (2) 1.2 % (1) European 2.5% (2) 3.7% (3) Asian 0 1.2% (1) Other 11.3% (9) 12.2% (10)

136
In summary, there was a high level of congruency for all variables studied
between the control and intervention groups in regard to family member
characteristics.
5.2 Patient Demographics
5.2.1 Age of patients
The mean age of patients in the control group (n = 80) was 58.8 years (range of 17
to 86 years, SD = 17.38) whereas the intervention group (n = 82) had a mean age
of 56.27 (range of 15 to 92 years, SD =16.14). A two-sample t-test was performed
having examined and met the underlying assumptions. Results indicated the
groups were not significantly different (t = .905, df = 159, p = .37).
The same age groups were used for comparison of the control and intervention
groups as performed with family members. Predictably, in both groups, the vast
majority of patients were over 60 years of age. The control group had smaller
numbers in the 36 – 45, and 46 - 60 year age groups and larger numbers in the
greater than 60 year age group. Under 36 years of age were very similar in both
groups (Table 5.7).
Table 5.7: Age of patients.
Age group in years Control % (n)
Intervention % (n)
<36 12.5% (10) 12.3% (10) 36 – 45 7.5% (6) 14.9% (12) 46 – 60 20.0% (16) 25.9% (21) >60 60.0% (42) 46.9% (39)

137
5.2.2 Gender of patients Both the control and intervention set of patients were predominantly male with a
higher percent of males in the control group (Table 5.8). A chi square analysis was
performed after checking the underlying assumptions for this categorical data.
Results show there was no significant difference between the two groups (χ2 =
.586, df = 1, p = .444).
Table 5.8: Gender of patients.
Gender of patient Control % (n )
Intervention % (n)
Male 73.8% (59) 68.3% (56) Female 26.3% (21) 31.7% (26)
5.2.3 Expected or unexpected admission to ICU Some patients admitted to ICU have been told in advance that they should expect
to be nursed in this area. Following major surgery is one such instance where
patients and family members are told beforehand that a period of time will be
spent in ICU following the operation. This is either as a prophylactic measure or
for specific treatment only available in ICU. Other admissions, however, are not
premeditated. Trauma following a motor vehicle accident is an example of an
unexpected admission.
There were slightly more expected admissions in the control sample with 56
(70%) patients anticipating their admission to ICU (Table 5.9). Chi square
analysis was performed on this categorical data and statistically these groups were
not significantly different (χ2 = .79, df = 1, p = .374).

138
Table 5.9: Patients’ admission type.
Admission to ICU Control % (n)
Intervention % (n)
Expected admission 70.0% (56) 63.4% (52) Unexpected admission 30.0% (24) 36.6% (30)
5.2.4 Degree of illness of patients The APACHE III scores were calculated from clinical data entered for each
patient at midnight and on discharge from ICU by the bed-side nurse. In some
cases the data for APACHE III scores were not completed by the nurses and
consequently there were missing data for both the control and intervention groups.
The APACHE III scores measured the degree of illness while in ICU. The mean
and standard deviation for the intervention group were less, thus indicating that
this group was less ill than the control group participants (Table 5.10). The
distribution indicated both samples were skewed in a positive direction to a lower
APACHE III score. As the underlying assumptions for the two sample t-test were
not met, the non-parametric Mann-Whitney U test was examined in regards to its
underlying assumptions. These assumptions include:
1. Random samples,
2. Similar shape and variability across distributions, and
3. Independence of the two sample groups (Polit & Hungler, 1996).
Having met these assumptions, the Mann-Whitney U test was performed and
revealed that the control group of patients was significantly sicker than the
intervention group (Z = -2.054, p = .040) when the APACHE III scores were
compared.

139
Table 5.10: Patients’ APACHE III scores.
APACHE III score Control (n = 72) Intervention (n = 75) Minimum 20.00 21.00 Maximum 143.00 116.00 Median 55.00 47.00
5.2.5 Reason for admission to ICU
The researcher documented the basis for each patient’s admission to ICU. Cardiac
surgery was the greatest reason for both groups’ admission to the ICU. Post-
operative care following Abdominal Aortic Aneurysm (AAA) repair constituted
the second most common reason for admission and the remaining patients were
divided into admission diagnoses as outlined in Table 5.11. Multi-trauma cases
numbered 6 in the control group whereas in the intervention group there was 1.
This may have accounted for some of the differences in the APACHE III scores
for the control and intervention groups. Other patients were admitted with
diagnoses for which there were either one or two representatives. To summarise,
medical and nursing care following surgery was the predominant reason for
admission to ICU for both groups. Cardiac surgery clearly formed the largest sub-
group for both the control and intervention groups.
Table 5.11: Reason for admission to ICU.
Reason for admission Control % (n)
Intervention % (n)
Cardiac surgery 40.0% (32) 32.9% (27) AAA 10.0% (8) 11.0% (9) Multi-trauma 7.5% (6) 1.2% (1) Head injury 3.8% (3) 7.3% (6) Pancreatic cancer 3.8% (3) 3.7% (3) AFBG 3.8% (3) 4.9% (4) Cerebral tumour 1.3% (1) 3.7% (3) Liver transplant 0 3.7% (3)

140
5.2.6 Length of patient stay in ICU During the data collection period the LOS of patients ranged from .42 days to the
longest LOS of 38 days. The mean LOS in ICU for control group participants was
very similar to the intervention group sample (Table 5.12). The distribution for
LOS in both samples was positively skewed to a shorter LOS. As values were not
normally distributed, the non-parametric Mann-Whitney U test was performed
having assessed underlying assumptions outlined above. Results indicated there
was no significant difference between the control and intervention groups’ LOS
(Z = -.982, p = .326).
Table 5.12: Length of patient stay in days.
LOS Control Intervention Minimum .53 .42 Maximum 38.00 34.79 Median .97 .96
5.3 Summary of sample To summarise, the control and intervention groups were significantly different
when the degree of illness was considered. Statistical analyses of all other patient
and family member factors showed there was no significant difference between
the control and intervention groups. That is, the control and intervention groups
were not significantly different when age, gender, relationship to patient, previous
admission to ICU and nationality of the family members were compared.
Similarly, the age of the patient, gender, admission type and LOS for the control
and intervention groups were not statistically different.

141
In conclusion, this chapter presented the characteristics of the study with regard to
the sample of family members and patients. Participants have been described and
comparisons made between the control and intervention groups within Phase
Three of the study. The following chapter will present findings to the five research
questions.

142
CHAPTER 6: RESULTS
6.0 Introduction The previous chapter presents the characteristics of Phase Three participants.
Family members and patients were described and comparisons made between the
control and intervention groups. The analyses of the previous chapter established
that the control and intervention were not significantly different with the
exception of the APACHE III scores. This chapter presents further analysis of the
data based upon the aims of the research and the five research questions
sequentially.
6.1 Question 1- Level of Uncertainty What was the level of ‘uncertainty in illness’ in family members before transfer
from ICU as measured by Mishel’s PPUS-FM Scale?
The control and intervention samples’ mean level of uncertainty before transfer
were normally distributed with the values recorded in Table 6.1. The first analysis
performed was an independent sample t-test to analyse the difference between the
two groups’ means. The Levene’s test indicated that the samples did not have
equal variances (p = .020) and therefore the non-parametric equivalent test, the
Mann-Whitney U test, was performed. This analysis showed that statistically
there was no significant difference between the control and intervention groups’
level of ‘uncertainty in illness’ before transfer ( Z = -.411, p = .681).

143
Table 6.1: PPUS-FM before transfer. PPUS-FM before transfer Control (n = 80) Intervention (n = 82) Mean 77.22 78.93 SD 15.31 11.51 Range 36-107 44-107
That is, the control and intervention groups’ ‘uncertainty in illness’ scores before
transfer were not significantly different. The actual levels of ‘uncertainty in
illness’ for the study will be compared with other studies’ findings within Chapter
7, the Discussion Chapter. The next research question, Question 2 has two parts
and will now be reported.
6.2 Question 2 - Uncertainty and anxiety 6.2.1 Question 2.1 Was there a relationship between family members’ ‘uncertainty in illness’ as
measured by PPUS-FM (Mishel,1997) and anxiety levels as measured by STAI-
state (Spielberger et al., 1983)?
‘Uncertainty in illness’ and state anxiety scores were calculated for both the
control and intervention groups. As outlined in the results of Question One, the
level of ‘uncertainty in illness’ was not significantly different between groups
therefore it was possible to combine the two groups’ data for further analysis. To
determine if this was also possible with the STAI-state scores, the mean values of
the control and intervention group’s STAI-state scores were compared. The mean
and standard deviations for the control and intervention groups are presented in
Table 6.2.

144
Table 6.2: State anxiety before transfer.
STAI – state Control (n = 80) Intervention (n = 82) Means 41.24 41.62 SD 13.21 13.42 Range 20-67 20-80
As all assumptions were met and the variances were found to be equal, an
independent t-test was performed to test the difference between the control and
intervention groups in relation to the STAI - state scores. There was no
significant difference between the two groups (t = -.182, df = 160, p = .856). This
permitted subsequent analyses on the STAI- state scores to be performed using
combined data from both groups as was the case for ‘uncertainty in illness’.
The relationship between PPUS-FM and the STAI-state scores before transfer was
examined using correlation analysis. Pearson’s correlation coefficient, r, measures
the strength of a linear relationship between the two variables on a scale of –1 to
+1 when both variables are recorded on an interval or ratio scale. Assumptions
underlying the use of Pearson product-moment correlation include:
1. Data for variables obtained from same participant,
2. Data should be interval or ratio in nature,
3. Scores should be normally distributed,
4. The relationship between the two variables should be linear, and
5. Homoscedasticity – variability in scores for one variable is roughly the same
at all values of the other variable (Polit & Hungler, 1999).
The underlying assumptions were examined and found to be met. The scatterplot
indicated that there was a linear relationship between PPUS-FM and STAI-state
scores with the scores clustered around the regression line.

145
Pearson product-moment correlation analysis indicated that the state anxiety
scores before transfer were significantly related to the levels of PPUS-FM before
transfer (r = .493, R2 = .243, F = 50.994, p < .000). The state anxiety scores
accounted for 24.3% of the variance of ‘uncertainty in illness’ scores (Table 6.3).
As the r value is positive, the linear relationship is positive and therefore as PPUS-
FM scores increase, so do the STAI-state scores.
6.2.2 Question 2.2
Were patient and family member’ factors significantly related to PPUS-FM
scores?
To examine the relationship between demographic factors, patient variables and
PPUS-FM scores, a series of Pearson product-moment correlations were
performed using PPUS-FM scores before transfer and factors with continuous data
- age, APACHE III, education level, LOS, and social support. Assumptions as
outlined above were examined and found to be met with all factors. Results
indicated that all of these factors were only weakly and not significantly related to
the PPUS-FM scores (Table 6.3)
Table 6.3: Correlational analysis of PPUS-FM before transfer and demographic factors.
Factor R R2 F P
STAI - state score .493 .243 50.994 .000** Family members’ age .072 .005 .824 .365 Education .012 .000 .022 .883 APACHE III .036 .001 .188 .666 LOS .103 .011 1.716 .129 Social Support Score .128 .016 2.648 .106
(p<.001)**

146
Nationality of the family member was not analysed as previously discussed. One
way analysis of variance (ANOVA) was used for the categorical data – gender,
relationship with patient, previous ICU experience and unexpected or expected
nature of admission. This test is used for a dependent variable (for example,
PPUS-FM) measured on an interval or ratio scale and when the independent
variable is a nominal or categorical scale (for example, gender) (Polit, 1996).
Assumptions include:
1. Populations from which samples taken are normally distributed,
2. Samples independent and randomly chosen, and
3. Samples drawn from populations having equal variances (Martin & Pierce,
1994).
Levene’s test for equality of variances was performed in each case and checked to
be <.05 in order to meet assumption three before continuing with the analysis.
Results indicated that being male or female and previous ICU experience was not
significantly related to the PPUS-FM scores (Table 6.5). The relationship of the
family member to the patient was significantly related (F = 2.944 [4,156], p =
.022, η2 = .070). This infers from the partial eta squared, that the relationship with
the patient accounted for 7% of the variance of ‘uncertainty in illness’. Post hoc
analysis of mean uncertainty scores for the different relationship groups (Table
6.4) was performed to analyse group interaction using a Tukey test. This
compared all possible pairs of groups. Results indicated that the only significant
difference was that the “parent” group of family members reported higher mean
scores than did the “child” group. The mean difference was 11.38 which was
significant (p = .015) (Table 6.4).
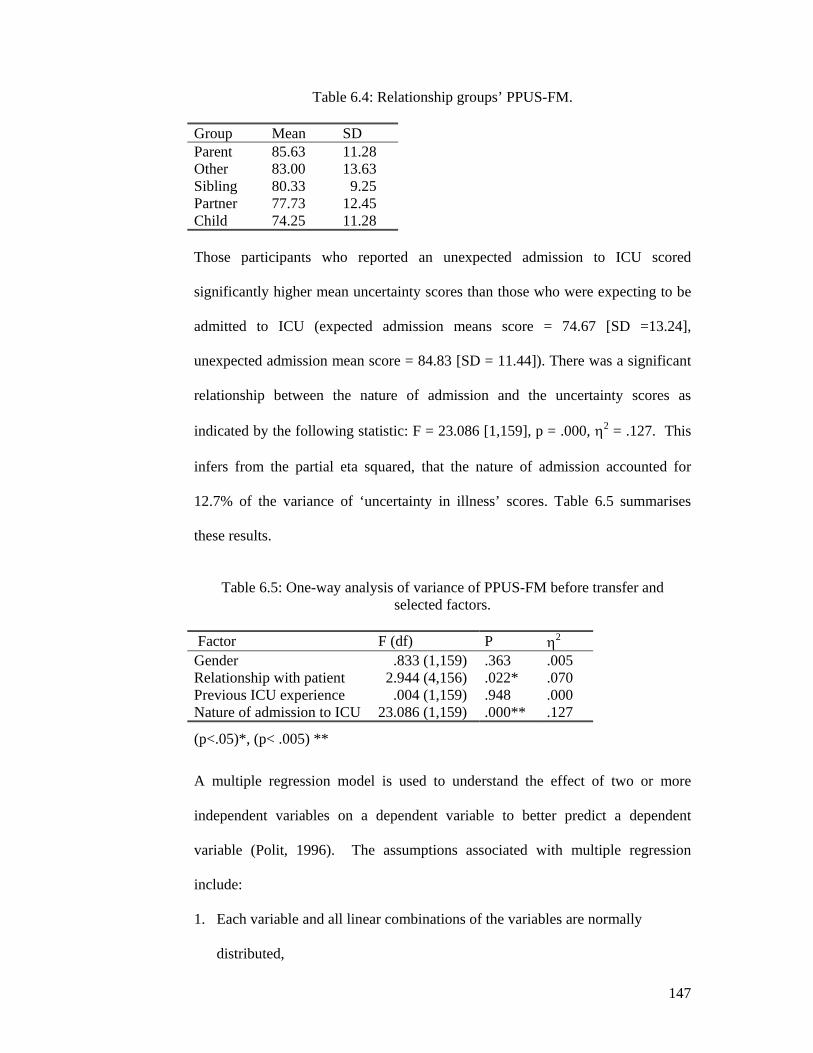
147
Table 6.4: Relationship groups’ PPUS-FM.
Group Mean SD Parent 85.63 11.28 Other 83.00 13.63 Sibling 80.33 9.25 Partner 77.73 12.45 Child 74.25 11.28 Those participants who reported an unexpected admission to ICU scored
significantly higher mean uncertainty scores than those who were expecting to be
admitted to ICU (expected admission means score = 74.67 [SD =13.24],
unexpected admission mean score = 84.83 [SD = 11.44]). There was a significant
relationship between the nature of admission and the uncertainty scores as
indicated by the following statistic: F = 23.086 [1,159], p = .000, η2 = .127. This
infers from the partial eta squared, that the nature of admission accounted for
12.7% of the variance of ‘uncertainty in illness’ scores. Table 6.5 summarises
these results.
Table 6.5: One-way analysis of variance of PPUS-FM before transfer and
selected factors.
Factor F (df) P η2 Gender .833 (1,159) .363 .005 Relationship with patient 2.944 (4,156) .022* .070 Previous ICU experience .004 (1,159) .948 .000 Nature of admission to ICU 23.086 (1,159) .000** .127
(p<.05)*, (p< .005) **
A multiple regression model is used to understand the effect of two or more
independent variables on a dependent variable to better predict a dependent
variable (Polit, 1996). The assumptions associated with multiple regression
include:
1. Each variable and all linear combinations of the variables are normally
distributed,

148
2. Linearity is assumed between all pairs of variables, and
3. Homoscedasticity – that is, the variability in scores from one variable is
approximately the same at all values of another variable (Polit, 1996).
To assess underlying assumptions a scatterplot of residuals against predicted
values was performed and found to have no clear relationship thus complying with
assumption three above (Coakes & Steed, 2001).
Three variables (nature of admission, relationship with patient, and state anxiety
levels before transfer) were found to be significantly related to ‘uncertainty in
illness’ and these factors were analysed using a multiple regression model.
Categorical factors with more than two categories require dummy coding which
involves the creation of a series of dichotomous dummy variables that contrast
members in one category with all others (Polit, 1996). The new predictors were
then used in the multiple regression analysis. When controlling for the variables
of anxiety before transfer and nature of admission, none of the relationship
variables were significant (Table 6.6). The relationship variable accounted for
only .7% of the variance of uncertainty over and above the 32.3% accounted for
by anxiety before transfer and the unexpected nature of the admission. That is,
when the three variables (state anxiety before transfer, relationship with patient
and nature of admission) were analysed in a multivariate model they accounted for
33% of the ‘uncertainty in illness’ scores (F = 14.163, adjusted R2 = .330) .

149
Table 6.6: Multiple regression of PPUS-FM and selected factors.
Factor B St Error Beta (β) T P Relationship
• Spouse -2.83 4.13 -.105 -.684 .495 • Sibling .37 5.08 .007 .072 .943 • Child -6.02 4.24 -.204 -1.418 .158 • Parent -.92 4.82 -.022 -.191 .849
Expected/ Unexpected
8.57 1.87 .300 4.582 .000**
STAI .463 .067 .456 6.959 .000** (p<.005) **
In summary, the level of state anxiety significantly affected the ‘uncertainty in
illness’ levels and accounted for 24.3% of the PPUS-FM scores. When admission
was unexpected there was a significant relationship with higher ‘uncertainty in
illness’ scores accounting for 12.7% of the PPUS-FM values. The relationship of
the family member to the patient accounted for 7% of the PPUS-FM scores.
Collectively, the three factors accounted for 33% of the variance of PPUS-FM
scores.
No other variables were significantly related to the PPUS-FM in this sample. The
following section reports the relationship between state anxiety scores and patient
and family member’ factors.
6.2.3 Question 2.3
Were patient and family member’ factors significantly related to STAI – state
scores?
As in the previous section examining PPUS-FM, a series of Pearson product-
moment correlation were performed to determine relationships between STAI-
state scores and factors with continuous data - age, APACHE III, education level,

150
social support and LOS. Assumptions as outlined previously were examined and
found to be met with all factors.
One-way ANOVAs were used for the categorical data – gender, relationship with
patient, previous ICU experience and unexpected or expected nature of admission.
Assumptions previously listed were examined and met by all factors. As with the
PPUS-FM analysis, nationality of the family member was not analysed.
The family member’s age, years of education, patients’ APACHE III score, and
patients’ LOS were not significantly related to the family members’ STAI-state
scores as indicated by the p results >.05. Family members’ level of social support
as measured by the MOS SSS (Sherbourne & Stewart, 1991) was significantly
related to the STAI -state (r[1/160] = -.243, R2 = .059, F = 10.0005, p = .002).
The social support factor accounted for 5.9% of the variance of state anxiety
scores (Table 6.7). As there is a negative r value for the social support score it can
be said that as social support increases, the state anxiety scores decrease. This will
be discussed in the following chapter.
Table 6.7: Correlational analysis of state anxiety before transfer and
selected factors.
Factor R r2 F P
Family members’ age .148 .022 3.608 .059 Education .067 .004 .715 .399 APACHE III .127 .016 2.392 .124 Social Support Score -.243 .059 10.005 .002** LOS .005 .000 .004 .952
(p < .005)**

151
One-way ANOVA undertaken with the categorical data occurred following
assessment of underlying assumptions. Analyses indicated the gender of the
family member, relationship with the patient, previous ICU experience, nature of
the admission (unexpected or expected), were not significantly related to the state
anxiety scores (Table 6.8).
Table 6.8 One-way analysis of variance of state anxiety before transfer and
selected factors. Factor F (df) P η2 Gender .505 (1,160) .478 .003 Relationship with patient .740 (4,157) .566 .018 Previou s ICU experience .077 (1,160) .782 .000 Nature of admission to ICU 2.482 (1,160) .117 .015
One variable, the amount of social support, was significantly related to STAI –
state scores before transfer. The social support score accounted for 5.9% of
variance of STAI-state score. As reported earlier in Question 2.1, the other factor
which was significantly related to anxiety was ‘uncertainty in illness’ which
accounted for 24.3% of variance. No other variables were significantly related to
STAI-state scores.
6.2.4 Summary of Question 2 In this study, there was a significant relationship (p<.001) between family
members’ ‘uncertainty in illness’ and state anxiety levels. The second component
of the question examined selected demographic and patient related factors and
‘uncertainty in illness’ and state anxiety. The factors significantly related to
PPUS-FM included the nature of admission (unexpected or expected), the STAI-
state scores and the relationship of the family member to the patient. Collectively
these accounted for 33% of the variance of PPUS-FM scores. The factors

152
significantly related to the STAI – state scores were the level of social support
and ‘uncertainty in illness’ which collectively accounted for 30.2% of the variance
of STAI-state scores. Results of Question 3 will now be reported.
6.3 Question 3: Intervention’s effect on uncertainty and anxiety
Has the introduction of the intervention led to a reduction in the ‘uncertainty in
illness’ and state anxiety scores?
The initial analysis involved comparing the before transfer and after transfer
anxiety and uncertainty for both the control and intervention groups. A paired t-
test has been used as the control and intervention groups have been demonstrated
to come from the same population and difference between means with and without
the intervention can be attributed to the treatment effect (Coakes & Steed, 2001).
Before analysis occurred the underlying assumptions of the paired t-test were
examined and found to be met in all but assumption two which requires the
sample to be randomly sampled. The assumptions include those for all t-tests:
1. Data should be interval or ratio level of measurement,
2. Sampling from the population of interest should be random,
3. Scores should be normally distributed, and
4. There is normality of population difference scores. That is, the difference
between the scores for each participant should be normally distributed (Coakes &
Steed, 2001).
The state anxiety mean scores before and after transfer for the control and
intervention groups showed both groups had reduced scores following transfer.
The paired t-test analysis of the state anxiety scores indicated there was significant

153
reduction in the control (t [df = 79] = 3.60, p = .001) and intervention group (t [df
= 81] = 2.81, p = .006) scores after transfer from ICU (Table 6.9).
Table 6.9: State anxiety before and after transfer.
Group STAI before transfer
Mean SD STAI after transfer Mean SD
T (DF) P 2-tailed
Control 41.24 13.21 37.11 13.45 3.60 (79) .000** Intervention 41.62 13.42 37.72 13.92 2.81 (81) .006*
(p < .05)*, (p < .005)**.
The ‘uncertainty in illness’ mean scores before and after transfer for the control
and intervention groups also showed a reduction after transfer for both groups. A
paired t-test analysis of the PPUS-FM scores indicated there was significant
reduction in the intervention group scores (t [df = 80] = 2.21, p = .029) but not in
the control group (t [df = 79] = .80, p = .424) after transfer from ICU (Table
6.10).
Table 6.10: PPUS-FM before and after transfer.
Group PPUS-FM before transfer
Mean SD
PPUS-FM after transfer
Mean SD
T (DF) P 2-tailed
Control 77.22 15.31 76.24 17.64 .80 (79) .424 Intervention 78.93 11.51 76.38 15.99 2.21 (80) .029*
(p < .05)*
To summarise, these results indicated that both the control and intervention group
experienced a significant reduction in their levels of anxiety following patient
transfer from ICU to a general ward. In this sample, the reduction was greater in
the control group but both control and intervention groups’ lower levels were
significant at the p<.05 level. The level of ‘uncertainty in illness’ for the
intervention group reduced significantly at the level at the p<.05 level of
significance, however, the control group did not show a significant reduction.

154
Following the above analyses, additional tests were performed as random
assignment of sample was not possible in this study due to its quasi-experimental
design (Polit & Hungler, 1999). Although by independent t-test analysis the
control and intervention groups were shown to not be significantly different in
regard to state anxiety and ‘uncertainty in illness’, pre-test scores still could be
influential (Polit & Hungler, 1999). That is, pre-existing differences between the
two groups may have occurred and Analysis of Covariance (ANCOVA) permits
post-hoc statistical control of such extraneous variables (Polit & Hungler, 1999).
Two ANCOVAs were performed. These examined the differences between the
control and intervention groups’ post transfer ‘uncertainty in illness’ and state
anxiety by reducing systematic bias, as well as within-groups error, in the analysis
(Coakes & Steed, 2001). To determine whether the independent variable was
indeed having an effect, the influence of the covariate on the dependent variable
was statistically controlled during the analysis (Coakes & Steed, 2001). Pre
transfer scores were used as covariates to control for any differences in pre-
transfer scores. The assumptions underlying ANCOVA analysis include those for
ANOVA analysis and the assumption of homogeneity of regression across groups
(Polit, 1996). That is, the covariate (PPUS-FM before transfer or STAI-state
before transfer scores) should have the same relationship with the dependent
variable in each group (control and intervention) being compared.
Assumptions were checked. Normality of samples and equality of variances were
found to be satisfactory by examining the distribution graph and Levene’s equality

155
of variances. The relationship of the covariates and dependent variables in each
group were found to be linear by way of scatterplots.
The ANCOVA analyses reported the data means and standard deviation of the
PPUS-FM and STAI scores in the post-transfer period with estimated marginal
means accounting for pre-transfer levels for the two groups (Table 6.11).
Table 6.11: PPUS-FM and state anxiety after transfer. Variable Control
Intervention
Mean (SD) Estimated marginal mean (SD)
Mean (SD) Estimated marginal mean (SD)
PPUS-FM 76.24 (17.64) 77.06 (15.13) 76.38 (15.99) 75.57 (15.01) STAI– state 37.11 (13.45) 37.23 14.93) 37.72 (13.92) 37.59 (14.80)
An ANCOVA analysis was performed for the control and intervention groups
using the pre-transfer STAI –state scores as the covariate and the post-transfer
scores as the dependent variable. Results indicated there was no significant change
in either groups’ STAI-state scores when controlled for the pre-transfer levels of
anxiety (Table 6.12).
The second ANCOVA analysis was performed using the pre-transfer PPUS-FM
scores as the covariate and the post-transfer scores as the dependent variable.
Results showed there was no significant change in either groups’ PPUS-FM
scores when controlled for the pre-transfer levels of uncertainty (Table 6.12).
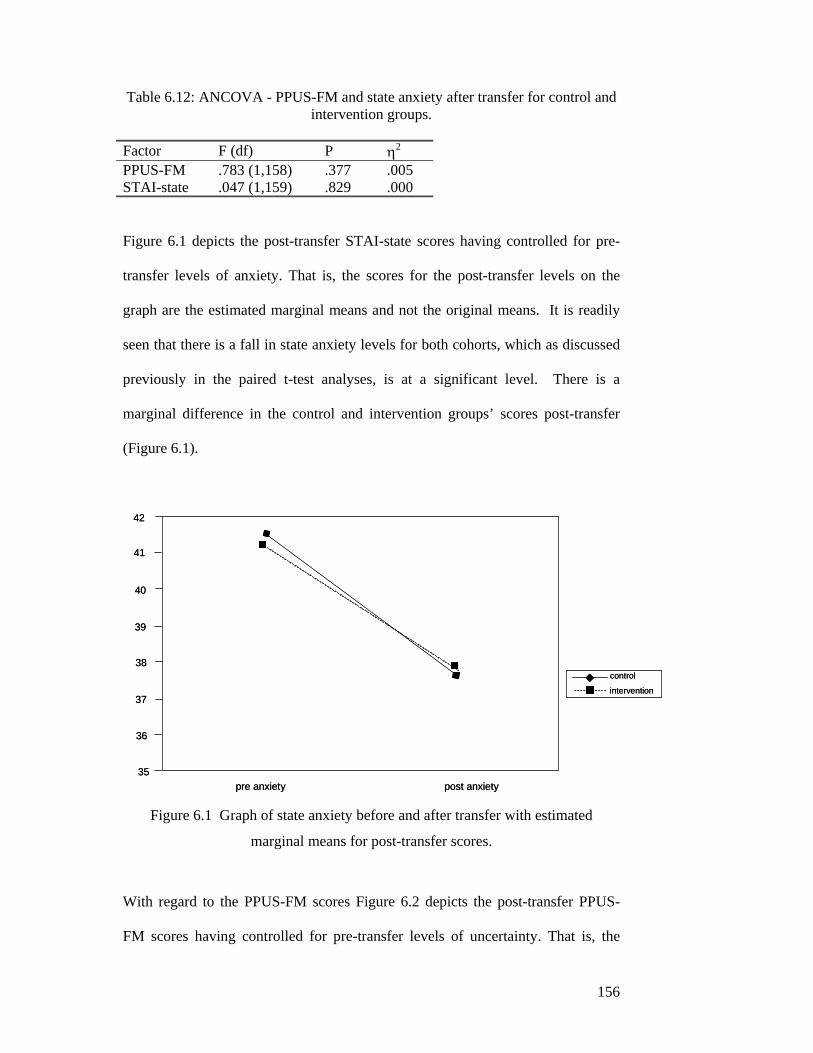
156
Table 6.12: ANCOVA - PPUS-FM and state anxiety after transfer for control and intervention groups.
Factor F (df) P η2 PPUS-FM .783 (1,158) .377 .005 STAI-state .047 (1,159) .829 .000
Figure 6.1 depicts the post-transfer STAI-state scores having controlled for pre-
transfer levels of anxiety. That is, the scores for the post-transfer levels on the
graph are the estimated marginal means and not the original means. It is readily
seen that there is a fall in state anxiety levels for both cohorts, which as discussed
previously in the paired t-test analyses, is at a significant level. There is a
marginal difference in the control and intervention groups’ scores post-transfer
(Figure 6.1).
Figure 6.1 Graph of state anxiety before and after transfer with estimated
marginal means for post-transfer scores.
With regard to the PPUS-FM scores Figure 6.2 depicts the post-transfer PPUS-
FM scores having controlled for pre-transfer levels of uncertainty. That is, the
control
intervention
42
41
40
39
38
37
36
35pre anxiety post anxiety
control
intervention
42
41
40
39
38
37
36
35pre anxiety post anxiety

157
scores for the post-transfer levels on the graph are the estimated marginal means
and not the original means which have been shown to drop significantly for the
intervention group in the paired t-test. There was however, not a significant
difference between the intervention and control group post-transfer PPUS-FM
mean values when controlled for pre transfer scores. Contrary to the situation
with state anxiety this graph shows a fall in uncertainty levels for the intervention
group. The control group’s uncertainty before and after transfer showed little
difference in the scores post-transfer as depicted by the horizontal line joining the
pre and post transfer uncertainty scores. The graph shows, however, how the
intervention group’s estimated marginal mean is obviously lower following
transfer than the control group’s mean (Figure 6.2).
Figure 6.2 Graph of PPUS-FM before and after transfer with estimated marginal
means for post-transfer scores.
The effect size and power were calculated for ‘uncertainty in illness’ as this was a
core analysis for the study which showed an interesting but statistically non-
73
74
75
76
77
78
79
80
preuncertainty
post
controlintervention

158
significant result. The power for the analysis of ‘uncertainty in illness’ was .01
and the effect size was similarly very low at .1. Post-hoc calculations were
performed on the sample size required to achieve a power of .8. The required
sample size was 1616 participants per group. This sample size was not feasible or
possible with the available resources and indicates that for this study, the resulting
small effect size was the contributing factor in not achieving a statistically
significant result.
6.3.1 Summary of Question 3 Therefore, in summary, both groups had a significant reduction in state anxiety
scores following transfer but when controlled for pre transfer scores, there was no
significant difference between the control and intervention groups’ scores. Only
the intervention group showed a significantly reduced level of ‘uncertainty in
illness’ following transfer but when controlled for pre-transfer scores, the PPUS-
FM score was not significantly lower than those in the control group. However, as
seen in Figure 6.2, the PPUS-FM scores for the intervention group showed a
decrease not seen in the control group results. The next section reports the results
of Question 4 which has five parts.
6.4 Question 4: Family members’ perception of transfer
There are five parts to this question all of which relate to how family members’
perceive components of their transfer from ICU. Results are presented in Table
6.13.
6.4.1 Question 4.1 Has the introduction of the intervention led to an improvement in family
members’ satisfaction with regard to their information needs?

159
The first part of Question 4 relates to the family members’ satisfaction in regard to
their information needs before transfer. Satisfaction with information was
measured by four questions on the survey completed by family members in the
general ward. The sub-scale had a Cronbach’s alpha reliability coefficient of .87
and .86 across two collection points. This is an index of the degree to which all
the different items in a scale are measuring the same attribute and is termed
internal consistency (Polit, 1996). The composite ‘satisfaction with information’
scores were calculated for the control and intervention groups with the higher
score indicating higher degrees of satisfaction. The control and intervention
groups’ histogram were negatively skewed towards participants being satisfied
which precludes the use of an independent t-test analysis. The equivalent non-
parametric test, the Mann-Whitney U test was examined for underlying
assumption and found to be met except for the random sampling in assumption
three. These assumptions include:
1. Similar shape and variability across distributions,
2. Independence of the two sample groups, and
3. Random samples (Polit & Hungler, 1996).
The results show that the intervention group had a higher median score for
satisfaction in regard to information (control median score = 16, intervention
median score = 17). Results indicate that the intervention group was significantly
more satisfied with the transfer information than the control group (Z = -2.433, p
= .015).

160
6.4.2 Question 4.2
Has the introduction of the intervention led to an improvement in ICU nursing
staff communication with family members?
The second part to Question 4 examined how family members perceived the
communication by the ICU nurse about transfer plans for the patient. Two
questions on the survey constituted this sub-scale with the higher number
indicating better communication. The Cronbach’s alpha coefficient was quite low
at .55 and .45 across two collection times for the two-item sub-scale. Therefore, as
there was not sufficient overlap in the items to form a sub scale which measures
the same attribute, each item was treated separately.
The first question asked participants if information given to them was easy to
understand. Family members in the control group had a lower mean score than the
intervention group (Table 6.13). An independent t-test analysis was performed
having first examined and found to be met the following assumptions underlying
the test except for assumption two:
1. Data should be interval or ratio level of measurement,
2. The scores should be randomly sampled from the population of interest, and
3. Scores should be normally distributed (Polit & Hungler, 1996).
Results show that the intervention group mean score was significantly higher than
the control group with the level of significance p<.001 (t = -3.194, df =160, p =
.002). This means that the intervention group found the information given to them
significantly easier to understand than the control group.

161
The second question asked participants if they were told about transfer plans as
they were being made. The intervention group had a higher mean and smaller
standard deviation for this question (Table 6.13). To compare the two groups’
means statistically, an independent t-test was initially performed. This showed
unequal variances and therefore the Mann-Whitney U non-parametric test
equivalent was performed following assessment of the underlying assumptions.
The analysis indicated that the intervention group was told significantly more
about transfer plans than the control group as indicated by the following statistic
(Z = -3.531, p < .000).
Table 6.13: Family members’ transfer results.
Question Control
Mean (SD) Intervention Mean (SD)
Z T (df) P
Told about transfer as plans being made
3.73 (1.53) 4.52 (.919) -3.531 .000**
How well prepared 3.91 (1.36) 4.52 (.919) -3.256 .001** Information that worried you?
1.45 (.614) 1.24 (.46) -2.257 .024*
Information easy to understand
4.04 (.834) 4.40 (.606) -3.19(160) .002**
(p<.05 *), (p<.005 **)
6.4.3 Question 4.3
Has the introduction of the intervention led to an improvement in the overall
preparedness of family members for transfer?
The third component of Question 4 asked if the intervention improved the overall
preparation for transfer for the family member? Participants were asked to
evaluate their overall preparedness for the transfer and to respond to one survey
question with five choices from “not at all prepared” to being “well prepared”.
Both the control and intervention groups’ results were negatively skewed towards
162
being better prepared. The control group had fewer participants who felt they were
“well prepared” (n = 39; 48.8%) than the intervention group who had 59
participants (68.6%) “well prepared”. At the other end of the scale, the
intervention group had only one participant (n = 1.2%) who indicated they
considered they were “not at all prepared”. The control group, however, had
seven participants (8%) respond that they were “not at all prepared”.
When comparing the control and intervention groups’ results, t-test analysis
indicated variances were unequal therefore not complying with an underlying
assumption that variances are equal. Therefore the Mann-Whitney U test was
performed. There was a significantly difference in how well prepared they felt as
shown by the following statistic (Z = -3.256, p = .001) (Table 6.13). These results
suggest that the intervention group experienced a transfer period for which they
felt better prepared than that experienced by the control group. The following part
of Question 4 will report on information given to family members which worried
or frightened them. This data has been reported both in a quantitative manner and
then with the verbatim comments from their responses to an open-ended question.
6.4.4 Question 4.4 Were family members worried or frightened by information given to them and
what was the information that caused this concern?
There were two sections to this question and the quantitative data is reported first.
Participants were given three choices when asked if there was information given
to them that worried or frightened them. The choices included “no worries”,
“some worries” or “quite a few worries” on a three-point scale. Forty-nine

163
participants (56.3%) in the control group responded that they were not told
anything that worried or frightened them during the pre-transfer process compared
to the intervention group which recorded 63 participants (73.3%) not having
anything told to them that worried or frightened them. Comparison of the mean
scores for the control and intervention groups were performed initially with a two-
sample t-test but as variances were not equal a Mann-Whitney U test was
required. This analysis indicated that the control group was significantly more
worried than the intervention group about information told to them before transfer
from ICU at the level of significance of p<.05 (Z = -2.257, p = .024) (Table 6.13).
The second section of this question asked an open-ended question allowing for
comment from participants. When participants were asked to write in their own
words on what worried or frightened them, 51.9% (n = 40) in the control and
61.7% (n = 50) in the intervention group indicated they did not have concerns and
no comment was made. The other written comments have been coded and
grouped under a range of categories (Table 6.14).
Table 6.14: Areas of worry for family members.
Source Control n (%)
Intervention n (%)
No comment 40 (51.9%) 50 (61.7%) General Apprehension 9 (11.7%) 1 (1.2%) More information wanted 9 (11.7%) 7 (8.6%) Unsure of diagnosis 6 (7.7%) 3 (3.7%) Ward expectations unsure 4 (5.1%) 0 Very clearly explained 2 (2.4%) 7 (8.6%) Potential pain 1 (1.2%) 0 Misinformation given 1 (1.2%) 1 (1.2%) No information requested 1 (1.2%) 0 Too much information 0 1 (1.2%)

164
The following section gives examples of each category. One participant was quite
specific about their worries and wrote they were concerned about potential pain
for the patient. Others, however, had more general concerns regarding
expectations in the general ward. Four participants (5.1%) in the control group
and no participants in the intervention group indicated this was an area of concern
for them. An example of a comment under the area of ward expectations was:
“My wife and I were a little concerned at first when our son was transferred from ICU as we were somewhat apprehensive as to what to expect in the ward.” (response # 1)
Uncertainty regarding the diagnosis concerned and worried some participants with
the following an example of this group of responses:
“Unsure because of the state of the head injuries.” (response # 41)
A number of participants indicated that in general terms they were apprehensive
about the outcome which caused worry for nine (11.7%) in the control group but
one (1.2%) reported this type of worry in the intervention group. An example of
family members’ general apprehension was:
“Doctors told me the operation went well but he was not out of danger until he woke up because he had suffered TIAs [Transient Ischaemic Attacks] before. It took the nurses in ICI three attempts to wake him over a period of five hours.” (response # 36)
One participant noted they had not requested any information and two participants
(2.4%) in the control group and seven (8.6%) in the intervention group
commented that things were very clearly explained. For example:
“Education, information and availability of staff was very good.” (response # 48)
Others, however, would have liked more information and the following was an
example:

165
“The concern that he seemed unstable but was being moved – assumed he was OK but more detail explanation would have been useful.” (response # 9)
Also within the category of wanting more information were two responses from
family members in the intervention group who wrote that their relative was to be
transferred to the Infectious Diseases ward and this was a cause for worry. The
following example however, demonstrates that the information was forthcoming.
“Nurse did not know what sort of a ward my wife was being transferred to. I also had difficulty understanding how and why a patient that is immuno-suppressed is transferred to an infectious diseases ward, however, when explained by the ICU doctor the issue was cleared.” (response # 52)
On the other hand, one respondent in the intervention group thought too much
information presented a worry to them as indicated by their response:
“About stopping the heart to go on the heart-lung machine. The whole process of heart by-pass is just amazing but daunting procedure to be told about.” (response # 54)
Receiving misinformation was a cause of worry for one participant from both the
control and intervention group. An example follows:
“Misinformation re return time to ICU – was told he was back and after waiting was told that “really it was a mistake – he had only just been wheeled through into ICU”. Very upset but understand it was a communication error.” (response #18)
To summarise, the majority of participants (control 51.9%, intervention 61.7%)
did not express a need to comment further on the information provided to them.
This is somewhat congruent with responses to the preceding question where
responses indicate that for the majority (control 56.3%, intervention 73.3%),
family members were not worried by the information given to them. For those
who recorded worries about information given to them, the control group was

166
more apprehensive about the situation than the intervention group and both groups
said they wanted more information. More in the intervention group wrote that the
information was very clearly given to them. Comments written by participants
related to information given to them by both medical and nursing staff.
6.4.5 Question 4.5
What information did family members wish they had been told?
The final part to Question 4 examined the results of participants’ responses to the
open-ended question where they were asked to reflect on anything they wish they
had been told before transfer from ICU. The control group had 24 participants
who did not answer this question whereas the intervention group had seven. At
times, participants wrote two comments, which fell into two categories, and these
comments therefore will be reported separately. Thirty-six (38.7%) responses
from the control sample wrote that there was not anything else they wished they
had been told whereas 52 (63.4%) responded in this way in the intervention group.
Participants’ comments have been grouped under a range of categories (Table
6.15).
Table 6.15: Information family members wanted.
Source Control Responses
n = 93 (%) Intervention n = 82 (%)
Adequate information given 36 (38.7%) 52 (63.4%) No response 24 (25.8%) 7 (8.7%) Wanted more information generally 10 (10.7%) 5 (6.2%) Staff did a great job 9 (9.8%) 6 (7.5%) Lack of information about transfer 6 (6.4%) 2 (2.5%) More information about diagnosis 3 (3.2%) 2 (2.5%) Lack of communication 3 (3.2%) 3 (3.7%) Wanted more information about ward 2 (2.1%) 3 (3.7%)

167
The following section will present some examples of their verbatim comments
starting with the category of adequate information given
“No everything I needed to know was volunteered.” (response #18)
The category of “staff did a great job” complimented the ICU staff on their high
quality of care and sometimes compared this with the general ward care, as seen
in the following example:
“ NO, I was thoroughly satisfied with the information and assistance I received in ICU by nurses and doctors. I wish it was the same in the general wards (doctors are
not as accessible as in ICU).” (response # 50)
The perception of a lack of information about transfer was reported by six in the
control group and by two in the intervention group. One participant from the
control group wrote:
“ Information on his progress, on their [ICU staff] transfer plans beforehand, and regarding the environment of the general ward.” (response # 4)
Others wanted more information specifically related to the diagnosis as indicated
by this comment:
“ A definite reason for his injuries.” (# response 5)
Requiring more information about the ward was reported as something some
participants would have liked. One participant in the control group wrote:
“How many people in the ward, visiting hours, and how many allowed in the room at one time, whether patient was going to be fed, facilities available to patient e.g. television.” (response # 32)
Wanting more information in a general sense was a common theme, however,
twice as many participants in the control group highlighted that this was a concern
for them than those in the intervention group. One participant wrote:
“More [information] about my wife’s illness, not just bits at a time”. (response # 32)

168
General comments were made relating to a lack of communication in a broad
sense as depicted in the following example:
“Not really told much about transfer. I expected him to be in ICU longer.” (response # 14)
Another comment within this category took a broader look at the communciation
involving ICU and the general ward staff and their care
“ Wish we had been told he wouldn’t be reviewed until weekday (transferred on Saturday morning). We would have requested staying in ICU until Monday. Written communication between doctors in ICU and ward was inadequate…. Naso gastric tube re-inserted ???necessary (just taken out in ICU).
Authority for pain relief was not easily accessible in ward (nurse didn’t want to give panadol without doctor’s
authority and he was in pain and no doctor around) - this was not anticipated.” (response # 64)
To summarise, the majority of participants in both the intervention and control
groups considered they had sufficient information, however, the intervention
group recorded 16 more positive responses than did the control group. The ICU
staff were praised by participants in both groups but others wanted more specific
information in the area of patient diagnosis, transfer and general ward. The need
for improved communication was considered important to a few participants.
6.4.6 Summary of Question 4 To summarise the results of the first three parts of Question 4, the intervention
group of family members experienced significantly higher levels of satisfaction
with the information given to them before transfer from ICU. Data revealed the
intervention group similarly recorded significantly higher levels of information
they could understand. They also recorded significantly higher results when asked
if they were told about transfer plans as they were being made. The intervention

169
group was significantly better prepared for transfer than those in the control
group.
The results to the final two parts of Question 4 revealed that 65.3% of the control
group participants and 73.3% of the intervention group participants were not
worried about information given to them before transfer. Data on participants’
concern relating to the information given to them revealed that the intervention
group had fewer worries than those in the control group. Finally, 63.4% of the
intervention group and 45% of the control group thought they had been told
sufficient information. The areas the control group highlighted for additional
information included information about the ward and patient diagnosis whereas
both groups saw the need for improved communications in some instances. The
following section reports results from research Question 5.
6.5 Question 5 - ICU nurses’ perception of intervention
The 110 ICU nurses recruited into the project (91.6% recruitment) were given a
questionnaire at the completion of the study if they had transferred a patient and
family to a general ward (n = 40). Of these 40, 33 completed questionnaires were
returned to the researcher (82.4% return rate). Of the seven not collected, three
staff members were away on holiday, another three had left the hospital and the
final one was not forthcoming after two reminder notes.
6.5.1 Question 5.1
What was the ICU nurses’ perception of their unit’s attitude to families and how
important are family members to patients’ recovery?

170
All participants considered their unit’s attitude to family members was either
“quite good” (n = 25, 75.8%) or “excellent” (n = 8, 24.2%) on a five point scale
from “not very good” to “excellent”. When asked the importance of family
members to a critically ill patient’s recovery on a five point scale from “not
important” to “very important”, 24 (72.7%) considered family members were
“very important” to a critically ill patient’s recovery. The remaining nine (27.3%)
considered families were “important”. That is, 100% of participants considered
family members were “important” or “very important” to patients’ recovery.
6.5.2 Question 5.2
What was the ICU nurses’ perception of the level of importance of the process of
transfer from ICU for families?
On a five-point scale from “not important” to “very important”, participants were
asked how important the transfer process was for family members. Data indicated
that 93.9% (n = 31) considered that the transfer process was either “important” or
“very important” for families (Table 6.16).
Table 6.16: Importance of transfer process for family members.
Importance n (%) Very important 20 (60.6%) Important 11 (33.3%) Not sure 2 (6.1%) Slightly important 0 Not important 0
6.5.3 Question 5.3
Has the intervention provided a useful means to improve discussion with family
members from ICU nurses’ perspective and would they recommend its use?

171
Participants recorded how many times they had used the structured pre transfer
method for transferring families and patients to the ward (Table 6.17).
Table 6.17: Times RNs used intervention.
Number of times used n (%) 1 15 (37.5%) 2-5 16 (40.0%) 6-9 2 (5.0%) More than 10 0
The sample was asked two questions relating to discussion which occurred as a
result of the intervention. One question related to whether the intervention helped
to provide a framework for discussion and the other asked if it promoted
discussion about the patient. With regard to the first question on the helpfulness of
the intervention in providing a framework for discussion, participants had a five
point scale on which to respond: “very helpful”, “quite helpful”, “unsure”,
“helpful at times” and “not helpful”. Twenty-nine participants (90.6%) indicated
that the structured pre-transfer educational method was either “quite helpful” or
“very helpful” in providing a framework for discussion (Table 6.18).
Table 6.18: Helpfulness of intervention as a framework for discussion.
Factor n (%) Very helpful 13 (40.6%) Quite helpful 16 (50.0%) Unsure 1 (3.1%) Helpful at times 2 (6.2%) Not helpful 0 The second question asked if the intervention promoted discussion about the
patient’s illness. On the five point scale from “no” discussion to a “great deal” of
discussion, 60% of participants considered that it promoted “some discussion” or

172
“a great deal of discussion” about the sick patient. No one indicated it promoted
“no discussion” (Table 6.19).
Table 6.19: Discussion promoted by intervention.
Amount of discussion n (%) No 0 Minimal 7 (17.5%) Not sure 1 (2.5%) Some discussion 20 (50%) Yes, a great deal 4 (10%)
The next part to this question related to information participants thought were
missing from the educational brochure which was designed to stimulate
discussion. Results from this open-ended question indicated that 28 (84.8%)
participants thought there was nothing missing from the brochure and five wrote
other comments on their surveys. There were comments that information on what
to bring for patients on a ward would be helpful – for example, toiletries and
pyjamas.
Finally, the participants were asked if they would recommend the introduction of
the intervention to support all transfers from ICU. They were able to select from
four responses of “no”, “not sure”, “yes, with changes” and “definitely”. A
majority (75.8%, n = 25) of participants indicated that they would “definitely”
recommend the introduction of the structured pre-transfer educational method to
support all transfers from their unit. Two were “not sure” and the remaining six
said that “yes, it should be introduced with changes” (Table 6.20).

173
Table 6.20: Future use of intervention.
Introduction of intervention n (%) No 0 Not sure 2 (6.1%) Yes, with changes 6 (18.2%) Definitely 25 (75.8%)
6.5.4 Summary of Question 5 In summary, all participants thought their unit’s attitudes towards family members
was either “quite good” or “excellent” and that family members were an important
factor in the successful recovery of patients. They also thought that the transfer
process from ICU was an important event for families.
A large proportion of participants thought the intervention provided a useful
framework and promoted discussion with family members. Most participants
thought the brochure was complete in its current form with 94% indicating it
should be introduced for all transfers from ICU.
6.6 Summary of results
This chapter has reported results for each of the five research questions. The first
research question analysed the ‘uncertainty in illness’ scores for the control and
intervention groups before transfer and found these levels to be not significantly
different. That is, the control and intervention groups had similar levels of
uncertainty before transfer from ICU thus indicating their baseline uncertainty
levels were well matched and thus able to be readily compared after transfer in
relation to the intervention. As predicted in the study’s Conceptual Framework,
the second research question found a significant relationship existed between
‘uncertainty in illness’ scores and state anxiety with state anxiety accounting for

174
24.3% of the variance of ‘uncertainty in illness’. It also reported that when the
admission was unexpected there were significantly higher levels of ‘uncertainty in
illness’. The final factor investigated which affected the level of uncertainty was
when the family member was the parent as opposed to the child of the patient
there were significantly higher levels of uncertainty. In regards to anxiety levels,
the factor which significantly affected family members’ anxiety scores was the
level of social support they experienced.
Question 3 examined the effect of the intervention on PPUS-FM and STAI-state
scores. Results showed that STAI-state scores reduced significantly following
transfer for both groups and that both groups recorded similar post transfer levels
when controlled for pre-transfer STAI scores. The PPUS-FM scores, although not
significantly different in the after transfer period when controlled for pre-transfer
scores, showed a definite fall in uncertainty scores for those in the intervention
group as opposed to the control group who did not experience this fall. Graph 6.2
(p. 157) depicts this clearly as it shows the control group before and after transfer
levels of uncertainty to be almost a horizontal line whereas the intervention group
has an obvious drop in uncertainty.
Analysis of Question 4 showed that the intervention group scored significantly
higher levels of satisfaction with their transfer based upon the structured pre
transfer educational method. The intervention group was significantly more
satisfied with the information about transfer given to them by the ICU nurse than
was the case for the control group who experienced an ad hoc transfer process.
The intervention group were also given significantly more information about

175
transfer as plans were being made than was the control group. In addition, the
intervention group were given this information in a way they could understand
significantly more than was the case for the control group. The intervention group
were significantly less worried about the information given to them than was the
control group. Sixty-one point seven percent of the intervention group thought
they had no concerns about the information given to them as opposed to the
control group who had 51.9% with no concerns. The major areas of concern for
participants in the control group included general apprehension about the transfer
(11.7%) and worries about the diagnosis (7.7%), whereas the intervention group
recorded only 1.2% of participants generally apprehensive and 3.7% worried
about information on the diagnosis. Finally, 63.4% of intervention group
considered they had been given adequate information about transfer whereas a
lower percentage of 38.7% of the control group felt they had been given adequate
information.
The final research question asked the ICU nurses’ opinions on families and the
efficacy of the intervention. Collectively they considered families were important
and that transfer out of ICU was an important event for families. They reported
that the intervention contributed positively to enhancing communication with
family members as 90.6% of the nurses thought it was helpful providing a
framework for discussion with family members. Ninety-four percent of the ICU
nurses indicated the method should be introduced for all transfers from ICU.

176
CHAPTER 7: DISCUSSION
7.0 Introduction The previous chapter has outlined the results of data analysis in relation to the four
phases of the study which developed and evaluated an intervention to improve
family members’ transfer from ICU. Anxiety was significantly related to
‘uncertainty in illness’ in family members at the time of transfer from ICU. The
unexpected admission to ICU and parental relationship were two significant
contributors to the development of uncertainty whereas the amount of social
support significantly affected the level of state anxiety. However, the introduction
of the intervention did not reduce the levels of state anxiety in the intervention
group but the levels of uncertainty reduced although not at a significant rate. It
will be argued that although not statistically significant, ‘uncertainty in illness’
levels in the intervention group reduced whereas the control group did not, thus
supporting the notion that clinical significance may well have been achieved. The
intervention statistically improved family members’ perception of the transfer
process and ICU nurses recommended its introduction for all ICU transfers.
This study has methodological strengths that have improved on those used in prior
research in the field. Firstly, this research has examined the factor, ‘uncertainty in
illness’ in detail in a cohort of ICU family members for the first time. Secondly,
the current study is the first of its kind to examine an intervention in relation to
reducing anxiety and uncertainty of family members around transfer from ICU.
Thirdly, the study evaluated family members’ satisfaction and nurses’ perception
of the intervention in helping them to support the transfer process thus reporting

177
data from two vital stakeholders in the transfer process. Fourthly, the intervention
is based upon sound educational principles of Knowles’ Adult Learning Theory
(1980) to ensure information is individualised and promotes understanding for
each participant. Other studies have not documented their founding educational
principles which leads one to question the soundness of their theoretical base.
Finally, where possible, standardised psychometric instruments were used which
allows for both replication and comparisons to be drawn with other studies.
This chapter discusses the outcomes of the study and the factors found to
contribute to the presence of anxiety and uncertainty. The findings will be
examined in relation to contemporary literature on anxiety and ‘uncertainty in
illness’. Limitations of the study will also be discussed.
7.1 Phase One The aim of Phase One of the study was to document important and relevant
information to provide the key points for the foundation of nurse/family member
discussion before transfer. Family members and critical care nurses provided the
data for this phase to ensure the information was relevant to family members’
needs as suggested by Knowles (1980) and others (Scriven & Tucker, 1997).
Family members surveyed in Phase One of the study agreed with results from
previous Australian studies which state the need for information around the time
of transfer is one of the greatest needs of families in a critical illness situation
(Choate & Stewart, 2002; Johnson, 1999; Russell, 1996; Russell, 1999a). Seventy
percent of participants in the present study rated being included in planning for

178
transfer as “important” or “very important”. These family members, along with
other previous studies, identified as highly important, the need to know and be
involved at the early stages of transfer planning (Liddle, 1989; Millar, 1991;
Molter, 1979; O’Neill Norris & Groves, 1986). Their inclusion in the process is
suggested as a way to facilitate their adjustment to subsequent changes in patient
management which occurs in a general ward (Foss & Tenholder, 1993).
Adjustment is needed as transfer from ICU is reported as a stressor which induces
anxiety for family members (Liddle, 1989; Millar, 1991; Roberts, 1976; Streater et
al., 2001) and adequate preparation can reduce this anxiety (Schwartz & Brenner,
1979; Spatt et al., 1986). Information about the predicted outcome of the illness
was reported as “important” or “very important” by 80% (n =16) of participants
and 75% (n =15) thought they should be informed about proposed treatment. This
information is central to the ongoing care for the patient, which the expert panel
considered was a significant role for the family.
The Australian expert panel’s comments regarding the importance of family
members to critically ill patients, concurred with previous international studies
(Hickey & Leske, 1992; Leske, 1992; Scullion, 1994; Spatt et al., 1986) which
considered families to be an important feature in patients’ recovery process. When
family members’ needs are not met they respond in a way that affects patient
recovery (Mendonca & Warren, 1998). This can occur as a result of an inability
to take in information (Odell, 2000) and make decisions on patients’ behalf
(Cagan, 1988), or through relationship disturbances and psychological distress
(Elpern, Patterson, Glaskey, & Bone, 1992; Mishel, 1997) which affect important
issues concerning the patient.

179
The Australian expert panel considered that the transfer from ICU required nurses
to give family members specific information about the current illness state, the
new ward environment and changing ward expectations. They agreed that family
members should be informed regarding the physical environment such as
bathroom and kitchen facilities, chapel location, close affordable accommodation
and the need to care for oneself. Together these support services could contribute
to the physical and emotional well being of the family members thus enabling
them to cope with the information regarding the critical illness situation (Leske,
1986).
The expert panel of critical care nurses rated the current transfer processes from
ICU to ward areas as being poorly undertaken in their experience and that family
members were frequently not included in planning for transfer. This was in spite
of the fact that family members’ inclusion in planning for transfer has been
reported consistently in the literature over the past two decades as a primary need
of the family (Cutler & Garner, 1995; Daley, 1984; Flanagan, 1996; Leske, 1991;
Molter, 1979). This infers clinical practice is not reflecting nursing research
outcomes of current best practice evidence and the question needs to be asked as
to why evidence of best practice is not being embraced by clinicians? Fox and
Jeffrey (1997) reported that over half of the nurses in their study thought it was
unrealistic for them to provide psychosocial family support such as discussion of
family coping strategies. In the current study psychosocial factors may emerge
during discussion of imminent transfer as family members are about to leave an
environment and situation with which they have become familiar and move to one
which is foreign. This together with other findings by Fox and Jeffrey (1997) that

180
nurses tended to implement family friendly interventions when the intervention
was part of the unit’s protocol suggests barriers to clinical best practices in an ICU
where planning for transfer has no guidelines for nurses.
Emotional reactions by family members can deter nurses from communicating
with families (Hickey & Lewandowski, 1988). However, inappropriate behaviour
may be the result of family members not having their fundamental needs met as
they try to grapple with unfamiliar stressful circumstances (Benner et al., 1999). A
study performed by Kleinpell and Powers (1992) examined the needs of family
members in ICU, and concluded that the requirement for information was a
universal need which nurses should endevour to meet. By way of assisting and
supporting nurses in this objective, many studies suggest the use of descriptive
brochures (Bradenburg & Gifford 1997; Cutler & Garner, 1995; Kleinpell &
Powers, 1992; Lange, 1989; Leith, 1999; Shannon, 1973) to provide information
as an adjunct to face to face communication (Henneman & Cardin, 1992; Scriven
& Tucker, 1997). The written word provides tangible information (Henneman &
Cardin, 1992) which supports understanding and recall of information
(Henneman, McKenzie & Dewa, 1992) at a time when facts are difficult to
remember (Robb, 1997). It is important, however, that there is an understanding
and compliance with educational principles involved with effective learning such
as seen with Knowles’ Adult Learning Principles (1980). In particular, the family
members’ readiness and motivation to learn about the illness and imminent
transfer, together with their previous experiences and need for application for the
information (Knowles, 1980) need to be stylised to meet individual’s information
needs. The brochure itself needs to have legible print, nonjustified lines, use of

181
headings, attractive appearance, and professional development to enhance the
utility of the brochure (Scriven & Tucker, 1997). All of these features can been
seen in the current brochure used to support the intervention.
Although the use of brochures is a recognised way of providing information,
evaluation of such interventions in the critical care area is an essential but
frequently forgotten part of the process (Bradenburg & Gifford 1997; Kleinpell &
Powers, 1992; Lange, 1989; Leith, 1999; Scriven & Tucker, 1997). Adequate
nurse preparation in the way of education on the implementation of the family
related intervention is also an essential component for success (Fox & Jeffrey,
1997). Thus it is suggested that the use of quality printed material with sufficient
educational support for nurses assists them to fulfil this primary family members’
need for information.
7.2 Phase Two
The second phase of the study was a consultative phase where information from
Phase One of the study was collated to form the content for a brochure to support
patient transfer. Three teachers reviewed the wording for the brochure and
ensured the language was congruent with an eighth grade literacy level as
suggested by nurse researchers (Lange, 1989; Macey & Bouman, 1991).
Following recommendations from the teachers for alterations in the wording,
nursing personnel reviewed the material ensuring the product met institutional
needs, an important step should one wish to introduce material into an
organisation such as a hospital (Bradenburg & Gifford, 1997). Bradenburg and
Gifford (1997) advocate a multidisciplinary team approach to the development of

182
such material. This occurred in the current study with representation from the
target audience (family members) to ensure it addressed the needs of the group for
which it was designed, together with feedback from doctors and nurses in the
initial development phases. The intervention was introduced into the ICU during
Phase Three of the study which had a pre-test, post-test design. Discussion on
this phase and Phase Four of the study will follow by addressing each of the five
research questions in order.
7.3 Question 1 What was the level of ‘uncertainty in illness’ in family members before transfer
from ICU as measured by Mishel’s PPUS-FM Scale?
The level of ‘uncertainty in illness’ has not previously been described in family
members in an ICU environment therefore this study provides additional
information to enhance understanding and strategies of reducing uncertainty. In
the area of oncology nursing, uncertainty has been related to psychological
maladjustment with relationship disturbances, psychological distress (Mishel,
1997) and reduced life satisfaction (Hilton, 1994). When uncertainty occurs,
coping strategies are immobilised thus reducing one’s ability to adjust to a
situation (Hilton, 1994). According to Mishel’s theory of ‘uncertainty in illness’
(1981), with uncertainty comes an inability to decipher and interpret a situation
accurately. This lack of perception thus impairs adaptation to the new illness
event, in this case transfer from ICU, which is appraised in a negative light
(Coyle, 2001; Mishel, 1988). In general terms, transfer from ICU is a positive step
as patients no longer require the complicated, often highly invasive medical and
183
nursing support. When families perceive this positive step as a negative
development, inappropriate coping strategies may come into force.
Family members provide the one constant for the patient in the new ward
environment and their support in the ongoing rehabilitation is essential (Millar,
1991). However, uncertainty is said to have an “immobilising effect on coping
processes” (Hilton, 1994, p. 15) which may impact significantly on family
members ability to provide this necessary support. Family members’ adaptation
and coping strategies may prove to be inadequate in managing the transfer and
new illness situation (Mishel, 1988), leading to feelings of helplessness, confusion
(Hilton, 1994) and ineffective adaptation to the situation (Mishel, 1988). The
current study’s situation involved the imminent transfer from ICU following a
critical illness.
The present study’s family members’ uncertainty scores recorded means of 77.22
and 78.93 for the control and intervention groups. Mishel (1997) reports
uncertainty scores for family members from 12 data samples. These range from
means of 69.3 (SD = 13.9) for family members (n = 30) of patients with a
myocardial infarction to 89.0 (SD = 12.8) for family members with a relative with
alzheimers’ disease (n = 20). Only raw data scores are given and the condition,
timing and related factors are not described therefore limiting further
comparisons. Mishel’s (1997) data sets report on small sample sizes, which
reduces the generalisability of the findings.

184
With these limitations highlighted, the current sample mean scores fall within
midrange of Mishel’s (1997) reported scores. Mishel (1997) reports one score for
family members from a mixed ICU (n = 43) where the mean uncertainty score
was 78.6 (SD = 10.4). These results are the same as those reported in the current
study. Articles describing studies in detail provide additional understanding of the
concept of uncertainty but are not readily comparable to the current study due to
different populations and study settings (Northouse et al., 1995; Yarcheski, 1988).
Northouse et al. (1995) examined the husbands of wives who had received a
diagnosis of recurrent breast cancer. Their uncertainty levels had a higher mean
score (mean = 84.2, SD = 15.7) than the current study (77.22, 78.93). Transfer
from ICU indicates an improvement in patients’ condition whereas a recurrence of
a potentially life threatening condition could understandable generate more
uncertainty. The changing course of their wives’ illness and lack of clarity of what
would happen next were factors in their high uncertainty scores (Northouse et al.,
1995). Northouse et al. (1995) suggested that the husbands’ high uncertainty
levels were closely related to the amount of information they received from health
professionals. They recommended partners should be included in intervention
strategies designed to assist with their response to the illness situation (Northouse
et al., 1995) as was seen in the method of the current study. An additional feature
of Northouse et al.’ study (1995) was the gender bias of the all male sample.
When controlling for gender Mishel (1997) reports that with samples of 135 males
and 223 female family members, males recorded higher ‘uncertainty in illness’
scores (male = 82.3, SD = 16.6, females = 78.2, SD = 15.2). Therefore, Northouse

185
et al.’s results (1995) may be skewed to obtaining a higher mean uncertainty score
as all participants were male.
Illness situations do not have to be acute in nature. Chronic illness continues to
stimulate feelings of uncertainty as described by Yarcheski (1988) in a study of
parents with adolescent children with cystic fibrosis attending a routine clinic
appointment. The mean ‘uncertainty in illness’ score for parents (n = 32) was
74.74 (SD = 15.23), four points lower than that recorded for the current study.
The level of uncertainty in Yarcheski’s study (1988) underscores the fact that even
in long-term illness uncertainty remains a factor as participants grapple with
managing and anticipating illness progression (Yarcheski, 1988).
Mishel further developed additional versions of her original tool developed in
1980 for adult patients in an acute hospital setting. Three other versions are now
available. These include a version for patients in a community setting, parents of
sick children and family members with an ill relative. The adult and community
scales, although measuring the same phenomenon, have different numbers of
items to the parents of sick children and the family version. This limits the
comparison of mean scores for the current study to those using the family or
parent version as the scoring range is the same with these tools. The family
version (PPUS-FM) was the last tool designed by Mishel with normative data
becoming available in 1996 (Mishel, 1997). In this case, the recency of the
availability of the tool to other researchers has limited the number of studies
conducted and reported in the literature thus restricting comparisons with the
current study.

186
In summary, the current study’s levels of ‘uncertainty in illness’ is similar to
previous studies and highlights the need for further understanding of this
phenomenon for family members in the critical care area. Uncertainty inhibits
coping and prevents adjustment to new situations. Information provided by nurses
is suggested as an effective intervention in reducing uncertainty for family
members at the time of transfer from ICU. Further investigation of the concept
of uncertainty is reported in Question 2 which examined the relationship between
uncertainty and anxiety scores together with factors significantly related to each
factor. This discussion follows.
7.4 Question 2 7.4.1 Question 2.1 Was there a relationship between family members’ ‘uncertainty in illness’ as
measured by PPUS-FM (Mishel, 1997) and anxiety levels as measured by STAI –
state (Spielberger et al., 1983)?
The levels of state anxiety recorded mean levels of 41.24 and 41.62 for the control
and intervention groups, or medium levels of anxiety (Spielberger et al.). When
compared with Spielberger et al.’s normative data (1983) for working adults
(mean = 35.59, SD = 10.54) the level in the study’s sample was considerably
higher indicating the current sample were more anxious prior to transfer from ICU
than working adults. The scores are very similar to those of a medical/surgical
patient cohort where a mean score of 42.4 was recorded (Spielberger et al., 1983).
It is difficult, however to make comparisons between patients and their families.
In a study by Bouvé et al. (1999), state anxiety scores for parents of children being
transferred from a paediatric intensive care unit (PICU) recorded a mean value of

187
47.00 (SD = 9.66) for the control group and 45.16 (SD = 9.77) for the
intervention group. These values are higher than those recorded in the current
study and may reflect the different population and paediatric setting. The inclusion
criteria may also have impacted upon recording higher anxiety levels as parents
were only eligible if it was their infant’s first admission to a PICU, whereas the
current study did not exclude participants for whom this was a subsequent ICU
admission. Although Bouvé et al.’s study was a randomised control trial, the
small sample size (control group n = 19) reduces generalisability of results.
Chartier and Coutu-Wakulczyk (1989) measured state anxiety on family members
in a surgical ICU and reported state anxiety levels of 47.9 (SD 12.02) which were
higher than levels reported in the present study. Two features are suggested as
reasons for the higher levels of anxiety. The first is related to the method of data
collection. Participants were recruited during their first visit to ICU but Chartier
and Coutu-Wakulczyk (1989) provide no information as to when the data
collection occurred. While patients are in ICU their condition potentially varies
enormously, with some quite stable periods and other life threatening events
throughout their stay. A number of variables are therefore potentially affecting
family members’ anxiety when the time of data collection is not standardized.
Another feature of Chartier and Coutu-Wakulczyk’s study (1989) is that there was
no limit to the number of family members per patient who participated whereas in
the present study only one family member per patient completed the
questionnaires. There were up to five family members for some patients in
Chartier and Coutu-Wakulczyk’s study (1989). This has the potential to skew the
results towards the anxiety levels of patients with many family members

188
participating. In the present study, anxiety scores were also examined in relation
to uncertainty levels.
As postulated in the Conceptual Framework for the study, a significant positive
relationship was found to exist in the current study between uncertainty scores and
STAI-state scores. The relationship between these factors commonly found in
illness has only recently been examined statistically (Deane & Degner, 1998). No
study has been conducted in an ICU setting thus limiting comparison with other
findings. The present study’s results of a positive relationship between state
anxiety levels and uncertainty are however, supported by findings by Wong and
Bramwell (1992) with women following discharge from mastectomy surgery and
with women after a benign breast lump diagnosis (Deane & Degner, 1998).
Another study suggests that as the perception of transfer as a threat reduces, so
does the psychological parameters of stress (Poe, 1982). Although the
relationship in Poe’s study examines uncertainty and stress (rather than anxiety),
this can be extrapolated to the concept of anxiety as the level of stress is a
precursor to state anxiety (Spielberger et al., 1983). Cognitive appraisal of the
stressful event leads to a certain level of anxiety and the concurrent feelings of
uncertainty (Mishel, 1988) as demonstrated in the current study. The relationship
between the two concepts supports the design and implementation of interventions
directed to decreasing uncertainty or anxiety.

189
7.4.2 Question 2.2
Were patient and family member’ factors significantly related to PPUS-FM
scores?
‘Uncertainty in illness’ in the current study was significantly related to anxiety as
discussed in the previous question. It was also related to the unexpected nature of
the admission into ICU. This association is predictable and supports the
conceptualisation of uncertainty, which reasons that unfamiliarity with an event,
and more specifically, lack of knowledge and understanding increases uncertainty
(Mishel & Braden, 1988). Mishel (1983) found that there was a significant
positive relationship between uncertainty levels and parents’ perception of the
seriousness of their child’s illness. Public conceptualisation of an emergency
admission to ICU rightly invokes perceptions of a critical illness situation, which
is accompanied by feelings of uncertainty. This extends to the time of transfer
from ICU and hence it is important for critical care nurses to have an
understanding of uncertainty. Hughes (1993) found that uncertainty was greatest
at the time of diagnosis, which in the case of unexpected admissions to an ICU,
frequently occurs during the ICU period. Contrary to Mishel and Braden (1987),
this study did not find a significant relationship between uncertainty scores and
social support although Mishel and Braden’s study (1987) only found this
relationship at the time of illness diagnosis. Knowing the diagnosis alone is
suggested to be insufficient in reducing uncertainty as research by Mast (1998)
found that women experienced higher levels of uncertainty when there was no
known cause for symptoms even when a diagnosis of breast cancer was known.

190
The other factor significantly related to uncertainty in the current study was the
relationship of the participant to the patient. When the participant was a parent as
opposed to the child of patients, their level of uncertainty was significantly higher.
It needs to be noted however, that all participants who were parents in the current
study saw their child admitted to ICU as a result of a sudden health incident such
as a motor vehicle accident. That is, none of the parents knew that their child was
going to be admitted to ICU as part of a planned procedure or operation. This
could well provide an explanation as to the significant nature of their elevated
levels of ‘uncertainty in illness’.
Other studies have not reported how the relationship to the patient affects
uncertainty levels. The current study’s results, however, indicate this data is
worthy of collection and that special consideration should be given to parents of
patients in ICU at the time of transfer.
7.4.3 Question 2.3
Were patient and family member’ factors significantly related to STAI scores?
Factors related to anxiety in the current study included uncertainty as previously
discussed, and the level of social support. Receiving assistance from others is
thought to be a primary way to manage critical illness situations as it provides an
effective method for coping (Sherbourne & Stewart, 1991). This is supported by
the current study where participants with increased levels of social support had
reduced levels of state anxiety. The need for supportive relatives was also
reported in qualitative studies (Chen, 1990; Coulter, 1989) which described family

191
members’ need to discuss their concerns with others as a means of coping with the
situation. The ICU environment initially presents a foreign and threatening setting
and social support networks allow dependence upon others to interpret particular
events and treatments (Mishel, 1988) together with a means of protecting persons
from threatening outcomes (Mishel & Braden, 1987). McHale and Smith (1993)
suggest nurses use a family assessment tool to identify deficits in social networks
whereas McClowry (1992) suggests non-specified progressive family
assessments. Hayes (1990) who writes from an ICU perspective suggests the
simpler option of informing family members how to contact the social worker as a
way to address social support.
Authors have criticised studies that do not examine demographic factors such as
age and gender within their studies as they contend they may contribute
significantly to their experience (Holden et al., 2002). The current study, however,
did examine these factors and found that age was the only factor which achieved
close to an accepted level of significance (p = .059). Other authors report
however, that as family members’ age increased, their state anxiety reduced
significantly (Chartier & Coutu-Wakulczyk, 1989).
7.5 Question 3 Has the introduction of the intervention led to a reduction in the ‘uncertainty in
illness’ and state anxiety levels?
Analysis of the current study examined anxiety and uncertainty levels before and
after transfer. The after transfer mean levels of state anxiety and uncertainty

192
reduced for both the control and intervention groups following transfer to a
general ward. This is not unexpected, as one criterion for participation in the
study was that patients were recovering at the time of transfer. That is, the move
to a general ward was evidence of a positive progression in the wellness path for
participants. As predicted, family members recorded lower mean levels of anxiety
and uncertainty in the after transfer surveys. To test the value of the intervention
in reducing anxiety and uncertainty, comparisons were made of the mean values
of the control and intervention groups’ results. When statistically controlled for
pre-transfer anxiety scores there was no significant difference in anxiety after
transfer for participants in the intervention group. That is, both the control and
intervention groups had reduced anxiety and recorded similar levels to each other
after transfer. In this study, the intervention did not have an influence on reducing
anxiety levels which is perhaps understandable when one considers the critical
illness was not alleviated but merely showing signs of positive progression
enabling transfer to a general ward. Participants remained anxious (at a reduced
level) and having the ICU nurse explain an individualised transfer plan was
insufficient at reducing the complex phenomenon of anxiety.
The intervention group did have an obvious decline in ‘uncertainty in illness’
levels not seen in the control group whose uncertainty levels remained unchanged
after transfer. It was interesting to note that the control group levels of uncertainty
before and after transfer were almost identical whereas the intervention group
showed a distinct drop in uncertainty levels as previously stated. Although not
statistically significant, there was what may be seen as a suggestion of a clinically
significant drop in uncertainty levels in the intervention group. Discussion of

193
clinical significance as opposed to statistical significance is complex and requires
support from other research tools and assessment. As this study is the first of its
kind examining ‘uncertainty in illness’ where an intervention has reduced
uncertainty, it is not possible to draw on other research suggesting values which
could be viewed as clinically significant. It is nevertheless encouraging that
uncertainty levels reduced for those experiencing the structured pre-transfer
educational method of transfer and therefore warrants further research. A study
which also evaluated participants’ coping strategies along side ‘uncertainty in
illness’ levels would provide additional data for future discussion on clinically
significant changes in uncertainty levels.
The drop in uncertainty levels can be explained by Mishel’s theory of ‘uncertainty
in illness’ (1983) which postulates that consistent information from a credible
source (such as an ICU nurse) which is unambiguous and simplified to meet
individual levels of comprehension reduces uncertainty. The transfer brochure
encouraged and supported nurses to individualising information for family
members and the phraseology used was in plain English to enhance understanding
and reduce barriers, which can occur when medical terms are used. The small
effect size of the current study, however, is an indication that additional measures
could be incorporated into the transfer process to further reduce uncertainty.
Only two studies were located which have examined both state anxiety and
‘uncertainty in illness’ (Deane & Degner, 1998; Wong & Bramwell, 1992) and no
papers were found which examined the effect of an intervention on anxiety and
uncertainty. Although this necessarily limits discussion with previous research,

194
comparisons can be made with intervention studies which have examined one of
these factors.
Parallels can be made with a small study by Toth (1980) who also evaluated a
structured education pre-transfer programme. She measured anxiety levels using
measurements such as blood pressure, pulse and the Institute for Personality and
Ability Testing (IPAT) Anxiety Scale with 20 coronary care patients on the day
before and the day of transfer (control [n = 10], intervention [n = 10]). As in the
current study, Toth (1980) found there was no difference in anxiety levels as
measured by the psychological scale (IPAT) but there was a significant reduction
in the intervention group’s physiological parameters on the day of transfer. It
would have been of interest to further analyse participants’ anxiety levels once in
the general ward to ascertain the effect of the intervention after transfer. Further
comparison with the current study is limited, however, due to the different sample
and measuring tools in Toth’s study.
Interventions from a range of other studies have focussed on increasing
communication to reduce anxiety levels and have had mixed results (Bokinski,
1992; Bouvé et al., 1999; Halm, 1990; Poe, 1982; Raleigh et al., 1990). Bokinski
(1992) used a family conference (ICU nurse, ward nurse and family member) as
an intervention and measured family members’ anxiety before and after transfer
from a neuroscience ICU. A significant drop in anxiety levels occurred for the
intervention group following transfer in this study which was limited by its small
sample size (control group n = 9).

195
The use of information to reduce the effect of anxiety on patients and families
have revealed that family members’ anxiety levels are significantly higher than
those of patients (Raleigh et al., 1990; Russell, 1999a) which supports
interventions focussing on family members such as in the present study. The
current study and others (Halm, 1990; Raleigh et al., 1990) found an information
based intervention did not result in a significant drop in anxiety scores whereas
Poe (1989) saw a significant fall in state anxiety levels for patients post
myocardial infarct around the time of transfer. Poe’s small study (n = 16) is
reported with limited information on the data and analyses as the focus for the
article is on how nurses can improve communication with patients in the form of a
structured education plan. Further insight into reasons for the results is therefore
limited by a lack of information available to the reader.
It is suggested that transfer following a critical illness still constitutes a crisis
situation for family members. Feelings of worry, nervousness, and apprehension
continue (Halm, 1990; Saarmann, 1993) thereby retaining elevated levels of
anxiety. Yet it is understandable that, as found in the current study, there is a
significant drop in state anxiety for all participants after transfer as the move to a
general ward is tangible proof of an improved condition and sign of progress (Poe,
1982). Uncertainty levels will now be reviewed in relation to other studies in the
area.
Although there are a number of studies (Mishel, 1983a; Mishel 1983b; Mishel,
1988; Mishel, 1990; Mishel & Braden, 1987; Mishel, Padilla, Grant, & Sorenson,
1991; Mishel & Sorenson, 1991; Northouse et al., 1995; Wineman, Schwetz,
196
Goodkin, & Rudick, 1996; Wong & Bramwell, 1992; Yarcheski, 1988) using
Mishel’s framework (1981) to understand uncertainty, they all focus upon
defining, explaining, and testing relationships with other variables in various
populations rather than evaluating interventions. This is particularly interesting as
in general, studies (Mishel, 1981; Mishel, 1983a; Mishel, 1983b; Mishel, 1988;
Mishel & Sorenson, 1991; Nelson, 1996; Wineman et al., 1996) have reported
similar results confirming the principles of the theory. On a positive side, the
studies provide extensive evidence as a foundation for intervention studies thus
increasing the likelihood of effective outcomes.
‘Uncertainty in illness’ in the present study, as mentioned previously, did not drop
significantly for those experiencing the intervention when controlled for pre-
transfer uncertainty. The intervention group did, however, have an obvious
decrease in uncertainty not seen in the control group. That is, the control group’s
uncertainty levels remained unchanged whereas the intervention group saw a
definite (although not significant) decrease (Figure 6.2). It is encouraging that the
intervention may have benefited participants by decreasing uncertainty levels
which is consistent with the theoretical underpinnings of uncertainty. Mishel
(1988) highlights the importance of information relating to the illness within the
framework of reducing uncertainty along with the need for the information to
come from a credible source. ICU nurses are respected for their knowledge and
expertise (Holden et al., 2002; Meyer, 1992) and are therefore seen as an authority
to provide vital information to family members thus enhancing their
understanding of the situation and reducing uncertainty (Mishel, 1988).

197
Educational material in the form of brochures is advocated as an effective method
to support face-to-face communication (Brandenburg & Gifford, 1997; Henneman
et al., 1992; Henneman & Cardin, 1992; Shannon, 1973) as family members are
reported to forget information said to them in stressful circumstances (Odell,
2000; Robb, 1997). The brochure developed by the researcher for the current
study was designed to provide a framework based on recognised educational
principles to support nurses in their communication with family members about
transfer from ICU.
7.6 Question 4
7.6.1 Question 4.1
Has the introduction of the intervention led to an improvement in family
members’ satisfaction with regard to their information needs?
Family members’ needs during a critical illness in ICU have been reported
extensively in the literature for the past 25 years (Holden et al., 2002; Leske,
1992; Molter, 1979), however few studies have examined the level of satisfaction
with how their needs have been met. Consistently studies have documented
family members’ need for information and involvement in the transfer process
(Coyle, 2001; Micik & Borasi, 2002; Saarmann, 1993) and this was the focus for
the current study. Nurses have been identified as the person who best meets
family members’ need for information about transfer plans from the perspective of
both the family and ICU nurses’ (Quinn et al., 1996). As family members’
needs have been established, research focusing on investigating and testing

198
interventions aimed at meeting these needs should be instigated to provide
evidence for their implementation into clinical practice.
Results from the current study indicate that family members experiencing the
intervention were significantly more satisfied with the information given to them
by the ICU nurse than those experiencing the previous ad hoc transfer
information. The pre-transfer education intervention was designed to work as a
framework for the nurse to follow in their discussions with the family member.
This provided direction and facilitated communication and understanding as
points were discussed (Knowles, 1980). Educational interventions using brochures
designed without a nurse/family member interaction, have not reported significant
increases in family members’ satisfaction with information (Henneman et al.,
1992). Although other studies (Henneman et al., 1992; Kleinpell & Powers, 1992)
have examined the degree of family member satisfaction in regard to transfer
plans, they are not intervention studies and therefore have no control group for
comparison therefore making the results arbitrary and only relevant to their study
sites at that time.
7.6.2 Question 4.2 Has the introduction of the intervention led to an improvement in ICU nursing
staff communication with family members?
ICU nurses’ primary focus is patient care as the patient’s critical illness demands
constant nursing attention. Those who embrace an holistic approach to their
nursing, however, will be inclusive of family members as they understand the

199
general systems concept of the impact of family members upon the patient and the
patient on the family (McClowry, 1992). Family members try to maintain stability
within the dynamic environment of a critical illness as they adopt mechanisms to
enable homeostasis (Wright & Leahey, 1994). Communicating with family
members helps meet family members’ needs for understanding the situation as part
of their adaptive process (Mishel, 1988). As stated previously, however, nurses
state that they feel under-prepared to deal with family members (Benner et al.,
1999; Chaboyer et al., 2002) and some authors suggest they use avoidance
techniques to minimise their contact with them (Dunkel & Eisendrath, 1983; Fox &
Jeffrey, 1997).
Being prepared for discussing aspects of patient care with family members may
present difficulties in the busy schedule of ICU nursing (Chaboyer et al., 2002; Fox
& Jeffrey, 1997; Quinn et al., 1992). This, together with a lack of confidence in
coping with families may contribute to a lack of family involvement and
understanding of patient issues. The development of an interventional tool to assist
nurses with their communication is suggested as a positive way of supporting
nurses and family members as demonstrated in the present study.
The structure of the brochure allowed for an individualised approach to the
interaction as statements acting as prompts were listed on the brochure. For
example, one prompt for discussion was “Do you understand the plan of care for
your relative?” This was very broad and lent itself to an in-depth discussion should
family members have little idea of treatment plans. In fact, on a couple of
occasions, family members in the present study stated they had no idea of the plans

200
for the patient and the nurse organised a case conference with the intensivist, the
nurse and the family member to discuss the patient situation in depth. Without the
intervention this opportunity may have been missed.
The language level used for the brochure was set at eighth grade level of literacy as
suggested by Lange (1989) but demographic data of the educational level of
participants indicated that some of the sample did not have an educational standard
to that level (control n = 8; intervention n = 4). This would be of greater concern if
the brochure was a stand-alone intervention without the supplementation of face to
face communication and also assumes education occurs only in formal school
settings and not as part of life experience. The language level used appeared
appropriate as results from the intervention group scored significantly higher scores
in the item regarding understanding the language used by nurses. In addition, they
also felt they were told about transfer plans as they were being made significantly
more than those in the control group. Being told about transfer and understanding
the language used are recognised family needs (Molter, 1979).
7.6.3 Question 4.3
Has the introduction of the intervention led to an improvement in the overall
preparedness of family members for transfer?
Transfer from the security of ICU can be anxiety producing (Russell, 1999a;
Saarmann, 1993) as family members try to adjust to the thought of reduced staffing
levels (Roberts, 1976) and monitoring of patient observations (Jenkins & Rogers,
1995; Keogh, 2001), and altered expectations that accompany a move to a general
ward (Foss & Tenholder, 1993; Leith, 1999). Preparation for transfer should

201
commence early in the ICU stay to facilitate the adjustment to what is a natural
progression in most instances (Chaboyer et al., 2002; Reedy, 1993). This is not
always possible as in practice, transfers occur in response to demands on beds and
staffing levels. Therefore, it is suggested that an intervention which is structured
(Chaboyer et al., 2002), clear and easy to follow, allows nurses to plan a suitable
time to cover the material in the brochure to fit with patient care needs while family
members are visiting. The intervention in the present study was successful in
achieving this as evidenced by the significant difference in the way the intervention
group felt prepared for transfer as opposed to the control group. A strength of this
study was that family members were asked how well prepared they felt for transfer
when they were in the general ward. This permitted them to reflect on the situation
and as the brochure was individualised for them they could refer to it after the
initial conversation with the ICU nurse. Retention of information is problematic in
anxiety producing situations (Odell, 2000) and having the brochure to keep
provided key information discussed with the nurse for future reference (Scriven &
Tucker, 1997).
7.6.4 Question 4.4
Were family members’ worried or frightened by information given to them and
what was the information that caused this concern?
An opportunity to speak with the patient’s nurse about their condition is valued by
family members as they are regarded as the best providers of information (Deane
& Degner, 1998). One on one conversation with the bed-side nurse affords the
opportunity for family members to clarify and check on particular points which

202
concern them. Medical terms, proposed treatments and future therapies can be of
great concern to family members if they do not understand why they are
instigated and how they potentially will assist recovery. The intervention was
designed to incorporate the answering of family members’ questions and therefore
stimulate conversation with the nurse. As the nurse chose when the brochure
content was to be covered they would have planned a time outside usual patient
care activities thus allowing for a degree of dedication to the conversation. This
dedicated time was successful in improving communication for the intervention
group where 73.3% (n = 63) of the sample were not worried or frightened by
information given to them. This reflects the benefits of nurse/family discussion
focussed on the information needs of family members and may have contributed
to rapport building and family members feeling comfortable asking their
questions. An understanding that family members’ cognitive ability affects their
comprehension and retention in anxious situations (Deane & Degner, 1998) may
explain the fact that 26.7% (n = 19) of the sample found that some things were of
concern to them.
The present study supports the statement that ICU nurses need direction in regard
to the information family members need about the transfer from ICU. The ad hoc
method of transfer did not result in positive outcomes for family members who
wrote that they wanted information about the general ward. That is, some nurses
in the control group did not explain details of the new environment and nine times
more family members in the control group wrote that they were generally
apprehensive following conversations with the nurse about the impending transfer.
Needing to know a diagnosis is a fundamental need by family members (Molter,
203
1979) and their comments made on transfer about this may be explained in part,
by the nature of ICU admissions which include illnesses of unknown aetiology.
However, twice as many in the control group wrote this was a concern for them
thus indicating there may have been a problem with communication.
The structure of the intervention supported a methodical approach based upon
research about family members’ needs at the time of transfer. With the key
points to follow, the nurses were able to give family members the information
they needed but interestingly, there were still some family members who desired
more information. One comment highlighted the need for ICU nurses to be aware
of details of the wards to which they transfer. One nurse on staff did not know
what one of the wards specialised in and rather than offering to check for the
family member, she just said she didn’t know. In this case, the family member
went and found the ward and asked for information directly from the ward. This
is indicative of the definite need for information felt by families, however, other
family members may not have the confidence to seek out this information for
themselves. The following question asked family members for specific
information they would have like to have.
7.6.5 Question 4.5 What information did family members wish they had been told?
Literature suggests that in crisis situations, family members may use containment
as a means of reducing the impact of a potentially threatening situation
(McClowry, 1992) such as transfer from ICU (Saarmann, 1993). Authors suggest

204
families may try to cope with the threat by denying the severity of the situation
and particularly at the time of transfer, the prognosis for the patient. Family
members may try to cope by not asking questions or seeking help to meet their
needs (Daley, 1984; McClowry, 1992; Molter, 1979) which may be evidenced in
the present study’s control group where 25% of participants did not write any
comment regarding information they wished they had been told. This
interpretation is supported by a previous question’s result, which indicated that the
control group was not as well prepared for transfer as those who experienced
additional communication about transfer.
Those from the control group who commented stated they wanted basic
information about the transfer and the new ward. This has been written in the
literature as a fundamental need for families for the last two decades (Holden et
al., 2002; Molter, 1979) and for these needs to feature in the current study is
evidence that nurses are not proactive in meeting this fundamental need. Bouvé
et al. (1999) suggests this could be a result of ICU nurses’ extensive knowledge of
the transfer process making it easy for them to assume everyone has this
information. Alternatively, nurses may feel family members will ask if they want
to know but this has been challenged (Artinian, 1992; Cohen et al, 1988; Daley,
1984; McClowry, 1992; Molter, 1979). Whether family members request
information or not, some in the current study wrote that they felt there was a lack
of communication about transfer. As stated previously, the timing of transfers is
frequently when family members are not in attendance (Saarmann, 1993) which
may impact upon their questions about transfer.

205
7.7 Question 5 7.7.1 Question 5.1 What was the ICU nurses’ perception of their unit’s attitude to families and how
important were family members to patients’ recovery?
Family friendly ICUs are a result of an understanding of the importance and
interdependence of family members and patients (Cody, 1996; Friedmann, 1993;
Hayes, 1990). They promote family involvement in patient care and an openness
to visitors (Benner et al., 1999) as they value family members’ ability to orientate
(Dyer, 1995) and offer material support to the patient (Dunkel & Eisendrath,
1983). Family members assist the nursing staff to know the patient better (Dunkel
& Eisendrath, 1983) and help plan for on-going care and are thus an essential
component of critical care nursing. The current study showed that 100% (n = 33)
of the ICU nurses believed their unit’s attitude to family members was positive
and concurred with authors who agree that family members are important to
patients’ recovery (Leske, 1992). However, in practice, nurses’ attitudes are not
always reflected in their actions. As the researcher collected the data for this
study she observed strict visiting hours enforcement with family members told not
to come before eleven o’clock next morning as doctors’ ward rounds occur and
because it was a very busy period for nurses. Only in exceptional circumstances
was this practice varied. This lends support to the need for further education with
resultant policy change to support congruency between what nurses espouse and
clinical practice.

206
7.7.2 Question 5.2 What was the ICU nurses’ perception of the level of importance of the process
of transfer from ICU for families?
Research studies indicate ICU nurses perceive family members’ need for
information as less important than do the family members themselves (Kleinpell
& Powers, 1992; Lynn-McHale & Bellenger, 1988; O’Neill Norris & Grove,
1986). This is a significant finding when one considers nurses respond to family
members’ needs based upon their perception of what is required (Kleinpell &
Powers, 1992). When nurses’ perception and reality are not congruent there is
the possibility that nurses are focussed upon meeting inappropriate family
members’ needs.
Nurses in the current study considered the transfer process for families was
important. This assessment is confirmed by previous studies where family
members rate the transfer process as an important aspect from their perspective
(Kleinpell & Powers, 1992; Lynn-McHale & Bellenger, 1988; O’Neill Norris &
Grove, 1986). This is a promising situation as researchers suggest that when
nurses understand family members’ needs the introduction of interventions
directed at meeting these needs are supported (O’Neill Norris & Grove, 1986).
7.7.3 Question 5.3 Has the intervention provided a useful means to improve discussion with family
members from ICU nurses’ perspective and would they recommend its use?

207
The structured pre-transfer intervention was successful in promoting discussion
about transfer with family members. The nurses considered it provided a useful
framework for this discussion as it had a sequence of prompts which all nurses
followed. Logical sequence and written information to both reinforce the spoken
word, and keep for future reference, are suggested as ways for family members to
retain information (Deane & Degner, 1998; Scriven & Tucker, 1997). ICU nurses
who are busy with patient care needs are thus supported by having a framework
to follow without having to pre-plan the transfer discussion. The points listed
incorporate important family member information needs and are therefore not
reliant on the perception of individual nurses to family members’ needs. This
will only occur, however, if the nurse follows the prompts as outlined and does
not skip any points. It needs to be reinforced that many family members will not
ask questions for a variety of reasons already discussed (Daley, 1984) thus a
structured programme is advocated (McClowry, 1992). The nurses’ need for
assistance with the planning for transfer was evident in the current study by their
overwhelming promotion of the intervention for all transfers from the unit. That
is, nurses in the current study recommended the introduction of the structured pre-
transfer education process for all transfers from ICU.
7.8 Study’s findings in relation to Conceptual Framework The findings from this study can be readily linked to the Conceptual Framework
developed by the researcher having engaged with the literature. ‘Uncertainty in
illness’ has not previously been reported in a cohort of ICU family members thus
the present study significantly adds to existing knowledge of uncertainty. The
findings confirm the existence and relationship between state anxiety and
‘uncertainty in illness’ for family members around the time of transfer from ICU.

208
Socio-demographic characteristics such as the level of social support and
unexpected nature of the admission, are significant factors in how family members
experience transfer from ICU. The use of a structured pre-transfer education
method improved family members’ satisfaction with transfer as predicted.
Although anxiety was not reduced by the intervention the reduced levels of
‘uncertainty in illness’ support the undertaking of future research in this area.
This current study has added further depth and added clarification to the existing
knowledge of family members around transfer and supports the General System
Theory (von Bertalanffy, 1973) which claims that when one family member is
affected, all family members are affected and attempt to maintain stability within
the dynamic environment as they adopt mechanisms to enable homeostasis
(Wright & Leahey, 1994).
7.9 Limitations There are several limitations to this study. These are related to sampling,
reliability, and data collection procedures. A limitation of this study is the
restricted ability to generalise the findings to the entire population of ICU family
members due to participant selection criteria and the single study site. The
selection criteria included only those patients who were improving at the time of
transfer and therefore findings must be evaluated and discussed from this
perspective where family members may well be less anxious and uncertain as the
patient’s condition is improving. The high proportion of patients were elective
surgery cases which also may have impacted upon the anxiety and uncertainty
levels of family members. All participants were drawn from one study site and
although it was a large public hospital it may have had particular sample

209
demographics not representative of the entire ICU population which extends into
the private health sector and large regional centres.
While two of the instruments used in this study were selected as relevant to the
present study, and they were reported to have high reliability and validity, they
had not previously been used in an ICU population. There may be variations
between the present population and the population where these instruments have
been developed and tested. The researcher developed family members’
satisfaction with transfer questions for the purposes of the present study by using a
literature review and data from Phase One of the study. However, inter-item
correlation was low for the communication factor and thus items had to be
considered individually. Further validity and reliability testing is an important
future consideration should this instrument be used in other populations.
The researcher who collected all the data for the study, was not employed by the
hospital. Although this is a strength in the area of consistency in data collection
methods, it may have influenced participant responses as they perceive the
research to be removed from their hospital experience. There were no previous
studies found similar to the present study where interventions had been tested.
This restricted comparisons and contrasts with the current study and therefore
replication of this study is required.
Chapter 8 summarises the major findings from the current study and discusses
implications for the future. These will be divided into the area of future research,
education and clinical practice.

210
CHAPTER 8: CONCLUSIONS
8.0 Introduction The purpose of this study was to improve the experience of transfer from ICU for
family members and ICU nurses. A structured pre-transfer educational process to
individualise and improve communication between nurses and family members
was developed and evaluated by way of the following research questions.
Question 1: What was the level of ‘uncertainty in illness’ in family members
before transfer from ICU as measured by Mishel’s PPUS-FM Scale?
Question 2.1 Was there a relationship between family members’ ‘uncertainty in
illness’ as measured by PPUS-FM (Mishel, 1997) and anxiety
levels as measured by STAI – state (Spielberger et al.,1983)?
2.2 Were patient and family member’ factors significantly related to
PPUS-FM?
2.3 Were patient and family member’ factors significantly related to
STAI – state scores?
Question 3. Has the introduction of the intervention led to a reduction in the
‘uncertainty in illness’ and state anxiety levels?
Question 4.1 Has the introduction of the intervention led to an improvement in
family members’ satisfaction with regard to their information
needs?
4.2 Has the introduction of the intervention led to an improvement in
ICU nursing staff communication with family members ?
4.3 Has the introduction of the intervention led to an improvement in
the overall preparedness of family members for transfer?

211
4.4 Were family members’ worried or frightened by information given
to them and what was the information that caused this concern?
4.5 What information did family members wish they had been told?
Question 5.1 What was the ICU nurses’ perception of their unit’s attitude to
families and how important were family members to patients’
recovery?
5.2 What was the ICU nurses’ perception of the level of importance of
the process of transfer from ICU for families?
5.3 Has the intervention provide a useful means to improve discussion
with family members from ICU nurses’ perspective and would they
recommend its use?
In order for these questions to be answered, the Phase Three methodology
employed was a quantitative quasi-experimental pre-test, post-test non-equivalent
control group design with a four phase plan. Phase One data were obtained from
family members of patients discharged from ICU and from a panel of expert
critical care nurses. The expert panel considered that family members needed
information regarding the intended plans for transfer together with information
about the new ward and its different staff. The expert panel also considered
information on the different expectations in the general ward was important for
family members to have explained to them. Finally, they considered information
relating to the support systems available to family members needed to be
highlighted with contact details written down.

212
The family members surveyed wanted information on the geographical location of
the ward, contact details of the general ward and the names of the doctors caring
for the patient. Details about the future treatment and prognosis were very
important to them.
The data from Phase One informed the content for the development of the
educational brochure which comprised Phase Two of the study. Three teachers
provided feedback to ensure the language and level of literacy were congruent
with an eighth grade student level. Senior hospital personnel reviewed the draft
brochures before final production of the brochure.
Phase Three had a pre-test, post-test design which evaluated the impact of a
structured pre-transfer educational method on family members with relatives
transferred from ICU. Phase Four evaluated ICU nurses’ perception of the
usefulness of the structured pre-transfer educational method in supporting the
transfer process. This chapter highlights the major findings of this study and
outlines conclusions drawn from this research with suggestions for future
direction.
8.1 Research questions A critical illness requiring ICU nursing is universally understood as a traumatic
event for patients. Family members of ICU patients have more recently been
accepted as legitimate recipients of nurses’ attention. ICU research centred on
family members has been developing over the past two decades and has focussed
on the identification of their needs. Few studies have examined if family
members’ needs are met and still fewer have evaluated interventions designed to

213
meet family needs. The following section outlines conclusions drawn from the
current research intervention in relation to each of the five research questions.
8.1.1 Question 1
What was the level of ‘uncertainty in illness’ in family members before transfer
from ICU as measured by Mishel’s PPUS-FM Scale?
This study is unique in its investigation of ‘uncertainty in illness’ in ICU family
members. It reports mean levels of 77.22 and 78.93 which are equivalent to those
of smaller undescribed studies of ICU family members (Mishel, 1997) and lower
levels than husbands of wives who had recurrent breast cancer (Northouse et al.,
1995). While Northouse et al.’s study reported higher scores, this was argued to
relate to the sampling method and gender bias of the all male participants, together
with the different nature of the illness situations. The current study documents
levels of uncertainty in ICU family members and supports the need for nurses to
be knowledgeable about this psychological factor and ways it can be reduced.
8.1.2 Question 2 Question 2.1 Was there a relationship between family members’ ‘uncertainty in
illness’ as measured by PPUS-FM (Mishel, 1997) and anxiety
levels as measured by STAI – state (Spielberger et al., 1983)?
A significant relationship was found to exist between state anxiety and
‘uncertainty in illness’, thus reporting for the first time the link between these two
psychological factors in family members in ICU. The state anxiety scores
accounted for 24.3% of the variance of ‘uncertainty in illness’ scores and as the

214
anxiety scores increased so did the uncertainty scores. This result is congruent
with studies of women with breast cancer (Wong & Bramwell, 1992) and breast
surgery (Deane & Degner, 1998). Documentation of this direct relationship assists
future research direction in this area as does an understanding of factors
significantly related to uncertainty and anxiety.
Question 2.2 Were patient and family member’ factors significantly related to
PPUS-FM?
Three variables were found to be significantly related to ‘uncertainty in illness’.
The first was state anxiety as discussed in Question 2.1. The second factor related
to when an admission to ICU was unexpected. When admission was unexpected,
‘uncertainty in illness’ was significantly increased. This relationship is
predictable when one considers the immediate admission period but highlights
that at the time of transfer from ICU, heightened feelings of uncertainty continue
for family members. ICU nurses’ understanding of this relationship allows for
particular attention to be given to this sub-group of the ICU population who may
adopt adverse coping strategies as a result of high uncertainty levels (Mishel,
1997).
The third factor significantly related to uncertainty was the nature of the
relationship to the patient. When the family member was the parent of the patient
as opposed to the child, their level of uncertainty was significantly higher. This
reflects the protecting role adopted by parents as they endevour to keep their
children safe from harm. An understanding of this group’s heightened level of
uncertainty may assist nurses in supporting parents as they grapple with the

215
situation of a critical illness in their offspring. It was also highlighted in the
Discussion Chapter that the parents of critically ill children in this study were also
not anticipating the admission to ICU and therefore this factor may well have
compounded their ‘uncertainty in illness’ levels.
Question 2.3 Were patient and family member’ factors significantly related to
STAI – state scores?
One factor (other than ‘uncertainty in illness’) significantly affected the state
anxiety scores. This factor was the level of social support experienced by family
members in this study. Those with higher levels of social support had lower
levels of anxiety thus supporting the notion that assistance from a personal support
system provides an effective method of coping during a critical illness situation.
This highlights the fact that family members with few mechanisms for accessing
personal social support may benefit from an ICU based social support system.
Communication with family members regarding their social support opportunities
would be advantageous in initiating first contact with alternative social support.
8.1.3 Question 3.
Has the introduction of the intervention led to a reduction in the ‘uncertainty in
illness’ and state anxiety levels?
The intervention of an individualised structured pre-transfer process conducted by
the bed-side nurse did not significantly reduce the anxiety or uncertainty when
pre-transfer scores were taken into account. The stimulus, the critical illness,
continued to exist at the time of transfer, and this created anxiety about the future

216
in spite of improved levels of information and communication. There was,
however, a reduction of uncertainty for the intervention group not seen in the
control group. Although not statistically significant, there was what may prove to
be a clinically significant drop in uncertainty levels. This was encouraging and
supports this study’s Conceptual Framework and Mishel’s theory on ‘uncertainty
in illness’ (1988). In addition, the results justify additional research designed to
reduce uncertainty by improving the level of understanding by family members.
Additional data collection and analysis of family members’ coping strategies to
further investigate what a clinically significant drop in uncertainty levels may be,
is endorsed.
8.1.4 Question 4 Question 4.1 Has the introduction of the intervention led to an improvement in
family members’ satisfaction with regard to their information
needs?
4.2 Has the introduction of the intervention led to an improvement in
ICU nursing staff communication with family members ?
4.3 Has the introduction of the intervention led to an improvement in
the overall preparedness of family members for transfer?
4.4 Were family members’ worried or frightened by information given to
them and what was the information that caused this concern?
4.5 What information did family members wish they had been told?
The conclusions from Research Question 4 will be stated collectively. From the
family members’ perspective, the intervention significantly improved their

217
satisfaction with having their information needs met. Information needs are a
fundamental need expressed by family members and are integral to their
understanding and coping with transfer from ICU (Leske, 1992). This study
utilised a structured pre-transfer method of transfer for ICU nurses to follow
which significantly improved the transfer experience for family members. Few
studies have measured whether information needs have been met therefore this
study fills a gap in research by rigorously evaluating the efficacy of a nursing
intervention with a sample of 162 family members and 40 ICU nurses.
It is suggested that family information needs were met in the current study by
improving the level of communication between the bed-side nurses and family
members by providing support and direction to the ICU nurse. The intervention
group recorded significantly higher levels of communication than did the control
group who had significantly more concerns and worries about the information
given to them in the pre-intervention period where ad hoc transfers occurred. An
overall assessment by family members experiencing the intervention confirmed
they felt significantly better prepared for transfer than those who did not
experience the intervention. Whether being better prepared for transfer
extrapolates to positive coping strategies and decision- making ability was beyond
the scope of this study but is worthy of future research activity.
The inclusion of qualitative data in this study strengthens its interpretive ability as
it gives insight into the meaning behind some quantified results which by their
very nature, are limiting. The intervention group was less worried by information
given to them by the bed-side nurse before transfer and recorded more participants

218
who felt they had been given sufficient information about transfer than did the
control group. The intervention proved to have positive outcomes in relation to
the type of information participants wished they were told with the majority of the
intervention group (63.4%) considering they had been given adequate information
in contrast to the control group (38.7%) who recorded a number of information
deficits. Therefore, when one examines the information needs of family members
one can conclude that the structured pre-transfer method of transfer was
successful in providing relevant information to family members in a way they
could understand.
8.1.5 Question 5 Question 5.1 What was the ICU nurses’ perception of their unit’s attitude to
families and how important were family members to patients’
recovery?
5.2 What was the ICU nurses’ perception of the level of importance of
the process of transfer from ICU for families?
5.3 Has the intervention provide a useful means to improve discussion
with family members from ICU nurses’ perspective and would they
recommend its use?
The conclusions from Question 5 will also be presented together. The nurses
considered their ICU had a positive attitude towards family members and
considered the transfer process to constitute an important event for families. Such
an environment supports the recognition of the important part family members

219
play in patient recovery and this positive attitude needs to be encouraged and
capitalised upon with family centred interventions.
The success of the intervention extended beyond the perspective of family
members and included a positive outcome for ICU nurses who used the structured
pre-transfer method. ICU nurses found it helpful in supporting the
communication with family members with 96.8% indicating it provided a useful
framework for them to use and 94% recommended its introduction for all transfers
from ICU. These are impressive results and are indicative of the need for ICU
nurses to be supported in their role of transferring patients and family members. It
suggests those who have used it think highly of the intervention, which increases
the likelihood of its adoption into unit protocols and its subsequent use for all
transfers.
8.2 Future direction In order to support clinical practice and encourage further research and education
in family centred nursing in ICU the following recommendations are proposed.
8.2.1 Recommendations for practice
This study and others over the past two decades have shown that family members
need to be included in the plans for transfer from ICU. These studies’ findings
need to be embraced by ICU nurses who are seen as the best person to discuss the
transfer plans with family members. The current study’s results suggest the
introduction of a structured pre-transfer educational method for family members
as it has been shown to:
• improve communication with families,

220
• prepare family members for transfer, and
• provide a structured and effective framework for nurses to follow in order
that they meet the family members’ needs.
In addition, results suggest that there are three sub-sets of the ICU population with
additional needs. These include those family members who unexpectedly have a
relative admitted to ICU, those who are parents of the patient, and those with little
or no social support. In view of the research findings, it is recommended that ICU
nurses pay particular attention to the needs of family members within these three
categories in an attempt to reduce their uncertainty and anxiety and allow them to
better cope with the situation of transfer from ICU.
8.2.2 Recommendations for education Educational opportunities which arise from this research include the need to
encourage clinical practice which reflects current rhetoric on the importance of
family members to patients. That is, positive family friendly attitudes and beliefs
need to be congruent with clinical practice. By highlighting ways positive
attitudes can be demonstrated by ICUs is just one aspect of nurse education which
could produce positive results. Furthermore, an understanding by nursing staff of
the importance to patients of meeting family members’ psychosocial needs may
well assist them in accepting this as part of their role. This can be approached by a
variety of ways on a local level such as by the provision of an experienced nurse
peer mentor who role models positive family orientated nursing care. In addition,
in-service education, ward based article reviews, and posters with evidence-based
research outcomes concerning family needs are other strategies which can
highlight family issues. The importance of family members’ specific information
needs, including transfer planning, should be incorporated as an essential

221
component of new staffs’ orientation to ICUs together with unit protocols which
incorporate transfer planning. At this time, the new staff would have the
opportunity to develop an understanding of the unit’s philosophy and application
of family friendly practices with the provision of a peer mentor who would
provide additional ongoing support of the clinical application of family centred
nursing.
Educational links with other ICUs through such technologies as video or tele-
conferencing provides the opportunity for ICUs to encourage peers by sharing
strategies of family friendly practices beyond the context of a single ICU. This
interaction could foster collective participation from ICU nurses.
A broader perspective on enhancing education about families for nurses would
include consideration of existing specialist courses. Post-graduate critical care
programmes which include evidence-based research on the impact of families on
patients, support the principles of holistic nursing in ICU. Such programmes
would include not only the importance of the family to the patient, but also the
importance of nurses striving to identify and meet family needs as part of their
care of the patient. Nurses report they feel under-prepared to meet the needs of
families (Chaboyer et al., 2002; Fox & Jeffrey, 1997; Scullion, 1994) and are thus
highlighting to educators, deficits in their knowledge and practice base which
needs to be addressed.

222
8.2.3 Recommendations for research Few studies examined were interventional in nature, therefore limiting the
comparisons and contrasts with the current study. Replication of this study is
therefore recommended to provide additional evidence. The following
recommendations for future research are made to further explore the
psychological factors of anxiety and ‘uncertainty in illness’ in ICU family
members.
• Repeating the present study in a paediatric ICU is advocated as the data
suggested parents of patients may require special consideration due to their
increased ‘uncertainty in illness’ levels.
• A similar study using a multi site design would further increase the
generalisability of the findings and provide additional evidence from
which conclusions may be drawn.
• Coping strategies, according to Mishel’s theory of ‘uncertainty in illness’,
are compromised with high levels of uncertainty. Therefore, studies which
test interventions against ways people cope would add a further dimension
incorporating the concept of clinically significant results as opposed to the
statistical significance of uncertainty levels.
• A study designed to incorporate on-going planning for transfer using
current bed-side computer based technology to track information given to
family members as an adjunct to the structured pre-transfer educational
method is suggested as a way to further support family members and
nurses who work in a technologically advanced environment.
• A study which extends the scope of the current study by adding a visit
from an ICU nurse the following day in the general ward to follow up on

223
any issues arising from the transfer from ICU is suggested to further
improve outcomes.
• The current study was limited to those patients who were improving at the
time of discharge which excluded those families whose relative was
leaving ICU for palliative care. The needs of these families could well be
quite different to those in the current study and a project dedicated to
improving outcomes for these family members and patients is worthy of
investigation.
• The current study also excluded those family members who could not read
and write English. Another study designed to meet the information needs
of this sub-sample would expand the current understanding of family
needs around transfer and offer support to those who may well feel
alienated by language.
8.3 Summary This chapter has outlined the major findings from the study and drawn
conclusions from the results of the research questions. The study recorded for the
first time the level of ‘uncertainty in illness’ for family members in ICU before
and after transfer. This provides baseline data for future study comparisons as the
research method incorporated a control group who experienced ad hoc transfer
methods and an intervention group who had a structured transfer process.
Anxiety levels were not affected in this study by the method of transfer however,
results were encouraging as ‘uncertainty in illness’ in the intervention group
recorded reduced levels than those seen in the control group. The intervention

224
proved to be very successful from the perspective of family members’ satisfaction
with transfer. Family members experiencing the structured pre-transfer method
were significantly better prepared for transfer and recorded significantly higher
levels of satisfaction with having their information needs met than those who
experienced ad hoc transfers.
Almost exclusively (96.8%), the ICU nurses found the structured pre-transfer
method to be supportive and helpful when transferring patients and family
members from ICU. They recognised their need for help in transferring patients
and family members from ICU and 94% recommended the introduction of the
intervention for all future transfers. This result indicates that when the intervention
is introduced into the unit there will be universal support for its implementation as
they acknowledge the benefits it brings both family members and themselves.
Suggestions for further research and recommendations for clinical practice and
education have been outlined and include amongst others, replication of the study
either in a paediatric or multi-site setting. In the area of education, it is suggested
that post-graduate courses require further emphasis upon addressing the needs of
families in ICU and ICU practices need to accurately reflect the important part
family members contribute to the health and recuperative ability of patients. This
is supported by the notion that the single most contributing factor to one’s health
is one’s family (Friedman, 1998).

225
Appendices
Appendix A – Expert Panel Information and Consent Form Phase One – Invitation, information letter and consent form for registered nurses
to join the expert panel.
Queensland University of Technology Letterhead
Investigator: Marion Mitchell
School of Nursing, Queensland University of Technology Telephone: 07 3382 1225 Email: [email protected]
Title: Family outcomes following client transfer from an Intensive Care Unit: an
educational intervention.
I am writing to invite you to become a member of an expert panel that will be formed to provide advice and guidance for this research study which seeks to improve critical care nursing practice during the transfer of families and patients from an intensive care unit to general wards. This study is the basis of a dissertation in the degree of Doctor of Philosophy at QUT and will be performed by Marion Mitchell under the guidance of an academic staff member, Professor Mary Courtney. The research study
This research study seeks to improve and gain additional understanding of the transfer process from the perspective of family members of critically ill patients. Purpose of the research This project aims to: 1. collaborate with relatives and nurses to determine relevant transfer
information requirements 2. examine the concept of uncertainty for relatives as it relates to the transfer
process of intensive care clients 3. produce a client and family focused educational brochure, which is
informative and easy to read 4. provide a structured pre-transfer process to facilitate dialogue and
information sharing with family members and nursing staff 5. determine the efficacy of the intervention in reducing family anxiety and
uncertainty following transfer 6. measure the relative’s level of satisfaction with the transfer process

226
7. evaluate the benefits of a structured pre-transfer method as perceived by intensive care nurses.
Duration of the participant’s involvement As a member of the expert panel, your participation in this project will involve two parts. 1) The first component involves your completion of the questionnaire which is
attached. The questions relate to your opinions and ideas relating to the process of transfer. This should take no longer than ten minutes to complete. The data will be collated by the researcher.
2) The second component of your participation involves an invitation for you to meet with the researcher and others in the expert panel to discuss the issues raised. The Sydney World Congress for Critical Care in October provides an opportunity to bring the group together to prioritise the information you have given on the questionnaire responses. This session will take no longer than one hour. The results from this discussion, together with data being collected from relatives, will form the basis for an educational brochure being developed by the researcher.
Participation in this project is voluntary and you may elect to withdraw at any time without comment or penalty. A decision not to participate, or to withdraw, will have no impact upon any involvement you may have with Queensland University of Technology or Griffith University and will not affect your employment. Possible material risks to participants Participation in this project does not involve any known risk to the participants. However, should you feel any discomfort or distress completing the questionnaire please contact the researcher. Should you feel any discomfort or distress during the focus group discussion, the researcher, will close the discussion. Benefits that may result from the research
1. Relatives better prepared for transfer 2. Improved relative’s satisfaction with transfer method 3. Reduction in relative’s anxiety 4. Understanding of the level of uncertainty in relatives
Other benefits that may result are: • Establishment of a structured pre-transfer educational method for the clinical
area • Participation of critical care nurses in the research process, • Increased collaboration between practitioners and researchers and • A greater awareness by critical care nurses of the needs relating to transfer of
family members of critically ill patients. Confidentiality of the data Only the researcher will know the identities of the participants. All summaries of the questionaries and the focus group meeting will be kept in a locked filing

227
cabinet and only the researcher will have access to them. No identifying information about the participants will be used in any paper that may result from this research. Questions or concerns You are welcome to contact Marion Mitchell regarding any questions or concerns you may have about this research study. If at any time you are not satisfied with this response you may contact Associate Professor Helen Edwards, Head of School of Nursing on 07 3864 3844. Should you have any concerns relating the ethical conduct of this research please feel free to contact the Secretary of the University Human Research Ethics Committee on 07 3864 2902. The study has also been approved by the Princess Alexandra Hospital Research Ethics Committee and a representative may be contacted on 3240 5856. Feedback to participants Feedback will be provided to participants in this study, initially through the focus group discussion, and subsequently via group email and publications. Instructions for return of questionnaire
The stamped self-addressed envelope may be used for returning the questionnaire and consent form. I thank you for your consideration of this research project and I look forward to hearing from you soon. Kind regards Marion Mitchell.
228
Consent Form Phase One – Expert Panel.
Queensland University of Technology Letterhead
Researcher: Marion Mitchell QUT, School of Nursing Telephone: 07 3382 1225 Project title: Family outcomes following client transfer from an Intensive Care Unit: an educational intervention The investigator conducting this research project abides by the principles governing the ethical conduct of research and, at all times, avows to protect the interests, comfort and safety of all participants. This form and the accompanying participant information package have been given to you for your own protection. They contain an outline of the study and possible risks. Your signature below will indicate that; 1. you have received the subject information package and have read its
contents; 2. you clearly understand the nature of the study and the possible risks
involved; and that you have been given the opportunity to discuss the contents of the Participant Information Package with the investigator prior to the commencement of the study;
3. you understand that all the data which you have provided will only be revealed to the investigators. When the results of the study are published you will remain anonymous;
4. your participation is voluntary and therefore may be terminated at any moment by you without comment or penalty, and without jeopardising your involvement with the Queensland University of Technology or Griffith University;
5. you may direct any inquiries and further questions to Marion Mitchell at the School of Nursing, Griffith University on 07 3382 1225. You may also direct complaints and concerns regarding the ethical conduct of this investigation to the Secretary of Queensland University of Technology Research Ethics Committee, on 07 3864 2902. A representative of the Princess Alexandra Hospital Research Ethics Committee may also be contacted on 07 3240 5856.
6. you will receive feedback on your results at the end of the session, via email and by way of publications;

229
7. you agree to participate in the study as set out in the Subject Information Package for the research project entitled “Family outcomes following client transfer from an Intensive Care Unit: an educational intervention” as part of a postgraduate thesis for a Doctor of Philosophy for Marion Mitchell.
Registered Nurse: ______________________________ Date: ____________
Witness: ______________________________________ Date: ____________
Print Name: ___________________________________
I have explained the nature and purpose of this study to the above participant and
have answered their questions.
Investigator: ___________________________________ Date: _____________

230
Appendix B: Expert Panel Questionnaire Instructions: 1. Please circle your responses by choosing one answer per question. 2. After you have completed the questionnaire, please place it in the envelope
supplied and return it to the researcher. 1) From your experience, are relatives included in transfer plans of their family
member moving from ICU to the general ward as plans are being made? 1 2 3 4 5
always sometimes not sure hardly ever never
2) How would you rate your unit’s current transfer procedure for critical care patient’s relatives? 1 2 3 4 5 excellent quite good not sure not very good poor
3) How would you rate your hospital’s attitude to family members?
1 2 3 4 5 excellent quite good not sure not very good poor
4) How important are family members to critically ill patient’s recovery? 1 2 3 4 5
not important slightly important not sure important very important
5) In your experience, do close relatives accompany their family member upon
transfer to general wards? 1 2 3 4 5 always sometimes not sure seldom never 6) How important is it for relatives to know the number of patients per room in the
general ward? 1 2 3 4 5
not important slightly important not sure important very important
7) How important is it for relatives to have access to phones in the general ward?
1 2 3 4 5 not important slightly important not sure important very
important 8) How important is it for relatives to know the nurse:patient ratios in the general
ward? 1 2 3 4 5
not important slightly important not sure important very important

231
9) How important is it for relatives to understand patient expectation by the nurses in the general ward?
1 2 3 4 5 not important slightly important not sure important very important
10) In your experience, do close relatives know that a different health care team (nurses and doctors etc.) will be caring for their family member in the general ward?
1 2 3 4 5 always sometimes not sure seldom never 11) What information do you consider is important for family before their relative
is transferred from the ICU to a general ward? Please list. ………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
Focus Group Arrangements: I am willing to attend the focus group during the 8th World Congress in Sydney in October. Yes ❐ No ❐ The researcher will contact you closer to the time to provide details of the time and place for the focus group meeting during the 8th World Congress of Intensive Care Medicine. Please complete your contact details: phone ……………………., and/or E-mail address …………………………
Thank you for completing this questionnaire. Please place the completed
questionnaire and signed Consent Form in the stamped self-addressed envelope provided and return it to the researcher.

232
Appendix C: Phase One Information for Family Members.
Queensland University of Technology Letterhead
Investigator: Marion Mitchell School of Nursing, Queensland University of Technology Telephone: 07 3382 1225 Email: [email protected]
Project Title: Family outcomes following client transfer from an Intensive Care
Unit: an educational intervention.
The researcher invites you to participate in a study which seeks to improve the critical care nursing practice during the transfer of families and patients from the intensive care unit to general wards. This study is the basis of a degree of Doctor of Philosophy at Queensland University of Technology and will be performed by Marion Mitchell under the guidance of an academic staff member, Professor Mary Courtney. The research study
This research study seeks to improve and gain additional understanding of the transfer process from the perspective of family members of critically ill patients. Purpose of the research The project aims to: 1. gain information about the transfer of relatives and their loved ones from
Intensive Care to the general ward 2. improve the transfer process for relatives Duration of your involvement Your participation in this project will involve filling out a survey form which is attached. The questions relate to your opinions and experiences about the transfer from intensive care to the general ward. The survey should take no longer than ten minutes to complete. The results from these surveys will provide important information for the researcher who is developing a brochure to improve the transfer process for relatives. Participation in this project is voluntary and you may elect to withdraw at any time without comment or penalty. A decision not to participate, or to withdraw, will have no impact upon your relative’s present or future care in any way. The ward nurses have no involvement in this project.
233
Possible material risks to participants Participation in this project does not involve any known risk to the participants. However, should you feel any discomfort or distress completing the survey form please contact the researcher. The social worker or pastoral care officer is available if you would like to talk to someone. You may contact them by phoning switch on 3240 2111 if the need arises. Benefits that may result from the research
1. Relatives better prepared for transfer 2. Improved relative’s satisfaction with transfer method
Confidentiality of the data Only the researcher will know the identities of the participants. All summaries of the surveys will be kept in a locked filing cabinet and only the researcher will have access to them. No identifying information about the participants will be used in any paper that may result from this research. Questions or concerns You are welcome to contact Marion Mitchell regarding any questions or concerns you may have about this research study. If at any time you are not satisfied with this response you may contact Associate Professor Helen Edwards, Head of School of Nursing on 07 3864 3844. Should you have any concerns relating the ethical conduct of this research please feel free to contact the Secretary of the University Human Research Ethics Committee on 07 3864 2902. The study has also been approved by the Princess Alexandra Hospital Research Ethics Committee and a representative may be contacted on 3240 5856. Instructions for return of questionnaire The stamped self-addressed envelope may be used for returning the survey. Alternatively you can place your completed questionnaire in the envelope and give it to the ward receptionist who will forward it to the researcher. Thank you for your consideration of this project and I look forward to receiving your comments. Kind regards Marion Mitchell.

234
Appendix D: Phase One Family Members’ Questionnaire
Instructions: please indicate your response to the following questions by circling one answer per question.
Not Im
portant
Slightly
Not Sure
Important
Very Im
portant
How important are the following : (1) To have an understanding of the ward name and
location before your loved one is transferred?
1
2
3
4
5
(2) To know the general ward’s phone number before your relative is transferred?
1 2 3 4 5
(3) To know the number of patients each nurse has to care for in the general ward before your relative moves there?
1 2 3 4 5
(4) To know the general ward visiting hours before your relative moves there?
1 2 3 4 5
5) To know the name of the doctor caring for your relative in the new ward?
1 2 3 4 5
(6) To know the number of patients per room in the general ward before your relative moves there?
1 2 3 4 5
(7) To be included in the transfer process as plans are being made to move your relative out of Intensive Care?
1 2 3 4 5
(8) To be informed, prior to transfer, about the expected outcome of your relative’s illness?
1 2 3 4 5
(9) To be informed, prior to transfer, about the proposed treatments for your relative?
1 2 3 4 5
(10) In your experience, are families considered important within this hospital?
1 2 3 4 5

235
(11) In your experience how often do staff use everyday language when speaking to you? Please circle one response.
1 2 3 4 5
all the time sometimes not sure seldom never
(12) What information do you consider important to have prior to your
relative’s transfer from the Intensive Care Unit to the ward?
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
Thank you for completing this questionniare. Please place the completed questionniare in the self-addressed, stamped envelope provided and either give it to the ward receptionist or mail it to the researcher.

236
Appendix E: Pre-Transfer Brochure

237

238
Appendix F: Phase Two - Information for Teachers.
Queensland University of Technology Letterhead
Investigator: Marion Mitchell
School of Nursing, Queensland University of Technology Telephone: 07 3382 1225 Email: [email protected]
Project Title: Family outcomes following client transfer from an Intensive Care
Unit: an educational intervention.
I am writing to invite you to participate in a study to improve critical care nursing practice during the transfer of families and patients from an intensive care unit to general wards. You will be given a draft brochure containing information nurses will discuss with relatives before their sick relative is transferred to a general ward. This study is the basis of a dissertation in the degree of Doctor of Philosophy at QUT and will be performed by Marion Mitchell under the guidance of an academic staff member, Professor Mary Courtney. The research study
This research study seeks to improve and gain additional understanding of the transfer process from the perspective of family members of critically ill patients. Purpose of the research This project aims: 1. To collaborate with relatives and nurses to determine relevant transfer
information requirements 2. To produce an easy to read brochure for nurses and relatives Duration of the participant’s involvement Your participation in this project involves reading and commenting on a draft brochure and completing the attached feedback form. This should take no longer than fifteen minutes. The audience for the information contained in the brochure needs to equate to eighth grade literacy level. The brochure needs to be simple and easy to read. Your suggestions will form the basis for an educational brochure being developed by the researcher. Participation in this project is voluntary and you may elect to withdraw at any time without comment or penalty.

239
Possible material risks to participants Participation in this project does not involve any known risk to the participants. However, should you feel any discomfort or distress while reading the information please contact the researcher. Benefits that will result from the research
1. Preparation of an educational brochure for use by intensive care nurses 2. Relatives are better prepared for the transfer of their relative from Intensive
Care to a general ward 3. Improve relative satisfaction following transfer. Confidentiality of the data Only the researcher will know the identities of the participants. All summaries of your comments will be kept in a locked filing cabinet and only the researcher will have access to them. No identifying information about the participants will be used in any paper that may result from this research. Questions or concerns You are welcome to contact Marion Mitchell regarding any questions or concerns you may have about this research study. If at any time you are not satisfied with this response you may contact Associate Professor Helen Edwards, Head of School of Nursing on 07 3864 3844. Should you have any concerns relating the ethical conduct of this research please feel free to contact the Secretary of the University Human Research Ethics Committee on 07 3864 2902. Feedback to participants Feedback will be provided to participants in this study via email. Instructions for return of feedback form
The stamped, self-addressed envelope may be used for returning your comments and feedback form. I thank you for your consideration of this project and I look forward to hearing from you soon. Kind regards Marion Mitchell.

240
Appendix G: Two – Teachers’ Feedback Sheet.
1. Is the brochure clearly written for an eighth grade audience?
Yes ❐ No ❐
2. If not, how can this be improved?
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
3. Is the brochure too long?
Yes ❐ No ❐
4. Is the brochure too short?
Yes ❐ No ❐
5. Is the information too complex for an eighth grade literacy level?
Yes ❐ No ❐
6. Please add any additional comments.
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
Please return this feedback form in the stamped, self-addressed envelope provided. Thank you for your feedback and comments.

241
Appendix H: Phase Three – Information and Consent Form for Family Members.
Queensland University of Technology Letterhead
Investigator: Marion Mitchell
School of Nursing, Queensland University of Technology Telephone: 07 3382 1225 Email: [email protected]
Project Title: Family outcomes following client transfer from an Intensive Care
Unit: an educational intervention.
I am writing to invite you to participate in a study which seeks to improve critical care nursing practice during the transfer of families and patients from the intensive care unit to general wards. This study is the basis of a degree of Doctor of Philosophy at Queensland University of Technology and will be performed by Marion Mitchell under the guidance of an academic staff member, Professor Mary Courtney. The research study
This research study seeks to improve and gain additional understanding of the transfer process from the perspective of family members of critically ill patients. Purpose of the research The project aims to: 1. Gain information about the transfer of relatives and their loved ones from
Intensive Care to the general ward 2. Improve the transfer process for relatives Duration of your involvement Your participation in this project will involve filling out a survey form which is attached. The questions relate to the process of transfer you experience. There will be another survey form to complete once your relative is transferred to the ward. These surveys should take no longer than twenty to thirty minutes to complete. It is very important that both surveys are completed. The results from these surveys will provide important information for the researcher who will is trying to improve the transfer process for relatives. The researcher will need to obtain some information about your relative. This information includes how long your relative’s stay is in intensive care, what is wrong with your relative, their age, gender and nationality. Participation in this project is voluntary and you may elect to withdraw at any time without comment

242
or penalty. A decision not to participate, or to withdraw, will have no impact upon your relative’s present or future care in any way. Possible material risks to participants Participation in this project does not involve any known risk to the participants. However, should you feel any discomfort or distress completing the survey forms please contact the researcher. A social worker or pastoral care officer is also available if you would like to speak with them. They can be contacted by way of the hospital switch on 3240 2111 if the need arises. Benefits that may result from the research
1. Relatives better prepared for transfer 2. Improved relative’s satisfaction with transfer method
Confidentiality of the data Only the researcher will know the identities of the participants. All surveys will be kept in a locked filing cabinet and only the researcher will have access to them. No identifying information about the participants will be used in any paper that may result from this research. Questions or concerns You are welcome to contact Marion Mitchell regarding any questions or concerns you may have about this research study. If at any time you are not satisfied with this response you may contact Associate Professor Helen Edwards, Head of School of Nursing on 07 3864 3844. Should you have any concerns relating the ethical conduct of this research please feel free to contact the Secretary of the University Human Research Ethics Committee on 07 3864 2902. The study has also been approved by the Princess Alexandra Hospital Research Ethics Committee and a representative may be contacted on 3240 5856. Instructions for return of questionnaires
The stamped, self-addressed envelope may be used for returning the questionnaires or you can place your completed questionnaires in the envelope and give it to the ward receptionist who will forward it to the researcher. I thank you for your consideration of this project and I look forward to receiving your comments. Kind regards Marion Mitchell.

243
Phase Three Consent Form for Family Members.
Queensland University of Technology Letterhead
Researcher: Marion Mitchell Queensland University of Technology, School of Nursing Telephone: 07 3382 1225 Project Title: Family outcomes following client transfer from an Intensive Care
Unit: an educational intervention The investigator conducting this research project abides by the principles governing the ethical conduct of research and, at all times, avows to protect the interests, comfort and safety of all participants. This form and the accompanying participant information package have been given to you for your own protection. They contain an outline of the study and possible risks. Your signature below will indicate that; 1. you have received the subject information package and have read its
contents; 2. you clearly understand the nature of the study and the possible risks
involved; and that you have been given the opportunity to discuss the contents of the Participant Information Package with the investigator prior to the commencement of the study;
3. you understand that all the data which you have provided will only be
revealed to the investigators. When the results of the study are published you will remain anonymous;
4. your participation is voluntary and therefore may be terminated at any
moment by you without comment or penalty, and without jeopardising the current and future care your relative is receiving;
5. you may direct any inquiries and further questions to Marion Mitchell at
the School of Nursing, Griffith University on 07 3382 1225. You may also direct complaints and concerns regarding the ethical conduct of this investigation to the Secretary of Queensland University of Technology Research Ethics Committee, on 07 3864 2902. A representative of the Princess Alexandra Hospital Research Ethics Committee may be contacted on 3240 5856.

244
6. you agree to participate in the study as set out in the Subject Information Package for the research project entitled “Family outcomes following client transfer from an Intensive Care Unit: an educational intervention” as part of a postgraduate thesis for a Doctor of Philosophy for Marion Mitchell.
Relative: ______________________________________ Date: ____________
Witness: ______________________________________ Date: ____________
Print Name: ___________________________________
I have explained the nature and purpose of this study to the above participant and have answered their questions.
Investigator ____________________ Date ___________

245
Appendix I: Phase Three and Four- Information and Consent Form for Nurses.
Queensland University of Technology Letterhead
Investigator:
Marion Mitchell School of Nursing, Queensland University of Technology Telephone: 07 3382 1225 Email: [email protected]
Project Title: Family outcomes following client transfer from an Intensive Care
Unit: an educational intervention.
I am writing to invite you to participate in a research study to improve critical care nursing practice during the transfer of families and patients from the intensive care unit to general wards. This study is the basis of a degree of Doctor of Philosophy at Queensland University of Technology and will be performed by Marion Mitchell under the guidance of an academic staff member, Professor Mary Courtney. The research study
This research study seeks to improve and gain additional understanding of the transfer process from the perspective of family members of critically ill patients. Purpose of the research This project aims: 1. To collaborate with relatives and nurses to determine relevant transfer
information requirements 2. To examine the concept of uncertainty for relatives as it relates to the
transfer process of intensive care clients 3. To produce a client and family focused educational brochure, which is
informative and easy to read 4. To provide a structured pre-transfer process to facilitate dialogue and
information sharing with family members and nursing staff 5. To determine the efficacy of the intervention in reducing family anxiety
and uncertainty following transfer 6. To measure the relative’s level of satisfaction with the transfer process 7. To evaluate the benefits of a structured pre-transfer method as perceived
by intensive care nurses. Duration of your involvement Your participation in this project will involve two components.

246
1. Attendance at one in-service education sessions. These will be scheduled at a range of different times for your convenience. During these sessions the researcher will explain a structured pre-transfer method for transferring relatives and their ill family member out of ICU to the general ward. The method involves the use of a brochure to help structure and individualise the information you give to each family before transfer. This method of transfer preparation will then be implemented into the ICU and all patients will be transferred by this method. Relatives will be surveyed in ICU by the researcher before being given the transfer information. Relatives will also be surveyed once they are in the general ward.
2. You will be asked to complete a questionnaire giving your opinions and ideas relating to the process of transfer.
Participation in this project is voluntary and you may elect to withdraw at any time without comment or penalty. A decision not to participate, or to withdraw, will have no impact upon your position in ICU or any involvement with QUT or Griffith University. Possible material risks to participants Participation in this project does not involve any known risk to the participants. However, should you feel unable to answer any questions raised by the family during the structured pre-transfer process, please speak with the nurse in charge of the shift. Should other issues emerge for you, please contact the researcher. A counselling service is available if you would like to speak with someone. Counselling services are available either at PAH via the hospital switch on 3240 2111or alternatively at QUT on 3864 3488 if the need arises. Benefits that may result from the research
1. Relatives better prepared for transfer 2. Improved relative’s satisfaction with transfer method 3. Establishment of a more family focused transfer process
Other benefits that may result are; • A structured pre-transfer educational method for the clinical area • Participation of critical care nurses in the research process, • Increased collaboration between practitioners and researchers and • A greater awareness by critical care nurses of the needs relating to transfer of
family members of critically ill patients.
Confidentiality of the data Only the researcher will know the identities of the participants and your name will not appear on the questionnaire. All information will be kept in a locked filing cabinet and only the researcher will have access to them. No identifying information about the participants will be used in any paper that may result from this research.

247
Questions or concerns You are welcome to contact Marion Mitchell regarding any questions or concerns you may have about this research study. If at any time you are not satisfied with this response you may contact Associate Professor Helen Edwards, Head of School of Nursing on 07 3864 3844. Should you have any concerns relating the ethical conduct of this research please feel free to contact the Secretary of the University Human Research Ethics Committee on 07 3864 2902. Feedback to participants Feedback will be provided to participants in this study through intensive care in-service sessions, and subsequently via publications. Please contact me if you would like to participate. Kind regards Marion Mitchell.

248
Phase Three Consent Form for Critical Care Nurse
Queensland University of Technology Letterhead
Researcher: Marion Mitchell QUT, School of Nursing Telephone: 07 3382 1225 Project title: Family outcomes following client transfer from an Intensive Care
Unit: an educational intervention The investigator conducting this research project abides by the principles governing the ethical conduct of research and, at all times, avows to protect the interests, comfort and safety of all participants. This form and the accompanying participant information package have been given to you for your own protection. They contain an outline of the study and possible risks. Your signature below will indicate that; 1. you have received the subject information package and have read its
contents; 2. you clearly understand the nature of the study and the possible risks
involved; and that you have been given the opportunity to discuss the contents of the Participant Information Package with the investigators prior to the commencement of the study;
3. you understand that all the data which you have provided will only be
revealed to the investigators. When the results of the study are published you will remain anonymous;
4. your participation is voluntary and therefore may be terminated at any
moment by you without comment or penalty, and without jeopardising your involvement with the Queensland University of Technology;
5. you may direct any inquiries and further questions to Marion Mitchell at
the School of Nursing, Griffith University on 07 3382 1225. You may also direct complaints and concerns regarding the ethical conduct of this investigation to the Secretary of Queensland University of Technology Research Ethics Committee, on 07 3864 2902.
6. you will receive feedback on your results during in-service sessions, and
through publications;

249
7. you agree to participate in the study as set out in the Subject Information Package for the research project entitled “Family outcomes following client transfer from an Intensive Care Unit: an educational intervention” as part of a postgraduate thesis for a Doctor of Philosophy for Marion Mitchell.
Registered Nurse: ______________________________ Date: ____________
Witness: ______________________________________ Date: ____________
Print Name: ___________________________________
I have explained the nature and purpose of this study to the above participant and
have answered their questions.
Investigator ________________________ Date________________

250
Appendix J: Phase Three Family Members’ Questionnaire before Transfer
PART ONE INSTRUCTIONS:
Please read each statement. Take your time and think about what each statement says. Then place an “X” under the column that most closely measures how you are feeling about your relative TODAY. If you agree with a statement, then you would mark under either “Strongly Agree” or “Agree”. If you disagree with a statement, then mark under either “Strongly Disagree” or “Disagree”. If you are undecided about how you feel about your relative, then mark under “Undecided” for that statement. Please respond to every statement. (1) I don’t know what is wrong with my relative. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(2) I have a lot of questions without answers. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _________ _______ _________ ________ _________
(3) I am unsure if my relative’s illness is getting better or worse. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(4) It is unclear how bad my relative’s pain will be. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5)
_______ _______ ________ ________ _________
(5) The explanations they give about my relative seem hazy to me. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(6) The purpose of each treatment for my relative is clear to me. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(7) I do not know when to expect things will be done to my relative. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(8) My relative’s symptoms continue to change unpredictably. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________

251
(9) I understand everything explained to me. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(10) The doctors’ say things to me that could have many meanings. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(11) I can predict how long my relative’s illness will last. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(12) My relative’s treatment is too complex to figure out. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(13) It is difficult to know if the treatments or medications my relative is getting are helpful.
Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(14) There are so many different types of staff, it’s unclear who is responsible for what.
Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(15) Because of the unpredictability of my relative’s illness, I cannot plan for the future.
Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(16) The course of my relative’s illness keeps changing. He/she has had good and bad days.
Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(17) It’s vague to me how I will manage the care of my relative after he/she leaves the hospital.
Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(18) It’s not clear what is going to happen to my relative. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________

252
(19) I usually know if my relative is going to have a good or bad day. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(20) The results of my relative’s tests are inconsistent. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(21) The effectiveness of the treatment is undetermined. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(22) It is difficult to determine how long it will be before I can care for my relative by myself.
Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(23) I can generally predict the course of my relative’s illness. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(24) Because of the treatment, what my relative can do and cannot do keeps changing. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(25) I’m certain they will not find anything else wrong with my relative. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(26) They have not given my relative a specific diagnosis. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(27) My relative’s physical distress is predictable; I know when it is going to get better or worse.
Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(28) My relative’s diagnosis is definite and will not change. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________

253
(29) I can depend on the nurses to be there when I need them. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(30) The seriousness of my relative’s illness has been determined. Strongly Agree Agree Undecided Disagree Strongly Disagree
(1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(31) The doctors and nurses use everyday language so I can understand what they are saying.
Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
(32) I am ……….. years of age.
(33) I am [please tick] Female ❐ Male ❐ (34) Number of years of education = …………….. years.
(35) My sick relative is in the Intensive Care Unit because they need treatment
for: [please fill in below] _________________________________________________________________
_________________________________________________________________
_________________________________________________________________
_________________________________________________________________
PART TWO
DIRECTIONS A number of statements which people have used to describe themselves are given below. Read each statement and then circle the appropriate number to the right of the statement to indicate how you feel right now, that is, at this moment. There are no right or wrong answers. Do not spend too much time on any one statement but give the answer which seems to describe your present feelings best.
Not at A
ll
Somew
hat
Moderately So
Very M
uch So
(36) I feel calm ...................................................................................... 1 2 3 4 (37) I feel secure..................................................................................... 1 2 3 4 (38) I feel tense....................................................................................... 1 2 3 4

254
(39) I feel strained ..................................................................................1 2 3 4 (40) I feel upset .......................................................................................1 2 3 4 (41) I am presently worrying over possible misfortunes ........................1 2 3 4 (42) I feel satisfied ..................................................................................1 2 3 4 (43) I feel frightened ...............................................................................1 2 3 4 (44) I feel comfortable ............................................................................1 2 3 4 (45) I feel self-confident .........................................................................1 2 3 4 (46) I feel nervous ...................................................................................1 2 3 4 (47) I am jittery .......................................................................................1 2 3 4 (48) I feel indecisive ...............................................................................1 2 3 4 (49) I am relaxed.....................................................................................1 2 3 4 (50) I feel content....................................................................................1 2 3 4 (51) I am worried ....................................................................................1 2 3 4 (52) I feel confused.................................................................................1 2 3 4 (53) I feel steady .....................................................................................1 2 3 4 (54) I feel pleasant ..................................................................................1 2 3 4 (55) I feel nervous and restless ...............................................................1 2 3 4 (56) I feel satisfied with myself ..............................................................1 2 3 4 (57) I wish I could be as happy as other seem to be ...............................1 2 3 4 (58) I feel like a failure ...........................................................................1 2 3 4 (59) I feel rested......................................................................................1 2 3 4 (60) I am “calm, cool, and collected” .....................................................1 2 3 4 (61) I feel difficulties are piling up so that I cannot overcome them......1 2 3 4 (62) I worry too much over something that really doesn’t matter ...........1 2 3 4 (63) I am happy.......................................................................................1 2 3 4 (64) I have disturbing thoughts...............................................................1 2 3 4 (65) I lack self-confidence ......................................................................1 2 3 4 (66) I feel secure .....................................................................................1 2 3 4

255
(67) I make decisions easily ................................................................... 1 2 3 4 (68) I feel inadequate ............................................................................. 1 2 3 4 (69) I am content .................................................................................... 1 2 3 4 (70) Some unimportant thought runs through my mind and bothers me 1 2 3 4 (71) I take disappointments so keenly that I can’t put them out ............ 1 2 3 4
of my mind (72) I am a steady person ....................................................................... 1 2 3 4 (73) I get in a state of tension or turmoil as I think over my recent ....... 1 2 3 4 concerns and interests.
(74) My nationality is [please circle]
a) Australian b) Indigenous Australian c) European d) Asian e) Other, please state _______________________________________
(75) My relationship to the patient is [please circle] a) Spouse/partner b) Brother or sister c) Child d) Parent e) Other, please state _______________________________________ (76) Before this admission, I have visited or been a patient in an Intensive Care Unit
[please tick] Yes ❐ No ❐
Thank you for completing this questionnaire. Please place the completed questionnaire in the stamped, self addressed envelope provided and either mail it
or give it to the researcher or ward receptionist.

256
Appendix K: Phase Three – Family Members’ Questionnaire after Transfer
PART ONE INSTRUCTIONS:
Please read each statement. Take your time and think about what each statement says. Then place an “X” under the column that most closely measures how you are feeling about your relative TODAY. If you agree with a statement, then you would mark under either “Strongly Agree” or “Agree”. If you disagree with a statement, then mark under either “Strongly Disagree” or “Disagree”. If you are undecided about how you feel about your relative, then mark under “Undecided” for that statement. Please respond to every statement. (1) I don’t know what is wrong with my relative. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (2) I have a lot of questions without answers. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _________ _______ _________ ________ _________ (3) I am unsure if my relative’s illness is getting better or worse. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (4) It is unclear how bad my relative’s pain will be. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (5) The explanations they give about my relative seem hazy to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (6) The purpose of each treatment for my relative is clear to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (7) I do not know when to expect things will be done to my relative. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________

257
(8) My relative’s symptoms continue to change unpredictably. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (9) I understand everything explained to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (10) The doctors’ say things to me that could have many meanings. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (11) I can predict how long my relative’s illness will last. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (12) My relative’s treatment is too complex to figure out. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (13) It is difficult to know if the treatments or medications my relative is getting are helpful. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (14) There are so many different types of staff, it’s unclear who is responsible for what. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (15) Because of the unpredictability of my relative’s illness, I cannot plan for the future. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (16) The course of my relative’s illness keeps changing. He/she has had good and bad days. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________

258
(17) It’s vague to me how I will manage the care of my relative after he/she leaves the hospital. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (18) It’s not clear what is going to happen to my relative. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (19) I usually know if my relative is going to have a good or bad day. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (20) The results of my relative’s tests are inconsistent. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (21) The effectiveness of the treatment is undetermined. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (22) It is difficult to determine how long it will be before I can care for my relative by myself. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (23) I can generally predict the course of my relative’s illness. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (24) Because of the treatment, what my relative can do and cannot do keeps changing. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (25) I’m certain they will not find anything else wrong with my relative. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________

259
(26) They have not given my relative a specific diagnosis. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (27) My relative’s physical distress is predictable; I know when it is going to get better or worse. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (28) My relative’s diagnosis is definite and will not change. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (29) I can depend on the nurses to be there when I need them. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (30) The seriousness of my relative’s illness has been determined. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________ (31) The doctors and nurses use everyday language so I can understand what they are saying. Strongly Agree Agree Undecided Disagree Strongly Disagree (1) (2) (3) (4) (5) _______ _______ ________ ________ _________
PART TWO
DIRECTIONS
A number of statements which people have used to describe themselves are given below. Read each statement and then circle the appropriate number to the right of the statement to indicate how you feel right now, that is, at this moment. There are no right or wrong answers. Do not spend too much time on any one statement but give the answer which seems to describe your present feelings best.
Not at A
ll
Somew
hat
Moderately So
Very M
uch So
(32) I feel calm....................................................................................... 1 2 3 4 (33) I feel secure..................................................................................... 1 2 3 4

260
(34) I feel tense .......................................................................................1 2 3 4 (35) I feel strained...................................................................................1 2 3 4 (36) I feel upset .......................................................................................1 2 3 4 (37) I am presently worrying over possible misfortunes ........................1 2 3 4 (38) I feel satisfied ..................................................................................1 2 3 4 (39) I feel frightened ...............................................................................1 2 3 4 (40) I feel comfortable ............................................................................1 2 3 4 (41) I feel self-confident .........................................................................1 2 3 4 (42) I feel nervous ...................................................................................1 2 3 4 (43) I am jittery .......................................................................................1 2 3 4 (44) I feel indecisive ...............................................................................1 2 3 4 (45) I am relaxed.....................................................................................1 2 3 4 (46) I feel content....................................................................................1 2 3 4 (47) I am worried ....................................................................................1 2 3 4 (48) I feel confused.................................................................................1 2 3 4 (49) I feel steady .....................................................................................1 2 3 4 (50) I feel pleasant ..................................................................................1 2 3 4 PART THREE
INSTRUCTIONS Next are some questions about the support that is available to you. Please answer each question. (51) About how many close friends and close relatives do you have (people you feel at ease with and can talk to about what is on your mind? Write in the number of close friends and close relatives:

261
People sometimes look to others for companionship, assistance, or other types of support. How often is each of the following kinds of support available to you if you need it? Please circle one number on each line. None
of the time
A little of the time
Some of the time
Most of the time
All of the time
(52) Someone to help you if you were confined ......1 2 3 4 5
to bed (53) Someone you can count on to listen to you ......1 2 3 4 5
when you need to talk (54) Someone to give you good advice about ..........1 2 3 4 5
a crisis (55) Someone to take you to the doctor if ...............1 2 3 4 5
you needed it (56) Someone who shows you love and affection....1 2 3 4 5
(57) Someone to have a good time with...................1 2 3 4 5
(58) Someone to give you information to help you..1 2 3 4 5
understand a situation (59) Someone to confide in or talk to about ............1 2 3 4 5
yourself or your problem (60) Someone who hugs you....................................1 2 3 4 5
(61) Someone to get together with for relaxation.....1 2 3 4 5
(62) Someone to prepare your meals if you were ....1 2 3 4 5
unable to do it yourself (63) Someone whose advice you really want...........1 2 3 4 5
(64) Someone to do things with to help you get.......1 2 3 4 5
your mind off things (65) Someone to help with daily chores if you ........1 2 3 4 5
were sick (66) Someone to share your most private worries....1 2 3 4 5
and fears with (67) Someone to turn to for suggestions about how.1 2 3 4 5
to deal with a personal problem (68) Someone to do something enjoyable with ........1 2 3 4 5
(69) Someone who understands your problems .......1 2 3 4 5
(70) Someone to love and make you feel wanted ....1 2 3 4 5

262
FINAL SECTION DIRECTIONS
Please consider the information given to you in the Intensive Care Unit by the
NURSE. One response per question please.
(71) How satisfied were you with information about the transfer of your relative
regarding having your questions answered honestly? very a little quite very dissatisfied dissatisfied unsure satisfied satisfied (1) (2) (3) (4) (5)
_______ ________ ________ __________ ________ (72) How satisfied were you with information given to you about the environment of
the general ward before going there for the first time ? very a little quite very dissatisfied dissatisfied unsure satisfied satisfied (1) (2) (3) (4) (5)
_______ ________ ________ __________ ________ (73) How satisfied were you with the information about what is being done for your
relative following transfer? very a little quite very dissatisfied dissatisfied unsure satisfied satisfied (1) (2) (3) (4) (5)
_______ ________ ________ __________ ________ (74) Was the information given to you easy to understand?
quite difficult not very easy unsure easy very easy (1) (2) (3) (4) (5)
_______ ________ ________ __________ ________
(75) How satisfied were you with specific information about your relative’s progress? very a little quite very dissatisfied dissatisfied unsure satisfied satisfied (1) (2) (3) (4) (5)
_______ ________ ________ __________ ________ (76) Were you told about transfer plans while they were being made?
no very little information unsure some information yes given given
(1) (2) (3) (4) (5) _______ ________ ________ __________ ________
(77) Was there anything you were told that worried or frightened you? Please tick
your answer. No ❐ Some things ❐ Yes, quite a few ❐
263
(78) Please comment on your answer above. ________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
(79) Overall, how well prepared were you for the transfer of your relative? not prepared not well a little well at all prepared unsure prepared prepared
(1) (2) (3) (4) (5) _______ ________ ________ __________ ________
(80) Looking back, was there anything you wish you had been told? Please comment. _______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
Thank you for completing this questionnaire. Please place the completed questionnaire
in the self addressed envelope provided and either give it to the researcher or ward
receptionist.

264
Appendix L: Phase Four ICU Nurses’ Questionnaire (1) Approximately, how many times have you used the structured pre-transfer
method using the brochure? 1 2 3 4
1-5 6-10 11-20 greater than 20 .
(2) Was it helpful in providing a framework for your discussion? 1 2 3 4 5
not at all helpful at times not sure quite helpful very helpful (3) Did it promote discussion about the sick family member? 1 2 3 4 5 No Minimal Not sure Some discussion Yes, a great deal (4) Were there important aspects missing from the brochure? Please comment: ……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… (5) Would you recommend the introduction of the brochure to support all transfers from your unit? 1 2 3 4 Yes Yes, with changes Not sure No (6) Please comment on your above answer.
……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………… (7) How would you rate your unit’s attitude to family members?
1 2 3 4 5 excellent quite good not sure not very good poor
(8) How important are family members to critically ill patient’s recovery? 1 2 3 4 5
not important slightly important not sure important very important
(9) In your opinion, how important is the transfer process for relatives? 1 2 3 4 5
not slightly not sure important very important important important
Thank you for completing this questionnaire. Please place the completed
questionnaire in the seeled stamped, self-addressed envelope provided and return it to the researcher.

265
References Andersson- Segesten, K. (1991). Patients’ experience of uncertainty in illness in
two intensive coronary care units, Scandinavian Journal of Caring Science, 5(1), 43-47.
Artinian, N. T. (1991). Strengthening nurse-family relationships in critical care,
AACN Clinical Issues in Critical Care Nursing, 2(2), 269-275. Ballard, K. S. (1981). Identification of environmental stressors for patients in a
surgical intensive care unit, Issues in Mental Health Nursing, 3, 89-108. Barbetti, J. & Choate, K. (2003). Intensive care liaison nurse services:
implementation at a major metropolitan hospital, Australian Critical Care, 16(2), 46-52.
Benner, P., Hooper-Kyriakidis, P., & Stannard, D. (1999). Clinical Wisdom and
Interventions in Critical Care: Thinking-In-Action Approach, Philadelphia: W. B. Saunders Company.
Benzer, H., Mutz, N., & Pauser, G. (1983). Psychosocial sequelae of intensive
care, International Anaesthetic Clinics, 21(2), 169-180. Bokinskie, J. C. (1992). Family Conferences: a method to diminish transfer
anxiety, Journal of Neuroscience Nursing, 24(3), 129-133. Bouvé, L. R., Rozmus, C. L., & Giordano, P. (1999). Preparing parents for their
child’s transfer from the PICU to the pediatric floor, Applied Nursing Research, 12(3), 114-120.
Bowling, A. (1997). Research Methods in Health: Investigating Health and
Health Services, Buckingham: Open University Press. Braden, C. J. (1990). A test of the self-help model: learned response to chronic
illness experience, Nursing Research, 39(1), 42-47. Bradenburg, M., & Gifford, J. (1997). Developing a multidisciplinary brochure to
teach patients and families about life-sustaining treatments, Dimensions of Critical Care Nursing, 16(6), 328-332.
Breu, C., & Dracup, K. (1978). Helping the spouses of critically ill patients,
American Journal of Nursing, 78(1), 50-53. Brookfield, S. D. (1986). Understanding and facilitating adult learning. Milton
Keyes: Open University Press. Broome, M. E. (1985). Working with the family of a critically ill child, Heart &
Lung, 14(4), 368-372 .
266
Burns, N., & Grove, S. K. (1995). Understanding Nursing Research. Philadelphia: W.B. Saunders Company.
Burr, G. (1996). Unfinished business: interviewing family members of critically
ill patients, Nursing Inquiry, 3, 172-177. Caffarella, R. S. (1993). Self-directed learning. In S. B. Merriam (Ed.), New
Directions for Adult and Continuing Education: An Update on Adult Learning Theory (pp. 25-35). San Francisco: Jossey-Bass.
Cagan, J. (1988). Weaning parents from intensive care unit care, American
Journal of Maternal Child Nursing, 13, July/August, 275-277. Caine, R. M. (1989). Families in crisis: making the critical difference, Focus on
Critical Care, 16(3), 184-189. Chaboyer, W., Foster, M., Kendall, E., & James, H. (2002). ICU nurses’
perceptions of discharge planning: a preliminary study, Intensive and Critical Care Nursing, 18, 90-95.
Chartier, L., & Coutu-Wakulczyk, G. (1989). Families in ICU: their needs and
anxiety level, Intensive Care Nursing, 5, 11-18. Chavez, C. W., & Faber, L. (1987). Effect of an education-orientation program on
family members who visit their significant other in the intensive care unit, Heart & Lung, 16(1), 92-99.
Chen, Y. (1990). Psychological and social support systems in intensive and
critical care, Intensive Care Nursing, 6, 59-66. Coakes, S. J., & Steed, L. G. (2001). SPSS analysis without anguish, version 10.0.
Brisbane: John Wiley and Sons. Choate, K., & Stewart, M. (2002). Reducing anxiety in patients and families
discharged from ICU, Australian Nursing Journal, 10(5), 29.
Cody, A. (1996). Helping the vulnerable of condoning control within the family: where is nursing? Journal of Advanced Nursing, 23, 882-886.
Cohen, M. Z., Craft, M. J., & Titler, M. (1988). Families in critical care settings: where fear leads to silence, Phenomenology and Pedagogy, 6(3), 147-157.
Compton, P. (1990). Critical illness & intensive care units: what it means to the
client, Critical Care Nurse, 11(1), 50-56. Cooper, G. S., Sirio, C. A., Rotondi, A. J., Shepardson, L. B., & Rosenthal, G. E.
(1999). Are readmissions to the intensive care unit a useful measure of hospital performance? Medical Care, 37(4), 399-408.
Coulter, M. A. (1989). The needs of family members in intensive care units,
Intensive Care Nursing, 5, 4-10.

267
Coyle, M. A. (2001). Transfer anxiety: preparing to leave intensive care,
Intensive and Critical Care Nursing, 17(3), 138-143. Craven, R. F., & Sharp, B. H. (1972). The effects of illness on family function,
Nursing Forum, 11(2), 186-193. Curry, S. (1995). Identifying family needs and stresses in the intensive care unit,
British Journal of Nursing, 4(1), 15-19. Cutler, L., & Garner, M. (1995). Reducing relocation stress after discharge from
the intensive therapy unit, Intensive & Critical Care Nursing, 11(6), 333-335.
Daley, L. (1984). Families in critical care - the perceived immediate needs of
families with relatives in the intensive care setting, Heart & Lung, 13(3), 231-237.
Deane, K. A., & Degner, L. F. (1998). Information needs, uncertainty, and anxiety
in women who had a breast biopsy with benign outcome, Cancer Nursing, 21(2), 117-126.
Derham, C. (1991). An evaluation of the preoperative information given to
patients by intensive care nurses, Intensive Care Nursing, 7(2), 80-85. Dossey, B. M. (2000) Florence Nightingale: Mystic, Visionary, Healer.
Springhouse, Penn: Springhouse Publishing Company. Dunkel, J., & Eisendrath, S. (1983). Families in the intensive care unit: their effect
of staff, Heart & Lung, 12(3), 258-261. Dyer, I. D. (1991). Meeting the needs of visitors – a practical approach, Intensive
Care Nursing, 7(3), 135-147. Dyer, I. (1995). Preventing the ITU syndrome or how not to torture an ITU
patient! Part 1, Intensive and Critical Care Nursing, 11, 130-139. Elpern, E. H., Patterson, P. A., Gloskey, D., & Bone, R. C. (1992). Patients’
preferences for intensive care, Critical Care Medicine, 20(1), 43-47. Farvis, M. (2002). The family: an important nursing resource for holistic client
care, Australian Nursing Journal, 10(5), 1-3. Flanagan, V., Slattery, M. J., Chase, N. S., Meade, S. K., & Cronenwett, L. R.
(1996). Mothers’ perceptions of the quality of their infants’ back transfer: a pilot study results, Neonatal Network, 15(2), 27-33.
Flick, U. (2002). An introduction to qualitative research, (2nd ed.). London: Sage
Publications.
268
Foss, K. R., & Tenholder, M. F. (1993). Expectations and needs of persons with family members in an intensive care unit as opposed to a general ward, Southern Medical Journal, 86(4), 380-384.
Fowlie, P., Francis, H., & Russell, S. (2000). A perioperative communication link
with families, Canadian Nurse, 8, September, 30-33. Fox, S. & Jeffrey, J. (1997). The role of the nurse with families of patients in ICU:
the nurses’ perspective, Canadian Journal of Cardiovascular Nursing, 8(1), 17-23.
Freichels, T. A. (1991). Needs of family members of patients in the intensive care
unit over time, Critical Care Nursing Quarterly, 14(3), 16-29. Friedman, M. M. (1998). Family Nursing: Research, Theory, and Practice, (4th
ed.). Connecticut: Appleton and Lange. Gaskins, S., & Brown, K. (1992). Responses among individuals with human
immunodeficiency virus infection, Applied Nursing Research, 5, 111-121. Hall-Smith, J., Ball, C., & Coakley, J. (1997). Follow-up services and the
development of a clinical nurse specialist in intensive care, Intensive and Critical Care Nursing, 13, 243-248.
Halm, M. A. (1990). Effects of support groups on anxiety of family members
during critical illness, Heart and Lung, 19(1), 62-71. Halm, M. A., Titler, M. G., Kleiber, C., Johnson, S. K., Montgomery, L. A., Craft,
M. J., Buckwalter, K., Nicholson, A., & Megivern, K. (1993). Behavioral responses of family members during critical illness, Clinical Nursing Research, 2(4), 414-437.
Hayes, E. (1990). Needs of family members of critically ill patients – a Northern
Ireland perspective, Intensive Care Nursing, 6, 25-29. Henneman, E. A., & Cardin, S. (1992). Need for information: interventions for
practice, Critical Care Nursing Clinics of North America, 4(4), 615-621. Henneman, E. A., McKenzie, J. B., & Dewa, C. S. (1992). An evaluation of
interventions for meeting the information needs of families of critically ill patients, American Journal of Critical Care, 1(3), 85-93.
Hickey, M. L., & Leske, J. S. (1992). Needs of families of critically ill patients:
state of the science and future directions, Critical Care Nursing Clinics of North America, 4(4), 645- 649.
Hickey, M., & Lewandowski, L. (1988). Critical care nurses’ role with families: a
descriptive study, Heart & Lung, 17(6), 670-676.
269
Higgins, L. W. (1999). Nurses’ perceptions of collaborative nurse-physician transfer decision making as a predictor of patient outcomes in a medical intensive care unit, Journal of Advanced Nursing, 29(6), 1434-1443.
Hilton, B. A. (1989). The relationship of uncertainty, control, commitment, and
threat of recurrence to coping strategies used by women diagnosed with breast cancer, Journal of Behavioral Medicine, 12, 39-54.
Hilton, B. A. (1994). The uncertainty stress scale: its development and
psychometric properties, Canadian Journal of Nursing Research, 26(3), 15-30.
Holden, J., Harrison, L., & Johnson, M. (2002). Families, nurses and intensive
care patients: a review of the literature, Journal of Clinical Nursing, 11, 140-148.
Hughes, K. K. (1993). Psychosocial and functional status of breast cancer
patients: the influence of diagnosis and treatment choice, Cancer Nursing, 16(3), 222-229.
Jacono, J., Hicks, G. Antonioni, C., O’Brien, K., & Rasi, M. (1990). Comparison
of perceived needs of family members between registered nurse and family members of critically ill patients in intensive care and neonatal intensive care units, Heart & Lung, 19(1), 72-78.
Jenkins, D. A., & Rogers, H. (1995). Transfer anxiety in patients with myocardial
infarction, British Journal of Nursing, 4(21), 1248-1252. Johnson, P. (1999). Rural people’s experiences of critical illness involving inter-
hospital transportation: a qualitative study, Australian Critical Care, 12(1), 12-16.
Johnson, S. (2001). Family therapy saves the planet: Messianic tendencies in the
family systems literature, Journal of Marital and Family Therapy, 27(1), 3-11.
Jones, J., Hoggart, B., Withey, J., Donaghue, K., & Ellis, B.W. (1979). What the
patients say: a study of reactions to an intensive care unit. Intensive Care Medicine, 5, 89-92.
Jones, C., & O’Donnell, C. (1994). After Intensive Care - what then? Intensive
and Critical Care Nursing, 10, 89-92. Keen, T., & Weir, P. (1995). Chapter 10, Building bridges: primary nursing in a
mental health unit. In K. Kendrick, P. Weir, & E. Rosser (Eds.), Innovations in Nursing Practice (pp. 179-197). London: Edward Arnold.
Keogh, S. (2001). Parents’ experiences of the transfer of their child from the PICU
to the ward: a phenomenological study. Nursing in Critical Care, 6(1), 7-13.
270
Kidd, P. S., & Parshall, M. B. (2000). Getting the focus and the group: enhancing analytical rigor in focus group research. Qualitative Health Research, 10(3), 293-308.
Kleinpell, R. M., & Powers, M. J. (1992). Needs of family members of intensive
care unit patients, Applied Nursing Research, 5(1), 2-8. Knaus, W. A., Wagner, D. P., Draper, E. A., Zimmerman, J. E., Bergner, M.,
Bastos, P. G., Sirio, C. A., Murphy, D. J., Lotring, T., Damiano, A., & Harrell, F. E. (1991). The APACHE III prognostic system: risk prediction of hospital mortality for critically ill hospitalized adults, Chest, 100(6), 1619-1636.
Knowles, M. (1980). The modern practice of adult education: from pedagogy to
andragogy. New York: Cambridge, The Adult Education Company. Koller, P. A. (1991). Family needs and coping strategies during illness crisis,
AACN Clinical Issues in Critical Care Nursing, 2(2), 338-345. Krueger, R., & Casey, M. (2000). Focus Groups: A Practical Guide for Applied
Research (3rd ed.). London: Sage Publication, Inc. Lange, J. W. (1989). Developing printed materials for patient education,
Dimensions of Critical Care Nursing, 8(4), 250-258. La Lopa, J. M., & Marecki, R. F. (1999). The critical role of quality in the tourism
system, Quality Progress, 32(8), 37-41. Leith, B. A. (1999). Patients’ and family members’ perceptions of transfer from
intensive care, Heart & Lung, 28(3), 210-218. Leske, J. S. (1986). Needs of relatives of critically ill patients: a follow up, Heart
& Lung, 15(2), 189-193. Leske, J. S. (1991). Overview of family needs after critical illness: from
assessment to intervention, AACN Clinical Issues in Critical Care Nursing, 2(2), 220-226.
Leske, J. S. (1992). Needs of adult family members after critical illness:
prescriptions for interventions, Critical Care Nursing Clinics of North America, 4(4), 587-596.
Lethbridge, B., Somboon, O., & Shea, H. L. (1976). The transfer process,
Canadian Nurse, 72(10), 39-40. Ley, P. (1979). Memory for medical information, British Journal of Social and
Clinical Psychological, 18, 245-255. Liddle, K. (1989). Reaching out …to meet the needs of relatives in intensive care
units, Intensive Care Nursing, 4, 146-159.

271
Lynn-McHale, D. J., Corsetti, A., Brady-Avis, E., Shaffer, R., McGrory, J., &
Rothenberger, C. (1997). Pre-operative ICU tours: are they helpful? American Journal of Critical Care, 6(2), 106-115.
Lynn-McHale, D. J., & Bellinger, A. (1988). Need satisfaction levels of family
members of critical care patients and accuracy of nurses’ perceptions, Heart and Lung, 17(4), 447-453.
Lynn-McHale, D. J., & Smith, A. (1993). Comprehensive assessment of families
of the critically ill. In G. D. Wegner & R. J. Alexander (Eds.), Readings in Family Nursing (pp. 309-328). Philadelphia: J. B. Lippincott Company.
McAllister, L. (1997). An adult learning framework for clinical education. In L.
McAllister, M. Lincoln, S. McLeod, & D. Maloney (Eds.), Facilitating Learning in Clinical Settings (pp. 13-26). London: Stanley Thornes.
McClowry, S. G. (1992). Family functioning during a critical illness: a systems
theory perspective, Critical Care Nursing Clinics of North America, 4(4), 559-564.
McDowell, I., & Newell, C. (1996). Measuring Health: A guide to Rating Scales
and Questionnaires. Oxford: Oxford University Press. McKinney, A. A., & Melby, V. (2002). Relocation stress in critical care: a review
of the literature, Journal of Clinical Nursing, 11, 149-157. McShane, R. E. (1991). Family theoretical perspectives and implications for
nursing practice, AACN Clinical Issues in Critical Care Nursing, 2(2), 210-219.
Macey, B. A., & Bouman, C. C. (1991). An evaluation of validity, reliability, and
readability of the Critical Care Family Needs Inventory, Heart & Lung, 20(4), 398-403.
Maillet, R. J., Pata, I., & Grossman, S. (1993). A strategy for decreasing anxiety
of ICU transfer patients and their families, Nursing Connections, 6(4), 5-8. Marsden, C. (1992). Family-centred critical care: an option or obligation?
American Journal of Critical Care, 1(3), 115-117. Martin, P., & Pierce, R. (1994). Practical Statistics for the Health Sciences.
Melbourne: Thomas Nelson Australia. Mast, M. E. (1995). Adult uncertainty in illness: a critical review of research,
Scholarly Inquiry for Nursing Practice: an International Journal, 9(1), 3-23.

272
Mast, M. E. (1998). Survivors of breast cancer: illness uncertainty, positive reappraisal, and emotional distress, Oncology Nursing Forum, 25(3), 555-562.
Mendonca, D., & Warren, N. A. (1998). Perceived and unmet needs of critical
care family members (advances in cardiac and pulmonary surgery), Critical Care Nursing Quarterly, 21(1), 58-68.
Meyer, C. (1992). Making a critical difference, American Journal of Nursing,
92(7), 61-68. Merriam, S. B. (1996). Updating our knowledge of adult learning, Journal of
Continuing Education in the Health Professions, 16(3), 136-143. Micik, S., & Borbasi, S. (2002). Effect of support programme to reduce stress in
spouses whose partners ‘fall off’ clinical pathways post cardiac surgery. Australian Critical Care, 15(1), 33-40.
Millar, B. (1991). Caring and the family in the critical care unit. Surgical Nurse,
4(3), 4-9. Mishel, M. H. (1981). The measurement of uncertainty in illness, Nursing
Research, 30(5), 258-263. Mishel, M. H. (1983a). Adjusting the fit: development of uncertainty scales for
specific clinical populations, Western Journal of Nursing Research, 5(4), 355-370.
Mishel, M. H. (1983b). Parents’ perception of uncertainty concerning their
hospitalized child, Nursing Research, 32(6), 324-330. Mishel, M. H. (1988). Uncertainty in illness, IMAGE: Journal of Nursing
Scholarship, 20(4), 225-232. Mishel, M. H. (1995). Response to “adult uncertainty in illness: a critical review
of research”, Scholarly Inquiry for Nursing Practice: an International Journal, 9(1), 25-29.
Mishel, M. H. (1997). Uncertainty in Illness Scales Manual. Chapel Hill:
University of North Carolina. Mishel, M. H., & Braden, C. J. (1987). Uncertainty a mediator between support
and adjustment, Western Journal of Nursing Research, 9(1), 43-57. Mishel, M. H., & Braden, C. J. (1988). Finding meaning: antecedents of
uncertainty in illness, Nursing Research, 37(2), 98-103. Mishel, M. H., Padilla, G., Grant, M., & Sorenson, D. S. (1991). Uncertainty in
illness theory: a replication of the mediating effects of mastery and coping, Nursing Research, 40(4), 236-240.

273
Mishel, M. H., & Sorenson, D. S. (1991). Uncertainty in gynaecological cancer: a test of the mediating functions of mastery and coping, Nursing Research, 40(3), 167-171.
Molter, N. C. (1979). Needs of relatives of critically ill patients: a descriptive
study, Heart & Lung, 8(2), 332-339. Nettle, C., Pavelich, J., Jones, N., Beltz, C., Laboon, P., & Pifer, P. (1993). Family
as client: using Gordon’s health pattern typology, Journal of Community Health Nursing, 10(1), 53-61.
Nelson, J. P. (1996). Struggling to gain meaning: living with the uncertainty of
breast cancer, Advances in Nursing Science, 18(3), 59-76. Northouse, L. L., Laten, D., & Reddy, P. (1995). Adjustment of women and their
husbands to recurrent breast cancer, Research in Nursing & Health, 18, 515-524.
Odell, M. (2000). Patient’s thoughts and feelings about their transfer from
intensive care to the general ward, Journal of Advanced Nursing, 31(2), 322-329.
Ogden, J. (1996). Health Psychology: A Textbook. Buckingham: Open
University Press. O’Neill Norris, L., & Groves, S. K. (1986). Investigation of selected psychosocial
needs of family members of critically ill adult patients, Heart & Lung, 15(2), 194-199.
Parrinello, K. (1984). Patients’ evaluation of a teaching booklet for arterial bypass
surgery, Patient Education and Counseling, 5(4), 183-188. Plowright, C. I. (1996). Revisiting visiting in intensive therapy units, Intensive
and Critical Care Nursing, 12, 231-238. Poe, C. M. (1982). Minimising stress-of-transfer responses, Dimensions of
Critical Care Nursing, 1(6), 364-374. Polit, D. F. (1996). Data Analysis & Statistics for Nursing Research. London:
Appleton & Lange. Polit, D.F., & Hungler, B.P. (1997). Essentials of Nursing Research: Methods,
Appraisal, and Utilization, (4th Ed.). Philadelphia: J. B. Lippencott-Raven Publishers.
Polit, D. F., & Hungler, B. P. (1999). Nursing Research Principles & Methods
(6th Ed.). Philadelphia: J. B. Lippincott-Raven Publishers. Provine, R. C. (1986). The challenges of patient education in critical care, Critical
Care Nurse, 6(2), 22 & 24.

274
Quinn, S., Redmond, K., & Begley, C. (1996). The needs of relatives visiting
adult critical care units as perceived by relatives and nurses: part 2, Intensive and Critical Care Nurse, 12, 239-245.
Raleigh, E. H., Lepczyk, M., & Rowley, C. (1990). Significant others benefit from
preoperative information, Journal of Advanced Nursing, 15, 941-945. Reedy, J. E. (1993). Transfer of a patient with a ventricular assist device to a non-
critical care area, Heart & Lung, 22(1), 71-76. Rice, P. L., & Ezzy, D. (1999). Qualitative research methods: a health focus.
Melbourne: Oxford University Press. Robb, Y. (1997). Family nursing in intensive care. In D. A. Whtye (Ed.),
Explorations in Family Nursing (pp. 131-150). London: Routledge. Roberts, S. L. (1976). Behavioral Concepts and the Critically Ill Patient.
Englewood Cliffs, N.J.: Prentice Hall. Rukholm, E., Bailey, P., Coutu-Wakulczyk, G., & Bailey, W. B. (1991). Needs
and anxiety levels in relatives of intensive care unit patients, Journal of Advanced Nursing, 16, 920-928.
Russell, S. (1996). Who knows where they go? Quality of life after intensive care,
Australian Nursing Journal, 3(8), 20-22. Russell, S. (1999a). An exploratory study of patients’ perceptions, memories and
experiences of an intensive care unit, Journal of Advanced Nursing, 29(4), 783-791.
Russell, S. (1999b). Reducing readmissions to the intensive care unit, Heart &
Lung, 28(5), 365-372. Russell, S. (2000). Continuity of care after discharge from ICU, Professional
Nurse, 15(8), 497-500. Saarmann, L. (1993). Transfer out of critical care: freedom or fear? Critical Care
Nursing Quarterly, 16(1), 78-85. Schactman, M. (1989). Transfer stress in patients after myocardial infarction,
Focus on Critical Care, 14(2), 34-37. Schwartz, L. P., & Brenner, Z. R. (1979). Critical Care unit transfer: reducing
patient stress through nursing interventions, Heart & Lung, 8(3), 540-546. Scriven. A., & Tucker, C. (1997). The quality and management of written
information presented to women undergoing hysterectomy, Journal of Clinical Nursing, 6, 107-113.

275
Scullion, P. A. (1994). Personal cost, caring and communication: an analysis of communication between relatives and intensive care nurses, Intensive and Critical Care Nursing, 10(1), 64-70.
Shannon, V. J. (1973). The transfer process: an area of concern for the CCU
nurse, Heart & Lung, 2(3), 364-367. Sherbourne, C. D., & Stewart. A. L. (1991). The MOS social support survey,
Social Science Medicine, 32, 705-714. Simpson, T. F.; Armstrong, S. & Mitchell. S. 1989 Critical Care Management
Heart & Lung, 18(4), 325-332. Snow, K. P. (2002). Theories of organizational & social systems: a transitioning
Russian perspective. Futurics, 26(1/2), 20-36. Soehren, P. (1995). Stressors perceived by cardiac surgical patients in the
intensive care unit, American Journal of Critical Care, 4(1), 71- 76. Spatt, L., Ganas, E., Hying, S., Kirsch, E. R., & Kosh, M. (1986). Informational
needs of families of intensive care unit patients, Quarterly Review Bulletin, 12(1), 16-21.
Spielberger, C., Gorsuch, R., & Lushene, R. (1983). Manual for the State-Trait
Anxiety Inventory. Palo Alto, CA.: Consulting Psychologist Press. Streater, C., Golledge, J., Sutherland, H., Easton, J., MacDonald, R., McNamara,
R., Looise, A., & Gelling, L. (2001). The relocation experiences of relatives leaving a neurosciences critical care unit: a phenomenological study. Nursing in Critical Care, 6(4), 163-170.
Talbot, L. A. (1995). Principles and Practices of Nursing Research. St Louis:
Mosby-Year Book, Inc. Teasdale, K. (1993). Information and anxiety: a critical reappraisal, Journal of
Advanced Nursing, 18, 1125-1132. Thompson, T. L. (1985). Discharge planning for critical care, Critical Care Nurse,
5(6), 48-51. Titler, M. G., Bombei, C., & Schutte, D. L. (1995). Developing family-focused
care, Critical Care Nursing Clinics of North America, 7(2), 375-386. Titler, M. G., Cohen, M. Z., & Craft, M. J. (1991). Impact of adult critical care
hospitalization: perceptions of patients, spouses, children, and nurses, Heart & Lung, 20(2), 174-182.
Toth, J. C. (1980). Effect of structured preparation for transfer on patient anxiety on leaving coronary care unit, Nursing Research, 29(1), 28-34.

276
von Bertalanffy L. (1973). General System Theory: Foundations Development Applications. Norwich: Penguin University Books.
Waitkoff, B., & Imburgia, D. (1990). Patient education and continuous
improvement in a phase 1 cardiac rehabilitation program, Journal of Nursing Quality Assurance, 5(1), 38-48.
Walters, A. J. (1995). A heumeneutic study of the experiences of relatives of
critically ill patients, Journal of Advanced Nursing, 22, 998- 1005. Watts, S., & Brooks, A. (1997). Patients’ perception of pre-operative information
they need about events they may experience in the intensive care unit, Journal of Advanced Nursing, 26, 85-92.
Webb, C., & Kevern J. (2001). Focus groups as research method: a critique of
some aspects of their use in nursing research. Journal of Advanced Nursing, 33(6), 798-805.
Wellard, S. (1997). Constructions of family nursing: a critical exploration,
Contemporary Nurse, 6(2), 78- 84. Whall, A. L. (1993). The family as the unit of care in nursing: a historical review.
In G. D. Wegner & R. J. Alexander (Eds.), Readings in Family Nursing (pp.3-13). Philadelphia: J. B. Lippincott Company.
Whire, P. (1997). The role of the critical care nurse in counselling families about
advanced directives, Critical Care Nursing Clinics of North America, 9(1), 53-57.
Wilkinson, P. (1995). A qualitative study to establish the self-perceived needs of
family members of patients in a general intensive care unit, Intensive and Critical Care Nursing, 11, 77-86.
Wineman, N. M., Schwetz, K. M., Goodkin, D. E., & Rudick, R. A. (1996).
Relationships among illness uncertainty, stress, coping and emotional wellbeing at entry into a clinical drug trial, Applied Nursing Research, 9(2), 53-60.
Wong, C. A., & Bramwell, L. (1992). Uncertainty and anxiety after mastectomy
for breast cancer, Cancer Nursing, 15(5), 363-371. Wooley, N. (1990). Crisis theory: a paradigm of effective intervention with
families of critically ill people, Journal of Advanced Nursing, 15, 1402-1408.
Wright, L. M., & Leahey, M. (1994). Nurses and Families: a Guide to Family
Assessment and Intervention, (2nd ed.). Philadelphia: F.A. Davis and Company.

277
Yarcheski, A. (1988). Uncertaitny in illness and the future, Western Journal of Nursing Research, 10(4), 401-413.
Ziemer, M. M. (1983). Effects of information on post-surgical coping, Nursing
Research, 32(5), 282-287.