Embed Size (px)
Citation preview

Research Article
Quantitative Analysis of Immune Infiltrates inPrimary MelanomaRobyn D. Gartrell1, Douglas K. Marks2, Thomas D. Hart3, Gen Li4,Danielle R. Davari3, Alan Wu5, Zo€e Blake2, Yan Lu2, Kayleigh N. Askin3,Anthea Monod6, Camden L. Esancy2, Edward C. Stack7, Dan Tong Jia8,Paul M. Armenta8, Yichun Fu8, Daisuke Izaki3, Bret Taback9, Raul Rabadan6,Howard L. Kaufman10, Charles G. Drake2, Basil A. Horst11, and Yvonne M. Saenger2
Abstract
Novelmethods to analyze the tumormicroenvironment (TME)are urgently needed to stratify melanoma patients for adjuvantimmunotherapy. Tumor-infiltrating lymphocyte (TIL) analysis,by conventional pathologic methods, is predictive but is insuffi-ciently precise for clinical application. Quantitative multipleximmunofluorescence (qmIF) allows for evaluation of the TMEusing multiparameter phenotyping, tissue segmentation, andquantitative spatial analysis (qSA). Given that CD3þCD8þ cyto-toxic lymphocytes (CTLs) promote antitumor immunity, whereasCD68þ macrophages impair immunity, we hypothesized thatquantification and spatial analysis of macrophages and CTLswould correlate with clinical outcome. We applied qmIF to104 primary stage II to III melanoma tumors and found thatCTLs were closer in proximity to activated (CD68þHLA-DRþ)macrophages than nonactivated (CD68þHLA-DR�) macro-phages (P < 0.0001). CTLs were further in proximity from
proliferating SOX10þmelanoma cells than nonproliferating ones(P < 0.0001). In 64 patients with known cause of death, wefound that high CTL and low macrophage density in the stroma(P ¼ 0.0038 and P ¼ 0.0006, respectively) correlated withdisease-specific survival (DSS), but the correlation was less signi-ficant for CTL and macrophage density in the tumor (P ¼ 0.0147and P ¼ 0.0426, respectively). DSS correlation was strongestfor stromal HLA-DRþ CTLs (P ¼ 0.0005). CTL distance toHLA-DR� macrophages associated with poor DSS (P ¼ 0.0016),whereas distance to Ki67� tumor cells associated inversely withDSS (P ¼ 0.0006). A low CTL/macrophage ratio in the stromaconferred a hazard ratio (HR) of 3.719 for death from melanomaand correlated with shortened overall survival (OS) in the com-plete 104 patient cohort by Cox analysis (P ¼ 0.009) and meritsfurther development as a biomarker for clinical application.Cancer Immunol Res; 6(4); 481–93. �2018 AACR.
IntroductionCutaneous melanoma is an aggressive disease, even when
localized, with 40% of patients with stage II to III melanomadeveloping recurrent disease (1). Current histopathologic
methods, including conventional immunohistochemistry(IHC) evaluation of formalin-fixed paraffin-embedded (FFPE)tissues, have been unable to identify precise biomarkers capa-ble of identifying patients at greatest risk for recurrence (2).Advancements in clinically applicable histopathologic methodsfor evaluating the tumor microenvironment (TME) are essentialfor patient care and, in particular, selecting patients to receiveimmunotherapies. In preclinical research settings, flow cyto-metry (FC) offers detailed evaluation of infiltrating immunecells and supplements conventional IHC. However, clinicalapplication of FC is limited because FC can only be performedon fresh tissue. Obtaining fresh tissue is only feasible when alarge volume of excess tumor is available, a rare occurrence forprimary melanomas, and harvesting fresh tissue requires closecoordination between multiple clinicians in an already over-burdened health care setting. In contrast, FFPE samples areroutinely banked on every patient who has tumor resectionand/or biopsy and is a much more practical source of materialfor immune phenotyping.
In early-stage melanoma, traditional tumor, node, and metas-tasis (TNM) staging does not precisely assess the risk of recurrenceof an individual patient. The American Joint Committee onCancer (AJCC) defines stage II melanoma based on tumordepth >1.01 mm with ulceration and >2.01 mm with or withoutulceration, and stage III disease is defined by locoregional metas-tasis (1, 3). Stage III disease is further subclassified based on
1Departments of Pediatrics, Pediatric Hematology/Oncology and Medicine,Hematology/Oncology, Columbia University Medical Center/New York Presby-terian, New York, New York. 2Department of Medicine, Division of Hematology/Oncology, Columbia University Medical Center/New York Presbyterian, NewYork, New York. 3Columbia University, Columbia College, New York, New York.4Department of Biostatistics, Mailman School of Public Health, Columbia Uni-versity, New York, New York. 5Mailman School of Public Health, ColumbiaUniversity, New York, New York. 6Department of Systems Biology, ColumbiaUniversity, New York, New York. 7PerkinElmer, Hopkinton, Massachusetts.8Columbia University, College of Physician and Surgeons, New York, New York.9Department of Surgery, Columbia University Medical Center/New York Pres-byterian, New York, New York. 10Department of Surgery, Rutgers CancerInstitute, New York, New York. 11Department of Dermatopathology, ColumbiaUniversity Medical Center, New York, New York.
Note: Supplementary data for this article are available at Cancer ImmunologyResearch Online (http://cancerimmunolres.aacrjournals.org/).
Corresponding Author: Yvonne M. Saenger, Columbia University Medical Cen-ter, 161 FortWashingtonAvenue, NewYork, NY 10032. Phone: 212-317-6313; Fax:212-317-6340; E-mail: [email protected]
doi: 10.1158/2326-6066.CIR-17-0360
�2018 American Association for Cancer Research.
CancerImmunologyResearch
www.aacrjournals.org 481
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

volumeof lymphnodemetastasis (1, 3). Unfortunately, completestaging is often not performed because patients are reluctant toundergo lymph node dissection, particularly in light of studiesdemonstrating insignificant impact on clinical outcomes (3, 4).Even for patients who do undergo full clinical staging, a highdegree of heterogeneity among patients within the same stagegroup remains, evidenced by the 50% survival rate at 5 years forstage IIC disease (1). Thus, significant limitations to traditionalstage classification in melanoma exist, impeding identification ofhigh-risk patients who might be expected to obtain the greatestbenefit from either enhanced radiographic surveillance or adju-vant immunotherapy (IO).
IO, which has changed the clinical landscape of metastaticmelanoma, is most effective in lower disease burden, whentumor-mediated immunosuppression is minimal (5). Thus, IOhas the potential to be effective in the adjuvant setting. How-ever, although these agents have demonstrated efficacy inmelanoma, they also introduce the potential for immuneadverse effects (IAE), including colitis, pneumonitis, and myo-carditis (6, 7). In the metastatic setting, there is a highertolerance for IAEs. However, the lack of precise predictive toolshas contributed to stalling the application of IO to the adjuvantsetting due to both the safety concerns and expense of con-ducting these trials in large populations that include many low-risk patients. Thus, prognostic biomarkers are urgently neededto identify which patients are at greatest risk for recurrence andfor stratification of clinical trials (8).
Tumor-infiltrating lymphocytes (TIL), a heterogeneousgroup of lymphocytes within the TME, are a positive prognos-ticator in melanoma (9–16). TIL assessment, however, is sub-ject to significant interobserver variability, thus limiting clinicalutility (11, 12). Detailed analysis of TILs shows that CD8þ
cytotoxic T lymphocytes (CTL) correlate best with survival, butgeneralizable and reproducible methods to analyze TIL com-position have not yet been developed (17). Other cells ofimportance in the TME are macrophages. Although the roleof macrophages has been controversial, discrepancies inreported data are attributable to diverse subgroups of macro-phages that either support an effective antitumor response(M1 type) or promote tumor growth (M2 type; refs. 18–21).M2 macrophages are capable of producing enzymes, includingindoleamine-pyrrole 2,3-dioxygenase (IDO) and arginase,which inhibit CTL activity through tryptophan and L-argininedepletion (22). M2 macrophages have also been found toexpress PD-L1, the known inhibitory ligand of the PD-1 recep-tor found on T-lymphocytes (20). In addition to modulatingCTL function, macrophages are implicated in tumor growth,demonstrating capacity to promote neovascularization throughproduction of angiogenic peptides, including VEGF (23). Giventhat these immunosuppressive mechanisms require eitherdirect contact or close proximity to CTLs, a strong biologicrationale exists for pathologic approaches capable of evaluatingthe spatial relationships between these immune subsets.Although proximity analysis is a limited surrogate for potentialcellular interactions, prior clinicopathologic data in melanomasupport the utility of analyzing spatial localization of immunecells within tumors (24). Thus, the immune score takes intoaccount the position of lymphocyte infiltration within the TME.Macrophage infiltration, specifically when present at the inva-sive front but not within the tumor as a whole, has been shownto correlate with poor survival in stage I/II disease (25).
Although CTLs are known to play a protective role and macro-phages a deleterious one, these findings have not been appliedto clinical practice (26, 27).
In order to address the need for detailed phenotyping ofimmune infiltrates in FFPE samples, we apply quantitative mul-tiplex immunofluorescence (qmIF) to analyze the TME in primarymelanoma tumors (28). QmIF uses a serial IHC approach thatincludes the application of fluorophores of distinct wavelengths,allowing for staining andvisualizationofmultiple antigenswithinthe same tissue specimen. Subsequently, multispectral, high-resolution images are obtained, which are then analyzed usingmachine learning algorithms. This approach allows for moresophisticated computational analysis, including automated phe-notyping for objective density and spatial assessment of immunecell phenotypes within the TME (28–35). QmIF requires iterativetraining to develop tissue and cell classification algorithms (Sup-plementary Figs. S2–S5) and can ultimately augment analysiscapacities beyond traditional IHC evaluation (31–33, 35).
In addition to enhanced automated quantitation of cell phe-notypes over manual review by a pathologist, qmIF is capable ofanalyzing cells based on tissue segmentation to determine wheth-er cells are located in tumor or stromal compartments. Digitalpathology using qmIF offers the ability to perform quantitativespatial analysis (qSA) to evaluate the proximity of individualimmune cell subsets to each other, as well as to tumor cells (28).Precise tissue segmentation and localization of immune cells isnot evaluable with traditional IHC because the manual nature ofanalysis is inherently subjective and introduces observer bias.Digital pathology approaches, using machine-based learningalgorithms to evaluate large tissue areas and complex cell phe-notypes, have been validated across multiple solid tumor types(28–38). Several studies use qSA to study tissue segmentationand distance relationships of multiple cell phenotypes (32, 33,36–39). The importance of tissue segmentation to define preciselocation of lymphocytes within the TME is established by theImmunoscore method, wherein the leading edge of the tumor isdifferentiated from the center of the tumor (2). However, locationof the leading tumor edge generally requires expert pathologyguidance. Thus, Immunoscore has not been applied to primarymelanoma, in part, because it is complicated to reproduciblydefine the leading edge in these small and heterogeneous neo-plasms (8, 32–35). Prior IHCwork, including Immunoscore, doesnot provide qSA of the location of immune cells relative to othercells within the tumor.
In prior work, to more comprehensively characterize theTME, as well as identify a 53 immune gene mRNA panel, ourgroup applied a NanoString assay, comprised principally ofgenes associated with a Th1 immune response, which correlateswith disease-specific survival (DSS) in two independent patientpopulations (13). NanoString assays are both quantitative andnonsubjective but are more costly than IHC and requirehomogenization of tissue, precluding evaluation of spatiallocalization of immune cells. Although the NanoString datadid not suggest a prominent role for macrophage lineage cellsin tumor progression, this might have been due to the lack ofinformation regarding spatial localization of the macrophages.We hypothesized that further spatial characterization of themacrophages, together with additional phenotypic markers,might clarify the role of macrophages in tumor progression.For example, macrophages at the leading tumor edge markhigh-risk patients (40). Markers of activation and antigen
Gartrell et al.
Cancer Immunol Res; 6(4) April 2018 Cancer Immunology Research482
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

presentation, including HLA-DR, aid in the separation of mac-rophage phenotypes, such that HLA-DR� macrophages aremore likely to be inflammatory and HLA-DRþ macrophagesare more likely to favor antitumor immunity (41–43).
Thus, to further expand our capacity to assess the TME, we useqmIF to evaluate stage II to III primary melanoma. We includedCTLs and macrophages as proposed biomarkers, while addingHLA-DR and Ki67 for further evaluation due to previous studiesshowing the addition of thesemarkers to be important features ofimmune cell activation (8, 30, 40, 44). In a cohort of 104 patients(Table 1), we performed tissue segmentation, cellular phenotyp-ing, automated density, and qSA of immune cell subsets. We findthat low CTL/macrophage ratio in the stroma correlated withshortened DSS and overall survival (OS) in stage II to IIImelanoma.
Materials and MethodsPatients and samples
The study was approved by Columbia University MedicalCenter's (CUMC) Institutional Review Board. A patient databaseof stage II to III melanoma patients at CUMC was created retro-spectively by searching surgical pathology records from 2000 to2012 for "melanoma." Dermatopathology reports were firstscreened retrospectively for tumor size, finding tumors 1.01 to
2.00 mm with ulceration and 2.01 to 10 mm. After reviewing1,139 patient records, we identified 765 stage II to III patients. Ofthese 765 patients, 219 had available survival data, defined asknown date of death and/or 24 months documented clinicalfollow-up. Hematoxylin and eosin (H&E) slides were reviewedwith a dermatopathologist, and 183 patients had confirmedtumors, whereas 36 had no melanoma in the residual specimen.Wide local excision and post biopsy specimenswere excluded dueto concerns for immune infiltrate post biopsy, thus leaving 142patients. During the staining process 17 were lost due to tissuedestruction, 19 had staining artifact, 4 were too small, and 2 wereunable to be analyzed using the image analysis software, leaving atotal of 104 analyzable samples (Supplementary Fig. S1; Supple-mentary Table S1). One hundred four patients were analyzed(Table 1), 64 with known recurrence status at the time of lastfollow-up or death (Supplementary Table S2) and 40 patientswith unknown cause of death. This cohort consists ofmore stage II(n ¼ 91) than stage III (n ¼ 13) and more males (n ¼ 75) thanfemales (n¼ 29). Median depth was 2.5 mm, and 65% of tumorswere ulcerated. Fifty-nine and 33 patients had non-brisk TILs andbrisk TILs, respectively, as determined by a dermatopathologist(B.A. Horst), whereas 2 had absent TILs and 10 were not assesseddue to absence of the tumor base (16).
StainingFull-section 5-mm slides of tissue specimens were stained
using Opal multiplex 6-plex kits, according to the manufac-turer's protocol (PerkinElmer), for DAPI, CD3 (clone LN10;Leica; 1:200 dilution), CD8 (clone 4B11; Leica; ready to use:RTU), CD68 (clone KP1; Biogenex, RTU); SOX10 (clone BC34;Biocare; 1:300), HLA-DR (clone LN-3; Abcam; 1:200 dilution),and Ki67 (clone MIB1; Abcam; RTU). Opal multiplexing is aserial immunohistochemistry method that relies on tyramidesignal amplification (TSA; refs. 30, 45), which creates anamplification of signal that then covalently binds to theepitope in a specific manner (27, 46). Primary and secondaryantibody complexes are subsequently removed for serialimmunofluorescence, while the covalent fluorescent signalremains. Single controls and an unstained slide were stainedwith each group of slides.
Multispectral imagingH&E slides were viewed by a dermatopathologist to deter-
mine representative areas for multispectral image capture at20� magnification using Mantra (PerkinElmer Images wereanalyzed using inForm software (PerkinElmer; Fig. 1A–G; Sup-plementary Figs. S2–S5). Five representative areas were chosenby the dermatopathologist: (i) three areas with tumor and up to50% stroma and (ii) two areas with tumor only (at least 90%tumor). These images were factored equally into the analysis foreach patient. Mantra captures spectral information from amultiplexed panel of targets using a multispectral camera. Forsamples of small size, a minimum of two areas meeting theabove criteria were required for inclusion. For spectral unmix-ing, examples of each fluorophore are taken from single-stainedslides for each antibody, as well as a representative autofluor-escence spectrum from an unstained sample. Images from eachof these single-stained and unstained slides were used to createa multispectral library in inForm. Intensity of each fluorescenttarget was extracted from the multispectral data using linearunmixing (47).
Table 1. Melanoma patient characteristics of the OS cohort
(n ¼ 104)Clinical characteristicsGender, n (%)Male 75 (72.1)Female 29 (27.9)
Age, n (range)Median 74.5 (22–96)
Location of tumor, n (%)Trunk 61 (58.7)Extremity 41 (39.4)Unknown 2 (1.9)
Stage, n (%)II 91 (87.5)III 13 (12.5)
Pathologic characteristicsDepth (mm)Median, n (range) 2.5 (0.6–26)
Ulceration, n (%)Absent 36 (34.6)Present 65 (62.5)Unknown 3 (2.9)
TILs, n (%)Absent 2 (1.9)Non-brisk 59 (56.8)Brisk 33 (31.7)Unknown 10 (9.6)
Outcome characteristicsPatient follow-up (months)Median, n (range) 45 (4–173)
OS (months)Alive (at least 2 years), n (%) 31 (29.8)Dead, n (%) 73 (70.2)
DSS (months)Alive or NED at death, n (%) 42 (40.4)Dead with melanoma, n (%) 22 (21.2)Unknown, n (%) 40 (38.4)
Abbreviations: DSS, disease-specific survival; NED, no evidence of disease;TILs, tumor-infiltrating lymphocytes.
QmIF and qSA Define a Biomarker in Melanoma
www.aacrjournals.org Cancer Immunol Res; 6(4) April 2018 483
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

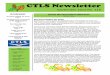
Figure 1.
Characterization of the tumor immunemicroenvironment with qmIF, includingevaluation of spatial distribution ofCTLs relative to tumor cells and CD68þ
macrophages. Processing of slidesdone in inForm (PerkinElmer). Stepsfor analysis using inForm representedusing a single image from 1 patient. A,Multiplex image of a melanoma stainedusing qmIF. DAPI (nuclei, blue), SOX10(tumor, red), CD3 (T cells, cyan), CD8(CTLs, magenta), CD68 (macrophages,green), Ki67 (proliferation marker,yellow), HLA-DR (activation marker,orange). B, Area from the multipleximage (marked by white inset)zoomed in as DAPI only. C, Cellsegmentation of zoomed DAPI image.D–G, Representative analysis stepsof the image in A. D, Tissuesegmentation. E, Phenotyping showingbase phenotypes: macrophages(green), T cells (cyan), tumor (red), andother (blue). F, Scoring withrepresentation of HLA-DR scoring(orange). G, Representative visualexample of nearest-neighbor analysisto evaluate the distance betweenCD3þCD8þ (pink) and SOX10þKi67þ
(yellow). H, Density of CTLs and CD68þ
macrophages (n ¼ 104). CD3þCD8þ
(far left, P < 0.0001); CD3þCD8þHLA-DRþ (middle left, P < 0.0001); CD68þ
(middle right, P < 0.0001); CD68þHLA-DRþ (far right, P < 0.0001). I, Mediandistance of CTLs to SOX10þKi67� (red)or SOX10þKi67þ (blue) grouped (left,P < 0.0001; n ¼ 86). Matched mediandistance to Ki67� and Ki67þ per patient(right). J, Median distance ofCD3þCD8þ to CD68þHLA-DR� (red) orCD68þHLA-DRþ (blue) grouped (left, P< 0.0001; n ¼ 97). Matched mediandistance to HLA-DR� and HLA-DRþ perpatient (right). Macrophages: Mj.Statistical comparison performed usingMann–Whitney test. � , P� 0.05; �� , P�0.01; ��� , P � 0.001; ���� , P � 0.0001.A–G images: white bars ¼ 10 mm.
Gartrell et al.
Cancer Immunol Res; 6(4) April 2018 Cancer Immunology Research484
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

Image analysisImages were analyzed using inForm software (PerkinElmer;
Fig. 1A–G). Tissue segmentation was performed by highlightingexamples of SOX10þ tumor and SOX10� stroma or nontumortissue, allowing the algorithm to "learn" each tissue type andsegment image based on gross morphology (Fig. 1D and Supple-mentary Fig. S2). Supplementary Fig. S2 provides example oftissue segmentation using SOX10 for five images from a singlepatient. Cellular and subcellular compartments were defined by acounterstain (DAPI) to define the nucleus of each cell (Fig. 1B),with each associatedmembrane detected via presence of a specificstain (CD3, CD8, or CD68; Fig. 1C). Cell segmentation wasadjusted based on minimum DAPI signal to accurately locate allcells, splitting of cells in order to avoid hypersegmentation andhyposegmentation, and growing and shrinking the nuclei to fitboth tumor and immune cells (Fig. 1A–C; Supplementary Fig. S3).Supplementary Fig. S3 shows each of the five images from a singlepatient with associated DAPI and cell segmentation of the whole20� image, as well as a zoomed image of the top right cornershowing both DAPI and cell segmentation enlarged. Cells werethen phenotyped by using the phenotyping step of inForm. Ten to15 cells for each base variable were selected to train the phenotyp-ing algorithm: tumor (SOX10þ, red dots), T cells (CD3þ, cyandots), macrophages (CD68þ, green dots), and other (negative forSOX10, CD3, and CD68, blue dots; Fig. 1E; Supplementary Fig.S4). Supplementary Fig. S4 shows representative phenotyping offive images for a single patient. The last step in inFormwas scoring.The images were scored for intensity based on each individualsecondary marker for further phenotyping of HLA-DR, CD8, andKi67 (Fig. 1F; Supplementary Fig. S5). Supplementary Fig. S5shows scoring in the tumor and stroma for CD8 on five imagesfrom a single patient. Finally, data obtained from all representa-tive images were compiled to yield values for each patient. Imagedata were exported from inForm version 2.2.1 (PerkinElmer). TheinForm data from all images for each patient were processed inseparate software designed in RStudio (version 0.99.896; https://github.com/thmshrt/transform_essential). In this software,images were combined and analyzed to concatenate variables(i.e., CD3þCD8þHLA-DRþ) and determine density and distanceof distinct phenotypes. High and low CTL and macrophagedensity was defined as above and low a cutoff defined by CARTanalysis, as well as determined using ROC curves and AUC cutoff.
Statistical analysisAnalysis was completed with GraphPad Prism Version 7.02
(GraphPad Software), and statistical significance was defined asP � 0.05. The need for multiple comparison correction wasbypassed by considering unique nearest neighbors in the analysis,which was analyzed using RStudio version 0.99.896 (CRAN) andSpotfire software (TIBCO). Unique nearest-neighbor analysis wasapplied to define spatial relationships between cellular pheno-types. Median distance was calculated across all images for eachpatient (13).
The effect of the density and distance of immune cell subsets onsurvival was further analyzed using classification and regressiontree (CART) analysis. Kaplan–Meier curves were obtained for DSSandOS in R Version 3.3.1 (CRAN). P values were calculated usingthe log-rank (Mantel–Cox) test. Receiver operating characteristic(ROC) curves, standard univariate and multivariate Cox propor-tional hazards analysis, and Pearson correlation matrix testingwere performed using RStudio.
ResultsCTLs are closer to nondividing tumor cells and to activatedmacrophages
We first sought to characterize the TME in primary melanomausing qmIF. Based on published data suggesting that CTLs limitcancer progression, whereas macrophages promote it, we selectedCTLsandmacrophages as candidatebiomarkers (40).Weanalyzed104 primary tumors for total number of CTLs andmacrophages inboth tumor and stroma (Fig. 1H). In order to characterize the levelof activationof these cell types,wealso includedHLA-DR, amarkerof cellular activation previously shown to predict response to anti-PD1 therapy, andKi67, amarker of cell division (11, 40).CTLs andmacrophages were evaluated based on expression ofHLA-DR (Fig.1H). All immune cells analyzed were significantly more prevalentin the stroma than in the tumor (Fig. 1H).
We next applied qSA, using nearest-neighbor analysisto evaluate relationships between expression of Ki67 andHLA-DR on macrophages and tumor cells and spatial locali-zation of these cells to CTLs. We found that CTLs were spatiallycloser to tumor cells when they were not proliferating (Ki67�;P < 0.0001; Fig. 1I, left). When evaluating each patient indi-vidually, we showed CTLs were closer to nonproliferatingtumor cells in nearly all samples having both Ki67þ and Ki67�
tumor cells (n ¼ 86; Fig. 1I, right). This result is consistent withthat reported in the literature showing that melanomas withhigher rates of proliferation have lower frequencies of infil-trating CTLs (18).
We found that HLA-DR is expressed on CD68þmacrophages,CTLs, and, as previously reported, melanoma cells (9). Weevaluated the distance of CTLs to SOX10þ tumor and CD68þ
macrophages using nearest-neighbor analysis. We found thatCTLs were closer to CD68þ macrophages when they wereHLA-DRþ (P < 0.0001; Fig. 1J, left). The median CTL distanceto macrophages is shown for individual patients matched forboth HLA-DRþ and HLA-DR� cells (n ¼ 97; Fig. 1J, right).HLA-DR expression on tumor cells did not significantly impactdistance to CTLs (P ¼ 0.0846; Supplementary Fig. S6A).
CTL infiltration correlates inversely with risk of death frommelanoma
Among the 104 patients included, we performed a subsetanalysis on 64 patients for whom cause of death was known(Supplementary Table S2) to determine whether density of CTLsin tumor or stroma correlate with DSS. Marked differences in thedensity of CTLs were observed between patients, as depictedin Fig. 2A and B with tumor specimens demonstrating high andlow CTL infiltration, respectively.
We next evaluated density of CTLs in the stroma and tumorusing CART analysis to determine whether density could stratifypatients in terms of DSS. Specifically, using CART cutoffs, wecreated KM curves to assess the effect of CTL density on DSS inboth tumor and stroma. We found that a high density of CTLs inthe stroma (P ¼ 0.0038) and tumor (P ¼ 0.0147) correlatedwith DSS (Fig. 2C and D), consistent with prior reports thatCTLs conferred favorable prognosis (10–12, 17, 43). We nextevaluated whether subsets of CTLs might predict prognosis moreaccurately. The density of CTLs expressing HLA-DR (activatedT cells) correlated significantly with DSS in the stroma (P ¼0.0005; Fig. 2E) but was less significantly correlated in tumor(P ¼ 0.0167; Fig. 2F). Ki67-expressing CTLs, however, did not
QmIF and qSA Define a Biomarker in Melanoma
www.aacrjournals.org Cancer Immunol Res; 6(4) April 2018 485
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

correlate with DSS in the stroma (P ¼ 0.1737; SupplementaryFig. S6B) or tumor (P ¼ 0.2161; Supplementary Fig. S6C). Thus,assessment of an activation marker appeared to enhance cor-relation with DSS, whereas including a proliferation markerreduced the correlation between CTL density and DSS.
We further analyzed CTLs by evaluating their distance to pro-liferating (SOX10þKi67þ) and nonproliferating (SOX10þKi67�)
tumor cells. As stated above (Fig. 1I), CTLs were preferentiallylocated closer to SOX10þKi67� cells.We found that close distanceof CTLs to nonproliferating tumor cells (Ki67�) stratified DSS(P ¼ 0.0006; Fig. 2G). However, the distance of CTLs toproliferating tumor cells (Ki67þ) did not significantly correlatewith DSS (P ¼ 0.0618; Fig. 2H). The distance of CTLs to tumorcells, with or without HLA-DR expression, also did not effect
Figure 2.
Infiltration of CTLs in tumor andstroma and distance of CTLs tononproliferating tumor cellsassociates with DSS. Melanoma slideswere stained for qmIF with DAPI(blue), SOX10 (red), CD3 (cyan),CD8 (magenta), CD68 (green),Ki67 (yellow), and HLA-DR (orange).Multiplex images of melanomashowing (A) high and (B) lowinfiltration of CTLs in tumor.Kaplan–Meier (KM) curves werecreated using classification andregression tree (CART) analysis foreach variable shown in C–H. C, High(n ¼ 57) and low (n ¼ 7) densityof CD3þCD8þ cells in the stroma(P¼0.0038).D,High (n¼ 38) and low(n¼ 26) CD3þCD8þ cells in the tumor(P ¼ 0.0147). E, High (n ¼ 57) andlow (n¼ 7) density of CD3þCD8þHLA-DRþ cells in the stroma (P ¼ 0.0005).F, High (n ¼ 38) and low (n ¼ 26)density of CD3þCD8þHLA-DRþ cells inthe tumor (P ¼ 0.0167). G, Far (n ¼ 7)and close (n ¼ 54) distance ofCD3þCD8þ cells to SOX10þKi67�
tumor cells (P ¼ 0.0006). H, Far(n ¼ 25) and close (n ¼ 29) distancefrom CD3þCD8þ cells toproliferating (SOX10þKi67þ) tumorcells (P ¼ 0.0618). Statisticalcomparison performed using log-rank(Mantel–Cox) test. ns, not significant(P > 0.05); � , P � 0.05; �� , P � 0.01;��� , P � 0.001; ���� , P � 0.0001.White bars in A and B, 10 mm.
Gartrell et al.
Cancer Immunol Res; 6(4) April 2018 Cancer Immunology Research486
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

DSS (P ¼ 0.8436 and P ¼ 0.0899, respectively; SupplementaryFig. S6D and S6E).
HLA-DR�macrophagedensity correlateswithhigh riskof deathfrom melanoma
Because we determined that CTLs, particularly in the stroma,correlatedwith a favorable prognosis,wenext evaluateddensity ofCD68þ macrophages in each patient with complete clinicalfollow-up. Figure 3A shows a representative multiplex imagefrom a melanoma tumor with CD68þ macrophage infiltrate,and Fig. 3B shows the same image with only CD68 and DAPIstaining to demonstrate how these cells were visualized. UsingCART cutoffs, we created KM curves evaluating the effect ofCD68þ macrophage density on DSS in both the tumor andstroma. In contrast to CTLs, high density of macrophages in thestroma (P¼ 0.0006) and tumor (P¼ 0.0426) was associated withpoor DSS (Fig. 3C and D). Based on our evaluation of macro-phages with and without HLA-DR, we found that high density ofHLA-DR� macrophages in stroma (P ¼ 0.0013, Fig. 3E) andtumor (P¼ 0.0163, Supplementary Fig. S6F) indicated poor DSS.However, density of HLA-DRþ macrophages in the stroma (P ¼0.0637) and tumor (P ¼ 0.1027) had no significant impacton survival (Fig. 3F; Supplementary Fig. S6G). Thus, CD68þ
macrophages in the stroma, but not in the tumor, correlatedwith DSS, and this correlation was substantially driven by theHLA-DR� macrophage subset.
Given that macrophage density was associated with poorsurvival, we next tested whether the distance of CTLs to macro-phages with or without HLA-DR correlated with survival. Wefound that close distance of CTLs to CD68þHLA-DR� macro-phages segregated with shorter DSS (P ¼ 0.0016; Fig. 3G). Closedistance of CTLs to CD68þHLA-DRþmacrophages also indicatedpoor prognosis but was less robust (P ¼ 0.0388; Fig. 3H). Thus,HLA-DR�macrophages in the stroma conferred a poor prognosis,and the distance between HLA-DR� macrophages and CTLs alsowas associated with survival, with a shorter distance indicatingpoor outcome.
Low CTL/macrophage is associated with inferior survival instage II to III melanoma
Because we determined that CTLs associated with prolongedsurvival, whereas macrophages in the stroma associated withshortened survival, we sought to integrate these cell types intoone biomarker for clinical application.We first tested whether thedistance between the twomost impactful populations in terms ofsurvival, CTLs and HLA-DR� macrophages, segregated with clin-ical outcome. Figure 4A shows a representativemultiplex image ofa melanoma tumor containing CD68þHLA-DR� macrophagesand a selected region containing CD68þHLA-DR� macrophages,designated by white arrows (Fig. 4A, inset). We further analyzedand compared distance of CTLs to HLA-DR� macrophages usingan ROC curve to find the area under the curve (AUC) for deathfrom melanoma over the time of follow-up. We found that thedistance of CTLs to HLA-DR� macrophages was significant viaROC (AUC ¼ 0.682, P ¼ 0.011, cutoff ¼ 165.54 pixels; Fig. 4B,left). Using the AUC cutoff (165.54) to create a binary analysisof the 61 patients with distance values, excluding 3 patientswith no CTLs, to evaluate DSS and Cox proportional hazards(Supplementary Table S3), we found that close distance ofCTLs to HLA-DR� macrophages correlated with shorter survival(P ¼ 0.0077; Fig. 4B, right).
Consistent with our hypothesis that the densities of CTLs andmacrophages both have a significant impact on survival, wesought to analyze the ratio of these cells in each patient to createamore clinically impactful biomarker that would also allow us toinclude patients for whom there are no CTLs detected in thesample. We found that a low CTL/macrophage ratio wassignificant for death from melanoma using ROC (AUC ¼0.724, P ¼ 0.026, cutoff ¼ 2.557; Fig. 5A). We then used theAUCcutoff to create a binary analysis of all 64patientswithDSS toanalyze, using a KM curve. We found that a low CTL/macrophageratio predicted poor prognosis (P¼ 0.0033; Fig. 5B). UnivariableCox analysis showed that a low CTL/macrophage ratio indicatedpoor prognosis [P ¼ 0.006; hazards ratio (HR) ¼ 3.719, 95%confidence interval (CI) ¼ 1.451–9.533; Fig. 5D]. In this popu-lation of 64 patients, among other clinical parameters includingstage, gender, age, location and depth, only stage was found to besignificant (Fig. 5D). Multivariable Cox regression was mostsignificant when stage, ulceration, and CTL/macrophage ratiowere included (P ¼ 0.002; Fig. 5D). Further analysis found thatlow CTL/macrophage ratio also correlated with poor DSS at the2-year and 5-year time points (Supplementary Fig. S7).
To further evaluate the robustness of the CTL/macrophage ratioin predicting prognosis, we analyzed all 104 patients for OS (notethat the cause of death was not known for all the patients). Usingthe AUC cutoff (2.557) to create a binary of all patients to evaluateusing a KM curve, we found that a low CTL/macrophage ratiopredicted poorOS (P¼ 0.0076; Fig. 5C).Univariable Cox analysisshowed that a low CTL/macrophage ratio indicated poor prog-nosis (P ¼ 0.009, HR ¼ 1.873, 95% CI ¼ 1.170–2.997), whereasall other variables were not found to be significant (Fig. 5D).Contrary to DSS, multivariable analysis in the OS cohort of 104patients showed that ulceration and stage did not enhance therobustness of the model (P ¼ 0.066; Fig. 5D). We found that theCTL/macrophage ratio in the stroma correlated with the presenceof TILs, using Pearson correlationmatrix (Table 2). No significantcorrelation between the densities of CTLs and macrophages wasfound, suggesting that they play independent roles in tumorprogression (P ¼ 0.225, Table 2; Supplementary Table S4).
DiscussionTechnological advances using machine learning allow for pre-
cise and reproducible quantitation of immune populations with-in the TMEusingqmIF (30, 41, 48–50). TheOpal stainingmethodcombined with qmIF imaging and analysis, unlike other multi-plex methods, allows for evaluation using a single slide ratherthan layering of stains using multiple slides (43). Multiplexstaining of a single slide using qmIF provides high resolution ofeach individual cell, thereby allowing for tissue segmentation,multiparameter phenotyping of cells, and precise qSA, all ofwhichwere not previously possible. Althoughpathology expertiseis required for the initial training algorithm, automation ofsubsequent image analysis minimizes subjectivity of interpreta-tion. Because qmIF offers the advantage of using a single slide forprocessing and automation for analysis, thismethodwill bemoreclinically applicable, especially for predictive biomarkers andmayalso be useful diagnostically. QmIF has been successfully per-formed in multiple tumor types, including melanoma, breastcancer, lung cancer, and Hodgkin lymphoma (41, 48–50). Spe-cifically, this method was successfully used using 6-plex qmIF toevaluate 17patientswithmelanoma,finding that the ratio ofCTLs
QmIF and qSA Define a Biomarker in Melanoma
www.aacrjournals.org Cancer Immunol Res; 6(4) April 2018 487
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

to PD-L1 or FOXP3 is capable of predicting TIL generationfollowing adoptive T-cell therapy (51). For our study, we pro-posed a biomarker developed using this technique that incorpo-rates both density assessment, including precise tissue segmen-
tation and multiparameter phenotyping, and qSA in early-stagemelanoma patients (13, 52).
We achieved precise tissue segmentation with automated dif-ferentiation of tumor from stroma through qmIF analysis of
Figure 3.
High infiltration of CD68þ
macrophages in the tumor and stromaand close distance of CTLs to HLA-DR�
macrophages associates with poorDSS.A,Multiplex image of amelanomaslide stained using qmIF for DAPI(blue), SOX10 (red), CD3 (cyan),CD8 (magenta), CD68 (green),Ki67 (yellow), and HLA-DR (orange).B, Multiplex image of melanomashowing DAPI (blue) and CD68(green) for macrophages. KM curveswere created using CART analysis foreach variable shown in C–H. C, High(n ¼ 7) and low (n ¼ 57) density ofCD68þ macrophages in the stroma(P¼0.0006).D,High (n¼ 55) and low(n¼9) density of CD68þmacrophagesin the tumor (P ¼ 0.0426). E, High(n ¼ 18) and low (n ¼ 46) density ofCD68þHLA-DR� macrophages in thestroma (P ¼ 0.0013). F, High (n ¼ 10)and low (n ¼ 54) density ofCD68þHLA-DRþ macrophages instroma (P ¼ 0.0637). G, Far (n ¼ 47)and close (n ¼ 14) distance of CTLs toHLA-DR� macrophages (P ¼ 0.0016).H, Far (n ¼ 9) and close (n ¼ 52)distance of CTLs to HLA-DRþ
macrophages (P ¼ 0.0388). Statisticalcomparison performed using log-rank(Mantel–Cox) test. ns: not significant(P > 0.05); � , P � 0.05; �� , P � 0.01;��� , P � 0.001; ���� , P � 0.0001).White bars in A and B, 10 mm.
Gartrell et al.
Cancer Immunol Res; 6(4) April 2018 Cancer Immunology Research488
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

the TME. This analysis was built on prior IHC literature demon-strating that macrophages in the peritumor stroma were moresignificant to clinical outcome than those within the tumorproper. This builds on prior research showing that macrophagesat the "leading edge" of the tumor are prognostic, but ourautomated method for tissue segmentation allows for potentialrapid clinical application across institutions (13, 24). Because the
qmIF method allows for quantification of cells with multipleconcatenated markers, as well as automated assessment of mor-phology, we were able to accurately define the CTL/macrophageratio specifically within the tumor-associated stroma, allowingfor a precise and quantifiable biomarker. The potential for qmIFto allow for qSA exists, by evaluating the minimum distancebetween different cell phenotypes using nearest-neighbor
Figure 4.
Close distance of CD68þHLA-DR� macrophages to CTLs associates with poor prognosis in stage II to III melanoma. A, Multiplex image of melanoma withselected region (left) shown again, including only HLA-DR, DAPI, and CD68 stains (right). White arrows: HLA-DR� macrophages. B, ROC curve for distanceof CTLs to HLA-DR� macrophages (Mj; n ¼ 61, AUC ¼ 0.682, P ¼ 0.011) and KM curve using the AUC cutoff (P ¼ 0.0077), far (n ¼ 42), close (n ¼ 19).Statistical comparison performed using log-rank (Mantel–Cox) test.�� , P � 0.01. White bars in A and inset, 10 mm.
QmIF and qSA Define a Biomarker in Melanoma
www.aacrjournals.org Cancer Immunol Res; 6(4) April 2018 489
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

analysis. Using qSA, we can analyze distance to and fromdifferent immune cells, as well as immune cell distance to indi-vidual tumor cells.
In terms of prognosis, also consistent with prior IHC literature,we found that high density of CTLs, particularly in the stroma,wasa favorable indicator (13). Specifically, we found that CTLs in thestroma were significantly more prognostic than overall CD8density with both ROC and univariable Cox analysis. The factthat CTL density within each compartment of the tissue wasmoresignificant than total density without tissue segmentation mayindicate that there is a biologic difference between tumor andstroma, as identified by our algorithm, such that each is bestevaluated independently.
The CTL density in the tumor was also favorable but lesssignificant. This may have been due to the increased CTL densityin the stroma in comparison to the tumor, impacting statisticalanalysis, but may also indicate that the biology of the stroma ismore critical for progression. Among CTLs, the activated HLA-DRþ subset was prognostic, whereas dividing, Ki67þ CTLs hadfewer effects, suggesting that activation status of CTLs affectsclinical outcome. Using qSA, our findings showed that CTLs werespatially closer to nondividing tumor cells (Ki67�) and activatedmacrophages (HLA-DRþ), consistent with established findingsthat melanomas with a high proliferation rate are less infiltrated(13). CTLs may inhibit melanoma differentiation, or rapidlygrowing tumor may exclude CTLs. Close spatial proximity
Figure 5.
Establishing CTL/macrophage ratio in stroma as a biomarker for stage II to III melanoma. CTL/macrophage ratio in the stroma using the ROC curve andthe Cox proportional hazards model. A, ROC curve for the CTL/macrophage ratio in the stroma (n ¼ 64, AUC ¼ 0.724, P ¼ 0.026, cutoff ¼ 2.557). B, DSS KMcurve using the AUC cutoff (P ¼ 0.0033 in 64 patients, high (n ¼ 33), low (n ¼ 31)). C, Overall survival (OS) KM curve using the AUC cutoff [n ¼ 104, P ¼ 0.0076,high (n ¼ 52), low (n ¼ 52)]. D, Univariable and multivariable Cox analysis of DSS (n ¼ 64) and OS (n ¼ 104) patients. Statistical comparison for DSS andOS performed using log-rank (Mantel–Cox) test. Values in bold are significant at P � 0.05. � , P � 0.05; �� , P � 0.01; ��� , P � 0.001; ���� , P � 0.0001.
Gartrell et al.
Cancer Immunol Res; 6(4) April 2018 Cancer Immunology Research490
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

of CTLs to nonproliferating tumor (Ki67�) segregated withgood DSS, perhaps because proximity allowed for cytotoxicantitumor activity.
Although spatial proximity is a limited surrogate for interactionbetween cells, our finding that close proximity of CTLs to HLA-DR�macrophages was associated with poor survival is consistentwith the hypothesis that interactions between CTLs and macro-phages promote inflammation and impair antitumor immunity.Further functional studies are needed to delineate the role spatialproximity plays in facilitating cellular communication within theTME. In the evaluation of macrophage density segmentation, ourfindings showed that high density of CD68þ macrophages, par-ticularly in the stroma, strongly conferred an unfavorable prog-nosis in stage II to III melanoma and was driven by HLA-DR�
macrophages, as HLA-DRþ macrophages did not significantlyaffect prognosis. No direct correlation between CTL density andmacrophage density was found, implying two distinct biologicprocesses. Macrophages, thus, may cause local tissue destruction,increasing tumor growth via a mechanism not directly related toCTLs or antitumor immunity (53–55).
Our proposed biomarker, the CTL/macrophage ratio, is con-sistent with our original hypothesis that CTLs play a favorablerole, whereas macrophages play a deleterious one. Distancebetween CTLs and HLA-DR� macrophages was also prognostic,raising the possibility that interactions between these two subsetsmay inhibit immune surveillance by the CTLs. Specifically, thestromal CTL/macrophage ratio demonstrated superior prognosticvalue over independent CTL and macrophage density, with thehighest AUC on ROC analysis. Consistent with the prior literatureshowing thatmacrophage densitywithin the leading edge, but notthe center of the tumor, is prognostic, we found no correlation byCox between macrophage density within the tumor and clinicaloutcome. Thus, focusing on the stroma avoids including addi-tional macrophage data that may dilute the predictive power ofthe biomarker.
One limitation to our study was that IHC analysis wassubject to an inherent sampling bias due to heterogeneity. Inorder to address tissue heterogeneity, we sampled five repre-sentative areas determined by a trained dermatopathologistwho was blinded to the clinical data. Notably, pathologistshave been able to reproducibly evaluate TIL infiltration basedon representative areas of the tumor suggesting that there islimited variability in assessment between pathologists (12, 55).Although pathology expertise is required for the initial trainingalgorithm, automation of subsequent image analysis mini-mizes subjectivity of interpretation. In the future, it may be
possible to apply additional machine learning algorithms toeliminate the role of the pathologist and, thus, any possiblesubjectivity in image selection. A second limitation of our studywas that all 104 patients came from a single center. We werealso not able to analyze 42 patients due to poor tissue quality,suggesting that further technical refinement is needed, partic-ularly in specimens stored for longer than 10 years and for verysmall tumors. Validation in additional populations is neededfor clinical application.
In this work, we presented a quantitative analysis combiningassessment of multiparameter immune phenotypes, tissuesegmentation, and qSA in primary melanoma using qmIF.Using this method, we also identified a biomarker for potentialclinical application, demonstrating the value of this approach.Our findings were consistent with known biology of primarymelanoma tumors and provide a more quantitative andaccurate biomarker in the population studied than the standardTIL analysis, which demonstrated only borderline significance.An accurate prognostic clinical biomarker in early-stage mela-noma is needed to select patients in the development oftherapeutic adjuvant protocols. This is of particular importancegiven that melanoma may recur years after diagnosis, furthercomplicating the development of predictive biomarkers in anever-changing immunotherapy landscape. QmIF as a platformhas significant, and untapped, potential for defining novelbiomarkers. The CTL/macrophage ratio in the stroma ofprimary melanoma tumors merits further development as abiomarker for clinical application.
Disclosure of Potential Conflicts of InterestR.D. Gartrell has presented at workshops for PerkinElmer, for which she
received travel reimbursement. H.L. Kaufman is CMO at Replimune and is aconsultant/advisory board member for SapVax and EMD Serono. No potentialconflicts of interest were disclosed by the other authors.
DisclaimerThe content is solely the responsibility of the authors and does not neces-
sarily represent the official views of the NIH.
Authors' ContributionsConception and design: R.D. Gartrell, Y.M. SaengerDevelopment of methodology: R.D. Gartrell, D.K. Marks, Y. Lu, E.C. Stack,R. Rabadan, B.A. Horst, Y.M. SaengerAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): R.D. Gartrell, D.K. Marks, T.D. Hart, D.T. Jia,P.M. Armenta, Y. Fu, D. Izaki, H.L. Kaufman, B.A. Horst, Y.M. SaengerAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): R.D. Gartrell, D.K. Marks, T.D. Hart, G. Li,
Table 2. Pearson correlation matrix
Variables Details Age Stage Location Depth Ulceration TILsCD68þ
stromaCD8/CD68stroma
CD8þ
stroma
Age �55 vs. <55 1 �0.333 0.026 �0.006 �0.071 �0.008 �0.038 �0.066 �0.051Stage III vs. II �0.333 1 �0.127 �0.139 �0.215 �0.115 �0.089 �0.238 �0.031Location Extremity vs. trunk 0.026 �0.127 1 �0.006 �0.051 0.171 �0.039 �0.002 0.083Depth �2 mm vs. <2 mm �0.006 �0.139 �0.006 1 �0.269 0.054 �0.079 �0.060 �0.224Ulceration Positive vs. negative �0.071 �0.215 �0.051 �0.269 1 0.005 0.026 0.044 0.145TILs Absent, non�brisk,
brisk�0.008 �0.115 0.171 0.054 0.005 1 �0.072 �0.265 �0.504
CD68þ stroma High vs. low �0.038 �0.089 �0.039 �0.079 0.026 �0.072 1 0.584 0.162CD8/CD68 stroma Low vs. high �0.066 �0.238 �0.002 �0.060 0.044 �0.265 0.584 1 0.564CD8þ stroma Low vs. high �0.051 �0.031 0.083 �0.224 0.145 �0.504 0.162 0.564 1
NOTE: Correlation of CTL/macrophage ratio with TILs (P¼ 0.044), CD8þ stroma (P < 0.0001), and CD68þ stroma (P < 0.0001). Correlation with depth, ulceration,age, and stage also shown. n ¼ 58; 6 patients were removed due to unknown status for ulceration or TILs.Values in bold are significant at P � 0.05.
QmIF and qSA Define a Biomarker in Melanoma
www.aacrjournals.org Cancer Immunol Res; 6(4) April 2018 491
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

D.R. Davari, A. Wu, K.N. Askin, A. Monod, E.C. Stack, D.T. Jia, D. Izaki,R. Rabadan, H.L. Kaufman, C.G. Drake, Y.M. SaengerWriting, review, and/or revision of the manuscript: R.D. Gartrell, D.K. Marks,T.D. Hart, G. Li, D.R. Davari, Z. Blake, K.N. Askin, A.Monod, E.C. Stack, D.T. Jia,Y. Fu, B. Taback, R. Rabadan, H.L. Kaufman, C.G. Drake, B.A. Horst,Y.M. SaengerAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases):R.D.Gartrell,D.K.Marks, T.D.Hart, D.R.Davari,Z. Blake, C.L. Esancy, D.T. Jia, B.A. Horst, Y.M. SaengerStudy supervision: Y.M. Saenger
AcknowledgmentsThis publication was supported by the National Center for Advancing
Translational Sciences, National Institutes of Health, through grant
number 1TL1TR001875-01 (R.D. Gartrell, W.K. Chung, PI) and NationalCancer Institute Cancer Clinical Investigator Team Leadership Award,supplement to Herbert Irving Comprehensive Cancer Center Supportthrough grant number P30 CA013696-41 (R.D. Saenger, S.G. Emerson,PI). This project also received funding from Swim Across America (R.D.Gartrell) and the 2014 Landon Foundation–AACR Innovator Award for CancerImmunology Research, grant number 14-20-27-SAEN (Y.M. Saenger).
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received July 13, 2017; revised November 6, 2017; accepted February 15,2018; published first February 21, 2018.
References1. Balch CM, Gershenwald JE, Soong SJ, Thompson JF, Atkins MB, Byrd DR,
et al. Final version of 2009 AJCC melanoma staging and classification.J Clin Oncol 2009;27:6199–206.
2. Galon J, Fox BA, Bifulco CB, Masucci G, Rau T, Botti G, et al. Immunoscoreand Immunoprofiling in cancer: an update from the melanoma andimmunotherapy bridge 2015. J Transl Med 2016;14:273.
3. Balch CM, Gershenwald JE, Soong SJ, Thompson JF, Ding S, Byrd DR, et al.Multivariate analysis of prognostic factors among 2,313 patients with stageIII melanoma: comparison of nodal micrometastases versus macrometas-tases. J Clin Oncol 2010;28:2452–9.
4. Faries MB, Thompson JF, Cochran AJ, Andtbacka RH,Mozzillo N, Zager JS,et al. Completion dissection or observation for sentinel-nodemetastasis inmelanoma. N Engl J Med 2017;376:2211–22.
5. Gulley JL, Arlen PM, Madan RA, Tsang KY, Pazdur MP, Skarupa L, et al.Immunologic and prognostic factors associated with overall survivalemploying a poxviral-based PSA vaccine in metastatic castrate-resistantprostate cancer. Cancer Immunol Immunother 2010;59:663–74.
6. Eggermont AM, Chiarion-Sileni V, Grob JJ, Dummer R, Wolchok JD,Schmidt H, et al. Prolonged survival in stage III melanoma with ipilimu-mab adjuvant therapy. N Engl J Med 2016;375:1845–55.
7. Johnson DB, Balko JM, Compton ML, Chalkias S, Gorham J, Xu Y, et al.Fulminant myocarditis with combination immune checkpoint blockade.N Engl J Med 2016;375:1749–55.
8. Sivendran S, Chang R, Pham L, Phelps RG, Harcharik ST, Hall LD, et al.Dissection of immune gene networks in primarymelanoma tumors criticalfor antitumor surveillance of patients with stage II-III resectable disease.J Invest Dermatol 2014;134:2202–11.
9. LeeN, Zakka LR,MihmMCJr, Schatton T. Tumour-infiltrating lymphocytesin melanoma prognosis and cancer immunotherapy. Pathology 2016;48:177–87.
10. Clemente CG, Mihm MC Jr, Bufalino R, Zurrida S, Collini P,Cascinelli N. Prognostic value of tumor infiltrating lymphocytes inthe vertical growth phase of primary cutaneous melanoma. Cancer1996;77:1303–10.
11. Azimi F, Scolyer RA, Rumcheva P, Moncrieff M, Murali R, McCarthy SW,et al. Tumor-infiltrating lymphocyte grade is an independent predictor ofsentinel lymph node status and survival in patients with cutaneousmelanoma. J Clin Oncol 2012;30:2678–83.
12. Busam KJ, Antonescu CR, Marghoob AA, Nehal KS, Sachs DL, Shia J, et al.Histologic classification of tumor-infiltrating lymphocytes in primarycutaneous malignant melanoma. A study of interobserver agreement. AmJ Clin Pathol 2001;115:856–60.
13. Gajewski TF, Schreiber H, Fu YX. Innate and adaptive immune cells in thetumor microenvironment. Nat Immunol 2013;14:1014–22.
14. Ladanyi A. [Prognostic value of tumor-infiltrating immune cells in mel-anoma]. Magy Onkol 2013;57:85–95.
15. Mihm MC Jr, Mule JJ. Reflections on the histopathology of tumor-infiltrating lymphocytes in melanoma and the host immune response.Cancer Immunol Res 2015;3:827–35.
16. Elder DE, Guerry Dt, VanHorn M, Hurwitz S, Zehngebot L, Goldman LI,et al. The role of lymph node dissection for clinical stage I malignantmelanoma of intermediate thickness (1.51–3.99 mm). Cancer 1985;56:413–8.
17. Erdag G, Schaefer JT, Smolkin ME, Deacon DH, Shea SM, Dengel LT, et al.Immunotype and immunohistologic characteristics of tumor-infiltratingimmune cells are associated with clinical outcome in metastatic melano-ma. Cancer Res 2012;72:1070–80.
18. Komohara Y, Jinushi M, Takeya M. Clinical significance of macrophageheterogeneity in human malignant tumors. Cancer Sci 2014;105:1–8.
19. Ostuni R, Kratochvill F,Murray PJ,NatoliG.Macrophages and cancer: frommechanisms to therapeutic implications. Trends Immunol 2015;36:229–39.
20. Schupp J, Krebs FK, Zimmer N, Trzeciak E, Schuppan D, Tuettenberg A.Targeting myeloid cells in the tumor sustaining microenvironment. CellImmunol 2017;2017 Nov 2. pii: S0008-8749(17)30190-9.
21. Mills CD, Kincaid K, Alt JM, Heilman MJ, Hill AM. M-1/M-2 macrophagesand the Th1/Th2 paradigm. J Immunol 2000;164:6166–73.
22. van Baren N, Van den Eynde BJ. Tumoral immune resistance mediatedby enzymes that degrade tryptophan. Cancer Immunol Res 2015;3:978–85.
23. Corliss BA, AzimiMS,Munson JM, Peirce SM,MurfeeWL.Macrophages: aninflammatory link between angiogenesis and lymphangiogenesis. Micro-circulation 2016;23:95–121.
24. Jensen TO, Schmidt H,Moller HJ, HoyerM,ManieckiMB, Sjoegren P, et al.Macrophage markers in serum and tumor have prognostic impact inAmerican Joint Committee on Cancer stage I/II melanoma. J Clin Oncol2009;27:3330–7.
25. Tsujikawa T, Kumar S, Borkar RN, Azimi V, Thibault G, Chang YH, et al.Quantitative multiplex immunohistochemistry reveals myeloid-inflamedtumor-immune complexity associated with poor prognosis. Cell Rep2017;19:203–17.
26. Garcia-Martinez E, Gil GL, Benito AC, Gonzalez-Billalabeitia E, ConesaMA,GarciaGarcia T, et al. Tumor-infiltrating immune cell profiles and theirchange after neoadjuvant chemotherapy predict response and prognosis ofbreast cancer. Breast Cancer Res 2014;16:488.
27. Mansfield JR. Multispectral imaging: a review of its technical aspects andapplications in anatomic pathology. Vet Pathol 2014;51:185–210.
28. Ali HR, Dariush A, Provenzano E, Bardwell H, Abraham JE, Iddawela M,et al. Computational pathology of pre-treatment biopsies identifies lym-phocyte density as a predictor of response to neoadjuvant chemotherapy inbreast cancer. Breast Cancer Res 2016;18:21.
29. Chang AY, Bhattacharya N, Mu J, Setiadi AF, Carcamo-Cavazos V, Lee GH,et al. Spatial organization of dendritic cells within tumor draining lymphnodes impacts clinical outcome in breast cancer patients. J Transl Med2013;11:242.
30. Stack EC, Wang C, Roman KA, Hoyt CC. Multiplexed immunohisto-chemistry, imaging, and quantitation: a review, with an assessment oftyramide signal amplification, multispectral imaging and multiplexanalysis. Methods 2014;70:46–58.
31. Peck AR, Girondo MA, Liu C, Kovatich AJ, Hooke JA, Shriver CD, et al.Validation of tumor protein marker quantification by two independentautomated immunofluorescence image analysis platforms. Mod Pathol2016;29:1143–54.
32. Carstens JL, Correa de Sampaio P, Yang D, Barua S, Wang H, Rao A, et al.Spatial computation of intratumoral T cells correlates with survival ofpatients with pancreatic cancer. Nat Commun 2017;8:15095.
Gartrell et al.
Cancer Immunol Res; 6(4) April 2018 Cancer Immunology Research492
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

33. Feng Z, Bethmann D, Kappler M, Ballesteros-Merino C, Eckert A, Bell RB,et al.Multiparametric immuneprofiling inHPV-oral squamous cell cancer.JCI Insight 2017;2. pii: 93652.
34. Kawakami F, Sircar K, Rodriguez-Canales J, Fellman BM, Urbauer DL,Tamboli P, et al. Programmed cell death ligand 1 and tumor-infiltratinglymphocyte status in patients with renal cell carcinoma and sarcomatoiddedifferentiation. Cancer 2017;123:4823–31.
35. Carey CD, Gusenleitner D, Lipschitz M, Roemer MGM, Stack EC, Gjini E,et al. Topological analysis reveals a PD-L1 associated microenvironmentalniche for Reed-Sternberg cells in Hodgkin lymphoma. Blood 2017;130:2420–30.
36. Yeong J, Thike AA, Lim JC, Lee B, Li H, Wong SC, et al. Higher densities ofFoxp3þ regulatory T cells are associated with better prognosis in triple-negative breast cancer. Breast Cancer Res Treat 2017;163:21–35.
37. Nawas S HA, Koelbe K, Yuan Y. Beyond immune density: critical role ofspatial. Mod Pathol 2015;28:766–77.
38. Algars A, Irjala H, Vaittinen S, Huhtinen H, Sundstrom J, Salmi M, et al.Type and location of tumor-infiltrating macrophages and lymphaticvessels predict survival of colorectal cancer patients. Int J Cancer 2012;131:864–73.
39. Galon J, Bindea G, Mlecnik B, Angell H, Lagorce C, Todosi AM, et al.[Intratumoral immunemicroenvironment and survival: the immunoscore].Med Sci (Paris) 2014;30:439–44.
40. Johnson DB, Estrada MV, Salgado R, Sanchez V, Doxie DB, Opalenik SR,et al. Melanoma-specific MHC-II expression represents a tumour-autono-mous phenotype and predicts response to anti-PD-1/PD-L1 therapy.Nat Commun 2016;7:10582.
41. Barbieri G, Rimini E, CostaMA. Effects of human leukocyte antigen (HLA)-DR engagement on melanoma cells. Int J Oncol 2011;38:1589–95.
42. Ma J, Liu L, Che G, Yu N, Dai F, You Z. The M1 form of tumor-associatedmacrophages in non-small cell lung cancer is positively associated withsurvival time. BMC Cancer 2010;10:112.
43. Colloby PS,West KP, Fletcher A. Is poor prognosis really related toHLA-DRexpressionbymalignantmelanoma cells?Histopathology1992;20:411–6.
44. Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJ, Robert L, et al.PD-1 blockade induces responses by inhibiting adaptive immune resis-tance. Nature 2014;515:568–71.
45. Bobrow MN, Harris TD, Shaughnessy KJ, Litt GJ. Catalyzed reporterdeposition, a novel method of signal amplification. Application to immu-noassays. J Immunol Methods 1989;125:279–85.
46. Bobrow MN, Shaughnessy KJ, Litt GJ. Catalyzed reporter deposition, anovel method of signal amplification. II. Application tomembrane immu-noassays. J Immunol Methods 1991;137:103–12.
47. Bainer R, Frankenberger C, Rabe D, An G, Gilad Y, Rosner MR. Geneexpression in local stroma reflects breast tumor states and predicts patientoutcome. Sci Rep 2016;6:39240.
48. Rubin JT, Elwood LJ, Rosenberg SA, Lotze MT. Immunohistochemicalcorrelates of response to recombinant interleukin-2-based immunother-apy in humans. Cancer Res 1989;49:7086–92.
49. Guidolin D, Ruggieri S, Annese T, Tortorella C, Marzullo A, Ribatti D.Spatial distribution of mast cells around vessels and glands in humangastric carcinoma. Clin Exp Med 2017;17:531–9.
50. Feng Z, Puri S, Moudgil T, Wood W, Hoyt CC, Wang C, et al. Multi-spectral imaging of formalin-fixed tissue predicts ability to generatetumor-infiltrating lymphocytes from melanoma. J Immunother Cancer2015;3:47.
51. Mitchell RT, Camacho-Moll ME, Macdonald J, Anderson RA, Kelnar CJ,O'Donnell M, et al. Intratubular germ cell neoplasia of the human testis:heterogeneous protein expression and relation to invasive potential.Mod Pathol 2014;27:1255–66.
52. Vasaturo A, Halilovic A, Bol KF, Verweij DI, Blokx WA, Punt CJ, et al. T celllandscape in a primary melanoma predicts the survival of patients withmetastatic disease after their treatment with dendritic cell vaccines. CancerRes 2016;76:3496–506.
53. Jadus MR, Irwin MC, Irwin MR, Horansky RD, Sekhon S, Pepper KA,et al. Macrophages can recognize and kill tumor cells bearing themembrane isoform of macrophage colony-stimulating factor. Blood1996;87:5232–41.
54. Keller R, Keist R, Wechsler A, Leist TP, van der Meide PH. Mechanisms ofmacrophage-mediated tumor cell killing: a comparative analysis of theroles of reactive nitrogen intermediates and tumor necrosis factor. Int JCancer 1990;46:682–6.
55. Piris A, MihmMC Jr. Progress inmelanoma histopathology and diagnosis.Hematol Oncol Clin North Am 2009;23:467–80, viii.
www.aacrjournals.org Cancer Immunol Res; 6(4) April 2018 493
QmIF and qSA Define a Biomarker in Melanoma
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360

2018;6:481-493. Published OnlineFirst February 21, 2018.Cancer Immunol Res Robyn D. Gartrell, Douglas K. Marks, Thomas D. Hart, et al. Quantitative Analysis of Immune Infiltrates in Primary Melanoma
Updated version
10.1158/2326-6066.CIR-17-0360doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerimmunolres.aacrjournals.org/content/suppl/2018/02/21/2326-6066.CIR-17-0360.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/6/4/481.full#ref-list-1
This article cites 53 articles, 12 of which you can access for free at:
Citing articles
http://cancerimmunolres.aacrjournals.org/content/6/4/481.full#related-urls
This article has been cited by 7 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/6/4/481To request permission to re-use all or part of this article, use this link
on March 13, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst February 21, 2018; DOI: 10.1158/2326-6066.CIR-17-0360