Embed Size (px)
Citation preview
2
ORIGINAL ARTICLE
ABSTRACTAim: to identify quality of life in HIV patients and to
investigate associated factors.Methods: a cross-sectional comparative study of HIV
patients visiting the outpatient clinic at Cipto Man-gunkusumo National Central Hospital and Dharmais Cancer Hospital was conducted between March and June 2003. Subjects were patients willing to fill in the SF-36 questionnaire, and willing to undergo physical examination and laboratory tests. Multivariate analysis was performed to identify the determinant factors that dominantly affect the quality of life in HIV patients.
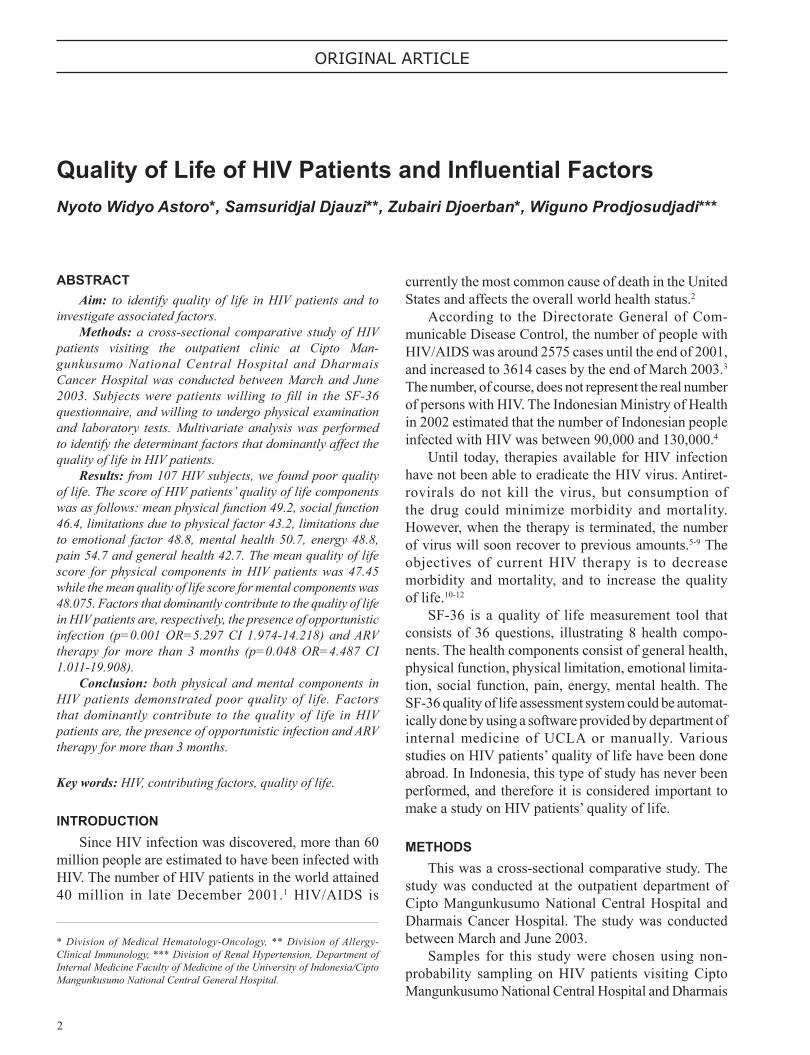
Results: from 107 HIV subjects, we found poor quality of life. The score of HIV patients’ quality of life components was as follows: mean physical function 49.2, social function 46.4, limitations due to physical factor 43.2, limitations due to emotional factor 48.8, mental health 50.7, energy 48.8, pain 54.7 and general health 42.7. The mean quality of life score for physical components in HIV patients was 47.45 while the mean quality of life score for mental components was 48.075. Factors that dominantly contribute to the quality of life in HIV patients are, respectively, the presence of opportunistic infection (p=0.001 OR=5.297 CI 1.974-14.218) and ARV therapy for more than 3 months (p=0.048 OR=4.487 CI 1.011-19.908).
Conclusion: both physical and mental components in HIV patients demonstrated poor quality of life. Factors that dominantly contribute to the quality of life in HIV patients are, the presence of opportunistic infection and ARV therapy for more than 3 months.
Key words: HIV, contributing factors, quality of life.
INTRODUCTIONSince HIV infection was discovered, more than 60
million people are estimated to have been infected with HIV. The number of HIV patients in the world attained 40 million in late December 2001.1 HIV/AIDS is
Quality of Life of HIV Patients and Inuential FactorsNyoto Widyo Astoro*, Samsuridjal Djauzi**, Zubairi Djoerban*, Wiguno Prodjosudjadi***
* Division of Medical Hematology-Oncology, ** Division of Allergy-Clinical Immunology, *** Division of Renal Hypertension, Department of Internal Medicine Faculty of Medicine of the University of Indonesia/Cipto Mangunkusumo National Central General Hospital.
currently the most common cause of death in the United States and affects the overall world health status.2
According to the Directorate General of Com-municable Disease Control, the number of people with HIV/AIDS was around 2575 cases until the end of 2001, and increased to 3614 cases by the end of March 2003.3 The number, of course, does not represent the real number of persons with HIV. The Indonesian Ministry of Health in 2002 estimated that the number of Indonesian people infected with HIV was between 90,000 and 130,000.4
Until today, therapies available for HIV infection have not been able to eradicate the HIV virus. Antiret-rovirals do not kill the virus, but consumption of the drug could minimize morbidity and mortality. However, when the therapy is terminated, the number of virus will soon recover to previous amounts.5-9 The objectives of current HIV therapy is to decrease morbidity and mortality, and to increase the quality of life.10-12
SF-36 is a quality of life measurement tool that consists of 36 questions, illustrating 8 health compo-nents. The health components consist of general health, physical function, physical limitation, emotional limita-tion, social function, pain, energy, mental health. The SF-36 quality of life assessment system could be automat-ically done by using a software provided by department of internal medicine of UCLA or manually. Various studies on HIV patients’ quality of life have been done abroad. In Indonesia, this type of study has never been performed, and therefore it is considered important to make a study on HIV patients’ quality of life.
METHODSThis was a cross-sectional comparative study. The
study was conducted at the outpatient department of Cipto Mangunkusumo National Central Hospital and Dharmais Cancer Hospital. The study was conducted between March and June 2003.
Samples for this study were chosen using non-probability sampling on HIV patients visiting Cipto Mangunkusumo National Central Hospital and Dharmais
3
Vol 39 • Number 1 • January - March 2007 Quality of Life of HIV Patients and Inuential Factors
Cancer Hospital. The inclusion criteria were HIV patients aged 17 years or older and able to communicate. The exclusion criteria were refusal to participate in the study and incomplete questionnaire. The dependent variable in this study was quality of life, while the independent variables were sex, age, level of education, employment status, HIV stage, time to HIV diagnosis, route of transmission, duration of injecting drug use, ARV therapy, CD 4 level, total lymphocyte count, anemia, and opportunistic infection. Data analysis was using the backward multivariate method. Then the collected data variables were processed using the SPSS version 10.0 computer program.
RESULTSDuring the course of the study, which was done
between March and June 2003, we consecutively obtained 107 patients. All subjects were included in the study. The subjects in this study consisted of 94 male (87.9%) and 13 female (12.1%) patients. There were 37 patients (35.6%) aged 20 to 24 years and 44 patients (41.1%) aged 25 to 30 years, with a mean age of 26.56 years. With regard to the level of education, most subjects were middle school graduates (85 patients, or 79.5%). Most subjects (67 patients, or 62.6%) were not in active employment.
In terms of clinical characteristics, most patients were in stage B (55 patients or 51.4%). Ninety patients (84.1%) have had HIV for less than 1 year. The route of HIV through IDU (intravenous drug user) was found in 80 patients (74.8%). Fifty patients (46.8%) used intravenous drug injection for less than 5 years. Most patients (73 patients or 68.2%) have never had ARV therapy.
The mean age of the subjects was 26.56 years old (median 25.0), the mean duration of using drug injection was 3.6 years, and the mean cigarette consumption was 10.15 cigarettes per day. The mean total lymphocyte count was 1.112.73 per microliter.
The mean CD4 level in the patients was 239.51 per microliter, the mean haemoglobin level was 10.80 gram per microliter, the mean SGOT level 101.93, the mean SGPT level 65.21, the mean serum albumin level 2.91, the mean globulin level 3.39, and mean total bilirubin level 1.12.
Opportunistic infection was found in 64 patients (59.8%), fty-two patients (48.6%) smoked more than 10 cigarettes per day, and 60 patients (56.1%) had anemia.
Figure 1. Quality of life score of HIV patients (n=107)
Note: Physical F = physical function; Social F = social function; Physical L = limitation due to physical factors; Emotional L = limitation due to emotional factors; MH = mental health; GH =

4
Nyoto Widyo Astoro, et al Acta Med Indones-Indones J Intern Med
At the end of this study, 11 patients (10.3%) died and 96 patients (89.7%) were still alive.
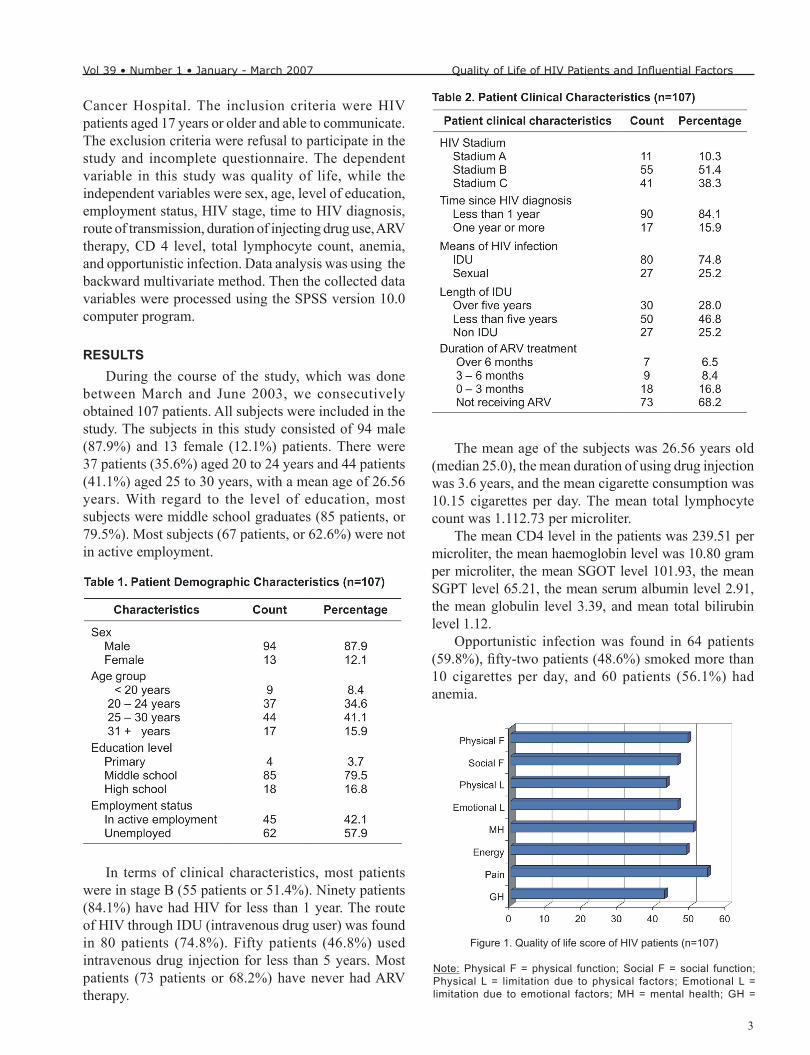
Figure 2. Score for physical and mental components
Note: PCS = physical component summary; MCS = mental component summary
The HIV patients’ quality of life scores for the following componentswere as follows: mean physical function 49.2, social function 46.4, limitation due to physical factor 43.2, limitation due to emotional factor 48.8, and general health 42.7.
The mean quality of life score for the physical components in HIV patients was 47.45, while the mean quality of life score for the mental component was 48.075.
For the study subjects’ quality of life distribution, 40 patients (37.4%) had good quality of life, and 67 patients (62.6.8%) had poor quality of life. We classied quality of life in HIV patients into two groups: good if the score is > 61 and poor if the score is < 61. The distribution of good quality of life classication was 37.4%.
HIV patients in symptomatic stage had 3.31 times greater probability of having poorer quality of life compared to those in an asymptomatic stage (p=0.000), HIV patients with opportunistic infection had 8.089 times poorer quality of life compared to patients without

5
Vol 39 • Number 1 • January - March 2007 Quality of Life of HIV Patients and Inuential Factors
opportunistic infection (p=0.000) and anemic HIV patients showed 2.87 times poorer quality of life (p=0.017), patients not receiving ARV therapy and patients receiving ARV therapy for less than 3 months had 10.272 times poorer quality of life compared to patients that receiving ARV therapy for more than 3 months (p=0.000).
Multivariate analysis using backward logistic regression demonstrated that variables dominantly associated with quality of life were the presence of opportunistic infection, and ARV therapy of more than 3 months.
DISCUSSIONThis is a cross-sectional study on the quality of life
in HIV patients. This study has obvious limitations since it only included patients from the outpatient department at Cipto Mangunkusumo National Central Hospital and Dharmais Cancer Hospital. To our knowledge, so far there has been no study on the quality of life of HIV patients in Indonesia.
Most of HIV patients were male (87.9%). The mean age of the HIV patients in this study was 26.56 years. In statistical analysis, age and sex did not seem to interfere with the quality of life. This result is similar to studies by Hays et al and Miners et al.8,9
HIV transmission through IDU in this study was 74.8%, similar to the study by Maulana (73.1%) at Cipto Mangunkusumo National Central Hospital. Statistically, the route of HIV transmission did not inuence the quality of life. This nding is similar to the previous study by Hays et al,37 who found that the quality of life in HIV patients did not differ between the IDU group and other methods of transmission.
The largest portion of HIV stage was stage B (51.4%). Those in the symptomatic stage had 3.31 times poorer quality of life (CI 2.442-4.487 p=0.000) compared to those in the asymptomatic stage. This HIV stage interferes with the quality of life, as found in the study by Lorenz et al and Bing et al. However, multivariate analysis using backward logistic regression did not nd HIV stage to be dominantly related with quality of life. The study by Lorenz et al,10 which involved 2267 HIV patients, found that patients in the symptomatic stage had poorer quality of life compared to patients in the asymptomatic stage. Bing et al11 studied 2295 gay males infected with HIV and found that symptomatic patients had poorer quality of life compared to patients in the asymptomatic stage.
Most of HIV patients did not work (64.9%). There was no statistical difference in quality of life between employed and unemployed HIV patients.
Based on the formal education variable, most HIV patients graduated from high school (81.31%). Formal education did not statistically inuence the quality of life. This is different with the study by Hays et al,37 which found that formal education affected the quality of life. This difference might be due to a difference in sample size.
All the above variables with p<0.25 were included in the multivariate analysis. The included variables were education level, working status, the duration of injection usage, HIV stage, the presence of opportunistic infection, ARV therapy, anemia, CD4 level, and total lymphocyte level.

6
Nyoto Widyo Astoro, et al Acta Med Indones-Indones J Intern Med
There were 84.1% patients known to have been infected with HIV in the last one year, while the mean duration of IDU usage was 3.6 years. This is different from the study result by Campsmith et al, which found most of their patients had been infected with HIV for more than one year; only 29.1% were infected with HIV for less than 1 year. Time to HIV diagnosis and duration of IDU usage were not statistically related to quality of life. This is similar to the study by Campsmith et al,12 which involved 3778 HIV patients and found no difference between the quality of life in HIV patients that had been diagnosed less than 1 year and more than 1 year.
More than half of HIV patients had opportunistic infection (59.8%). HIV patients with opportunistic infection had 8.1 times poorer quality of life (CI 3.31-19.64 p=0.000) compared to patients without opportunistic infection. From multivariate analysis, we found that opportunistic infection seemed to be dominantly related with poorer quality of life. This result is similar to the study by Lorenz et al and Badia et al. The study by Lorenz et al10 in 2267 HIV patients found that patients with opportunistic infection experienced poorer quality of life compared to patients without opportunistic infection. A cohort study by Badia et al13 in 296 HIV patients found that a decrease in opportunistic infection could signicantly improve the quality of life.
Most HIV patients (68.2%) did not receive ARV therapy although most of them were in symptomatic stage. This is different compared to other studies, whereby most HIV patients had had ARV therapy, such as in the study by Campsmith et al,12 where 65% of HIV patients received ARV therapy. This is due to limited access of HIV patients in Indonesia to ARV, besides the relatively expensive price of ARV. Access to ARV is currently being widened in order to easily obtain ARV inexpensively. Patients receiving ARV therapy for 3 months or above showed 10.27 times better quality of life (CI 2.71-38.97; p=0.000) compared to the patients that did not receive ARV therapy and patients who received it for less than 3 months. Multivariate analysis found that ARV therapy for more than 3 months had a dominant relationship with quality of life. This is similar to the study by Badia et al. Badia et al14 conducted a three month cohort study on 296 HIV patients and found that patients receiving ARV therapy for 3 months demonstrated better quality of life compared to the condition before ARV therapy. The result was also supported by Penedo et al,15 who were studied 116 HIV patients. They found that patients compliant to ARV therapy have better quality of life.
The mean Hb level of HIV patients was 10.8 gram/dl. The mean Hb level in Volberding38 study was 9.6 gram/dl. Some of the patients had anemia (43.9%). The prevalence of anemia in HIV patients ranges between 63% and 95%.38 HIV patients with anemia had 2.87 times poorer quality of life (CI 1.28-6.44; p = 0.017) compared to the non-anemic ones. Anemia seemed to affect the quality of life, but from multivariate analysis we found that anemia did not demonstrate a dominant relationship with quality of life. This is similar to the Volberding study. The Volberding16 study involved 146 anemic HIV patients and followed them for 12 weeks, and found that recovery of anemia in HIV patients will improve the patient’s quality of life.
The mean CD4 count of HIV patients was 239.51 cells/mmk while mean total lymphocyte count was 1112.73 cells/mmk. The mean CD4 count in the study by Volberding16 was 126 cells/mmk, 408.53 cells/mmk in the study by Penedo et al,17 and 327 cells/mmk in the study by Badia et al.13 Both CD4 count and total lymphocyte count did not affect the quality of life. The result was similar to the study by Hays et al. Hays37 found that the quality of life in HIV patients with a CD4 count of over 200 cells/mmk and CD4 count of under 200 cells/mmk were not statistically signicant.
The mean quality of life in HIV patients was poor. Score of HIV patients’ quality of life components: mean physical function 49.2, social function 46.4, limitation due to physical factor 43.2, limitation due to emotional factor 48.8, mental health 50.7, energy 48.8, pain 54.7, and general health 42.7. All quality of life components that consist of 8 components had a lower score compared to other studies, such as Bini et al and Gerbaud et al, and Hays et al. The study by Bini et al18 in the United States on 100 HIV patients showed a mean score for physical function of 82.3, a social function of 61.9, limitation due to physical factor 75.0, limitation due to emotional factor 82.7, mental health 64.0, energy 67.5, and pain 65.2. Gerbaud et al14 studied 108 patients in France and found higher mean scores in all quality of life components. Differences among other researchers were due to differences in research methods, sample characteristics, and location of study. Although the formal education level of HIV patients was more or less the same as other researchers, knowledge on HIV infection may possibly be lower. Most HIV patients were unemployed, and most of them contracted an opportunistic infection which would worsen the HIV patient’s general condition. Most have not had ARV therapy although most HIV patients already had indications of ARV therapy, which was

7
Vol 39 • Number 1 • January - March 2007 Quality of Life of HIV Patients and Inuential Factors
proved that most of HIV patients are symptomatic. This creates differences in HIV patients’ quality of life.
The quality of life scores for the physical component and mental component were also low, which means that both physical and mental condition in HIV patients in this study is poor.
In multivariate analysis, the most dominant variables affecting quality of life were found to be the presence of opportunistic infection and ARV therapy for more than 3 months. Therefore, in the effort to improve HIV patients’ quality of life we need to prevent opportunistic infection and to give therapy whenever opportunistic therapy is present. The role of ARV therapy to the quality of life in HIV patients was also signicant, therefore access to ARV in HIV patients should be widened so that HIV patients could obtain ARV easily with inexpensive price. According to Samsuridjal et al, the most frequent oppor-tunistic infection was candidosis (80%) and tuberculosis (40.1%). Efforts should be made to provide inexpensive medications for candidosis therapy, while anti tuberculosis drugs have been available with a very cheap price in community health centers.
CONCLUSIONThis study shows that the mean quality of life in
HIV patients at Cipto Mangunkusumo National Central Hospital and Dharmais Cancer Hospital is relatively low. The quality of life in HIV patients was found to be lower compared to the studies in developed countries. The quality of life in HIV patients was dominantly inuenced by, respectively, the presence of opportunistic infection and receiving ARV therapy for more than 3 months.
Differences found between this study and other existing studies were due to differences in study method, in sample characteristics, and in the places of study. Therefore, a broader study in outpatient and inpatient clinics in several hospitals is recommended, so that the result could be widely applied.
REFERENCES1. UNAIDS/WHO. AIDS epidemic update. 2001. p. 1-22.2. Gourevitch MN. The epidemiology of HIV and AIDS. Med
Clin North Am. 1996;80:1223-38.3. Direktorat Jendral P2MPL Depkes. Jakarta; 2003.4. Monitoring the AIDS pandemic. The status and trends of
HIV/AIDS/STI epidemics. 5. McDaniel JS, Chung JY, Brown L, Cournos F, et al. Practice
guideline for treatment of patients with HIV/AIDS. Am J Psychiatry. 2000;11S:1-50.
6. Alexander C. Pallative and end-of-life care. A guide to the clinical care of woman with HIV. 2000:343-76.
7. Hawari D, Jabar A, Saputasari T. Aspek psikologis/psikiatrik and psikososial patient. Seri tafsir Al Qur’an bil ilmi 04. Ilmu kedokteran jiwa. Kanker. 1999;348-65.
8. Loren KA, Shapiro MF, Asch SM, Bozzette SA, et al. Associa-tions of symptoms and health-related quality of life: nding from a national study of persons with HIV infection. Ann Intern Med. 2001;134:854-60.
9. Miners AH, Sabin CA, Mocroft A, Youle M, et al. Health-related quality of life in individuals infected with HIV in era of HAART. HIV Clin Trial. 2001;2:484-92.
10. Bing EG, Hays RD, Jacobson LP, Chen B, et al. Health-related quality of life among people with HIV disease: result from the multicenter AIDS cohort study. Qual Life Res. 2000;9:55-63.
11. Coon SJ, Kaplan RM. Assesing health-related quality of life: application to drug therapy. Clin Therapeutic. 1992;14:850-8.
12. Sullivan PS, Hanson DL, Chu SY, Jones JL, Ward JW. Epidemiology of anemia in human immunodeciency virus: results from The Multistate Adult and Adolescent Spectrum of HIV Disease Survilance Project. Blood. 1998;91:301-8.
13. Gerbaud L, Laurichesse H, Biolay S, Gourdon F, et al. Health related quality of life in HIV patiens: preliminary result of a prospective study. Mapi Research Institute. 2003. p. 17-8.
14. Bini EJ, Baskies MA, Achkar JM, Maslow MJ. Impact of HIV infection on health-related quality of life in patiens with chronic hepatitis C. (cited 2003 Marc 14). Available from: http://www.natap.org/Impact%20of%20Infection%20on%20Health-Related%20Quality.
15. Nieuwkerk PA, Gisolf EH, Colebunders R, Wu AW et al. Quality of life in asymptomatic and symptomatic HIV infected patients in a trial of ritonavir/saquinavir therapy. AIDS. 2000;14:181-7.
16. Hays RD, Cunningham WE, Sherbourne CD, Wilson IB, et al. Health-related quality of life in patients with human immunodeciency virus infection in the United States: result from the HIV cost and services utilization study. Am J Med. 2000;108:714-22.
17. Campsmith ML, Nakashima KA, Davidson AJ. Self-reported health-related quality of life in person with HIV infection: result from a multi-site interview project. (cited 2003 Nov 9) Available from: http://www.hqlo.com/content/1/1/12.
18. Tozzi V, Balestra P, Galgani S, Murri R, et al. Neurocognitive performance and quality of life in patients with HIV infection. AIDS Res. 2003;19:643-52.





























