Embed Size (px)
Citation preview

Quality of life, impotence, and activity level in arandomized trial of immediate repair versussurveillance of small abdominal aortic aneurysmFrank A. Lederle, MD,a Gary R. Johnson, MS,b Samuel E. Wilson, MD,c Charles W. Acher, MD,d DavidJ. Ballard, MD, PhD,e Fred N. Littooy, MD,f Louis M. Messina, MD,g for the Aneurysm Detection andManagement Veterans Affairs Cooperative Study, Minneapolis, Minn; West Haven, Conn; Orange, Calif;Madison, Wis; Dallas, Tex; Maywood, Ill; and San Francisco, Calif
Objective: We compared long-term health-related quality-of-life outcome after randomization to immediate elective repairor imaging surveillance, and in relation to time of elective repair, in patients with small asymptomatic abdominal aorticaneurysm (AAA).Methods: This randomized clinical trial was carried out in 16 Veterans Affairs medical centers. Study subjects were patientsat good surgical risk, aged 50 to 79 years, with AAAs 4.0 to 5.4 cm in diameter. Interventions included immediate opensurgical AAA repair or imaging surveillance every 6 months with repair reserved for AAAs that became symptomatic orenlarged to 5.5 cm. Main outcome measures considered were SF-36 health status questionnaire, prevalence of impotence,and maximum activity level, which were determined at randomization and at all follow-up visits.Results: Eleven hundred thirty-six patients were randomized and followed up for 3.5 to 8 years (mean, 4.9 years). The tworandomized groups did not differ significantly for most SF-36 scales at most times, but the immediate repair group scoredhigher overall in general health (P < .0001), which was particularly evident in the first 2 years after randomization, andslightly lower in vitality (P < .05). The baseline value of one SF-36 scale, physical functioning, was an independentpredictor of mortality. Overall, more patients became impotent after randomization to immediate repair compared withsurveillance (P < .03), but this difference did not become apparent until more than 1 year after randomization. Maximumactivity level did not differ significantly between the two randomized groups, but decline over time was significantlygreater in the immediate repair group (P < .02).Conclusions: For most quality-of-life measures and times there was no difference between randomized groups. Immediaterepair resulted in a higher prevalence of impotence more than 1 year after randomization, but was also associated withimproved perception of general health in the first 2 years. (J Vasc Surg 2003;38:745-52.)
Each year in the United States more than 30,000patients undergo elective repair of asymptomatic abdomi-nal aortic aneurysm (AAA).1 The purpose of elective AAArepair is to prevent future rupture. Risk for rupture in-creases with AAA diameter, but the optimal AAA diameterat which to offer elective repair has been the subject ofextensive debate. Recently two randomized trials comparedimmediate elective repair with surveillance for small asymp-tomatic AAAs and found that repair of AAAs smaller than5.5 cm does not improve survival.2,3 We report health-related quality-of-life outcome during one of these trials,
the Aneurysm Detection and Management (ADAM) Study(Veterans Affairs Cooperative Study No. 379).3
METHODS
Details of the ADAM study design have been publishedpreviously3,4 and are briefly reviewed here. Eligible patientswere 50 to 79 years of age, had AAAs 4.0 to 5.4 cm indiameter on centrally read computed tomography scanswithin 12 weeks before randomization, and had neitherprevious aortic surgery or probable need for aortic surgery(other than abdominal aneurysm repair) within the next 6months, evidence of AAA rupture, recent rapid AAA expan-sion, suprarenal or juxtarenal aneurysm or known largethoracic aneurysm, severe heart, lung, liver, or renal disease,recent major surgery or angioplasty, expected survival lessthan 5 years, probable noncompliance, severe debilitation,nor inability to give informed consent.
Patients were recruited over 5 years at 16 VeteransAffairs medical centers and randomized to immediate opensurgical repair or surveillance. In the immediate repairgroup, standard open repair was to be performed within 6weeks of randomization. In the surveillance group, AAAwas measured with ultrasonography or computed tomog-raphy every 6 months and repair was deferred until the AAAwas 5.5 cm in diameter or larger or symptoms of rupture
From Department of Medicine, Veterans Affairs Medical Center,a Minne-apolis, Minn, VA Cooperative Studies Program Coordinating Center,b
West Haven, Conn, Department of Surgery, University of California,Irvine,c Orange, Calif, Department of Surgery, Veterans Affairs MedicalCenter,d Madison, Wis, Baylor Health Care System,e Dallas, Tex, Depart-ment of Surgery, Veterans Affairs Medical Center,f Hines, Ill, and Depart-ment of Surgery, University of California, San Francisco.g
Competition of interest: none.Supported by the Cooperative Studies Program of the Department of
Veterans Affairs Office of Research and Development, Washington, DC.Reprint requests: Frank A. Lederle, MD, Professor of Medicine, Veterans
Affairs Medical Center (III-0), Minneapolis, MN 55417. (e-mail:[email protected]).
Copyright © 2003 by The Society for Vascular Surgery.0741-5214/2003/$30.00 � 0doi:10.1016/S0741-5214(03)00423-3
745

developed. Study nurses collected interim history and ques-tionnaire data on all patients before randomization and atclinic visits scheduled every 6 months thereafter during the8-year study. Patients in the surveillance group with unre-paired AAA underwent AAA imaging and measurement atthese visits. Telephone interviews were conducted if pa-tients failed to attend clinic visits. For analysis, actual visitswere assigned to the closest scheduled time.
We have reported the primary outcome of total mor-tality3; here we report quality-of-life outcome. Generalhealth status was measured with the SF-36, a brief ques-tionnaire derived from the Medical Outcomes Study,which has been extensively tested and used in numerousresearch projects.5 The SF-36 evaluates eight health dimen-sions: physical functioning, role limitations due to physicalproblems, social functioning, bodily pain, general mentalhealth, role limitations due to emotional problems, vitality,and general health perceptions. These have been aggre-gated into two summary measures, a physical componentsummary and a mental component summary.5 SF-36health status questionnaires were completed by the patientand reviewed for completeness by the study nurse. Also ateach visit, patients were asked by the study nurse to ratetheir sexual function as normal, impotent, retrograde ejac-ulation, or other, and to rate their maximum activity level assedentary, mild activity, moderate activity, or vigorousactivity. The study nurse was available to further explain thequestions as needed.
All data were entered twice and checked with computeralgorithms. Comparison of randomized groups was byintent to treat. P values are for two-tailed tests. Indepen-dent predictors of mortality were evaluated with forwardstepwise regression. Some SF-36 scores include imputationfor missing responses, according to the standard scoringalgorithm.6 Responses to the SF-36 were treated as contin-uous variables, and were compared between treatments andbetween follow-up visits, with unpaired and paired t tests,respectively. Treatment effect and change in SF-36 re-sponse over time were also assessed in repeated measuresmodels, assuming unstructured covariance and using treat-ment assigned and baseline measurements as covariates(SAS PROC MIXED; SAS Institute, Cary, NC).
The prevalence of impotence at each visit was thenumber of “impotent” responses divided by the total num-ber of responses. A general estimating equation model(SAS PROC GENMOD; SAS) was used to assess treatmenteffect of repeated measures. Impotence rate was comparedbetween treatments at individual time points with the �2
test, and the direction and magnitude of within-patientchanges between visits was assessed with the McNemar testfor symmetry. An overall trend in impotence (unadjustedforwithin-patient changes)wasdeterminedwith theCochran-Armitage test for trend.7
Maximum activity level was treated as an ordinal re-sponse variable, and within-visit treatment comparisonswere made with the Wilcoxon rank sum test.8 Paired com-parisons between visits and before and after AAA repairwere performed with the Wilcoxon signed rank test for shift
in distribution.8 A repeated measures model assuming un-structured covariance was used to analyze the change inactivity level over time. The “before repair” value shown forprevalence of impotence and for maximum activity level isthe last value obtained before AAA repair, with the nextvalue assigned as 6 months after repair.
RESULTS
Five hundred sixty-nine patients were randomized tothe immediate repair group, and 567 were randomized toimaging surveillance. Patient characteristics at baseline havebeen reported.3 Mean patient age was 68 years, 99% ofpatients were men, and 94% of patients were white. Thetwo groups did not differ significantly at randomization inmean values of any of the SF-36 scales, prevalence ofimpotence, mean maximum activity levels, or any othercharacteristics, except for a previously reported small differ-ence in serum creatinine level.3
Patients were followed up for 3.5 to 8 years (mean, 4.9years). All AAAs were asymptomatic at baseline and at allroutine follow-up visits, during which quality of life datawere collected. By the end of the study, AAA repair hadbeen performed in 92.6% of the immediate repair group(72.1% within 6 weeks after randomization) and 61.6% ofthe surveillance group. As reported,3 143 patients in theimmediate repair group died, compared with 122 patientsin the surveillance group (relative risk for immediate repairgroup, 1.21; 95% confidence interval [CI], 0.95-1.54).There were 19 AAA-related deaths in each group (relativerisk for immediate repair group, 1.03; 95% CI, 0.54-1.94).9 Eighty-five percent of follow-up visits were com-pleted in the immediate repair group, and 87% in thesurveillance group (P � .02).3 Responses for specific qual-ity of life outcome were missing in fewer than 0.5% ofcompleted visits; exact numbers are given in the figures.SF-36 questionnaires were obtained later for some missedvisits, resulting in slightly higher numbers.
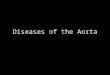
SF-36 scores for the two groups are shown in Fig 1. AllSF-36 scales showed significant decrease over time for theentire study population (P � .001). There was no signifi-cant difference between the two groups after randomiza-tion for most SF-36 scales, but the general health score wassignificantly higher in the immediate repair group at re-peated measures analysis (P � .0001). This overall differ-ence was reflected in significantly higher scores (P � .05) atindividual time points from 6 months to 2 years. Repeatedmeasures analysis also indicated a small difference in vitalityfavoring the surveillance group (P � .05). Several othertime point comparisons were nominally significant (P �.05), but should be interpreted with caution because of thelarge number of comparisons. These included better scoresin the immediate repair group at 6 months in mental health,and worse scores at 5 years in physical functioning and at6.5 years in role—physical. The baseline value of one SF-36scale, physical functioning, was an independent predictor ofmortality during the trial.
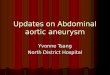
Impotence was reported by more than a third of pa-tients at randomization (Fig 2). Overall, at repeated mea-
JOURNAL OF VASCULAR SURGERYOctober 2003746 Lederle et al

Fig 1. Mean SF-36 scores by treatment group. All scores are 0 to 100, with 100 representing better health. Asterisksat individual time points represent P � .05. See text for overall differences. Black circles, Immediate repair group; opencircles, surveillance group.
JOURNAL OF VASCULAR SURGERYVolume 38, Number 4 Lederle et al 747

Fig 2. Prevalence of impotence by treatment group. Overall, at repeated measures analysis, impotence was significantlyincreased after randomization in immediate repair group (P � .03).
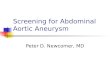
Fig 3. Prevalence of impotence in all study patients who underwent AAA repair. “New” impotence is not shown beforerepair, because there was no previous record for comparison.
JOURNAL OF VASCULAR SURGERYOctober 2003748 Lederle et al

sures analysis, impotence was significantly increased afterrandomization in the immediate repair group (P � .03).Comparison of specific time periods shows that this differ-ence was not significant at 6 or 12 months after random-ization, but was significant from 18 months to 4 years (P �.05; Fig 2). This pattern does not reflect the difference inrate of AAA repair between the two groups, which wasgreatest in the first month after randomization and declinedsteadily afterward.3 When the rate of impotence is exam-ined in all patients who underwent repair, regardless ofrandomization group, a steady increase in prevalence overtime is noted (P � .0001), without a marked increaseimmediately after AAA repair (Fig 3). Fewer than 3% ofpatients reported retrograde ejaculation at any time duringthe study.
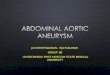
Overall, maximum activity level did not differ signifi-cantly between the two randomized groups at repeatedmeasures analysis. However, there was a significant interac-tion between treatment and follow-up time (P � .02)indicating that worsening in maximum activity score wasgreater in the immediate surgery group (equivalent tocrossed curves with differing slopes). In comparison be-tween individual time points (which should be interpretedcautiously), the two groups did not differ at any time except6 years, when patients in the surveillance group reportedhigher activity levels (P � .04, Fig 4). Compared with levelsbefore repair in all patients who underwent repair, regard-
less of randomization group, maximum activity level de-creased significantly over time (P � .0001; Fig 5).
DISCUSSION
In this randomized trial of patients with small asymp-tomatic AAAs, immediate elective AAA repair and imagingsurveillance resulted in generally similar outcome in thequality-of-life measures assessed. Immediate repair resultedin increased impotence more than 1 year after randomiza-tion, but was also associated with improved perception ofgeneral health, particularly in the first 2 years.
Baseline SF36 scores for our patients are slightly lowerthan for patients of similar age with very small AAA in arandomized trial of propranolol,10 are similar to nationalnorms for men aged 65 years or older,6 but are higher thanscores for unselected Veterans Affairs medical center out-patients11,12 or patients undergoing AAA repair at Brighamand Women’s Hospital.13 Our finding that baseline SF-36physical functioning scale was an independent predictor ofmortality is consistent with an earlier VA CooperativeStudy, in which baseline SF-36 physical component sum-mary was an independent risk factor for death after coro-nary artery bypass graft surgery.14
Our findings of improvement in some SF-36 scoresafter repair of asymptomatic AAA, although seeminglyparadoxical, are consistent with previous studies. Two stud-ies reported significant improvement in the SF-36 mental
Fig 4. Maximum activity level by treatment group.
JOURNAL OF VASCULAR SURGERYVolume 38, Number 4 Lederle et al 749

health and role—physical scales 6 months after open AAArepair compared with preoperative levels, in addition toimprovement in bodily pain in one of the studies15 and inthe role—emotional scale in the other.13 These improve-ments followed initial reduction in SF-36 scores 4 to 6weeks after the procedure. The only other randomized trialof immediate repair versus surveillance, the UK Small An-eurysm Trial (UKSAT), reported significant improvementin SF-20 general health and bodily pain scales 12 monthsafter randomization in the immediate repair group.16 Theauthors of these earlier studies attributed their findings toreduced fear of rupture15 and to relief at surviving a majorprocedure,13 providing, perhaps, an empiric demonstrationof Churchill’s observation that “Nothing in life is so exhil-arating as to be shot at without result.”17Another factorthat may have contributed to higher quality-of-life scores inthe surgery group in our study and in earlier studies is theselective early removal of frail patients from the surgerygroup as a result of operative death, as was suggested afterthe UKSAT.18 Our results could also be affected by loss ofpatients from later death.
The improvements documented in our study and inearlier studies are also consistent with the previously de-scribed “placebo effect” of surgery. In 1958 Dimond et al19
reported marked improvement in angina and exercise tol-erance after sham coronary artery bypass graft surgery.More recently Fischer et al20 observed that patients retro-
spectively reported improvement in disability after arthro-plasty, although serial measurements revealed worsening(in our study, improvements were seen in serial measures).However, of 87 patients interviewed after elective openAAA repair, one third reported a decrease in functionalstatus, and the same proportion said they had not fullyrecovered from surgery after a mean of 34 months.21
Our findings suggest that, while elective open AAArepair may cause impotence, this outcome may occur lessoften and more gradually than previously believed. Retro-spective surveys have reported rates of new impotence inmore than 80% of men with previously normal functionwho underwent open AAA repair,22,23 but are subject torecall and response bias. Magee et al24 surveyed men beforeand after AAA repair, and found new impotence in 31 of119 (26%) with previously normal function, but there wasno control group who did not undergo repair for compar-ison. The findings of these uncontrolled studies have beencited as reason to favor endovascular over open repair.25
However, our findings suggest that the small increase inimpotence immediately after open AAA repair may reflectlittle more than background increase in impotence overtime in this population (Fig 3). Open repair appears tocause a moderate increase in late impotence (Fig 2), thoughwhy this would occur is not clear. Impotence is one of theoutcomes being assessed in an ongoing VA CooperativeStudy comparing open with endovascular AAA repair.
Fig 5. Maximum activity level in all study patients who underwent AAA repair.
JOURNAL OF VASCULAR SURGERYOctober 2003750 Lederle et al

Our study was limited almost entirely to men, and theresults may not apply to women with AAA. A secondlimitation is that our findings on impotence and maximumactivity level were each based on a single question designedfor use in this study. Questionnaires designed to assesserectile dysfunction have been developed,26 but were notavailable when our study was begun. Also, this report is ofsecondary trial outcomes and involves multiple compari-sons; thus some marginal P values, particularly for compar-isons of individual time points, may represent chance alone.P values were presented unadjusted because determiningprecise numbers of relevant comparisons is problematic andadjustment itself is controversial.27
We previously reported that immediate repair of AAAless than 5.5 cm does not improve survival. We report herethat immediate repair results in quality of life scores similarto those obtained with surveillance, although late impo-tence is somewhat more common and perception of gen-eral health is transiently improved.
The ADAM Veterans Affairs Cooperative Study also includedthe following persons: Coauthors: Donovan B. Reinke, MD,Diagnostic Radiology Service, Veterans Affairs Medical Center,Minneapolis, Minn; Ian L. Gordon, MD, Department of Surgery,Veterans Affairs Medical Center, Long Beach, Calif; Edmund P.Chute, MD, Department of Surgery, Veterans Affairs MedicalCenter, Minneapolis, Minn; William C. Krupski, MD, Departmentof Surgery, Veterans Affairs Medical Center, Denver, Colo; DennisBandyk, MD, Department of Surgery, Veterans Affairs MedicalCenter, Tampa, Fla; Steven J. Busuttil, MD, Department of Sur-gery, Veterans Affairs Medical Center, Cleveland, Ohio; Gary W.Barone, MD, Department of Surgery, Veterans Affairs MedicalCenter, Little Rock, Ark; Steven Sparks, MD, Department ofSurgery, Veterans Affairs Medical Center, San Diego, Calif; LindaM. Graham, MD, Department of Surgery, Veterans Affairs Medi-cal Center, Ann Arbor, Mich; Joseph H. Rapp, MD, Departmentof Surgery, Veterans Affairs Medical Center, San Francisco, Calif;Michel S. Makaroun, MD, Department of Surgery, Veterans Af-fairs Medical Center, Pittsburgh, Pa; Gregory L. Moneta, MD,Department of Surgery, Veterans Affairs Medical Center, Port-land, Ore; Robert A. Cambria, MD, Department of Surgery,Veterans Affairs Medical Center, Milwaukee, Wis; Raymond G.Makhoul, MD, Department of Surgery, Veterans Affairs MedicalCenter, Richmond, Va; Darwin Eton, MD, Department of Sur-gery, Veterans Affairs Medical Center, Miami, Fla; Howard J.Ansel, MD, Diagnostic Radiology Service, Veterans Affairs Medi-cal Center, Minneapolis, Minn; Julie A. Freischlag, MD, Depart-ment of Surgery, Veterans Affairs Medical Center, Los Angeles,Calif.
Investigators at Veterans Affairs medical centers: G. B.Zelenock, C. Shanley, C. Sekerak, M. Lingg, and L. Trohallis, AnnArbor, Mich; A. W. Averbook, C. L. Mesh, K. Kaelin, T. O’Malley,E. Wingard, J. Lindesmith, and J. Francosky, Cleveland, Ohio; A.Furst, M. Tabbara, A. A. Nunez, G. Paperwalla, K. Nunez, C.Estep, and J. Taylor, Miami, Fla; P. Strecker and L. Schoening,Denver, Colo; J. Maggio and W. Cote, Maywood, Ill; M. Moursi,B. W. Thompson, B. Kackley, B. Chesser, R. Little, and T. Wood,Little Rock, Ark; C. Kohl, G. Scully, R. Complin, and M. Akkine-pali, Long Beach, Calif; J. Archibald, J. Fitzsimons, and T. J.Havlik, Madison, Wis; W. D. Payne, M. L. Schwartz, C. Proebstle,R. Hedblad, and M. Richardson, Minneapolis, Minn; S. Muluk, C.Slivka, N. Carnegie, T. DeBoo, J Freidel, and J. Fuhs, Pittsburgh,Pa; R. A. Yeager, J. M. Edwards, L. Enger, R. Jemerson, T.Williams, and R. McCartney, Portland, Ore; A. Grimsdale, L.Bartnicki, and L. T. Joyner, Richmond, Va; S. Dwyer, D. Collins,S. Vann Smith, and H. Daughenbaugh, San Francisco, Calif; R. J.
Hye, E. J. Plecha, Y. G. Wolf, G. Cali, T. Scala, and R. Hull, SanDiego, Calif; D. Bou-Eid and M. Jackson Maynard, Tampa, Fla;J. A. Freischlag, C. Kallio, S. Framberg, S. Towne, and C. Weller,Milwaukee, Wis.
Data monitoring board: G. P. Clagett, Dallas, Tex; J. D.Corson, Iowa City, Iowa; W. C. Cushman, Memphis, Tenn; C. S.Landefeld, San Francisco, Calif; T. G. Karrison, Chicago, Ill; andJ. P. Matts, Minneapolis, Minn.
Outcomes committee: M. D. McDaniel, White River Junc-tion, Vt; G. C. Lamb, Milwaukee, Wis; and C. de Virgilio, Tor-rance, Calif.
Planning committee: J. L. Cronenwett, Hanover, NH; D. B.Matchar, Durham, NC; C. R. B. Meritt, New Orleans, La; andC. W. Cole, Ottawa, Ont, Canada.
Cooperative studies program coordinating center: P. N.Peduzzi (Director), C. M. Harris, I. Haddock, L. Durant, V.Williams-Estes, A. Hudson, R. Vinisko, R. Bartozzi, R. Kilstrom,K. Riester, K. Newvine, R. Goodwin, D. Collins, P. Antonelli, M.Smith, L. Franklin, P. Collins, S. Marcinauskis, W. Carr, and B.Hunter, West Haven, Conn.
Project coordinators: M. A. Haas and J. M. Larson, Minne-apolis, Minn.
Central CT laboratory: H. J. Ansel, Minneapolis, Minn.Cooperative studies program administration at depart-
ment of veterans affairs central office: P. W. Lavori (ActingChief), J. R. Feussner (previous Chief), J. Gough, S. Berkowitz, D.Deykin (previous Chief), J. Gold, and P. C. Huang.
REFERENCES
1. Lawrence PF, Gazak C, Bhirangi L, et al. The epidemiology of surgicallyrepaired aneurysms in the United States. J Vasc Surg 1999;30:632-40.
2. The UK Small Aneurysm Trial Participants. Long-term outcomes ofimmediate repair compared with surveillance of small abdominal aorticaneurysms. N Engl J Med 2002;346:1445-52.
3. Lederle FA, Wilson SE, Johnson GR, Reinke DB, Littooy FN, AcherCW, et al, for the Aneurysm Detection and Management (ADAM)Veterans Affairs Cooperative Study Investigators. Immediate repaircompared with surveillance of small abdominal aortic aneurysms.N Engl J Med 2002;346:1437-44.
4. Lederle FA, Wilson SE, Johnson GR, et al. Design of the abdominalaortic Aneurysm Detection and Management (ADAM) Study. J VascSurg 1994;20:296-303.
5. Ware JE Jr, Kosinski M, Bayliss MS, McHorney CA, Rogers WH,Raczek A. Comparison of methods for the scoring and statistical analysisof SF-36 health profile and summary measures: summary of results fromthe Medical Outcomes Study. Med Care 1995;33(suppl A):S264-79.
6. Ware JE Jr, Snow KK, Kosinski M, Gandek B. SF-36 Health SurveyManual and Interpretation Guide. Boston, Mass: Nimrod Press, 1993.
7. Armitage P. Test for linear trends in proportions and frequencies.Biometrics 1955;11:375-86.
8. Hollander M, Wolfe DA. Nonparametric statistical methods. New York,NY: Wiley, 1973.
9. Lederle FA, & for the Aneurysm Detection and Management VeteransAffairs Cooperative Study Group. Small abdominal aortic aneurysms.N Engl J Med 2002;347:1114 [letter].
10. The Propranolol Aneurysm Trial Investigators. Propranolol for smallabdominal aortic aneurysms: results of a randomized trial. J Vasc Surg2002;35:72-9.
11. Weinberger M, Samsa GP, Hanlon JT, Schmader K, Doyle ME, et al.An evaluation of a brief health status measure in elderly veterans. J AmGeriatr Soc 1991;39:691-4.
12. Kazis LE, Miller DR, Clark J, Skinner K, Lee A, Rogers W, et al.Health-related quality of life in patients served by the Department ofVeterans Affairs: results from the Veterans Health Study. Arch InternMed 1998;158:626-32.
13. Mangione CM, Goldman L, Orav EJ, Marcantonio ER, Pedan A,Ludwig LE, et al. Health-related quality of life after elective surgery:measurement of longitudinal changes. J Gen Intern Med 1997;12:686-97.
JOURNAL OF VASCULAR SURGERYVolume 38, Number 4 Lederle et al 751

14. Rumsfeld JS, McWhinney S, McCarthy M Jr, Shroyer AL, VillaNuevaCB, O’Brien M, et al. Health-related quality of life as a predictor ofmortality following coronary artery bypass graft surgery. Participants ofthe Department of Veterans Affairs Cooperative Study Group on Pro-cesses, Structures, and Outcomes of Care in Cardiac Surgery. JAMA1999;281:1298-303.
15. Perkins JM, Magee TR, Hands LJ, Collin J, Galland RB, Morris PJ.Prospective evaluation of quality of life after conventional abdominalaortic aneurysm surgery. Eur J Vasc Endovasc Surg 1998;16:203-7.
16. UK Small Aneurysm Trial Participants. Health service costs and qualityof life for early elective surgery or ultrasonographic surveillance for smallabdominal aortic aneurysms. Lancet 1998;352:1656-60.
17. Churchill WS. The story of the Malakand Field Force: an episode offrontier war. London, England: Longmans, Green, and Co, 1898:p172.
18. Pretre R, Turina MI. Facts, at last, on management of small infrarenalaortic aneurysms. Lancet 1998;352:1642-3.
19. Dimond EG, Kittle CF, Crockett JE. Evaluation of internal mammaryartery ligation and sham procedure in angina pectoris. Circulation1958;18:712-3.
20. Fischer D, Stewart AL, Bloch DA, Lorig K, Laurent D, Holman H.Capturing the patient’s view of change as a clinical outcome measure.JAMA 1999;282:1157-62.
21. Williamson WK, Nicoloff AD, Taylor LM Jr, Moneta GL, Landry GJ,Porter JM. Functional outcome after open repair of abdominal aorticaneurysm. J Vasc Surg 2001;33:913-20.
22. May AG, DeWeese JA, Rob CG. Changes in sexual function followingoperation on the abdominal aorta. Surgery 1969;65:41-7.
23. Lee ES, Kor DJ, Kuskowski MA, Santilli SM. Incidence of erectiledysfunction after open abdominal aortic aneurysm repair. Ann VascSurg 2000;14:13-9.
24. Magee TR, Scott DJ, Dunkley A, St Johnston J, Campbell WB, BairdRN, et al. Quality of life following surgery for abdominal aortic aneu-rysm. Br J Surg 1992;79:1014-6.
25. Zarins CK, Wolf YG, Lee WA, Hill BB, Olcott C IV, Harris EJ, et al.Will endovascular repair replace open surgery for abdominal aorticaneurysm repair? Ann Surg 2000;232:501-7.
26. Rosen R, Riley A, Wagner G, Osterloh I, Kirkpatrick J, Mishra A. TheInternational Index of Erectile Function (IIEF): a multidimensionalscale for assessment of erectile dysfunction. Urology 1997;49:822-30.
27. Perneger TV. What’s wrong with Bonferroni adjustments. BMJ 1998;316:1236-8.
Submitted Nov 27, 2002; accepted Mar 10, 2003.
Authors requested to declare conditions of research funding
When sponsors are directly involved in research studies of drugs and devices, the editors will ask authors to clarify theconditions under which the research project was supported by commercial firms, private foundations, or government.Specifically, in the methods section, the authors should describe the roles of the study sponsor(s) and theinvestigator(s) in (1) study design, (2) conduct of the study, (3) data collection, (4) data analysis, (5) datainterpretation, (6) writing of the report, and (7) the decision regarding where and when to submit the report forpublication. If the supporting source had no significant involvement in these aspects of the study, the authors shouldso state.
JOURNAL OF VASCULAR SURGERYOctober 2003752 Lederle et al