Embed Size (px)
Citation preview

6
Epilepsy & Behavior 2, 284–287 (2001)
doi:10.1006/ebeh.2001.0173, available online at http://www.idealibrary.com on
BRIEF COMMUNICATION
Quality-of-Life Assessment in Patients Treatedwith Vagus Nerve Stimulation
Erhan Ergene, M.D., Pamela K. Behr, R.N.,and Jerry J. Shih, M.D.1
Department of Neurology, University of New Mexico School of Medicine,915 Camino De Salud NE, Albuquerque, New Mexico 87131-5281
Received December 1, 2000; revised February 26, 2001;accepted for publication March 5, 2001
Vagus nerve stimulation (VNS) is a novel therapy used in patients with medically intractable epilepsy.We administered a Quality of Life in Epilepsy—10 (QOLIE-10) questionnaire consisting of questionsdesigned to assess the patients’ rating of their memory, level of physical and mental well-being,energy, depression, worries about seizures and work, social limitations, and overall quality of life onVNS treatment. The questionnaire was administered before and at 1–3 weeks, 5–7 weeks, 3 months,6 months, and 9–12 months after the initiation of VNS in 17 patients. QOLIE-10 scores were signifi-cantly better after the initiation of the therapy as compared with baseline (P < 0.01). There was nocorrelation between the improvement in QOLIE-10 scores and the reduction in seizure frequency,decreased severity of seizures, or increased level of energy/alertness. We conclude that VNS therapyis associated with a significant improvement in subjective quality of life. © 2001 Academic Press
Key Words: vagus nerve stimulation; quality of life; refractory epilepsy.
INTRODUCTION
Vagus nerve stimulation (VNS) is a novel adjunctivetherapy used in patients with medically intractable,focal-onset epilepsy (1–3). Previous studies haveshown that VNS induces a reduction in seizure fre-quency comparable to that produced by major anti-epileptic drugs (1, 3). Besides the reduction in seizurefrequency, an important consideration for patientswith epilepsy is the overall effect of treatments theyreceive on the quality of their lives. Hence, the assess-ment and monitoring of changes in quality of life asperceived by patients have been part of many clinicalstudies evaluating the effectiveness of new antiepilep-tic treatments (4, 5).
1 To whom correspondence should be addressed. Fax: (505) 272-692. E-mail: [email protected].
284
The purpose of the present prospective study was toinvestigate if VNS therapy produced subjective im-provements in quality of life in patients with epilepsyrefractory to pharmacological treatments. Preliminaryresults from this study have been published in abstractform (6).
METHODS
Seventeen patients (6 female, 11 male) with partial-onset epilepsy were studied in a prospective fashion.The average patient age was 33.8 years (range, 11–55years). All patients had persistent, frequent seizuresdespite appropriate medical management. They werenot candidates for surgical treatment either because ofa documented bilaterally independent onset of sei-zures from two hemispheres or because they were notinterested in surgical treatment. The etiologies of sei-
1525-5050/01 $35.00Copyright © 2001 by Academic Press
All rights of reproduction in any form reserved.

285Brief Communication
zures in study patients included cerebral palsy/peri-natal brain injury in 5 patients, mesial temporal scle-rosis in 3, traumatic brain injury in 2, subarachnoidhemorrhage due to aneurysm in 1, cavernous angio-mas in 1, and a history of meningitis during infancy in1. The cause of seizures was unknown in 4 patients.All patients agreed to be treated with VNS.
Prior to implantation of the VNS device and initia-tion of treatment, the patients were asked to respondto a questionnaire, Quality of Life in Epilepsy Inven-tory—10 (QOLIE-10), to assess their baseline subjec-tive quality of life. QOLIE-10, developed by Cramer etal. (7), consists of 10 questions designed to assess thepatients’ subjective rating of their memory, level ofphysical and mental well-being, energy, depression,worries about seizures and work, social limitations,and overall quality of life. Each item in the question-naire is ranked on a scale of 1 to 5, and the patientreceives a total scale score of 10 to 50 by answering allthe questions.
One to three weeks after the initial administration ofQOLIE-10, a VNS device was surgically implanted inall patients. The device was turned on 2 weeks afterimplantation. Standard stimulation parameters of30-Hz signal frequency, 500-ms pulse width, 30 s ofon-time, and 5 min of off-time were used. The stimu-lation intensity was initially set at 0.25 mA, and grad-ually increased to tolerance over a 2- to 3-month pe-riod, with a final value of 1.0 to 2.5 mA in all patients.
After the baseline assessment, QOLIE-10 was againadministered at 1–3 weeks, 5–7 weeks, 3 months, 6months, and 9–12 months after the initiation of VNS.
In addition, during each follow-up visit, the patientswere asked if there were any changes in seizure fre-quency, severity, and/or level of energy and alertnessfollowing seizures. The answers to each of these ques-tions for each patient were noted as “increased,” “de-creased,” or “no change.” The presence of any sideeffects or subjective complaints attributable to thetreatment was also noted. All patients were on stabledoses of two or three antiepileptic drugs (AEDs)throughout the study.
Total QOLIE-10 score at each time point followingthe initiation of VNS treatment for each patient wascompared with the baseline QOLIE-10 score of thesame patient prior to the initiation of treatment. Forthe assessment of statistically significant changes inscale scores across time, a one-way analysis of vari-ance (ANOVA) for repeated measures was performed.In addition, QOLIE-10 scores were compared, usingan ANOVA of contrast variables, in patients with and
without decreased seizure frequency, severity, andincreased level of energy. A two-tailed P value wasused to determine statistical significance.
RESULTS
Mean QOLIE-10 scores were significantly improved(lower total QOLIE-10 scale scores) at all time pointsafter the initiation of VNS therapy as compared withthose at baseline (P , 0.01) throughout the study of1-year duration. These results are graphically illus-trated in Fig. 1.
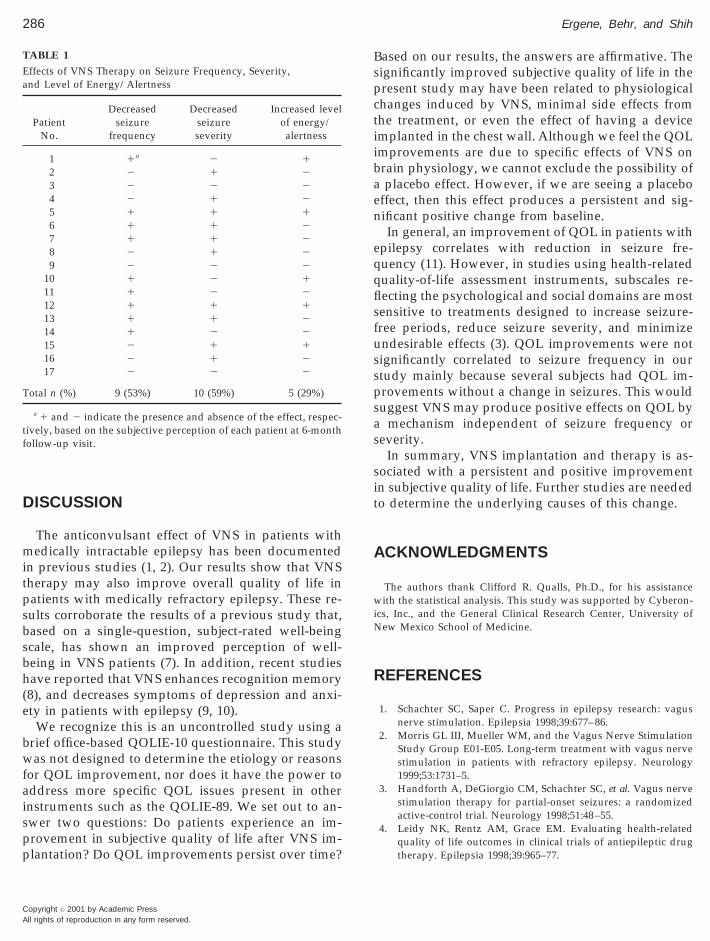
At the 6-month follow-up visit, 53% of patients re-ported a notable decrease in their seizure frequencywhile on VNS treatment. In addition, 59% of pa-tients experienced a decrease in severity of seizuresregardless of change in frequency. Twenty-nine per-cent of patients felt an increased level of energy andalertness. Various effects of VNS therapy are sum-marized in Table 1. An analysis of the interactionbetween QOLIE-10 scores and the reduction in seizurefrequency, seizure severity, and increased level ofenergy/alertness showed that there was no correla-tion between the improved QOLIE-10 scores and thesevariables.
Side effects from VNS were minimal, and includedirritation/spasm in throat in 4 patients, difficultybreathing in 1 patient, difficulty speaking in 1 patient,epigastric discomfort in 1 patient, and increased snor-
FIG. 1. Improvement in QOLIE-10 scores over time. MaximumQOLIE-10 score is 50 (worst). ANOVA indicated that the mean totalscale scores were significantly better (lower QOLIE-10, total scores)at all time points after the initiation of the therapy than baseline(P , 0.01). Bars: 6SEM.
ing in 1 patient.
Copyright © 2001 by Academic PressAll rights of reproduction in any form reserved.
T
tf
286 Ergene, Behr, and Shih
A
DISCUSSION
The anticonvulsant effect of VNS in patients withmedically intractable epilepsy has been documentedin previous studies (1, 2). Our results show that VNStherapy may also improve overall quality of life inpatients with medically refractory epilepsy. These re-sults corroborate the results of a previous study that,based on a single-question, subject-rated well-beingscale, has shown an improved perception of well-being in VNS patients (7). In addition, recent studieshave reported that VNS enhances recognition memory(8), and decreases symptoms of depression and anxi-ety in patients with epilepsy (9, 10).
We recognize this is an uncontrolled study using abrief office-based QOLIE-10 questionnaire. This studywas not designed to determine the etiology or reasonsfor QOL improvement, nor does it have the power toaddress more specific QOL issues present in otherinstruments such as the QOLIE-89. We set out to an-swer two questions: Do patients experience an im-provement in subjective quality of life after VNS im-plantation? Do QOL improvements persist over time?
TABLE 1
Effects of VNS Therapy on Seizure Frequency, Severity,and Level of Energy/Alertness
PatientNo.
Decreasedseizure
frequency
Decreasedseizureseverity
Increased levelof energy/alertness
1 1a 2 12 2 1 23 2 2 24 2 1 25 1 1 16 1 1 27 1 1 28 2 1 29 2 2 2
10 1 2 111 1 2 212 1 1 113 1 1 214 1 2 215 2 1 116 2 1 217 2 2 2
otal n (%) 9 (53%) 10 (59%) 5 (29%)
a 1 and 2 indicate the presence and absence of the effect, respec-ively, based on the subjective perception of each patient at 6-monthollow-up visit.
Copyright © 2001 by Academic Pressll rights of reproduction in any form reserved.
Based on our results, the answers are affirmative. Thesignificantly improved subjective quality of life in thepresent study may have been related to physiologicalchanges induced by VNS, minimal side effects fromthe treatment, or even the effect of having a deviceimplanted in the chest wall. Although we feel the QOLimprovements are due to specific effects of VNS onbrain physiology, we cannot exclude the possibility ofa placebo effect. However, if we are seeing a placeboeffect, then this effect produces a persistent and sig-nificant positive change from baseline.
In general, an improvement of QOL in patients withepilepsy correlates with reduction in seizure fre-quency (11). However, in studies using health-relatedquality-of-life assessment instruments, subscales re-flecting the psychological and social domains are mostsensitive to treatments designed to increase seizure-free periods, reduce seizure severity, and minimizeundesirable effects (3). QOL improvements were notsignificantly correlated to seizure frequency in ourstudy mainly because several subjects had QOL im-provements without a change in seizures. This wouldsuggest VNS may produce positive effects on QOL bya mechanism independent of seizure frequency orseverity.
In summary, VNS implantation and therapy is as-sociated with a persistent and positive improvementin subjective quality of life. Further studies are neededto determine the underlying causes of this change.
ACKNOWLEDGMENTS
The authors thank Clifford R. Qualls, Ph.D., for his assistancewith the statistical analysis. This study was supported by Cyberon-ics, Inc., and the General Clinical Research Center, University ofNew Mexico School of Medicine.
REFERENCES
1. Schachter SC, Saper C. Progress in epilepsy research: vagusnerve stimulation. Epilepsia 1998;39:677–86.
2. Morris GL III, Mueller WM, and the Vagus Nerve StimulationStudy Group E01-E05. Long-term treatment with vagus nervestimulation in patients with refractory epilepsy. Neurology1999;53:1731–5.
3. Handforth A, DeGiorgio CM, Schachter SC, et al. Vagus nervestimulation therapy for partial-onset seizures: a randomizedactive-control trial. Neurology 1998;51:48–55.
4. Leidy NK, Rentz AM, Grace EM. Evaluating health-relatedquality of life outcomes in clinical trials of antiepileptic drugtherapy. Epilepsia 1998;39:965–77.

287Brief Communication
5. Baker GA, Camfield C, Camfield P, et al. Commission onoutcome measurement in epilepsy, 1994–1997: final report.Epilepsia 1998;39:213–31.
6. Ergene E, Behr P, Shih JJ. Subjective quality of life improve-ment in patients treated with vagus nerve stimulation. Epilep-sia 1999;40(S7):221–2.
7. Cramer JA, Perrine K, Devinsky O, Meador KJ. A brief ques-tionnaire to screen for quality of life in epilepsy: the QOLIE-10.Epilepsia 1996;37:577–82.
8. Devinsky O. Clinical uses of the quality-of-life in epilepsyinventory. Epilepsia 1993;34(suppl 4):S39–44.
9. Clark KB, Naritoku DK, Smith DC, Browning RA, Jensen RA.
Enhanced recognition memory following vagus nerve stimu-lation in human subjects. Nat Neurosci 1999;2:94–8.
10. Nikolov BG, Harden CL, Pick L, et al. Mood and anxietychanges in epilepsy patients treated with 3 different antisei-zure interventions. Epilepsia 1999;40(S7):58.
11. Leidy NK, Elixhauser A, Vickrey B, Means E, Willian MK.Seizure frequency and the health-related quality of life ofadults with epilepsy. Neurology 1999;53:162–6.
12. Ettinger AB, Nolan E, Vitale S, Schindler RJ, Cramer J, Weis-brot DM. Changes in mood and quality of life in adult epilepsypatients treated with vagus nerve stimulation. Epilepsia 1999;
40(S7):62.Copyright © 2001 by Academic PressAll rights of reproduction in any form reserved.





























