Embed Size (px)
Citation preview

doi: 10.1111/joim.12611
Vagus nerve stimulation: a new promising therapeutic tool ininflammatory bowel diseaseB. Bonaz 1,2, V. Sinniger1,2 & S. Pellissier1,3
From the 1University Clinic of Hepato-Gastroenterology, University Hospital; 2University Grenoble Alpes, Grenoble Institute of Neurosciences(GIN), Inserm (U1216), Grenoble; and 3Laboratoire Inter-Universitaire de Psychologie, Personnalit�e, Cognition et Changement Social (LIP/PC2S), University Savoie Mont-Blanc, Chamb�ery, France
Content List – Read more articles from the symposium: 13th Key Symposium – Bioelectronic Medicine:Technology Targeting Molecular Mechanisms.
Abstract. Bonaz B, Sinniger V, Pellissier S (UniversityHospital, Grenoble; Grenoble Institute ofNeurosciences (GIN), Inserm, Grenoble;Laboratoire Inter-Universitaire de Psychologie,Personnalit�e, Cognition et Changement Social(LIP/PC2S), Chamb�ery, France). Vagus nervestimulation: a new promising therapeutic tool ininflammatory bowel disease (Key Symposium). JIntern Med 2017; 282: 46–63.
Inflammatory bowel disease (IBD), that is Crohn’sdisease (CD) and ulcerative colitis, affects about1.5 million persons in the USA and 2.2 million inEurope. The pathophysiology of IBD involvesimmunological, genetic and environmental factors.The treatment is medico-surgical but suspensive.Anti-TNFa agents have revolutionized the treat-ment of IBD but have side effects. In addition, anon-negligible percentage of patients with IBD stopor take episodically their treatment. Consequently,a nondrug therapy targeting TNFa through aphysiological pathway, devoid of major side effectsand with a good cost-effectiveness ratio, would beof interest. The vagus nerve has dual anti-inflam-matory properties through its afferent (i.e.hypothalamic–pituitary–adrenal axis) and efferent(i.e. the anti-TNFa effect of the cholinergic anti-inflammatory pathway) fibres. We have shown thatthere is an inverse relationship between vagal toneand plasma TNFa level in patients with CD, andhave reported, for the first time, that chronic vagusnerve stimulation has anti-inflammatory proper-ties in a rat model of colitis and in a pilot studyperformed in seven patients with moderate CD.
Two of these patients failed to improveafter 3 months of vagus nerve stimulation but fivewere in deep remission (clinical, biological andendoscopic) at 6 months of follow-up and vagaltone was restored. No major side effects wereobserved. Thus, vagus nerve stimulation providesa new therapeutic option in the treatment of CD.
Keywords: inflammatory bowel disease, vagus nerve,vagus nerve stimulation.
Abbreviations: ACh, acetylcholine; ANS, autonomicnervous system; CAN, central autonomic network;CAP, cholinergic anti-inflammatory pathway;CDAI, Crohn’s disease activity index; CD, Crohn’sdisease; CDEIS, Crohn’s disease endoscopic indexof severity; CRP, C-reactive protein; DMNV, dorsalmotor nucleus of the vagus; DNBS, dinitrobenzenesulphonic; DSS, dextran sulphate sodium; EEG,electroencephalogram; fMRI, functional magneticresonance imaging; GI, gastrointestinal; HPA, hy-pothalamic–pituitary–adrenal; HRV, heart ratevariability; IBD, inflammatory bowel disease; IL,interleukin; LC, locus coeruleus; LPS, lipopolysac-charide; MAPK, mitogen-activated protein kinase;MPOA, myeloperoxidase activity; NTS, nucleustractus solitarius; PB, parabrachial nucleus; PVH,paraventricular nucleus of the hypothalamus; RA,rheumatoid arthritis; TNBS, trinitrobenzene sul-phonic acid; TNF, tumour necrosis factor-alpha;tVNS, transcutaneous vagus nerve stimulation;UC, ulcerative colitis; VNS, vagus nerve stimula-tion; VN, vagus nerve; a7nAChR, alpha7nicotinicacetylcholine receptor.
Introduction
Inflammatory bowel disease (IBD) is a group oforganic diseases, classically divided into Crohn’s
disease (CD) and ulcerative colitis (UC), involvingthe gastrointestinal (GI) tract, particularly thecolon and small intestine for CD, starting early inlife (between 15 and 30 years) and evolving by
46 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Key Symposium

alternating periods of flares and remissions ofvariable duration. Symptoms are characterized byabdominal pain, diarrhoea, fever, weight loss andextra-intestinal (skin, eyes, joints) manifestations.IBD affects about 1.5 million persons in the USAand 2.2 million in Europe. One hypothesis toexplain the rising incidence and prevalence ofIBD is the ‘Westernization’ of our lifestyle.
The pathophysiology of IBD involves immunolog-ical, genetic and environmental factors [1]. Stress,through brain–gut interactions, may play a role[2]. Indeed, stress increases intestinal permeabil-ity, modifies immunity and stimulates the sympa-thetic nervous system whilst inhibiting the vagusnerve (VN) thus disturbing the equilibrium of theautonomic nervous system (ANS). An imbalance ofthe ANS has been reported in IBD, with sympa-thetic dysfunction in CD [3] and vagal dysfunctionin UC (4). We have reported that dysautonomia inIBD may be dependent on psychological adjust-ment [4] and correlated with a pro-inflammatoryprofile [5].
Medical treatment is not curative in IBD, and thereis a recurrence of the disease after treatmentdiscontinuation. IBD treatment is represented bysteroids, immunosuppressants (azathioprine, mer-captopurine, methotrexate) and biological agents[antitumour necrosis factor-alpha (TNFa), anti-adhesion molecules]. TNFa is a key cytokine inIBD and anti-TNFa therapies are presently the goldstandard treatment [6]; however, a large proportionof patients with IBD become refractory to availabletherapeutic options partly due to side effects [7].This may explain why 20–40% of patients with IBDare not compliant with treatment [8].
Thus, nondrug therapies, represented by leucocy-tapheresis, faecal transplantation and stem cell-based therapies, appear of interest in the treatmentof IBD and are popular with patients. Amongstthese nondrug therapies, the emerging field ofbioelectronic medicine, based on the bidirectionalinteraction between the nervous system and theimmune system in the regulation of inflammation,is topical. These neuro-immune interactions aredysregulated in IBD. Neuromodulation, as a ther-apeutic approach, opens a new era in the treatmentof IBD. Amongst the potential therapeutic neuronalpathways, the VN, based on its anti-inflammatoryproperties, is the most likely therapeutic target inparticular through VN stimulation (VNS).
Anatomy of the VN
The VN is the longest nerve in the body innervatingnumerous organs including the GI tract. The VN isthe main component of the parasympathetic ner-vous system. The VN innervates all the GI tractexcept the rectum in the rat [9] and until thesplenic flexure in humans [10]; the distal GI tract(i.e. the left colon and rectum) is innervated by thesacral parasympathetic nucleus through the pelvicnerves. However, some anatomists consider thatthe VN innervates all the GI tract in humans [11].The VN is a mixed nerve composed mainly ofunmyelinated fibres, with 80% afferent fibreswhich convey visceral, somatic and taste sensa-tions and 20% efferent fibres which are involved inthe control of GI motility and secretion.
Preganglionic neurons of vagal efferents originatein the dorsal motor nucleus of the vagus (DMNV)located in the medulla, below the nucleus tractussolitarius (NTS) which receives vagal afferents. Inthe GI tract, these preganglionic neurons areconnected to postganglionic neurons of the entericnervous system (i.e. the ‘gut brain’) which providesautonomy to the functioning of the GI tract.Acetylcholine (Ach), the neuromediator of the VN,is released both at the ends of the VN, binding tonicotinic receptors, and at the ends of the post-ganglionic neurons localized in the enteric nervoussystem, binding to nicotinic or muscarinic recep-tors. Vagal efferent fibres do not reach directly tothe intestinal lamina propria [12] but form cholin-ergic synapses onto enteric neurons innervatingthe lamina propria that respond to locally releasedinflammatory stimuli [13]. These enteric neuronsare the ultimate effectors in the regulation of gutimmunity, but are under the influence of the VN[14].
Vagal afferent fibres originate from the mucosa tothe muscle layers of the GI tract with their cellbodies located in the nodose ganglia. They relayinformation to the NTS, with a rostro-caudalviscerotopy [15], and to the area postrema locatedin the medulla, above and in close proximity to theDMNV to form the dorsal vagal complex. Vagalafferents are able to detect peripheral immune-related events and to generate adapted autonomic,endocrine and behavioural responses via centralreflex pathways. The NTS sends viscerosensoryinformation to the DMNV to influence the func-tioning of vagal efferent fibres through vago-vagal
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 47
Journal of Internal Medicine, 2017, 282; 46–63

reflexes [16]. Vagal sensory information arriving inthe NTS is also projected to numerous areas of theCNS [17–19] such as the parabrachial (PB) region,the locus coeruleus (LC), the periventricularnucleus of the thalamus, the central nucleus ofthe amygdala, the paraventricular nucleus of thehypothalamus (PVH), the medial preoptic area,the arcuate nucleus of the hypothalamus and theventrolateral medulla (A1 noradrenergic nucleus).This integration of visceral information generatesan autonomic, behavioural and endocrineresponse. NTS neurons may directly modulate theactivity of neurons of the LC and its widespreadnoradrenergic projections [20]. Neurons of therostral ventrolateral medulla provide one of twomajor sources of afferent inputs to the LC [21],which sends projections to widespread areas of thecortex involved in stress-related behaviours andaffective disorders [22]. The PVH projects to the bednucleus of the stria terminalis, the dorsomedialand arcuate hypothalamic nuclei, the medial pre-optic area, the periventricular nucleus of the tha-lamus, the PB region and the nucleus tegmentidorsalis lateralis [23]. The PB nucleus in turnprojects to the central nucleus of the amygdala, thebed nucleus of the stria terminalis and the PVH[24]. The PVH projects directly to the NTS [23],thereby establishing a feedback loop between theNTS and the forebrain. Thus, visceral informationvehiculated by the VN is integrated in a centralautonomic network (CAN) which modulates thefunctioning of the ANS and the endocrine response[i.e. the hypothalamic–pituitary–adrenal (HPA)axis]. Zagon has questioned whether the VN couldmediate the sixth sense [22], based on the hypoth-esis that sensory inputs originating from the inter-nal environment, such as ‘gut feelings’, act tomodify the perception of the outside world andinfluence the elicited behavioural response.
Anti-inflammatory properties of the VN
The VN has a dual anti-inflammatory role throughboth its afferent and efferent fibres. The anti-inflammatory properties through the activation ofvagal afferentswerefirst describedbyHarris in1950[25]. Indeed, peripheral lipopolysaccharide (LPS)administration induces the release of pro-inflam-matory cytokines such as interleukin (IL)-1b, whichactivates vagal afferents by binding to glomus cellsof most paraganglia of the VN that express IL-1receptors [26]. This effect is prevented by vagotomy[27]. Subsequently, neurons activated in the NTSsend projections to corticotrophin-releasing factor-
containing neurons of the parvocellular part of thePVH inducing the release of adrenocorticotropichormone by the pituitary thus stimulating gluco-corticoid secretion by the adrenal glands. This anti-inflammatory pathway is known as the HPA axis.
The anti-inflammatory properties of vagal efferentfibres were more recently described by Tracey andcolleagues in 2000. These authors showed thatseptic shock induced in rats by intravenous LPSwas prevented by VNS of the distal cut end of theleft cervical VN trunk thus activating efferent fibres[28]. VNS inhibited TNFa synthesis in the liver,attenuated peak serum TNFa levels and preventedthe development of shock. They showed that Ach,which is thought to be released at the distal end ofthe VN, decreased the release of pro-inflammatorycytokines such as TNFa, IL-1b, IL-6 and IL-18, butnot the anti-inflammatory cytokine IL-10, in LPS-stimulated human macrophage cultures. They ter-med this neuro-immune pathway through vagalefferents ‘the cholinergic anti-inflammatory path-way’ (CAP) through which the brain modulatessystemic inflammatory responses to endotoxin [29](Fig. 1). This pathway was incorporated into an‘inflammatory reflex’ in which the activation ofvagal afferents by LPS was followed by stimulationof vagal efferents through a vago-vagal excitatoryanti-inflammatory reflex. This group also showedthat the Ach receptor that was involved in thisreflex was the a7 nicotinic Ach receptor (a7nAChR)of macrophages, because this effect was dampenedin a7 knockout animals [30]. At the cellular level,the CAP acts through a7 subunit-mediated Jak2-STAT3 activation [31] and miR-124 modulatesLPS-induced cytokine production by targeting sig-nal transducer and activator of STAT3 to decreaseIL-6 production and TNFa-converting enzyme toreduce TNFa release [32].
However, the exact anatomical interaction betweenthe VN and intestinal macrophages is the subject ofdebate as the VN is not directly connected toresident macrophages in the gut. Indeed, the VNinteracts with enteric neurons which express neu-ronal nitric oxide synthase, vasoactive intestinalpeptide and choline acetyltransferase and arelocated within the gut muscularis in close contactwith these macrophages [33]. Thus, the vagalmodulation of these intestinal macrophages is notdirectly mediated by vagal efferents but throughthese enteric neurons. Mikkelsen et al. [34] did notobserve any contact between vagal efferents andresident macrophages; however, contact between
Vagus nerve stimulation in IBD / B. Bonaz et al.
48 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2017, 282; 46–63

cholinergic myenteric neurons and macrophagesexpressing the a7nAChR was recently described byMatteoli et al. [35].
Is the spleen a target of the CAP?
The spleen, a source of TNFa, is innervated by thesympathetic splenic nerve originating from thecoeliac ganglion [36]. Tracey and colleagues havesuggested that the VN activates the splenic nervethrough a vago-sympathetic synergistic effect [37](Fig. 1). They showed that Ach was released in thecoeliac mesenteric ganglia by VNS and then boundto the postsynaptic a7nAChR of the splenic nerveto release noradrenaline in the spleen [38]. It wasshown that noradrenaline binds to the beta2adrenergic receptor of splenic lymphocytes whichrelease ACh that acts on the a7nAChR of splenicmacrophages to inhibit the release of TNFa by thespleen [39]. In such a way, the VN could have ananti-TNFa effect either indirectly on peripheralmacrophages or at the level of the spleen.
However, this anatomical pathway is debated assome authors did not find any direct or indirectinnervation of the spleen by the VN [40], whereasothers have reported that VN efferent fibres inner-vate the coeliac and superior mesenteric ganglia inthe coeliac plexus [41, 42]. Cholinergic nerve fibressurrounding catecholaminergic neurons wereobserved in the coeliac ganglia in mice [43]. Buijset al. [44] showed that the spleen receives not onlya sympathetic input via the arteries but also aparasympathetic input via both tips of the spleen.Gautron et al. [45] reported that the cholinergicfibres observed in the spleen originate from cholin-ergic postganglionic sympathetic neurons located
in the paravertebral and/or prevertebral chains.Activation of the CAP observed after central cholin-ergic activation by intracerebroventricular infusionof the M1 muscarinic ACh receptor agonist in miceis suppressed after vagotomy or splenic neurec-tomy [46]. However, Cailotto et al. [33], usinganterograde tracing, did not reveal any dextran-labelled vagal fibres in the mesenteric ganglion orspleen. Martelli et al. [47] proposed a model with anon-neural link between the VN and the spleenwhere the a7nAChRs are located on the peripheralterminals of the splenic sympathetic nerves. Whenstimulated by ACh from incoming T cells, theseterminals release noradrenaline which binds tobeta adrenergic receptors on splenic macrophagesto suppress their release of TNFa.
The involvement of the spleen in the CAP has alsobeen described by Ji et al. [48] who showed thatcentral cholinergic activation induced by theacetylcholinesterase inhibitor galantamine or amuscarinic ACh receptor agonist improved colitisin mice and this effect was suppressed aftervagotomy, splenic neurectomy or splenectomy.Xue et al. [49] also showed that VNS failed toprotect against septic shock in rats followingsplenectomy or common coeliac branch vagotomy,indicating that the spleen may be a vital target ofthe CAP. Recently, Inoue et al. [50] confirmed theinvolvement of splenocytes in the anti-inflamma-tory effect of a preventive 10-min VNS in a mousemodel of ischaemia–reperfusion injury (Table 1).Moreover, this effect was only observed witha7nAChR-positive splenocytes and not with a7-knockout mice splenocytes. We have also shownthat a concomitant 3-h VNS in acute trinitroben-zene sulphonic acid (TNBS)-induced colitis in rats
TNFα
Lymphocytes
ACh
Macrophages NE
Spleen
Activation of the HPA axis
Ach?Celiac ganglion
Macrophage
ACh
α7nAChR
Cytokines
ACh
Entericneuron
NE
Preganglionicsympatheticneuron
Adrenalchromaffin cells
Peripheral blood NE/EPI
Splenic nerve NETNFα
NE
The vago-parasympatheticreflex
The vago-sympatheticreflex
NTSDMNV
Fig. 1 Pathways targeted bythe vagus nerve (VN) for itsanti-inflammatory properties(from [112]). Ach, acetylcholine;NE, noradrenaline; TNFa,tumour necrosis factor-alpha;HPA, hypothalamic–pituitary–adrenal; VNS, vagus nervestimulation; a7nAChR,alpha7nicotinic acetylcholinereceptor; E, norepinephrine;and EPI, epinephrine.
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 49
Journal of Internal Medicine, 2017, 282; 46–63

Table 1 Chronic inflammatory diseases as potential indications for treatment with vagus nerve stimulation (VNS):experimental and clinical studies
Inflammatory
disease VNS device and stimulation parameters Primary outcome References
Rheumatoid arthritis Cyberonics VNS implantable
system
Change in rheumatoid arthritis
DAS
Clinical trial:
NCT01552538
(ongoing)
Rheumatoid arthritis Cyberonics implantable VNS
system (60 s at tolerated
output current, 10 Hz, 250 ls
pulse width, 4 times/day)
Inhibition of TNFa production
Disease severity improvement
[94]
Juvenile idiopathic
arthritis
t-VNS NEMOS� device Effect of tVNS on the in vitro
release of LPS-inducible IL-1
and IL-6 from whole blood
Clinical trial:
NCT01924780
(ongoing)
Kidney
ischaemia–reperfusion
injury
Implantable VNS electrodes in
mice (50 lA intensity,
frequency 5 Hz, duration
1 ms, 10 min)
Decrease plasma TNFa
Involvement of splenocytes
[50]
Sepsis Cervical stimulation and t-VNS Decrease plasma TNFa [114]
Hypertension Animal model, intermittent
VNS (20 Hz, pulse width
500 ls, 1.0 mA, 7 s on/66 s
off); Cyberonics VNS system
(implantable)
Decrease in mean arterial
blood pressure and
arrhythmia episodes
[115]
Hypertension Acute VNS (10–30 Hz, 0.5–
3 mA, 10 s on/>2 min off or
until basal values); multi-
electrode spiral cuff
Decreased heart rate and blood
pressure
Clinical trial:
NCT00983632
(completed)
Case study [116]
Crohn’s disease Chronic VNS animal model of
colitis (Cyberonics device;
5 Hz, 1 mA, pulse width
500 ls, 10 s on/90 s off,
continuously for 5 days)
Decrease in mRNA pro-
inflammatory cytokines (IL-6,
TNFa) and MPOA
Improvement in macroscopic
index of colitis
[88]
Crohn’s disease Chronic VNS (Cyberonics
device; 10 Hz at tolerated
output intensity, 500 ls, 30 s
on/5 min off continuously)
Improvement in clinical
disease index, endoscopic
index, HRV, CRP, EEG and
faecal calprotectin
Clinical trial:
NCT01569503
(ongoing) and
[91,92]
Postoperative ileus Interventional abdominal VNS Gastrointestinal transit and
symptoms and pro-
inflammatory cytokines
Clinical trial:
NCT02524626
(ongoing)
Postoperative ileus Acute abdominal VNS in pig
model of POI (5 and 20 Hz,
0.5 and 1 ms pulse width)
Safety and feasibility [117]
Vagus nerve stimulation in IBD / B. Bonaz et al.
50 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2017, 282; 46–63

is able to modify splenocyte activation [51]. How-ever, the anatomical interaction between theperipheral cholinergic system and immune cells isstill unclear because of technical difficulties withthe presently available neuroanatomical methods.Besides the release by neurons, ACh can also bereleased by epithelial and immune cells, theso-called non-neuronal ACh [52]. The immunecell-derived ACh suppresses the release of pro-in-flammatory cytokines by macrophages. Thus, thegut-associated lymphoid tissue may play a role inthe immunomodulatory actions of peripheral AChand VNS.
Nonvagal theory of the inflammatory reflex: the splanchnic anti-inflammatory pathway
Recently, Martelli et al. [53] did not observe anyeffect of vagotomy on the TNFa response to LPS,arguing that the VN was not involved in the CAP,whereas Borovikova et al. [28] reported a 20%higher concentration of plasma TNFa in vago-tomized rats. In addition, Borovikova et al. showedthat vagotomized animals had significantly lowerconcentrations of plasma corticosterone; by con-trast, Martelli et al. [47] found that all animals,whether or not vagotomized, had the same level ofcorticosterone. The increased levels of TNFaobserved by Borovikova et al. could be explainedby the lower corticosterone levels found in vago-tomized animals. Both splenic and splanchnicnerves are activated after intravenous LPS adminis-tration [54], but this activation was not suppressedafter vagotomy whereas splenic sympathetic nerveactivity returned to baseline levels after cutting thesplanchnic nerve, which induced a huge increase inTNFa levels [55]. Based on these results, the sameauthors [53] argued that the splanchnic anti-inflammatory pathway is the efferent arm of a
neural reflex that controls inflammation. It shouldbe noted that these data have been obtained in amodel of septic shock with intraperitoneal or intra-venous LPS administration and must be confirmedin other inflammatory models. Both the sympa-thetic and parasympathetic (VN) systems could alsofunction synergistically or alternatively accordingto the homeostatic state, to control exacerbatedinflammatory responses. The VN can control sple-nic nerve activity indirectly through a CNS reflex,but not through a direct efferent pathway. Indeed,activation of the coeliac ganglion, at the origin of theinnervation of the spleen, could be mediated bybrain nuclei which are part of the CAN and thatgenerate patterns of autonomic responses via theirprojections to preganglionic sympathetic neuronsin the spinal cord. Moreover, the sympatheticoutflow is regulated by five cell groups in the brain[56, 57]: the PVH, the A5 noradrenergic cell group,the caudal raphe region, the rostral ventrolateralmedulla and the ventromedial medulla. Activationof the afferent arm of the inflammatory reflex couldactivate the CAN, through projections from the NTS,to modulate the sympathetic nervous systemthrough these five cell groups. In such a pathway,the VN could thus induce an indirect anti-inflam-matory reflex by activating the sympathetic nervoussystem.
Role of the VN and the CAP in experimental models of colitis
The anti-inflammatory role of the VN has beendemonstrated in animal models of dextran sul-phate sodium (DSS)- [58] and TNBS-induced colitis[59] following vagotomy [58] or peripheral or cen-tral injection of cholinesterase inhibitors [60].
The first experimental study was performed byMiceli and Jacobson in 2003 [60]. The authors
Table 1 (Continued )
Inflammatory
disease VNS device and stimulation parameters Primary outcome References
Systemic lupus
erythematosus
tVNS (5 min daily for 4
consecutive days)
Musculoskeletal pain
SLE disease activity
Inflammatory cytokines
Clinical trial:
NCT02822989
(ongoing)
Systemic lupus
erythematosus
VNS concept for SLE [118]
DAS, disease activity score; TNFa; tumour necrosis factor-alpha; t-VNS, transcutaneous vagus nerve stimulation; LPS,lipopolysaccharide; IL, interleukin; MPOA, myeloperoxidase activity; HRV, heart rate variability; CRP, C-reactive protein;EEG, electroencephalogram; SLE, systemic lupus erythematosus; POI, postoperative ileus.
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 51
Journal of Internal Medicine, 2017, 282; 46–63

examined the role of the CAP in modulating theseverity of acute dinitrobenzene sulphonic (DNBS)acid-induced colitis in rats, a classical model ofUC. They used anticholinesterase drugs in cholin-ergic hyper-responsive and resistant Flinder’s ratswith colitis. These rats were obtained by selectivebreeding of Sprague Dawley rats for low (Flindersresistant) and high (Flinders sensitive) sensitivityto the anticholinesterase agent diisopropyl fluo-rophosphate [61]. The Flinders sensitive ratsshowed enhanced behavioural and physiologicalresponses to cholinergic agonists and had elevatedlevels of muscarinic receptors in several brainregions, whereas the response of Flinders resistantrats to cholinergic agonists was similar to that ofrandomly bred Sprague Dawley rats [61, 62]. Theseverity and characteristics of colitis in the Flin-der’s rats were compared with the inflammatoryresponse in Sprague Dawley rats. The animalsreceived an acetylcholinesterase inhibitor,physostigmine (central and peripheral inhibitor)or neostigmine (peripheral inhibitor), 30 minbefore the induction of colitis and controls receivedsaline. The contribution of peripheral versus cen-tral cholinergic modulation of DNBS-induced col-itis was compared by studying macroscopicdamage score, myeloperoxidase activity [(MPOA)an estimate of granulocyte infiltration] and smoothmuscle thickness in the colitis segment. Comparedto control Sprague Dawley rats with colitis, nosignificant increase in these characteristics wasobserved in Flinders sensitive rats. Neostigmineand physostigmine pretreatment improved all theinflammatory characteristics; the effect was signif-icantly higher with physostigmine thus supportinga greater protective effect of the central pathway.
Ghia et al. have investigated the protective effect ofthe VN in experimental models of colitis. In aninitial study [58], they assessed the disease activityindex, macroscopic and histological damage,serum amyloid-P level and MPOA in rats withDSS-induced colitis, in healthy and vagotomizedC57BL/6 mice, and in mice deficient in macro-phage colony-stimulating factor-induced and withDSS-induced colitis. They showed that the VNplays an anti-inflammatory role in colitis via amacrophage-dependent mechanism involving nico-tinic receptors. In a further study [63], the authorsexamined whether vagal integrity confers long-lasting protection by studying DNBS- and DSS-induced inflammatory responses in the colon at9–61 days postvagotomy. The increase in inflam-matory indices was substantially diminished in
mice with colitis induced 21, 33 and 61 dayspostvagotomy. This was accompanied by increasedproduction of IL-10, TGF-b, FOXP3 and corticos-terone. These findings indicate that if vagal integ-rity is an important protective factor, othercounter-inflammatory mechanisms play a role ifvagal integrity is compromised beyond 2 weeks.The same group has also shown that centralcholinergic activation by treatment with the acetyl-cholinesterase inhibitor galantamine or a mus-carinic ACh receptor agonist improved colitis inmice through a VN-to-spleen circuit and that thiseffect was abolished by vagotomy or splenicneurectomy [48].
Vagal tone in patients with IBD
As mentioned above, IBD involves the brain–gutaxis and thus the ANS as a mediator. Conse-quently, exploring the activity of the ANS andparticularly vagal tone is of major interest. Severalmethods are available to investigate autonomicactivity, and each will have advantages and disad-vantages. Amongst these methods, heart rate vari-ability (HRV) is a reliable noninvasive tool that canbe used to quantify vagal activity. It is not time-consuming and can easily be used in routineclinical practice provided good HRV practice isrespected. HRV has the potential to provide addi-tional valuable insight into physiological andpathological conditions and to enhance risk strat-ification and prediction [64]. HRV reflects beat-to-beat changes in RR intervals which are related tothe efferent sympathetic and parasympatheticfibres of the ANS. Parasympathetic fibres arecarried in the VN. The sinoatrial node is thepacemaker responsible for the initiation of theheartbeat and displays an intrinsic rhythm at amean rate of 100–110 action potentials per min.This intrinsic rhythm is primarily influenced byautonomic nerves. At rest, the influence of the VNis greater than that of the sympathetic nerve. Thisvagal tone reduces the resting heart rate to 60–80 beats per min. Respiration is a major driver ofthe autonomic input to the sinus node, with adecrease in vagal input during inspiration and anincrease during expiration at the origin of thesinusoidal variation of heart rate; the amplitudeof the variation reflects the importance of vagalbrake [65]. A decrease in vagal tone induces areduction in HRV. A variety of internal and externalstimuli that change the balance between sympa-thetic and vagal tone influences the moment-to-moment heart rate. ANS imbalance with a shift
Vagus nerve stimulation in IBD / B. Bonaz et al.
52 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2017, 282; 46–63

towards increased sympathetic and decreasedvagal tone is associated with a higher risk ofchronic diseases. Taking into account the vis-cera–brain relationships, HRV assessment isbecoming an important marker in the detection ofvagal tone impairment and thus the impairment ofthe CAP. This should be useful in the prediction ofprognosis in several chronic inflammatory diseases[65]. Separate investigations of HRV in IBD, CDand UC have revealed that during remission, somepatients exhibit low vagal tone. In an initial study[4], we observed that vagal tone was related to theemotional adjustment of patients (high vs. lownegative emotions) and to their way of coping withthe disease. A positive coping style had a biologicalcost, for instance in CD, as it was associated withlow vagal tone. In contrast in UC, a positive copingstyle was associated with high vagal tone. Thisstudy revealed the importance of (i) separatingpopulations of patients with IBD within studiesand (ii) psychological factors on vagal tone. Morerecently, we have shown that patients with CD whohave low vagal tone at rest present higher plasmalevels of TNFa and higher salivary levels of cortisolthan patients who exhibit high vagal tone [5]. Thisimportant finding highlighted the shift of theparasympathetic balance towards a stress modein this disease as a form of allostatic load associ-ated with dysregulation of the innate immuneregulation of pro-inflammatory cytokines by theVN. This disruption of the homeostatic status andthe impairment of the CAP make patients morevulnerable to stressful life events and to the emer-gence of a flare. Consequently, measuring restingvagal tone over time may be useful (i) to predict thisvulnerable state, (ii) to determine the need for anadapted enforcement therapy such as VNS and (iii)to follow the efficacy of this therapy on theparasympathetic system.
VNS
VNS was first performed for suppression of sei-zures by JL Corning in the early 1880s [66] but notused again until 1938 when Bailey and Bremer [67]reported that VNS in the cat synchronized theactivity in the orbital cortex. The first VNS devicefor the treatment of drug-resistant epilepsy inhumans was reported in 1990 [68]. VNS wasapproved by the European Medicines Agency andthe US Food and Drug Administration (FDA) for thetreatment of drug-refractory epilepsy in Europe in1994 and in the USA in 1997, respectively. VNSwas also approved in 2005 by the FDA for drug-
refractory depression, based on improvements infeeling of well-being, mood, alertness, memory andthinking skills, independent of seizure activity, inpatients who received implantable VNS for refrac-tory epilepsy and a 1-year open-label extension of anegative sham-controlled study in 205 patientsperformed over 10 weeks [69, 70]. More than100 000 VNS devices have been implanted forepilepsy and ~4000 for depression (data fromCyberonics, Houston, TX, USA).
The numerous central projections of the VN arelikely to be responsible for the anti-epileptic andantidepressive properties of vagal afferent stimu-lation in humans although the neuronal mecha-nisms are still not well understood. Amongst brainstructures involved in the effects of VNS, theneocortex, hippocampus, thalamus and LC play arole [71]. A role of vagal afferent C-fibres has beenproposed in the anti-epileptic effect of VNS buttheir destruction did not suppress the influence ofVNS on the inhibition of seizures in rats thussuggesting that activation of vagal A- and B-fibreswas involved [72].
Five different parameters (intensity, frequency,pulse width, on-time and off-time) of stimulationare used for VNS in epilepsy and depression: forexample, intensity 0.5–3.5 mA, frequency 20–30 Hz, pulse width 250–500 ls and stimulationon-time 30–90 s followed by 5 min off-time. A largerange of frequencies (2–300 Hz) of VNS-inducedelectroencephalographic desynchronization of the‘enc�ephale isol�e’ cat that was abolished by aligature of the proximal end of the vagal trunk[73], thus supporting a role of vagal afferent fibresin this effect. High-frequency VNS is more effectivethan low-frequency VNS [74]. Frequencies of 50 Hzand above induced irreversible damage of the VN[75]. VNS performed using anti-epileptic parame-ters induced c-fos expression in rat brain nucleiinvolved in the genesis and regulation of seizuressuch as the amygdala, cingulate cortex, LC andhypothalamus [76]. Human brain imaging studieshave shown modifications in regions that receiveVN afferents such as the thalamus, cerebellum,orbitofrontal cortex, limbic system, hypothalamusand medulla [77]. A 50% seizure reduction isobserved in patients after 2–3 years of VNS treat-ment, showing that a long latency is required forthe efficacy of this treatment [78].
VNS is classically performed through a spiralelectrode wrapped around the left cervical VN in
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 53
Journal of Internal Medicine, 2017, 282; 46–63

the neck [79]. To avoid major cardiac adverseevents, VNS is performed on the left VN becauseof a weaker influence on the heart rate than theright VN (the left VN innervates the atrioventricularnode and the right VN innervates the sinoatrialnode) [80]. The electrode wrapped on the left VN isconnected via a subcutaneous cable to a pulsegenerator located in the left chest wall. The elec-trode is implanted (~1-h duration) under generalanaesthesia by a neurosurgeon. The VNS device ismanufactured by Cyberonics and composed of apair of helical electrodes (2 or 3 mm diameter), abattery-powered generator, a tunnelling tool, soft-ware and programming tools (http://us.cyberonics.com/en/). The price of the generator pulse(model 102) plus the electrode (model 302) isapproximately €9300. Due to the use of a lower-frequency stimulation than for epilepsy (10 Hz vs.20/30 Hz), the generator battery is longer lasting(~5–10 years) for CD treatment. Implantable VNS issafe and well tolerated and withdrawals are rare[74]. The most common minor adverse events arevoice alteration, cough, dyspnoea, paraesthesia,nausea, headache and pain, which decline overtime and are easily controlled by reducing stimu-lation intensity [81].
Because the concept of the CAP is based on theinvolvement of vagal efferents, VNS is used at lowfrequency (1–10 Hz) in inflammatory conditions.Indeed, in the referent work of Borovikova et al.[28], VNS was performed in rats with cervicalvagotomy and applied at low frequency to thedistal cut end (thus stimulating vagal efferents) ofthe VN using the following parameters: 5 V, 2 msand 1 Hz. Bernik et al. [82] performed VNS ofeither the left or right VN, in anesthetized Lewisrats with intact vagi, at either 1 or 5 V (2 ms, 5 Hz)for 20 min continuously, during LPS injection. Theauthors showed that VNS prevented endotoxin-induced hypotension, and this effect was preventedby surgical or chemical vagotomy. de Jonge et al.[31] performed VNS in a mouse model of postop-erative ileus (intestinal manipulation) by stimulat-ing the distal part of the ligated or cut left VN trunkthus activating vagal efferents. VNS (5 Hz for 2 msat 1 or 5 V) was performed 5 min before and15 min after intestinal manipulation. VNSimproved postoperative ileus by activating STAT3in intestinal macrophages. In a murine model ofburn-induced intestinal barrier injury, Costantiniet al. [83] performed VNS (1 Hz, 2 mA) of the rightVN and showed increased activation of enteric glialcells and attenuation of the burn-induced
intestinal barrier injury. This protective effect wasprevented by abdominal vagotomy, thus confirm-ing that VN efferent fibres are involved in themodulation of gut barrier integrity after injury. Thesame group [84] also showed that VNS preventedtrauma/haemorrhagic shock-induced decrease inthe CD103+ dendritic cell population and modu-lated the Treg/Th17 balance in the mesentericlymph node. VNS promotes tolerance to inflamma-tion in the gut, thus supporting its ability tomodulate the inflammatory set point and to alterthe response to injury. O’Mahony et al. [85] haveshown that the loss of vagal anti-inflammatorysignalling is associated with reduced numbers ofCD4+CD25+Foxp3+ Treg cells in mice with DSS-induced colitis. VNS performed at 10 Hz, preferen-tially activating vagal efferents, did not inducedeleterious side effects [77, 86], and no significantdifference was found in withdrawal rates betweenhigh and low stimulation groups in a recentCochrane review [74]. Low-frequency (5–10 Hz)VNS is considered to activate vagal efferents;however, we have shown in a functional magneticresonance imaging (fMRI) neuronal connectivitystudy in anaesthetized rats with intact vagi thatlow-frequency VNS is also able to activate vagalafferents [87]. This is in agreement with the abovehypothesis that the anti-inflammatory effect of theVN may be indirect via the CNS.
VNS in IBD
We have reported the first study of VNS in anexperimental model of TNBS-induced colitis (Th-1-induced inflammation) resembling CD in awakerats [88] (Table 1). Chronic VNS was performedwith an external stimulator in freely moving ani-mals for 5 days (3 h day�1), starting 1 h beforeinduction of colitis, using stimulation parametersadapted from previous studies: 1 mA, 5 Hz,500 ls, 10 s on/90 s off (continuous cycle) [89].Control rats received an implant but were notstimulated. Colonic inflammation was controlledusing physiological (e.g. body weight, temperature,locomotor activity), macroscopic (area of lesions),histological and biological characteristics (e.g.MPOA, cytokine and cytokine-related mRNAs),both at the level of the damaged colon andimmediately above (1-cm length proximal to themost anterior aspect of the macroscopicallyobserved damage) where colitis was less severe.A multivariate index of colitis using these charac-teristics was then generated for better character-ization of colonic inflammation (Fig. 2). VNS
Vagus nerve stimulation in IBD / B. Bonaz et al.
54 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2017, 282; 46–63

reduced body weight loss and inflammatory mark-ers as observed above the lesion by histologicalscore and MPOA quantification. The anti-inflam-matory effect of VNS was also confirmed by theimprovement of the multivariate index of colitis.These results have potential therapeutic implica-tions for the treatment of patients with IBD. In asimilar approach, Sun et al. [90] performed VNSfor 3 h per day for 6 days (0.25 mA, 20 Hz,500 ms, 30 s on/5 min off continuously) in amodel of TNBS-induced colitis in rats. The effectof chronic VNS on colonic inflammation wasevaluated by disease activity index, histologicalscores, MPOA and production of inducible nitricoxide synthase, TNF-a and IL-6. The expressionlevels of mitogen-activated protein kinases (MAPK)family members, IjB-a and nuclear NF-jB p65were determined by immunoblotting. All thesefactors were significantly decreased by VNS. Inaddition, VNS reduced the phosphorylation ofMAPKs and prevented the nuclear translocationof NF-jB p65. Even though the stimulation fre-quencies were not identical (5 Hz in our study forefferent VNS vs. 20 Hz in the study by Sun et al.[90] for afferent VNS), both these studies showedthat VNS decreases colonic inflammation. Sunet al. also performed HRV analysis to evaluate the
sympatho-vagal balance and showed that VNSsignificantly restored this balance and particularlyvagal tone that was altered by colitis.
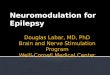
In a translational approach, we performed a pilotstudy of VNS in patients with CD (ClinicalTrial.govidentifier: NCT01569503; Table 1) using VNS as analternative to anti-TNFa treatment or in treatment-na€ıve patients. To date, nine patients with moder-ate CD have been implanted with a Cyberonicneurostimulator (model 102) and electrode (model302), and the following stimulation parameterswere used: intensity 0.5–1.5 mA, frequency 10 Hz,pulse width 500 ls and stimulation on-time 30 sfollowed by 5 min off-time. We have recently pub-lished the 6-month results from the first sevenpatients. The first patient received an implant inApril 2012 and the last patient in December 2014.At the 6-month follow-up, 5 of 7 patients hadresponded to VNS with clinical [Crohn’s diseaseactivity index (CDAI)], biological [C-reactive protein(CRP), faecal calprotectin] and endoscopicimprovement/healing [Crohn’s disease endoscopicindex of severity (CDEIS)] (Table 2). Two patientswho had worsened were withdrawn from the studyafter 3 months; one underwent surgery (ileocecalresection) but still has an active stimulator(1.5 mA), and the other received combinationtherapy (azathioprine plus infliximab) whilst theVNS intensity was turned down to 0.5 mA. Onlyone of the six patients, still receiving VNS at6 months, is also receiving immunosuppressanttherapy (azathioprine) [91]. VNS restored the sym-patho-vagal balance which was disequilibrated atstudy inclusion for all the patients (Fig. 3). Nomajor side effects were observed, in particular noclinically relevant cardiac effects, and the devicewas well tolerated; the pulse generator and leadsdid not have to be removed at any time. The mostcommonminor effects (voice alteration/hoarsenessand throat pain) were those classically describedunder VNS and related to the stimulation (30 s on/5 min off). These results show that VNS is feasibleand is of potential interest in the treatment ofactive CD; however, further investigation in a largerlongitudinal cohort of patients with CD is required.Another clinical study of VNS in CD was recentlylaunched and is ongoing (ClinicalTrials.gov identi-fier: NCT02311660; SetPoint Medical Corporation).
VNS also induced central modifications as observedby electroencephalographic recordings in the firstCD patient to undergo VNS implantation at week 6and months 6, 9 and 12 after implantation.
10Control
VNS/saline
noVNS/TNBS
VNS/TNBS
∗∗∗ ∗∗∗
9
Mul
tivar
iate
Col
itis
Inde
x (r
elat
ive
unit)
876543210
Fig. 2 Vagus nerve stimulation (VNS) improves an exper-imental model of inflammatory bowel disease in rats,shown by the modification of a multivariate index of colitisabove and in the lesion (relative units) for the four groups ofanimals: (i) VNS and trinitrobenzene sulphonic acid(TNBS)-induced colitis (VNS/TNBS); (ii) no VNS and TNBS-induced colitis (noVNS/TNBS); (iii) VNS and no colitis(VNS/saline); and (iv) no stimulation or colitis (control). Asignificant increase in this index was observed in thenoVNS/TNBS group compared to control animals(***P < 0.001). A significant decrease (***P < 0.001) inthis index was observed in the VNS/TNBS group comparedto rats in the noVNS/TNBS group (n ≥ 12). From [88].
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 55
Journal of Internal Medicine, 2017, 282; 46–63
Significant modifications were observed in restingEEGat all frequencybands. In particular, activationwas observed in themediofrontal electrodes for bothlow- and high-frequency bands with the mostimportant activation for the theta band, and addi-tional activation was found in the occipital elec-trodes for the gamma band. Significant correlationswere observed betweenEEGand thehigh-frequencycomponent of HRV, a marker of vagal tone, for eachfrequency band. The changes that we observed inthe theta and gamma bands support involvement offorebrain areas in the effect of VNS on HRV and anindirect pathway of VNS. In addition, the low vagaltone observed in this patient before VNS wasprogressively improved to normal values duringthe 1-year period of VNS and the patient was in deep(clinical and endoscopical) remission [92].
VNS in other inflammatory conditions
VNS should be of interest in other inflammatorydiseases such as rheumatoid arthritis (RA),another TNFa-mediated disease. For example,knockdown of the a7nAChR in RA fibroblast-likesynoviocytes favoured the production of inflamma-tory mediators, and activation of a7nAChR reducedarthritis in an experimental model of RA [93].Therefore, stimulation of the CAP by VNS improvedan experimental arthritis model whilst aggravationof arthritis was observed after unilateral cervicalvagotomy, as well as in a7nAChR-knockout mice.In a translational approach, the authors of thisstudy [93] performed VNS in patients with RA(ClinicalTrials.gov identifier: NCT01552941; Set-Point Medical Corporation). This study was com-pleted in May 2014 and the results have recentlybeen published [94]. They showed that VNS per-formed with the Cyberonics device (30-s stimula-tion; 1.0-mA output current; pulse frequency of20 Hz; pulse width of 500 ls, up to four timesdaily) inhibited production in the peripheral bloodof TNFa (for up to 84 days), IL-1b and IL-6 inpatients with RA. Concomitantly, RA disease sever-ity measured by validated clinical scores improvedsignificantly. This clinical trial has been prolongedby a long-term observational study (ClinicalTrials.-gov identifier: NCT01552538; Table 1). In an inter-esting study, Koopman et al. [95] also reported thatautonomic dysfunction precedes the developmentof RA. They observed lower parasympathetic activ-ity and decreased expression of the parasympa-thetic a7nAChR on peripheral blood monocytes,and higher sympathetic hormone (noradrenaline)levels in patients at risk of developing RA. TheirTa
ble2
Effect
ofvagusnervestimulation(VNS)for6monthsonclinical,biologicalandphysiologicalch
ara
cteristics
insevenCrohn’s
diseasepatients
(from
[91])
CDAI
CDEIS
CRP(m
gL�1)
Faecalcalprotectin
(lgg�1)
Perceivedviscera
l
pain
(VAS0–1
0)
HRV
(LF/HFra
tio)
Pre-V
NS
Post-VNS
M6
Pre-V
NS
Post-VNS
M6
Pre-V
NS
Post-VNS
M6
Pre-V
NS
Post-VNSM6
Pre-V
NS
Post-VNS
M6
Pre-V
NS
Post-VNS
M6
P1
330
121
11
37
0<100
<100
21
8.2
3.2
P2
358
EXIT
30
EXIT
88
EXIT
1577
EXIT
4EXIT
2.1
EXIT
P3
221
107
80
69
<100
<100
43
8.2
1.7
P4
354
EXIT
14
EXIT
166
EXIT
847
EXIT
5EXIT
6.3
EXIT
P5
227
18
02
33500
<100
21
0.3
1.3
P6
233
38
83
21
63500
1706(M
3)
60
4.5
3.5
P7
264
178
72
22
244
<100(M
2)
3.5
21.8
1.4
Active
disease
>150
≥6>5mgL�1
>100lgg�1
––
P,patient;
M,month
;EXIT,patientremovedfrom
stu
dy(stu
dyexit);CDAI,Crohn’s
diseaseactivityindex;CDEIS,Crohn’s
diseaseendoscopic
indexof
severity;CRP,C-reactiveprotein;VAS,visualanaloguescale;HRV,heart
rate
variability;LF,low
frequency;HF,highfrequency.
Vagus nerve stimulation in IBD / B. Bonaz et al.
56 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2017, 282; 46–63

interpretation was that autonomic dysfunctionwould play a role in the aetiopathogenesis of RArather than being the result of chronic inflammation.Thus, evaluation of vagal tone in pro-inflammatoryconditions could be useful for following treatmentefficacy and also as a predictive marker of furtherdisease evolution.
VNS was also studied in postoperative ileus inhumans (ClinicalTrials.gov identifier: NCT01572155; Katholieke Universiteit Leuven) becauseexperimental studies showed that the CAP improvedan experimental postoperative ileus model [96]; theresults of this clinical study are pending.
Noninvasive VNS
The development of new noninvasive VNS tech-niques which do not require surgical implantationof the electrode and neurostimulator, such astranscutaneous VNS (tVNS) of the auricular conchawhich is innervated by the VN [97], is of interest(Fig. 4). Stimulation of this anatomical area of theear has been shown, using fMRI in humans, toactivate brain areas such as the NTS known to havecentral projections from the VN [98]. Stimulation ofthe auricular branch of the VN protects endotox-aemic rats from LPS-induced inflammation [99].The Cerbomed NEMOS stimulator (Erlangen,
Pretreatment Month 6
20Pa�ents
(166)
(88)
123
Study e
Study e4567
15
10
5
#§
0
Pretreatment Month 6
Pretreatment Month 6
Pretreatment Month 6
CDAI
Vagal tone
CDEIS
HFnu
LF/HF
CRPX
X
Ac�ve disease
Remission
Ac�ve disease
Remission
10
50
100
150
200
250
300
350
400
2 3 4Pa�ents
5 6 7
0
0
1
2
3
4
5
6
7
8
10
20
30
40
50
60
70
80
90
100
11
5
6
25
2 3 4Pa�ents
5 6 7
#:faecal calprotec�n > 100 μg g–1; §: faecal calprotec�n < μg g–1
Stud
y ex
it
Stud
y ex
itSt
udy
exit
Stud
y ex
it
\\
Fig. 3 The effects of vagusnerve stimulation in sevenpatients with active Crohn’sdisease over a 6-month follow-up period on clinical [Crohn’sdisease activity index (CDAI)](a), biological [C-reactiveprotein (CRP)] (b), endoscopic[Crohn’s disease endoscopicindex of severity (CDEIS)] (c)and autonomic [high frequencyin normalized units (HFnu; i.e.vagal tone) and low frequency/high frequency ratio (LF/HF;i.e. sympatho-vagal balance)](d) characteristics. Dashedlines show clinical remission,CDAI <150; cut-off level forCRP, 5 lg L�1; endoscopicremission, CDEIS <6;homeostatic range, HFnu 50;and sympatho-vagal balance,equilibrated ratio of LF/HF ~1.From [91].
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 57
Journal of Internal Medicine, 2017, 282; 46–63

Germany) is an external device using an intra-auricular electrode (like an earphone) to stimulatethe auricular branch of the VN [100]. This devicereceived the European approval (CE mark) in 2010for treatment of epilepsy and is currently availablein Germany, Austria, Switzerland and Italy. Like-wise, the electroCore LLC gammaCore device(Basking Ridge, NJ, USA) is a noninvasive VNS totreat primary headache. This device is composed oftwo stainless steel round discs in contact with theskin to deliver a low-voltage electrical signal to thecervical VN through a portable stimulator. Lermanet al. [101] have shown that noninvasive tVNS withthe electroCore device decreases cytokine andchemokine levels in the blood of healthy controlsubjects. Thus, the gammaCore and NEMOSdevices are of potential interest for the treatmentof inflammatory digestive disorders and otherinflammatory conditions such as RA. However,such noninvasive devices are subject to lack ofpatient compliance.
Fig. 4 Different types of device for vagus nerve stimula-tion (VNS). Invasive VNS system (left): VNS therapy system(Cyberonics); noninvasive VNS systems (right): NEMOS(Cerbomed) (top) and gammaCore (electroCore LLC) (bot-tom). From [113].
HypnosisMeditation
Tai ChiYoga...
VNafferents
VNefferents
VNCCK
ACh
a7nAChR
MacrophageTNF
Pharmacologicalactivation:CNI 1493
Galantamine
VNS
Nicotinic agonists:NicotineGTS-21
AR-R17779...
Anti-TNF
Nutritionalstimulation
Fig. 5 Stimulation of thecholinergic anti-inflammatorypathway to dampen tumournecrosis factor-alpha (TNFa)through nicotinic agonists,nutritional stimulation, vagusnerve stimulation (VNS) orcomplementary medicine. From[2]. CCK, cholecystokinin; Ach,acetylcholine; VN, vagus nerve;VNS, vagus nerve stimulation;a7nAChR, alpha7nicotinicacetylcholine receptor.
Vagus nerve stimulation in IBD / B. Bonaz et al.
58 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2017, 282; 46–63

VN modulation through the use of complementary medicine
Acupuncture and meditation seem to activate theVN, increasing its tone and reducing heart rate andrelease of inflammatory cytokines [102]. Acupunc-ture is used in traditional Chinese medicine for thetreatment of a diverse range of disorders of internalorgans. Lim et al. [103] have recently shown thatTNFa production induced by LPS administration inmice was decreased by acupuncture at the zusanliacupoint (stomach36, ST36). Downregulation ofTNFa mRNA and protein levels was observed in thespleen following acupuncture, which was restoredby splenic neurectomy and vagotomy. Hypnosisaffects HRV, shifting the balance of the sympatho-vagal interaction towards enhanced parasympa-thetic activity,concomitantwithreducedsympathetictone [104]. Hypnosis prolongs clinical remission inpatients with quiescent UC [105]. Yoga [106, 107]and mindfulness meditation [108] are also able toincrease vagal tone. Consequently, these comple-mentary approachesmay be useful in the treatmentof patients with IBD through the activation of theCAP. Nutritional therapies may also have an impacton the inflammatory status of the body. Indeed,ingestion of dietary fat stimulates the release ofchemical messengers such as cholecystokinin thatlead to attenuation of the inflammatory response(TNF-a) via the efferent VN and nicotinic receptors[109]. Recent studies showed that high-lipid enteralnutrition improves inflammationand tissuedamage[110]aswell asmucosalmast cell activation throughthe CAP [111]. Figure 5 summarizes the differentmodes of activation of the CAP.
Conclusion
The VN, through the CAP, has an anti-inflamma-tory role. Bioelectronic medicine uses bioelec-tronic devices to modulate the electrical activityof the nervous system for the treatment of patientswith, for example, IBD and other chronic inflam-matory conditions such as RA. VNS is a safetechnique, as previously shown in epilepsy anddepression, using an intrinsic physiological anti-inflammatory pathway, and is able to restoresympatho-vagal balance. As a nondrug treatment,VNS as monotherapy should avoid the significantside effects of drug treatments used in IBD suchas infections, lymphomas and nonmelanoma skincancers. In addition, invasive VNS has the advan-tage compared with noninvasive VNS of being ableto avoid therapeutic compliance problemsreported with drugs. The development of
noninvasive VNS methods, such as tVNS orgammaCore, is of interest. The use of VNS couldbe extrapolated to other inflammatory disorderssuch as RA, psoriasis and postoperative ileus.However, we believe that more data are requiredand the VNS parameters used to treat inflamma-tory conditions need to be better characterized, inparticular the duration, intensity and frequency ofstimulation.
Conflict of interest statement
None of the authors has any conflicts of interest.No funding was received for this review.
Author contributions
All authors approved the final version of themanuscript. All persons designated as authorsqualify for authorship, and all those who qualifyfor authorship are listed.
References
1 Danese S, Fiocchi C. Etiopathogenesis of inflammatory
bowel diseases. World J Gastroenterol 2006; 12: 4807–12.
2 Bonaz BL, Bernstein CN. Brain-gut interactions in
inflammatory bowel disease. Gastroenterology 2013; 144:
36–49.
3 Lindgren S, Lilja B, Rosen I, Sundkvist G. Disturbed
autonomic nerve function in patients with Crohn’s disease.
Scand J Gastroenterol 1991; 26: 361–6.
4 Pellissier S, Dantzer C, Canini F, Mathieu N, Bonaz B.
Psychological adjustment and autonomic disturbances in
inflammatory bowel diseases and irritable bowel syndrome.
Psychoneuroendocrinology 2010; 35: 653–62.
5 Pellissier S, Dantzer C, Mondillon L et al. Relationship
between vagal tone, cortisol, TNF-alpha, epinephrine and
negative affects in Crohn’s disease and irritable bowel
syndrome. PLoS ONE 2014; 9: e105328.
6 Billiet T, Rutgeerts P, Ferrante M, Van Assche G, Vermeire S.
Targeting TNF-alpha for the treatment of inflammatory
bowel disease. Expert Opin Biol Ther 2014; 14: 75–101.
7 McLean LP, Cross RK. Adverse events in IBD: to stop or
continue immune suppressant and biologic treatment.
Expert Rev Gastroenterol Hepatol 2014; 8: 223–40.
8 Cerveny P, Bortlik M, Vlcek J, Kubena A, Lukas M. Non-
adherence to treatment in inflammatory bowel disease in
Czech Republic. J Crohns Colitis 2007; 1: 77–81.
9 Altschuler SM, Escardo J, Lynn RB, Miselis RR. The central
organization of the vagus nerve innervating the colon of the
rat. Gastroenterology 1993; 104: 502–9.
10 Netter FH. Atlas of Human Anatomy. USA: Ciba-Geigy
Corporation. Ardsley, 1989.
11 Delmas J, Laux G. Anatomie M�edico-Chirurgicale du Syst�eme
Nerveux V�eg�etatif: (sympathique & parasympathique). Paris:
Masson, 1933.
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 59
Journal of Internal Medicine, 2017, 282; 46–63

12 Berthoud HR, Carlson NR, Powley TL. Topography of efferent
vagal innervation of the rat gastrointestinal tract. Am J
Physiol 1991; 260: R200–7.
13 Sharkey KA, Kroese AB. Consequences of intestinal inflam-
mation on the enteric nervous system: neuronal activation
induced by inflammatory mediators. Anat Rec 2001; 262:
79–90.
14 Margolis KG, Stevanovic K, Karamooz N et al. Enteric
neuronal density contributes to the severity of intestinal
inflammation. Gastroenterology, 2011. 141: 588–98, 598
e1-2.
15 Altschuler SM, Bao XM, Bieger D, Hopkins DA, Miselis RR.
Viscerotopic representation of the upper alimentary tract in
the rat: sensory ganglia and nuclei of the solitary and spinal
trigeminal tracts. J Comp Neurol 1989; 283: 248–68.
16 Rinaman L, Card JP, Schwaber JS, Miselis RR. Ultrastruc-
tural demonstration of a gastric monosynaptic vagal circuit
in the nucleus of the solitary tract in rat. J Neurosci 1989; 9:
1985–96.
17 Ricardo JA, Koh ET. Anatomical evidence of direct projec-
tions from the nucleus of the solitary tract to the hypotha-
lamus, amygdala, and other forebrain structures in the rat.
Brain Res 1978; 153: 1–26.
18 Sawchenko PE. Central connections of the sensory and
motor nuclei of the vagus nerve. J Auton Nerv Syst 1983; 9:
13–26.
19 Ruggiero DA, Underwood MD, Mann JJ, Anwar M, Arango V.
The human nucleus of the solitary tract: visceral pathways
revealed with an “in vitro” postmortem tracing method. J
Auton Nerv Syst 2000; 79: 181–90.
20 Van Bockstaele E.J., Peoples J., Telegan P. Efferent projec-
tions of the nucleus of the solitary tract to peri-locus
coeruleus dendrites in rat brain: evidence for a monosynap-
tic pathway. J Comp Neurol, 1999; 412: 410–28.
21 Aston-Jones G, Ennis M, Pieribone VA, Nickell WT, Shipley
MT. The brain nucleus locus coeruleus: restricted afferent
control of a broad efferent network. Science 1986; 234: 734–
7.
22 Zagon A. Does the vagus nerve mediate the sixth sense?
Trends Neurosci 2001; 24: 671–3.
23 Conrad LC, Pfaff DW. Efferents from medial basal forebrain
and hypothalamus in the rat. II. An autoradiographic study
of the anterior hypothalamus. J Comp Neurol 1976; 169:
221–61.
24 Norgren R. Taste pathways to hypothalamus and amygdala.
J Comp Neurol 1976; 166: 17–30.
25 Harris GW. The hypothalamus and endocrine glands. Br Med
Bull 1950; 6: 345–50.
26 Goehler LE, Relton JK, Dripps D et al. Vagal paraganglia
bind biotinylated interleukin-1 receptor antagonist: a possi-
ble mechanism for immune-to-brain communication. Brain
Res Bull 1997; 43: 357–64.
27 Watkins LR, Goehler LE, Relton JK et al. Blockade of
interleukin-1 induced hyperthermia by subdiaphragmatic
vagotomy: evidence for vagal mediation of immune-brain
communication. Neurosci Lett 1995; 183: 27–31.
28 Borovikova LV, Ivanova S, Zhang M et al. Vagus nerve
stimulation attenuates the systemic inflammatory response
to endotoxin. Nature 2000; 405: 458–62.
29 Pavlov VA, Wang H, Czura CJ, Friedman SG, Tracey KJ. The
cholinergic anti-inflammatory pathway: a missing link in
neuroimmunomodulation. Mol Med 2003; 9: 125–34.
30 Wang H, Yu M, Ochani M et al. Nicotinic acetylcholine
receptor alpha7 subunit is an essential regulator of inflam-
mation. Nature 2003; 421: 384–8.
31 de Jonge WJ, van der Zanden EP, The FO et al. Stimulation
of the vagus nerve attenuates macrophage activation by
activating the Jak2-STAT3 signaling pathway. Nat Immunol
2005; 6: 844–51.
32 Sun Y, Li Q, Gui H et al. MicroRNA-124 mediates the
cholinergic anti-inflammatory action through inhibiting the
production of pro-inflammatory cytokines. Cell Res 2013;
23: 1270–83.
33 Cailotto C, Gomez-Pinilla PJ, Costes LM et al. Neuro-
anatomical evidence indicating indirect modulation of
macrophages by vagal efferents in the intestine but not in
the spleen. PLoS ONE 2014; 9: e87785.
34 Mikkelsen HB, Thuneberg L, Rumessen JJ, Thorball N.
Macrophage-like cells in the muscularis externa of mouse
small intestine. Anat Rec 1985; 213: 77–86.
35 Matteoli G, Gomez-Pinilla PJ, Nemethova A et al. A distinct
vagal anti-inflammatory pathway modulates intestinal mus-
cularis resident macrophages independent of the spleen.
Gut, 2014. 63: 938–48.
36 Bellinger DL, Felten SY, Lorton D, Felten DL. Origin of
noradrenergic innervation of the spleen in rats. Brain Behav
Immun 1989; 3: 291–311.
37 Rosas-Ballina M, Ochani M, Parrish WR et al. Splenic nerve
is required for cholinergic antiinflammatory pathway control
of TNF in endotoxemia. Proc Natl Acad Sci U S A 2008; 105:
11008–13.
38 Rosas-Ballina M, Olofsson PS, Ochani M et al. Acetyl-
choline-synthesizing T cells relay neural signals in a vagus
nerve circuit. Science 2011; 334: 98–101.
39 Olofsson PS, Rosas-Ballina M, Levine YA, Tracey KJ.
Rethinking inflammation: neural circuits in the regulation
of immunity. Immunol Rev 2012; 248: 188–204.
40 Bratton BO, Martelli D, McKinley MJ, Trevaks D, Anderson
CR, McAllen RM. Neural regulation of inflammation: no
neural connection from the vagus to splenic sympathetic
neurons. Exp Physiol 2012; 97: 1180–5.
41 Berthoud HR, Powley TL. Characterization of vagal innerva-
tion to the rat celiac, suprarenal and mesenteric ganglia. J
Auton Nerv Syst 1993; 42: 153–69.
42 Berthoud HR, Powley TL. Interaction between parasympa-
thetic and sympathetic nerves in prevertebral ganglia: mor-
phological evidence for vagal efferent innervation of ganglion
cells in the rat. Microsc Res Tech 1996; 35: 80–6.
43 Downs AM, Bond CE, Hoover DB. Localization of alpha7
nicotinic acetylcholine receptor mRNA and protein within
the cholinergic anti-inflammatory pathway. Neuroscience
2014; 266: 178–85.
44 Buijs RM, van der Vliet J, Garidou ML, Huitinga I, Escobar
C. Spleen vagal denervation inhibits the production of
antibodies to circulating antigens. PLoS ONE 2008; 3:
e3152.
45 Gautron L, Rutkowski JM, Burton MD, Wei W, Wan Y,
Elmquist JK. Neuronal and nonneuronal cholinergic struc-
tures in the mouse gastrointestinal tract and spleen. J Comp
Neurol 2013; 521: 3741–67.
46 Munyaka P, Rabbi MF, Pavlov VA, Tracey KJ, Khafipour E,
Ghia JE. Central muscarinic cholinergic activation alters
interaction between splenic dendritic cell and CD4+ CD25�T cells in experimental colitis. PLoS ONE 2014; 9: e109272.
Vagus nerve stimulation in IBD / B. Bonaz et al.
60 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2017, 282; 46–63

47 Martelli D, McKinley MJ, McAllen RM. The cholinergic anti-
inflammatory pathway: a critical review. Auton Neurosci
2014; 182: 65–9.
48 Ji H, Rabbi MF, Labis B, Pavlov VA, Tracey KJ, Ghia JE.
Central cholinergic activation of a vagus nerve-to-spleen
circuit alleviates experimental colitis. Mucosal Immunol
2014; 7: 335–47.
49 Xue N, Liang H, Yao H, Song XM, Li JG. The role of spleen in
vagus nerve stimulation for treatment against septic shock
in rats. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2011; 23:
263–6.
50 Inoue T, Abe C, Sung SS et al. Vagus nerve stimulation
mediates protection from kidney ischemia-reperfusion
injury through alpha7nAChR+ splenocytes. J Clin Invest
2016; 126: 1939–52.
51 Picq CA, Clarencon D, Sinniger VE, Bonaz BL, Mayol JF.
Impact of anesthetics on immune functions in a rat model of
vagus nerve stimulation. PLoS ONE 2013; 8: e67086.
52 Wessler I, Kirkpatrick CJ, Racke K. Non-neuronal acetyl-
choline, a locally acting molecule, widely distributed in
biological systems: expression and function in humans.
Pharmacol Ther 1998; 77: 59–79.
53 Martelli D, Farmer DG, Yao ST. The splanchnic anti-
inflammatory pathway: could it be the efferent arm of
the inflammatory reflex? Exp Physiol 2016; 101: 1245–1252.
54 MacNeil BJ, Jansen AH, Janz LJ, Greenberg AH, Nance DM.
Peripheral endotoxin increases splenic sympathetic nerve
activity via central prostaglandin synthesis. Am J Physiol
1997; 273: R609–14.
55 Martelli D, Yao ST, Mancera J, McKinley MJ, McAllen RM.
Reflex control of inflammation by the splanchnic anti-
inflammatory pathway is sustained and independent of
anesthesia. Am J Physiol Regul Integr Comp Physiol 2014;
307: R1085–91.
56 Strack AM, Sawyer WB, Platt KB, Loewy AD. CNS cell groups
regulating the sympathetic outflow to adrenal gland as
revealed by transneuronal cell body labeling with pseudora-
bies virus. Brain Res 1989; 491: 274–96.
57 Strack AM, Sawyer WB, Hughes JH, Platt KB, Loewy AD. A
general pattern of CNS innervation of the sympathetic
outflow demonstrated by transneuronal pseudorabies viral
infections. Brain Res 1989; 491: 156–62.
58 Ghia JE, Blennerhassett P, Kumar-Ondiveeran H, Verdu EF,
Collins SM. The vagus nerve: a tonic inhibitory influence
associated with inflammatory bowel disease in a murine
model. Gastroenterology 2006; 131: 1122–30.
59 Bai A, Guo Y, Lu N. The effect of the cholinergic anti-
inflammatory pathway on experimental colitis. Scand J
Immunol 2007; 66: 538–45.
60 Miceli PC, Jacobson K. Cholinergic pathways modulate
experimental dinitrobenzene sulfonic acid colitis in rats.
Auton Neurosci 2003; 105: 16–24.
61 Overstreet DH. The Flinders sensitive line rats: a genetic
animal model of depression. Neurosci Biobehav Rev 1993;
17: 51–68.
62 Overstreet DH, Russell RW, Crocker AD, Gillin JC,
Janowsky DS. Genetic and pharmacological models of
cholinergic supersensitivity and affective disorders. Experi-
entia 1988; 44: 465–72.
63 Ghia JE, Blennerhassett P, Collins SM. Vagus nerve integrity
and experimental colitis. Am J Physiol Gastrointest Liver
Physiol 2007; 293: G560–7.
64 Task Force of the European Society of Cardiology the North
American Society of Pacing. Heart rate variability: standards
of measurement, physiological interpretation, and clinical
use. Circulation, 1996; 93: 1043–65.
65 Cygankiewicz I, Zareba W. Heart rate variability. Handb Clin
Neurol 2013; 117: 379–93.
66 Lanska DJ. J.L. Corning and vagal nerve stimulation for
seizures in the 1880s. Neurology 2002; 58: 452–9.
67 Bailey P, Bremer F. A sensory cortical representation of the
vagus nerve: with a note on the effects of low blood
pressure on the cortical electrogram. J Neurophysiol 1938;
1: 405–12.
68 Penry JK, Dean JC. Prevention of intractable partial seizures
by intermittent vagal stimulation in humans: preliminary
results. Epilepsia 1990; 31(Suppl 2): S40–3.
69 Rush AJ, Marangell LB, Sackeim HA et al. Vagus nerve
stimulation for treatment-resistant depression: a random-
ized, controlled acute phase trial. Biol Psychiatry 2005; 58:
347–54.
70 Rush AJ, Sackeim HA, Marangell LB et al. Effects of
12 months of vagus nerve stimulation in treatment-resistant
depression: a naturalistic study. Biol Psychiatry 2005; 58:
355–63.
71 Fanselow EE. Central mechanisms of cranial nerve stimula-
tion for epilepsy. Surg Neurol Int 2012; 3(Suppl 4): S247–54.
72 Krahl SE, Senanayake SS, Handforth A. Destruction of
peripheral C-fibers does not alter subsequent vagus nerve
stimulation-induced seizure suppression in rats. Epilepsia
2001; 42: 586–9.
73 Zanchetti A, Wang SC, Moruzzi G. Effect of afferent vagal
stimulation on the electroencephalogram of the cat in
cerebral isolation. Boll Soc Ital Biol Sper 1952; 28: 627–8.
74 Panebianco M, Rigby A, Weston J, Marson AG. Vagus nerve
stimulation for partial seizures. Cochrane Database Syst Rev
2015; 3: CD002896.
75 Groves DA, Brown VJ. Vagal nerve stimulation: a review of
its applications and potential mechanisms that mediate
its clinical effects. Neurosci Biobehav Rev 2005; 29: 493–
500.
76 Naritoku DK, Terry WJ, Helfert RH. Regional induction of fos
immunoreactivity in the brain by anticonvulsant stimulation
of the vagus nerve. Epilepsy Res 1995; 22: 53–62.
77 Chae JH, Nahas Z, Lomarev M et al. A review of functional
neuroimaging studies of vagus nerve stimulation (VNS). J
Psychiatr Res 2003; 37: 443–55.
78 Morris GL III, Mueller WM. Long-term treatment with vagus
nerve stimulation in patients with refractory epilepsy. The
Vagus Nerve Stimulation Study Group E01-E05. Neurology
1999; 53: 1731–5.
79 Reid SA. Surgical technique for implantation of the neuro-
cybernetic prosthesis. Epilepsia 1990; 31(Suppl 2): S38–9.
80 Hamlin RL, Smith CR. Effects of vagal stimulation on S-A
and A-V nodes. Am J Physiol 1968; 215: 560–8.
81 Ben-Menachem E. Vagus nerve stimulation, side effects, and
long-term safety. J Clin Neurophysiol 2001; 18: 415–8.
82 Bernik TR, Friedman SG, Ochani M et al. Pharmacological
stimulation of the cholinergic antiinflammatory pathway. J
Exp Med 2002; 195: 781–8.
83 Costantini TW, Bansal V, Krzyzaniak M et al. Vagal nerve
stimulation protects against burn-induced intestinal injury
through activation of enteric glia cells. Am J Physiol Gas-
trointest Liver Physiol 2010; 299: G1308–18.
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 61
Journal of Internal Medicine, 2017, 282; 46–63

84 Morishita K, Coimbra R, Langness S, Eliceiri BP, Costantini
TW. Neuroenteric axis modulates the balance of regulatory T
cells and T-helper 17 cells in the mesenteric lymph node
following trauma/hemorrhagic shock. Am J Physiol Gas-
trointest Liver Physiol 2015; 309: G202–8.
85 O’Mahony C, van der Kleij H, Bienenstock J, Shanahan F,
O’Mahony L. Loss of vagal anti-inflammatory effect: in vivo
visualization and adoptive transfer. Am J Physiol Regul
Integr Comp Physiol 2009; 297: R1118–26.
86 LomarevM,DenslowS,NahasZ,ChaeJH,GeorgeMS,Bohning
DE. Vagus nerve stimulation (VNS) synchronized BOLD fMRI
suggests that VNS in depressed adults has frequency/dose
dependent effects. J Psychiatr Res 2002; 36: 219–27.
87 Reyt S, Picq C, Sinniger V, Clarencon D, Bonaz B, David O.
Dynamic Causal Modelling and physiological confounds: a
functional MRI study of vagus nerve stimulation. NeuroI-
mage 2010; 52: 1456–64.
88 Meregnani J, Clarencon D, Vivier M et al. Anti-inflammatory
effect of vagus nerve stimulation in a rat model of inflam-
matory bowel disease. Auton Neurosci 2011; 160: 82–9.
89 Bernik TR, Friedman SG, Ochani M et al. Cholinergic
antiinflammatory pathway inhibition of tumor necrosis
factor during ischemia reperfusion. J Vasc Surg 2002; 36:
1231–6.
90 Sun P, Zhou K, Wang S et al. Involvement of MAPK/NF-
kappaB signaling in the activation of the cholinergic anti-
inflammatory pathway in experimental colitis by chronic
vagus nerve stimulation. PLoS ONE 2013; 8: e69424.
91 Bonaz B, Sinniger V, Hoffmann D et al. Chronic vagus nerve
stimulation in Crohn’s disease: a 6-month follow-up pilot
study. Neurogastroenterol Motil 2016; 28: 948–53.
92 Clarencon D, Pellissier S, Sinniger V et al. Long term effects
of low frequency (10 Hz) vagus nerve stimulation on EEG and
heart rate variability in Crohn’s disease: a case report. Brain
Stimul 2014; 7: 914–6.
93 Koopman FA, Schuurman PR, Vervoordeldonk MJ, Tak PP.
Vagus nerve stimulation: a new bioelectronics approach to
treat rheumatoid arthritis? Best Pract Res Clin Rheumatol
2014; 28: 625–35.
94 Koopman FA, Chavan SS, Miljko S et al. Vagus nerve
stimulation inhibits cytokine production and attenuates
disease severity in rheumatoid arthritis. Proc Natl Acad Sci
U S A 2016; 113: 8284–9.
95 Koopman FA, Tang MW, Vermeij J et al. Autonomic dys-
function precedes development of rheumatoid arthritis: a
prospective cohort study. EBioMedicine 2016; 6: 231–7.
96 The FO, Boeckxstaens GE, Snoek SA et al. Activation of
the cholinergic anti-inflammatory pathway ameliorates
postoperative ileus in mice. Gastroenterology 2007; 133:
1219–28.
97 Peuker ET, Filler TJ. The nerve supply of the human auricle.
Clin Anat 2002; 15: 35–7.
98 Frangos E, Ellrich J, Komisaruk BR. Non-invasive access to
the vagus nerve central projections via electrical stimulation
of the external ear: fMRI evidence in humans. Brain Stimul
2015; 8: 624–36.
99 Zhao YX, He W, Jing XH et al. Transcutaneous auricular
vagus nerve stimulation protects endotoxemic rat from
lipopolysaccharide-induced inflammation. Evid Based Com-
plement Alternat Med 2012; 2012: 627023.
100 Stefan H, Kreiselmeyer G, Kerling F et al. Transcutaneous
vagus nerve stimulation (t-VNS) in pharmacoresistant
epilepsies: a proof of concept trial. Epilepsia 2012; 53:
e115–8.
101 Lerman I, Hauger R, Sorkin L et al. Noninvasive transcuta-
neous vagus nerve stimulation decreases whole blood cul-
ture-derived cytokines and chemokines: a randomized,
blinded. Healthy Control Pilot Trial. Neuromodulation
2016; 19: 283–90.
102 Oke SL, Tracey KJ. The inflammatory reflex and the role of
complementary and alternative medical therapies. Ann N Y
Acad Sci 2009; 1172: 172–80.
103 Lim HD, Kim MH, Lee CY, Namgung U. Anti-inflammatory
effects of acupuncture stimulation via the vagus nerve. PLoS
ONE 2016; 11: e0151882.
104 Aubert AE, Verheyden B, Beckers F, Tack J, Vandenberghe
J. Cardiac autonomic regulation under hypnosis assessed
by heart rate variability: spectral analysis and fractal
complexity. Neuropsychobiology 2009; 60: 104–12.
105 Keefer L, Taft TH, Kiebles JL, Martinovich Z, Barrett TA,
Palsson OS. Gut-directed hypnotherapy significantly aug-
ments clinical remission in quiescent ulcerative colitis.
Aliment Pharmacol Ther 2013; 38: 761–71.
106 Tyagi A, Cohen M. Yoga and heart rate variability: A
comprehensive review of the literature. Int J Yoga 2016; 9:
97–113.
107 Tyagi A, Cohen M, Reece J, Telles S, Jones L, Heart rate
variability, flow, mood and mental stress during yoga
practices in yoga practitioners, non-yoga practitioners and
people with metabolic syndrome. Appl Psychophysiol
Biofeedback 2016; 41: 381–393.
108 Azam MA, Katz J, Fashler SR, Changoor T, Azargive S, Ritvo
P. Heart rate variability is enhanced in controls but not
maladaptive perfectionists during brief mindfulness medi-
tation following stress-induction: a stratified-randomized
trial. Int J Psychophysiol 2015; 98: 27–34.
109 Luyer MD, Greve JW, Hadfoune M, Jacobs JA, Dejong CH,
Buurman WA. Nutritional stimulation of cholecystokinin
receptors inhibits inflammation via the vagus nerve. J Exp
Med 2005; 202: 1023–9.
110 de Haan JJ, Lubbers T, Hadfoune M et al. Postshock inter-
vention with high-lipid enteral nutrition reduces inflamma-
tion and tissue damage. Ann Surg 2008; 248: 842–8.
111 de Haan JJ, Hadfoune M, Lubbers T et al. Lipid-rich enteral
nutrition regulates mucosal mast cell activation via the
vagal anti-inflammatory reflex. Am J Physiol Gastrointest
Liver Physiol 2013; 305: G383–91.
112 Bonaz B, Sinniger V, Pellissier S. Anti-inflammatory prop-
erties of the vagus nerve: potential therapeutic implications
of vagus nerve stimulation. J Physiol 2016; 594: 5781–90.
113 Bonaz B, Sinniger V, Pellissier S. Vagal tone: effects on
sensitivity, motility, and inflammation. Neurogastroenterol
Motil 2016; 28: 455–62.
114 Wang DW, Yin YM, Yao YM. Vagal modulation of the
inflammatory response in sepsis. Int Rev Immunol 2016;
35: 415–33.
115 Annoni EM, Xie X, Lee SW et al. Intermittent electrical stimu-
lation of the right cervical vagus nerve in salt-sensitive hyper-
tensive rats: effects on blood pressure, arrhythmias, and
ventricular electrophysiology. Physiol Rep 2015; 3: e12476.
116 Rozman J, Peclin P, Knezevic I, Mirkovic T, Gersak B,
Podbregar M. Heart function influenced by selective mid-
cervical left vagus nerve stimulation in a human case study.
Hypertens Res 2009; 32: 1041–3.
Vagus nerve stimulation in IBD / B. Bonaz et al.
62 ª 2017 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2017, 282; 46–63

117 Wolthuis AM, Stakenborg N, D’Hoore A, Boeckxstaens GE.
The pig as preclinical model for laparoscopic vagus nerve
stimulation. Int J Colorectal Dis 2016; 31: 211–5.
118 Das UN. Current and emerging strategies for the treatment
and management of systemic lupus erythematosus based on
molecular signatures of acute and chronic inflammation. J
Inflamm Res 2010; 3: 143–70.
Correspondence: Bruno Bonaz, Clinique Universitaire d’H�epato-
Gastroent�erologie, CHU Grenoble, CS-10217, 38043 Grenoble
Cedex 09, France.
(fax: +33476765297; e-mail: [email protected])
Vagus nerve stimulation in IBD / B. Bonaz et al.
ª 2017 The Association for the Publication of the Journal of Internal Medicine 63
Journal of Internal Medicine, 2017, 282; 46–63