-
merzomFCLPar
Departamento de Biologia Celular e Molecular e Bioagentes
Patognicos, Faculdade de Medicina-FMRP, Universidade de So Paulo,
14049-900 Ribeiro Preto-SP, Brazil
a r t i c l e i n f o
and metronidazole suffer from one major drawback: the difcultyto
maintain therapeutic concentrations of the agent in the peri-
wavelength and are able to produce several reactive oxygen
spe-cies (ROS) that activate biologic systems [913]. In particular,
alarge number of micro-organisms (including oral species) havebeen
reported to be killed by PDT [14,15] and virulence
factors(lipopolysaccharides and proteases) have also been shown to
bereduced by photosensitization. Because it is easy to access the
peri-odontal pocket, periodontitis would be very amenable to
treatmentby PDT [1518]. Hence, the photosensitizer can be placed
directlyinto the pocket which can then be irradiated either through
thethin gingival tissues or via an optical ber placed directly
into
Corresponding author at: Universit Paris Descartes, Hpital
Europen GeorgesPompidou, 56 rue Leblanc, 75737 Paris Cedex 15,
France. Tel.: +33 (0) 1 53 98 80 76;fax: +33 (0) 1 53 98 79 58.
E-mail addresses: [email protected] (S. Sguier),
[email protected] (S.L.S. Souza), [email protected] (A.C.V.
Sverzut), [email protected] (A.R. Simioni), [email protected]
(F.L. Primo), [email protected] (A.
Bodineau), [email protected] (V.M.A. Corra),
Journal of Photochemistry and Photobiology B: Biology 101 (2010)
348354
Contents lists availab
Journal of Photochemistry an
journal homepage: [email protected] (B.
Coulomb), [email protected] (A.C. Tedesco).to a specic decrease of
antigen-presenting cells populations according to the drug delivery
system used. 2010 Elsevier B.V. All rights reserved.
1. Introduction
It is well known that inammatory periodontal diseases are
ini-tiated and maintained by the bacterial plaque and its
metabolicproducts which trigger the local inltration of inammatory
cellsassociated with the degradation of extracellular matrix
molecules[1,2]. Neither mechanical plaque removal nor ushing or
rinsingwith disinfectants allows the total eradication of bacterial
reser-voirs within periodontal pockets. Current therapeutic
strategiesfor periodontitis that use antimicrobial agents such as
tetracyclines
odontal pocket for a sufcient length of time to ensure
eradicationof the bacteria present [3,4].
To supplement the armament of antibacterial measures and
de-crease the inammatory process, in recent years different
attemptswere made to introduce photodynamic therapy (PDT) as a
newtreatment of chronic periodontitis [38]. PDT is based on the
injec-tion, ingestion, or topical application of photosensitizers
dyes (usu-ally using drug delivery systems (DDS) such as liposomes
ornanoemulsions) followed by visible light activation. These
photo-sensitizers are chemical compounds that absorb light at a
specicArticle history:Received 23 March 2010Received in revised
form 6 August 2010Accepted 10 August 2010Available online 17 August
2010
Keywords:PDTPeriodontal diseaseAntigen-presenting cellDendritic
cellPhthalocyanine1011-1344/$ - see front matter 2010 Elsevier B.V.
Adoi:10.1016/j.jphotobiol.2010.08.007a b s t r a c t
The aim of this study was to evaluate the effects of the
photodynamic therapy (PDT) on the inammatoryinltrate and on the
collagen network organization in human advanced chronic
periodontitis. Two differ-ent drug delivery systems (DDS) were
tested (liposomes and nanoemulsions) to determine if the effects
ofPDT could differ according to the DDS used.Sixteen patients
presenting two teeth with chronic advanced periodontitis and
important tooth
mobility with clinical indication of extraction were included in
the group liposomes (group L, n = 8) orin the group nanoemulsions
(group N, n = 8) in order to compare the effects of each DDS. Seven
daysbefore extractions one tooth of each patient was treated with
PDT using phthalocyanine derivatives asphotosensitizers and the
contralateral tooth was taken as control. In group L the density of
gingivalcollagen bers (66 19%) was signicantly increased (p <
0.02) when compared to controls (35 21%).Concerning the
antigen-presenting cells, PDT had differential effects depending on
the drug deliverysystem; the number of macrophages was signicantly
decreased (p < 0.05) in group L while the numberof Langerhans
cells was signicantly decreased in group N (p < 0.02). These
ndings demonstrate thatPDT presents an impact on gingival
inammatory phenomenon during chronic periodontitis and leadsService
dOdontologie, Hpital Louis Mourier, rue des Renouillers, 92700
Colombes, FrancedDepartamento de Cirurgia, Traumatologia
Buco-Maxilo-Facial e Periodontia, Faculdade de Odontologia-FORP,
Universidade de So Paulo, 14040-904 Ribeiro Preto-SP, BrazileImpact
of photodynamic therapy on inachronic periodontitis
Sylvie Sguier a,b,c,, Sergio L.S. Souza d, Anna C.V. SvAgns
Bodineau b,c, Vani M.A. Corra e, Bernard CoulaDepartamento de
Qumica, Faculdade de Filosoa, Cincias e Letras de Ribeiro
Preto-FbUniversit Paris Descartes, Hpital Europen Georges Pompidou,
56 rue Leblanc, 75737cll rights reserved.matory cells during
human
ut d, Andreza R. Simioni a, Fernando L. Primo a,b b, Antonio C.
Tedesco a
RP, Universidade de So Paulo, 14040-901 Ribeiro Preto-SP,
Brazilis Cedex 15, France
le at ScienceDirect
d Photobiology B: Biology
vier .com/locate / jphotobiol
-
anaesthetic inltration into the biopsy site, and deformation
or
nd Pcompression of the samples. Gingival samples of control and
trea-ted teeth were obtained from the inner part of the ap (that
was incontact with the root) in the buccal marginal gingiva.
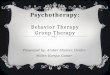
2.3. Photodynamic therapy (PDT) and laser treatment (Fig. 1)
The PDT was performed using phthalocyanine derivatives
asphotosensitizers (NzPC and AlClPC) and two different drug
deliverysystems were used: liposomes (n = 8, group L) and
nanoemulsions(n = 8, group N). The photosensitizer was applied on
each surface ofthe tooth by placing the applicator at the bottom of
the periodontalpocket and was continuously deposited in a coronal
direction. Thisapplication was done three times with 5 min of
waiting betweenthe pocket avoiding damage to adjacent host tissues
[19] and dis-ruption of the normal microora [20]. However, there is
a lack ofin vivo studies evaluating the effect of PDT on the
gingival inam-matory cells and on the matrix macromolecules as
collagen bersduring human periodontal diseases.
The aim of this study was to evaluate the potential efciency
ofPDT on a limited number of patients presenting advanced
chronichuman periodontitis. Two drug delivery systems (DDS) were
tested(liposomes and nanoemulsions) in case of each DDS interacts
dif-ferently with a tissular target. The effect of PDT on the
inamma-tory cells, on the density of the collagen network and on
theexpression of metalloproteinases was evaluated from
gingivalbiopsies a week after the treatment.
2. Materials and methods
2.1. Patient population
The experimental protocol was reviewed and approved by
theInstitutions Human Research Committee and the protocol was
ap-proved on June 21, 2007 (protocol 2007.1.487.58.7, Ribeiro
Preto,So Paulo University, Brazil) and the experiments were
undertakenwith the understanding and written consent of each
subject. Six-teen patients (6 females, 10 males, aged 5065)
presenting twoteeth with a clinical diagnosis of advanced chronic
periodontitis,ultimate degree of tooth mobility (mobility IV,
horizontal and axialmobilities) and periodontal indication for
extraction were selected.For each selected patient, both teeth
presented the same degree ofgingival inammation and the equivalent
tooth mobility. Diagnosisof chronic periodontitis was established
on the basis of clinical andradiographic criteria (bone resorption)
according to the classica-tion system for periodontal diseases and
conditions [21]. The pa-tients included in this study had neither
other oral or systemicdiseases, nor any overt immunological
abnormalities and did nottake any preoperatory medication.
2.2. Study design
The study was performed using the split-mouth design. A totalof
16 pairs of contralateral maxillary or mandibulary teeth were
in-cluded. In each contralateral pair, one tooth was assigned as
con-trol whereas the other tooth was treated with
photodynamictherapy (PDT). No subgingival mechanical therapy
(scaling androot planing) was performed prior to PDT. All patients
were treatedby the same operator and the extractions of both teeth
(control andtreated) were performed 7 days after treatment by PDT.
Gingivaltissue samples, which otherwise would have been discarded,
wereobtained during surgery under local anaesthesia, avoiding
local
S. Sguier et al. / Journal of Photochemistry aeach application
and laser exposure was done 15 min after the lastapplication of the
photosensitizer. The laser used in this study wasan Eagle Diode
Laser (Quantum Technology, Brazil) with a wave-length of 670 nm, a
uence rate of 0.5 W/cm2 delivered during40 s (10 s for each face of
the tooth) and a total uence of 12.7 J/cm2.
2.4. Preparation of photosensitizers
Liposomes have been used as drug delivery systems since the1960s
[22]. NzPC is a silicon (IV) phthalocyanine derivative
(metalphthalocyanine) with two axial ligands substituted in the
macrocy-cle, belong to the second generation of photoactive agents
used inPDT. The incorporation of NzPC into the phospholipids
bilayer of L-a-phosphatidylcholine and
dimethyl-dioctadecylammoniumbro-mide (DDAB) was carried out
according to the modied injectionmethod described by Pelegrino et
al. [23]. Basically, 360 lL of anethanolic solution, which was 68.6
mmol/L phosphatidylcholine,0.19 mmol/L DDAB and 50 lL in NzPC, was
injected with a syringeinto 5 mL PBS, pH 7.4. The injection was
performed at 56 C, undermagnetic stirring and at ow rate 1
lL/s.
Nanoemulsion was obtained by spontaneous emulsicationprocess as
described by Primo et al. [24]. The natural soy phospho-lipids
Epikuron 170 (7.5%) and Miglyol 812 N oil (250 lL) were ob-tained
from Hulls Inc. (Puteaux, France) and initially dissolved in10 mL
of spectroscopic acetone at 55 C under magnetic stirrer.In the same
time the biopolymer Poloxamer 188 (SigmaAldrichCo., St. Louis, MO,
USA) at 7.5% was dissolved in ultra-pure waterto obtain an aqueous
phase. In the sequence the organic phasewas added slowly in aqueous
medium in the emulsication stepfor 20 min. After total
homogenization, the acetone was removedby reduced pressure at
approximately 6070 C for a nal volumeof 10 mL of nanoemulsion.
Chloroaluminum phthalocyanine (Sig-maAldrich Co., St. Louis, MO,
USA) was dissolved directly in Mi-glyol 812 N oil at 55 C for nal
concentration of 0.05 mg/mL innanoemulsion. Its incorporation in
the nanoemulsion was accom-plished on organic phase in emulsication
process as previouslydescribed [24]. The photophysical,
photochemical and photobio-logical properties and biological
responses of the phthalocyaninederivates were similar as revealed
in previous study from ourgroup and allow the comparison between
them [912].
2.5. Tissue preparation
Seven days after the treatment by PDT, for each patient,
thecontrol and treated teeth were removed and their marginal
sur-rounding periodontal tissues were immediately divided into
threeparts. The rst part was xed in 4% phosphate buffered
formalin,pH 7.4 and processed by routine laboratory techniques for
parafnembedding. The second part was immediately oriented in
meltingisopentane (Tissue-Tek OCT Compound, Sakura,
Zoeterwoude,Netherlands) so that the sulcular/gingival epithelium
and theunderlying connective tissue would be present in the same
section,and snap-frozen in liquid nitrogen. These two parts were
used forhistological and immunohistochemistry studies. The third
part wasmaintained during 48 h in Hanks medium at 37 C under an
atmo-sphere of 95% air, 5% CO2 and biochemical studies were
performedwith conditioned media from these organ cultures kept at
80 Cuntil the day of the study.
2.6. Histology and Immunohistochemistry
Serial sections (6 lm thick) were obtained from all
specimens.Frozen sections were air-dried at room temperature for 2
h, thenxed in acetone for 10 min and kept at 80 C until the day
ofthe study. For all specimens staining of collagen bers was
per-
hotobiology B: Biology 101 (2010) 348354 349formed with sirius
red F3Ba according to Junqueiras technique(35). For
immunohistochemistry, a panel of monoclonal antibodieswas used:
anti-CD45 (Leukocyte common antigen, dilution 1:100,
-
en Yvelines, France) contained 1 mg/mL of gelatin [25]
dispersed
icTec
nd Pin buffered solution consisting of 2.5 mL gel 1.5 M TrisHCl
pH8.8; 100 lL of sodium dodecyl sulfate (SDS) 10%, 4 mL
polyacryl-amide and 4 mL of distilled water pH 8.8 stacking gel
contained4% polyacrylamide in 0.125 M Tris, pH 6.8. Gels were
polymerizedby adding 50 lL of 10% ammonium persulfate and 10 lL of
0.1%TEMED. Samples (5 lL of conditioned medium) were half dilutedin
1 mol/L Tris pH 6.8 containing 50% glycerol and 0.4% bromophe-Dako,
Glostrup, Denmark), anti-CD8 (Suppressor/cytotoxic T lym-phocytes,
dilution 1:200, Dako), anti-CD4 (helper T lymphocytes,dilution
1:100, Dako), anti-CD68 (monocytes/macrophages, dilu-tion 1:200,
Dako), anti-CD1a (Langerhans cells, dilution 1:100,Dako) using an
avidinbiotinimmunoperoxidase technique aspreviously described in
the literature [2].
2.7. Zymography
Electrophoreses were carried out using a mini protean II
system(Biorad, Marnes la coquette, France). Ten per cent
polyacrylamidegels (10 cm height, 1.5 mm thickness) (Millipore,
Saint Quentin
Fig. 1. Schematic representation showing the technical procedure
of photodynamperiodontal pocket. (B) Application of the laser using
an Eagle Diode Laser (Quantumduring 40 s (10 s for each face of the
tooth) and a total uence of 12.7 J/cm2.350 S. Sguier et al. /
Journal of Photochemistry anol blue, and gels were run under
Laemmli conditions (40 mA, 1 h).Following electrophoresis, gels
were washed twice in 200 mL of2.5% Triton X-100 in distilled water
under constant mechanicalstirring, and incubated in 100 mM TrisHCl,
5 mM CaCl2, 0.005%Brij-35, 0.001% NaN3 pH 8.0 for 648 h at 37 C.
Gels were stainedwith 0.25% Coomassie brilliant blue G-250 (50%
methanol, 10%acetic acid) and destained appropriately (40%
methanol, 10% aceticacid). Proteinase activity was evident as clear
(unstained) zones. Fi-nally the gels were incubated for one hour in
5% methanol, 7.5%acetic acid and kept under cellophane as
previously described [2].
2.8. Quantitative determination of area fraction of collagen
bers,number of immunolabelled cell populations and zymogram lysis
bandsby computer-assisted image analysis
The evaluation of the area fraction (AA%) of collagen bers
wasdetermined in the whole of connective tissue visualized on the
sec-tion stained with sirius red. Histological sections were
observedunder a microscope (Zeiss Model Axioskop, Germany) using
a10 objective equipped with a video camera (Diagnostic,
USA).Captured images were transferred to a microcomputer in which
asoftware (Samba, Tribvn, France) calculated the area fraction(AA%)
occupied by the collagen bers.The number of immunolabelled cells
per unit area (number ofcells/mm2) was determined using the same
computer-assisted im-age analysis and the immunolabelled cells were
counted using 10or 20 objectives either in the gingival epithelium
or in the con-nective tissue, according to the cell density. As a
matter of fact, aprevious study [26] has shown that, as in the
connective tissue,the number of inammatory cells in the gingival
epithelium couldreect the severity of the inammatory phenomenon.
The CD45+cells, CD4+ cells, CD8+ cells and CD1a+ cells were
quantied inthe epithelium, the CD68+ cells were quantied in the
connectivetissue. For all the gingival samples ve elds per tissue
section,randomly selected, were analyzed. Thus, the number of
immunola-belled cell subsets for each sample represents the mean of
the vecountings.
The surface area and the color intensity of zymogram lysisbands
were analyzed using Image J software (Image J;
http:/rsb.in-fo.nih.gov/ij/index.html).
2.9. Statistical analysis
therapy. (A) Application of the photosensitizer by placing the
applicator in thehnology, Brazil) with a wavelength of 670 nm, a
uence rate of 0.5 W/cm2 delivered
hotobiology B: Biology 101 (2010) 348354The means of area
fractions occupied by collagen bundles(AA%), cell numbers and
amounts of matrix metalloproteinases(MMPs) between the control and
treated teeth were comparedusing the one-tailed Student t-test
(paired series). The criterionfor statistical signicance was dened
as a level of p < 0.05. The re-sults are given as mean and
standard deviation (mean SD) to de-scribe the dispersion of the
data.
3. Results
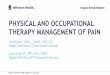
3.1. Area fraction (AA%) of collagen bers
In patients (n = 8) treated by PDT using liposomes (group L)
asdrug delivery system, the area fraction (AA%) of collagen bers(66
19%) was signicantly increased (p < 0.02) in gingival sam-ples
when compared with controls (35 21%) (Fig. 2).
In patients (n = 8) treated by PDT using nanoemulsions (groupN),
the area fraction of collagen bers (56 23%) was not signi-cantly
different when compared with group C (44 23%).
3.2. Inammatory cell populations
For CD45+ cells, CD8+ cells and CD4+ cells, no signicant
differ-ences were observed between controls and treated teeth
with
-
reatb
ea fr
rol a
nd PFig. 2. Histological staining of collagen bers with sirius
red F3Ba in control and t(group L). (A) Control gingival section of
a patient of group L showing stained collagen(B) Treated gingival
section of a patient of group L showing an increased of the
artherapy. E, epithelium; CT, connective tissue; Original
magnication 10.
Table 1Mean number (SD) of inammatory cell populations (number
of cells/mm2) in contnanoemulsions (group N).S. Sguier et al. /
Journal of Photochemistry aeither liposomes or nanoemulsions (Table
1). In both controlgroups (for groups L and N) the numbers of cell
populations werein accordance with those reported previously in
gingival sampleswith chronic periodontitis [27].
In patients treated by PDT using liposomes (group L), the
num-ber of CD68+ macrophages was signicantly decreased (p <
0.05) ingingival connective tissue (300 cells/mm2 187) when
comparedwith controls (585 cells/mm2 321) (Table 1 and Fig. 3).
In patients treated by PDT using nanoemulsions (group N),
thenumber of CD1a+ Langerhans cells was signicantly (p < 0.02)
de-creased in gingival epithelium (81 cells/mm2 39) when
comparedwith controls (150 cells/mm2 56) (Fig. 4).
3.3. Zymography
Whatever the drug delivery system (groups L and N), both proand
active forms of MMP-2 and MMP-9 were present in controland in
gingival samples treated by PDT. Nevertheless, after quanti-tative
analysis of zymogram lysis bands by computer-assisted im-age
analysis, no differences could be detected between control
andtreated gingival samples, either in group L or N (Fig. 5).
4. Discussion
In the present study, the application of photodynamic
therapy(PDT) was tested on diseased gingival tissues of a limited
number
CD45+ CD1a+(cells/mm2) (cells/mm2)
Group LControls 319 225 138 85Treatment 218 124 115 71P-value NS
NS
Group NControls 178 47 150 56Treatment 161 115 81 39P-value NS S
(p = 0.019)
The CD45+ cells, CD4+ cells, CD8+ cells and CD1a+ cells were
quantied in the epithelium(one-tailed Student t-test for paired
series) between control and treated gingival samplNS = not
signicant, S = signicative difference (p < 0.05).ed gingival
samples of patients treated by photodynamic therapy using
liposomesers (arrow) strongly destroyed and degraded during the
inammatory phenomenon.action of the collagen bers (arrow) a week
after the treatment by photodynamic
nd treated gingival samples by PDT in the group liposomes (group
L) and the group
hotobiology B: Biology 101 (2010) 348354 351of patients with
severe periodontitis using two drug delivery sys-tems (DDS,
liposomes and nanoemulsions) and gingival biopsieswere collected 1
week after the clinical treatment by PDT.
The phthalocyanine dyes used belong to a second generation
ofdyes with important production of reactive oxygen species,
mainlysinglet oxygen [28,29]. The main advance in the use of
phthalocy-anine as photosensitizer is the fact that this family of
dyes couldact by the two classical PDT mechanisms of radical
production(type I) or singlet oxygen (type II) according to Foote
[30]. Theassociation with the specic DDS allows a good
biodistribution ofphthalocyanine dyes and an excellent
stability.
Many studies [3,31] have shown that periodontopathogenicbacteria
are susceptible to lethal photosensitization and PDT hasbeen
reported in the literature to be effective in eradicating
variousmicro-organisms using different photosensitizers, different
wave-lengths of light, and different light sources [32]. Recent
clinicaland microbiological studies using PDT for periodontitis
were per-formed to evaluate the effectiveness of PDT as a primary
mode oftreatment or as an adjunct to non-surgical treatment of
scalingand root planning (SRP) compared to a conventional
non-surgicalSRP treatment. For some authors [33,34] the adjuvant
applicationof PDT seems appropriate to reduce inammatory symptoms
andto successfully treat infection with Fusobacterium nucleatum;
forother [35] PDT as an independent treatment or as an adjunct
toSRP was not superior (changes in clinical attachment level,
probingdepth, gingival recession, full-mouth plaque or bleeding
scores) tocontrol treatment of SRP. However, there is a lack of
histological
CD68+ CD8+ CD4+(cells/mm2) (cells/mm2) (cells/mm2)
585 121 122 76 157 111300 127 107 83 131 66S (p = 0.042) NS
NS
351 113 96 29 230 104305 105 102 96 161 78NS NS NS
, the CD68+ cells were quantied in the connective tissue.
Signicance of differenceses in each group.
-
nd P352 S. Sguier et al. / Journal of Photochemistry aand
biochemical studies evaluating the effect of PDT on the gingi-val
inammatory cells, on the matrix macromolecules as collagenbers and
on the expression of the metalloproteinases (MMPs)during human
periodontal diseases.
Our aim was to evaluate the consequence of PDT on the
inam-matory inltrate during human chronic periodontitis. Several
stud-ies reveal that PDT has a signicant impact on neutrophils
[36,37]
Fig. 4. Immunohistochemical staining of CD1a+ Langerhans cells
in control and treated g(group N). (A) Control gingival section of
a patient of group N showing numerous CD1a+ Lpatient of group N
showing a decreased number of immunolabelled CD1a+ Langerhans
cemagnication 10.
Fig. 5. Gelatin zymogram revealing gelatinase activities in the
supernatant of control (shown in zymogram, heterogenic gelatinase
activities were observed between patients (nmarginal gingiva of
each patient.
Fig. 3. Immunohistochemical staining of CD68+ macrophages in
control and treated ging(A) Control gingival section of a patient
of group L showing a large number of immunoTreated gingival section
of a patient of group L showing a decreased number of
immunepithelium; CT, connective tissue; Original magnication
20.hotobiology B: Biology 101 (2010) 348354but other studies
suggest a pro-tolerogenic effects of PDT on den-dritic cells [38]
or describe immunosuppressive effects of phthalo-cyanine PDT
mediated by CD4+ and CD8+ T cells [39]. Then, itseems that PDT has
an impact on different inammatory cell pop-ulations and it appears
that the composition and the extension ofthe inammatory inltrate
differ according the time (15 min to72 h) of cell analysis after
PDT as suggested by Prignano et al.
ingival samples of patients treated by photodynamic therapy
using nanoemulsionsangerhans cells in the gingival epithelium
(arrows). (B) Treated gingival section of alls in the gingival
epithelium (arrows). E, epithelium; CT, connective tissue;
Original
C) and treated (T) gingival explants by photodynamic therapy
using liposomes. As= 8) and no reproducible differences could be
detected between control and treated
ival samples of patients treated by photodynamic therapy using
liposomes (group L).labelled CD68+ macrophages in the upper
gingival connective tissue (arrows). (B)olabelled CD68+ macrophages
in the upper gingival connective tissue (arrows). E,
-
[7] N. Christodoulides, D. Nikolidakis, P. Chondros, J. Becker,
F. Schwarz, R. Rossler,
nd P[40]. In the present study, the analysis of inammatory
inltratewas performed 7 days after PDT and at that time, the number
ofsome inammatory cell populations was decreased.
Our ndings showed that Antigen-Presenting Cells (APC,
macro-phages and Langerhans cells) located in the inammatory
inltrateand known as one of the rst immune barrier against
pathogens, areparticularly sensitive to PDT. As amatter of fact,
the number ofmac-rophageswas signicantlydecreased after PDTusing
liposomes, andthe number of Langerhans cells (dendritic cells
family, APC)was alsosignicantly decreased after PDT using
nanoemulsions.
A previous study showed that PDT has immunomodulatoryactivity in
various mouse models and dendritic cells treated byPDT showed a
reduced capacity to stimulate the proliferation ofalloreactive T
cells [41]. The ability of PDT to down-regulate auto-immune
processes appears to be related to its capacity to inuencethe
immunostimulatory attributes of APC [38,42]. The PDT couldact on
APC in two ways: rst, by decreasing their number, and sec-ond, by
reducing their capacity of activation of T lymphocytes. As anal
result, PDT could reduce the inammatory phenomenon sinceit is well
known that APC are able on phagocytose and endocytoseprocesses and
thus, are cells specialized in the incorporation of for-eign
elements such as liposomes or nanoemulsions.
Interestingly, in our study, PDT targeted different cell
popula-tions depending upon the drug delivery system used.
ConcerningLangerhans cells in group N (nanoemulsions), our results
sug-gested that nanoemulsions could lead to their migration
towardsthe gingival connective tissue in order to realize the
antigenic pre-sentation. Concerning macrophages in group L
(liposomes), ourndings showed a decrease in the number of this cell
population,associated with an increase in the density of the
gingival collagen.Among the matrix macromolecules, collagen
quantitatively consti-tutes the major component of the gingival
connective tissue andplays a key role in its architecture due to
its bers organization.During the periodontal diseases, inammatory
cells including mac-rophages produce and release proteases (such as
metalloprotein-ases) and cytokines which, together, generate
periodontal tissuedestruction and a degradation of collagen bers.
In addition, mac-rophages are strongly implicated in the turnover
of matrix macro-molecules by phagocytose of collagen bers. In
patients treated byPDT using liposomes, the density of collagen
bers was signi-cantly increased in gingival samples when compared
with controls.This result could be linked to the signicant decrease
in the num-ber of the macrophages in this group.
Pathogenic bacteria and inammatory cells produce a numberof
enzymes and potent proteases capable of degrading host
tissuesleading to the periodontal destruction and the degradation
of col-lagen bers observed during periodontitis. Nevertheless,
studies onthe effect of photosensitizers in combination with light
in this con-text have, in general, focused on the effects of this
potential thera-peutic modality on the viability of the
micro-organisms or on thereduction of bacterial virulence factors
[43]. It is well known byexperiments on beagle dogs [17] and humans
[18] that PDT proce-dure induces a signicant reduction of
periodontopathogens-in-fected sites.
Thus, in the present study we also analyzed by zymography
theactivities of the gelatinases (MMP-2 and MMP-9) since the
activeform of MMP-9 has been proposed as a marker for the
clinicalseverity of periodontal diseases a previous study [2]. In
our condi-tions, the activities of the gelatinases were not
signicantly differ-ent between control and treated teeth with
either liposomes ornanoemulsions. It is likely that the
experimental period of 1 weekbetween the clinical treatment by PDT
and the teeth extractionwas unadapted to evidence eventual changes
in the MMPs expres-
S. Sguier et al. / Journal of Photochemistry asion. Furthermore,
it seems strongly possible that 7 days after PDTthere is a
re-colonisation of periodontal pocket by bacterialelements.A.
Sculean, Photodynamic therapy as an adjunct to non-surgical
periodontaltreatment: a randomized, controlled clinical trial, J.
Periodontol. 79 (2008)16381644.
[8] A. Braun, C. Dehn, F. Krause, S. Jepsen, Short-term clinical
effects of adjunctiveantimicrobial photodynamic therapy in
periodontal treatment: a randomizedclinical trial, J. Clin.
Periodontol. 35 (2008) 877884.
[9] C.N. Lunardi, J.C. Rotta, A.C. Tedesco, Synthesis,
photophysical andphotobiological study of synergic photosensitizer:
zinc-phthalocyanine withCa2+ chelating agent, Curr. Org. Chem. 11
(2007) 647654.
[10] M. Maftoum-Costa, K.T. Naves, A.L. Oliveira, A.C. Tedesco,
N.S. da Silva, C.Pacheco-Soares, Mitochondria, endoplasmic
reticulum and actin lamentbehavior after PDT with chloroaluminum
phthalocyanine liposomal in HeLacells, Cell Biol. Int. 32 (2008)
10241028.
[11] S.M.T. Nunes, F.S. Sguila, A.C. Tedesco, Photophysical
studies of zincphthalocyanines and chloroaluminium phthalocyanines
incorporated intoliposomes in the presence of additives, Braz. J.
Med. Biol. Res. 37 (2004)References
[1] M.A. Listgarten, Pathogenesis of periodontitis, J. Clin.
Periodontol. 13 (1986)418425.
[2] S. Seguier, B. Gogly, A. Bodineau, G. Godeau, N. Brousse, Is
collagen breakdownduring periodontitis linked to inammatory cells
and expression of matrixmetalloproteinases and tissue inhibitors of
metalloproteinases in humangingival tissue?, J Periodontol. 72
(2001) 13981406.
[3] P. Meisel, T. Kocher, Photodynamic therapy for periodontal
diseases: state ofthe art, J. Photochem. Photobiol. B 79 (2005)
159170.
[4] G. Jori, Photodynamic therapy of microbial infections: state
of the art andperspectives, J. Environ. Pathol. Toxicol. Oncol. 25
(2006) 505520.
[5] J.M. de Almeida, L.H. Theodoro, A.F. Bosco, M.J. Nagata, M.
Oshiiwa, V.G. Garcia,Inuence of photodynamic therapy on the
development of ligature-inducedperiodontitis in rats, J.
Periodontol. 78 (2007) 566575.
[6] J.M. de Almeida, L.H. Theodoro, A.F. Bosco, M.J. Nagata, M.
Oshiiwa, V.G. Garcia,In vivo effect of photodynamic therapy on
periodontal bone loss in dentalfurcations, J. Periodontol. 79
(2008) 10811088.Acknowledgements
We thank CAPES for nancial support CAPES/COFECUB 523/06,FAPESP
(Fundao de Amparo Pesquisa do Estado de So Paulo)for nancial
support, 07/55319-0 and 08/53719-4 A.R.S. (09/51729-5) and F.L.
Primo (09/15363-6), were the recipient of FA-PESP fellowships.In
conclusion, our ndings demonstrate that the treatment ofchronic
periodontitis by PDT leads to a specic decrease of
anti-gen-presenting cells populations according to the drug
deliverysystem. Thus, PDT might be considered as an effective
coadjuvanttreatment for chronic periodontal diseases by
supplementing theantibacterial mechanical measures. Furthermore,
the use of lipo-somes has the advantage to reduce the degradation
of the gingivalextracellular matrix. These results are thus
encouraging and nowjustify to initiate an additional study with an
increased numberof patients including an analysis of periodontal
pocket re-colonisa-tion by bacterial elements with time after
PDT.
5. Conict of interest and source of funding statement
The authors declare that they have no actual or potential
con-ict of interest including any nancial, personal or other
relation-ships with other people or organizations within 3 years
ofbeginning our submitted work that could inappropriately inu-ence,
or be perceived to inuence, our work.
This work was supported by grants from Fundao de Amparo
aPesquisa do Estado de So Paulo-FAPESP, So Paulo, Brasil; Conse-lho
Nacional de Desenvolvimento Cientco e Tecnlogico-CNPq,Braslia,
Brasil. This work was also supported by grants from ParisDescartes
University, France.
This collaboration between Paris Descartes University and
SaoPaulo University is supported by CAPES/COFECUB No. 523/06.
hotobiology B: Biology 101 (2010) 348354 353273284.[12] A.R.
Simioni, M.M. Pelisson, M. Beltrame Jr., A.C. Tedesco,
Photophysical and
photobiological studies of a silicon
tribenzonaphthoporphyrazinato
-
incorporated into liposomes for photodynamic therapy use, J.
Nanosci.Nanotechnol. 8 (2008) 32083215.
[13] J.P. Longo, S.P. Lozzi, A.R. Simioni, P.C. Morais, A.C.
Tedesco, R.B. Azevedo,Photodynamic therapy with
aluminum-chloro-phthalocyanine inducesnecrosis and vascular damage
in mice tongue tumors, J. Photochem.Photobiol. B 94 (2009)
143146.
[14] N. Kmerik, H. Nakanishi, A.J. MacRobert, B. Henderson, P.
Speight, M. Wilson,In vivo killing of Porphyromonas gingivalis by
toluidine blue-mediated photo-sensitization in an animal model,
Antimicrob. Agents Chemother. 47 (2003)932940.
[15] M. Wilson, Lethal photosensitisation of oral bacteria and
its potentialapplication in the photodynamic therapy of oral
infections, Photochem.Photobiol. Sci. 3 (2004) 412418.
[16] R.R. de Oliveira, H.O. Schwartz-Filho, A.B. Novaes Jr., M.
Taba Jr., Antimicrobialphotodynamic therapy in the non-surgical
treatment of aggressiveperiodontitis: a preliminary randomized
controlled clinical study, J.Periodontol. 78 (2007) 965973.
[17] B.W. Sigusch, A. Ptzner, V. Albrecht, E. Glockmann, Efcacy
of photodynamictherapy on inammatory signs and two selected
periodontopathogenic speciesin a beagle dog model, J. Periodontol.
76 (2005) 11001105.
[18] P. Chondros, D. Nikolidakis, N. Christodoulides, R. Rssler,
N. Gutknecht, A.Sculean, Photodynamic therapy as adjunct to
non-surgical periodontaltreatment in patients on periodontal
maintenance: a randomized controlledclinical trial, Lasers Med.
Sci. 24 (2009) 681688.
[19] Y.L. Qin, X.L. Luan, L.J. Bi, Y.Q. Sheng, C.N. Zhou, Z.G.
Zhang, Comparison oftoluidine blue-mediated photodynamic therapy
and conventional scalingtreatment for periodontitis in rats, J.
Periodontal Res. 43 (2008) 162167.
[20] X.L. Luan, Y.L. Qin, L.J. Bi, C.Y. Hu, Z.G. Zhang, J. Lin,
C.N. Zhou, Histologicalevaluation of the safety of toluidine
blue-mediated photosensitization toperiodontal tissues in mice,
Lasers Med. Sci. 24 (2009) 162166.
[21] G.C. Armitage, Development of a classication system for
periodontal diseasesand conditions, Ann. Periodontol. 4 (1999)
16.
[22] A.D. Bangham, M.M. Standish, J.C. Watkins, Diffusion of
univalent ions acrossthe lamellae of swollen phospholipids, J. Mol.
Biol. 13 (1965) 238252.
[23] A.C. Pelegrino, M. Carolina, A.F. Gotardo, A.R. Simioni,
M.D. Assis, A.C. Tedesco,
[27] S. Seguier, G. Godeau, N. Brousse, Collagen bres and
inammatory cells inhealthy and diseased human gingival tissues: a
comparative and quantitativestudy by immunohistochemistry and
automated image analysis, J. Periodontol.71 (2000) 10791085.
[28] M. Idowu, T. Nyokong, Photophysical and photochemical
properties of zincand aluminium phthalocyanines in the presence of
magnetic uid, J.Photochem. Photobiol. A: Chem. 188 (2007)
200206.
[29] A.R. Simioni, C. Vaccari, M.I. Re, A.C. Tedesco, PHBHV/PCL
microspheres asbiodegradable drug delivery systems (DDS) for
photodynamic therapy (PDT), J.Mater. Sci. 45 (2008) 580584.
[30] C.S. Foote, Denition of type-I and type-II photosensitized
oxidation,Photochem. Photobiol. 54 (1991) 659663.
[31] R. Malik, A. Manocha, D.K. Suresh, Photodynamic therapy a
strategic review,Indian J. Dent. Res. 21 (2010) 285291.
[32] M.A. Biel, Photodynamic therapy of bacterial and fungal
biolm infections,Meth. Mol. Biol. 635 (2010) 175194.
[33] B.W. Sigusch, M. Engelbrecht, A. Volpel, A. Holletschke, W.
Pster, J. Schutze,Full-mouth antimicrobial photodynamic therapy in
Fusobacteriumnucleatum-infected periodontitis patients, J.
Periodontol. 81 (2010) 975981.
[34] M.A. Atieh, Photodynamic therapy as an adjunctive treatment
for chronicperiodontitis: a meta-analysis, Lasers Med. Sci. 25
(2010) 605613.
[35] A. Azarpazhooh, P.S. Shah, H.C. Tenenbaum, M.B. Goldberg,
The effect ofphotodynamic therapy for periodontitis: a systematic
review and meta-analysis, J. Periodontol. 81 (2010) 414.
[36] P.C. Kousis, B.W. Henderson, P.G. Maier, S.O. Gollnick,
Photodynamic therapyenhancement of antitumor immunity is regulated
by neutrophils, Cancer Res.67 (2007) 1050110510.
[37] M.C. Morgan, R.M. Rashid, The effect of phototherapy on
neutrophils, Int.Immunopharmacol. 9 (2009) 383388.
[38] R. Broady, J. Yu, M.K. Levings, Pro-tolerogenic effects of
photodynamic therapywith TH9402 on dendritic cells, J. Clin. Apher.
23 (2008) 8291.
[39] N. Yusuf, S.K. Katiyar, C.A. Elmets, The immunosuppressive
effects ofphthalocyanine photodynamic therapy in mice are mediated
by CD4+ andCD8+ T cells and can be adoptively transferred to naive
recipients, Photochem.Photobiol. 84 (2008) 366370.
354 S. Sguier et al. / Journal of Photochemistry and
Photobiology B: Biology 101 (2010) 348354Photophysical properties
of crowned porphyrins, Photochem. Photobiol. 81(2005) 771776.
[24] F.L. Primo, M.V. Bentley, A.C. Tedesco, Photophysical
studies and in vitro skinpermeation/retention of
Foscan/nanoemulsion (NE) applicable tophotodynamic therapy skin
cancer treatment, J. Nanosci. Nanotechnol. 8(2008) 340347.
[25] C. Heussen, E.D. Dowdle, Electrophoretic analysis of
plasminogen activators inpolyacrylamide gels containing sodium
dodecyl sulfate and copolymerizedsubstrates, Anal. Biochem. 102
(1980) 196202.
[26] S. Seguier, G. Godeau, M. Leborgne, G. Pivert, N. Brousse,
Immunohistologicand morphometric analysis of cytotoxic T
lymphocytes in gingivitis, J.Periodontol. 70 (1999) 13831391.[40]
F. Prignano, T. Lotti, A. Spallanzani, S. Berti, V. de Giorgi, S.
Moretti, Sequentialeffects of photodynamic treatment of basal cell
carcinoma, J. Cutan. Pathol. 36(2009) 409416.
[41] D.E. King, H. Jiang, G.O. Simkin, M.O.K. Obochi, J.G. Levy,
D.W.C. Hunt,Photodynamic alteration of the surface receptor
expression pattern of murinesplenic dendritic cells, Scand. J.
Immunol. 49 (1999) 184192.
[42] D.W.C. Hunt, J.G. Levy, Immunomodulatory aspects of
photodynamic therapy,Exp. Opin. Invest. Drugs 7 (1998) 5764.
[43] N. Kmerik, M. Wilson, S. Poole, The effect of photodynamic
action on twovirulence factors of Gram-negative bacteria,
Photochem. Photobiol. 72 (2000)676680.
Impact of photodynamic therapy on inflammatory cells during
human chronic periodontitisIntroductionMaterials and methodsPatient
populationStudy designPhotodynamic therapy (PDT) and laser
treatment (Fig. 1)Preparation of photosensitizersTissue
preparationHistology and ImmunohistochemistryZymographyQuantitative
determination of area fraction of collagen fibers, number of
immunolabelled cell populations and zymogram lysis bands by
computer-assisted image analysisStatistical analysis
ResultsArea fraction (AA%) of collagen fibersInflammatory cell
populationsZymography
DiscussionConflict of interest and source of funding
statementAcknowledgementsReferences