Embed Size (px)
Citation preview

Pulmonary Physiology
of Athletes
Michael Ross, MD
Sports Medicine Physician
Rothman Institute
Director, The Performance Lab

VO2=CO x (A-V)O2

VO2=CO x (A-V)O2
• CO
• Cardiac Output
• Heart rate x Stroke Volume

VO2=CO x (A-V)O2

Arterial Oxygen
• =(Hgb x 1.39 x SaO2) + (PaO2 x 0.003)
Arterial Oxygen
• =(Hgb x 1.39 x SaO2) + (PaO2 x 0.003)

Arterial Oxygen
• =(Hgb x 1.39 x SaO2) + (PaO2 x 0.003)

Arterial Oxygen
• Hemoglobin
• Oxygen Saturation

Arterial Oxygen
• Oxygen Saturation
• Get the oxygen from outside the body to inside
the blood
• It’s gotta go through the lungs

VO2=CO x (A-V)O2

VO2=CO x (A-V)O2
Oxygen Extraction
• Mitochondria
• Oxygen diffusion:
capillary network

Exercise overview
• Endurance exercise is an interaction between the
heart, the lungs and the working muscle.

Training effect
• With endurance training, there are structural
changes that improve exercise performance
Heart Changes
• Increased LV size
• Increased LV wall thickness

Heart Changes
• Result in increased contractility, increased stroke
volume, increased cardiac output
Blood Changes
• Increase Red Blood Cell
mass
• Increase Plasma Volume
• Increase in total blood
volume results in
increased oxygen
carrying capacity

Muscle Changes
• Increase in Mitochondria
number and function
• Increase in type I fibers
• Increase in capillary
network

Lung Changes
None

Lung Changes
• There are no measurable
structural changes in the
lung

• The muscle’s ability to use oxygen is greater that
the ability to deliver oxygen to the working muscle

• Although there are no structural changes in the
lung from endurance training…
• The response to exercise by the respiratory
system has a large functional increase
Lung function changes
• Changes occur with exercise.
• Ventilation can increase 20 times with exercise
over baseline
• Increase in respiratory muscle endurance

Exercise Function
• As exercise intensity
increases the muscle
demand for oxygen
increases
• The heart and lungs work
together to supply that
demand

• At low intensity exercise, more oxygen is being
inhaled than carbon dioxide is being exhaled.
• Below the onset of lactic acid, increases in
ventilation precisely compensate for Acid
increase by controlling exhaled CO2

• As intensity increases, beyond the onset of lactic
acid (anaerobic metabolism) there is 4 times as
much CO2 to exhale.
• The increased demand for oxygen as well as the
increased needed to exhale the CO2 results in an
increase in ventilation.
• Increasing ventilation results in an increase in
both the size of each breath (tidal volume) and
the breathing frequency.
• Initially there is an increase in tidal volume until a
physiologic and anatomic limit is reached.
• Further increases in ventilation come from an
increase in breathing frequency.

Respiratory Muscles
• The increase in ventilation is carried out by
reparatory muscles
• Diaphragm as well as accessory muscles

Respiratory Muscles
• Create negative pressure to pull air into the lungs
• As intensity increases, pressure increases to
overcome airway resistance
• Upper airway dilates, glottis opens, bronchial
muscles relax
• As intensity increases, expiratory muscles are
recruited to help empty the lungs
• Increase in respiratory muscle strength is the only
pulmonary adaptation to exercise

Respiratory Limitations
• Exercise Induced
Hypoxemia
• Expiratory Flow Limitation
• Respiratory Muscle
Fatigue
• Exercise Induced Asthma
• Vocal Cord Dysfunction

Exercise-Induced Hypoxemia
• Oxygen Saturation can drop below 90% at max
intensity
• Occurs in up to 50% of athletes
• More common in women at a lower intensity
• Affects performance

Expiratory Flow Limitation
• Seen during heavy exercise
• Leads to hyperinflation/incomplete emptying
• Decreases lung compliance
• Pressure increases beyond the closing pressure
of the airways

Expiratory Flow Limitation
• Pressure increases lead to
increased after load
• Decreased stroke volume
and cardiac output

Expiratory Flow Limitation
• Women have smaller lung volumes and narrower
airways for a given volume
• More prone to EFL
• Masters athletes have a normal loss of recoil
leading to a reduction in maximal flow volume
loops

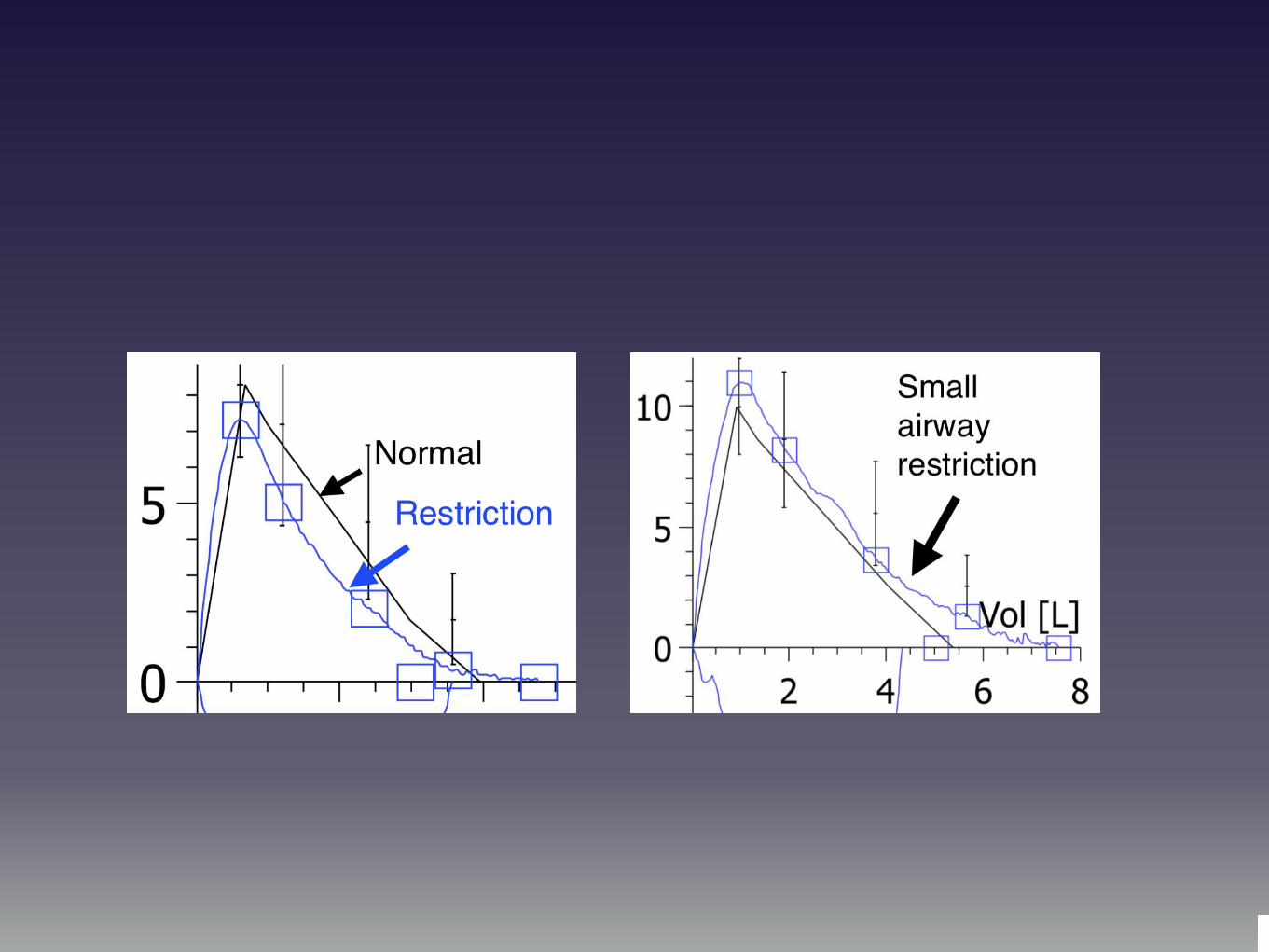
Expiratory Flow Limitation
• Diagnosed with
exercise flow-volume
loops
• Seen in the small
airways

Expiratory Flow Limitation
• Treat the airways responsible for air trapping

Respiratory Muscle Fatigue
• 4kg of muscle that can help
with respiration
• Diaphragm is fatigue
resistant
• The remaining accessory
muscles are fatiguable

Respiratory Muscles
• Can be trained by volume or resistanceSports Med. 2012 Aug 1;42(8):707-24.
• Both can be useful, sample size and
measurements make utility murky
• Bodybuilders have stronger respiratory muscle
strengthJ Sports Med Phys Fitness. 2013 Apr;53(2):139-45.

Respiratory Muscle Training
• Volume Loading
• Increases in maximum voluntary ventilation
• Resistive Training
• increased inspiratory pressure
Respiratory Muscle Training
• Inspiratory muscle strength
and endurance improved in
most studies.J Strength Cond Res. 2013 Jun;27(6):1643-63.
• Dependent on the type of
RMT employed.
Be a Rock Star

Exercise Induced Asthma
Traditionally diagnosed as a >10% drop in FEV1 after
exercise
Implies that pre-exercise levels are normal
(FEV1>80% predicted)
Symptoms include cough, shortness of breath

False Positives and
Negatives
74 Collegiate Athletes
16 positives
16 negatives using bronchodilator
4 positives using bronchodilator
The diagnosis of asthma and exercise-induced bronchospasm in division I athletes.Clin J Sport Med. 2009 Nov;19(6):482-6.

Prevalence
Forty-two of 107 athletes (39%)
were EIB positive.
Thirty-six of 42 EIB-positive
athletes (86%) had no prior
history of EIB or asthma.
Symptoms were not predictive of
EIB (P=0.44).

Prevalence
The prevalence of EIB was 36% in athletes with
negative symptoms and 35% for those with positive
symptoms.
Athletes in high-ventilation sports were significantly
more symptomatic (48%) than athletes in low-
ventilation sports (25%) (P=0.02)
Prevalence of exercise-induced bronchospasm in a cohort of varsity college athletes.Med Sci Sports Exerc. 2007 Sep;39(9):1487-92.

Exercise Induced Asthma
Exercise induced changes in lung mechanics
Underlying asthma that worsens with exercise

Exercise Induced Asthma
Symptoms occur after exercise
So, why do we care?

Respiratory Mechanics
As exercise intensity increases, tidal volumes
increase, followed by an increase in breathing
frequency
As frequency increases, expiratory time decreases
and inspiratory time increases

Respiratory Mechanics
As exercise intensity increases, increasingly more
anaerobic (Type II, Fast twitch, white meat) fibers are
recruited
Under anaerobic conditions CO2 is formed 4 times
more than aerobic exercise
Increased ventilatory demand to compensate for rise
in CO2

Respiratory Mechanics
Less time in expiration
More CO2 to expire

Respiratory Mechanics
Bronchoconstriction makes exhalation more difficult
If the lungs aren’t empted of CO2, they can’t be filled
with O2

VO2 = CO x (A-V)O2
VO2 = Cardiac Output x (Arterial O2 -Venous O2)
VO2 = HR x SV x (Arterial O2 -Venous O2)

VO2 = CO x (A-V)O2
VO2 = Cardiac Output x (Arterial O2 -Venous O2)
VO2 = HR x SV x (Arterial O2 -Venous O2)

Exercise Induced Asthma
Clearly affects exercise, even if symptoms are after
exercise
Why is it hard to treat?
Why do symptoms persist despite normal tests?

Small and Large Airways
FEV1
FEF 25/75

FEV1
Large airway measure.
Asthma is diagnosed when FEV1 is less than 80% of
predicted
Exercise asthma is diagnosed when there is a 7-10%
drop in FEV1 before and after exercise

Flow Volume Loop
Fl
o
w

Flow Volume Loop
Fl
o
w

FEF 25-75
Small airway measurements.
Vital Capacity is divided into quarters.
The first 25% of Vital Capacity is FEF25
The first 50% of Vital Capacity is FEF50
The first 75% of Vital Capacity is FEF75

Flow Volume Loop
Fl
o
w

Small Airways
The pathophysiology in asthma involves not only the
proximal large airways, but also the distal small
airways
The small airways are an important therapeutic target
Extensive disease can be present in the small airways
with little abnormality in conventional pulmonary
function tests.
Usmani OS, Barnes PJ. Ann Med. 2011 Jun 17. Assessing and treating small airways disease in asthma and chronic obstructive pullmonary disease

Exercise Flow Volume Loop

FEF25-75
Small airways
Small airways do not necessarily cause shortness of
breath with exercise
May cause cough
Small airways may be responsible for muscle fatigue

Small Airway Restriction
Small Airway Prevalence PosterSmall Airway Prevalence Poster

Results
Methods
Our current working definition of asthma ignores
the fact that athletes frequently have a FEV1 that
is higher than expected. Athletes may have
airway restriction that is not measured by FEV1
alone. Perhaps the lack of diagnostic utility of the
FEV1 explains the lack of utility of symptoms and
history. If an athlete has dyspnea with exertion, it
is important to look at comprehensive measures of
lung function, not just the FEV1. This study looks
at multiple lung parameters to examine the
prevalence of abnormalities.
In this retrospective review, 304 athletes with
exercise related respiratory symptoms or fatigue
were tested to exhaustion using a ramp protocol.
Pulmonary function testing was performed before
and 10 minutes after exercise by recording both
large airway measurements (FEV1) and the small
airways measurements (FEF 25/75.)
Clinical Relevance
Conclusion
Background
Figure 1
Figure 1 : Normal FEV1 and small airway
restriction
304 athletes were included. 281 (92.4%) had
normal or above normal pre-exercise FEV1
(average FEV1 = 104.92% of predicted)(SD
14.26). FEF 25/75 averaged 70.73% of predicted
in the normal FEV1 group (SD 24.7).
Of the normal FEV1 group, 183 (65.12%) had
small airway limitations (F25/75 <80.)
23 athletes (7.6%) had reduced FEV1 pre-
exercise (average=62.7% of predicted)(SD 13.11).
23 of 23 (100%) of these athletes had below
normal FEF 25/75 values (<80%predicted)
(average = 38.9% of predicted)(SD 15.7).
Following exercise, the normal FEV1 group had
43 subjects (15.3%) with significant decreases in
FEV1 of > 10% (Average decrease was 17.6%
)(SD 7.07) that would qualify as exercise-induced
bronchospasm. 10 of these 43 (23.2%) subjects
also had a decrease in the FEF 25/75 of > 26%
(average change was 15.7)(SD was 19.38).
In the abnormal FEV1 group, 5 of the 23 subjects
(21.7%) had a drop in their FEV1 following
exercise, with 0 of 25 (0%) subjects showing
worsening FEF 25/75 (decrease > 26%).
Athletes presenting with fatigue and/or respiratory
symptoms during exertion had less than predicted
small airway measurements.
By only including FEV1 in the diagnosis of asthma
and exercise induced asthma, small airway
pathology in nearly half of the “normal” patients is
overlooked. Because the treatment is different for
exercise induced asthma and baseline asthma
that worsens with exercise, better criteria for
asthma in athletes must be developed so that
athletes who need treatment aren’t overlooked.
Small Airway Disease Prevalence in Athletes Michael Ross, MD, Brandon Eck, DO
Rothman Institute of Orthopedics, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania
Purpose
To examine the prevalence of small airway
disease in athletes
Figure 2
Figure 2: Flow/Volume loop with higher than
normal FEV1 and scooping of the descending
limb

Results
Methods
Asthma in athletes can be difficult to diagnose.
Because of the higher than normal lung volumes,
an athlete may be in bronchospasm yet still have
normal lung volumes when compared to the
reference values for the general population. It is
hypothesized that if there is a limitation of airflow,
the Vital Capacity during exhalation (VCex) will be
less than the maximal Vital Capacity (VCmax) and
the resultant VCex/VCmax ratio (VC ratio) will be
less than 1. This study examines the relationship
between the VC ratio and asthma.
Retrospective review of 359 Cardio-Pulmonary
Exercise Tests in athletes were reviewed. The
VCex/VCmax ratio was calculated for every
patient. A VCex/VCmax ratio less than one was
labeled as limited expiratory flow. A VCex/VCmax
ratio of one was considered normal. The
associations between lower VCmax ratios and
lung function was evaluated.
Clinical Relevance
Conclusion
Background
Figure 1
Figure 1 : Spirogram demonstrating a
decreased VCex/VCmax ratio
A Spearman rho was used to analyze the
relationship between the VCex/VCmax ratio and
FEV1, FEV1 change with exercise, FEF50, FEF50
change with exercise and FEV1%. Pre-exercise
FEV1, Post-exercise FEV 1, and percent change
of FEV1 were all significantly but not strongly
associated (rho = 0.16 to 0.24).
Using the VCex/VCmax ratio is helpful for
screening for asthma and exercise-induced
asthma in athletes using spirometry.
The VCex/VCmax ratio correlates with the FEV1
as well as an exercise-associated change in
FEV1, making this a good screening tool for
baseline asthma in athletes as well as exercise
induced asthma. The VCex/VCmax ratio has a
role in the diagnosis of asthma in athletes in
whom the FEV1 values might otherwise be normal
for the general population, but might be lower than
expected for athletes. Treating asthma for a
normalization of the VCex/VCmax ratio might be
viable in patients with exertional dyspnea.
VCex/VCmax Ratio as an indicator of asthma in athletesMichael Ross, MD, Brandon Eck, DO
Rothman Institute of Orthopedics, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania
Purpose
To examine the role of using VCex/VCmax as a
diagnostic tool for asthma in athletes

VCex/VCmax

Results
Methods
Asthma in athletes can be difficult to diagnose.
Symptoms are less likely to be an aid in diagnosis
and baseline lung volumes may be elevated
because of endurance training.
Endurance athletes have an average FEV1 of
112% of predicted. If endurance athletes are
compared to the normal population, an athlete
may have normal values but still be broncho-
contstricted. The FEV1/FVC ratio has been used
in the diagnosis and stratification of chronic lung
disease but it has not yet been used for athletes.
The study examines the utility of an internal
comparison (FEV1/FVC ratio) to diagnose asthma
in athletes.
A retrospective chart review was performed on
304 patients who underwent Cardio Pulmonary
Exercise Testing. Pre and post exercise
FEV1/FVC ratios were calculated and compared
to Gold Criteria for pulmonary obstruction.
Clinical Relevance
Conclusion
Background
Figure 1
Figure 1 : Post exercise FEV1/FVC values in
the GOLD Criteria
A linear regression analysis was completed to
evaluate the relationship between the FEV1/FVC
ratio and Gold Criteria. There is a significant
correlation between post exercise FEV1/FVC ratio
and worsening obstruction measured by the
GOLD criteria. P=0.0002
The post-exercise FEV1/FVC ratio is a useful for
diagnosing asthma in athletes who have
undergone an exercise challenge test.
By comparing the athlete to his own lung function,
the difficulty in trying to compare an athlete to the
normal population can be avoided.
The post-exercise FEV1/FVC ratio allows
diagnosis of exercise related asthma conditions
even if the athletes have normal FEV1 compared
to the predicted values, resulting in fewer missed
diagnoses. Establishing a diagnosis of baseline
obstruction is important in differentiating between
baseline asthma and exercise-induced
bronchoconstriction, as the treatment options
differ between the two conditions.
FEV1/FVC Ratio as an indicator of asthma in athletesMichael Ross, MD, Brandon Eck, DO
Rothman Institute of Orthopedics, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania
Purpose
To examine the role of FEV1/FVC as a diagnostic
tool for asthma in athletes.
Table 1
Table 1 : GOLD Criteria
0
0.2
0.4
0.6
0.8
Controls
Gold 1
Gold 3
0.74 0.8
0.59
0.53
0.45FE
V1/F
VC
Gold 1 FEV1/FVC < 0.7 FEV1 <80% perdicted
Gold 2 FEV1/FVC < 0.7 50%<FEV1 < 80% predicted
Gold 3 FEV1/FVC < 0.7 30%<FEV1<50% predicted
Gold 4 FEV1/FVC < 0.7 FEV1 <30% predicted

Lactic Acidosis
Hydrogen Ions are buffered by Bicarbonate
H+ + HCO3- <=> H2CO3 <=> H2O + CO2
Water and Carbon Dioxide are exhaled

Muscle Fatigue
Accumulation of H+ leads to muscle fatigue
Decrease in both force and velocity of contractions

Small Airway Restriction

Treatment
Inhaled corticosteroids and Beta agonists: HFA
aerosols provide better penetration for small airways
Formoterol/budesonide, ciclesonide,
beclomethasone, flunisolide
Inhaled beta agonists v. Leukotriene agonists for peak
flow declines

Treatment
Pulmonary Rehabilitation: Endurance training to help
increase metabolic compensation for lactic acidosis
Physical training showed improvement in maximum
oxygen uptake without affecting pulmonary function
People with stable asthma should be able to
exercise without symptom exacerbation. Cochrane Database Syst Rev. 2013
Sep 30;9:CD001116. Physical training for asthma.Carson.

Thank You
• Questions?

Vocal Cord Dysfunction
Normal Breathing:
Vocal cords open with
respiration and close with
swallowing

Vocal Cord Dysfunction
Abnormal Breathing:
Vocal cords paradoxically close
with inhalation or early
expiration

VCD Symptoms
Inspiratory difficulty
Choking sensation
Stridor
Concommitant psychiatric diagnosis

VCD: Triggers
Idiopathic
Acid Reflux
Post-nasal drip

VCD Exam
Inspiratory wheeze at larynx does not transmit to
thorax

Diagnosis
Laryngoscopy (60% sensitive if asymptomatic--100%
sensitive during an attack)
Truncated inspiratory limb on flow/volume loop

Vocal Cord Dysfunction
Fl
o
w

VCD: Treatment
Speech Pathology =>Breathing Manuvers
rapid, shallow panting
diaphragmatic breathing
nasal breathing
straw/purse-lipped/hissing breathing

VCD Treatment
H2 Blockers/Proton Pump Inhibitors
Nasal Steroids/Antihistamines
Psychological counseling
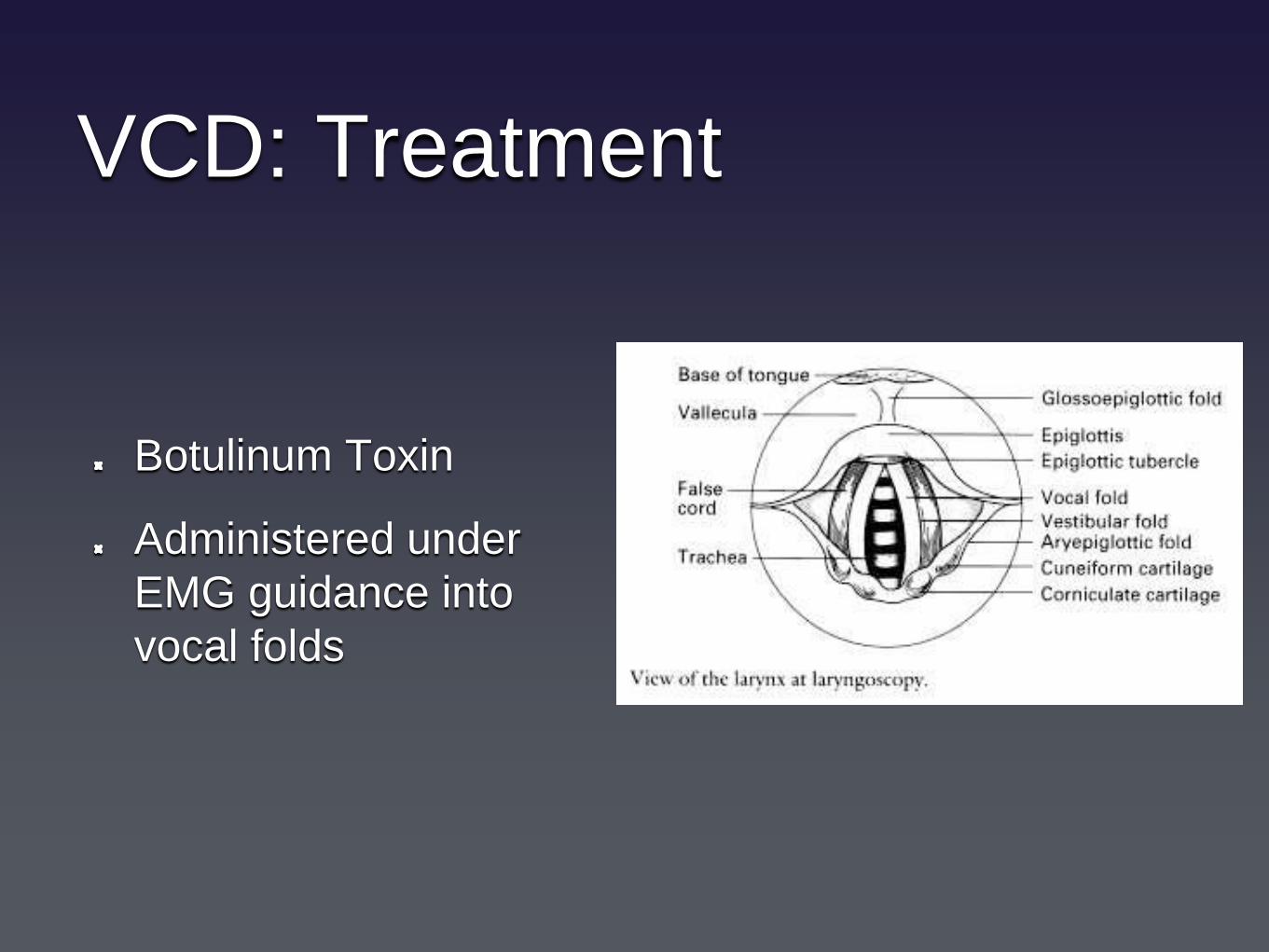
VCD: Treatment
Botulinum Toxin
Administered under
EMG guidance into
vocal folds

Vocal Cord Dysfunction
Consider in patients with refractory asthma
More than half have concomitant asthma

Exercise Induced Asthma
Large Airways (FEV1 decline) are responsible for
shortness of breath
Small Airways (FEF25/75) are responsible for lactic
acidosis and expiratory flow limitations
Exercise Flow/Volume loops allow for correlation
between performance and airway disease





























