Embed Size (px)
Citation preview

Psychosocial support for IDUs and effects on HCV treatment
Bernd Schulte

Determinants for heath care utilisation
Andersen 1995
Health caresystem
Externalenvironment
Predisposingcharacteristics
Enablingresources
Need
Personalhealth
practices
Use ofhealth
services
Perceivedhealth status
Evaluatedhealth status
Consumersatisfaction
Environment Population characteristics OutcomesHealthbehaviour
Influenceable variables for HCV treatment success
Knowledge Access to HCV care Readiness for HCV treatment Improved HCV treatment outcomes
– Health related quality of life– Sustained virological response (SVR)

Influenceable variables for HCV treatment success
Knowledge Access to HCV care Readiness for HCV treatment Improved HCV treatment outcomes
– Health related quality of life– Sustained virological response (SVR)

Knowledge Improvement Among MMT Clients in a Hepatitis Intervention Program RCT: 256 alcohol drinking MMT clients Interventions:
MI-Individual vs. MI-Group vs. Nurse-led HHP Measures:
– 6-item HBV & 7-item HCV “Knowledge & Attitudes towards Hepatitis tool”
– Baseline and 6-month follow-up
Nyamathi et al. 2010

Improvement Among MMT Clients in a Hepatitis Intervention Program Overall, knowledge of HCV/HBV increased
significantly from pretest to posttest (P < .0001)
Nyamathi et al. 2010
Program type
Improvement in knowledge mean (SE)
HBV HCV
MI-I 3.08 (0.36) 3.78 (0.42)
MI-G 2.62 (0.44) 4.17 (0.36)
NL-HHP 3.33 (0.42) 4.24 (0.42)

Influenceable variables for HCV treatment success
Knowledge Access to HCV care Readiness for HCV treatment Improved HCV treatment outcomes
– Health related quality of life– Sustained virological response (SVR)

Managed care networks (MCN) to improve access to HCV specific care
Majority of HCV+ individuals referred by medical staff (i.e. GPs), most of them not attending HCV clinic
Single mode of referral is not effective enough Interventions: Managed care networks (MCN)
– Incorporation of relevant stakeholders– Referral protocol, educational sessions – Referral pathway including nonmedical referrals– Outreach clinics in drug treatment- and prison clinics.
Tait et al. 2009
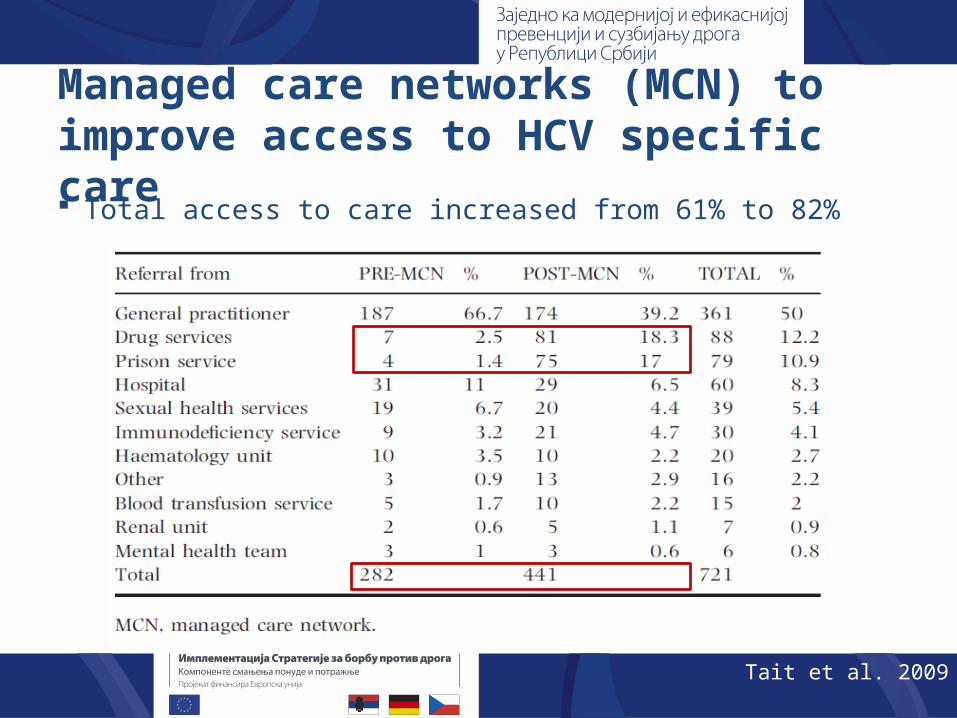
Managed care networks (MCN) to improve access to HCV specific care Total access to care increased from 61% to 82%
Tait et al. 2009
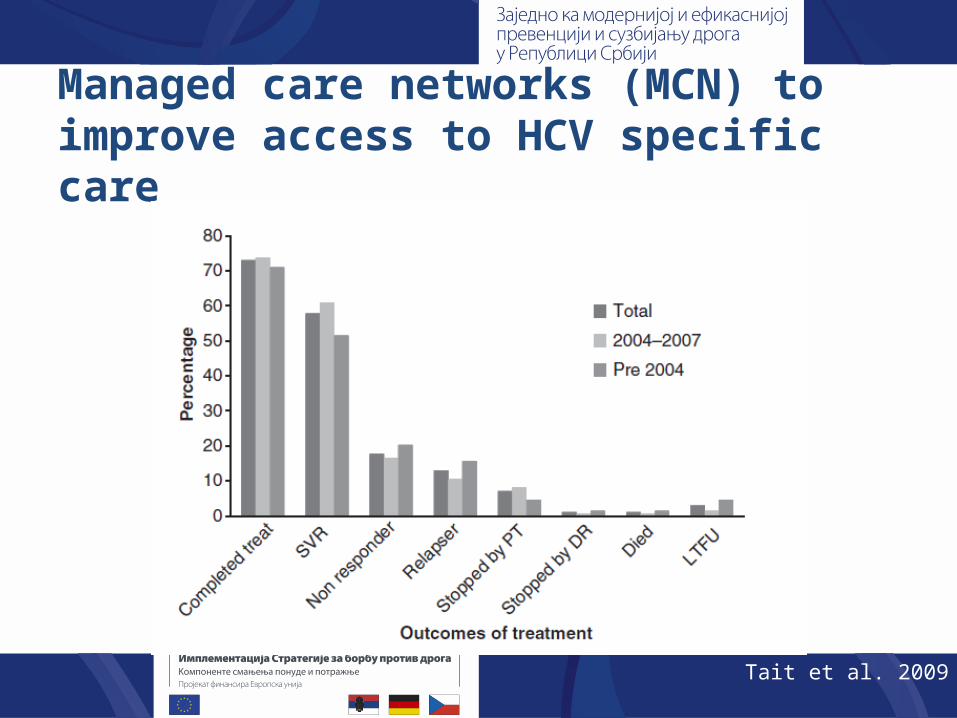
Managed care networks (MCN) to improve access to HCV specific care
Tait et al. 2009

Influenceable variables for HCV treatment success
Knowledge Access to HCV care Readiness for HCV treatment Improved HCV treatment outcomes
– Health related quality of life– Sustained virological response (SVR)

20-minute educational program to accept HCV treatment
Gupta et al. 2009

Influenceable variables for HCV treatment success
Knowledge Access to HCV care Readiness for HCV treatment HCV treatment uptake Improved HCV treatment outcomes
– Health related quality of life– Sustained virological response (SVR)

HCV self-management programme RCT: 132 HCV+ patients Intervention: 6-weeks HCV self-management
programme (2-h weekly) vs. information-only Main measures at baseline and 6 weeks later:
– HRQOL: SF-36; HQLQ – HCV knowledge: 15 item questionnaire– Self-efficacy: HCV-specific self-efficacy questions
Groessl et al. 2010

HCV self-management programme Self-management programmes can improve HCV
disease knowledge and HRQOL
Groessl et al. 2010
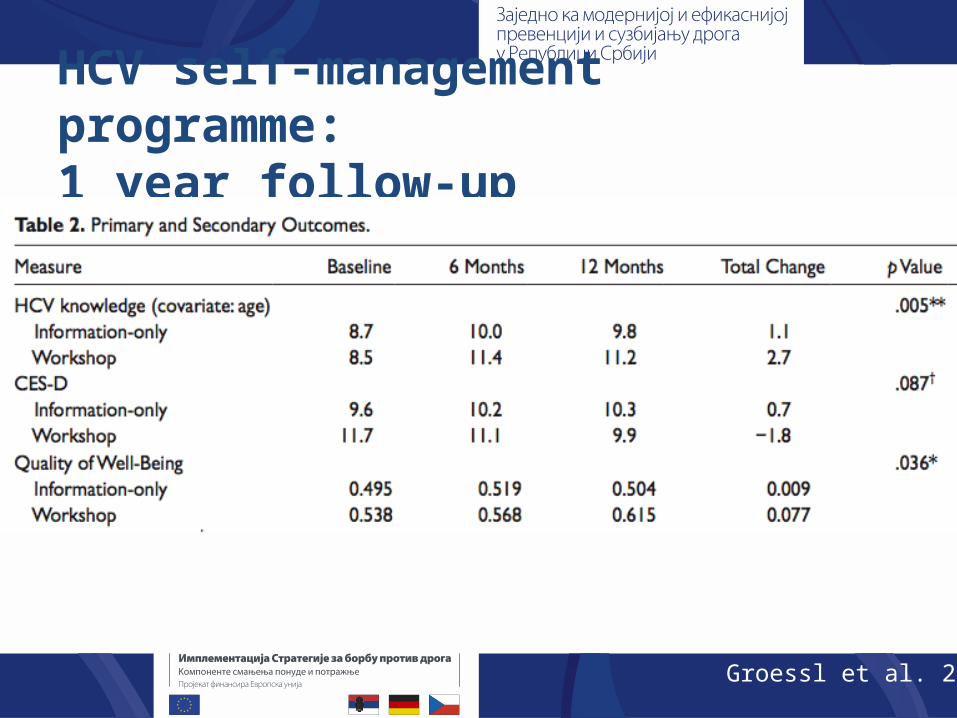
HCV self-management programme: 1 year follow-up
Groessl et al. 2013

HCV self-management programme and SVR
Groessl et al. 2013

Influenceable variables for HCV treatment success
Knowledge Access to HCV care Readiness for HCV treatment HCV treatment uptake Improved HCV treatment outcomes
– Health related quality of life– Sustained virological response (SVR)

Nurse-led psychoeducation and SVR RCT: 244 HCV+ GT1 patients Intervention: Medical consultation + systematic
nurse-led PE vs. medical consultation Measure: SVR evaluated at 12 and 24 weeks after
the end of treatment
Larrey et al. 2011
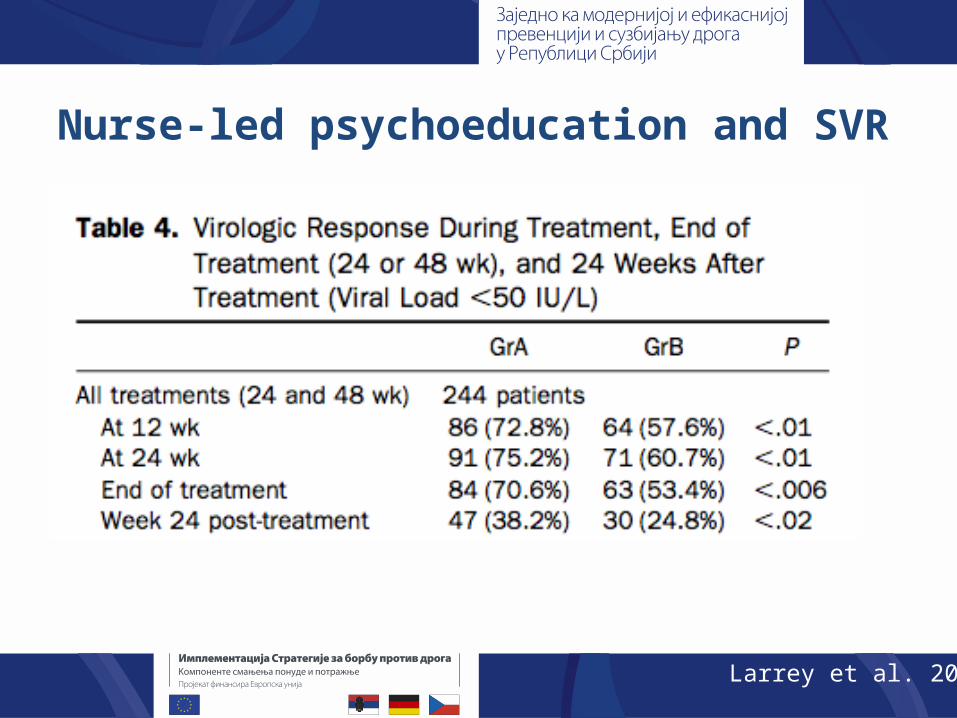
Nurse-led psychoeducation and SVR
Larrey et al. 2011

Multidisciplinary support programme increases the efficiency of HCV treatment RCT: 447 patients in antiviral HCV treatment Intervention:
– Multidisciplinary support programme (MSP): (Hepatologist/Nurse, Psychologist, Pharmacists, Psychiatrist)
– Treatment as usual (TAU) (Hepatologist/Nurse)
– 3 groups: MSP, TAU, MSP validation group Measures:
– Impact of MSP on adherence to HCV treatment– Efficacy (SVR)
Carrion et al. 2013

MSP increases efficiency of HCV treatment
Carrion et al. 2013
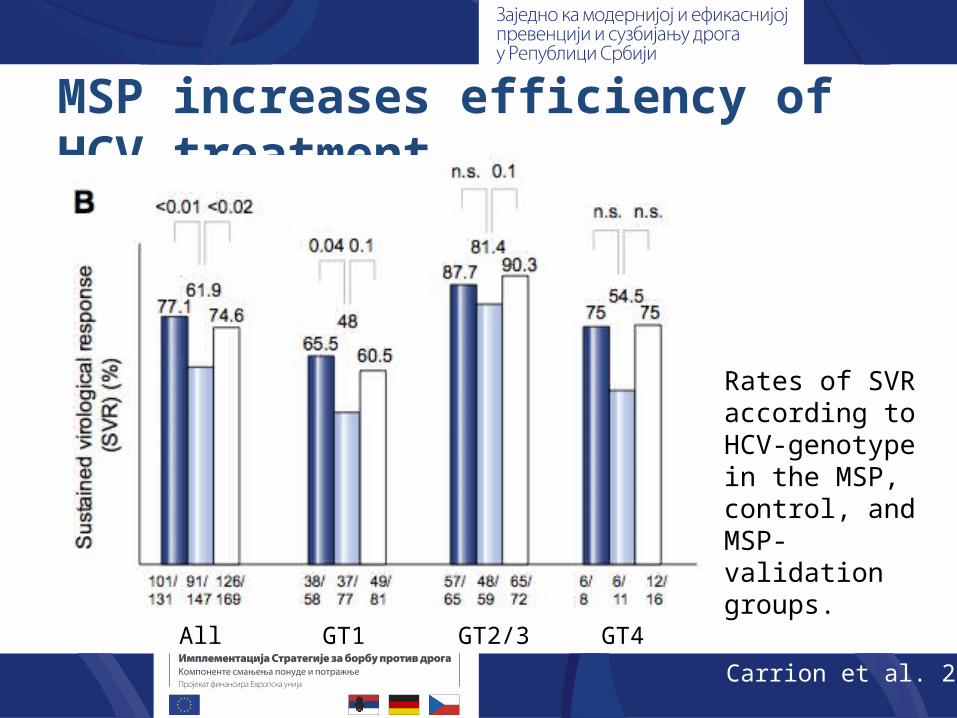
MSP increases efficiency of HCV treatment
Rates of SVR according to HCV-genotype in the MSP, control, and MSP-validation groups.
All GT1 GT2/3 GT4
Carrion et al. 2013

Psychoeducation Improves Hepatitis C Virus Treatment in Opioid Substitution Controlled, Prospective Multicenter Trial with 189
OST patients in antiviral HCV treatment HCV specific PE (group) intervention vs. TAU
– Module 1: HCV infection, risk factors, etc.– Module 2: HCV treatment, side effects, etc. – Module 3: Coping strategies, self-help, etc.
PE sessions and follow-ups– GT1/4: 12 + 10 – GT2/3: 12 PE + 5
Reimer et al. 2013

Psychoeducation Improves Hepatitis C Virus Treatment in Opioid Substitution
Figure 1: Completion of treatment depending on GT and PE
Reimer et al. 2013

Psychoeducation Improves Hepatitis C Virus Treatment in Opioid Substitution
Figure 2: SVR depending on GT and the number of attended PE sessions
Reimer et al. 2013
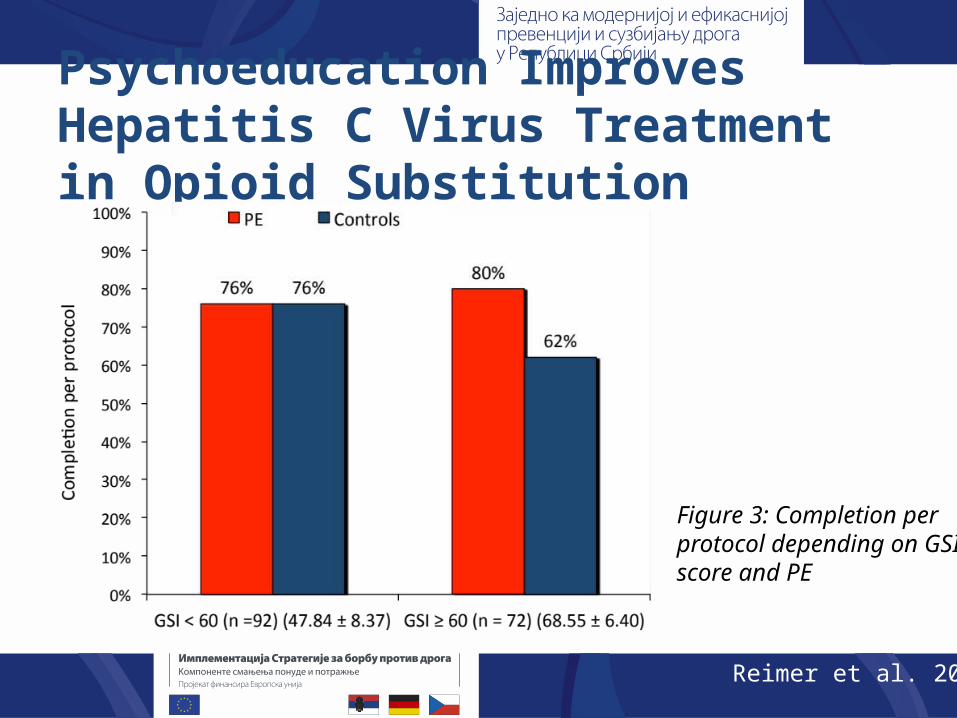
Psychoeducation Improves Hepatitis C Virus Treatment in Opioid Substitution
Figure 3: Completion per protocol depending on GSI score and PE
Reimer et al. 2013

Determinants for heath care utilisation
Andersen 1995
Health caresystem
Externalenvironment
Predisposingcharacteristics
Enablingresources
Need
Personalhealth
practices
Use ofhealth
services
Perceivedhealth status
Evaluatedhealth status
Consumersatisfaction
Environment Population characteristics OutcomesHealthbehaviour
KNOWLEDGE and COMPETENCE
COSTS
MOTIVATION
SVR
HRQOL




![[TÍTULO DEL DOCUMENTO] - idUS](https://img.dokumen.tips/doc/110x75/6251ffe8d7e93009e44c24ac/ttulo-del-documento-idus.jpg)

























