Embed Size (px)
Citation preview

J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r . com/ loca te / j p ro t
Review
Proteomics and biomarkers in clinical trials fordrug development
Jung-min Lee⁎, Jasmine J. Han, Gary Altwerger, Elise C. KohnMolecular Signaling Section, Medical Oncology Branch, Center for Cancer Research, National Cancer Institute, NIH, Bethesda,Maryland, United States
A R T I C L E I N F O
⁎ Corresponding author at: 10 Center Dr. MSC7735; fax: +1 301 480 0074.
E-mail address: [email protected] (J. Lee
1874-3919/$ – see front matter. Published bydoi:10.1016/j.jprot.2011.04.023
A B S T R A C T
Available online 4 May 2011
Proteomics allows characterization of protein structure and function, protein–proteininteractions, and peptide modifications. It has given us insight into the perturbations ofsignaling pathways within tumor cells and has improved the discovery of new therapeutictargets and possible indicators of response to and duration of therapy. The discovery,verification, and validation of novel biomarkers are critical in streamlining clinicaldevelopment of targeted compounds, and directing rational treatments for patientswhose tumors are dependent upon select signaling pathways. Studies are now underwayin many diseases to examine the immune or inflammatory proteome, vascular proteome,cancer or disease proteome, and other subsets of the specific pathology microenvironment.Successful assay verification and biological validation of such biomarkers will speeddevelopment of potential agents to targetable dominant pathways and lead to selection ofindividuals most likely to benefit. Reconsideration of analytical and clinical trials methodsfor acquisition, examination, and translation of proteomics data must occur before wemarch further into future of drug development.Published by Elsevier B.V.
Keywords:ProteomicsBiomarkersClinical trialDrug developmentCancerTargeted therapy
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26332. Definitions of a biomarker and proteomics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26333. Proteomics technologies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26334. Components of validation for biomarkers in drug development . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26345. Approaches for the identification of potential therapeutic targets and biomarkers . . . . . . . . . . . . . . . . . . . 26356. Challenges and opportunities for biomarkers for targeted therapies . . . . . . . . . . . . . . . . . . . . . . . . . . . 26367. Identification of biomarkers as therapeutic targets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26368. Criteria for development of validated therapeutic targets in clinical trials . . . . . . . . . . . . . . . . . . . . . . 26379. Biomarkers and targeted therapy in clinical trials for drug development . . . . . . . . . . . . . . . . . . . . . . . 2638
10. Linking proteomics and genomics data for drug development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2638
1906, Building 10, Room 12N/226, Bethesda, MD 20892-1906, United States. Tel.: +1 301 443
).
Elsevier B.V.

2633J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
11. Future direction of biomarker, proteomics for drug development . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263912. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2639Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2639References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2639
1. Introduction
Advances in biotechnology and improved understanding ofcancer anddisease biologyhave shifted the treatmentparadigmto targeted therapy. We have enhanced our ability to guideapplication of new and existing treatments with development,assay verification, biological validation and application ofbiomarkers. However, to be successful, we need a thoroughunderstanding of the relationship between putative biomarkersand treatment effects. We must consider new clinical trialdesigns that may consist of randomized cohorts, prospectivelyplanned endpoints, and/or post-hoc analyses. These strategieswill succeed if reliable, adequately powered, biologically vali-dated biomarkers are identified and appropriately applied forprospective patient selection via clinical trials. Continuedinclusion of preplanned biological correlates will allow ongoingoptimization of targeted therapy. These eventswill guide futuredirections of proteomics, affecting how we integrate proteomicinformation into the selection of therapy for advanced andrecurrent cancers, and other diseases. For the purposes of thisdiscussion, most examples will emanate from the oncologyliterature, where these issues and advances are at the forefrontof current controversy.
2. Definitions of a biomarker and proteomics
Abiomarker isdefinedbyAtkinsonetal. in theUSFoodandDrugAdministration (FDA) Biomarker Definitions Working Group as“a characteristic that is objectively measured and evaluated asan indicator of normal biologic processes, pathogenic processes,or pharmacologic responses to a therapeutic intervention” [1].Those characteristics that are informative for clinical outcomecan be categorized broadly as prognostic or predictive bio-markers. Prognostic biomarkers classify patients into subgroupswith distinct expected clinical outcomes, such as progression ordeath, but they do not inform the choice of therapy. Conversely,predictive biomarkers should identify subgroups of patientswhose tumors are likely to have therapeutic sensitivity orresistance based upon marker status [2,3].
For example, breast cancers with either HER2 amplification,or triple negative status (negative for estrogen receptor,progesterone receptor, and HER2 amplification), are recognizedas poor-risk subgroups and those designations are therebynegative prognostic biomarkers [4,5]. HER2 amplification alsofunctions as apositive predictivebiomarker. HER2 amplificationdefines a subgroup of breast cancer patients for whomtrastuzumab and other anti-HER2 interventions have highlikelihood of providing benefit, positively predicting outcometo agent(s) [6]. Conversely, excision repair cross-complementa-tion group 1 (ERCC1) is both a positive prognostic and a negativepredictivemarker in non-small cell lung cancer (NSCLC) [7]. The
International Adjuvant Lung Cancer Trial showed that highERCC1 protein expression was associated with improvedsurvival in patients who did not receive chemotherapy. But,thebenefit of adjuvant cisplatin-based chemotherapywasmoreprofound in patients with low ERCC1 expression due to reducedplatinum-DNA adduct repair [8] [9] [10]. Lastly, in advancedcolorectal cancer, the benefit of the anti-EGFR monoclonalantibody, cetuximab, appears limited to patients with tumorswith wild-type KRAS genotype [11]. This indicates that KRASwild type status could and should be used to select patients forcetuximab therapy. Thus, knowledge of molecular and proteinevents will enlighten clinical decision making from differentpoints of view.
Proteomics is a tool with which to characterize proteinstructure, function, protein–protein interactions, and associ-ated protein modifications. These protein characteristicscollaborate to form complex signaling networks mediatingthe active cellular proteome. Proteomics output, patterns orindividual endpoints, also can be evaluated as biomarkers.Understanding the active proteome is critical for developmentof effective predictive and prognostic biomarkers. Onceidentified, key potential events in the proteome can beexploited for the development of targeted cancer treatments.This reinforces the need for application of high throughput,accurate, precise, sensitive, and specific tests for discoveryand endpoints validation, followed by rapid translation forpatient stratification.
3. Proteomics technologies
Technologies exploring the proteome for biomarker discoveryrange from classical immunohistochemistry and immunoas-says for single or small sets of proteins, to mass spectrometry(MS) and other high throughput approaches to examinemillions of peptides. Early MS use evaluated differentialpatterns of protein and peptide expression in patient serumand other biospecimens [12,13]. While preliminary data usingthe pattern approach was initially promising, the field hasmoved forward to sequence peptides and proteins, withsecondary individual entity validation as the diagnosticdiscriminant. Sequence information permits both develop-ment of biomarkers and/or therapeutic targets, and applica-tion of proteomic knowledge to advance understanding ofunderlying pathophysiology. Studies are now underway inmany diseases to examine selectively the immune or inflam-matory proteome, vascular proteome, cancer proteome, andother subsets of the disease-specific microenvironment.
Mass spectrometry techniques such as nanoflow liquidchromatography-tandem mass spectrometry (nanoLC-MS/MS)and matrix-assisted laser desorption/ionization time-of-flightmass spectrometry (MALDI-TOF MS) along with other

2634 J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
techniques such as immunocapture platforms have enabledhigh-throughput analysis of a proteomeor functional subsets ofthe proteome. Reverse phase protein assays (RPPA) have beenappliedmore recently as biased examinations of tissue proteinsin formats wherein protein lysates are arrayed on a solidsurface. Arrayed proteins are interrogated with standardizedantibodies specific for total and activated protein targetsallowing for investigation of pre-selected functional signalingoutputs [14,15].
These techniques have been applied to oncology tissuesamples, leading to the discovery of potential pathwaybiomarkers to detect disease and monitor established cancerthrough the course of treatment [16]. Carey et al. examined 80validated proteins from signaling pathways in advanced-stage, high-grade serous ovarian carcinoma cases via RPPAto identify expressed proteins associated with response toprimary chemotherapy [17]. Normalization of CA125, anestablished biomarker, by the 3rd cycle of platinum-basedchemotherapy was chosen as the primary outcome measureof response; TGF-β pathway signaling correlated strongly withchemoresistance in this study. RPPA were also used in headand neck squamous cell carcinoma (HNSCC) to examine 60protein endpoints in matched tumor and nonmalignantbiopsy specimens from 23 patients. This paired analysisapproach identified 18 differentially elevated proteins includ-ing PKCι [18]. PKCι is overexpressed in 70% of squamous cellNSCLC with amplification of 3q26, which harbors PKCι andPIK3CA, the p110 α catalytic phosphoinositide-3-kinase (PI3K)subunit gene [19]. This is an example of a discovery-basedRPPA application that also has yielded information that can beconsidered for future clinical benefit.
4. Components of validation for biomarkers indrug development
The FDA began the Critical Path Initiative in 2004, aiming toimprove discovery, validation, and production of currenttherapeutics by focusing on selected areas. It defined 6 focusedtopics in 2006, identifying biomarker development as one ofthe two most important necessary advances. This key areaaddresses creation of improved tools, such as biomarkers, forevaluation of clinical therapies. The recommendation for co-development of a drug and a selective biomarker was firstdescribed in a draft FDA guidance in 2005. Co-developmentimplies generation of processes and guidelines describinganalytical (technical) test validation (alsoknownasverification),clinical test validation (demonstration of biological validation),
Table 1 – Components of validation for biomarkers in clinical tr
Analytical validation(also known as verification)
Clinical validation
Accuracy Sensitivity: true positive desPrecision Specificity: true negative desReproducibility Behavior of biomarker in a p
as a function of biological vaIntrinsic measurements of error Positive and negative predic
and clinical utility (Table 1) [20]. Thismarked the FDA's first steptoward integrating rapidly evolving biology of cancer and otherdiseases into existing regulatory processes; it is anticipated thatthis mandate will be applied to targeted drug development formany medical needs. Currently, the FDA recommends applica-tion of a verified and validated biomarker for the identificationof the target clinical subpopulation when employing the use ofa drug for which subpopulation targeting is identified as partof drug registration. For example, the Table of Valid GenomicBiomarkers in theContext ofApprovedDrug Labels, availableonthe FDA website (http://www.fda.gov/Drugs/ScienceResearch/ResearchAreas/Pharmacogenetics/ucm083378.htm) detailstrastuzumab and the required indications for treating patientswith HER-2 amplified tumor. The initial test identifying theHER-2 amplified subpopulation was required for FDA approvalbefore trastuzumab received approval for adjuvant treatmentof women with lymph node-positive, HER-2 over-expressingbreast cancer [21]. Incorporation of predictive biomarkersinto clinical trials during the drug development process willtranslate into greater accuracy in selecting target patientsubgroups.
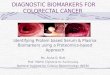
Both verification and validation of biomarkers is necessaryfor their appropriate application for targeted therapeuticsselection and their use as drug response marker(s) in clinicalpractice. The interpretation of validation is broad and mostoftenhas beendescribedas theprocess of linking abiomarker toclinical or behavioral endpoints. The broad concept of valida-tion includes “efforts to confirm the accuracy, precision, andeffectiveness of results and can be defined as analytical andclinical validation” [22]. Analytical (technical) validation is nowcalledverification.Analyticmethodverification is theprocessofconfirming the assay, its performance characteristics, and therequired optimal conditions to generate reproducibility andaccuracy of the assay [22–24]. Clinical or biological validation isrelated to how a certain marker behaves in a population andbetween populations, depending on biological variabilitywithinthe population [22]. Both clinical and analytical validation needto be incorporated into clinical correlative studies for biomarkerand drug development [25] although ultimately they may fallto different review and registration paradigms. To date, mostputative biomarkers have fallen short of adequate biologicalvalidation even where verification has been confirmed throughFDA review. The integration of verified and validated proteomicbiomarkers into clinical drug development programs willexpedite pipeline decision-making process by adding criticalinformation about the pharmacologic and/or pharmacody-namic mechanism(s) and efficacy of a potential therapeuticagent as shown in the cartoon in (Fig. 1).
ials for drug development.
Clinical utility
ignation Evaluation of risk and benefit of diagnosis andconsequent treatment resulting from the testignation
opulationriabilitytive value

Prospective clinicaltrial stratified by
biomarker
Biomarker andtarget
validation
Retrospectivebiomarkeranalyses
RAS
b-RAF
MEK
p-ERK1/2
EGFR
New targetidentification
New drug development
Fig. 1 – The decision-making process of drug development incorporating proteomics. Proteomic profiling has been applied foridentification of predictive markers and therapeutic targets through retrospective analyses. The discovery and validation ofbiomarkers would lead to development of new potential drugs via prospective clinical trials stratified by biomarker for moreeffective targeted therapy in recurrent cancers.
2635J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
5. Approaches for the identification of potentialtherapeutic targets and biomarkers
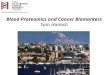
What is the best approach with which to identify and charac-terize a biomarker for drug selection? One is a biomarker-forward, focused, target-associated view specifically addressingbiomarkers emanating from the drug development hypothesisto select patients for therapy prospectively. Alternatively, anagnostic, trial-backwards, view would apply biased selectionretrospectively with biological validation of translational end-points against patient outcome in targeted agents' trials (Fig. 2).
The first approach requires definition, verification, andvalidation of biomarkers selected for their defined targetmodulation, and is an immediate and logical extension of thedrug development process. This approach would lead rapid-ly to patient stratification prior to therapy if clinically suc-cessful; this requires the discriminant to be “spot-on”. Therecent success of selective b-Raf inhibitors for V600E BRAFmutant melanoma is an example of a biomarker-forwardselection where prior knowledge of BRAF mutations wasrequired [26]. This is illustrated also in treatment of HER-2overexpressing breast, gastric, and other cancers, where therequirement for >2 copies of HER2 by FISH or a 3+ IHC stainare required and have been shown to predict clinical potentialfor trastuzumab and other HER2-directed treatments [27].The biomarker-forward approach is limited in that it leaveslittle room for unanticipated on-target effects and may missimportant off-target outcomes.
The trial-backwards approach allows investigation, identifi-cation, and examination of potential biomarkers in the contextof molecular therapeutic clinical investigation. This identifica-tion approach includes evaluation of initially unanticipatedevents and has the capacity to uncover important off-targetevents. Examination of prospectively collected biospecimenseither within the trial design or post-hoc analysis may yieldbroader results than the narrow trial-forward approach. Thestratification of benefit to cetuximab as a function of EGFRmutation, overexpression, and downstream pathway activa-tion, was studied retrospectively in advanced colorectal cancer.Here,mutational activation of KRASwas shown to be a negativepredictive biomarker foroutcome [11]. Thiswasunexpected, butscientifically logical when considered in the context of thebiochemical pathways involved.
Retrospective analysis of candidate biomarkers in cancer clin-ical trials has been the most common early biomarker approachused to date. Unfortunately, many reports are exploratory andcorrelative and only a very small number of putative biomarkersmove forward to full verification and validation. This is the basisfor arguments for prospectively planned proteomic and geneticbiomarker profiling pre- and post/during treatment, with tissueacquisition following clear standard operating procedures, andpowered for definitive analysis. Applying biomarker-backwardsapproaches for discovery followed by powered prospectivebiomarker-forward studies for biological validation and con-firmation may reduce the primary problem of indiscriminateapplication of targeted agents in many diseases expediting anexpensive and time consuming drug development process.

Fig. 2 – Prospective and retrospective approaches for identification of potential biomarkers. A biomarker-forward, focused,target-associated prospective approach specifically address biomarkers to select patients for therapy. Alternatively, anagnostic, trial-backwards, retrospective approach would apply biased selection with biological validation of translationalendpoints against patient outcome in targeted agents' trials.
2636 J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
6. Challenges and opportunities for biomarkersfor targeted therapies
Recent high-throughput molecular proteomic technologieshave yielded potential in both identification and developmentof biomarkers and therapeutic targets. Treatment of patientswith advanced NSCLC with EGFR tyrosine kinase inhibitors(TKIs) is established for first-line, maintenance, and subse-quent treatment in patients with EGFR mutations [28–31].Although EGFR mutation is a validated predictive marker forfirst-line therapy in patients with advanced NSCLC, only 70%to 75% of patients will respond and all the patients willeventually develop resistance to the therapy. Thus, it is acontinuing challenge to optimize predictive biomarkers withwhich to pre-select patients with EGFR mutations who willnot benefit from EGFR TKI treatment. These biomarkers arelikely also to provide insight into the biology of the treatmentresistance.
The insulin like growth factor receptor (IGFR) pathwayinteracts with the EGFR pathway, and plays an important roleas a resistant mechanism to EGFR TKI treatment. Signalingthrough the IGF-1R is required for neoplastic transformationby a number of oncogenes, and therefore makes IGF-1R anattractive target for anticancer treatment [32]. Figitumumab, aneutralizing IGF-1R antibody, has been examined in a NSCLCphase III study [33]. Both tissue- and serum-based IGF-1pathway-related proteins, including IGF-I and IGF-I bindingproteins, are included for study as potential biomarkers forresistance to EGFR TKIs and sensitivity to IGF-1R inhibitors.Matei et al. examined b-Raf and ERK in ovarian cancers, andphosphorylated (p)-ERK in peripheral blood lymphocyte (PBL)to evaluate response prediction for sorafenib, a drug targetingc-Raf and VEGFR2. Protein quantities of the logical down-stream or related targets, ERK and b-Raf and pretreatment
pERK in PBLs, were not associated with tumor response orsurvival. But, high on-treatment pERK levels on RPPA wereassociated with better tumor response and lower risk of tumorprogression in treated patients. This is exploratory evidencethat these could be applied as surrogate markers of sorafenibactivity [34]. Our group independently demonstrated thatsorafenib reduced pERK quantity in tumor tissue from solidtumor patients taking sorafenib. We showed this wasassociated with improved clinical benefit; other descriptivebiomarkers related to the activity of sorafenib were identified(Azad and Kohn [35], and manuscript in preparation). Thus,examination of the biology of the drug resistance would offerthe opportunity of new insights of the biology of treatmentresistance for future clinical benefit.
7. Identification of biomarkers as therapeutictargets
Identification of biomarkers and potential drug targets hasbeen approached via both an unbiased high throughput andselective protein analyses. High throughput MS with se-rum and tissues yielded high sensitivity and specificity inidentification of multiple diagnostic protein signatures [36].Bateman et al. analyzed microdissected cancer epithelial cellsderived from 25 breast cancer patients using liquid chroma-tography (LC)−/MS. Comparative analysis of stage 0 and stageIII patients revealed 113 proteins that significantly differ-entiated between these groups. Known factors associatedwithdisease pathogenesis, such as CDH1 and CTNNB1, as well asthose previously implicated in breast cancer, such as TSP-1,were identified [37]. These data uncovered new protein can-didates indicative of disease stage and recurrence in breastcancer warranting further investigation for diagnostic utility

Table 2 – Four criteria and examples for credentialingtherapeutic targets.
Criteria Examples
The target was present. Rheumatoid arthritis [70] TNFαoverexpression was present andwas etiologic in driving localinflammation and tissue destruction
The target was activated. Crohn's disease [44] TNFαoverexpression was a driving event.
The target was altered bythe intervention.
Ovarian cancer [34] Ras/Raf/ERKpathway was altered by sorafenib,a c-RAF kinase inhibitor.
The target alteration wasassociated with theclinical outcome.
Breast cancer [6] HER2 amplificationwas associated with improved survivalby trastuzumab, an anti-HER2neutralizing antibody.
2637J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
and as potential targets. An examplewhere this progression ofevents has occurred is the development of mesothelin as ascreening diagnostic, a biomarker, and as a molecular targetfor successful drug development. Mesothelin is overexpressedin mesothelioma, and pancreatic, lung, and ovarian cancers[38]. Although mesothelin was initially identified throughglobal gene profiling, all subsequent studies were done inselective proteome-basedmethods, as an immunohistochem-ical marker in tumors, and with serum mesothelin measuredin ELISA or bead based immunoassay [39]. It has beendemonstrated to be positively interactive with CA125 in thediagnostics of ovarian cancer [40], and shown recently to bea biological binding partner of CA125 [41]. Mesothelin wassubsequently examined as a potential druggable target,resulting in the successful development of an anti-mesothelinimmunotoxin, SS1P [42], and a neutralizing monoclonalantibody, amatuximab (MORAb009) [43]. Therapeutic benefithas been reported for both as treatment for patients withmesothelin-expressing tumors.
Introduction of targeted therapies, also called biologicaltherapies or biologics, into cancer therapy and therapy ofother diseases, such as psoriasis and rheumatoid arthritis(RA), are the result of focused drug development derived fromnew understanding of the underlying pathophysiology.Agents used in biological therapy include biological productsthat regulate the immune system, e.g. vaccines are nowtermed immunotherapies. In many situations, it has meant amarkedly different approach to treatment, displacing tradi-tional cytotoxic chemotherapy in cancer, and steroids, anti-malarials, and gold in RA. However, early application of thesebiologics has not been promising in all clinical venues,including in treatment of some solid tumors. This may bedue to indiscriminant application of biologics to all patientswith a general cancer subtype diagnosis. We now know, aswith the many types of arthritis, that there are phenotypicallysimilar cancers belong to different molecular subsets ofdisease. The cancers in the different subsets may have dif-ferent driving molecular events. This could lead to an under-appreciation of potentially beneficial agents when the agentsare applied indiscriminately across all subtypes. Furtherdevelopment of biomarker application in trial design mayimprove clinical outcome, require fewer patients for analysis,and perhaps yield stronger results.
8. Criteria for development of validatedtherapeutic targets in clinical trials
Discovery, verification, and validation of reliable biomarkersare necessary in this time of ever more complex disease inorder to optimally qualify drugs and their targets. Four criteriashould be realized in clinical credentialing of a target (Table 2)in order to result in successful targeted therapy where thebiological drive is known. Simply, these include demonstra-tion of target against which the drug is focused, documenta-tion that the target is active, that the agent affects its target,and that this translates into clinical benefit. For example, if apro-inflammatory driving event is defined to due to activationof the TNFα protein signaling network, neutralizing antibodiesto the TNFα axis should be successful [44,45]. In clinic,
infliximab and other monoclonal antibodies targeting TNFαhave shown efficacy in inducing andmaintaining remission inpatients with Crohn's disease [44]. This example shows wherethe application of proteomics aided in the elucidation ofdisease of mechanism can be translated into clinical applica-tion. Incorporation of mechanism criteria into developmentand design will maintain focus on identification of clinicallyuseful targets and biomarkers and should improve lead agentselection and clinical advancement.
Oncology is one of the most active new areas of targeteddrug and biomarker development. HER2 is a successful targetwhere all four criteria are satisfied by three FDA-approvedagents, trastuzumab, pertuzumab, and lapatinib [6,46]. Here, itis proven that when HER2 is amplified in most cases, it also isactivated. The agents inhibit this activation and have beenshown to be clinically valuable. However, few trials are beingconducted to evaluate selective targets or general proteomicprofiling to date. Additional trials are necessary to develop theknowledge required to optimally direct biomarker and thera-peutic development. While HER2 is regarded as perhaps themost successful of the molecular targets, there are manybiochemical signaling eventswaiting to bemined in the tumormicroenvironment.
There are also examples in oncology for which the criteriaof presence and activation of target are fulfilled, but no clinicalactivity of a therapeutic target was observed. Evaluation ofthe criteria using proteomics in prospectively collected clinicalsamples allowed examination of why targeted therapieshave not result in clinical benefit. EGFR is overexpressed inapproximately 50% of ovarian cancer [47] and some studiesshowed over-expression of EGFR correlated with poor prog-nosis in advanced stage ovarian cancer patients [48–50].However, targeted inhibition of the prognostic factor, EGFR,has not resulted in patient benefit. This is an example whereprognostic factors may be neither predictive nor sufficient fortherapeutic targeting. Posadas et al. reported that treat-ment with the EGFR inhibitor, gefitinib, lacked clinical ben-efit in ovarian cancer [51]. RPPA evaluation of paired biopsiesobtained prior to gefitinib treatment and after one monthdemonstrated drug-associated reduction of phosphoryla-tion of c-kit and EGFR, and these changes correlated withtreatment-induced GI toxicity, indicating a pharamcodynamiclink [52]. A follow-on phase II clinical trial of vandetanib, an

2638 J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
inhibitor of both EGFR and VEGFR2 also was negative [53]. Itwas designed to examine on-target effects of both EGFR andVEGFR2. RPPA analysis of paired biopsies again showed EGFRactivation was inhibited, but inhibition of VEGFR activationwas not observed. The clinical pharmacodynamic effects alsoindicated EGFR inhibition without activity against VEGFR2.These data reinforced the lack of a therapeutically importantEGFR drive in ovarian cancer. Further proteomic examinationof the tissue could identify other activated signaling events forsubsequent targeting.
Angiogenesis is a targetable event of particular interest[54]. A dose escalation and proof of mechanism study inpatients with solid tumors tested the combination of sorafe-nib, a c-Raf kinase inhibitor, with the neutralizing anti-VEGFmonoclonal antibody, bevacizumab. This phase I studyincorporated a novel design for drug exposure and acquisitionof tumor samples for proteomic endpoint analysis. Patientswere randomized to receive monotherapy for the firstmonth, bracketed by collection of tumor tissue and bloodand functional imaging; combination therapy was initiatedwith the second month and included an additional biopsyand set of imaging. RPPA was used to examine tissue proteinendpoints. The results indicated on-target effects for bothdrugs when used alone: reduction in activated ERK bysorafenib, and angiogenesis inhibition by bevacizumab (Azadand Kohn [35,55], and manuscript in preparation). This studyshowed the molecularly targeted combination of sorafeniband bevacizumab is biologically active in an on-target fashionwith promising clinical activity in recurrent epithelial ovariancancer patients [56]. The exploratory imaging endpoints willbe examined as predictive biomarkers and the proteomicendpoints confirmed in a second. An understanding of theeffects of targeted therapeutics on signaling networks andcorrelated biomarkers is essential in order to guide subse-quent steps and registration trial design. Proteomics can yielda breadth of information from which to assess a given can-didate target. A key advance would be the ability to detectpresence or stage of disease and/or response to targetedtherapy through validated surrogate in blood or tissue bio-markers. The presence of such a bridge can rapidly triage alengthy list of lead biologic target candidates prior to investingexcess amount of time, money and hope of patients on thedevelopment of new drugs suitable for use in cancer therapy.
9. Biomarkers and targeted therapy in clinicaltrials for drug development
Drug development is typically divided into segments oflead compound identification, preclinical development, andclinical development. The entire process can cost billions ofdollars and is a narrow pyramid where few drugs make it tomarket. Strategies for patient stratification and personalizedmedicine must be developed, verified, and validated duringthe preclinical and clinical development phases. Early con-sideration of the biomarker/outcome/patient stratificationrelationship may shorten time to the clinic and improve costand time of drug development by allowing focused applicationof agent where they are most likely to succeed. Biomarkervalidation needs to be incorporated into optimal trial design,
with appropriate statistical power for those endpoints as well.Retrospective biomarker analyses may be fraught with sub-optimal power to discern an effect because of unavailablepatient specimens or inconsistent quality control of availablebiospecimens. Conversely, if marker-based analyses wereplanned prospectively pre- and during/post-treatment, andtissue specimens were available on all or most patients,adequate statistical power may remain with which tocompare the clinical outcome against the biomarker(s). Thebenefit of this approach is the ability to obtain new knowledgewith increasing likelihood of success.
Current clinical trials using proteomics for biomarkerdiscovery and/or evaluation are ongoing in many types ofcancers and other diseases. Recent technologies employingprotein microarrays such as RPPA has allowed for quantifica-tion of multiple endpoints in a high-throughput fashion.These endpoints include expression levels of key proteins andtheir activated forms that compose critical signaling nodesinvolved in proliferation, survival, and angiogenesis. Forexample, the PI3K pathway has been shown to be a drivingpathway in subsets of serous ovarian cancer due to a commonsomatic gain-of-function mutation on chromosome 3p inPI3KCA, described above for lung cancer and occurringcommonly in a variety of solid tumors. Molecular activationof PI3K drives the Akt pathway, yielding a strong survivalsignal [57]. Agents against PI3K itself and its protein effectorsAkt andmTOR are now in clinical investigation in ovarian andother cancers [58,59]. Proteomic assays are being applied toevaluate modulation of PI3K/AKT/mTOR pathway [60–62].
There are other pathways downstream of receptor tyrosinekinase (RTK)s, in addition to the PI3K/AKT pathway, for whichtherapeutics have been developed and proteomic endpointscan be analyzed. Most are downstream signals from RTKs andintegrins via the Src/Ras/Raf/MEK pathway. The mitogen-activated protein kinase, MEK, and its effector, ERK, is onesuch RTK downstream target. Knowledge of these down-stream pathway protein targets also facilitates agent selec-tion. Application of pathway dissection has led to an ongoingphase II collaborative study of the MEK inhibitor, AZD6244, inmultiple myeloma (NCT00551070). Annunziata et al. demon-strated MAF oncogene upregulation in 30% of multiplemyeloma cases occurring through MEK-ERK regulation ofMAF transcription. Subsequent MEK inhibition induced apo-ptosis selectively in MAF-expressing myelomas [63]. Thisstudy provided the proof of concept of MEK/ERK/MAF as atarget for therapeutic intervention in multiple myeloma [64]leading to the present trial. Genomic analysis of MAF may notbe necessary if activation of MEK and ERK is demonstrated tobe predictive for response. These studies hint at a promisethat proteomic markers can be identified and used to guideselecting and developing drugs in cancer.
10. Linking proteomics and genomics data fordrug development
Several validated molecular tests performed in tumor tissueor assessing the patient's genome are now part of standardtherapeutic decision making in breast, colorectal, and lungcancers [6,11,28]. Another successful example of biomarkers

2639J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
by genomics is the development of imatinib mesylate.Imatinib inhibits the BCR-ABL fusion protein translocation,c-KIT mutation, and platelet derived growth factor receptor(PDGFR). This molecular-targeted drug is highly efficacious inchronic myeloid leukemia [65] [66] and gastrointestinalstromal tumor [67]. These genomic changes provided both apredictive biomarker and a therapeutic target for this ratio-nally designed small molecule. Many genetic events translateinto definable proteomic changes; linking genomic andproteomic data for biomarker and a therapeutic target at theprotein level is ongoing in many fields. These proteomicsanalyses will provide predictive molecular marker(s) for thetargeted drug to apply to therapeutic decision-making.Clinical trials are underway at multiple institutions analyzingthe value of proteomics data in clinical decisions [68].
A recently presented phase II study [69], BATTLE (biomark-er-integrated approaches of targeted therapy for lung cancerelimination; NCT00409968), demonstrated that biomarkertailored targeted lung cancer treatments may improve patientoutcome. This study identified subgroups of patients withadvanced NSCLC who were more likely to benefit from aspecific agent(s) based on biomarker analyses done usingfresh tissue biopsies. Overall, it did not yield a dramaticclinical benefit, 46% of patients had stable disease or partialresponse after 8 weeks of treatment with a median overallsurvival 9 months compared with 30% on traditional chemo-therapy for advanced NSCLC. However, this example demon-strates progress has been made in stratifying patients basedon biomarkers who will benefit from the biomarker-defineddrugs. Thus, comprehensive proteomic and genomic profilingfor advanced cancers shows promise in addressing the goalsof predictive biomarkers for effective and targeted patient andtherapy selections.
11. Future direction of biomarker, proteomicsfor drug development
Incorporating proteomics and biomarkers into clinical trialsremains an important direction for drug development. Assayverification and biological validation remain critical forconfidence in application of biomarkers and new targetidentification. Rigorous peer reviewed data and approvalshould be required for best patient safety and benefit, andcost/benefit, minimizing general application of assays. Verifi-cation and validation of tests will be a key step in maximizingthe clinical and commercial success of a biomarker. Suchvalidated biomarkers may yield clean selection criteria fordefined subsets of patients susceptible to specific targetedtherapies. In the future, proteomics can be applied to identifyoptimally targeted agent(s) and biologically effectivedose(s) foreach patient's disease, allowing for the monitoring of responseand relapse, and engineering of new drugs and strategies tocircumvent resistance mechanisms. Comprehensive systemsbiology proteomic approaches applied to cancers will bothhelp the patient and tumor community. This also will create acomprehensive database of information pairing genomicchange with proteomic expression with agents that maysuccessfully target that proteomic drive. Organized studies areneeded in order to initiate this direction.
Such is the biomarker strategy-based prospective clinicaltrial design conducted by Mills and colleagues. The “T9” (TenThousand Tumors Ten Thousand Tests Ten Thousand Thera-pies) project will test with genomic and proteomic technologiesthe tumors of 10,000 patientswith relapsed refractory cancer forwhom are at high risk for recurrence with no therapeuticstandard of care. These results will be applied towardsidentification of best treatment considerations. This trial wasdesigned prospectively to develop an atlas of mutation and co-mutations in patients entering clinical trials and to developcohorts of patients with rare gene aberrations. It will helpassociate these mutations and co-mutations with clinicaloutcomes and allow evaluation of molecular evolution inmetastases and due to treatment. Unlike other foundation orcommercial approaches that are available, this is designed as aprospective clinical trial, presenting the investigative compo-nent and optimizing informed consent. This example project ispositioned on the backbone of genomic change; the findings tobe applied clinically are those that alter the protein target andtheprotein signaling pathway and are organized to evaluate thereliability of individualized treatment decision making.
12. Conclusions
Emerging proteomic technology is being applied to help selectpatients who may be more likely to benefit from targetedtherapies and will bring to reality the clinical adoption ofmolecular proteomic stratification. Comprehensive proteomicprofiling and trial-focused endpoint profiling will be critical fordevelopment of biomarkers and potential drug targets. Proteo-mics will help dissect these protein signaling pathways to definethe preferable targets of molecular therapy. Incorporatingtranslational endpoints of preplanned biologic correlates in aprospective validation study remains an important method toguide future direction of proteomics. The discovery of novel,validatedbiomarkersignatureswill broadenourunderstandingofthe disease and will lead to development of new potential drugsfor more effective targeted therapy in recurrent cancers. Theseevents will guide future directions of proteomics as a tool of newbiomarker and drug discovery in cancer and other diseases.
Acknowledgement
This work was supported by the Intramural Program of theCenter for Cancer Research, National Cancer Institute, USA.
R E F E R E N C E S
[1] AtkinsonAJCW,DeGruttolaV,DeMetsDL,DowningGJ,HothDF,Oates JA, et al. Biomarkers and Surrogate Endpoints: PreferredDefinitions and Conceptual Framework. Clin Pharmacol Ther2001;69:89–95.
[2] Simon R, Altman DG. Statistical aspects of prognostic factorstudies in oncology. Br J Cancer 1994;69:979–85.
[3] Sargent DJ, Conley BA, Allegra C, Collette L. Clinical trialdesigns for predictive marker validation in cancer treatmenttrials. J Clin Oncol 2005;23:2020–7.

2640 J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
[4] Dent R, Trudeau M, Pritchard KI, Dent R, Trudeau M,Pritchard KI, et al. Triple-negative breast cancer: clinicalfeatures and patterns of recurrence. Clin Cancer Res 2007;13:4429–34.
[5] Paik S, Hazan R, Fisher ER, Sass RE, Fisher B, Redmond C, et al.Pathologic findings from the National Surgical AdjuvantBreast and Bowel Project: prognostic significance of erbB-2protein overexpression in primary breast cancer. J Clin Oncol1990;8:103–12.
[6] Hudis CA. Trastuzumab–mechanism of action and use inclinical practice. N Engl J Med 2007;357:39–51.
[7] Allingham-Hawkins D, Lea A, Levine S. ERCC1 ExpressionAnalysis to Guide Therapy in Non-Small Cell Lung Cancer.PLoS Curr 2010;2:RRN1202.
[8] Olaussen KA, Dunant A, Fouret P, Brambilla E, André F,Haddad V, et al. DNA repair by ERCC1 in non-small-cell lungcancer and cisplatin-based adjuvant chemotherapy. N Engl JMed 2006;355:983–91.
[9] Olaussen KA, Mountzios G, Soria JC. ERCC1 as a risk stratifierin platinum-based chemotherapy for nonsmall-cell lungcancer. Curr Opin Pulm Med 2007;13:284–9.
[10] CoboM, Isla D, Massuti B, Montes A, Sanchez JM, Provencio M,et al. Customizing cisplatin based on quantitative excisionrepair cross-complementing 1 mRNA expression: a phase IIItrial in non-small-cell lung cancer. J Clin Oncol 2007;25:2747–54.
[11] Karapetis CS, Khambata-Ford S, Jonker DJ, O'Callaghan CJ, TuD, Tebbutt NC, et al. K-ras mutations and benefit fromcetuximab in advanced colorectal cancer. N Engl J Med2008;359:1757–65.
[12] Denkert C, Budczies J, Kind T, Weichert W, Tablack P, SehouliJ, et al. Mass spectrometry-based metabolic profiling revealsdifferent metabolite patterns in invasive ovarian carcinomasand ovarian borderline tumors. Cancer Res 2006;66:10795–804.
[13] Lemaire R, Menguellet SA, Stauber J, Marchaudon V, Lucot JP,Collinet P, et al. Specific MALDI imaging and profiling forbiomarker hunting and validation: fragment of the 11Sproteasome activator complex, Reg alpha fragment, is a newpotential ovary cancer biomarker. J Proteome Res 2007;6:4127–34.
[14] Sheehan KM, Calvert VS, Kay EW, Lu Y, Fishman D, Espina V,et al. Use of reverse phase protein microarrays and referencestandard development for molecular network analysis ofmetastatic ovarian carcinoma. Mol Cell Proteomics 2005;4:346–55.
[15] Winters M, Dabir B, Yu M, Kohn EC. Constitution and quantityof lysis buffer alters outcome of reverse phase proteinmicroarrays. Proteomics 2007;7:4066–8.
[16] Tchabo NE, Liel MS, Kohn EC. Applying proteomics in clinicaltrials: assessing the potential and practical limitations inovarian cancer. Am J Pharmacogenomics 2005;5:141–8.
[17] Carey MS, Agarwal R, Gilks B, Swenerton K, Kalloger S, SantosJ, et al. Functional proteomic analysis of advanced serousovarian cancer using reverse phase protein array: TGF-betapathway signaling indicates response to primarychemotherapy. Clin Cancer Res 2010;16:2852–60.
[18] Frederick MJ, VanMeter AJ, Gadhikar MA, Henderson YC, YaoH, Pickering CC, et al. Phosphoproteomic analysis of signalingpathways in head and neck squamous cell carcinoma patientsamples. Am J Pathol 2011;178:548–71.
[19] Singh B, Stoffel A, Gogineni S, Poluri A, Pfister DG, Shaha AR,et al. Amplification of the 3q26.3 locus is associated withprogression to invasive cancer and is a negative prognosticfactor in head and neck squamous cell carcinomas. Am JPathol 2002;161:365–71.
[20] Marrer E, Dieterle F. Promises of biomarkers in drugdevelopment–a reality check. Chem Biol Drug Des 2007;69:381–94.
[21] Romond EH, Perez EA, Bryant J, Suman VJ, Geyer Jr CE,Davidson NE, et al. N Engl J Med 2005;353:1673–84.
[22] Brenner DE, Normolle DP. Biomarkers for cancer risk, earlydetection, and prognosis: the validation conundrum. CancerEpidemiol Biomarkers Prev 2007;16:1918–20.
[23] Chau CH, Rixe O, McLeod H, Figg WD. Validation of analyticmethods for biomarkers used in drug development. ClinCancer Res 2008;14:5967–76.
[24] Wagner JA. Overview of biomarkers and surrogate endpointsin drug development. Dis Markers 2002;18:41–6.
[25] Pepe MS, Etzioni R, Feng Z, Potter JD, Thompson ML,Thornquist M, et al. Phases of biomarker development forearly detection of cancer. J Natl Cancer Inst 2001;93:1054–61.
[26] Flaherty KT, Puzanov I, Kim KB, Ribas A, McArthur GA,Sosman JA, et al. Inhibition of mutated, activated BRAF inmetastatic melanoma. N Engl J Med 2010;363:809–19.
[27] Rayson D, Richel D, Chia S, Jackisch C, van der Vegt S,Suter T. Anthracycline-trastuzumab regimens forHER2/neu-overexpressing breast cancer: current experienceand future strategies. Ann Oncol 2008;19:1530–9.
[28] Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, OkimotoRA, Brannigan BW, et al. Activating mutations in theepidermal growth factor receptor underlying responsivenessof non-small-cell lung cancer to gefitinib. N Engl J Med2004;350:2129–39.
[29] Hirsch FR, Varella-Garcia M, Bunn Jr PA, Franklin WA,Dziadziuszko R, Thatcher N, et al. Molecular predictors ofoutcome with gefitinib in a phase III placebo-controlled studyin advanced non-small-cell lung cancer. J Clin Oncol 2006;24:5034–42.
[30] Tsao MS, Sakurada A, Cutz JC, Zhu CQ, Kamel-Reid S, Squire J,et al. Erlotinib in lung cancer - molecular and clinicalpredictors of outcome. N Engl J Med 2005;353:133–44.
[31] Hirsch FR, Herbst RS, Olsen C, Chansky K, Crowley J, Kelly K,et al. Increased EGFR gene copy number detected byfluorescent in situ hybridization predicts outcome innon-small-cell lung cancer patients treated with cetuximaband chemotherapy. J Clin Oncol 2008;26:3351–7.
[32] Zha J, Lackner MR. Targeting the insulin-like growth factorreceptor-1R pathway for cancer therapy. Clin Cancer Res2010;16:2512–7.
[33] Jassem J, Langer CJ, Karp DD, Mok T, Benner RJ, Green SJ, et al.Randomized, open label, phase III trial of figitumumab incombinationwith paclitaxel and carboplatin versus paclitaxeland carboplatin in patients with non-small cell lung cancer(NSCLC). J Clin Oncol 2010;28:15s suppl;abstr7500.
[34] Matei D, Sill MW, Lankes HA, DeGeest K, Bristow RE, Mutch D,et al. Activity of Sorafenib in Recurrent Ovarian Cancer andPrimary Peritoneal Carcinomatosis: A Gynecologic OncologyGroup Trial. J Clin Oncol 2011;29(1):69–75.
[35] Azad NS, MY RH, Davidson B, FiggWD, Calvo K, Venkatasen A,et al. Translational proof of mechanism (PoM) for sorafenibwith bevacizumab: Endpoint analysis and clinical activity.J Clin Oncol 2009;27 abst3574.
[36] Hood BL, Stewart NA, Conrads TP. Development ofhigh-throughput mass spectrometry-based approaches forcancer biomarker discovery and implementation. Clin LabMed 2009;29:115–38.
[37] Bateman NW, Sun M, Bhargava R, Hood BL, Darfler MM,Kovatich AJ, et al. Differential Proteomic Analysis ofLate-Stage and Recurrent Breast Cancer from Formalin-FixedParaffin-Embedded Tissues. J Proteome Res 2011;10(3):1323–32.
[38] Hassan R, Bera T, Pastan I. Mesothelin: a new target forimmunotherapy. Clin Cancer Res 2004;10:3937–42.
[39] Shah CA, Lowe KA, Paley P, Wallace E, Anderson GL, McIntoshMW, et al. Influence of ovarian cancer risk status on thediagnostic performance of the serum biomarkers mesothelin,

2641J O U R N A L O F P R O T E O M I C S 7 4 ( 2 0 1 1 ) 2 6 3 2 – 2 6 4 1
HE4, and CA125. Cancer Epidemiol Biomarkers Prev 2009;18:1365–72.
[40] McIntosh MW, Drescher C, Karlan B, Scholler N, Urban N,Hellstrom KE, et al. Combining CA 125 and SMR serummarkers for diagnosis and early detection of ovariancarcinoma. Gynecol Oncol 2004;95:9–15.
[41] Kaneko O, Gong L, Zhang J, Hansen JK, Hassan R, Lee B, et al. Abinding domain onmesothelin for CA125/MUC16. J Biol Chem2009;284:3739–49.
[42] Hassan R, Bullock S, Premkumar A, Kreitman RJ, Kindler H,Willingham MC, et al. Phase I study of SS1P, a recombinantanti-mesothelin immunotoxin given as a bolus I.V. infusionto patients with mesothelin-expressing mesothelioma,ovarian, and pancreatic cancers. Clin Cancer Res 2007;13:5144–9.
[43] Hassan R, Cohen SJ, Phillips M, Pastan I, Sharon E, Kelly RJ,et al. Phase I Clinical Trial of the Chimeric Anti-MesothelinMonoclonal AntibodyMORAb-009 in Patients withMesothelinExpressing Cancers. Clin Cancer Res 2010;16(24):6132–8.
[44] Colombel JF, Sandborn WJ, Reinisch W, Mantzaris GJ,Kornbluth A, Rachmilewitz D, et al. Infliximab, azathioprine,or combination therapy for Crohn's disease. N Engl J Med2010;362:1383–95.
[45] Maini RN, Elliott MJ, Brennan FM, Williams RO, Chu CQ,Paleolog E, et al. Monoclonal anti-TNF alpha antibody as aprobe of pathogenesis and therapy of rheumatoid disease.Immunol Rev 1995;144:195–223.
[46] Baselga J, GelmonKA,VermaS,WardleyA,Conte P,MilesD, et al.Phase II trial of pertuzumab and trastuzumab in patients withhuman epidermal growth factor receptor 2-positive metastaticbreast cancer that progressed during prior trastuzumab therapy.J Clin Oncol 2010;28:1138–44.
[47] Ilekis JV, Connor JP, Prins GS, Ferrer K, Niederberger C,Scoccia B. Expression of epidermal growth factor andandrogen receptors in ovarian cancer. Gynecol Oncol1997;66:250–4.
[48] Psyrri A, Kassar M, Yu Z, Bamias A, Weinberger PM, MarkakisS, et al. Effect of epidermal growth factor receptor expressionlevel on survival in patients with epithelial ovarian cancer.Clin Cancer Res 2005;11:8637–43.
[49] Niikura H, Sasano H, Sato S, Yajima A. Expression ofepidermal growth factor-related proteins and epidermalgrowth factor receptor in common epithelial ovarian tumors.Int J Gynecol Pathol 1997;16:60–8.
[50] Sewell JM, Macleod KG, Ritchie A, Smyth JF, Langdon SP.Targeting the EGF receptor in ovarian cancer with thetyrosine kinase inhibitor ZD 1839 (“Iressa"). Br J Cancer2002;86:456–62.
[51] Posadas EM, Liel MS, Kwitkowski V, Minasian L, Godwin AK,Hussain MM, et al. A phase II and pharmacodynamic study ofgefitinib in patients with refractory or recurrent epithelialovarian cancer. Cancer 2007;109:1323–30.
[52] Posadas EM, Kwitkowski V, Kotz HL, Espina V, Minasian L,Tchabo N, et al. A prospective analysis of imatinib-inducedc-KIT modulation in ovarian cancer: a phase II clinicalstudy with proteomic profiling. Cancer 2007;110:309–17.
[53] Annunziata CM, Walker AJ, Minasian L, Yu M, Kotz H, WoodBJ, et al. Vandetanib, designed to inhibit VEGFR2 and EGFRsignaling, had no clinical activity as monotherapy forrecurrent ovarian cancer and no detectable modulation ofVEGFR2. Clin Cancer Res 2010;16:664–72.
[54] Kerbel R, Folkman J. Clinical translation of angiogenesisinhibitors. Nat Rev Cancer 2002;2:727–39.
[55] Azad NS, EMP, Kwitkowski VE, Annunziata CM, Barrett T,Premkumar A, Kotz HL, et al. Increased efficacy and toxicitywith combination anti-VEGF therapy using sorafenib andbevacizumab. J Clin Oncol 2006;24:18s (suppl;abstr:3004).
[56] Lee JM, Sarosy GA, Annunziata CM, Azad N, Minasian L, KotzH, et al. Combination therapy: intermittent sorafenib withbevacizumab yields activity and decreased toxicity. Br JCancer 2010;102:495–9.
[57] Shayesteh L, Lu Y, Kuo WL, Baldocchi R, Godfrey T, Collins C,et al. PIK3CA is implicated as an oncogene in ovarian cancer.Nat Genet 1999;21:99–102.
[58] Gonzalez-Angulo AM, Hennessy BT, Mills GB. Future ofpersonalized medicine in oncology: a systems biologyapproach. J Clin Oncol 2010;28:2777–83.
[59] Kornblau SM, Tibes R, Qiu YH, Chen W, Kantarjian HM,Andreeff M, et al. Functional proteomic profiling of AMLpredicts response and survival. Blood 2009;113:154–64.
[60] NanjundanM, Byers LA, Carey MS, Siwak DR, Raso MG, Diao L,et al. Proteomic profiling identifies pathways dysregulated innon-small cell lung cancer and an inverse association ofAMPK and adhesion pathways with recurrence. J ThoracOncol 2010;5:1894–904.
[61] Murph MM, Smith DL, Hennessy B, Lu Y, Joy C, Coombes KR,et al. Individualized molecular medicine: linking functionalproteomics to select therapeutics targeting the PI3K pathwayfor specific patients. Adv Exp Med Biol 2008;622:183–95.
[62] Stemke-Hale K, Gonzalez-Angulo AM, Lluch A, Neve RM, KuoWL, Davies M, et al. An integrative genomic and proteomicanalysis of PIK3CA, PTEN, and AKT mutations in breastcancer. Cancer Res 2008;68:6084–91.
[63] Bergsagel PL, Kuehl WM. Molecular pathogenesis and aconsequent classification of multiple myeloma. J Clin Oncol2005;23:6333–8.
[64] Annunziata CM, Hernandez L, Davis RE, Zingone A, Lamy L,Lam LT, et al. A mechanistic rationale for MEK inhibitortherapy in myeloma based on blockade of MAF oncogeneexpression. Blood 2010.
[65] Druker BJ, Talpaz M, Resta DJ, Peng B, Buchdunger E, Ford JM,et al. Efficacy and safety of a specific inhibitor of the BCR-ABLtyrosine kinase in chronic myeloid leukemia. N Engl J Med2001;344:1031–7.
[66] Druker BJ, Sawyers CL, Kantarjian H, Resta DJ, Reese SF, FordJM, et al. Activity of a specific inhibitor of the BCR-ABLtyrosine kinase in the blast crisis of chronicmyeloid leukemiaand acute lymphoblastic leukemia with the Philadelphiachromosome. N Engl J Med 2001;344:1038–42.
[67] Demetri GD, von Mehren M, Blanke CD, Van den Abbeele AD,Eisenberg B, Roberts PJ, et al. Efficacy and safety of imatinibmesylate in advanced gastrointestinal stromal tumors. N EnglJ Med 2002;347:472–80.
[68] Pao W, Kris MG, Iafrate AJ, Ladanyi M, Jänne PA, Wistuba II,et al. Integration of molecular profiling into the lung cancerclinic. Clin Cancer Res 2009;15:5317–22.
[69] Edward S, Kim RSH, Jack Lee J, Blumenschein Jr George R, TsaoAnne, Alden Christine M, et al. The BATTLE trial(Biomarker-integrated Approaches of Targeted Therapy forLung Cancer Elimination): personalizing therapy for lungcancer. Proceedings of the 101st Annual Meeting of theAmerican Association for Cancer Research; 2010 Apr 17–20 ;Washington DC Philadelphia (PA); AACR;2010 Abstract LB-12010.
[70] Scott DL, Kingsley GH. Tumor necrosis factor inhibitors forrheumatoid arthritis. N Engl J Med 2006;355:704–12.