-
il
nn, U
ralia
Article history:
Accepted 15 January 2015
Keywords:ProprioceptionMusculoskeletal rehabilitation
Introduction: Proprioception can be impaired in gradual-onset
musculoskeletal pain disorders and
for assessment and interventions is of vital importance in
musculoskeletal rehabilitation. In Part 1 of this
of the spine and extremities. Reference is made to research
whereinterventions have been reported to demonstrate positive
effectson proprioception. A special focus is made on exercise
therapy.
ia, or force sense-built devices orare frequently
7; Docherty et al.,l., 2002; Dochertyrman et al., 2009),tting.
Researcherstests for the spineeveloped for some
and renement of clinical tests is needed.
2.1. Clinical apparatus
Goniometers, inclinometers, pressure sensors, and laser-pointers
are affordable and easy-to-use in a clinical context.There is also
scope for new affordable and accurate technology thatincludes
smartphones with built-in accelerometers and gyros,
* Corresponding author.
Contents lists availab
Manual T
w
Manual Therapy 20 (2015) 378e387E-mail address:
[email protected] (N.C. Clark).of clinical assessment
and intervention methods for proprioception body parts (e.g.
cervical spine) than others. Further developmenttrol.
Proprioception fullls roles in feedback and feedforwardsensorimotor
control and regulation of muscle stiffness, beingspecically
important for movement acuity, joint stability, co-ordination, and
balance. Cervical proprioception is uniquelyimportant for head-eye
co-ordination and movement control.Proprioception can be disturbed
in musculoskeletal disorders dueto pain, effusion, trauma, and
fatigue. A variety of assessment pro-cedures and interventions have
been developed to specically testand enhance proprioception,
respectively. We present an overview
measuring joint position sense (JPS), kinesthes(Roijezon et al.,
2015). In the laboratory, customexpensive computer-interfaced
equipmentemployed (Lephart et al., 1994; Borsa et al., 1991998;
Waddington et al., 2000; Callaghan et aand Arnold, 2008; Benjaminse
et al., 2009; Leabut are typically impracticable in the clinical
seand clinicians have attempted to develop clinicaland extremities,
although some tests are more dProprioception is essential for
well-adapted sensorimotor con- Clinical assessment of
proprioception should employ tests forAssessmentIntervention
1.
Introductionhttp://dx.doi.org/10.1016/j.math.2015.01.0091356-689X/
2015 Elsevier Ltd. All rights reserved.motor control, causes and
ndings of altered proprioception in musculoskeletal conditions, and
generalprinciples of assessment and interventions.Purpose: The aim
of this second part is to present specic methods for clinical
assessment and in-terventions to improve proprioception in the
spine and extremities.Implications: Clinical assessment of
proprioception can be performed using goniometers,
inclinometers,laser-pointers, and pressure sensors. Manual therapy,
taping, and bracing can immediately enhanceproprioception and
should be used to prepare for exercise interventions. Various types
of exercise (activejoint repositioning, force sense, co-ordination,
muscle performance, balance/unstable surface, plyo-metric, and
vibration training) should be employed for long-term enhancement of
proprioception.
2015 Elsevier Ltd. All rights reserved.
2. Clinical assessment of proprioceptionReceived in revised
form4 January 2015 two-part Masterclass we presented a theory-based
overview of the role of proprioception in sensori-Received 6
November 2014 following trauma. Understanding of the role of
proprioception in sensorimotor dysfunction and
methodsMasterclass
Proprioception in musculoskeletal rehabassessment and
intervention
Nicholas C. Clark a, *, Ulrik Roijezon b, Julia Treleavea School
of Sport, Health, and Applied Science, St Mary's University,
Twickenham, Londob Department of Health Sciences, Lule University
of Technology, Lule, Swedenc CCRE Spine, Division of Physiotherapy,
SHRS, University of Queensland, Brisbane, Aust
a r t i c l e i n f o a b s t r a c t
journal homepage: witation. Part 2: Clinical
c
nited Kingdomle at ScienceDirect
herapy
w.elsevier .com/math
-
camera systems such as the Kinect, the Wii Balance Board,
andother video-based technology.
2.2. Specic tests
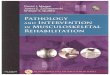
2.2.1. Joint position senseFor the cervical spine, active JPS
testing can use a laser-pointer
attached to a headband to determine patients' ability to
relocateto the neutral starting position with the eyes closed after
per-forming an active head movement (e.g. right rotation) (Fig. 1).
Thedifference between the starting and end position can be
measuredin millimetres, and the joint position error then
calculated in de-grees (Roren et al., 2009; Chen and Treleaven,
2013). This method isreliable and valid when compared to
sophisticated laboratoryequipment (Swait et al., 2007; Roren et
al., 2009; Chen andTreleaven, 2013). Errors greater than 4.5 are
considered to indi-cate abnormal cervical active JPS. Others have
used the cervicalrange of motion (CROM) device to measure cervical
active JPS andfound this to also be a reliable and valid method
(Wibault et al.,2013; Treleaven et al., 2015).
For the extremity joints, goniometers (universal, bubble,
digital)can also be used tomeasure active JPS. The sequence of
events is thesame as that described for laboratory measurement of
active JPS(see Masterclass Part 1) (Roijezon et al., 2015).
Depending on the
N.C. Clark et al. / Manual Thedevice used and the extremity
joint measured, reliability andmeasurement error of active movement
goniometry can rangewidely (Gabbe et al., 2004; Lephart et al.,
2007; Dickson et al., 2012;Kolber and Hanney, 2012; Hamid et al.,
2013), and this should becarefully considered if goniometry is used
to measure active JPS ofextremity joints. For the shoulder joint,
laser-pointer active JPStests have also been developed and
showpromise in thosewith andwithout shoulder injury (Balke et al.,
2011). There is potential forusing the laser-pointer to measure JPS
in other joints but, to date,there is limited research.
2.2.2. KinesthesiaFor the cervical spine, kinesthesia can be
assessed by following a
trace or intricate pattern as accurately as possible. This can
be avisual trace (e.g. gure-of-eight, zig-zag pattern) (Woodhouse
et al.,
Fig. 1. Cervical Joint Position Sense Assessment. The patient is
seated with the laserpointer attached to a headband, 90 cm from the
target. The target is adjusted so thatthe laser projects to the
centre of the target. They are asked to concentrate on thisresting
head position and then close the eyes. They then perform an active
movementto comfortable limits and return to the resting head
position as accurately as possible.
The difference between the initial and end position can be
measured in millimetresand then converted to degrees.2010) or by
following a computer generated marker that is movingin a more
unpredictable pattern (e.g. the y) (Kristjansson et al.,2004).
Outcome variables usually used here are the meandisplacement or
time on target. Advances in smart phone sensorshavemade the y
technologymore readily accessible to clinicians(Kristjannson,
2014), although recent work has also been con-ducted to investigate
the feasibility of a low cost quantitativemethod using video
analysis of the patient tracing a pattern with ahead-mounted laser
(Pereira et al., 2015).
2.2.3. Force senseForce sense can be measured by the accuracy of
reproducing a
specic target force. For example, the pressure biofeedback
deviceused for assessing the cranio-cervical exion test could
beconsidered a method of assessing force sense in the cervical
spine(Jull, 2000). The ability to hold steadily or the accuracy in
achievingand maintaining a desired pressure can be used. Others
have alsoused custom-made dynamometry placed at the mandible to
mea-sure precision and accuracy of maintaining low load upper
cervicalexor force levels (O'Leary et al., 2005).
2.3. Non-specic tests
2.3.1. Balance testsBalance tests, such as timed single-leg
stance tests, have his-
torically been used to measure lower extremity (e.g. ankle)
pro-prioception. As discussed previously (see Masterclass Part
1)(Roijezon et al., 2015), these tests are not specic tests of
proprio-ception since balance is a product of integrating sensory,
centralnervous system (CNS), and motor functions (Macpherson
andHorak, 2013). Nevertheless, balance tests could potentially give
anindication of improvement following proprioceptive training.
Bal-ance tests can be modied to try to bias proprioception by,
forexample, closing the eyes, adding neck torsion, or using
unstablesurfaces (Roijezon et al., 2015).
2.3.2. Oculomotor and eye-head coordination testsOculomotor and
eye-head co-ordination assessment in people
with neck pain is important as cervical spine afferents have
aunique and important role in maintaining eye and head
movementcontrol (Corneil et al., 2002; Peterson, 2004). At present,
clinicaltests incorporate qualitative assessment of the ability to:
1) main-tain gaze while moving the head; 2) co-ordinate eye and
headmovement; 3) eye follow while keeping the head still in neck
tor-sion compared to neck neutral positions (Fig. 2). Recent
researchhas found these clinical tests to be reliable and able to
discriminatebetween chronic neck pain and asymptomatic individuals
(DellaCasa et al., 2014), and are described in detail
elsewhere(Treleaven, 2008; Grip et al., 2009; Treleaven et al.,
2011).
3. Clinical interventions to improve proprioception
In Part 1 of this Masterclass (Roijezon et al., 2015), the
impor-tance of addressing causes of altered proprioception and
rehabili-tation techniques intended to enhance proprioception
wereintroduced. Pain, effusion, and fatigue can be common
aftermusculoskeletal injury, result in impaired
proprioception(Treleaven et al., 2003; Anderson and Wee, 2011; Cho
et al., 2011),and, consequently, are barriers against effective
interventions forenhancing proprioception and sensorimotor control.
Therefore, it isimportant to administer techniques to reduce pain,
effusion, andfatigue in order to facilitate the implementation of
effective in-terventions to enhance proprioception. Augmentation of
somato-sensory information via passive techniques such as
manual
rapy 20 (2015) 378e387 379therapy, soft tissue techniques, and
taping or bracing can be
-
Some researchers have reported that specic soft tissue
techniquescan signicantly and positively affect extremity joint
propriocep-tion dened by measures of active JPS (Henriksen et al.,
2004).
3.2. Taping and bracing
Taping and bracing techniques are adjunct interventions used
toobtain specic clinical effects including, for example, pain
relief,swelling control, and protect injured anatomical
structures(Macdonald, 2004). Another clinical goal of applying
athletic tape(Fig. 3) and different types of brace is to enhance
proprioception(Macdonald, 2004) via stimulation of mechanoreceptors
respond-ing to skin stretch and compression during joint motion
(Martinand Jessell, 1991; Rothwell, 1994). Authors have reported
that theapplication of selected athletic taping techniques, elastic
bandages,and neoprene sleeves can immediately and signicantly
enhancespinal and extremity proprioception in uninjured and injured
in-dividuals (Lephart et al., 1992; Jerosch et al., 1995; Jerosch
andPrymka, 1996; Simoneau et al., 1997; McNair and Heine,
1999;Newcomer et al., 2001; Callaghan et al., 2002; Chu et al.,
2002;Chang et al., 2010).
Therapy 20 (2015) 378e387N.C. Clark et al. / Manual380important.
Exercise therapy is a vital component in enhancingproprioception
and will be considered in detail. In order to deducethat a clinical
intervention yields a proprioceptive effect, one of thespecic
modalities of proprioception (JPS, kinesthesia, force sense)must be
measured before and after the intervention. The followingsections
will, therefore, refer only to research where this hasoccurred.
3.1. Manual therapy
Joint mobilisation/manipulation can create a controlled
stretchto capsuloligamentous tissue (Kaltenborn, 1999; Greenman,
2003),which is populated with multiple types of
mechanoreceptors(Kennedy et al., 1982; McLain and Raiszadeh, 1995;
Michelson andHutchins, 1995; Steinbeck et al., 2003; Moraes et al.,
2011), therebyaffecting proprioceptive feedback to the CNS. Authors
have re-ported that joint passive movement techniques can have an
im-mediate and signicantly benecial effect on spinal and
extremityproprioception (Heikkila et al., 2000; Vicenzino et al.,
2005;Palmgren et al., 2006; Learman et al., 2009; Ju et al., 2010;
Haavikand Murphy, 2011). Similarly, soft tissue techniques
including awide variety of body segment massage and localized
connectivetissue techniques mechanically affect the skin,
connective tissue(e.g. fascia), and muscles (Goats and Keir, 1991;
Goats, 1994;Greenman, 2003), which are also richly innervated with
mecha-noreceptors (Yahia et al., 1992; Rothwell, 1994; Stecco et
al., 2007).
Fig. 2. Eye Follow in Neck Torsion. The patient keeps the head
still while followingwith the eyes as accurately as possible a
moving target (e.g. or a pen) with the eyes.The target is moved
slowly side to side (20 per second through a visual angle of
40).The test is repeated with the neck in torsion (head still but
with the trunk rotated up to45) then repeated on the opposite side.
Any difference noted in smooth eye follow(quick catch up eye
movements) in these positions compared to the neutral position
isnoted.Fig. 3. Proprioception Knee Taping Technique (Modied from
Callaghan et al., 2002).Copyright Nicholas Clark. Reproduced with
permission.
-
3.3. Exercise therapy
Any active exercise can be considered proprioceptive
trainingbecause it will generate a barrage of afferent impulses to
the CNSfrom joint and muscle-tendon mechanoreceptors (Clark
andHerrington, 2010; Clark and Lephart, 2015). Thus, active
exerciseswould seem a vital component in augmenting
proprioception(Perez et al., 2004; Lagerquist et al., 2012; Clark
and Lephart, 2015).There is, however, much overlap across the
potential purposes,goals, and clinical uses for any single
exercise. Terminology used inexercise therapy (e.g. proprioceptive
training, strength training)can mean different things to different
clinicians and researchers. Asingle exercise can result in multiple
different physiological andphysical adaptations in several body
systems. In general, exercisetherapy refers to the performance of
repeatedmovements as part ofa goal-directed training programme to
improve a physiological orphysical characteristic (Clark and
Lephart, 2015). For the purpose ofthis paper we offer simplistic
denitions according to the primarycharacteristics of the exercise
task, introduce basic concepts, offerselected clinical examples,
and present research reports on theeffect of an exercise type on
proprioception.
3.3.1. Active joint repositioning trainingObservation of injury
mechanisms suggests that there are spe-
head to a pre-determined target angle, or returning the head
asclosely as possible to the initial position after movement,
checkingaccuracy by opening the eyes (Revel et al., 1994). For the
extrem-ities, both open (Fig. 4) and closed kinetic chain exercises
can beemployed with emphasis on repositioning training
occurringwithin the specic range-of-motion associated with a
specicinjury type (Borsa et al., 1994; Lephart and Henry, 1996).
Headrepositioning training with eyes open and eyes closed has
beendemonstrated to improve cervical JPS patients with chronic
neckpain (Revel et al., 1994; Jull et al., 2007). For peripheral
joints,including the shoulder and knee, the addition of a low
externalload to a limb segment (5e10% bodyweight) signicantly
improvedthe accuracy of joint repositioning tasks in uninjured
individuals(Lamell-Sharp et al., 2002; Brindle et al., 2006; Suprak
et al., 2007).
3.3.2. Force sense trainingPerception of force and effort can be
trained by activating a
muscle or muscle group to a predetermined amount of force,
ormaintaining the same amount of force for a dened
period-of-time(e.g. 10 s) (Jull et al., 2007). Cranio-cervical exor
training using thepressure biofeedback unit (Fig. 5) has
demonstrated improvedprecision for maintaining a low level upper
cervical exion force inpeople with neck pain (O'Leary et al.,
2007), and improved forcepressure levels achieved in people with
cervicogenic headache (Jull
ointioce
N.C. Clark et al. / Manual Therapy 20 (2015) 378e387 381cic
points in a joint's range-of-motion at which a joint is at risk
ofinjury. For example, non-contact injuries occur between 9 and
22
plantarexion in the ankle (Mok et al., 2011), 10 and 60 exion
inthe knee (Koga et al., 2010), and at extremes of external
rotation inthe shoulder (Wassinger and Myers, 2011). This suggests
there maybe a position of vulnerability in a joint's
range-of-motion that maybe related to proprioceptive decits (Myers
and Lephart, 2000).Active joint repositioning training involves a
similar procedure tothat used in JPS testing: a starting
positon/angle and target posi-tion/angle are selected, and training
involves moving from oneposition to another as closely as possible,
holding each for a shortduration (e.g. 5 s) (Myers and Lephart,
2000; Suprak et al., 2007). Adifference between JPS testing and
training is that visual feedbackcan be permitted for how accurately
the task is performed. For thecervical spine, training can be
performed by actively moving the
Fig. 4. Shoulder Joint Active Repositioning Training. A target
angle that lies at a specic protation). A low external load is
added to the limb (e.g. 1 kg dumb-bell) to enhance propr0 external
rotation, and then eccentrically externally rotate as closely as
possible to the tar
and then concentrically return to the start position. This can
be performed with eyes openet al., 2002).
3.3.3. Co-ordination trainingCo-ordination is the process of
controlling the activation of
many different muscles so that they act together simultaneously
asa single functional unit (Gordon, 1991), and the process of
inte-grating different body parts in specic movement patterns
(Kent,2006). Co-ordination training has a different
connotationcompared to movements in other types of exercise
therapy. Weconsider co-ordination training to have primary emphasis
oncueing an individual to specically concentrate on very ne
aspectsof sequencing and linking multiple muscles and/or
body-parts. Co-ordination training, thus, requires precise verbal
cueing for theclinician and a high cognitive demand for the
patient. Examples ofco-ordination training are preferential
activation of one muscle
within the range-of-motion associated with shoulder injury is
chosen (e.g. 80 externalption via increased mechanoreceptor
stimulation. The individual is instructed to start at
get angle, isometrically hold for up to ve seconds, concentrate
on feeling the position,or eyes closed. Copyright Nicholas Clark.
Reproduced with permission.
-
in uninjured military cadets (Rogol et al., 1998). General
ankleanisometric elastic resistance strength training was reported
tosignicantly enhance ankle inversion and plantarexion active JPSin
athletes with functional ankle instability (Docherty et al.,
1998),
Fig. 6. Side-Lying Loaded Ankle Eversion. An external load is
added to the foot (e.g. 2kg ankle-weight). The individual is then
instructed to perform dynamic eversionagainst gravity. Traditional
resistance training programme design methods are applied(e.g. 3
sets 10 repetitions, 3 sessions per week). Copyright Nicholas
Clark.Reproduced with permission.
Theversus another muscle within a synergistic muscle group (Jull
et al.,2007), specic eye-head-neck co-ordination during neck
move-ments (Revel et al., 1994; Humphreys and Irgens, 2002), and
foot-shank-thigh co-ordination on an elliptical training device
(Leeet al., 2014). Different types of co-ordination training
haveenhanced proprioception of the spine and extremities.
Cranio-cervical exor training focusing on use of the deep upper
cervicalexors versus the supercial cervical exors can
signicantlyenhance cervical active JPS in people with neck pain
(Jull et al.,2007). Eye head neck co-ordination exercises
demonstratesimproved JPS in people with neck pain (Humphreys and
Irgens,2002). Fine foot orientation training during external
perturba-tions on an elliptical training device has been shown to
signicantlyimprove passive foot kinesthesia during full
weight-bearingmovements in uninjured adults (Lee et al., 2014).
Whole body co-ordination exercises including yoga and tai chi have
also demon-
Fig. 5. Force sense training using the pressure biofeedback unit
(PBU) in cranio-cervical exion training (CCFT). The patient is
given feedback of the force appliedduring the incremental stages of
CCFT (22e30 mmHg) from the PBU. Patients closetheir eyes during the
task and then open them to check they have reached theappropriate
level.
N.C. Clark et al. / Manual382strated improvements in
proprioception (Tsang and Hui-Chan,2003; Cramer et al., 2013).
3.3.4. Muscle performance trainingThe terms muscle performance
and muscle strength both
broadly refer to the ability of a muscle to produce force,
regardlessof the action (isometric vs. anisometric), load (body
segment vs.free-weight), or intensity (low load vs. high load)
(Mayhew andRothstein, 1985; Sapega, 1990; Clark, 2001). Muscles
must rstpossess inherently sufcient muscle strength before they
caneffectively control the mass, orientation, and alignment of
bodysegments (Borsa et al., 1994; Hodges and Moseley,
2003;Macpherson and Horak, 2013). Muscle performance training
usu-ally involves the repeated activation of skeletal muscle around
aprimary axis-of-rotation and in a single plane-of-motion,
typicallyagainst some resistance (body segment or an added external
load),with the primary intent of modifying muscle force
generatingcharacteristics. Examples are side-lying loaded shoulder
externalrotation, double-leg bodyweight squats, and side-lying
loadedankle eversion (Fig. 6). Muscle performance training has been
re-ported to benecially modify proprioception. In the
spine,controlled head lift exercise in people with neck pain
demonstratedimproved force sense (O'Leary et al., 2007). Scapular
and gleno-humeral anisometric bodyweight and dumb-bell strength
traininghas been reported to signicantly improve glenohumeral
active JPSrapy 20 (2015) 378e387and ankle invertor and evertor
isokinetic strength training has alsobeen reported to signicantly
improve ankle inversion passive JPSin recreational athletes with
functional ankle instability (Sekir et al.,2007).
3.3.5. Balance/unstable surface trainingBalance is the process
of maintaining the body's center of mass
within its base of support via appropriate internal
momentsresisting destabilizing external moments acting on the
body(Macpherson and Horak, 2013). Balance is the result of
feedbackand feed-forwards corrective movements at multiple joints
tomaintain the position and orientation of one body segment
relativeto another over the base-of-support (Macpherson and
Horak,2013). Balance training typically involves performing
exercises onan unstable surface (e.g. rocker-board, inatable
devices) (Clark andHerrington, 2010). Examples of balance training
exercises arestanding balance tasks on soft surfaces or
wobble-boards (Beinertand Taube, 2013), performing cervical
movements whilst chal-lenging balance (Gatti et al., 2011),
press-ups on a Swiss-ball (Myersand Lephart, 2000), and single-leg
squats on a rocker-board (Fig. 7)(Clark and Herrington, 2010).
Single-leg stance, tandem stance, anddouble-leg stance on a
wobble-board has enhanced cervical spineactive JPS in a group of
people with sub-clinical neck pain (Beinertand Taube, 2013). Lower
extremity wobble-board training hasenhanced ankle active
kinesthesia (active movement
-
to mid-stance of gait, lower extremity extensors use
eccentricmuscle actions to decelerate the body, followed by very
brief iso-metric muscle actions, before transitioning to concentric
muscleactions to accelerate the body from mid-stance to push-off
(Komi,1992; Chu, 1998). Plyometric training uses the SSC as a
keyfeature during the execution of exercise drills. Plyometric
trainingmust be executed rapidly with meticulous technique
withemphasis on the transition between eccentric and
concentricmuscle actions being as fast and short duration as
possible (Chu,1998). Examples of plyometric training exercises are
kneeling 90-90 shoulder internal-external rotations against elastic
resistance(Swanik et al., 2002) (Fig. 8), double-leg barrier jumps
(Chu, 1998)(Fig. 9), and single-leg in-place (vertical) hops (Clark
andHerrington, 2010). Plyometric training can benecially
modifyproprioception of the extremities. Kneeling 90-90 shoulder
inter-nal-external rotations against elastic resistance and ball
throwing
Therapy 20 (2015) 378e387 383N.C. Clark et al. /
Manualdiscrimination) in uninjured, elite rugby league
players(Waddington et al., 1999), Australian Rules Football
players(Waddington et al., 2000), and independent older
people(Waddington and Adams, 2004). Swiss-ball training was shown
tosignicantly improve knee passive JPS in uninjured students (Cuget
al., 2012). Upper extremity wobble-board training has been
re-ported to signicantly enhance shoulder active
kinesthesiafollowing shoulder dislocation (Naughton et al., 2005).
A lowerextremity exercise programme including a rocker-board,
wobble-board, mini trampoline, tilted platform, and uneven walkway
hasalso been reported to signicantly improve ankle passive JPS
inadults with functional ankle instability (Eils and Rosenbaum,
2001).
3.3.6. Plyometric trainingMany functional tasks demonstrate an
eccentric-isometric-
concentric sequence of muscle actions termed the
stretch-shortening cycle (SSC) (Chu, 1998). For example, from
foot-strike
drills against a mini-trampoline have been reported to
signicantlyimprove glenohumeral active JPS and passive kinesthesia
in unin-jured elite swimmers (Swanik et al., 2002). Jump-landing
andjump-landing with change-of-direction training has been
reportedto signicantly improve knee active kinesthesia in
uninjuredAustralian Rules Football players (Waddington et al.,
2000).
Fig. 7. Single-Leg Rocker-Board Squat. Copyright Nicholas Clark.
Reproduced withpermission.Fig. 8. Kneeling 90-90 Plyometric
Shoulder Internal-External Rotation (From Swaniket al., 2002). The
individual is instructed to perform concentric shoulder
internalrotation to 90 , hold the position for two seconds, and
then release the isometric holdso that the tubing rapidly recoils
and pulls the shoulder into external rotation. As soonas the
desired amount of external rotation is achieved, the individual is
instructed tostop the external rotation recoil and again perform
concentric internal rotation to 90 .Traditional plyometric training
programme design methods are applied (e.g. 3 sets
15 repetitions, 2 sessions per week). Copyright Nicholas Clark.
Reproduced withpermission.
-
3.3.7. Vibration training
Fig. 9. Double-Leg Barrier Jumps. Copyright Ni
N.C. Clark et al. / Manual The384Vibration is a mechanical event
that demonstrates rapid oscil-latory movements and is a powerful
stimulus for the musclespindle (Goodwin et al., 1972; Roll and
Vedel, 1982). Vibrationtraining involves exercising with a device
that produces a vibrationstimulus (e.g. vibration platform), where
the combination of mus-cle activationwith the rapid small amplitude
change in direction ofjoint motion becomes a powerful stimulus for
the muscle spindle(Cardinale and Bosco, 2003). The intensity of the
vibration isdetermined by the amplitude and frequency of the
oscillations(Cardinale and Bosco, 2003), and devices vibrating from
5 to 50 Hzare typically used in training (Fontana et al., 2005;
Moezy et al.,2008; Tripp et al., 2009). Examples of vibration
training includeFig. 10. Modied push-ups on a vibration
platform.modied push-ups (Hand et al., 2009) (Fig.10), bodyweight
double-leg squats and bodyweight lunges onto a vibration platform
(Moezyet al., 2008). Vibration training can alter proprioception of
the spineand extremities. Isometric neck extension using a sling
systemwithsuperimposed vibration stimuli signicantly enhanced force
sense(steadiness) of the cervical spine in chronic neck pain
(Muceli et al.,2011). Postural exercise involving lumbar
hyperlordosis isometricholds while standing on a vibration platform
signicantly improvedsingle-session lumbar spine active JPS (Fontana
et al., 2005), andisometric elbow exion holding a vibrating
dumb-bell has beenreported to signicantly enhance elbow active JPS
within in a singletraining session (Tripp et al., 2009). Isometric
and anisometricdouble-leg and single-leg balance, squat, and lunge
exercises on avibrating platform has also shown improvement in knee
active JPSafter anterior cruciate ligament reconstruction (Moezy et
al., 2008).cholas Clark. Reproduced with permission.
rapy 20 (2015) 378e3874. Summary
Clinical assessment of proprioception can be performed
usinggoniometers, inclinometers, laser-pointers, and pressure
sensors.These devices can be employed in a clinical context within
tests ofactive JPS and kinesthesia, and force sense. Balance tests
can also beemployed in a clinical context for measuring integrated
sensori-motor control of balance, but it should be remembered that
theseare not able to isolate proprioception alone. In the cervical
spine,head and eye movement control should also be assessed as one
ofthe important roles of proprioception. Following
musculoskeletalinjury, pain, effusion, and fatigue can result in
impaired proprio-ception, and so these causes of impaired
proprioception should betreated alongside the implementation of
other interventions.
Manual therapy interventions (joint mobilisations,
manipula-tions, soft tissue techniques) taping, and bracing show
the ability toimmediately and benecially affect proprioception.
Several types ofexercise therapy have also demonstrated long-term
improvementsin proprioception in the spine and the extremities.
Althoughmanual therapy, taping, and bracing can immediately and
bene-cially affect proprioception, concern has been statedwith
regards tothe size and duration of therapeutic effects of passive
interventions(Cook, 2011). Nevertheless, these passive
interventions can beemployed immediately prior to same-session
active rehabilitation
-
Table 1Proposed specic example exercises to benecially affect
proprioception of different body parts.
Exercise type Cervical spine Lumbar spine Upper limb Lower
limb
Active jointrepositioning (JPS)training visualfeedback
Repositioning head to neutraland other points in ROM
usinglaser-pointer (sitting, standing,SLS)
Repositioning spine to neutral,points in range (sitting,
standing,four-point kneeling)
OKC and CKC shoulder, elbow,wrist, nger repositioning
todifferent points in ROM
OKC and CKC hip, knee, anklerepositioning to different pointsin
ROM
Path-of-motion(kinesthesia)training
Following a line or pattern (zig-zag, gure-of-eight,
computergenerated) using a laser-pointer on the head or
motionsensors
Tracing patterns with laser-pointerMovement acuity exercises of
wristand ngers (using smartphone orsurfpad)
Tracing pattern with laser-pointer (letters of alphabet withfoot
and ankle)
Force sense training CCFT with PBUForce and effort
perceptiontraining using a dynamometerat pre-determined
percentageof isometric MVMA (exors,extensors, lateral
exors,rotators)
Abdominal muscle training withPBUForce and effort perception
trainingusing a dynamometer at pre-determined percentage of
isometricMVMA (exors, extensors, lateralexors)
Force and effort perception trainingof hand and ngers with
grip/pinchdynamometerForce and effort perception trainingusing a
dynamometer at pre-determined percentage of isometricMVMA (shoulder
external rotators,elbow exors, wrist extensors)
Force and effort perceptiontraining using a dynamometerat
pre-determined percentageof isometric MVMA (hipexternal rotators,
knee exors,ankle evertors)
Co-ordinationtraining
Head-eye co-ordinationTrunk-head co-ordinationEye, head, trunk,
arm co-ordinationCCFTNeck extension with neutralupper cervical
spineGaze stability (eyes still, headmoves into exion, extensionand
rotation)Eye follow side to side head stillin head neutral and in
torsion
TrA-multidus co-activationUL and LL movement whilemaintaining
trunk stability (neutrallumbar spine)Pilates
Scapular inter-muscular co-ordination (scapular upwardrotation
force couple)Rotator cuff co-ordination withgross UL
movementsWrist, hand, nger ne co-ordination tasks
Gluteus maximus-hamstringsco-ordination during prone SLRGluteus
medius-TFL co-ordination during hipabduction
variationsPelvis-hip-knee-ankle-footalignment training during
CKCtasksKnee valgus-varus movementcontrol during CKC
tasksFoot-shank-thigh co-ordinationon elliptical trainerTai Chi
Muscle performancetraining
CCFT low-load enduranceCervical extensor training infour-point
kneeling externalloadHead-lifts into exion,extension, lateralexion
external load
TrA, multidus enduranceCurl-upsTrunk extensor, front-plank,
side-plank isometric holds
Bodyweight strength trainingResistance training
machinesFree-weightsElastic resistance training
Bodyweight strength trainingResistance training
machinesFree-weightsElastic resistance training
Balance/unstablesurface training
Standing (eyes open or closed;narrow, tandem, SLS on rmthen soft
surface (foam) thenunstable surface (rocker board))Perform other
exercises whilein unstable positions (JPS, eyeco-ordination)Tandem
walk, walking withhead movementNeck resistance training
inslingsControl motion of a movingobject with the head and
neck(ball on head)
Standing (eyes open or closed;narrow, tandem, SLS on rm thensoft
surface (foam) then unstablesurface (rocker board))Sitting on a
Swiss-ball ULmovementsStabilising the trunk whileperforming active
UL movementswhile controlling an oscillating polePerforming active
movements oftrunk while controlling oscillatingpole or
Swiss-ball
Press-ups on a Swiss-ball orwobble-boardPress-ups with legs
elevated on aSwiss-ballWrist gyroscopic exercise balltrainingActive
UL movements whilecontrolling an oscillating poleControl of ball on
wall withshoulder and UL
Standing (eyes open or closed;narrow, tandem, SLS on rmthen soft
surface (foam) thenunstable surface (rocker board))Standing as
above distraction/perturbation from clinician(ball
throwing/catching, pelvicgirdle rhythmic stabilisations)Single-leg
squats on rocker-boardWobble-board, Swiss-ball,mini-trampoline
training
Plyometric training Plyoball sit-upsPlyoball back
extensionPlyoball long-sitting side throws
Kneeling 90-90 shoulder internal-external rotations against
elasticresistanceClapping press-upsBall throwing/catching against
mini-trampoline
Double-leg and single-leg hops,leaps, jumps,bounding barriers,
boxes,platformsDepth jumpsSkipping drills
Vibration training Neck extension resistancetraining with
vibration added
Lumbopelvic postural exerciseswhile standing of
vibrationplatform
Push-ups on vibration platformElbow, wrist movement
withvibrating dumb-bellsArm movement with oscillatingpole
Double-leg and single-legsquats on vibration platformLunges on
vibration platform
ROM range-of-motion.SLS single-leg stance.OKC open kinetic
chain.CKC closed kinetic chain.CCFT cranio-cervical exion
training.PBU pressure biofeedback unit.JPS joint position
sense.MVMA maximum voluntary muscle action.TrA transversus
abdominis.UL upper limb.LL lower limb.SLR straight leg raise.
N.C. Clark et al. / Manual Therapy 20 (2015) 378e387 385
-
Thewith a view to assisting patients to prepare for specic
exercisetherapy interventions and functional movements (Clark
andLephart, 2015). Thus, it is likely that a mixed mode
interventionapproach is optimal for enhancing proprioception in
clinicalpractice.
As discussed in Part 1 of this Masterclass (Roijezon et al.,
2015),different exercise types will affect the CNS in different
ways. Someexercises will preferentially affect supraspinal levels
of the CNS (e.g.cerebrum), while others preferentially affect
spinal cord levels and,therefore, inuence different aspects of
proprioception in differentfunctional contexts. The types of
exercise commonly used toimprove proprioception can vary according
to different functionaldemands of the body areas and joints.
Exercises (active jointrepositioning, force sense, co-ordination,
muscle performance,balance/unstable surface, plyometric, and
vibration training)should be used to facilitate long-term benecial
adaptations inproprioception and enhance overall sensorimotor
control (Clarkand Lephart, 2015). There is also evidence that
different exercisetypes can enhance proprioception in asymptomatic
individualsand, therefore, may have specic clinical utility for the
preventionand rehabilitation of musculoskeletal disorders.
Based on research presented here, examples of exercises
tobenecially affect proprioception of different body parts are
pro-posed in Table 1. Future directions should consider advances
inclinical assessment of proprioception, which is lacking in a
numberof areas. This might also direct future research towards
identifyingother interventions, or the most appropriate
combinations of in-terventions, to improve proprioception in
musculoskeletalrehabilitation.
References
Anderson V, Wee E. Impaired joint proprioception at higher
shoulder elevations inchronic rotator cuff pathology. Arch Phys Med
Rehab 2011;92:1146e51.
Balke M, Liem D, Dedy N, Thorwesten L, Balke M, Poetzl W, et al.
The laser-pointerassisted angle reproduction test for evaluation of
proprioceptive shoulderfunction in patients with instability. Arch
Orthop Trauma Surg 2011;131:1077e84.
Beinert K, Taube W. The effect of balance training on cervical
sensorimotor functionand neck pain. J Mot Behav 2013;45:271e8.
Benjaminse A, Sell T, Abt J, House A, Lephart S. Reliability and
precision of hipproprioception methods in healthy individuals. Clin
J Sport Med 2009;19:457e63.
Borsa P, Lephart S, Irrgang J, Safran M, Fu F. The effects of
joint position and di-rection of joint motion on proprioceptive
sensibility in anterior cruciateligament-decient athletes. Am J
Sports Med 1997;25:336e40.
Borsa P, Lephart S, Kocher M, Lephart S. Functional assessment
and rehabilitation ofshoulder proprioception for glenohumeral
instability. J Sport Rehabil 1994;3:84e104.
Brindle T, Uhl T, Nitz A, Shapiro R. The inuence of external
loads on movementprecision during active shoulder internal rotation
movements as measured by 3indices of accuracy. J Athl Train
2006;41:60e6.
Callaghan M, Selfe J, Bagley P, Oldham J. The effects of
patellar taping on knee jointproprioception. J Athl Train
2002;37:19e24.
Cardinale M, Bosco C. The use of vibration as an exercise
intervention. Exerc SportSci Rev 2003;31:3e7.
Chang H, Chou K, Lin J, Lin C, Wang C. Immediate effect of
forearm kinesio taping onmaximal grip strength and force sense in
healthy collegiate athletes. Phys TherSp 2010;11:122e7.
Chen X, Treleaven J. The effect of neck torsion on joint
position error in subjectswith chronic neck pain. Man Ther
2013;18:562e7.
Cho Y, Hong B, Lim S, Kim H, Ko Y, Im S, et al. Effects of joint
effusion on proprio-ception in patients with knee osteoarthritis: a
single-blind, randomizedcontrolled clinical trial. Osteoarthr
Cartil 2011;19:22e8.
Chu D. Jumping into plyometrics. 2nd ed. Illinois: Juman
Kinetics; 1998.Chu J, Kane E, Arnold B, Gansneder B. The effect of
a neoprene shoulder stabilizer on
active joint-reposition sense in subjects with stable and
unstable shoulders.J Athl Train 2002;37:141e5.
Clark N. Functional performance testing following knee ligament
injury. Phys TherSport 2001;2:91e105.
Clark N, Herrington L. The knee. In: Comfort P, Abrahamson E,
editors. Sportsrehabilitation and injury prevention. Chichester:
John Wiley; 2010. p. 407e63.
Clark N, Lephart S. Management of the sensorimotor system: the
lower limb. In:
N.C. Clark et al. / Manual386Jull G, Moore A, Falla D, Lewis J,
McCarthy C, Sterling M, editors. Grieve'smodern musculoskeletal
physiotherapy. Edinburgh: Elsevier; 2014 [in press].Cook C.
Immediate effects from manual therapy: much ado about nothing? J
ManManip Ther 2011;19:3e4.
Corneil BD, Olivier E, Munoz DP. Neck muscle responses to
stimulation of monkeysuperior colliculus. I. Topography and
manipulation of stimulation parameters.J Neurophysiol
2002;88:1980e99.
Cramer H, Lauche R, Hohmann C, Ludtke R, Haller H, Michalsen A,
et al. Random-ized-controlled trial comparing yoga and home-based
exercise for chronic neckpain. Clin J Pain 2013;29:216e23.
Cug M, Ak E, Ozdemir RA, Korkusuz F, Behm DG. The effect of
instability training onknee joint proprioception and core strength.
J Sports Sci Med 2012;11:468e74.
Della Casa E, Helbling JA, Meichtry A, Luomajoki H, Kool J.
Head-eye movementcontrol tests in patients with chronic neck pain;
inter-observer reliability anddiscriminative validity. Bmc
Musculoskelet Disord 2014;15.
Dickson D, Hollman-Gage K, Ojofeitimi S, Bronner S. Comparison
of functional anklemotion measures in modern dancers. J Dance Med
Sci 2012;16:116e25.
Docherty C, Arnold B. Force sense decits in functionally
unstable ankles. J OrthopRes 2008;26:1489e93.
Docherty C, Moore J, Arnold B. Effects of strength training on
strength developmentand joint position sense in functionally
unstable ankles. J Athl Train 1998;33:310e4.
Eils E, Rosenbaum D. A multi-station proprioceptive exercise
program in patientswith ankle instability. Med Sci Sports Exerc
2001;33:1991e8.
Fontana TL, Richardson CA, Stanton WR. The effect of
weightbearing exercise withlow frequency, whole body vibration on
lumbosacral proprioception: a pilotstudy on normal subjects. Aust J
Physiotherapy 2005;51:259e63.
Gabbe B, Bennell K, Wajswelner H, Finch C. Reliability of common
lower extremitymusculoskeletal screening tests. Phys Ther Sp
2004;5:90e7.
Gatti R, Faccendini S, Tettamanti A, Barbero M, Balestri A,
Calori G. Efcacy of trunkbalance exercises for individuals with
chronic low back pain: a randomizedclinical trial. J Orthop Sports
Phys Ther 2011;41:542e52.
Goats G. Massage. The scientic basis of an ancient art: part 1.
The techniques. Br JSports Med 1994;28:149e52.
Goats G, Keir K. Connective tissue massage. Br J Sports Med
1991;25:131e3.Goodwin G, McCloskey D, Matthews P. The contribution
of muscle afferents to
kinaesthesia shown by vibration induced illusions of movement
and by theeffects of paralysing joint afferents. Brain
1972;95:705e48.
Gordon J. Spinal mechanisms of motor coordination. In: Kandel E,
Schwartz J,Jessell T, editors. Principles of neural science.
London: Prentice-Hall Interna-tional; 1991. p. 581e95.
Greenman P. Principles of manual medicine. Philadelphia:
Lippincott; 2003.Grip H, Jull G, Treleaven J. Head eye
co-ordination and gaze stability using simul-
taneous measurement of eye in head and head in space movements
-potentialfor use in subjects with a whiplash injury. J Clin Monit
Comput 2009;23:31e40.
Haavik H, Murphy B. Subclinical neck pain and the effects of
cervical manipulationon elbow joint position sense. J Manip Physiol
Ther 2011;34:88e97.
Hamid M, Ali M, Yusof A. Interrater and intrarater reliability
of the active kneeextension (AKE) test among healthy adults. J Phys
Ther Sci 2013;25:957e61.
Hand J, Verscheure S, Osternig L. A comparison of whole-body
vibration andresistance training on total work in the rotator cuff.
J Athl Train 2009;44:469e74.
Heikkila H, Johansson M, Wenngren BI. Effects of acupuncture,
cervical manipula-tion and NSAID therapy on dizziness and impaired
head repositioning of sus-pected cervical origin: a pilot study.
Man Ther 2000;5:151e7.
Henriksen M, Hjrup A, Lund H, Christensen L, Danneskiold-Samse
B, Bliddal H.The effect of stimulating massage of thigh muscles on
knee joint position sense.Adv Physiotherapy 2004;6:29e36.
Hodges P, Moseley G. Pain and motor control of the lumbopelvic
region: effect andpossible mechanisms. J Electromyogr Kinesiol
2003;13:361e70.
Humphreys B, Irgens P. The effect of a rehabilitation exercise
program on headrepositioning accuracy and reported levels of pain
in chronic neck pain subjects.J Whiplash Relat Disord
2002;1:99e112.
Jerosch J, Hoffstetter I, Bork H, Bischof M. The inuence of
orthoses on the pro-prioception of the ankle joint. Knee Surg
Sports Traumatol Arthrosc 1995;3:39e46.
Jerosch J, Prymka M. Knee joint proprioception in normal
volunteers and patientswith anterior cruciate ligament tears,
taking special account of the effect of aknee bandage. Arch Orthop
Trauma Surg 1996;115:162e6.
Ju Y, Wang C, Cheng H. Effects of active fatiguing movement
versus passive re-petitive movement on knee proprioception. Clin
Biomech 2010;25:708e12.
Jull G. Deep cervical exor muscle dysfunction in whiplash. J
Musculoskelet Pain2000;8:143e54.
Jull G, Falla D, Treleaven J, Hodges P, Vicenzino B. Retraining
cervical joint positionsense: the effect of two exercise regimes. J
Orthop Res 2007;25:404e12.
Jull G, Trott P, Potter H, Zito G, Niere K, Shirley D, et al. A
randomized controlled trialof exercise and manipulative therapy for
cervicogenic headache. Spine 2002;27:1835e43.
Kaltenborn F. Manual mobilizations of the joints: the Kaltenborn
method of jointexamination and treatment. The extremities. 5th ed.,
vol. I. Oslo: Olaf NorlisBokhandel; 1999.
Kennedy J, Alexander I, Hayes K. Nerve supply of the human knee
and its functionalimportance. Am J Sports Med 1982;10:329e35.
Kent M. The Oxford dictionary of sports science and medicine.
3rd ed. Oxford:Oxford University Press; 2006.
rapy 20 (2015) 378e387Koga H, Nakamae A, Shima Y, Iwasa J,
Myklebust G, Engebretsen L, et al. Mecha-nisms for noncontact
anterior cruciate ligament injuries: knee joint kinematics
-
in 10 injury situations from female team handball and
basketball. Am J SportsMed 2010;38:2218e25.
Kolber M, Hanney W. The reliability and concurrent validity of
shoulder mobilitymeasurements using a digital inclinometer and
goniometer: a technical report.
Perez M, Lungholt B, Nyborg K, Nielsen J. Motor skill training
induces changes in theexcitability of the leg cortical area in
healthy humans. Exp Brain Res 2004;159:197e205.
Peterson BW. Current approaches and future directions to
understanding control ofhead movement. Brain Mech Integr Posture
Mov 2004:369e81.
N.C. Clark et al. / Manual Therapy 20 (2015) 378e387 387Int J
Sports Phys Ther 2012;7:306e13.Komi P. Stretch-shortening cycle.
In: Komi P, editor. Strength and power in sport.
Oxford: Blackwell Scientic; 1992. p. 169e79.Kristjannson E. The
y unit. 2014. www.neckcare.com.Kristjansson E, Hardardottir L,
Asmundardottir M, Gudmundsson K. A new clinical
test for cervicocephalic kinesthetic sensibility: The y. Arch
Phys Med Rehab2004;85:490e5.
Lagerquist O, Mang C, Collins D. Changes in spinal but not
cortical excitabilityfollowing combined electrical stimulation of
the tibial nerve and voluntaryplantar-exion. Exp Brain Res
2012;222:41e53.
Lamell-Sharp A, Swanik C, Tierney R. The effect of variable
joint loads on knee jointposition and force sensation. J Athl Train
2002;37:S29.
Learman K, Myers J, Lephart S, Sell T, Kerns G, Cook C. Effects
of spinal manipulationon trunk proprioception in subjects with
chronic low back pain during symp-tom remission. J Manip Physiol
Ther 2009;32:118e26.
Lee S, Ren Y, Chang A, Geiger F, Zhang L. Effects of pivoting
neuromusculartraining on pivoting control and proprioception. Med
Sci Sports Exerc2014;46:1400e9.
Lephart S, Henry T. The physiological basis for open and closed
kinetic chainrehabilitation for the upper extremity. J Sport
Rehabil 1996;5:71e87.
Lephart S, Kocher M, Fu F, Borsa P, Harner C. Proprioception
following anteriorcruciate ligament reconstruction. J Sport Rehabi
1992;1:188e98.
Lephart S, Smoliga J, Myers J, Sell T, Tsai Y. An eight-week
golf-specic exerciseprogram improves physical characteristics,
swing mechanics, and golf perfor-mance in recreational golfers. J
Strength Cond Res 2007;21:860e9.
Lephart S, Warner J, Borsa P, Fu F. Proprioception of the
shoulder joint in healthy,unstable, and surgically repaired
shoulders. J Shoulder Elb Surg 1994;3:371e80.
Macdonald R. Taping techniques. Principles and practice. 2nd ed.
Edinburgh: But-terworth Heinemann; 2004.
Macpherson J, Horak F. Posture. In: Kandel E, Schwartz J,
Jessell T, Siegelbaum S,AH,editors. Principles of neural science.
5th ed. New York: McGraw Hill; 2013.p. 935e59.
Martin J, Jessell T. Modality coding in the somatic sensory
system. In: Kandel E,Schwartz J, Jessell T, editors. Principles of
neural science. 3rd ed. London:Prentice-Hall International Inc;
1991. p. 341e52.
Mayhew T, Rothstein J. Measurement of muscle performance with
instruments. In:Rothstein J, editor. Measurment in physical
therapy. New York: Churchill Liv-ingstone; 1985. p. 57e101.
McLain R, Raiszadeh K. Mechanoreceptor endings of the cervical,
thoracic, andlumbar spine. Iowa Orthop J 1995;15:147e55.
McNair PJ, Heine PJ. Trunk proprioception: enhancement through
lumbar bracing.Archi Phys Med Rehab 1999;80:96e9.
Michelson J, Hutchins C. Mechanoreceptors in human ankle
ligaments. J Bone JtSurg 1995;77B:219.
Moezy A, Olyaei G, Hadian M, Razi M, Faghihzadeh S. A
comparative study of wholebody vibration training and conventional
training on knee proprioception andpostural stability after
anterior cruciate ligament reconstruction. Br J SportsMed
2008;42:373e8.
Mok K, Fong D, Krosshaug T, Engebretsen L, Hung A, Yung P, et
al. Kinematicsanalysis of ankle inversion ligamentous sprain
injuries in sports: 2 cases duringthe 2008 Beijing olympics. Am J
Sports Med 2011;39:1548e52.
Moraes M, Cavalcante M, Leite J, Macedo J, Sampaio M, Jamacaru
V, et al. Thecharacteristics of the mechanoreceptors of the hip
with arthrosis. J Orthop SurgRes 2011;6:58.
Muceli S, Farina D, Kirkesola G, Katch F, Falla D. Reduced force
steadiness in womenwith neck pain and the effect of short term
vibration. J Electromyogr Kinesiol2011;21:283e90.
Myers J, Lephart S. The role of the sensorimotor system in the
athletic shoulder.J Athl Train 2000;35:351e63.
Naughton J, Adams R, Maher C. Upper-body wobbleboard training
effects on thepost-dislocation shoulder. Phys Ther Sport
2005;6:31e7.
Newcomer K, Laskowski ER, Yu B, Johnson JC, An KN. The effects
of a lumbarsupport on repositioning error in subjects with low back
pain. Arch Phys MedRehab 2001;82:906e10.
O'Leary S, Jull G, Kim M, Vicenzino B. Specicity in retraining
craniocervical exormuscle performance. J Orthop Sports Phys Ther
2007;37:3e9.
O'Leary SP, Vicenzino BT, Jull GA. A new method of isometric
dynamometry for thecraniocervical exor muscles. Phys Ther
2005;85:556e64.
Palmgren PJ, Sandstrom PJ, Lundqvist FJ, Heikkila H. Improvement
after chiropracticcare in cervicocephalic kinesthetic sensibility
and subjective pain intensity inpatients with nontraumatic chronic
neck pain. J Manip Physiol Ther 2006;29:100e6.
Pereira M, Beaudin C, Grewal G, Wong V, Treleaven J. Cervical
movement sense:normative data for a clinical tool. J Eval Clin
Pract 2015 [in review].Revel M, Minguet M, Gergory P, Vaillant J,
Manuel JL. Changes in cervicocephalickinesthesia after a
proprioceptive rehabilitation program in patients with neckpain: a
randomized controlled study. Arch Phys Med Rehab 1994;75:895e9.
Rogol I, Ernst G, Perrin D. Open and closed kinetic chain
exercises improve shoulderjoint reposition sense equally in healthy
subjects. J Athl Train 1998;33:315e8.
Roijezon U, Clark N, Treleaven J. Proprioception in
musculoskeletal rehabilitation.Part 1: basic science and principles
of assessment and clinical intervention. ManTher 2015 [in
press].
Roll J, Vedel J. Kinaesthetic role of muscle afferents in man,
studied by tendon vi-bration and microneurography. Exp Brain Res
1982;47:177e90.
Roren A, Mayoux-Benhamou MA, Fayad F, Poiraudeau S, Lantz D,
Revel M. Com-parison of visual and ultrasound based techniques to
measure head reposi-tioning in healthy and neck-pain subjects. Man
Ther 2009;14:270e7.
Rothwell J. Control of human voluntary movement. 2nd ed. London:
Chapman andHall; 1994.
Sapega A. Muscle performance evaluation in orthopaedic practice.
J Bone Jt Surg Am1990;72:1562e74.
Sekir U, Yildiz Y, Hazneci B, Ors F, Aydin T. Effect of
isokinetic training on strength,functionality and proprioception in
athletes with functional ankle instability.Knee Surg Sports
Traumatol Arthrosc 2007;15:654e64.
Simoneau G, Degner R, Kramper C, Kittleson K. Changes in ankle
joint proprio-ception resulting from strips of athletic tape
applied over the skin. J Athl Train1997;32:141e7.
Stecco C, Gagey O, Belloni A, Pozzuoli A, Porzionato A, Macchi
V, et al. Anatomy ofthe deep fascia of the upper limb. Second part:
study of innervation. Mor-phologie 2007;91:38e43.
Steinbeck J, Brntrup J, Greshake O, Potzl W, Filler T,
Liljenqvist U. Neurohistologicalexamination of the inferior
glenohumeral ligament of the shoulder. J OrthopRes
2003;21:250e5.
Suprak D, Osternig L, van Donkelaar P, Karduna A. Shoulder joint
position senseimproves with external load. J Mot Behav
2007;39:517e25.
Swait G, Rushton AB, Miall C, Newell D. Evaluation of cervical
proprioceptivefunction. Spine 2007;32:E692e701.
Swanik K, Lephart S, Swanik C, Lephart S, Stone D, Fu F. The
effects of shoulderplyometric training on proprioception and
selected muscle performance char-acteristics. J Shoulder Elb Surg
2002;11:579e86.
Treleaven J. Sensorimotor disturbances in neck disorders
affecting postural stability,head and eye movement control. Man
Ther 2008;13:2e11.
Treleaven J, Jull G, Grip H. Head eye co-ordination and gaze
stability in subjects withpersistent whiplash associated disorders.
Man Ther 2011;16:252e7.
Treleaven J, Jull G, Sterling M. Dizziness and unsteadiness
following whiplashinjury: characteristic features and relationship
with cervical joint position error.J Rehab Med 2003;35:36e43.
Treleaven J, Peterson G, Landen Ludvigsson M, Kammermind S,
Peolsson A. Balance,dizziness and proprioception in patients with
chronic whiplash associateddisorders complaining of dizziness: a
prospective randomized study comparingthree exercise programs. Man
Ther 2014 [in review].
Tripp BL, Faust D, Jacobs P. Elbow joint position sense after
neuromuscular trainingwith handheld vibration. J Athl Train
2009;44:617e23.
Tsang WWN, Hui-Chan CWY. Effects of Tai Chi on joint
proprioception and stabilitylimits in elderly subjects. Med Sci
Sports Exerc 2003;35:1962e71.
Vicenzino B, Jordan K, BrandjerpornM, Teys P, Bisset L.
Mobilizationwith movementtreatment of the ankle changes joint
position sense in subjects with recurrentsprains: a preliminary
report. J Orthop Sports Phys Ther 2005;35:A-21.
Waddington G, Adams R. The effect of a 5-week wobble-board
exercise interventionon ability to discriminate different degrees
of ankle inversion, barefoot andwearing shoes: a study in healthy
elderly. J Am Geriatrics Soc 2004;52:573e6.
Waddington G, Adams R, Jones A. Wobble board (ankle disc)
training effects on thediscrimination of inversion movements. Aust
J Physiotherapy 1999;45:95e101.
Waddington G, Seward H, Wrigley T, Lacey N, Adams R. Comparing
wobble boardand jump-landing training effects on knee and ankle
movement discrimination.J Sci Med Sport 2000;3:449.
Wassinger C, Myers J. Reported mechanisms of shoulder injury
during the baseballthrow. Phys Ther Rev 2011;16:305e9.
Wibault J, Vaillant J, Vuillerme N, Dedering A, Peolsson A.
Using the cervical rangeof motion (CROM) device to assess head
repositioning accuracy in individualswith cervical radiculopathy in
comparison to neck- healthy individuals. ManTher 2013;18:403e9.
Woodhouse A, Stavdahl , Vasseljen O. Irregular head movement
patterns inwhiplash patients during a trajectory task. Exp Brain
Res 2010;201:261e70.
Yahia L, Rhalmi S, Newman N, Isler M. Sensory innervation of
human thor-acolumbar fascia. An immunohistochemical study. Acta
Orthop Scand 1992;63:195e7.
Proprioception in musculoskeletal rehabilitation. Part 2:
Clinical assessment and intervention1. Introduction2. Clinical
assessment of proprioception2.1. Clinical apparatus2.2. Specific
tests2.2.1. Joint position sense2.2.2. Kinesthesia2.2.3. Force
sense
2.3. Non-specific tests2.3.1. Balance tests2.3.2. Oculomotor and
eye-head coordination tests
3. Clinical interventions to improve proprioception3.1. Manual
therapy3.2. Taping and bracing3.3. Exercise therapy3.3.1. Active
joint repositioning training3.3.2. Force sense training3.3.3.
Co-ordination training3.3.4. Muscle performance training3.3.5.
Balance/unstable surface training3.3.6. Plyometric training3.3.7.
Vibration training
4. SummaryReferences