Embed Size (px)
Citation preview

Project: Ghana Emergency Medicine Collaborative
Document Title: Gastrointestinal Bleeding in the Pediatric Patient
Author(s): Michele Carney (University of Michigan), M.D., 2011
License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike-3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to use, share, and adapt it. These lectures have been modified in the process of making a publicly shareable version. The citation key on the following slide provides information about how you may share and adapt this material.
Copyright holders of content included in this material should contact [email protected] with any questions, corrections, or clarification regarding the use of content.
For more information about how to cite these materials visit http://open.umich.edu/privacy-and-terms-use.
Any medical information in this material is intended to inform and educate and is not a tool for self-diagnosis or a replacement for medical evaluation, advice, diagnosis or treatment by a healthcare professional. Please speak to your physician if you have questions about your medical condition.
Viewer discretion is advised: Some medical content is graphic and may not be suitable for all viewers.
1

Attribution Key
for more information see: http://open.umich.edu/wiki/AttributionPolicy
Use + Share + Adapt
Make Your Own Assessment
Creative Commons – Attribution License
Creative Commons – Attribution Share Alike License
Creative Commons – Attribution Noncommercial License
Creative Commons – Attribution Noncommercial Share Alike License
GNU – Free Documentation License
Creative Commons – Zero Waiver
Public Domain – Ineligible: Works that are ineligible for copyright protection in the U.S. (17 USC § 102(b)) *laws in your jurisdiction may differ
Public Domain – Expired: Works that are no longer protected due to an expired copyright term.
Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105)
Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain.
Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws in your jurisdiction may differ
Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee that your use of the content is Fair.
To use this content you should do your own independent analysis to determine whether or not your use will be Fair.
{ Content the copyright holder, author, or law permits you to use, share and adapt. }
{ Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. }
{ Content Open.Michigan has used under a Fair Use determination. }
2

Gastrointestinal Bleeding in the Pediatric Patient
Michele M. Carney, M.D.Combined EM Resident/PEM Fellow ConferenceNovember 9, 2011
3

Objective
Review the causes of upper and lower gastrointestinal bleeding in the pediatric population. Provide some diagnostic tools and management strategies for the most common offenders.
4

Introduction
• Bloody emesis or bloody stools are very anxiety provoking for parents
• Gastrointestinal bleeding is common in the pediatric population.
• Fortunately, most are from non-serious causes– Anal fissures, infectious, milk protein allergy, oral trauma,
prolapse gastropathy or esophagitis/gastritis
• Hemodynamically significant bleeding is uncommon.
5

Upper GI bleed
• Bleeding proximal to the ligament of Treitz.– Presents with:
• Hematemesis – vomiting bright red blood or coffee-ground material.
• Melena – black, tarry stools.– Time for gastric juices and bacteria degradation.
• If massive then hematochezia.– Shorter transit time.
– More blood loss than lower GI bleeding.
6

Ligament of Treitz
7
Source undetermined

Lower GI bleed
• Bleeding distal to the ligament of Treitz– Presents with:
• Hematochezia – bright red blood per rectum• Maroon stools – profuse bleed from distal small bowel
– The higher the bleed, the darker the stool
8

Is it really blood?
• Hemoccult kits– Used to test stool for blood.– Employs a peroxidase-like activity in hemoglobin to
oxidize with the reagent changing the color to blue.– False positive: red meat, horseradish, turnips, iron,
tomatoes and fresh red cherries.– False negatives: Vitamin C, storage for more than 4
days or outdated reagents or cards.– False negatives occur with emesis due to its acidic
nature.
9

Is it really blood?
– Gastroccult kits • Used to determine if blood is present in vomit.• Neutralizes the gastric acid in emesis making it
more accurate.
10

Clinical Evaluation• Hemodynamic stability
– Vitals• Tachycardia, orthostatic, hypotensive..
– Perfusion• Mental status, urine output, capillary refill…
• Blood in the oropharynx?• Hernia?• Skin exam: bruises, petechia, telangiectasia ,
jaundice?• Blood/fissures at the anus?
11

Causes: NeonatesNeonates (less than 1 month):
– Upper• Hemorrhagic disease of the newborn • Swallowed maternal blood• Stress gastritis
– Lower • Anal fissure• Allergic colitis• Hirshsprungs with enterocolitis• Malrotation with volvulus• Necrotizing enterocolitis
12

Case #1
• 5 day old ex)38 week breastfed neonate with hematemesis.
Vitals: • Temp: 36.5• HR: 150• RR:35• BP: 70/45
Sick or Not sick
13

Upper GI bleed: not sick• Swallowed maternal blood from delivery or
breast feeding– Apt test (don’t do at UM)
• APT (alum-precipitated toxoid) test• gastric contents of neonate mixed with 1% sodium
hydroxide• maternal hemoglobin turns rusty brown
– Kleihauer-Betke: sample exposed to acid to eliminate adult hemoglobin (quantitative test)
– Mom usually gives great history of painful nursing
• Gastritis from stressful birth
14

Upper or Lower GI bleed
• If the baby was born at home or mom refused Vitamin K shot Hemorrhagic disease of the newborn.– Vitamin K deficiency– Peaks 48 to 72 hours
• Other coagulopathies– Liver disease– Metabolic disease
15

Upper GI bleed
• If the history is unclear it is reasonable to check: – CBC– Coags– Chemistry with liver enzymes
16

Case #2• 5 day old ex) 36 week neonate presents with
bloody stool.
• Vitals: – Temp:37 – Heart rate: 190– Respiratory rate: 72– Blood pressure 76/45– Pulse ox: 97% on room air
Sick or Not sick?
17

18Source undetermined

Necrotizing enterocolitis (NEC)
• Overall rate of NEC in full term infants is approximately 0.7 per 1000 live births, which is almost 10% of all cases
• Mean age to presentation for full term is 4-5 days
• Mean age to presentation for premature is 10 days
19

Necrotizing enterocolitis (NEC)
• Most common acquired gastrointestinal disorder
• Small (most often distal) and/or large bowel becomes injured
• Intramural air, and may progress to frank necrosis with perforation Sepsis/Death
20

Necrotizing enterocolitis (NEC)
• Cause is unknown– Intestinal ischemia – Colonization by pathogenic bacteria– Excess protein substrate in the intestinal lumen
1. Santulli TV, Schullinger JN, Heird WC, et al. Acute necrotizing enterocolitis in infancy:a review of 64 cases. Pediatrics 1975;55(3):376–87.
2. Kosloske AM. Pathogenesis and prevention of necrotizing enterocolitis: a hypothesis basedon personal observation and a review of the literature. Pediatrics 1984;74(6):1086–92.
21

Necrotizing enterocolitis (NEC)
• Bowel rest • Nasogastric tube decompression• Fluid resuscitation• Blood and platelet transfusion if needed• Broad-spectrum antibiotics• Pediatric Surgery Consult
22

Case #3
• 4 week old male with poor feeding today presented with black stool
• Vitals:– Temp: 37.5– HR: 170– RR: 45– BP: 85/47– Pulse ox: 97%
23

Case #3
In the emergency department, patient’s vomit was green
24

Malrotation with volvulus
25Source undetermined

26Source undetermined

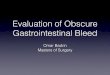
Malrotation
• 14 year old boy with recurrentabdominal pain andbilious emesis
27
Source undetermined

Malrotation
• Incidence of malrotation is 1 in 500 live births• 60% of volvulus cases occur in the first month of
life; 75% by 1 year of age• Volvulus occurs in 70% of neonatal malrotation
cases• No race predilection; male:female is 3:2• Morbidity: short-gut, TPN, SBO, recurrent
volvulus • Mortality: 3-9%
28

Malrotation
• Malrotation with midgut volvulus is the most critical surgical emergency in the newborn period
• Usually presents within the first weeks of life• Presents with the sudden onset of melena and
bilious vomiting in a previously health infant
29

Normal
• 4th and 5th week of gestation– Duodenal intestinal loop comes out and twists 90
degrees. Counterclockwise.– Cecal loop rotates 180 degrees.– Total of 270 degrees– Ileocecal valve in right lower quadrant – Ligament of Treitz in the left upper quadrant.– Long and strong mesenteric base
30

Malrotation
• Duodenal intestinal loop comes out but does not rotate.
• Cecal loop rotates 90 degrees instead of 180 degrees.
• Cecum ends up in the mid-upper abdomen.– Fixed by Ladd’s bands to the right lateral
abdominal wall.• Causes obstruction to duodenum.
31

Children (> 1 month to 2 years)
• Upper– Esophagitis/gastritis– Hypertrophic pyloric stenosis– Peptic ulcer disease– Esophageal varices from portal hypertension
• Lower– Anal fissure– Milk protein allergy– Intussusception– Hernia– Meckel’s diverticulum– Malrotation– Gastroenteritis
32

Upper GI bleed
• Significant bleeding regardless of the cause requires investigation– Gastric lavage to determine continuation of
bleeding– Proton pump inhibitors (IV) shown to reduce the
risk of rebleeding of ulcers, hospital stay and need for transfusion (adult studies)
– H2- receptor antagonists not found to be beneficial (adult studies)
33

Upper GI bleed
– Octreotide for esophageal varices *• Portal venous inflow and intravariceal pressure• 1 microgram/kg over 5 min. then 1 microgram/kg/hr• No great studies in pediatrics• Bleed from esophageal varices has a 30% mortality
rate**
– Endoscopy
*Octreotide in Pediatric Patients*Janice B. Heikenen, †John F. Pohl, ‡Steven L. Werlin, and §John C. BucuvalasJournal of Pediatric Gastroenterology and Nutrition35:600–609 © November 2002 Lippincott Williams & Wilkins, Inc., Philadelphia
**Management of portal hypertension in children. Mileti E, Rosenthal P.Curr Gastroenterol Rep. 2011 Feb;13(1):10-6. University of California, San Francisco, San Francisco, CA 94143-0136, USA. [email protected]
34

Upper GI bleed
• Resuscitation– If hemodynamically compromised
• Two large bore IV• 20cc/kg of normal saline given• Packed red blood cells given 15 cc/kg maintain
hematocrit near 30 g/dl• 5cc/kg PRBC raise Hct 5%• Fresh frozen plasma to correct coagulation
abnormalities 15 cc/kg• Platelet transfusion for platelets < 50
35

Case #4
• 2 year old female with choking episode, now with blood streaked vomitus
Vital Signs:Temp:36.6HR: 135RR:28BP:110/60Pulse ox: 98% on room air
36

Lower GI bleed
• Anal fissure• Gastroenteritis• Intussusception• Milk protein allergy• Meckel’s diverticulum• Malrotation
37

Case #5
15 month old female with chief complaint of lethargy.
Vital Signs:Temp: 37.5HR: 150RR: 32BP 90/54Pulse ox: 97% room air
38

Intussusception
• Most common cause of bowel obstruction ages 3 months to 5 years
• 50% occur between 3 months to 1 year• 80% occur by 2 years• Peak incidence at 7-8 months• 2-4 cases per 1000 live births• Male:female is 2:1• Mortality 1%
39

Intussusception: Presentation
• Severe colicky pain, legs and knees flexed• The infant may initially be comfortable and
play normally between the episodes but then progressively weaker and lethargic
• Less then 15% have the triad of pain, palpable sausage mass and currant jelly stools
40

Intussusception: Pathophysiology
• Telescoping of ileum into colon ileum compressed venous congestion swelling arterial compression ischemia
Bloody stools
41

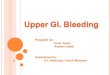
Intussusception: Ultrasound
42
Source undetermined

Intussusception
• Crescent sign LUQ
• Target sign RUQ
• Loss of hepatic outline
43
Source undetermined

Intussusception
• Study in South Africa showed that Burkitt lymphoma presented as intussusception
Intussusception as a presenting feature of Burkitt lymphoma: implications for management and outcome.
England RJ, Pillay K, Davidson A, Numanoglu A, Millar AJ.Department of Paediatric Surgery, Red Cross War Memorial Children's Hospital,
University of Cape Town, Klipfontein Road, Rondebosch, Cape Town, 7700, South Africa, [email protected].
44

Case # 6
• A six week old formula fed infant presents with two stools with a small amount of blood mixed with mucous
Vitals: • Temp: 37• HR: 130• RR: 32• BP: 72/49
Sick or not sick45

Cows milk protein allergy
• Immunologic hypersensitivity reaction to milk proteins
• 2-6% formula fed• 0.5% breast fed infants• 50-60% present with gastrointestinal/skin
symptoms• 30% respiratory symptoms
46

Management
• Removal of cow’s milk from the diet• 30% also allergic to soy• Need hydrolyzed protein formula
47

Finish StudyThe study involved 40 consecutive infants (mean age: 2.7 months) with visible rectal bleeding during a 2-year period at the Tampere University Hospital Department of Pediatrics
•18% turned out to be allergic colitis otherwise no cause was found•Suggested virus played a role
Rectal bleeding in infancy: clinical, allergological, and microbiological examination.Arvola T, Ruuska T, Keränen J, Hyöty H, Salminen S, Isolauri E. Department of Paediatrics, Tampere University Hospital, Tampere, Finland. [email protected]
48

Case #7
11 year old male with lethargy and pale appearance.
Vital signs:Temp: 37.7HR:140BP: 90/60Pulse ox: 95% room air
49

Case #7
• Labs revealed: hemoglobin level of 4.8 g/dl, and a hematocrit of 14.6%
By the way…he has been having bloody stools for 2 weeks
50

Meckel’s Diverticulum• Acid secreting mucosa• 2% (of the population)• 2 feet (from the ileocecal valve)• 2 inches (in length)• 2% are symptomatic• 2 types of common ectopic tissue (gastric and
pancreatic)• 2 years is the most common age at clinical
presentation• 2 times more boys are affected.
51

Meckel’s Diverticulum
• infants and preschool children– slight or massive GI bleeding - painless
• incomplete obliteration of omphalmomestenteric duct– ectopic gastric mucosa in the remnant– ulceration of mucosa across from the diverticulum
• Meckel Scan– Technetium pernechnetate has affinity for gastric
mucosa
52

GI bleeding in AdolescentsUpper•Peptic ulcer/gastritis•Prolapse (traumatic) gastropathy secondary to emesis•Mallory-Weiss syndrome•Coagulopathy •Esophageal varices
Lower•Bacterial enteritis•Inflammatory bowel disease•Colonic polyps•Anal fissure•Meckel’s diverticulum
53

Case # 8
• 2 year old male with history of asthma has ear pain for 2 days, now better after taking omnicef. Mom is concerned because she found blood in his stool.
• Vitals:– 37.5/122/23/97% on room air 96/63
54

Quiz
• 2 year old boy with bilious vomiting and bloody stools since last night. Presents today moderately ill, dehydrated with scaphoid abdomen and no bowel sounds. After ABC what is your next step?
55

• A. Ultrasound of abdomen• B. Upper GI• C. CT of the abdomen• D. Meckel scan• E. Upper endoscopic exam
56

• 12 year old boy S/P Kasai for biliary atresia presents with pruritis, mild icterus and hematemesis. Physical shows an anxious boy with normal vital signs, hepatosplenomegaly and prominent venous pattern over the abdomen. Stools are black and guaic positive. Cause of hematemesis:
57

• A. Peptic Ulcer disease• B. Esophageal varices• C. Posterior nasal bleeding• D. Prolapse gastropathy• E. Thrombocytopenia
58

• 5 year old with intermittent, painless bright red blood per rectum associated with bowel movements for the past 3 months. Inspection of the anus shows no fissures but blood on rectal exam. Most likely cause:
59

• A. Intussusception• B. Juvenile polyp• C. Meckel diverticulum• D. Peptic Ulcer disease• E. Ulcerative colitis
60

• 5 year old girl complains of severe perianal pain on stooling. Physical shows an intensely red, warm and tender perianal tissue. Rectal shows gross blood. What organism is causing these findings?
61

• A. Campylobacter• B. C. Diff• C. Streptococcal• D. Salmonella• E. Shigella
62