Embed Size (px)
Citation preview

Breast Cancer Research and Treatment54: 73–81, 1999.c© 1999Kluwer Academic Publishers. Printed in the Netherlands.
Report
Prognosis, treatment, and recurrence of breast cancer for women attending ornot attending the Screening Mammography Program of British Columbia
Ivo A. Olivotto1,2,4, Donna Mates2, Lisa Kan1, Jonathan Fung2, Rajiv Samant2,3,4, and Linda J.Warren Burhenne1,4
1The Screening Mammography Program of British Columbia and2The Breast Cancer Outcomes Unit, BritishColumbia Cancer Agency, Vancouver, BC, Canada;3The Fraser Valley Cancer Center, Surrey, BC;4The Universityof British Columbia, Vancouver, BC, Canada
Key words:breast cancer, outcomes, prognosis, screening mammography, treatment
Summary
Breast cancer screening programs have been initiated in many countries in the past decade. To determine the impactof the Screening Mammography Program of British Columbia (SMPBC), disease and treatment outcomes for womenwith breast cancer diagnosed in BC between 1989 and 1996 were compared on the basis of attendance at the SMPBC.An SMPBC attender was a women diagnosed with breast cancer within three years of an SMPBC screen, regardlesswhether the cancer was detected as a result of that screen. Of the 13,636 women aged 40–89 years diagnosed withbreast cancer in BC during the study period, 2,647 (19.4%) were SMPBC attenders. 73.5% of SMPBC attenders(N = 1,946) and 74.2% of non-attenders (N = 8,149) were referred to the BC Cancer Agency and had pathology,staging, treatment, and outcome information available. SMPBC attenders compared with non-attenders were morelikely to havein situdisease alone, and those with invasive cancers had smaller tumors which were less likely to havegrade III histology and less likely to have spread to axillary lymph nodes (allP < 0.001). SMPBC attenders weremore likely to be treated with breast conservation and less likely to receive adjuvant chemotherapy or tamoxifen(P < 0.001). Log-rank tests showed local(P = 0.017), distant(P < 0.001), and overall(P < 0.001) disease-freesurvival were better for SMPBC attenders. These favorable surrogate endpoints suggest that the benefits of breastscreening as demonstrated by randomized trials can be translated into community practice by an organized breastscreening program.
Introduction
Randomized clinical trials have demonstrated thatbreast screening with mammography reduces breastcancer specific mortality [1–4]. It has also been sug-gested that women who participate in breast screeningmay have other benefits such as having less radicalor less morbid treatment and more choice about treat-ment options [5]. In the hopes of translating theseresearch findings into benefits for women, organizedbreast screening programs were initiated in manyEuropean countries, Australia, and in eight of tenCanadian provinces between 1987 and 1997.
The purpose of this study was to determine thedegree to which the potential benefits of screeningmammography are being translated into practice by
an organized breast screening program. To do this,comparisons of the prognostic factors of the breastcancers diagnosed, treatment outcomes, and the patternof care received were made for women referred to theBritish Columbia Cancer Agency (BCCA), who hadeither attended the Screening Mammography Programof British Columbia (SMPBC) or had not attended theSMPBC. Attenders were women who had attended theSMPBC within three years prior to the diagnosis ofbreast cancer, regardless of whether the breast cancerwas detected at that screening. Non-attenders werewomen who did not attend the SMPBC within threeyears prior to the diagnosis of breast cancer, whethertheir breast cancers were diagnosed as palpable tumorsor by opportunistic screening in diagnostic facilities.In particular, we wanted to determine whether SMPBC

74 IA Olivotto et al.
attendance was associated with more favorable prog-nosis, better survival, and/or the use of less radical orless morbid treatment for women diagnosed with breastcancer when compared to other women with breast can-cer from the same geographically-defined populationdiagnosed over the same time-interval.
Methods
Context and data sources
The SMPBC is the longest running organized breastscreening program in Canada. It was initiated as a sin-gle fixed site in Vancouver in July, 1988 [6]. By 1997,geographic coverage of the province was achieved with23 services employing a variety of delivery modesincluding four mobile vans. Asymptomatic female res-idents of BC, Canada, age 40 and older are eligibleto attend for an annual, bilateral, two-view, screeningmammogram with no direct financial charge to the par-ticipant. Appointments are scheduled at the request ofthe women or by a physician’s referral. Recruitmentis currently targeted to women aged 50–74 years. Aphysical examination is not conducted at the screen-ing centre. Results are communicated to the womanand a designated family physician. Women with breastsymptoms, previous breast cancer, breast implants, orthose pregnant or lactating are not eligible to attendthe SMPBC but may be referred for mammography atcommunity diagnostic facilities. The provincial cancerregistry regularly notifies the SMPBC of all new breastcancers diagnosed in BC [7]. The SMPBC collects dataon all invasive orin situ breast cancers diagnosed inwomen who have previously attended the SMPBC andconducts a central pathology review on those cancers.The review diagnosis is used for recording pathologicalcharacteristics. The annual volume of SMPBC screensincreased each fiscal year (April 1 to March 31 ofthe following year) from 7,100 screens in 1988/89 to167,221 screens in 1996/97. The female population age40–89 years in BC increased from 645,949 in 1989 to828,715 in 1996 [8].
Mammography for diagnostic purposes is alsowidely available in BC and is an insured service ofthe provincial, universal-access health insurance plan.It has been estimated that a significant proportion of thebilateral mammograms performed in community diag-nostic facilities are for screening purposes [9]. Breastcancers detected by mammography in these facilitieswere not considered SMPBC-detected. The proportionof bilateral mammography services performed eachyear in BC that were provided by the SMPBC increased
as the program expanded, from less than 5% in 1989to 65% in 1996 [10].
The BCCA has the mandate of cancer control forthe BC population. This includes operation of four re-gional cancer centres delivering all radiation therapyin the province and the management of the budget forall antineoplastic drugs [11]. It also includes operationof the SMPBC, the provincial Pap-smear program, andthe BC Cancer Registry. A Breast Cancer OutcomesUnit (BCOU) at the BCCA maintains a database whichincludes demographic, pathology, staging, treatment,and recurrence information, and for deceased patientsthe date and cause of death, for all women diagnosedwith breast cancer and referred to the BCCA since Jan-uary 1, 1989. Unfortunately, although histology, site,age, sex, and date of diagnosis are collected by theBC Cancer Registry for all cancers diagnosed in BC,detailed pathology, staging, and treatment informationis not available. Cases referred to a BCCA facilitywith node-negative breast cancer and selected node-positive cases have a central pathology review and thisreview is used to classify pathology characteristics.Individual data on race, education, and income arenot prospectively collected and were not available foranalysis.
Subjects
Study subjects were all women with invasive orinsitu breast cancer diagnosed in BC between January1, 1989, and December 31, 1996. Since the SMPBCwas only accessible to female BC residents over theage of 40 years and screening participation is rarein women 90 years of age or older, women youngerthan 40 years and older than 89 years were excluded.The SMPBC is a screening program for asymptomatic,well women. Women who are pregnant or lactatingand those with a prior diagnosis of breast cancer arenot eligible to attend. To make the attender and non-attender groups as comparable as possible, cases withbreast cancer diagnosed from a death certificate, sur-viving ≤ 30 days from diagnosis (they would likelyhave been symptomatic), with a previous history ofbreast cancer (before 1989) or breast cancer diagnosedduring pregnancy, were excluded fom both the SMPBCand non-SMPBC groups. For women with bilateralbreast cancer diagnosed from 1989 to 1996, the firstdiagnosed breast cancer was included. For women withbilateral breast cancer diagnosed on the same date, thecancer with the higher pathological T-stage was usedin the analysis.

Breast screening attendance and outcomes75
Analyses
An electronic file of all SMPBC attendees with invasiveor in situ breast cancer diagnosed before January 1,1997, was merged with the BCOU and Cancer Registrydatabases using the patient’s unique personal healthnumber, Cancer Registry number, name, and dateof birth as matching parameters. Over 99% of caseswere matched successfully. SMPBC attenders includedboth screen-detected cases (diagnosed as a result ofan abnormal SMPBC screen) and post-screen casesdiagnosed within three years of a ‘normal’ SMPBCscreen or an abnormal screen for which a subsequentdiagnostic work-up had concluded without a diagno-sis of malignancy. All other cases were considered tobe SMPBC non-attenders. Some of these cases mayhave been detected by mammography in communitydiagnostic facilities. Interval cancers in a screeningprogram with, at that time, a policy to recall womenannually are those which occur within one year of anormal screening visit [7]. Including in the SMPBCattenders group, women with breast cancers diagnosedwithin three years of a screening visit was intentionallyconservative.
Approximately 74% of newly diagnosed breast can-cers are referred to the BCCA each year. Staging,treatment, and recurrence information are known forthese referred cases. Cases not referred to the BCCAfor initial consultation and treatment have usually beentreated with mastectomy and therefore do not usu-ally need radiation therapy. They also tend to havelower risk histology without indications for systemictherapy [11]. Detailed pathology, staging, and treat-ment information is not collected for the non-referredcases. Comparisons of pathology, treatment, and out-comes were therefore restricted to BCCA-referredcases (74%) regardless of SMPBC attendance. Local,regional, or distant recurrences and deaths from breastcancer reported within the BCOU by March 1, 1998,were analyzed. Subjects were censored from assess-ment of local recurrence after a regional recurrenceand from local or regional recurrence after a distantrecurrence. Three percent of subjects were consideredlost to follow-up and censored on the date of last contactbecause there was no known contact in the year priorto the date of analysis.
SPSS statistical software (SPSS Inc, version 6.1.2,Chicago, 1995) was used for analyses. Differencesbetween SMPBC attenders and non-attenders with re-spect to various prognostic and treatment variableswere tested using the Pearson chi-square statistic.Disease-free survival, defined as being free of regionaland/or distant recurrence or death from breast cancer,
for SMPBC attenders and non-attenders was estimatedusing the Kaplan–Meier method and compared usingthe log-rank statistic.
Results
Proportion of cancers detected by the SMPBC
There were 15,957 women between the ages of 40–89 years with a new diagnosis of breast cancer in BCbetween January 1, 1989, and December 31, 1996.Of these, 13,636 met eligibility criteria and form thestudy group. There were 603 women with bilateralbreast cancer and of these, 158 were diagnosed on thesame date. The median follow-up was 33 months forSMPBC attenders and 46 months for non-attenders.There were 2,647 (19.4%) cancers diagnosed amongSMPBC attenders and 10,989 cancers (80.6%) diag-nosed among SMPBC non-attenders. Of the cancersdiagnosed in SMPBC attenders, 1,962 (14.4% of allcancers) were screen-detected and 685 (25.9% of can-cers in SMPBC attenders) were detected within threeyears of an SMPBC exam but were not screen-detected(post-screen cancers). The post-screen cases were de-tected within one(n = 332), two (n = 200), or threeyears(n = 153) after their last screen.
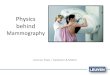
As the SMPBC expanded, SMPBC attenders ac-counted for an increasing proportion of cancers diag-nosed each year, increasing from 3% of breast cancersin BC newly diagnosed in 1989 to 30% in 1996 (Fig-ure 1). The overall SMPBC cancer detection rate fellfrom 4 cancers per 1000 participants in 1989 to 3.4cancers per 1000 participants in 1996 as an increas-ing proportion of SMPBC services were provided towomen returning for second and subsequent screens.Returning participants and younger women had lowercancer detection rates [12]. Over the entire study pe-riod, SMPBC attenders accounted for 19.5%, 24.2%,30.2%, and 26.1% of the cancers among women age40–49, 50–59, 60–69 and 70+ years, respectively.
Table 1 shows the distribution of factors associatedwith BCCA referral. The overall likelihood of BCCAreferral for SMPBC attenders and non-attenders wasremarkably similar, 73.5% and 74.2%, respectively.The proportion of cases referred to the BCCA annuallybetween 1989 and 1996 was 74.1 ± 2.4%. Youngerwomen (P < 0.001) and those living in urban ar-eas(P < 0.001) were more likely to be referred tothe BCCA for consultation regarding their primary oradjuvant therapy, whether SMPBC attenders or non-attenders. Complete pathology information is availablefor all SMPBC cases. Patients with indications for

76 IA Olivotto et al.
Figure 1. Between 1989 and 1996, an increasing proportion of women with newly diagnosedin situ or invasive breast cancer in BritishColumbia had attended the SMPBC within three years prior to their diagnosis of breast cancer (SMPBC attenders).
Table 1. Number and proportion of cases referred to the BC Cancer Agency(1989–1996)
SMPBC1 attenders SMPBC1 non-attendersN Referred (%) N Referred (%)
All referred 2,647 1,946 73.5 10,989 8,149 74.2
Age40–49 517 423 81.8 2,201 1,913 86.950–59 641 502 78.3 2,096 1,742 83.160–69 799 592 74.1 2,735 2,113 77.370+ 690 429 62.2 3,957 2,381 60.2
PathologyInvasive 2,369 1,712 72.3 10,187 7,523 73.8In situalone 278 234 84.2 802 626 78.1
Residence2
Urban 2,263 1,713 75.7 9,268 7,020 75.7Rural 363 229 63.1 1,644 1,115 67.8Unknown 21 4 19.0 77 14 18.2
1SMPBC is the Screening Mammography Program of British Columbia.2Urban and rural residence is defined by the postal code forward sortation area.

Breast screening attendance and outcomes77
Table 2. Prognostic variables of cancers for BC Cancer Agency referred subjects
SMPBC1 attenders SMPBC1 non-attenders Pearsonχ2
N (%) N (%) P (sig)
PathologyInvasive 1,712 88.0 7,523 92.3 < 0.001In situalone 234 12.0 626 7.7
Tumor size (mm)2
0–10 503 29.4 1,594 21.2 < 0.00111–20 647 37.8 2,339 31.121–50 362 21.1 2,378 31.6> 50 51 3.0 507 6.7Unknown/missing 149 8.7 705 9.4
Median tumor size (mm)2 15 19 < 0.0013
Histologic grade2
I 266 15.5 728 9.7 < 0.001II 834 48.7 3,076 40.9III 486 28.4 2,756 36.6Unknown/missing 126 7.4 963 12.8
Lymphatic/vascular invasion2
Absent 1,123 65.6 3,887 51.7 < 0.001Present 485 28.3 2,693 35.8Unknown/missing 104 6.1 943 12.5
Axillary node involvement2
Absent 1,138 66.5 3,808 50.6 < 0.001Present 432 25.2 2,602 34.6Unknown/missing 142 8.3 1,113 14.8
Overall stage4
0 234 12.0 626 7.7 < 0.001I 895 46.0 2,545 31.2II 514 26.4 2,977 36.5III 62 3.2 556 6.8IV 22 1.1 413 5.1Unknown/missing 219 11.3 1,032 12.7
1SMPBC is the Screening Mammography Program of British Columbia.2Invasive cases only.3Kruskal-Wallis 1-way ANOVA.4UICC 1997 TNM staging [13]. Cases without axillary pathology and no palpable axillary lymphnodes are assumed to be node-negative.In situcases are assumed to have no metastases.
adjuvant systemic therapy or radiation therapy weremore likely to be referred to the BCCA. For example,SMPBC cases referred to the BCCA were more likelyto have invasive cancer, nodal spread, grade III histol-ogy, or peritumoral lymphatic or vascular invasion (allP < 0.05) compared to SMPBC cases not referred tothe BCCA. There was no difference in the size distri-bution of the cancers(P = 0.64) comparing SMPBCreferred cases to those not referred to the BCCA.
Prognosis of cancers among SMPBC attenders andnon-attenders
Table 2 shows the distribution of prognostic factors forcancers diagnosed in BCCA referred, SMPBC atten-ders and non-attenders. The SMPBC cases were morelikely to have purein situ disease. Invasive cancersdiagnosed in SMPBC attenders were smaller, had amore favorable distribution of grades, and were less

78 IA Olivotto et al.
Table 3. Treatment of BC Cancer Agency referred women with invasive breast cancers(1989–1996)
SMPBC1 attenders SMPBC1 non-attenders Pearsonχ2
N (%) N (%) P (sig)
Definitive breast surgeryBreast conservation 1,109 64.8 4,071 54.1 < 0.001Total mastectomy 603 35.2 3,452 45.9
Axillary dissection 1,578 92.2 6,539 86.9 < 0.001Radiation therapy after BCS 1,084 91.6 3,688 87.6 < 0.001
Adjuvant systemic therapy2
None 814 47.5 2,680 35.6 < 0.001Tamoxifen alone 493 28.8 2,694 35.8Chemotherapy 392 22.9 2,060 27.4Other 6 0.4 37 0.5Missing 7 0.4 52 0.7
1SMPBC is the Screening Mammography Program of British Columbia.2Cases receiving both tamoxifen and chemotherapy are included as receiving chemotherapy.
Table 4. Five-year actuarial relapse of women with BC Cancer Agency referred, invasive breast cancers (1989–1996)
Type of relapse SMPBC1 attenders SMPBC1 non-attenders Attenders vs. non-attenders2
(%) (%) (P sig)
Local 4.9 7.2 0.017Regional 4.7 5.2 0.136Distant 10.5 19.6 < 0.001Any regional or distant relapse 15.5 27.2 < 0.001or death from breast cancer
1SMPBC is the Screening Mammography Program of British Columbia.2Probability of Kaplan–Meier log-rank statistic.
likely to have spread to lymphatic or vascular spacesin the primary tumor or to axillary lymph nodes (allP < 0.001). These findings are reflected in the over-all stage distribution, with more Stage 0–I and fewerStage II–IV presentations among the SMPBC cases(P < 0.001).
Treatment received by SMPBC attenders and non-attenders
Table 3 shows the treatment received by BCCA-referred subjects with invasive breast cancer. Womenattending the SMPBC were more likely to be treatedwith breast conserving surgery and less likely to receivechemotherapy, tamoxifen, or both. The majority ofwomen with invasive breast cancer had axillary lymphnode dissection although this was done slightly moreconsistently for attenders. If treated with breast conser-
vation, a high proportion of both groups had radiationtherapy to the breast, again slightly more consistentlyfor attenders.
Patterns of recurrence for SMPBC attenders and non-attenders
Table 4 shows that for women with invasive breastcancer, SMPBC attenders had lower five-year actuarialrates of local(P = 0.017) and distant recurrence(P <
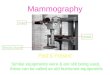
0.001) compared to non-attenders. Figure 2 showsthe Kaplan–Meier disease-free survival for SMPBCattenders and non-attenders with invasive breast can-cer. The five- and seven-year disease-free survivalrates are higher for SMPBC attenders compared tonon-attenders(P < 0.001).

Breast screening attendance and outcomes79
Figure 2. Disease-free survival for women with invasive breast cancer diagnosed in BC between 1989 and 1996 and referred to the BCCancer Agency. Disease-free survival was better for women diagnosed within three years of attendance at the Screening MammographyProgram of BC (SMPBC attenders) compared to women who did not attend the SMPBC(P < 0.001). SMPBC attendance is notsynonymous with a cancer being mammographically detected (see text).
Discussion
Since initiation of an organized mammographic screen-ing program in British Columbia in 1988, increasingproportions of the women diagnosed with breast cancereach year in the province have been SMPBC attenders.Nearly 75% of both the SMPBC attenders and non-attenders were referred to the BCCA and had prognos-tic, treatment, and outcome information available. Thecancers diagnosed in women within three years of at-tendance at the screening program were histologicallymore favorable, smaller, and less likely to have spreadto axillary lymph nodes compared to other womenwith breast cancer diagnosed over the same interval inBritish Columbia. SMPBC attenders were more likelyto be treated with breast conserving surgery and lesslikely to be subjected to the side-effects of adjuvantchemotherapy or tamoxifen. Even with this less radicalinitial therapy, the five- and seven-year actuarial ratesof freedom from recurrence are significantly better forwomen who attended the SMPBC.
The decision to offer regular mammographicscreening is based on the demonstration of reducedbreast cancer-specific mortality in prospective ran-domized clinical trials [1–4]. Observations of more
favorable stage and histologic features and better sur-vival for screen-detected cancers are, by themselves,insufficient evidence to recommend investing in breastscreening as public health policy because of the prob-lems of lead-time bias and the healthy volunteer phe-nomenon as discussed elsewhere [5, 14]. This study isnot an assessment of the efficacy of screening mam-mography. Rather, this is an analysis of whether thepotential benefits of screening as proven in randomizedtrials, can be translated into community practice.
In the randomized trials of breast screening, com-parison of the prognostic profile of cancers detectedin the invited as compared with the control groupshas identified surrogate intermediate endpoints asso-ciated with the mortality reductions in those trials[15, 16]. These endpoints include such factors asthe proportion of cancers smaller than 15 mm diam-eter or free of lymph node involvement at diagnosis.It has been suggested that these intermediate end-points might be useful to predict the likelihood thatan organized breast screening program will achieve itsmandate of mortality reduction on a population basis[17].
The prognostic profile of screen detected cancerswithin the SMPBC meet or exceed the targets derived

80 IA Olivotto et al.
from the randomized trials [12]. This study also demon-strates significant advantages in terms of prognosis,treatment, and recurrence for women who attendedthe screening program when compared to other breastcancer cases diagnosed in the same geographically-defined population over the same time interval. Thiswas observed even though the post-screen cancers wereincluded with the attenders. These results indicate thatit is possible to translate the benefits seen in randomizedtrials of breast screening, into a general populationin North America. A better prognosis for screen-ing program attenders has also been demonstrated inScandinavia [18, 19].
Since the mid 1990s, there has been a modest de-cline in breast cancer-specific mortality rates in Canadaand the USA [20, 21]. Some of this decline is likelydue to the increasing use of screening mammography.However, the use of adjuvant systemic therapy has alsoimproved considerably since the early 1980s, and hascontributed in part to the falling mortality rates [22–24].Crude breast cancer-specific mortality cannot be usedto evaluate the impact of screening mammography untilthe majority of women are routinely participating. Evenwith the organization and publicity of the SMPBC,fewer than 35% of the age-eligible female populationwas participating in this program in 1996/97 [12].
There has been a suggestion that the favorablesize distribution of cancers detected in the non-mammographic arm of the Canadian National BreastScreening Study may explain the lack of ability todemonstrate a survival advantage for the screening in-tervention in that trial [25]. If the usual medical care ofwomen in Canada was such that the prognostic profileof community-detected cancers was very good, onecould question the value of implementing organizedbreast screening programs on a population-wide basis.However, this study suggests that women who haveattended the SMPBC, if diagnosed with breast cancer,have a significantly better prognosis than women whohave not attended the SMPBC within three years ofdiagnosis. This observation holds even though the post-screen cancers, which have been shown previously tohave a worse prognosis than SMPBC-detected cases[7], were included with the attenders and women withmammographically-detected cancers from diagnosticfacilities were included with the non-attenders. Fur-thermore, the non-attenders received more adjuvantsystemic therapy, a factor which if anything shouldhave minimized observed differences in recurrencebetween the groups [22].
A limitation of the current study is the inability toreport on detailed pathology, staging, treatment, andoutcome information for the women not referred to aBCCA facility. In a national health survey, Canadianwomen who reported having recent mammography hadhigher levels of educational achievement and incomeadequacy compared to women who reported not havingrecent mammograms [9]. Such women are also morelikely to be treated with breast conservation, and ifso, to be referred to the BCCA for definitive radiationtherapy [26, 27]. On the other hand, previous studiesof women with node-negative breast cancer in BC haveshown that patients with worse prognostic features andtherefore an indication for chemotherapy or tamoxifenindependent of socioeconomic factors are also morelikely to be referred to the BCCA [11, 28]. Althoughit was not possible to assess this directly, these factorswere likely to be operating similarly among SMPBC at-tenders and non-attenders, because their observed ratesof BCCA referral were almost identical and the annualrates of referral were relatively constant between 1989and 1996.
The primary objective of organized breast cancerscreening is to reduce morbidity and mortality frombreast cancer. Organized programs have been initiatedin many areas of North America, Europe, and Australiain the past decade. For many programs including theSMPBC, adequate compliance, in the 70% and greaterrange as achieved in the randomized trials, has not beenrealized. This remains a challenge. In particular, it isdiscouraging that even with the availability of screen-ing on demand in BC, the majority of women withnewly diagnosed breast cancer in 1996 were not de-tected through the screening program. This analysis haspointed out the need and potential value of substantiallyincreasing recruitment to the SMPBC. A major initia-tive to increase participation in regular breast cancerscreening was launched in the fall of 1997. The goal isto reduce the number of palpable non-screen detectedcancers in BC by half within the next five years. Successwill depend on enhancing access and convincing healthcare providers and the public of the benefits of regularattendance for screening.
Acknowledgements
The authors thank Jeannine Soltys and Carol-Anne Kamitakahara for assistance in preparing themanuscript.

Breast screening attendance and outcomes81
References
1. Larsson L-G, Andersson I, Bjurstam N, Fagerberg G, FrisellJ, Tabar L, Nystrom L: Updated overview of the Swedishrandomized trials on breast cancer screening with mam-mography: age group 40–49 at randomization. Monogr NatlCancer Inst 22: 57–61, 1997
2. Nystrom L, Rutqvist LE, Wall S, Lindgren A, Lindqvist M,Ryden S, Andersson I, Bjurstam N, Fagerberg G, Frisell J,Tabar L, Larsson LG: Breast cancer screening with mam-mography: overview of Swedish randomised trials. Lancet341: 973–978, 1993
3. Kerlikowske K: Efficacy of screening mammographyamong women aged 40 to 49 and 50 to 69 years: comparisonof relative and absolute benefit. Monogr Natl Cancer Inst 22:79–86, 1997
4. Hendrick RE, Smith RA, Rutledge JH, Smart CR: Benefitof screening mammography in women age 40–49: a newmeta-analysis of randomized controlled trials. Monogr NatlCancer Inst 22: 87–92, 1997
5. National Institutes of Health Consensus DevelopmentPanel: National Institutes of Health consensus developmentconference statement: breast cancer screening for womenages 40–49, January 21–23, 1997. J Natl Cancer Inst 89:1015–1026, 1997
6. Clay MG, Hislop TG, Kan L, Olivotto IA, Warren BurhenneLJ: Screening mammography in British Columbia: 1988–1993. Am J Surg 167: 490–492, 1994
7. Hislop TG, Worth AJ, Kan L, Rousseau E: Post screen-detected breast cancer within the Screening MammographyProgram of British Columbia. Breast Cancer Res Treat 42:235–242, 1997
8. B.C. Stats.: Population estimates (1976, 1981, 1986,1991–1997) and projections (1998–2026). B.C. Ministry ofFinance and Corporate Relations.
9. Gaudette LA, Altmayer CA, Nobrega KMP, Lee J: Trendsin mammography utilization, 1981 to 1994. Health Reports8: 17–27, 1996
10. Olivotto IA, Kan L, Mates D, King S: Pattern of use andhealth system costs for bilateral mammography in BritishColumbia since initiating the Screening MammographyProgram of British Columbia. Can Med Assoc J 1998 (inpress).
11. Olivotto IA, Coldman AJ, Hislop TG, Trevisan CH, KulaJ, Goel V, Sawka C: Compliance with practice guidelinesfor node-negative breast cancer. J Clin Oncol 15: 216–222,1997
12. Screening Mammography Program of British Columbia:1996–1997 annual report
13. Sobin LH, Wittekind C (eds): TNM Classification of ma-lignant tumours, UICC 5th edition. Wiley-Liss, New York,1997
14. Feig SA: Methods to identify benefit from mammographicscreening of women aged 40–49 years. Radiology 201: 309–316, 1996
15. Tabar L, Fagerberg G, Duffy SW, Day NE, Gad A, GrontoftO: Update of the Swedish two-county program of mammo-graphic screening for breast cancer. Radiol Clin North Am30: 187–210, 1992
16. Feig SA: Determination of mammographic screening inter-vals with surrogate measures for women aged 40–49 years.Radiology 193: 311–314, 1994
17. Sickles EA: Breast cancer screening outcomes in womenages 40–49: Clinical experience with service screening us-ing modern mammography. Monogr Natl Cancer Inst 22:99–104, 1997
18. Norden T, Thurfell E, Hasselgren M, Lindgren A, NorgrenA, Bergstrom R, Holmberg L: Mammographic screeningfor breast cancer. What cancers do we find? Eur J Cancer33: 624–628, 1997
19. Hakama M, Pukkala E, Heikkila M, Kallio M: Effectivenessof the public health policy for breast cancer screening inFinland: population based cohort study. Br Med J 314: 864–867, 1997
20. Gaudette LA, Gao RN, Wysocki M, Nault F: Update onbreast cancer mortality, 1995. Health Reports 9: 31–34,1997
21. Chu KC, Tarone RE, Kessler LG, Ries LAG, Hankey BF,Miller BA, Edwards BK: Recent trends in U.S. breast cancerincidence, survival and mortality rates. J Natl Cancer Inst88: 1571–1579, 1996
22. Early Breast Cancer Trialists’ Collaborative Group: Sys-temic treatment of early breast cancer by hormonal, cy-totoxic or immune therapy: 133 randomized trials involv-ing 31,000 recurrences and 24,000 deaths among 75,000women. Lancet 399: 1–15, 71–85, 1992
23. Olivotto IA, Bajdik C, Plenderleith IH, Coppin CML,Gelmon KA, Jackson SM, Ragaz J, Wilson KS, Worth A:Adjuvant systemic therapy and survival from breast cancer.N Engl J Med 332: 805–810, 1994
24. Johnson TP, Ford L, Warnecke RB, Nayfield SG, KaluznyA, Cutter G, Gillings D, Sondik E, Ozer H: Effect of aNational Cancer Institute clinical alert on breast cancerpractice patterns. J Clin Oncol 12: 1783–1788, 1994
25. Narod SA: On being the right size: a reappraisal of mam-mography trials in Canada and Sweden. Lancet 349 (letter):1846, 1997
26. Hislop TG, Olivotto IA, Coldman AJ, Trevisan CH, Kula J,McGregor GI, Phillips N: Variations in breast conservationsurgery for women with axillary lymph node negative breastcancer in British Columbia. Can J Public Health 87: 390–394, 1996
27. Goel V, Olivotto I, Hislop TG, Sawka C, Coldman A,Holowaty EJ: Patterns of initial management of node-negative breast cancer in two Canadian provinces. Can MedAssoc J 156: 25–35, 1997
28. Sawka C, Olivotto I, Coldman A, Goel V, Holowaty E,Hislop TG: The association between population-basedtreatment guidelines and adjuvant therapy for node-negative breast cancer. Br J Cancer 75: 1534–1542, 1997
Address for offprints and correspondence:Ivo A. Olivotto, FR-CPC, Medical Leader, Screening Mammography Program ofBritish Columbia, BC Cancer Agency, 600 West 10th Avenue,Vancouver, BC, Canada, V5Z 4E6;Tel: 604-877-6000;Fax:604-877-0505;E-mail: [email protected]