Embed Size (px)
Citation preview

Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 I
Editorial Board
Print ISSN 2393-8692
Patrons Dr. D. Y. Patil (Founder President) Dr. Vijay D. Patil (President)
Advisors Prof. B. P . Sable (Chancellor) Dr. Sanjay Oak (Vice Chancellor) Dr. B. M. Hirdekar (Registrar) Mr. Uday Shende (Director)
Dr. Omkar Shetty (Dean)
Editor-in-chiefDr. Avinash P. Tamgadge (Vice Dean)
Joint EditorDr. Subraj Shetty
Editors Dr. Vivek P. Soni Dr. Rupinder Bhatia Dr. Sandeep S. Pagare Dr. Lalitagauri Mandke Dr. Arvind Shetty Dr. Mukul Padhye
Dr. Sheeba Gomes
Associate Editors Dr. S. S. Bhalerao Dr. Treville Pereira Dr. Sandhya Tamgadge Dr. Q. J. A Shakir Dr. Devanand Shetty Dr. Poonam Singh Dr. Roshni Thakur Dr. Sandeep Sharma Dr. Sameer Narkhede Dr. Leena Padhye Dr. Sumita Bhagwat Dr. Vimala N. Dr. Charushila S. Sardar Dr. Asha Rathod Dr. Gaurang Mistry Dr. Rajiv Singh Dr. Ashok Dabir Dr. Gitanjali Mandlik Dr. Gokul Venkateshwar Dr. Vasavi K. Dr. Sonal Vahanwala Dr. Mandavi Waghmare Dr. Uma Dixit Dr. Maina Gite Dr. Yogesh Kini Dr. Rubina Tabassum
Executive Editors Dr. Swati Gotmare Dr. Frank Mehta Dr. Unmesh Khanvilkar Dr. Karthik Shetty Dr. Sushma Sonawane Dr. Ashwini Kini Dr. Charu Girotra Dr. Naveenkumar Shetty Dr. Akshata Prabhu Dr. Shilpa Naik
Official Publication of D. Y. Patil University, School of Dentistry
Indian Journal of Oral Health and Research

II Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
Copyright
The entire contents of the Indian Journal of Oral Health and Research are protected under Indian and international copyrights. The Journal, however, grants to all users a free, irrevocable, worldwide, perpetual right of access to, and a license to copy, use, distribute, perform and display the work publicly and to make and distribute derivative works in any digital medium for any reasonable non-commercial purpose, subject to proper attribution of authorship and ownership of the rights. The journal also grants the right to make small numbers of printed copies for their personal non-commercial use.
Permissions
For information on how to request permissions to reproduce articles/information from this journal, please visit www.ijohr.org.
Disclaimer
The information and opinions presented in the Journal reflect the views of the authors and not of the Journal or its Editorial Board or the Publisher. Publication does not constitute endorsement by the journal. Neither the Indian Journal of Oral Health and Research nor its publishers nor anyone else involved in creating, producing or delivering the Indian Journal of Oral Health and Research or the materials contained therein, assumes any liability or responsibility for the accuracy, completeness, or usefulness of any information provided in the Indian Journal of Oral Health and Research, nor shall they be liable for any direct, indirect, incidental, special, consequential or punitive damages arising out of the use of the Indian Journal of Oral Health and Research. The Indian Journal of Oral Health and Research, nor its publishers, nor any other party involved in the preparation of material contained in the Indian Journal of Oral Health and Research represents or warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from the use of such material. Readers are encouraged to confirm the information contained herein with other sources.
AddressesEditorial OfficeDr. Avinash P. TamgadgeVice Dean, Professor and Head,Department of Oral Pathology and Microbiology,D.Y. Patil University, School of Dentistry,Nerul, Navi Mumbai-400 706, India.Ph: (+91) 9819619494Email: [email protected] Website: www.ijohr.org
Published byWolters Kluwer India Private LimitedB9, Kanara Business Centre,Off Link Road, Ghatkopar (E), Mumbai – 400075, India.Phone: 91-22-66491818 Website: www.medknow.com
Printed atNikeda Art Printers Pvt Ltd, Bhandup, Mumbai, India.
The journal
Indian Journal of Oral Health and Research (ISSN: Print 2393-8692), a publication of D. Y. Patil University, School of Dentistry, Navi Mumbai, is a peer-reviewed online journal with Semiannual print on demand compilation of issues published. The journal’s full text is available online at http://www.ijohr.org. The journal allows free access (Open Access) to its contents and permits authors to self-archive final accepted version of the articles on any OAI-compliant institutional / subject-based repository.
Abstracting and indexing informationThe journal is indexed/listed with British Library, CNKI (China National Knowledge Infrastructure), EBSCO Publishing’s Electronic Databases, Google Scholar, Journal Guide, Kudos, National Science Library, OpenJGate and TdNet.Information for AuthorsThere are no page charges for IJOHR submissions. Please check http://www.ijohr.org/contributors.asp for details.
All manuscripts must be submitted online at www.journalonweb.com/ijohr.
Subscription InformationCopies are sent to the members of ISN free of cost. A subscription to Indian Journal of Oral Health and Research comprises 2 issues. Prices include postage. Annual Subscription Rate for non-members-
•Institutional: INR 3000.00 for India USD 300.00 for outside India
•Personal: INR 1500.00 for India USD 150.00 for outside India
For mode of payment and other details, please visit www.medknow.com/subscribe.asp.
Claims for missing issues will be serviced at no charge if received within 60 days of the cover date for domestic subscribers, and 3 months for subscribers outside India. Duplicate copies cannot be sent to replace issues not delivered because of failure to notify publisher of change of address.
The journal is published and distributed by Wolters Kluwer India Private Limited. Copies are sent to subscribers directly from the publisher’s address. It is illegal to acquire copies from any other source. If a copy is received for personal use as a member of the association/society, one cannot resale or give-away the copy for commercial or library use.
The copies of the journal to the members of the Institute are sent by ordinary post. The editorial board, association or publisher will not be responsible for non receipt of copies. If any member/subscriber wishes to receive the copies by registered post or courier, kindly contact the publisher’s office. If a copy returns due to incomplete, incorrect or changed address of a member/subscriber on two consecutive occasions, the names of such members will be deleted from the mailing list of the journal. Providing complete, correct and up-to-date address is the responsibility of the member/subscriber.Nonmembers: Please send change of address information to [email protected] policiesThe journal accepts display and classified advertising. Frequency discounts and special positions are available. Inquiries about advertising should be sent to Wolters Kluwer India Private Limited, [email protected] journal reserves the right to reject any advertisement considered unsuitable according to the set policies of the journal.The appearance of advertising or product information in the various sections in the journal does not constitute an endorsement or approval by the journal and/or its publisher of the quality or value of the said product or of claims made for it by its manufacturer.
Official Publication of D. Y. Patil University, School of Dentistry
Indian Journal of Oral Health and Research
General Information

Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 III
CONTENTS
Vol 2 | Issue 1 January-June 2016
REVIEW ARTICLESThe Challenges of Cancer SurvivorsAshok K. Vikey, Deepali Gupta Vikey ........................................................................................................................ 1
Resorptive Cells in Health and DiseaseSwati Gautam, Arvind Sharma, Deepti Garg ............................................................................................................. 5
Cytokines and Other Inflammatory Mediators in Periodontal Health and DiseaseHarpreet Singh Grover, Rohit Saini, Pearl Bhardwaj, Amit Bhardwaj ...................................................................... 12
ORIGINAL ARTICLESRadiation Protection Awareness and Practices in Cameroon Dental Health Care FacilitiesAshu Michael Agbor, Clement Chinedu Azodo ........................................................................................................ 17
Association between Smoking, Body Mass Index, and Periodontal Disease: A Case–Control StudyShelly Arora, Srinivas Sulugodu Ramachandra, Kalyan C. Gundavarapu .............................................................. 23
Clinical Evaluation of Caries Removal in Primary Teeth Using Carie‑care and SmartPrep Burs: An In vivo StudyPooja Ravindra Shivasharan, A. Katge Farhin, Mayur Manohar Wakpanjar, Ashveeta Shetty ............................... 27
Dermatoglyphics: A Plausible Role in Dental Caries and Malocclusion?A. Deepti, Kapil Dagrus, Vandana Shah, M. Harish, Deepak Pateel, Nidhi Shah ................................................... 32
CASE REPORTSUnicystic Ameloblastoma Developing into a Hybrid Lesion of Rare Entity ‑ with Review of LiteratureSavina Gupta, Mukul Nandkumar Padhye, Gokul Venkateshwar, Sandhya Tamgadge, Hirkani Attarde ................ 36
Centroblastic Variant of Non‑Hodgkin’s Lymphoma of Mandible: A Rare Case ReportAnuradha E. Sunil, P. C. Anila Namboodiripad, Archana Mukunda, Neethu Kadar, K. A. Jassim ........................... 42
Management of Dentoalveolar Trauma in Late Mixed DentitionRupinder V. Bhatia, Ashwin Jawdekar, Namrata R. Mathrawala ............................................................................. 46
Peripheral Ossifying FibromaSonal Srivastava, Manaswita Tripathy, B. R. Chethan, Joel Dsilva ......................................................................... 51
An Unusual Case of Maxillary Central Giant Cell GranulomaRuchika Kapoor, Freny Rashmiraj Karjodkar, Kaustubh Sansare, Amaresh Chandra Dora ................................... 55
Official Publication of D. Y. Patil University, School of Dentistry
Indian Journal of Oral Health and Research

IV Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
The Indian Journal of Oral Health and Research now accepts articles electronically. It is easy, convenient and fast. Check following steps:
Indian Journal of Oral Health and Research on Web
Facilities
•Submission of new articles with images•Submission of revised articles•Checking of proofs•Track the progress of article until published
Advantages
•Any-time, any-where access•Faster review•Cost saving on postage•No need for hard-copy submission•Ability to track the progress•Ease of contacting the journal
Requirements for usage
•Computer and internet connection•Web-browser (Latest versions - IE,
Chrome, Safari, FireFox, Opera)•Cookies and javascript to be enabled in
web-browser
Online submission checklist
•First Page File (rtf/doc/docx file) with title page, covering letter, acknowledgement, etc.
•Article File (rtf/doc/docx file) - text of the article, beginning from Title, Abstract till References (including tables). File size limit 4 MB. Do not include images in this file.
•Images (jpg/jpeg/png/gif/tif/tiff): Submit good quality colour images. Each image should be less than 10 MB) in size
•Upload copyright form in .doc / .docx / .pdf / .jpg / .png / .gif format, duly signed by all authors, during the time mentioned in the instructions.
Help
•Check Frequently Asked Questions (FAQs) on the site
•In case of any difficulty contact the editor
1 Registration•Register from http://www.journalonweb.com/ijohr as a new
author (Signup as author)•Two-step self-explanatory process
2 New article submission•Read instructions on the journal website or download the same
from manuscript management site•Prepare your files (Article file, First page file and Images,
Copyright form & Other forms, if any)•Login as an author•Click on ‘Submit new article’ under ‘Submissions’•Follow the steps (guidelines provided while submitting the
article)•On successful submission you will receive an acknowledge-
ment quoting the manuscript ID
3 Tracking the progress•Login as an author•The report on the main page gives status of the articles and its
due date to move to next phase•More details can be obtained by clicking on the ManuscriptID•Comments sent by the editor and reviewer will be available
from these pages
4 Submitting a revised article• Login as an author•On the main page click on ‘Articles for Revision’•Click on the link "Click here to revise your article" against the
required manuscript ID•Follow the steps (guidelines provided while revising the article)•Include the reviewers’ comments along with the point to point
clarifications at the beginning of the revised article file. •Do not include authors’ name in the article file. •Upload the revised article file against New Article File -
Browse, choose your file and then click “Upload” OR Click “Finish”
•On completion of revision process you will be able to check the latest file uploaded from Article Cycle (In Review Articles-> Click on manuscript id -> Latest file will have a number with ‘R’, for example XXXX_100_15R3.docx)
http://www.journalonweb.com/ijohr

© 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow 1
HISTORICAL BACKGROUND
Today cancer has become major health menace, and the entire world is skirmishing against it. The united efforts from scientists, researchers, engineers, biological workers, and masters of technology, contributed to confine mortality. Simply cure of cancer is not a complete solution, but what about the prospect of survivors; who conquered on death?
What is cancer survivor? The issue appears to be very simple, but only inadequate people know the actuality. In 1985, Mullan coined the term “cancer survivor.” He defined it as “cancer survivor, is the person, who has diagnosed as fatal form of cancer and is therefore forced to face his or her mortality.”[1] With due course of time the National Coalition for Cancer Survivorship (NCCS) defined it as, “from the time of diagnosis and for the balance of life, a person diagnosed with cancer is a survivor.”[2] The substitute term for survivor includes alivers or thrivers. In 2000, the term “previvor” was introduced by an organization called Facing Our Risk of Cancer Empowered. This term is used for persons those who have not been diagnosed with cancer but have an inclination toward cancer.[3] Increased survival goes together with the routine needs of livelihood which leads to the development of facilities. This calls for identification of cancer survivors
with affected health‑related quality of life (HRQOL).[4] Efforts of National Cancer Survivorship agencies have doubled the survival rate of cancer patients.[4,5] The mutual data of cancer patients living at least 5 years postdiagnosis has increased from 50% in 1976 to over 64% in 2001. This attributes around one of every 640 adults between the ages of 20 and 39 years and is anticipated to continue to rise.[6] Despite increased longevity, the effectiveness of various approaches is not well understood. Hence, it is important to explore more information which enables individuals to revisit to energetic lives. In the majority of developed world, such as the USA, Australia, and European countries; the survival rates are variable from 1.5 to 5.2 per million persons per year.[7] Literature states that both adult and childhood cancer survivors have increased suicidal tendency.[8] Despite increased longevity, the effectiveness of various approaches to improve the quality of life is insufficient, so still survivors and survivorship is not well understood. Hence, it is important to explore more information regarding ill consequences of cancer, and at the same time, there is
The Challenges of Cancer SurvivorsAshok K. Vikey, Deepali Gupta Vikey1
Departments of Oral and Maxillofacial Pathology, and Microbiology and 1Prosthodontics, Sri Aurobindo College of Dentistry, Indore, Madhya Pradesh, India
ABSTRACTThe cancer is a major health threat, which is considered as the third major cause of death. In old days, childhood cancer was a mortal threat. However, a revolution in medical technology and research work; life expectation is improved. Hence, from 1995 onward, there is increased 5-year survival rate particularly, in children treated with cancer and around 80% attain adulthood. Even in other cancers, recent treatment advances have increased survival rate. However; still there is a lack of awareness and consideration toward long-term consequences in increasing survivors. Hence, merely elimination of cancer from the body is not enough; there is a call to work collectively for the betterment of rest of the life for the survivors. The survivorship project considers the need of time, but narrow work force (8%) of qualified group is the main concern.
Key words: Cancer survivors, health-related quality of life, psychosocial stress, survivorship
Review Article
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Ashok K. Vikey, Department of Oral and Maxillofacial Pathology, and Microbiology, Sri Aurobindo College of Dentistry, Indore, Madhya Pradesh, India. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???.

Vikey and Vikey: The cancer survivors
2 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
a need to motivate to lead energetic lives following the completion of cancer treatment. Because even after proper treatment, the survivors have various concerns such as psychosocial, physical, loss of self‑confidence, employment problems, pain, and family as well as a sexual imbalance. To get rid of from these ailments, there are suicidal attempts. Hence, more the literatures, more will be information for the survivors and will help in understanding the specifics of life so as to set their minds. This will focus light on nonsurvivors, various organizations, health providers, and society to get nearer to work for the betterment of the survivors.
DISCUSSION
The aim of survivorship project is to show the path to the cancer survivors toward healthy and active life. The National Cancer Survivorship Initiative (NCSI) agency is encouraging to provide proper services and solutions for the betterment of survivors. Following points must be taken into account while considering the improvement of life of cancer survivors:• Data of survivors each year• Pre‑ and post‑treatment health‑related issues• Economic and social impairments• Risks factors• Well‑planned scientific approach toward the future of
survivors• Encourage the researchers for better interventions• To develop a general guideline for clinicians.
The above features may be solved, but before that, we have to search for related after effects of the survivors. Researchers worked in this direction and found concerning problems to the survivors such as psychosocial, physical, lack of confidence, relationship, employment. The frenetic treatment program changes their daily routine, such as normal self‑care, housekeeping, and other works. Sympathy and feeling of being neglected are some concern of the survivor. Few of them overcome these hurdles, but few still have the psychological impairments, known as posttraumatic stress disorder (PTSD).[9] The studies showed PTSD is a major problem in the young population.[10] Cancer treatment along with cure of cancer, affects sexual life of patients, further leading to ovarian, or testicular failure leading to infertility.[11,12] Although there is an introduction of neoadjuvant chemotherapy (NAC) but at the same time, it has some proven significant side effects, including physical fitness, mild weakness, and HRQOL[13,14] which simply cannot be overlooked. However, again this is the topic of discussion because some studies advocate that; there is a positive correlation between physical activity and NAC indicating that NAC is not responsible for decrease physical activity.[15] But eventually, over a period, many survivors lose their employments leading to financial and social trauma. To overcome this burden, in spite of cancer‑related disabilities;
some survivors work to fulfill their expenses. However, complete recovery of financial loss is very difficult because physical as well as psychological factors affect on working hours and productivity by survivors.[16]
Earlier to 1970, childhood cancer was considered as universally fatal disease accompanied with other issues such as education, employment, marriage, and fertility.[17]
Adolescent and young adult survivorsThis group is placed between the ages of 15 and 39 years, which is continuously increasing and is a major part of survivors. This group has different issues as compared to adult survivors and nowadays due to increasing medical facilities; around 80% children treated with cancer attain adulthood. Therefore, it is important to put more collective efforts to work on this group.[18]
INTERVENTIONS
The historical background of survivorship program is quiet old, which began with the foundation of the New York Cancer Hospital in1884. Later on, in 1948, this was renamed as Memorial Hospital for Cancer and Allied Diseases and recently called as Memorial Sloan‑Kettering Cancer Center. So far, the period between1974 and 1976 is considered a turning point in the field of survivorship when people started thinking about consequences cancers on lives of survivors.[19] However, a worldwide message regarding this issue was raised by a young pediatrician, Fitzhugh Mullan, when he published an article, “Seasons of Survival” in 1985 and introduced term survivorship.[1] Later on, in 1996, the executive director for NCCS, formulated the quarries for logical and legal issues for easy approach, legal action plan, and accountability. For this, it is important to consider patient’s complete history, including name, detail address with contact, date, and stage of diagnosis of disease. Further, there should be the maintenance of record in the hospital which includes when and how the treatment modality was given to the patient, including surgeries and radiation therapy. In case of any complications or reaction during the intervention and corrective procedure for the same should be initiated and record must be maintained. Survivor care is not restricted up to improved longevity of life, but it should also consider the quality of life of survivors. Presently, we see appreciable work in this direction such as Children’s Oncology Group; which included overall intervention details so that patient may visit any health center without any difficulty. This will help clinician and patient both during follow‑up.[20] The NCSI has formulated its guidelines to generate newer approaches during research, which will be helpful for better planning and care of survivors.[21] There are some guidelines such as the history of survivorship to identify the risk factors, ongoing problems of patients, research targeting to health and psychosocial aspects of survivors and to expand literatures toward awareness, and regaining

Vikey and Vikey: The cancer survivors
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 3
smooth life. There is a demand to explore parameters which are supposed to monitor pre‑ and post‑treatment outcomes and their after effects, which may disturb the personal and social life of survivors.[22] The major issue of young survivors is infertility and is supported by sperm banking which relieved the stress and acted as an emotional battle against cancer.[23,24] There are many options for males and females such as freezing mature oocytes, ovarian tissues and protection of ovaries from gonadotoxic effects in women and testicular biopsy, semen collection, and freezing spermatozoa in males.[11,12] Researchers tried to manage infertility by various means such as prioritizing normality and marginalizing fertility ongoing infertility‑related matters, and fertility concerns dominating the cancer legacy.[25] In addition, “survivor care plans” are helpful for the survivors to lead a healthy life. Along with this cognitive behavior therapy is effective to minimize stress and other problems.[26] To encourage cancer survivors, the National Cancer Survivor Day Foundation organizes meaningful events since 1987 in the United States, Canada, and rest of countries. The basic concept being to show the world, how life is meaningful and productive. This event is organized on the 1st Sunday of every June preferably. Cancer survivor and survivorship have become a global agenda and need the attention of government and nongovernmental organizations. Increasing graph of survivors is alarming toward the development of health‑related needs, maintenance of infrastructure, financial, and social burdens. A synchronized agenda for research and practice is needed which will address cancer survivors’ long‑term medical, psychosocial, and practical needs across the survivorship path and may involve a new way of working in hospitals for providing follow‑up and holistic support.
CONCLUSION
Time demands the need to think for in‑depth examination of survivors with psychological distress and poor HRQOL. Because of lack of systematic follow‑up, we need to learn about the positive and negative aspects of treatments. Today, a question arises that who will take responsibility to monitor the health of survivors and assist in their recovery. There must be a commitment for the continued care, rehabilitation, and psychosocial fallout after treatment.
AcknowledgmentsThe presented work could not have been accomplished without dedication and invaluable help of my students. My special thanks to Dr. Trupti Chordia and Dr. Anjali Shujalpurkar for their help in editing the manuscript.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Mullan F. Seasons of survival: Reflections of a physician with cancer.
N Engl J Med 1985;313:270‑3.2. Sulik GA. Pink Ribbon Blues: How Breast Cancer Culture Undermines
Women’s Health. Anticancer Res 2013;33:746‑9.3. Harmon A. The DNA Age Cancer Free at Age 33, but Weighing
a Mastectomy. New York Times. Available from: www.nytimes.com/2007/09//16/health/16gene.html [Last retrieved on 2007 Sep 16].
4. Zeltzer LK, Lu Q, Leisenring W, Tsao JC, Recklitis C, Armstrong G, et al. Psychosocial outcomes and health‑related quality of life in adult childhood cancer survivors: A report from the childhood cancer survivor study. Cancer Epidemiol Biomarkers Prev 2008;17:435‑46.
5. Richards M, Corner J, Maher J. The national cancer survivorship initiative: New and emerging evidence on the ongoing needs of cancer survivors. Br J Cancer 2011;105 Suppl 1:S1‑4.
6. Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med 2006;355:1572‑82.
7. Vikey AK, Vikey D. Primary malignant melanoma, of head and neck: A comprehensive review of literature. Oral Oncol 2012;48:399‑403.
8. Recklitis CJ, Lockwood RA, Rothwell MA, Diller LR. Suicidal ideation and attempts in adult survivors of childhood cancer. J Clin Oncol 2006;24:3852‑7.
9. Hoffman KE, McCarthy EP, Recklitis CJ, Ng AK. Psychological distress in long‑term survivors of adult‑onset cancer: Results from a national survey. Arch Intern Med 2009;169:1274‑81.
10. Twombly R. Post‑traumatic stress disorder in childhood cancer survivors: How common is it? J Natl Cancer Inst 2001;93:262‑3.
11. Anderson RA, Themmen AP, Al‑Qahtani A, Groome NP, Cameron DA. The effects of chemotherapy and long‑term gonadotrophin suppression on the ovarian reserve in premenopausal women with breast cancer. Hum Reprod 2006;21:2583‑92.
12. Levine J, Canada A, Stern CJ. Fertility preservation in adolescents and young adults with cancer. J Clin Oncol 2010;28:4831‑41.
13. Safieddine N, Xu W, Quadri SM, Knox JJ, Hornby J, Sulman J, et al. Health‑related quality of life in esophageal cancer: Effect of neoadjuvant chemoradiotherapy followed by surgical intervention. J Thorac Cardiovasc Surg 2009;137:36‑42.
14. van Meerten E, van der Gaast A, Looman CW, Tilanus HW, Muller K, Essink‑Bot ML. Quality of life during neoadjuvant treatment and after surgery for resectable esophageal carcinoma. Int J Radiat Oncol Biol Phys 2008;71:160‑6.
15. Tatematsu N, Ezoe Y, Tanaka E, Muto M, Sakai Y, Tsuboyama T. Impact of neoadjuvant chemotherapy on physical fitness, physical activity, and health‑related quality of life of patients with resectable esophageal cancer. Am J Clin Oncol 2013;36:53‑6.
16. Short PF, Vasey JJ, Tunceli K. Employment pathways in a large cohort of adult cancer survivors. Cancer 2005;103:1292‑301.
17. Zebrack BJ, Zeltzer LK. Quality of life issues and cancer survivorship. Curr Probl Cancer 2003;27:198‑211.
18. Foster C, Fenlon D. Recovery and self‑management support following primary cancer treatment. Br J Cancer 2011;105 Suppl 1:S21‑8.
19. Jemal A, Clegg LX, Ward E, Ries LA, Wu X, Jamison PM, et al. Annual report to the nation on the status of cancer, 1975‑2001, with a special feature regarding survival. Cancer 2004;101:3‑27.
20. Freyer DR. Transition of care for young adult survivors of childhood and adolescent cancer: Rationale and approaches. J Clin Oncol 2010;28:4810‑8.
21. Tritter JQ, Calnan M. Cancer as a chronic illness? Reconsidering categorization and exploring experience. Eur J Cancer Care (Engl) 2002;11:161‑5.
22. Ogg SW, Hudson MM, Randolph ME, Klosky JL. Protective effects of breastfeeding for mothers surviving childhood cancer. J Cancer Surviv 2011;5:175‑81.

Vikey and Vikey: The cancer survivors
4 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
23. Chapple A, Salinas M, Ziebland S, McPherson A, Mac Farlane A. Fertility issues: The perceptions and experiences of young men recently diagnosed and treated for cancer. J Adolesc Health 2007;40:69‑75.
24. Saito K, Suzuki K, Iwasaki A, Yumura Y, Kubota Y. Sperm cryopreservation before cancer chemotherapy helps in the emotional battle against cancer. Cancer 2005;104:521‑4.
25. Stern C, Conyers R, Orme L, Barak S, Agresta F, Seymour J. Reproductive concerns of children and adolescent with cancer: Challenges and potential solutions. COAYA 2013;3:63‑78. http//dx.doi.org/10.2147/COAYA.S29766.
26. Osborn RL, Demoncada AC, Feuerstein M. Psychosocial interventions for depression, anxiety, and quality of life in cancer survivors: Meta‑analyses. Int J Psychiatry Med 2006;36:13‑34.

© 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow 5
INTRODUCTION
Bone is not inert tissue but dynamically metabolized connective tissue throughout life.[1] Old bone matrices are always replaced by newly formed matrices. This continual process, named bone remodeling, is important for maintaining bone volume and strength. Bone volume is maintained by the balance of bone resorption and bone formation. Bone cells consist of osteoblast lineage cells and osteoclast‑lineage cells.[2] Their differentiation and function are regulated by osteotropic hormones and cytokines.[3]
Bone resorption is necessary for many skeletal processes. It is an obligatory event during bone growth, tooth eruption, and fracture healing and is also necessary for the maintenance of an appropriate level of blood calcium. In the adult human skeleton, continuous physiological remodeling of bone is exclusively dependent on bone resorption. In several human diseases (e.g., malignant hypercalcemia and postmenopausal osteoporosis), enhanced bone resorption is the key pathophysiological event and therapies for these diseases are currently based on its inhibition. In contrast, some rare genetic disorders are manifested as decreased resorption and lead to osteopetrosis.[4] Resorption is a condition associated with either a physiologic or a pathologic process resulting in a loss of dentin, cementum, or bone.
Osteoclasts are cells essential for physiologic remodeling of bone and also play important physiologic and pathologic roles in the dentofacial complex. Osteoclasts and odontoclasts are necessary for tooth eruption yet result in dental compromise when associated with permanent tooth internal or external resorption.[5]
Osteoclasts are multinuclear cells derived from hematopoietic stem cells.[6] Bone resorption is a complex process involving highly coordinated interactions between osteoblasts and osteoclasts that are modulated by receptor activator of nuclear factor kappa‑B (RANK), RANK ligand (RANKL), and osteoprotegerin (OPG) system.[6]
This review describes morphological characteristics of resorptive cells and their implication in oral health and disease.
KEY RESORPTIVE CELLS
Monocytes and macrophagesMonocytes and macrophages, along with osteoclasts, play an important role in bone and tooth resorption. They are
Resorptive Cells in Health and DiseaseSwati Gautam, Arvind Sharma1, Deepti Garg
Departments of Oral Pathology and Microbiology and 1Prosthodontics, Bhojia Dental College, Baddi, Solan, Himachal Pradesh, India
ABSTRACTClastic cells are responsible for the resorption of mineralized matrix of hard tissues. Bone resorbing cells are called osteoclasts; however, they are able to resorb mineralized dental tissues or calcified cartilage, and then, they are called odontoclasts and chondroclasts, respectively. Clastic cells form when mononuclear precursors derived from a monocyte–macrophage cell lineage are attracted to certain mineralized surfaces and subsequently fuse and adhere to them for exerting their resorbing activity. The clastic cells are responsible for degradation of calcified extracellular matrix composed of organic molecules and hydroxyapatite. This process is mainly required in bone turnover and growth, spontaneous and induced (orthodontic) tooth movement, tooth eruption, and bone fracture healing, as well as in pathological conditions, such as osteoporosis, osteoarthritis, and bone metastasis. In addition, they are responsible for daily control of calcium homeostasis. Clastic cells also resorb the primary teeth for shedding before the permanent teeth erupt into the oral cavity.
Key words: Chondroclasts, hydroxyapatite, odontoclasts, osteoclasts
Review Article
Corresponding Author: Dr. Swati Gautam, Department of Oral Pathology and Microbiology, Bhojia Dental College, Budd, Baddi, Solan, Himachal Pradesh, India. E‑mail: [email protected]
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???.

Gautam, et al.: Resorptive cells
6 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
found in tissue sections adjacent to bone resorbing surfaces of rheumatoid arthritis, periodontal disease, periradicular granulomas and cysts, and in metastatic bone tumors.[7] These cells play a critical role in the development and healing of all wounds. Monocytes are recruited to the site of irritation by the release of many proinflammatory cytokines and thus differentiate into macrophages. The migration and recruitment of macrophages are regulated by macrophagic chemotactic factors that are derived from bone and tissue breakdown products and are controlled by increased intracellular levels of adenosine 3,5‑cyclic phosphate (cAMP) and calcium. Although macrophages have a structure similar to that of osteoclasts and the osteoclasts can also become multinucleated giant cells, macrophages lack a ruffled border that is attached to hard tissue substrates during resorption and do not create lacunae on the dentinal surface.[8]
CLASTIC CELLS
The cells involved in resorption other than monocytes and macrophages are osteoclasts, odontoclasts, dentinoclasts, and cementoclasts.[7] Osteoclasts are multinuclear cells derived from hematopoietic stem cells. Their differentiation pathway is common to that of macrophages and dendritic cells. Thus, a promyeloid precursor can differentiate into either an osteoclast, a macrophage, or a dendritic cell, depending on whether it is exposed to RANKL (also called tumor necrosis factor [TNF]‑related activation‑induced cytokine, OPG ligand or osteoclast differentiation factor), macrophage colony‑stimulating factor (M‑CSF), or granulocyte‑M‑CSF, respectively.[6] Odontoclasts probably have the same origin as osteoclasts. Odontoclasts are derived from tartrate‑resistant acid phosphatase (TRAP)‑positive circulating monocytes. Odontoclasts are generally smaller in size, having fewer nuclei and form smaller resorption lacunae than the osteoclasts.[9] Prostaglandin E2 (PGE2) may induce cementoclast formation by controlling the balance of RANKL/OPG expression levels in cementoblasts via the EP4‑cAMP‑protein kinase A (PKA) pathway, in a manner similar to that of parathyroid hormone‑related peptide (PTHrP). PGE2 stimulates cementoblast‑mediated cementoclast activity in vitro through control of RANKL, interleukin‑6 (IL‑6), and OPG mRNA and protein in cementoblasts, mainly via the EP4 pathway, similar to the role of PGE2 in osteoblasts.[10]
PHYSIOLOGY OF RESORPTION
To maintain stability and integrity of bone, it is constantly undergoing remodeling, with about 10% of bone material being renewed each year. Bone remodeling is a complex process that involves bone resorption performed by osteoclasts, followed by bone formation carried out by osteoblasts.[11] The complex process of bone resorption occurring during both physiologic and pathologic instances involves highly coordinated interaction between osteoblasts and osteoclasts that are modulated by enzymes, hormones, and RANK/RANKL/OPG
system. It is suggested that the OPG/RANKL/RANK system is instrumental for interactions between bone, vascular, and immune cells. These protein ligands function as paracrine regulators of osteoclastogenesis and bone metabolism and share homologies with members of the TNF receptor superfamily.[12]
Resorption requires cellular activities: Migration of the osteoclast to the resorption site, its attachment to bone, polarization and formation of new membrane domains, dissolution of hydroxyapatite, degradation of organic matrix, removal of degradation products from the resorption lacuna, and finally either apoptosis of the osteoclasts or their return to the nonresorbing stage. After migration of the osteoclast to a resorption site, a specific membrane domain, the sealing zone, forms under the osteoclast. The plasma membrane attaches tightly to the bone matrix and seals the resorption site from its surroundings.[13]
Integrins play an important role in the early phases of the resorption cycle. At least four different integrins are expressed in osteoclasts: avb3, avb5, a2b1, and avb1.[14]
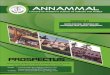
Resorbing osteoclasts contain not only the sealing zone but also at least three other specialized membrane domains: A ruffled border, a functional secretory domain, and a basolateral membrane. As the osteoclast prepares to resorb bone, it attaches to the bone matrix through the sealing zone and forms another specific membrane domain, the ruffled border. The ruffled border is a resorbing organelle, and it is formed by fusion of intracellular acidic vesicles with the region of plasma membrane facing the bone [Figure 1].
The main physiological function of osteoclasts is to degrade mineralized bone matrix. This involves dissolution of crystalline hydroxyapatite and proteolytic cleavage of the organic matrix, which is rich in collagen. Before proteolytic enzymes can reach and degrade collagenous bone matrix, tightly packed hydroxyapatite crystals must be dissolved.
Figure 1: Bone resorption

Gautam, et al.: Resorptive cells
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 7
It is now generally accepted that the dissolution of mineral occurs by targeted secretion of HCl through the ruffled border into the resorption lacuna.[15] After solubilization of the mineral phase, several proteolytic enzymes degrade the organic bone matrix although the detailed sequence of events at the resorption lacuna is still obscure. Two major classes of proteolytic enzymes, lysosomal cysteine proteinases and matrix metalloproteinases (MMPs) are responsible for matrix degradation.[16] After matrix degradation, the degradation products are removed from the resorption lacuna through a transcytotic vesicular pathway from the ruffled border to the functional secretory domain, where they are liberated into the extracellular space.[17]
The unique structural arrangement of the osteoclasts to hard tissues allows the cell to establish a microenvironment between the ruffled border and the bone, in which resorption takes place. The resorptive process itself can be described as being bimodal, involving the degradation of the inorganic crystal structure of hydroxyapatite and the organic structure of collagen, principally Type 1. The activated osteoclasts produce an acidic pH (3.0–4.5) in their microenvironment. At pH 5 or lower, the solubility of hydroxyapatite increases dramatically and resorption of hard tissue can occur. This acidic environment is primarily achieved through the action of a highly active polarized proton pump contained within the ruffled border. The enzyme carbonic anhydrase II (CA II), which is specific to osteoclasts, also plays a critical role in establishing a subosteoclastic acidic pH. The CA II catalyzes the intracellular conversion of CO2 to H2CO3, which provides a readily available source of H+ ions to be pumped into the subosteoclastic region.[9]
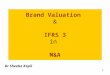
Odontoclasts are thought to differentiate from circulating progenitor cells such progenitor cells reside in the dental pulp and periodontal ligament (PDL), sharing similar characteristics with osteoclasts such as the expression of cathepsin K, cathepsin D, TRAP, MMPs‑9, H+‑ATPase, membrane Type 1‑MMP expression, and the formation of a clear zone and ruffled border.[5] RANK receptor is expressed by odontoclasts and RANKL by odontoblasts, pulp, and PDL fibroblasts [Figure 2].[18]
ROLE OF RESORPTIVE CELLS IN ORAL HEALTH AND DISEASES
Role in physiological root resorptionThe resorbing activity of odontoclasts is related to expression of the OPG/RANKL/RANK system by PDL cells. It has been shown that PDL cells, isolated from either nonresorbing deciduous teeth or permanent teeth, express OPG but not RANKL.[19] In the dental follicle environment, the ratio of OPG to RANKL supports, rather than inhibits, osteoclastogenesis. Cytotrophic factors released from the dental follicle and/or the stellate reticulum, such as PTHrP, interleukin‑1α, and
transforming growth factor‑β1, stimulate the expression of RANKL during permanent tooth eruption. Among these factors, PTHrP controls regulation of the relative expression levels of RANKL/OPG on dental follicle cells, as well as in human PDL cells. PTHrP increases RANKL and downregulates OPG expression via a cAMP/PKA protein kinase‑independent pathway, consequently leading to physiological root resorption of deciduous teeth and successful eruption of permanent teeth [Figure 3].[20]
Role in pathologic root resorptionDuring orthodontic tooth movement, on the compressed side of the tooth, RANKL expression is induced.[21] RANKL activates osteoclastogenesis, and this is better demonstrated by the acceleration of tooth movement, which is achieved after transfer of the RANKL gene to the periodontal tissue.[22] In contrast, it seems that on the tensile side of an orthodontically moving tooth, there is an increase in OPG synthesis. It has been reported that application of tensile stretching to osteoblasts results in induction of OPG mRNA in PDL cells, and this upregulation of OPG synthesis is reportedly magnitude dependent. Such tensile strain also induces a decrease of RANKL release and RANKL mRNA expression in cultured osteoblasts. The relative expression of OPG and RANKL on the tensioned and the compressed sides of the tooth regulates bone remodeling during orthodontic tooth movement [Figure 4].[12]
Role in periodontitisDuring an inflammatory response, cytokines, chemokines, and other mediators stimulate periosteal osteoblasts,
Figure 2: Activation of osteoclast

Gautam, et al.: Resorptive cells
8 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
altering the expression levels of RANKL on the osteoblast surface.[23] RANKL is expressed by osteoblasts in the form of a membrane‑bound protein or cleaved into a soluble form.[24] IL‑1 stimulates osteoclastogenesis and bone resorption, largely through upregulation of RANKL while TNF can stimulate osteoclastogenesis directly or indirectly through RANKL. Inhibition of RANKL caused a decrease in alveolar bone loss in several models of periodontal disease [Figure 5].[25]
Paget’s diseaseEvidence exists for a genetic predisposition for Paget’s disease with a gene locus identification on chromosome 18q‑21‑22. Most of the evidence centers on the gene factors capable of altering the normal osteoclast behavior. Malfunction of the RANK/RANKL/OPG pathway results in either too much or too little total bone formation. Further, IL‑6 plays an important role by increasing the hyper‑responsivity of the osteoclast and its precursor cells. Involvement of genes encoding RANK, OPG, VCP, and SQSTM1 in pagetoid diseases provides strong arguments for the role of deregulated NF‑κB signaling. This pathway is a key player in osteoclastogenesis that is to a large degree regulated by RANK and OPG. Both SQSTM1and VCP have a role in intracellular NF‑κB signaling; the former is a scaffolding protein facilitating NF‑κB signaling and the latter participates in proteasomal degradation of IκB, a downstream mediator of NF‑κB signaling.[26]
OsteopetrosisOsteopetrosis is also called “marble bone disease” due to the exaggerated bone density. The osteopetroses can be generally segregated into two clinical forms; the autosomal dominant, adult (benign) type and the autosomal recessive, infantile (malignant) form that is profoundly more severe; however, there are other forms that are associated with other organ systems (Villa et al., 2009). Numerous genes have been identified for their association with compromised osteoclast function. Four genes are most widely linked to human osteopetroses. Generally speaking, the severity of the osteoclast compromise is directly related to the severity of the phenotypic presentation of the condition.[5] The gene
for adult osteopetrosis has been mapped to chromosome 1p21.[27] Similar to bisphosphonate‑associated osteonecrosis, the pathogenesis of all true forms of osteopetrosis involves diminished osteoclast‑mediated skeletal resorption. The number of osteoclasts is often increased; however, as they fail to function normally, bone is not resorbed. This defective osteoclastic bone resorption, along with continued bone formation and endochondral ossification, leads to cortical bone thickening and cancellous bone sclerosis. The causes of osteoclast failure are unclear but may involve abnormalities in the osteoclast stem cell or its microenvironment, osteoblast precursor cells or the mature heterokaryon or in the bone matrix.[28] Alterations in the factors required for bone resorption, such as the synthesis of abnormal PTH or defective production of IL‑2 or superoxide, are also possible causes. Ultimately, impaired bone resorption results in skeletal fragility because fewer collagen fibrils connect osteons properly, and remodeling of woven bone to compact bone is defective [Figure 6].[28]
Role in myeloma bone diseaseMyeloma bone disease is due to interactions of myeloma cells with the bone marrow microenvironment and is associated with pathologic fractures, neurologic symptoms, and hypercalcemia. Adjacent to myeloma cells, the formation and activation of osteoclasts are increased, which results in enhanced bone resorption.[29] Malignant tumors capable of either forming skeletal metastases or causing hypercalcemia utilize the cellular machinery (osteoclasts) and molecular pathways (RANKL/RANK/OPG) of normal bone cell biology.[30] Focally or systemically enhanced osteoclastic activation results in tumor‑associated hypercalcemia, osteolysis, pathologic fractures, and severe pain.[31] Increased expression of RANKL by bone marrow stromal cells was associated with enhanced osteoclastogenesis, and this effect could be prevented by RANK‑Fc, a specific inhibitor of RANKL. Taken together, enhancement of marrow stromal (and possibly T cell) expression of RANKL by myeloma cells and direct RANKL expression by myeloma cells contribute to enhanced
Figure 3: Physiological root resorption
Figure 4: Pathological resorption

Gautam, et al.: Resorptive cells
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 9
osteoclastogenesis in the bone microenvironment in myeloma bone disease.[30]
Role in osteoarthritisThe articular joint is made up of several tissues, the main ones involved during osteoarthritis (OA) being the cartilage, synovial membrane, and subchondral bone, all of which are closely linked. The cartilage is the tough elastic material that covers and protects the ends of bone. In a healthy joint, it acts as a shock absorber when weight is exerted on the joint and its slippery surface allows the joints to move smoothly. Joint degeneration does occur, however, and OA is the most common joint disorder, affecting about 65% of individuals over 60 years of age.[32] In OA, a subchondral bone resorption/formation process has been shown to occur, in which there are phases of bone degradation and others of bone formation. Interestingly, factors such as OPG and RANKL, which constitute specific components capable of influencing the bone remodeling process, have been found to be expressed and modulated in human OA subchondral bone. In addition to subchondral bone, the OPG/RANK/RANKL triad has also been observed to be expressed by the other
articular cells. Indeed, articular chondrocytes also express each factor. OPG, RANK, and RANKL have been detected in the superficial zone of normal cartilage whereas during OA, their expression was found to extend to the middle zone.[33]
Role in neoplasiaIn neoplasia, bone remodeling can be disturbed as a result of increased bone turnover which may be confined to the site of metastases or be more generalized, most likely related to the secretion of PTHrP or other factors by the primary tumor. A significant increase in bone turnover is not uncommon and may result in substantial skeletal deficits, more marked at trabecular cancellous sites. Bone remodeling may also be disturbed due to an imbalance between bone resorption and formation. Most of the disturbances in bone remodeling associated with neoplasia result in significant amounts of bone loss not uncommonly associated with hypercalcemia.[34]
Role in osteoporosisOsteoporosis is defined as a decrease in bone mass coupled with a disorder in bone microarchitecture associated with as clinical consequence an increase in the risk of fracture. Fundamental to the pathogenesis of osteoporosis is an aberrant cell production relative to demand. In age‑related osteoporosis, there is an undersupply of osteoblasts relative to the needs for repair due to a decrease in osteoblastogenesis. Bisphosphonates correct the imbalance between bone resorption and formation, and the role of these agents is now established in the management of osteoporosis.[33]
Role in cyst enlargementThe most prominent destructive event connected with radicular cyst is the resorption of alveolar bone. The effector cells of this process are osteoclasts. Activated osteoclast will resorb the mineralized matrix and degrade organic components of bone.[34]
The RANKL and OPG can be identified in radicular cysts. Menezes et al. have identified the expression of both
Bacterial plaque accumulation in dentogingival area
Host immunoinflammatory response
Prolonged inflammation and amplification of immune response
Release of proinflammatory cytokines
IL-6,7, TNF
Osteoblaststromal
cells
Bradykinin, kallikrein
RANKL
Osteoclast precursorcells
OPG
osteoclastogenesis
Alveolar bone loss
Figure 5: Periodontitis
Figure 6: Osteopetrosis

Gautam, et al.: Resorptive cells
10 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
molecules in radicular cysts, with the number of RANKL being higher than OPG (the ratio of RANKL/OPG: 1.40 ± 0.04). Both RANKL and OPG are involved in osteoclasts signaling.[34]
Bone resorption is a complex process involving highly coordinated interactions between osteoblasts and osteoclasts that are modulated by the RANKL/RANK/OPG system. RANKL is secreted primarily by activated T‑cells and binds a cell surface receptor (RANK) to promote osteoclast differentiation and activation. Tay et al. showed immunostaining for RANKL within the fibrous wall of radicular cysts. That RANKL involved in osteoclast recruitment was confirmed by the demonstration of TRAP and calcitonin‑receptor‑positive osteoclasts adjacent to the RANKL‑positive cells.[35]
CONCLUSION
Bone remodeling is a fine‑tuned process insuring the maintenance of skeletal mass and integrity. Osteoclast and odontoclast functions are closely related to physiological and pathological clinical scenarios including craniofacial abnormalities, tooth eruption, and root resorption. Understanding the complex mechanisms that control osteoclast or odontoclast development and activation will provide insights in early detection and management of clinical challenges. The above disorders represent a few examples of the consequences of disturbances in this physiologically complex but carefully coordinated process on skeletal metabolism. Future translational studies should be carried out to elaborate how to modulate osteoclast or odontoclast function at the molecular level and develop therapeutic strategies to turn on or off osteoclastogenesis or odontoclastogenesis activation pathways and hence provide therapeutics for promoting bone remodeling or inhibiting bone resorption.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Cormack DH. Ham’s Histology. 9th ed. Philadelphia: J.B. Lippincott
Company; 1987.2. Lian JB, Stein GS, Canalis E, Robey PG, Boskey AL. Bone formation:
Osteoblast lineage cells, growth factors, matrix proteins and the mineralization process. In: Favus MJ, editor. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. Philadelphia: Lippincott Williams and Wilkins; 1999. p. 14‑29.
3. Morphology, function, and differentiation of bone cells Hiroaki Nakamura department of oral histology, Matsumoto Dental University. Shiojiri Jpn J Hard Tissue Biol 2007;16:5‑22.
4. Väänänen HK, Zhao H, Mulari M, Halleen JM. The cell biology of osteoclast function. J Cell Sci 2000;113(Pt 3):377‑81.
5. Wang Z, McCauley LK. Osteoclasts and odontoclasts: Signaling pathways to development and disease. Oral Dis 2011;17:129‑42.
6. Kamat M, Puranik R, Vanaki S, Kamat S. An insight into the regulatory mechanisms of cells involved in resorption of dental hard tissues. J Oral Maxillofac Pathol 2013;17:228‑33.
7. Shafer WG, Hine MT, Levy BM. A Textbook of Oral Pathology. Philadelphia: Saunders; 1993.
8. Rifkin BR, Baker RL, Somerman MJ, Pointon SE, Coleman SJ, Au WY. Osteoid resorption by mononuclear cells in vitro. Cell Tissue Res 1980;210:493‑500.
9. Ne RF, Witherspoon DE, Gutmann JL. Tooth resorption. Quintessence Int 1999;30:9‑25.
10. Oka H, Miyauchi M, Sakamoto K, Moriwaki S, Niida S, Noguchi K, et al. PGE2 activates cementoclastogenesis by cementoblasts via EP4. J Dent Res 2007;86:974‑9.
11. Proff P, Römer P. The molecular mechanism behind bone remodelling: A review. Clin Oral Investig 2009;13:355‑62.
12. Tyrovola JB, Spyropoulos MN, Makou M, Perrea D. Root resorption and the OPG/RANKL/RANK system: A mini review. J Oral Sci 2008;50:367‑76.
13. Väänänen HK, Karhukorpi EK, Sundquist K, Wallmark B, Roininen I, Hentunen T, et al. Evidence for the presence of a proton pump of the vacuolar H+‑ATPase type in the ruffled borders of osteoclasts. J Cell Biol 1990;111:1305‑11.
14. Nesbitt S, Nesbit A, Helfrich M, Horton M. Biochemical characterization of human osteoclast integrins. Osteoclasts express alpha v beta 3, alpha 2 beta 1, and alpha v beta 1 integrins. J Biol Chem 1993;268:16737‑45.
15. Blair HC, Teitelbaum SL, Ghiselli R, Gluck S. Osteoclastic bone resorption by a polarized vacuolar proton pump. Science 1989;245:855‑7.
16. Drake FH, Dodds RA, James IE, Connor JR, Debouck C, Richardson S, et al. Cathepsin K, but not cathepsins B, L, or S, is abundantly expressed in human osteoclasts. J Biol Chem 1996;271:12511‑6.
17. Nesbitt SA, Horton MA. Trafficking of matrix collagens through bone‑resorbing osteoclasts. Science 1997;276:266‑9.
18. Harokopakis‑Hajishengallis E. Physiologic root resorption in primary teeth: Molecular and histological events. J Oral Sci 2007;49:1‑12.
19. Oshiro T, Shibasaki Y, Martin TJ, Sasaki T. Immunolocalization of vacuolar‑type H+‑ATPase, cathepsin K, matrix metalloproteinase‑9, and receptor activator of NFkB ligand in odontoclasts during physiological root resorption of human deciduous teeth. Anat Rec 2001;264:305‑11.
20. Fukushima H, Jimi E, Kajiya H, Motokawa W, Okabe K. Tooth resorption via a cAMP/protein kinase A‑independent pathway. J Dent Res 2005;84:329‑34.
21. Oshiro T, Shiotani A, Shibasaki Y, Sasaki T. Osteoclast induction in periodontal tissue during experimental movement of incisors in osteoprotegerin‑deficient mice. Anat Rec 2002;266:218‑25.
22. Kanzaki H, Chiba M, Arai K, Takahashi I, Haruyama N, Nishimura M, et al. Local RANKL gene transfer to the periodontal tissue accelerates orthodontic tooth movement. Gene Ther 2006;13:678‑85.
23. Lerner UH. Inflammation‑induced bone remodeling in periodontal disease and the influence of post‑menopausal osteoporosis. J Dent Res 2006;85:596‑607.
24. Mizuno A, Kanno T, Hoshi M, Shibata O, Yano K, Fujise N, et al. Transgenic mice overexpressing soluble osteoclast differentiation factor (sODF) exhibit severe osteoporosis. J Bone Miner Metab 2002;20:337‑44.
25. Srinivasan PC. The role of inflammatory cytokines and the RANKL‑RANK‑OPG molecular triad in periodontal bone loss‑a review. J Clin Cell Immunol 2013 ;S13.
26. Chung PY, Hul WV. The role of genes in the pathogenesis of Pagets disease of bone. IBMS 2010;7:124‑33.
27. Van Hul W, Bollerslev J, Gram J, Van Hul E, Wuyts W, Benichou O, et al. Localization of a gene for autosomal dominant osteopetrosis (Albers‑Schönberg disease) to chromosome 1p21. Am J Hum Genet 1997;61:363‑9.
28. Whyte MP. Sclerosing bone disorders. In: Favus MJ, editor. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. 4th ed. New York: Lippincott Williams and Wilkins; 1999. p. 367‑83.

Gautam, et al.: Resorptive cells
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 11
29. Sezer O, Heider U, Zavrski I, Kühne CA, Hofbauer LC. RANK ligand and osteoprotegerin in myeloma bone disease. Blood 2003;101:2094‑8.
30. Guise TA. Molecular mechanisms of osteolytic bone metastases. Cancer 2000;88 12 Suppl: 2892‑8.
31. Pearse RN, Sordillo EM, Yaccoby S, Wong BR, Liau DF, Colman N, et al. Multiple myeloma disrupts the TRANCE/osteoprotegerin cytokine axis to trigger bone destruction and promote tumor progression. Proc Natl Acad Sci U S A 2001;98:11581‑6.
32. Tat SK, Pelletier JP, Velasco CR, Padrines M, Martel‑Pelletier J. New perspective in osteoarthritis: The OPG and RANKL system as a potential therapeutic target? Keio J Med 2009;58:29‑40.
33. Komuro H, Olee T, Kühn K, Quach J, Brinson DC, Shikhman A, et al. The osteoprotegerin/receptor activator of nuclear factor kappaB/receptor activator of nuclear factor kappaB ligand system in cartilage. Arthritis Rheum 2001;44:2768‑76.
34. Menezes R, Bramante CM, da Silva Paiva KB, Letra A, Carneiro E, Fernando Zambuzzi W, et al. Receptor activator NFκB‑ligand and osteoprotegerin protein expression in human periapical cysts and granulomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102:404‑9.
35. Tay JY, Bay BH, Yeo JF, Harris M, Meghji S, Dheen ST. Identification of RANKL in osteolytic lesions of the facial skeleton. J Dent Res 2004;83:349‑53.

12 © 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow
INTRODUCTION
Many biological events are strictly regulated by cell‑cell interactions, which are categorized into two forms: cognate (adhesive) interactions, achieved by mutual recognition between membrane‑bound cell‑surface molecules and cytokine‑mediated interactions.[1] Cytokines are soluble proteins that bind to specific receptors on target cells and initiate intracellular signaling cascades resulting in phenotypic changes in the cell via altered gene regulation. They are effective at low concentrations, are produced transiently in the tissues in which they are produced, induce their own expression in an autocrine or paracrine fashion, and have pleiotropic effects on a large number of cell types.[2]
Cytokines and selective inflammatory mediators play crucial roles in the maintenance of tissue homeostasis, a process which requires a delicate balance between anabolic and catabolic activities.[3] In particular, growth factors such as fibroblast growth factor (FGF), platelet‑derived growth factor (PDGF), insulin‑like growth factor (IGF), and transforming growth factor‑β (TGF‑β) are thought to play important roles in modulating the proliferation and migration of structural cells in the periodontium and the production of various extracellular matrices by these
cells. There is little doubt that excessive and continuous production of cytokines in inflamed periodontal tissues is responsible for the progress of periodontitis and periodontal tissue destruction. Particularly, inflammatory cytokines such as interleukin (IL)‑lα, IL‑β, IL‑6, and IL‑8 are present in the diseased periodontal tissues, and their unrestricted production seems to play a role in chronic leukocyte recruitment and tissue destruction.[1] The factors included in the cytokine molecule group are ILs, interferons, growth factors, cytotoxic factors, activating or inhibitory factors, colony stimulating factors, and intercrines.[1] As a rule, the synthesis of cytokines is inducible, although some factors are known to be produced constitutively. The mechanisms by which cytokines act on the target cells are classified into four types: autocrine, intracrine, juxtacrine, and paracrine.
CYTOKINES AND ROLE IN IMMUNITY
The innate immune system serves as the first line of defense against an unknown antigen. A series of pro‑inflammatory cytokines including IL‑1α /β, IL‑6, tumor necrosis
Cytokines and Other Inflammatory Mediators in Periodontal Health and Disease
Harpreet Singh Grover, Rohit Saini, Pearl Bhardwaj, Amit Bhardwaj
Department of Periodontology, Faculty of Dental Sciences, SGT University, Gurgaon, Haryana, India
ABSTRACTCytokines and selective inflammatory mediators play crucial roles in the maintenance of tissue homeostasis. Growth factors such as fibroblast growth factor, platelet-derived growth factor, insulin-like growth factor, and transforming growth factor-β are thought to play important roles in modulating the proliferation and migration of structural cells in the periodontium. These biomolecules have a range of overlapping functions to help engage and control immune and inflammatory responses.
Key words: Chemokines, fibroblast growth factor, insulin‑like growth factor, platelet‑derived growth factor, prostaglandins, transforming growth factor-β
Review Article
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Pearl Bhardwaj, Department of Periodontology, Faculty of Dental Sciences, SGT University, Gurgaon, Haryana, India. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???.

Grover, et al.: Cytokines in health and disease
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 13
factor‑alpha (TNF‑α), chemokines (IL‑8), and interferons are synthesized de novo following bacterial or viral infections. These cytokines are active in stimulating phagocytic cells, monocytes, macrophages, neutrophils, and endothelial cells to react against or bind to microorganisms and other immune cells to the site of infection.[4]
ROLE OF CYTOKINE EXPRESSION IN PERIODONTAL HEALTH AND DISEASE
Tissue homeostasis represents a delicate balance between anabolic and catabolic activities.
Cytokine expression in periodontal healthFibroblast growth factorFGFs are one of the well‑characterized cytokine families that can be found in many tissues. Two of the nine isoforms of FGF have been characterized in some detail: one is acidic FGF (aFGF; FGF‑1) and the other is basic FGF (bFGF; FGF‑2). Both FGFs bind to heparan sulfate, heparin, and fibronectin in the extracellular matrix. aFGF is primarily known for its effect on endothelial cell replication and neovascularization. Like aFGF, bFGF has angiogenic properties and is highly chemotactic and mitogenic for a variety of cell types. It stimulates bone cell replication and increases the number of cells of the osteoblastic lineage. FGF is a potent stimulator of periodontal ligament (PDL) cell migration and mitogenesis.[1]
Platelet‑derived growth factor (AA, AB, BB)PDGF, which was originally detected in the α‑granules of platelets, is a potent growth factor for various connective tissue cells. A plethora of other cell types also synthesize PDGF including macrophages, endothelial cells, fibroblasts, astrocytes, myoblasts, and smooth‑muscle cells. Platelets synthesize a mixture of the three possible isoforms (70% AB, 20% BB, and 10% AA), while epidermal growth factor (EGF)‑stimulated fibroblasts synthesize AA homodimers. Activated macrophages and placental cytotrophoblasts produce the BB homodimer. The binding of PDGF to several plasma proteins and extracellular matrix facilitates local concentration of the factor. PDGF functions as a local autocrine and paracrine growth factor. PDGF is a powerful promoter of cell migration and proliferation.[5]
Insulin‑like growth factors (I and II)Two different IGFs (IGF‑I and IGF‑II) have been described.[6] Both were isolated initially as serum factors with insulin‑like activities that could not be inhibited by anti‑insulin antibodies. The structure of both IGFs is homologous to human pro‑insulin. In periodontal research, it was shown that IGF‑I is chemotactic and mitogenic for PDL cells. Although a single application of IGF‑I only slightly induces periodontal tissue regeneration, several lines of evidence suggest that IGF‑I combined with other growth factors such as bFGF, PDGF, and TGF‑3 may augment the osseous wound‑healing process.[7]
Transforming growth factor‑bTGF‑β appears to be synthesized by all normal cells studied to date. The different isoforms of TGF‑β (TGF‑β1, TGF‑β2, and TGF‑β3) are encoded by different genes. TGF‑β is the most potent known growth inhibitor for epithelial cells, endothelial cells, fibroblasts, neuronal cells, lymphocytes, and hepatocytes. It stimulates the synthesis of connective tissue matrix components, such as collagen, fibronectin, proteoglycan, glycosaminoglycan, osteonectin, and osteopontin in many cell types, including PDL cells.[8] It also inhibits the degradation of matrix proteins by inhibiting the synthesis of metalloproteinases such as collagenase and by increasing the synthesis of proteinase inhibitors.[9]
Cementum‑derived growth factorCementum‑derived growth factor (CGF) was detected exclusively in cementum and was shown to be the major cementum mitogen for PDL cells and gingival fibroblasts. It has been suggested that CGF may promote the migration and growth of progenitor cells present in structures adjacent to the dentin matrix and participate in their differentiation into cementoblasts.[1]
Cytokine expression in periodontal diseaseTwo of the most important proinflammatory cytokines are IL‑1 and TNF‑α. Offenbacher in 1996 suggested that if the antibody/neutrophil response does not result in clearance, the outcome of monocyte/lymphocyte challenge is the secretion of catabolic cytokine and inflammatory mediator, which induce connective tissue and bone loss.
Interleukin‑1There are three IL‑1 ligands, IL‑1β, IL‑α, and IL‑1 receptor antagonist (IL‑1ra). IL‑1α and IL‑1β have similar biological activity, while IL‑1ra binds to IL‑1 receptors, but does not have agonist activity and acts as a competitive inhibitor.[10] IL‑1 was discovered by Gery et al. in 1972 and was described as a lymphocyte‑activating factor based on its mitogenic activity on lymphocytes. These biomolecules have a range of overlapping functions to help engage and control immune and inflammatory responses.[3] Following activation, it is synthesized by various cell types, including macrophages, monocytes, lymphocytes, vascular cells, brain cells, skin cells, and fibroblasts. IL‑1α and IL‑1β share only 27% homology at the amino acid level, but they have similar biological functions. It has been demonstrated that IL‑lα remains largely cell‑associated, whereas IL‑1β is released from the cell.
IL‑1 is known to stimulate the proliferation of keratinocytes, fibroblasts, and endothelial cells and to enhance fibroblast synthesis of type I procollagen, collagenase, hyaluronate, fibronectin, and prostaglandin E2 (PGE2). The local excessive production of IL‑I by cells composing the periodontium appears to be capable of stimulating gingival and PDL fibroblasts, in an autocrine or paracrine fashion, to induce the production of other cytokines, matrix‑degrading

Grover, et al.: Cytokines in health and disease
14 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
enzymes, and PGE2. These mediators may be responsible for effecting connective tissue destruction, leading to the loss of attachment. Thus, IL‑1 has been suggested to play a key role in promoting alveolar bone destruction in periodontal disease.[1] There is evidence that susceptibility to periodontal disease is influenced by genetic polymorphism of IL‑1 gene. Some studies report on an association between IL‑1 and severity of periodontal disease genotype.[11] In a meta‑analysis, it is demonstrated that IL‑1α and IL‑1β genetic variation are significant contributors to chronic periodontitis.[12]
Interleukin‑6It has pro‑inflammatory properties, plays a key role in acute inflammation, and promotes bone resorption. It also stimulates T‑cell differentiation.[2] IL‑6 is clearly an IL that mediates communication between a large number of cell types by playing a role in the proliferation and differentiation of B‑lymphocytes, hematopoietic progenitors, hepatocytes, and T‑lymphocytes.[3] IL‑6 is also one of the cytokines found in gingival crevicular fluid (GCF) of patients with refractory periodontitis, who are undergoing active bone loss.[12] In this way, IL‑6 which is a pro‑inflammatory cytokine contributed to periodontitis‑induced bone resorption.
Interleukin‑8Formerly known as neutrophil‑activating peptide‑1, it is a potent chemotactic factor for leukocytes. IL‑8 is secreted by a variety of cells, including monocytes, fibroblasts, lymphocytes, and endothelial cells.[1] In inflamed gingival tissue, it is expressed in epithelial cells and macrophages. It may play a significant role in the pathogenesis of periodontitis. It is likely that locally secreted IL‑8 induces neutrophil extravasation at the site of inflammation, and numerous neutrophils present in lamina propria and epithelium of inflamed gingiva may be detected by IL‑8.
Interleukin‑17These cells are termed as “Th‑17.” IL‑17 has been shown to stimulate epithelial, endothelial, and fibroblastic cells to produce IL‑6, IL‑8, and PGE2. It induces the receptor activator of nuclear factor‑kappa β ligand (RANKL) production of osteoblasts and influence osteoblastic bone resorption.[13] IL‑17 mediated inflammation in the initiation and progression of periodontal disease suggesting that Th‑17 cells may contribute to pathogenic tissue destruction that occurs in periodontal disease. IL‑17 seems to blur the lines between innate and adaptive immunity because it is secreted byadaptive immune system and it mediates the activation of products typical of innate inflammatory effects such as TNF‑α and IL‑1β. IL‑17 can modulate the RANKL/osteoprotegerin (OPG) ratio and increases RANKL expression and concomitantly decreases OPG expression in osteoblastic cells.[14]
Lymphokine expression by T‑cells in periodontal diseaseT‑cells play a crucial role in regulating a variety of immune responses by secreting various cytokine, formerly known as lymphokine.
Tumor necrosis factor‑alphaTNF refers to two associated proteins, TNF‑α and TNF‑β. There are two structurally similar TNF cell surface receptors, TNF receptor‑1 (TNFR‑1) and TNF receptor‑2 (TNFR‑2). These receptors activate different signaling pathways and have different cytoplasmic domains. Most of the inflammatory effects are mediated through TNFR‑1 signaling, while TNFR‑2 attenuates the inflammatory response induced by TNF.[15] TNF‑α is a pro‑inflammatory cytokine that is secreted mainly by monocytes and macrophages. It induces the secretion of collagenase by fibroblasts, resorption of cartilage and bone, and has been implicated in the destruction of periodontal tissue in periodontitis. It also activates osteoclasts and thus induces bone resorption.[1]
Interferon gammaIt is a lymphokine produced by activated T‑lymphocytes and natural killer cells that plays an important role in host defense mechanisms by exerting pleiotropic activities on a wide range of cell types. Cellular responses to interferon‑gamma (INF‑γ) are mediated by its heterodimeric cell surface receptor (IFN‑γR), which activates downstream signal transduction cascades, ultimately leading to the regulation of gene expression. As an inflammatory cytokine, INF‑γ was studied as a mediator of periodontal destruction in animal and human studies.[15]
Receptor activator of nuclear factor‑kappa B ligand‑receptor activator of nuclear factor‑kappa β‑osteoprotegerin axisRANK, RANKL, and OPG are cytokines that belong to TNF‑α super family. RANK is a receptor found on the surface of osteoclast precursors. When RANK binds to its ligand RANKL, it stimulates the differentiation of these precursor cells into mature osteoclasts. OPG competes with RANKL by binding to RANK without stimulating any differentiation. It is the ratio of RANKL and OPG expressions that is important in inflammation‑induced bone resorption, including periodontitis.[15]
ROLE OF RECEPTOR ACTIVATOR OF NUCLEAR FACTOR‑KAPPA BETA/OSTEOPROTEGERIN IN PERIODONTAL DISEASE
Bone resorption and formation are regulated by the relative concentrations of RANKL, RANKL receptor RANK on osteoclast precursor cells, and the soluble decoy receptor OPG. When RANKL expression is enhanced relative to OPG, RANKL is available to bind to RANK on osteoclast precursors, tipping the balance to favor the activation of osteoclast formation and bone resorption. The binding of RANKL to osteoclast precursors occurs at a stage when hematopoietic stem cells have differentiated from the colony forming unit (CFU) for granulocytes and macrophages to the CFU for macrophages (CFU‑M). Binding of RANKL to RANK on CFU‑M in the presence of macrophage colony stimulating factor

Grover, et al.: Cytokines in health and disease
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 15
induces differentiation of preosteoclast into a multinucleated cell that becomes a mature osteoclast, which then resorbs bone. When OPG concentrations are high relative to RANKL expression, OPG binds RANKL, inhibiting it to bind to RANK. Preventing the binding of RANKL to RANK leads to reduced formation of osteoclasts and apoptosis of pre‑existing osteoclasts.[16]
ROLE OF CYTOKINES IN BONE UNCOUPLING
Bone is resorbed by osteoclasts, following which new bone is laid down by osteoblasts in the resorption lacunae. Under physiologic conditions, the two activities are coupled, i.e., the amount of bone formed by osteoblasts is equal to that resorbed by osteoclasts. In pathologic processes such as periodontal disease and osteoporosis, the two processes are uncoupled, i.e., there is deficient bone formation following resorption.
The inflammatory process that leads to osteoclastogenesis and bone resorption may also be responsible for the failure to form adequate amount of new bone, i.e., inflammation causes uncoupling of bone formation following bone resorption. Osteoblast survival is a key factor in bone formation. TNF‑α stimulates the production of Dickkopf‑1 (DKK‑1), which suppresses bone formation by inhibiting the WNT (wingless WNT/beta catenin) pathway. DKK‑1, a negative regulator of WNT pathway, is up‑regulated by TNF stimulation through TNF‑1 receptor and p38 mitogen‑activating protein kinase signaling. The up‑regulated DKK‑1 not only promotes bone resorption but also blocks bone formation and repair in the diseased joint. Thus, inflammatory cytokines such as TNF‑α can limit bone formation by inhibiting osteoblast differentiation. In addition, the pro‑inflammatory cytokines may directly stimulate osteoblast or osteoblast precursor indirectly affect by stimulating expression of Fas, a potent apoptotic mediator. PDL cells are an important source of osteoblast precursors. TNF‑α‑induced apoptosis of PDL cells may affect the pool of osteoblast precursors.
Another mechanism for uncoupling is the reduced function of osteoblasts mediated by diminished production of bone matrix proteins. TNF‑α and TNF‑β induce a 2‑fold to 3‑fold reduction in synthesis of noncollagen bone matrix proteins such as osteocalcin by osteoblasts. TNF‑specific inhibitor, etanercept, promotes bone morphogenic protein‑2‑induced ectopic bone formation when applied systemically or locally in vivo, thereby improving the coupling process.[16]
CHEMOKINES IN PERIODONTAL DISEASE
Chemokines are a class of chemotactic cytokines that stimulate recruitment of relatively specific leukocytes subsets. They are secondary inflammatory mediators that are induced by external signals such as IL‑1 or TNF‑α,
growth factors, and viral and bacterial infection or their products.[10] Chemokines are divided into four sub‑families based on molecular structure (CXC, CX3C, CC, and C). The nomenclature has been revised according to the receptor nomenclature (CCL1, CXCL1, etc.). They are named by position of two cysteine residues compared with other amino acids. Chemokines are produced by various resident and infiltrating cells (fibroblasts, osteoblasts, mast cells, epithelial cells, and endothelial cells), they play a key role in inflammation by orchestrating the tissue distribution of leukocyte subsets in tissues and regulating cell migration and proliferation.
Activation of signaling pathways by chemokine receptor binding results in reorganization of the cell cytoskeleton, resulting in pseudopodia which permit the cell to move up the chemotactic gradient.[2] Chemokines that cause recruitment of leukocytes are termed as inflammatory. In persons with periodontitis, the level of IL‑8/CXCL8 in both periodontal tissue and GCF is drastically increased and has been correlated with disease severity.[17] Another chemokine that contribute to the enhanced severity of periodontal disease is MCP‑1, which is supposed to be a major chemoattractant of macrophages in periodontal disease. MCP‑1 activity in GCF is increased in the severity of disease.[10] One of the most abundantly expressed chemokines in periodontitis tissue is macrophage inflammatory protein 1, with expression localized in the connective tissue subjacent to pocket epithelium of inflamed gingival tissues.[7] Chemokines can also exert important effects on bone cells inducing the migration and activation of osteoclasts. In addition, stromal cell derived factor‑1 is a positive regulator of osteoclast function and recently identified as diseased periodontium.[10]
PROSTAGLANDINS IN PERIODONTAL DISEASE
PGs are derived from the hydrolysis of membrane phospholipids. Phospholipase A2 cleaves the sn‑2 position of membrane phospholipids to free arachidonic acid, a precursor of a group of small lipids known as eicosanoids. Arachidonic acid is metabolized by two major enzyme pathways. Lipoxygenases (LO) catalyse the formation of hydroxyeicosatetraenoic acids leading to the formation of leukotrienes (LTs). Cyclooxygenases (COX‑1 and COX‑2) catalyse the conversion of arachidonic acid into PGs prostacyclins and thromboxanes.[18] COX‑1 is a constitutive enzyme responsible for the formation of PGs with physiological functions, while COX‑2 is an inductive enzyme induced primarily by proinflammatory cytokines and leads to the formation of PGs involved in pathophysiological processes such as edema formation and fever.
PGs have 10 sub‑classes, of which D, E, F G, H, and I are the most important in inflammation. They are potent stimulators of bone formation and resorption and are produced by

Grover, et al.: Cytokines in health and disease
16 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
osteoblasts and PDL cells. They also have inhibitory effects on fully differentiated osteoblasts and osteoclasts.[12] PGE2 is a potent stimulator of alveolar bone resorption. PDL cells also produce PGE2 even when unstimulated. This secretion is enhanced by IL‑1b, TNF‑α, and LO. COX products (LTB4, thromboxanes, and PGE2, respectively) play important roles in systemic inflammation, endothelial cell activation, vascular EGF expression, and platelet aggregation.[18]
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Okada H, Murakami S. Cytokine expression in periodontal health and
disease. Crit Rev Oral Biol Med 1998;9:248‑66.2. Preshaw PM, Taylor JJ. How has research into cytokine interactions and
their role in driving immune responses impacted our understanding of periodontitis? J Clin Periodontol 2011;38 Suppl 11:60‑84.
3. Ebersole JL, Dawson DR 3rd, Morford LA, Peyyala R, Miller CS, Gonzaléz OA. Periodontal disease immunology: ‘double indemnity’ in protecting the host. Periodontol 2000 2013;62:163‑202.
4. Lunney JK. Cytokines orchestrating the immune response. Rev Sci Tech 1998;17:84‑94.
5. Giannobile WV. Periodontal tissue engineering by growth factors. Bone 1996;19 1 Suppl:23S‑37S.
6. Genco RJ. Current view of risk factors for periodontal diseases. J Periodontol 1996;67 10 Suppl:1041‑9.
7. Masada MP, Persson R, Kenney JS, Lee SW, Page RC, Allison AC. Measurement of interleukin‑1 alpha and ‑1 beta in gingival crevicular fluid: Implications for the pathogenesis of periodontal disease. J Periodontal Res 1990;25:156‑63.
8. Matsuda N, Lin WL, Kumar NM, Cho MI, Genco RJ. Mitogenic, chemotactic, and synthetic responses of rat periodontal ligament fibroblastic cells to polypeptide growth factors in vitro. J Periodontol 1992;63:515‑25.
9. Edward DR, Murphy G, Reynold JJ. Transforming growth factor beta. J Bone Miner 1987;6:1899‑904.
10. Graves DT. The potential role of chemokines and inflammatory cytokines in periodontal disease progression. Clin Infect Dis 1999;28:482‑90.
11. Kornman KS, Crane A, Wang HY, di Giovine FS, Newman MG, Pirk FW, et al. The interleukin‑1 genotype as a severity factor in adult periodontal disease. J Clin Periodontol 1997;24:72‑7.
12. Laine ML, Farré MA, González G, van Dijk LJ, Ham AJ, Winkel EG, et al. Polymorphisms of the interleukin‑1 gene family, oral microbial pathogens, and smoking in adult periodontitis. J Dent Res 2001;80:1695‑9.
13. Reinhardt RA, Masada MP, Kaldahl WB, DuBois LM, Kornman KS, Choi JI, et al. Gingival fluid IL‑1 and IL‑6 levels in refractory periodontitis. J Clin Periodontol 1993;20:225‑31.
14. Suresh S. A new paradigm in autoimmunity – Role in periodontal disease. Indian J Dent Adv 2011;3:583‑6.
15. Kayal RA. The role of osteoimmunology in periodontal disease. Biomed Res Int 2013;2013:639368.
16. Srinivasan PC. The role of inflammatory cytokines and the RANKL‑RANK‑OPG molecular triad in periodontal bone loss – A review. J Clin Cell Immunol 2013;S13:007.
17. Tsai CC, Ho YP, Chen CC. Levels of interleukin‑1 beta and interleukin‑8 in gingival crevicular fluids in adult periodontitis. J Periodontol 1995;66:852‑9.
18. Van Dyke TE, van Winkelhoff AJ. Infection and inflammatory mechanisms. J Clin Periodontol 2013;40 Suppl 14:S1‑7.

Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 17
INTRODUCTION
Radiation from diagnostic X‑rays constitutes the second largest source of whole body radiation exposure.[1] The diagnostic X‑rays are classified into dental and medical X‑rays based on the health care sector in which it is routinely performed. Dental X‑rays are one of the most frequent diagnostic investigations accounting for nearly one‑third of the total number of radiological examinations in developed countries.[2] Radiological examination is an integral part of clinical dental practice, offering incalculable benefits to the clinicians and patients. Its roles range from diagnosis, treatment planning, treatment guidance, prediction of prognosis to monitoring of treatment outcome.[3] The estimated average number of radiographs per examination across intraoral and panoramic procedures in the literature is 1.75–1.78.[4,5]
The exposure to radiation from these diagnostic X‑rays exerts adverse effects on humans, and these effects are
classified as deterministic and stochastic effects. The various histopathological reactions of tissues and organs that follow localized tissue irradiation, and the radiation syndromes that follow total body irradiation, constitute the deterministic effects while genetic effects and carcinogenesis constitute the stochastic effects.[6] Although no threshold is assumed for stochastic effects, the probability of stochastic effects characteristically dose‑dependent but the severity of the effects is independent of the dose.[6] The substantial reduction in radiation dose without compromising medical effectiveness is therefore necessary to reduce the stochastic radiation effects.[1] The optimization of radiation protection in order to minimize the effective dose exposure to patients and health care providers cannot be overemphasized.[7] The reason to optimize the radiation protection in dentistry is because the repeated exposures to the relatively low radiation doses of routine dental X‑ray heightens the risk of adverse consequences from cumulative doses. A dental X‑ray gives about 1 mrem, and a chest X‑ray about 6 mrem, but nearly all other X‑rays give far higher exposures: Pelvis, 90 mrem; abdomen, 150 mrem; spine, 400 mrem; and barium enema, 800 mrem.[8] The higher dental radiological exposure among the younger age groups may also allow enough time for the manifestation of the deterministic effects of radiation.
Radiation Protection Awareness and Practices in Cameroon Dental Health Care Facilities
Ashu Michael Agbor, Clement Chinedu Azodo1
Department of Community Dentistry, Universite des Montagnes Dental School, Bagante, Cameroon, 1Department of Periodontics, University of Benin, Benin City, Edo, Nigeria
Corresponding Author: Dr. Clement Chinedu Azodo, Department of Periodontics, Prof. Ejide Dental Complex, University of Benin Teaching Hospital, P.M.B. 1111, Ugbowo, Benin City 300001, Edo, Nigeria. E‑mail: [email protected]
ABSTRACTIntroduction: Strict adherence to the radiation exposure guidelines is mandatory when using X-rays for disease detection in order to minimize its harmful effects. The objective of this study was to determine the radiation protection awareness and practices in Cameroon Dental Health care facilities. Materials and Methods: This multiregional questionnaire-based study was conducted among dental clinics located in the capitals of the Littoral, Central, South West, and North West regions of Cameroon. Results: The majority 63 (90.0%) of the participants reported awareness of the adverse effects of radiation on patients and dental professionals. Only 22.9% reported awareness of the agency in-charge of X-ray protection and standardization in Cameroon. The majority of the X-ray machine were located inside the operating room of the dental clinic. The most vulnerable group to the effects of radiation reported was pregnant women while the most vulnerable part of the body to the effects of radiation reported was reproductive organs. The lead shield was the dominantly utilized radioprotective device among the participants. Six meters away from the direction of radiation was the most frequently adopted radioprotection positioning among the participants. Conclusion: Data from this study revealed that many aspects of radiation protection in dental radiology is suboptimal; hence, specific training in education and training in radiation protection is deemed necessary among dental health care professionals in Cameroon. It is recommended that Cameroon National Radiation Protection Agency should establish radiation protection guidelines in dental health care delivery.
Key words: Awareness, dental radiology, knowledge, practices, radiation protection
Original Article
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***

Agbor and Azodo: Radioprotection in dentistry
18 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
A number of epidemiological studies have provided evidence of increased risk of brain, salivary gland, and thyroid tumors from dental radiography.[9] The potential risk of radiograph inducing a fatal cancer in an individual has been estimated to be approximately 1 in 4 million per millirem.[10] The estimate of the probability of fatal cancer by the International Commission on Radiological Protection is 4 × 10−2 per microsieverts (Sv) for a working population and 5 × 10−2 per Sv for the total population.[6]
Dental radiation protection should be considered as a rule, which must be respected in order to protect health care providers, patients, and the environment. This should be in strict adherence to the as low as reasonably achievable (ALARA) concept which states that all exposure to radiation must be kept to a minimum.[11] All exposures to X‑rays should be clinically justified and each exposure should be expected to give the patient a net positive benefit.[12] Proper radiation protection measures in dental radiology include shielding, the adoption of recommended distance, and position to avoid occupational exposure to X‑radiation (primary radiation, leakage radiation, and scatter radiation). During X‑ray exposure, thyroid collar, lead apron, fast film, and film holding devices are used to protect the patients from excess exposure to radiation. Proper selection of exposure factors and good technique are also used for patient protection. Quality assurance program plays an essential part in dental radiation protection by improving diagnostic yield and limiting repeat examinations.[2] Dental X‑ray machine must be monitored for leakage radiation through the use of a film device that can be obtained from the dental X‑ray equipment manufacturers. In developing countries, old and obsolete radiation equipment are usually used without monitoring, posing a high potential occupational radiation exposure from leakage radiation, which occurs from faulty dental X‑ray tube head seal.[12]
Legislations for X‑radiation protection of the environment and workers in industries and health care in developing countries are either nonexistent or unimplemented because of lack of concern, inadequate manpower, and logistics. In Cameroon, the agency responsible for radiation protection is the National Radiation Protection Agency (NRPA), which was in the news on their acquisition of new state of the art equipment for determining the levels of exposure to ionizing radiation to which hospital and industrial workers in the country are subject to.[13] The importance of radiographs in dentistry justifies the need for proper radiation protection. The objective of this study was to determine the radiation protection awareness and practices in Cameroon Dental Health care facilities.
MATERIALS AND METHODS
Ethical considerationThe protocol for this study was reviewed and approval granted by the Cameroonian Ministry of Higher Education and Scientific Research.
Study design/settingThis cross‑sectional study was conducted among dental clinics located in Douala, Yaounde, Buea and Bamenda, which are the regional capitals of the Littoral, Central, South West, and North West regions of Cameroon, respectively.
Study populationA total of 71 dental clinics were approached but seventy of them consented and participated giving a 98.6% participation rate. The authority of consenting clinics nominated a participant who is actively involved in exposing patients to X‑rays. Informed consent was obtained from the nominated participant before the data collection.
Data collection toolA pretested self‑administered questionnaire designed by the authors was used for data collection and distributed to dental clinics with one nominated member of the dental team participating per clinic. The questionnaire was anonymous without identifiers. The questionnaire elicited information on professional status (dentist or dental auxiliary who are dental paraprofessionals), the frequency of radiograph daily, personnel involved in radiography, and area for taking radiographs. Other information obtained were the maintenance of X‑ray machine, knowledge of the effects of radiation on patients and health care providers, measures taken to prevent radiation exposure to both patient and dental health care provider, and awareness of the existence of the National Radiation Agency in Cameroon.
Data collection procedureThe questionnaires were hand delivered to the appointed representatives of the studied dental clinics and collected after filling the same day.
Data analysisData were subjected to descriptive and nonparametric statistics in the form of frequencies, percentages, and cross tabulation using Epi‑Info, version 3.5.2 (Center of Disease Control and Prevention, Atlanta, USA). Chi‑square was used to assess the strength of association and P < 0.05 was considered significant.
RESULTS
The response rate for the study (70/71) was 98.6%.
Demographic characteristics of the participantsThe majority of the participants were males (57.1%) and dental auxiliaries (51.4%). The age range of the participants was 23–58 years, and their mean age was 38.5 ± 8.5 years. The government and private owned dental clinics recorded 40.0% each. Most of the participants (94.3%) indicated that they have received training in dental radiography. Only three (4.3%) participants claimed that they have digital X‑ray units in their clinic. Twenty‑one participants (30.0%) claimed that they shoot, on average, more than three radiographs on

Agbor and Azodo: Radioprotection in dentistry
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 19
a daily basis. Only four (5.7%) of the participants reported that their clinic X‑ray machine was checked regularly [Table 1].
Awareness of adverse effect of the radiation and Cameroon radiation regulatory agencyAlthough a majority 63 (90.0%) of the participants reported awareness of the adverse effect of the radiation on patients and dental professionals, only 22.9% reported awareness of any agency in‑charge of X‑ray protection/standardization in Cameroon [Table 1].
Vulnerable groups to effect of radiationPregnant women, children, and the aged were reported as the most vulnerable group to effects of the radiation in descending order. There is no statically significance association between type of hospital, knowledge of vulnerable groups to effect of radiation, awareness of the adverse effect of the radiation, and Cameroon radiation regulatory agency (P > 0.05) [Table 1].
Vulnerable organs to effect of radiationReproductive organs were reported as the most vulnerable part of the body to effects of the radiation followed by the thyroid gland. However, about one‑third 23 (32.9%) stated no knowledge. There was a statistically significant association between the location of the dental clinic and the most vulnerable part of the body to effects of the radiation (P = 0.01) [Table 2].
Location of X‑ray machine, radioprotection device, and positioningIn terms of geographical location of the X‑ray machine, majority of the machine were inside the clinic [Table 3]. The lead shield was the dominantly utilized radioprotection device among the participants. Six meters away from the direction of radiation was the most frequently adopted radioprotective positioning among the participants. One‑fifth of the participants utilized perpendicular position
Table 1: Demographic characteristics and radiation awareness of the participantsCharacteristics Type of hospital n (%) P
Government Missionary Private TotalAge (years)
20-30 6 (21.4) 4 (28.6) 6 (21.4) 16 (22.9) 0.5031-40 10 (35.7) 4 (28.6) 9 (32.1) 23 (32.9)41-50 9 (32.1) 5 (35.7) 13 (46.4) 27 (38.6)51-60 3 (10.7) 1 (7.1) 0 (0.0) 4 (5.7)
Location (region)Litorral 14 (50.0) 2 (14.3) 16 (57.1) 32 (45.7) 0.02Central 10 (35.7) 6 (42.9) 11 (39.3) 27 (38.6)North West 2 (7.1) 4 (28.6) 1 (3.6) 7 (10.0)South West 2 (7.1) 2 (14.3) 0 (0.0) 4 (5.7)
Professional statusDental surgeon 14 (50.0) 4 (28.6) 16 (57.1) 34 (48.6) 0.21Dental auxiliaries 14 (50.0) 10 (71.4) 12 (42.9) 36 (51.4)
Daily radiographyNever 3 (10.7) 0 (0.0) 4 (14.3) 5 (7.1) 0.30Rarely 4 (14.3) 2 (14.3) 4 (14.3) 10 (14.3)≤3 11 (39.3) 6 (42.9) 17 (60.7) 34 (48.6)>3 10 (35.7) 6 (42.9) 5 (17.9) 21 (30.0)
Awareness of any agency in-charge of X-ray protection/standardization
Yes 7 (25.0) 4 (28.6) 5 (17.9) 16 (22.9) 0.69No 21 (75.0) 10 (71.4) 23 (82.1) 54 (77.1)
Awareness of adverse effect of radiation on patients/dental workers
Yes 27 (96.4) 12 (85.7) 24 (85.7) 63 (90.0) 0.30No 1 (3.6) 2 (14.3) 4 (14.3) 7 (10.0)
The most vulnerable group to effects of the radiation
Children 7 (25.0) 4 (28.6) 5 (17.9) 16 (22.9) 0.09Pregnant women 14 (50.0) 10 (71.4) 20 (71.4) 44 (62.9)Aged 7 (25.0) 0 (0.0) 3 (10.7) 10 (14.3)
Total 28 (100.0) 14 (100.0) 28 (100.0) 70 (100.0)

Agbor and Azodo: Radioprotection in dentistry
20 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
to the ray of radiation. There is no statically significance association between type of hospital, clinic X‑ray machine position, radioprotection positioning, and device among the participants (P > 0.05) [Table 3].
DISCUSSION
The implications of the young age of the participants are on the radiosensitive nature of tissues of younger people and that their prospective lifespan is likely to exceed the latent period of ionizing radiation. Added to this is the cumulative radiation exposure as 48.6% and 30.0% among the participants exposes 1–3 radiographs and more than three radiographs on the average daily, respectively.
Radiation protection agency in any country whether developed or developing country is expected to ensure that radiation safety legislation, established to protect the patient, operator, and the general public from radiation hazards are strictly adhered to. In this study, 63 (90.0%) of the participants reported awareness of the adverse effect of the radiation on patients and dental professionals but only 22.9% were aware of the agency in charge of radiation in Cameroon, NRPA. This
indicates that radiation control in dental practice may be poorly controlled due to the nonactive and functionality of agency in charge of monitoring and evaluation. This can be explained by reports of previous studies which stated that dentists who considered the laid down regulations by their country’s National Institute of Radiation Protection as wholly adequate had a high care attitude and dentists with high concern about radiation hazards, restricted their use of X‑ray examinations.[14] The anecdotal information on many X‑ray equipment used in Cameroon are fairly used, noncompliant with international standard, and have few engineers to effect repair thereby necessitating the need for Cameroon radioprotection agency to take a proactive step. Report of a study in Uganda revealed that most of the X‑ray equipment in that country were more than 30‑year‑old and only 15% of dentists knew when the equipment was last serviced.[15] There is therefore a need to increase radiation knowledge among oral health workers in Cameroon and improve collaboration between National Agency for Radiation Control and the Oral Health care workforce.
Long‑term effects are associated with small amounts of radiation absorbed repeatedly over a long period. Repeated
Table 3: Clinic X‑ray machine position, radioprotection positioning, and device among the participantsCharacteristics Type of hospital n (%) P
Government Missionary Private TotalGeographical location of the X-ray machine in the dental clinic
Behind dental chair 11 (39.3) 2 (14.3) 14 (50.0) 27 (38.6) 0.13Behind the reception 2 (7.1) 0 (0.0) 2 (7.1) 4 (5.7)By dental chair 14 (50.0) 12 (85.7) 11 (39.3) 37 (52.9)Others 1 (3.6) 0 (0.0) 1 (3.6) 2 (2.9)
Preventive measuresLead panel 1 (3.6) 0 (0.0) 0 (0.0) 1 (1.4) 0.53Lead shield 12 (42.9) 7 (50.0) 7 (25.0) 26 (37.1)Regulation of appliance 8 (28.6) 3 (21.4) 11 (39.3) 22 (31.4)Thyroid shield 0 (0.0) 0 (0.0) 1 (3.6) 1 (1.4)Nothing 7 (25.0) 4 (28.6) 9 (32.1) 20 (28.6)
Positions3 m2 in X-ray direction 8 (28.6) 1 (7.1) 14 (50.0) 22 (31.4) 0.90Direction of X-ray 2 (7.1) 1 (7.1) 4 (14.3) 7 (10.0)Perpendicular to the X-ray 6 (21.4) 4 (28.6) 4 (14.3) 14 (20.0)Six meters away from X-ray 12 (42.9) 8 (57.1) 6 (21.4) 26 (37.1)
Total 28 (100.0) 14 (100.0) 28 (100.0) 70 (100.0)
Table 2: The most vulnerable part of body to effects of the radiationAreas Location n (%) P
Litorral North West South West Central TotalBreast 3 (9.4) 1 (14.3) 0 (0.0) 1 (3.7) 4 (5.7) 0.01Reproductive organs 23 (71.9) 6 (85.7) 2 (50.0) 4 (14.8) 36 (51.4)Thyroids 2 (6.3) 0 (0.0) 2 (50.0) 3 (11.1) 7 (10.0)Don’t know 4 (12.5) 0 (0.0) 0 (0.0) 19 (70.4) 23 (32.9)Total 32 (100.0) 7 (100.0) 4 (100.0) 27 (38.0) 70 (100.0)

Agbor and Azodo: Radioprotection in dentistry
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 21
low levels of radiation exposure are linked to the induction of cancer, birth abnormalities, and genetic defects. Individual risks in dental radiography are small but are greater in the younger individuals below 30 years who are most frequently exposed. The regulation 6(1)(e) of IR(ME)R 2000 prohibits the carrying out of a medical exposure on a female of child‑bearing age without an enquiry as to whether they are pregnant.[16] Such an enquiry will not normally be necessary in dental radiography except in vertex occlusal projection because the primary X‑ray beam is likely to irradiate the pelvic area. If the examination is undertaken, the fetal dose must be kept to a minimum consistent with the diagnostic purpose, and the use of a lead apron is advised, principally because of the reassurance, it provides. In this study, pregnant women were considered as the most vulnerable group to the effects of radiation followed by children and the aged. The well‑documented embryological effect of radiation with obvious congenital defect in the literature may be the reason for this information among the participants. It is recognized that dental radiography is often avoided if the patient is known to be pregnant, essentially for psychological reasons. For the vast majority of dental projections, the pelvic area is not irradiated, and an acceptable course of action would be to explain to the pregnant patient that a dental radiograph delivers such a small dose to the fetus that the associated risk can be regarded as negligible. However, because of the emotive nature of radiography during pregnancy, the patient could be given the option of delaying the radiography. Children are susceptible to radiation damage than adults with the developing fetus being more vulnerable. The aged as rightly indicated by the participants are the least vulnerable based on the fact that latency period of radiation effect may outlive their life span.
Disease detection is one of the most important uses of dental radiographs. X‑radiation is harmful to living tissues but because the benefit of disease detection outweighs the risk of biologic damage, it has remained a part of daily dental practice. However, more radiation damage is known to occur with high doses because a rapid delivery of radiation does not allow time for cellular damage to be repaired. Extensive radiation injury also occurs when large areas of the blood are exposed because of the damage to the blood‑forming tissues. Critical organs exposed during dental radiographic procedures in the head and neck region include the following: Skin, thyroid gland, lens of the eye, and bone marrow. The most vulnerable part of the body to effects of the radiation was identified as thyroid by 10% with better knowledge obtained from the South West region while the majority of the participants reported reproductive organs. Although the sensitivity of reproductive organs to effect of radiation is linked to their replication rate, their exposure in dental radiographs is minimal. The thyroid gland has been identified as a critical organ in dental radiology because its damage diminishes the quality of life of the affected person.[17] The noted geographical difference in knowledge of most vulnerable part of the body to effects of the radiation is
in consonance with geographical differences in health practices among health workers. Despite the noted knowledge about the most vulnerable part of the body among the participants, one‑third (32.9%) lacked knowledge of vulnerable part of the body. This general lack of knowledge is cause for concern, not only because of the standard of radiation protection that is being practiced for the patients’ benefits, but also for their own protection. About one‑third (32.9%) of the participants gave do not know responses which collaborated the high level of “don’t know” responses reported in a survey among Ugandan dentists.[15]
Although radiographs are indispensable diagnostic tools, the increased effective doses of common intraoral and extraoral imaging techniques are high enough to warrant reconsideration of means to reduce patients’ exposure.[18] Adequate shielding can greatly reduce the occupational exposure in dental radiology. Protective barriers that absorb the primary beam can be incorporated into the office design, thus protecting the operator from primary and scatter radiation. Whenever possible, the dental radiographer should stand behind a protective barrier such as a wall during X‑ray exposure. Most dental offices incorporate adequate shielding in walls through the use of several thickness of common construction materials such as a dry wall.
However, in this study, most of the X‑ray machines were located inside the dental clinic making shielding a priority in radiation hazard protection. Lead protection of the abdomen has little relevance to dental radiation protection; however, thyroid shielding has some value.[19] Exposure reduction by the shielding varied from 5% to 56% for a complete‑mouth survey, 2–18% for a bitewing survey, and 10–79% for a panoramic survey. In a study, thyroid skin measured were 63–92% lower on children and 33–84% lower exposures on adults in offices in which shields were used as compared to offices in which they were not used.[20] The use of thyroid protection collars is an effective preventive measure against exceeding occupational organ dose limits which considerably reduces the effective dose. Therefore, thyroid protection collars should be a required component of dental X‑ray protection in accordance with the ALARA principle.[4,20] However, lead apron and thyroid shield was the most and rarely used radioprotection device, respectively, in this study. In comparison, leaded aprons in 95% for extraoral films and thyroid collars in 85% for intraoral films were among the radiation dose‑reducing strategies adopted in the North American Dental Schools.[21] Personal lead shielding devices significantly reduce gonadal dose in the case of accidental exposure.[22] Dose estimation revealed significantly larger effective dose per year in some dentists is explainable by lower lead aprons use.[22] The general poor knowledge and practices regarding radiation protection may lead some dentists and patients to receive considerably higher radiation doses than those recommended by the International Commission on Radiology protection unknowingly.

Agbor and Azodo: Radioprotection in dentistry
22 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
One of the most effective ways for the operator to avoid the primary beam and limit X‑radiation exposure is distance. The dental radiographer must stand at least 6 feet away from the X‑ray tube head during X‑ray exposure. When maintaining this distance is not possible, the protective barrier must then be used. Another important way for the operator to avoid the primary beam is to maintain proper positioning during X‑ray exposure. To avoid the primary beam, which travels in a straight line, the dental radiographer must be positioned perpendicular to the primary beam, or at 90° to 135° angle to the beam. About one‑third of the participants (31.4%) stand at least 2 m square in the direction of radiation, 20.0% perpendicular to the direction the ray of radiation, 37.1% at least 6 m away from the direction of radiation, and 10.0% in the direction of the radiation. A study in Belgium[23] showed that the distance of the dentist to the radiation tube during exposure was on the average 2.2 m, although 8% of the dentists assisted in holding the image receptor inside the patient’s mouth.
CONCLUSION
Data from this study revealed that many aspects of radiation protection in dental radiology is suboptimal; hence, specific training in education and training in radiation protection is deemed necessary among dental health care professionals in Cameroon. It is recommended that Cameroon NRPA should establish radiation protection guidelines in dental health care delivery.
REFERENCES1. Cohen BL. The nuclear energy option. In: How Dangerous is Radiation?
Ch. 5. Plenum Press; 1990. Available from: http://www.phyast.pitt.edu/~blc/book/chapter5.html. [Last accessed on 2013 Apr 01].
2. Anzai K, Ban N, Ozawa T, Tokonami S. Fukushima Daiichi nuclear power plant accident: Facts, environmental contamination, possible biological effects, and countermeasures. J Clin Biochem Nutr 2012;50:2‑8.
3. Roth J, Schweizer P, Gückel C. Basis of radiation protection. Schweiz Med Wochenschr 1996;126:1157‑71.
4. American Dental Association Council on Scientific Affairs. The use of dental radiographs: Update and recommendations. J Am Dent Assoc 2006;137:1304‑12.
5. Brocklebank LM. Dental radiology: Capture your image. Dent Update 1998;25:94‑6, 98, 100‑2.
6. Molander B. Panoramic radiography in dental diagnostics. Swed Dent J Suppl 1996;119:1‑26.
7. Bell GW. Use of dental panoramic tomographs to predict the relation between mandibular third molar teeth and the inferior alveolar nerve.
Radiological and surgical findings, and clinical outcome. Br J Oral Maxillofac Surg 2004;42:21‑7.
8. Araujo MT, Cury‑Saramago AA, Motta AF. Clinical and radiographic guidelines to predict pubertal growth spurt. Dent Press J Orthod 2011;16:98‑103.
9. Horner K, Hirschmann PN. Dose reduction in dental radiography. J Dent 1990;18:171‑84.
10. United Nations. Sources and effects of ionizing radiation. Report to the General Assembly with Annexes, United Nations Scientific Committee on Effects of Atomic Radiation (UNSCEAR). UN. New York; 1977.
11. National Council on Radiation Protection and Measurements (NCRP). Natural Radiation in the United States. NCRP Report No. 45. Washington DC; 1975.
12. Tanner RJ, Wall BF, Shrimpton PC, Hart D, Bungay DR. Frequency of Medical and Dental X‑Ray Examinations in the UK, 1997‑98 Report NRPB‑R320. Available from: http://www.hpa.org.uk. [Last accessed on 2013 Apr 01].
13. Cameroon National Radiation Protection Agency, NRPA Purchases Radiation Detection Machinery. Available from: http://www.news.cameroon‑today.com/cameroon‑national‑radiation‑protectionagency‑ nrpa‑purchases‑radiation‑ detection‑machinery/4507/#ixzz2Vh1DuKHt. [Last accessed on 2015 Apr 01]
14. Svenson B, Söderfeldt B, Gröndahl HG. Analysis of dentists’ attitudes towards risks in oral radiology. Dentomaxillofac Radiol 1996;25:151‑6.
15. Mutyabule TK, Whaites EJ. Survey of radiography and radiation protection in general dental practice in Uganda. Dentomaxillofac Radiol 2002;31:164‑9.
16. Horner K. Review article: Radiation protection in dental radiology. Br J Radiol 1994;67:1041‑9.
17. Bourgeois M, Wood RE, Pharoah MJ. Reducing transmitted radiation in dental radiography. Health Phys 1992;62:546‑52.
18. Ludlow JB, Davies‑Ludlow LE, White SC. Patient risk related to common dental radiographic examinations: The impact of 2007 International Commission on Radiological Protection recommendations regarding dose calculation. J Am Dent Assoc 2008;139:1237‑43.
19. Sikorski PA, Taylor KW. The effectiveness of the thyroid shield in dental radiology. Oral Surg Oral Med Oral Pathol 1984;58:225‑36.
20. Martínez Beneyto Y, Alcaráz Banos M, Pérez Lajarin L, Rushton VE. Clinical justification of dental radiology in adult patients: A review of the literature. Med Oral Patol Oral Cir Bucal 2007;12:E244‑51.
21. Geist JR, Katz JO. Radiation dose‑reduction techniques in North American dental schools. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:496‑505.
22. Wood RE, Harris AM, van der Merwe EJ, Nortjé CJ. The leaded apron revisited: Does it reduce gonadal radiation dose in dental radiology? Oral Surg Oral Med Oral Pathol 1991;71:642‑6.
23. Jacobs R, Vanderstappen M, Bogaerts R, Gijbels F. Attitude of the Belgian dentist population towards radiation protection. Dentomaxillofac Radiol 2004;33:334‑9.
How to cite this article: ???.
Source of Support: Nil, Conflict of Interest: None declared.

© 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow 23
INTRODUCTION
Cigarette smoking is considered as a major risk factor for mortality and morbidity around the world.[1] Smokers in the developing countries comprise 73% of the world’s smoking population, and these countries are at increased risk of health, economic, and social impacts of smoking‑related diseases.[1] Smoking‑related diseases have been the primary cause of mortality and morbidity for the past three decades in Malaysia.[2] Cigarette smoking is an established risk factor of oral and periodontal diseases. Scientific literature indicates that smoking and body weight are related.[3] Body mass index (BMI) and smoking are inversely related, and smoking cessation has been linked to weight gain.[3] Consumption of energy‑dense nutrient‑poor foods (sugar‑sweetened beverages, chips, and baked foods) has been a traditional risk factor for obesity.[4] Recent data have shown that obesity or weight gain is also associated with oral diseases, particularly chronic periodontal disease.[5] Adipose tissue secretes various
cytokines and hormones that are involved in the inflammatory cascade, thus indicating that similar pathways are linked in the pathophysiology of obesity and chronic periodontal disease. It has been suggested that obesity is second only to smoking as the strongest risk factor for chronic periodontal tissue destruction.[5,6]
A systematic review concluded a positive association between weight gain and chronic periodontal disease.[5] The study opined that these results were from limited evidence and suggested the need for more studies. The aim of this study was to evaluate the effect of smoking on BMI and periodontal status. The study also evaluates the correlation between these parameters (BMI, smoking, and periodontal status).
Association between Smoking, Body Mass Index, and Periodontal Disease:
A Case–Control StudyShelly Arora, Srinivas Sulugodu Ramachandra, Kalyan C. Gundavarapu
Faculty of Dentistry, SEGi University, Petaling Jaya, Malaysia
ABSTRACTIntroduction: Smoking and obesity are associated with chronic periodontal disease. Chronic periodontal disease has been suggested to be an associated risk factor for obesity. The aim of this study was to evaluate the effect of smoking on body mass index (BMI) and periodontal status of patients. Materials and Methods: A total of 134 subjects (67 smokers and 67 nonsmokers) aged between 24 and 45 years were included in the study. Periodontal status was categorized into healthy, gingivitis, and periodontitis (mild, moderate, and severe, and into localized and generalized). BMI was calculated using height and weight of the patients. A simple descriptive statistics was obtained by analyzing the collected data using MedCalc 15.4. Results: The results indicated that nonsmokers have higher BMI (mean = 23.4 kg/cm2, 95% confidence interval [CI] = 22.7–24) as compared to smokers (mean = 21.1 kg/cm2, 95% CI = 20.7–21.6). Among 134 subjects, 49 were suffering from chronic periodontitis. People in the overweight category were 26. Subjects who were both overweight and suffering from chronic periodontitis were only 6% (n = 8). Conclusions: The study found an association between periodontal disease and smoking, but no association between obesity and periodontal disease was noticed. Studies with larger sample size and patients from obesity clinics should be studied.
Key words: Body mass index, obesity, periodontal status, smoking
Original Article
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Shelly Arora, Faculty of Dentistry, SEGi University, No. 9, Jalan Teknologi, Taman Sains, Kota Damansara, Petaling Jaya, Selangor, Malaysia. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???

Arora, et al.: Association between smoking, body mass index, and periodontal disease
24 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
MATERIALS AND METHODS
A total of 158 patients reporting to Oral Health Center of the University and were approached to participate in the study. Among these patients, 134 subjects volunteered to participate in the study. The study was approved by the Institutional Review Board and Ethics Committee of the university. Informed consent was obtained from the participants. All the participants in the study were age and sex matched. Subjects in the age group of 25–45 years were included in the study. Subjects who were smoking ten or more cigarettes a day for more than a year were considered as smokers. Patients who were suffering from aggressive periodontitis and systemic diseases such as diabetes mellitus, hypertension, asthma, and cardiovascular disease were excluded from the study. The subjects were divided into the two groups: smokers (Group I) and nonsmokers (Group II). The periodontal statuses of all the subjects were examined by two calibrated examiners using a mouth mirror and the University of North Carolina‑15 probe. Subjects were categorized into healthy, chronic gingivitis, and chronic periodontitis. Chronic periodontitis was further categorized into localized and generalized based on extent and into mild, moderate, and severe based on severity. Chronic gingivitis and chronic periodontitis were diagnosed based on bleeding on probing and clinical attachment loss (CAL), respectively.[7] CAL of 1–2 mm, 3–4 mm, and >5 mm was used to categorize mild, moderate, and severe periodontitis.[7]
BMI was measured using height and weight of the subjects. BMI was calculated using the formula weight/square height.[8] BMI between 19 and 24, 25–29, and >30 kg/cm2 was categorized as normal, overweight, and obese, respectively. A simple descriptive statistics was obtained by analyzing the collected data using MedCalc 15.4 (Medcalc software bvba, Belgium).
RESULTS
Among the 158 patients approached to participate in the study, 134 agreed to be included in the study. Hence, the response rate was 85% which is good. Among 134 subjects, 67 were smokers and 67 nonsmokers, in the age range of 24–45 years. Among the smokers, 45 males and 22 females were present with an average age of 32 years. In the nonsmokers group, 41 were males and 26 were females with an average age of 30 years. An inverse relationship was observed between smoking and BMI. BMI was found to be higher among nonsmokers (mean = 23.4 kg/cm2, 95% confidence interval [CI] = 22.7–24) as compared to smokers (mean = 21.1 kg/cm2, 95% CI = 20.7–21.6) [Table 1]. Among smokers, 90% of the subjects were in the category of 18.5–24.9 kg/cm2 (normal). In nonsmokers, 58% were in the category of 18.5–24.9 kg/cm2 (normal) BMI and 37% were in the category of 25–29.9 kg/cm2 BMI (overweight).
Among the nonsmokers, 72% were diagnosed with chronic gingivitis and 28% were diagnosed with chronic periodontitis. Among the chronic periodontitis group, 8% were suffering from localized periodontitis of mild severity and 3% were having localized periodontitis of moderate severity. Around 5% had generalized periodontitis of mild severity and 6% had generalized periodontitis of moderate severity [Table 2]. Among smokers, 55% cases were diagnosed with chronic gingivitis and 45% were diagnosed with chronic periodontitis. In the localized periodontitis group, 16%, 4%, and 10% were suffering from mild, moderate, and severe variety of periodontitis, respectively. Under generalized periodontitis, 3% were mild and 10% were moderate periodontitis [Table 2].
Among 134 subjects, 26 were in the category of overweight (25.0–29.9 kg/cm2 BMI). Among these 26, 13.5% (n = 18) were having chronic gingivitis, 2.2% (n = 3) mild localized periodontitis, 0.75% (n = 1) moderate localized periodontitis, 0.75% (n = 1) mild generalized periodontitis, and 2.2% (n = 3) moderate generalized periodontitis. Among 134 subjects, 49 were suffering from chronic periodontitis. People in the overweight category were 26. Subjects who were both overweight and suffering from chronic periodontitis were only 6% (n = 8). There was no association found between BMI and chronic periodontitis.
Table 1: Age, gender, education, and mean body mass index in smokers and nonsmokersVariables Smokers NonsmokersAge
25-35 48 5235-45 16 12
GenderMale 45 41Female 22 26
EducationElementary 10 12Secondary 15 20Degree 42 35
Mean BMI (kg/cm2) 20.6892 23.229295% CI 20.0814-21.2970 22.4172-24.0411
BMI between 19-24, 25-29, and >30 kg/cm2 was categorized as normal, overweight, and obese, respectively. BMI: Body mass index, CI: Confidence interval
Table 2: Distribution of periodontitis in smokers and nonsmokersPeriodontitis category Smokers
(%)Nonsmokers
(%)Mild localized periodontitis 16 (11) 8 (5)Moderate localized periodontitis 4 (3) 5 (3)Severe localized periodontitis 10 (7) 0Mild generalized periodontitis 3 (2) 8 (5)Moderate generalized periodontitis 10 (7) 9 (6)Severe generalized periodontitis 0 0

Arora, et al.: Association between smoking, body mass index, and periodontal disease
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 25
DISCUSSION
Current scientific literature suggests obesity is a risk factor for development, progression, and severity for chronic periodontal disease. Quetelet index is used to quantify BMI into normal, overweight, and obese. Cigarette smoking is a modifiable risk factor for periodontal disease. Smoking also leads to decreased BMI and cessation of smoking is associated with weight gain. This study evaluated the association between smoking, obesity, and chronic periodontal disease.
The findings in our study showed a significant association between smoking and BMI. In smokers, the majority of the subjects (90%) had normal BMI, whereas in nonsmokers, 58% were in the normal BMI category, whereas 37% were in the overweight BMI category. Hence, BMI was lower in smokers compared to nonsmokers. The findings of our study are in agreement with literature reported earlier.[9‑12] This can be explained on the basis that nicotine consumption leads to suppression of appetite, decreased intake of food, and weight loss.[13] Clinicians who are attempting tobacco cessation on patients should be aware of the possibility of weight gain in these patients.[9] Clinicians should address this issue as well as in tobacco cessation therapies.[9]
In this study, 45% of smokers had chronic periodontal disease. Preclinical and clinical data are unanimous in demonstrating that smokers present increased susceptibility, greater severity, and faster progression of periodontal disease compared with nonsmokers.[14‑16] In comprehensive periodontal therapies, identification and adjustment of modifiable risk factors are significant. Studies have shown that patients benefit with improved periodontal health upon enrolling in smoking cessation programs since smoking is a modifiable risk factor. Hence, clinicians should encourage smokers to enroll in cessation strategies.[14]
Systematic reviews have found that overweight, obesity, weight gain, and increased waist circumference may be risk factors in initiation and development of periodontal disease.[5,6] Obesity is hypothesized to involve immune‑inflammatory alterations, and the condition has been related to increased susceptibility to periodontitis.[17] However, in the present study, there was no association observed between obesity and periodontal disease. This is in agreement with studies conducted by Awad et al.[18] and Kongstad et al.[19] Awad et al. concluded that mean age of 24 years was the possible reason for nonassociation between obesity and periodontal disease.[19] The mean age in the present study was 30 years. This could be the possible reason for nonassociation between obesity and periodontal disease. Awad et al. used pocket depths to diagnose periodontal disease in their subjects, which could result in underestimation of the periodontal disease.[18] In the present study, CAL was used to diagnose and quantify the severity of periodontal disease. de Castilhos et al. used CAL to measure and quantify periodontal disease
in their study on obesity and periodontal disease. The study showed no association between obesity and periodontal disease; however, positive between gingivitis and obesity was observed.[20]
Limitations of the studyThe design of the study was cross‑sectional in nature. The mean age of the patients was around 30 years, so application of the results of this study to the general population would not be appropriate. The small sample size is also a limitation of the study.
CONCLUSIONS
The study found an association between BMI and smoking, whereas no association was noticed between BMI and chronic periodontal disease. A significant association was observed between smoking and chronic periodontal disease. Smoking was confirmed as a risk factor for chronic periodontal disease. Longitudinal studies, studies with larger sample size and studies in obesity clinics could be useful in substantiating these findings.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Gilmore AB, Fooks G, Drope J, Bialous SA, Jackson RR. Exposing and
addressing tobacco industry conduct in low‑income and middle‑income countries. Lancet 2015;385:1029‑43.
2. Lim HK, Ghazali SM, Kee CC, Lim KK, Chan YY, Teh HC, et al. Epidemiology of smoking among Malaysian adult males: Prevalence and associated factors. BMC Public Health 2013;13:8.
3. Tian J, Venn A, Otahal P, Gall S. The association between quitting smoking and weight gain: A systemic review and meta‑analysis of prospective cohort studies. Obes Rev 2015;16:883‑901.
4. Drewnowski A. The real contribution of added sugars and fats to obesity. Epidemiol Rev 2007;29:160‑71.
5. Nascimento GG, Leite FR, Do LG, Peres KG, Correa MB, Demarco FF. Is weight gain associated with the incidence of periodontitis? A systematic review and meta‑analysis. J Clin Periodontol 2015;42:495‑505.
6. Keller A, Rohde JF, Raymond K, Heitmann BL. Association between periodontal disease and overweight and obesity: A systematic review. J Periodontol 2015;86:766‑76.
7. Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol 1999;4:1‑6.
8. Body Mass Index. Accessed from: https://www.en.wikipedia.org/wiki/Body_mass_index. [Last accessed on 2015 Jun 28].
9. Munafò MR, Tilling K, Ben‑Shlomo Y. Smoking status and body mass index: A longitudinal study. Nicotine Tob Res 2009;11:765‑71.
10. Dare S, Mackay DF, Pell JP. Relationship between smoking and obesity: A cross‑sectional study of 499,504 middle‑aged adults in the UK general population. PLoS One 2015;10:e0123579.
11. Macera CA, Aralis HJ, Macgregor AJ, Rauh MJ, Han PP, Galarneau MR. Cigarette smoking, body mass index, and physical fitness changes among male navy personnel. Nicotine Tob Res 2011;13:965‑71.
12. Plurphanswat N, Rodu B. The association of smoking and demographic

Arora, et al.: Association between smoking, body mass index, and periodontal disease
26 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
characteristics on body mass index and obesity among adults in the U.S 1999‑2012. BMC Obes 2014;1:18.
13. Jo YH, Talmage DA, Role LW. Nicotinic receptor‑mediated effects on appetite and food intake. J Neurobiol 2002;53:618‑32.
14. Nociti FH Jr., Casati MZ, Duarte PM. Current perspective of the impact of smoking on the progression and treatment of periodontitis. Periodontol 2000 2015;67:187‑210.
15. Santos A, Pascual A, Llopis J, Giner L, Kim DM, Levi P Jr., et al. Self‑reported oral hygiene habits in smokers and nonsmokers diagnosed with periodontal disease. Oral Health Prev Dent 2015;13:245‑51.
16. Visvanathan R, Mahendra J, NA, Pandisuba, Chalini. Effect of smoking on periodontal health. J Clin Diagn Res 2014;8:ZC46‑9.
17. Palle AR, Reddy CM, Shankar BS, Gelli V, Sudhakar J, Reddy KK. Association between obesity and chronic periodontitis: A cross‑sectional study. J Contemp Dent Pract 2013;14:168‑73.
18. Awad M, Rahman B, Hasan H, Ali H. The relationship between body mass index and periodontitis in Arab patients with type 2 diabetes mellitus. Oman Med J 2015;30:36‑41.
19. Kongstad J, Hvidtfeldt UA, Grønbaek M, Stoltze K, Holmstrup P. The relationship between body mass index and periodontitis in the Copenhagen City Heart Study. J Periodontol 2009;80:1246‑53.
20. de Castilhos ED, Horta BL, Gigante DP, Demarco FF, Peres KG, Peres MA. Association between obesity and periodontal disease in young adults: A population‑based birth cohort. J Clin Periodontol 2012;39:717‑24.

Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 27
INTRODUCTION
In every field of dentistry, an awareness regarding the importance of preserving tooth tissue, combined with a patient friendly approach is becoming self‑evident.[1] The best way to ensure maximum life for the natural tooth is to respect the sound tissue and protect it from damage by using minimally invasive techniques in restorative dentistry.[2] The current odontologic era is characterized by an increasing move toward less invasive treatment and toward preventive dentistry. The aim of minimally invasive restorative treatment in dentistry is selective removal of carious tissue and the preservation of the maximum amount of sound dental tissue.[1‑5]
Chemomechanical caries removal involves the chemical softening of carious dentin, followed by its removal with gentle excavation. It involves the selective removal of degraded collagen fibrils in carious dentin lesion while preserving the affected demineralized dentin layer.[6] Since 1970s many chemical compositions have been used for chemomechanical caries removal. These include GK – 101, Caridex, Carisolv, and enzymes.[6]
In the present study, Carie‑care (Inc., Bengaluru, Karnataka, India) was used for the noninvasive chemomechanical removal of dental caries. It is a gel‑based formulation containing a purified enzyme, derived from the plant Carica papaya (papaya) which exhibits antibacterial and anti‑inflammatory properties. It acts as a debris removing agent with no harmful effect on sound tissues because of the enzyme specificity along with the benefits of Clove oil which are analgesic and antiseptic.[7]
Another self‑limiting concept in mechanical caries removal has been brought into practice by the introduction of SmartPrep bur (SS White Burs, Inc., Lakewood, NJ, USA).[8] The paddle‑shaped bur used in this study has a unique flute design and is constructed from a medical‑grade polyether‑ketone‑ketone, with a particular hardness and wear resistance that reportedly enables it to remove only the soft caries‑infected dentin, leaving the caries‑affected dentin intact. It is utilized exclusively at low speed (500–800 rpm). The bur quickly dulls and vibrates when it encounters the more highly calcified caries‑affected dentin.[9]
Thus, the aim of this study was to evaluate clinically the efficiency of caries removal using a new chemomechanical agent (Carie‑care) compared to the SmartPrep burs for complete caries excavation including the need for local anesthesia, duration of the treatment, and the pain reaction.
Clinical Evaluation of Caries Removal in Primary Teeth Using Carie‑care and SmartPrep
Burs: An In vivo StudyPooja Ravindra Shivasharan, A. Katge Farhin, Mayur Manohar Wakpanjar, Ashveeta Shetty
Department of Pedodontics and Preventive Dentistry, Terna Dental College, Navi Mumbai, Mumbai, Maharashtra, India
Original Article
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
ABSTRACTBackground: Ultra conservative caries removal now has become an integral part of Minimal Invasive Dentistry. The main objective of deep caries removal is to conserve the tooth structure as well to maintain the integrity of pulpal health. Aim: To evaluate clinically the efficiency of caries removal using Carie-Care compared to the SmartPrep burs for complete caries excavation. Materials and Methods: Split mouth study was done in 64 children where caries excavation was done using Carie-Care on one side and Smart burs on the other side. The parameters assessed were complete caries excavation, pain reaction, need for local anesthesia and mean time required. Results: The differences between complete caries excavation, pain reaction and need for local anesthesia using both the techniques were statistically insignificant. Whereas the time taken for caries removal using Carie‑Care was significantly less than Smart burs (P = 0.001). Conclusion: Both the techniques can be used effectively for caries excavation in primary teeth.
Key words: Carie-care, caries, chemomechanical agents, SmartPrep bur
Corresponding Author: Dr. Pooja Ravindra Shivasharan, Department of Pedodontics and Preventive Dentistry, Terna Dental College, Sector 22, Plot No. 12, Nerul (W), Navi Mumbai ‑ 400 706, Mumbai, Maharashtra, India. E‑mail: [email protected]

Shivasharan, et al.: Clinical evaluation of caries removal using minimal invasive techniques
28 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
MATERIALS AND METHODS
Ethical clearance was obtained by institutional review board. Informed consent was obtained from parents or guardians to conduct the study. The study was conducted in the Department of Pedodontics and Preventive Dentistry, Terna Dental College, Nerul, Navi Mumbai. This study was a clinical controlled study (split‑mouth) where two methods of caries removal were compared in the same patient. The sample size was selected empirically and not based on any assumptions and statistical calculations. The study included a total of 32 healthy children aged 5–10 years. Each child had two contralateral primary teeth showing comparable open carious lesions. A total of 64 primary teeth were included in this study.
Selection criteria• Bilateral open carious lesion with dentin involvement• Opening should be large enough to allow penetration of
a small excavator• No proximal caries as evidenced by bitewing radiographs• Teeth without clinical or radiographic evidence of pulp,
furcation, or periapical pathosis.
Teeth were divided into two groups according to the method of caries removal. Each group consisted of 32 teeth.
Group I: Caries was removed using the Carie‑Care (Ecoworks Inc., Bengaluru, Karnataka, India).
Group II: Caries was removed using the SmartPrep burs (SS White Burs, Inc., Lakewood, NJ, USA).
Clinical proceduresTreatment was carried out according to the following steps:• No local anesthesia was given, unless required• Isolation was done using cotton rolls and saliva ejector[3]
• Caries removal was performed using either of the two methods.
Group I: Using the chemomechanical methodCarie‑Care (Ecoworks Inc., Bengaluru, Karnataka, India) was applied on the carious lesion according to the manufacturer’s instruction for 1 min [Figure 1]. The caries was gently excavated using blunt spoon excavator. Caries detecting dye was applied on the cavity for 10 s. Dye was water washed using three‑way syringe.
Group II: Using SmartPrep bursThis group consisted of 32 samples. The carious portion of these samples was excavated with the help of SmartPrep bur (SS White Burs, Inc., Lakewood, NJ, USA) at slow speed [Figure 2]. During the excavation procedure, there was no limitation to number of burs used, but the main aim was to remove all the carious portion of dentin.[10] Caries‑detector dye “Seek®” (Ultradent product Inc., USA) was applied on the cavity for 10 s and the dye was water washed using three‑way syringe [Figure 3] .
Assessment proceduresFor each patient, the following was recorded by the same investigator: Pain reaction using sound, eye and motor scale (SEM) according to Wright et al.[11] [Table 1].
Figure 1: Application of Carie‑care in the maxillary left primary canine
Figure 2: Caries excavation using SmartPrep bur
Figure 3: Application of caries detecting dye (Seek®)

Shivasharan, et al.: Clinical evaluation of caries removal using minimal invasive techniques
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 29
It is an objective method for pain assessment where measurement of comfort was taken according to three types of observations; SEM. The level of response for each observation was given a numerical value (score), and these values were averaged to obtain the comfort level [Table 1].
The need for local anesthesia which was given if the patient scored more than two in any of the SEM.[11]
The total working time, taken for caries removal and cavity preparation with either method, was recorded in minutes using a stopwatch. When anesthesia was given, time was recorded twice:1. The total working time of caries removal including time
of anesthesia administration2. Only the operative time of caries removal excluding time
of anesthesia administration.
Statistical methodsAll data were entered into a Microsoft Office Excel (version 2013) in a spreadsheet and checked for errors and discrepancies. Data analysis was done using Windows‑based “MedCalc Statistical Software” version 13.3.1 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2014).• The proportion of complete caries excavation was
compared between the Carie‑care and SmartPrep burs using Fischer’s exact test
• The comfort/pain levels using SEM was compared between the two groups (Carie‑care and SmartPrep burs) using Chi‑square test
• Mean working time was compared between the groups using unpaired t‑test.
RESULTS
Of 64 teeth, complete caries excavation was observed in 28 (43.75%) and 25 (39.07%) teeth with Carie‑care and SmartPrep burs, respectively. The comparison between both groups based on caries excavation was statistically insignificant [Table 2].
In the present study, local anesthesia was required for only one tooth using Carie‑care and three teeth using SmartPrep burs. Score 1 was observed in 48.44% with Carie‑care and
45.31% with SmartPrep burs. Score 3 was observed only in 1.56% and 4.69% using Carie‑care and SmartPrep burs, respectively. Both scores showed statistically insignificant result [Table 3, Graph 1].
The mean time required for the procedure was longer for SmartPrep burs (7.77 min) as compared to Carie‑care (4.53 min). On comparison of mean times between both the groups, the results showed statistically significant difference (P < 0.001) [Table 4].
DISCUSSION
The development of caries removal techniques in restorative dentistry is progressing toward a more biological and conservative direction. The chemomechanical caries removal technique became an area of interest in dental researches due to its concept of tissue preservation. As only carious dentin is removed, the painful removal of sound dentin is avoided and hence, the need for local anesthesia is minimized.[6]
In the chemomechanical method, partially degraded collagen in carious dentine will be chlorinated by chemomechanical caries removal solutions. This chlorination affected the secondary and/or quaternary structure of collagen by disrupting hydrogen bonding. Carious material removal was thus facilitated. The main advantage of this method is that it does not require complete patient cooperation.
Papacarie® (Formula and Acao, Sao Paulo – Brazil) is a chemomechanical caries removal product composed of papain, chloramine, toluidine blue, salts, and a thickening vehicle.[3] It obtains a synergistic action from each of its components that facilitates the removal of the decay with highly antimicrobial properties.
Table 1: Sound eye motor scaleObservation Comfort or pain level
Score 1Comfort
Score 2Discomfort
Score 3Moderately painful
Score 4Painful
Sounds No sounds indicating pain
Nonspecific sounds, possible pain indication
Specific verbal complaints, e.g., “ow” raises voice
Verbal complaints indicating intense pain, e.g., scream, sobbing
Eyes No eye signs of discomfort
Eyes wide, show of concern, no tears
Watery eyes, eyes flinching Crying, tears running down face
Motor Hands relaxed, no apparent body tenseness
Hands show some distress or tension; grasps chair due to discomfort, muscular tension
Random movements of arms or body without aggressive intention of physical contact, grimace twitch
Movements of hands to make aggressive physical contact, e.g., punching, pulling head away
Table 2: Complete caries excavationMethods used for caries excavation
Carie‑care (%) Smart burs (%) P28 (43.75) 25 (39.07) 0.324 NS
NS: Not statistically significant, Fischer’s exact test, significance value set at P≤0.05

Shivasharan, et al.: Clinical evaluation of caries removal using minimal invasive techniques
30 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
Kotb et al. clinically evaluated the efficiency of caries removal using Papacarie compared to the conventional drilling. The results showed that the Papacarie was as efficient as the drill in caries removal from open carious lesions with no significant difference in the operating time.[12]
Another study by Motta et al. concluded that chemomechanical caries removal with Papacarie provided a lesser degree of pain in comparison to conventional caries removal and did not require the use of local anesthesia.[13]
Carie‑care is a product that has been locally introduced and is used in the present study. It has its main active ingredient from papaya extract – an endoprotein, chloramines, and dye which is similar to the composition of Papacarie. In addition, the preparation contains specific percentages of essential oils from plant sources, which has anti‑inflammatory and mild anesthetic effect. The preparation also contains explicit gelling agent in accurate percentage to give exact consistency to gel so that when applied there is no spill over. Carie‑care has most of the ingredients from natural resources. It contains
essential oils which act as anti‑inflammatory agent. It not only softens infected dentin but gives additional advantage of anti‑inflammatory activity and aroma. Carie‑care is in the form of single preparation, which can be stored at 4° for more than 6 months.[14]
Dentinal caries removal is normally accomplished using rotary carbide burs and hand excavators. Carbide burs are superior at a higher speed but mostly are associated with noise, pain, overheating, vibration, and discomfort.[15] Therefore, special burs made of polymer material were used in Group II, and the hardness of this bur is less than that of healthy dentin but more than infected dentin.[16]
The hardness of sound dentin ranges from 54 to 65 KHN and carious dentin having a hardness of 20 KHN or less. The hardness of SmartPrep bur is 50 KHN, thus it removes only carious part of the dentin and gets worn off when comes in the contact with healthy dentin.[10]
Isik et al. compared the caries removal efficiency of polymer burs (Smartburs) and conventional carbide burs microbiologically and found polymer burs to be as effective as the conventional carbide burs in caries removal.[17] Prabhakar and Kiran in another study proved that carbon steel round burs removed caries lesions more efficiently than polymer burs, but they contributed to the over‑preparation of the cavity.[18] In a study done by Shakya et al., the time required for complete excavation procedure was significantly higher in SmartPrep bur group when compared to Diamond points and Carbide bur group.[10]
Caries‑detector dye “Seek®” (Ultradent product Inc., USA) was used to detect remaining caries in samples of this study. “Seek” is a glycol based dye, which stains outer carious dentin and spares affected dentin. It has been shown that dyes that were dispensed in higher molecular weight carriers exhibited reduced diffusion properties in porous tissues. Thus, caries detecting dyes prepared with higher molecular weight polypropylene glycols may prevent over‑staining and excessive removal of caries‑affected or sound dentin.
Gaddam et al. concluded that the mean time taken by stainless steel bur excavation was found to be less and caused more amount of dentinal tubule destruction when compared to Polymer Bur, Carisolv, and Papacarie.[19] Hegde et al. evaluated caries removal using Carie‑care system compared to conventional method among school children. Carie‑care showed a marginal increase in time compared to the conventional technique. Whereas, in the present study, the time required was less with Carie‑care when compared to SmarPrep burs.[7]
The reason for increased time consumption with SmartPrep burs in complete caries excavation may be because of changing the burs that abrade when in contact with hard dentin and attachment of another bur to the handpiece. The
84%
86%
88%
90%
92%
94%
96%
98%
100%
Carie Care Smart burs
Per
cent
age
Comfort / Pain level
Score 4
Score 3
Score 2
Score 1
Graph 1: Pain scores distributed according to cavity preparations in both methods of caries removal
Table 3: Comparison between Carie‑care and SmartPrep bur groups as regards sound, eyes and motor scale for pain assessmentNeed for anesthesia
Scores Carie‑care (%)
Smart burs (%)
P
Carie-care Score 1 (comfort) 31 (48.44) 29 (45.31) 0.305Score 2 (mild) - -
Smart burs Score 3 (moderately painful)
1 (1.56) 3 (4.69)
Score 4 (painful) - -NS: Not statistically significant; Chi‑squared test; significance value set at P≤0.05
Table 4: Mean time for proceduren Mean SD P
Carie-care 32 4.53 1.98 <0.0001*Smart burs 32 7.77 2.34
*Statistically significant; Independent samples t‑test; significance value set at P≤0.05. SD: Standard deviation

Shivasharan, et al.: Clinical evaluation of caries removal using minimal invasive techniques
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 31
number of burs used for complete caries excavation in every case of SmartPrep bur group was more than one.
CONCLUSION
Following conclusions can be derived from the present study:• Both the techniques: Carie‑care and SmartPrep burs can
be used effectively for caries excavation in primary teeth.• The comfort level and need for local anesthesia using
Carie‑care were comparable to SmartPrep burs.• The working time for caries excavation using SmartPrep
burs was more than Carie‑care which was statistically significant.
• Carie‑care was cost effective as compared to SmartPrep burs.
REFERENCES1. Sabalaite BR, Juskiene J. Chemomechanical caries removal for children.
Stomatologija 2005;7:40‑4.2. Bertassoni LE, Marshall GW. Papain‑gel degrades intact nonmineralized
type I collagen fibrils. Scanning 2009;31:253‑8.3. Bussadori SK, Castro LC, Galvão AC. Papain gel: A new chemo‑mechanical
caries removal agent. J Clin Pediatr Dent 2005;30:115‑9.4. Kumar J, Nayak M, Prasad KL, Gupta N. A comparative study of the
clinical efficiency of chemomechanical caries removal using Carisolv and Papacarie – A papain gel. Indian J Dent Res 2012;23:697.
5. Mickenautsch S, Yengopal V, Banerjee A. Atraumatic restorative treatment versus amalgam restoration longevity: A systematic review. Clin Oral Investig 2010;14:233‑40.
6. Beeley JA, Yip HK, Stevenson AG. Chemochemical caries removal: A review of the techniques and latest developments. Br Dent J 2000;188:427‑30.
7. Hegde AM, Preethi VC, Shetty A, Shetty S. Clinical evaluation of chemo‑mechanical caries removal using Carie‑care system among school children. Nitte Univ J Health Sci 2014;4:80‑4.
8. Kochhar GK, Srivastava N, Pandit IK, Gugnani N, Gupta M. An evaluation
of different caries removal techniques in primary teeth: A comparitive clinical study. J Clin Pediatr Dent 2011;36:5‑9.
9. Daniel W, Boston DM. New device for selective dentin caries removal. Quintessence Int 2004;3:40‑7.
10. Shakya VK, Chandra A, Tikku AP, Verma P, Yadav RK. A comparative evaluation of dentin caries removal with polymer bur and conventional burs – An in vitro study. Open J Stomatol 2012;2:12‑5.
11. Wright GZ, Weinberger SJ, Marti R, Plotzke O. The effectiveness of infiltration anesthesia in the mandibular primary molar region. Pediatr Dent 1991;6:238‑42.
12. Kotb RM, Abdella AA, El Kateb MA, Ahmed AM. Clinical evaluation of Papacarie in primary teeth. J Clin Pediatr Dent 2009;34:117‑23.
13. Motta LJ, Bussadori SK, Campanelli AP, da Silva AL, Alfaya TA, de Godoy CH, et al. Pain during removal of carious lesions in children: A randomized controlled clinical trial. Int J Dent 2013;2013:896381.
14. Venkataraghavan K, Kush A, Lakshminarayana C, Diwakar L, Ravikumar P, Patil S, et al. Chemomechanical caries removal: A review and study of an indigen‑ously developed agent (Carie Care (TM) Gel) in children. J Int Oral Health 2013;5:84‑90.
15. Banerjee A, Watson TF, Kidd EA. Dentine caries excavation: A review of current clinical techniques. Br Dent J 2000;188:476‑82.
16. Celiberti P, Francescut P, Lussi A. Performance of four dentine excavation methods in deciduous teeth. Caries Res 2006;40:117‑23.
17. Isik EE, Olmez A, Akca G, Sultan N. A microbiological assessment of polymer and conventional carbide burs in caries removal. Pediatr Dent 2010;32:316‑23.
18. Prabhakar A, Kiran NK. Clinical evaluation of polyamide polymer burs for selective carious dentin removal. J Contemp Dent Pract 2009;10:26‑34.
19. Gaddam D, Ghanashyam M, Vasa AA, Vasanthi D, Ramanarayana B, Mynampati P. Evaluation of the efficacy of caries removal using polymer bur, stainless steel bur, Carisolv, Papacarie – An in vitro comparative study J Clin Diagn Res 2015;7:42‑6.
How to cite this article: ???.
Source of Support: Nil, Conflict of Interest: None declared.

32 © 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow
INTRODUCTION
Dermatoglyphics has gained momentum in the recent years in anthropology, genetics, and medicine, serving as a tool to describe, compare, and contrast, and at times predict occurrences and risks for biomedical events occurring in these major disciplines.
Apart from its use in Forensic Science for identification of an individual, an association between fingerprint patterns and medical ailments such as diabetes, hypertension, psychosis, and breast cancer has also been established. Recently, the field of dental dermatoglyphics has gained momentum through recognition of irregular fingerprints among individuals with periodontitis, dental caries, and certain congenital anomalies such as cleft lip and palate.[1]
Dermatoglyphics is a useful tool for preliminary investigation of conditions with a suspected genetic basis. Furthermore, modes of inheritance patterns of dermatoglyphics trait and characters are hereditary. Hereditary factors contribute to many of the caries risk/resistance factors including pit and fissure morphology, enamel structure and composition, tooth eruption time, salivary flow and composition, arch form, dental spacing, immunologic function, and dietary preference.[2,3]
Dermatoglyphic patterns are broadly classified into three major types: whorl, loops, and arches which have been further
Dermatoglyphics: A Plausible Role in Dental Caries and Malocclusion?
A. Deepti, Kapil Dagrus1, Vandana Shah2, M. Harish2, Deepak Pateel3, Nidhi Shah4
Practitioner and Consultant Oral and Maxillofacial Pathologist, Bangalore, 1Department of Oral Pathology, K. M. Shah Dental College and Hospital, 2Department of Oral Pathology and Microbiology, K. M. Shah Dental College, Sumandeep Vidyapeeth,
Vadodara, Gujarat, India, 3Malaysian Allied Health Sciences University, Kualalampur, Malaysia, 4Department of Oral Pathology, Rajasthan Dental College, Jaipur, Rajasthan, India
ABSTRACTBackground: Palmistry in scientific terms is called as “dermatoglyphics” (“derma” means skin and “glyphic” means carvings). Dermatoglyphics as an independent field of study, even though it has a body of theory, methods, and applications; in many respects, it has been used as an adjunct to other disciplines, serving as a vehicle to resolve broader biomedical problems. Many studies have shown that hereditary factors play contributory role in the development of caries risk and malocclusion. This study was done to check whether dermatoglyphics plays a role in malocclusion and dental caries. Aim: To assess whether dermatoglyphics could help predict genetic susceptibility of children to dental caries and malocclusion. Materials and Methods: A total of 300 children aged 6–12 years were screened for dermatoglyphics, dental caries using decayed, missing, and filled teeth and discrete Fourier transform index and malocclusion using Angle’s classification. Statistical Analysis Used: To show significant difference between the expected frequencies and the observed frequencies in one or more categories, a Chi‑square test was applied. The observed difference was statistically significant and P = 0.03 (<0.05). Results: There was an increased frequency of loop in right hand digit 3 and 5 (middle and little finger) in caries positive participants. Eighty‑one percent of loop pattern was observed in digit 5 (little finger) of right hand in Class II malocclusion. Conclusion: Specific fingerprint patterns may be used as a potential noninvasive anatomical tool for mass screening of dental caries and malocclusion and for guiding future research.
Key words: Dental caries, dermatoglyphics, malocclusion
Original Article
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Kapil Dagrus, Department of Oral Pathology and Microbiology, K. M. Shah Dental College, Sumandeep Vidyapeeth, Vadodara, Gujarat, India. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???.

Deepti, et al.: Dermatoglyphics in dental caries and malocclusion
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 33
divided into various subtypes. These patterns are present on finger tips/buds.[4]
Dental caries is caused by host factors related to either the structure of dental enamel, immunologic response to cariogenic bacteria, or the composition of saliva. Genetic variation in host factors may contribute to increased risks for dental caries.[5]
The relative contribution of genes and the environment to the etiology of malocclusion has been a matter of controversy throughout the 20th century. Genetic mechanisms are clearly predominant during embryonic craniofacial morphogenesis, but environment is also thought to influence dentofacial morphology postnatally, particularly during facial growth.[6,7]
Dermatoglyphics is convenient, cost‑effective, and could help in predicting the phenotype of possible future health conditions.
The objective of this study was to assess whether dermatoglyphics could be used as predictive tool for malocclusion and dental caries.
MATERIALS AND METHODS
An approval was obtained from the Institutional Ethics Committee, Sumandeep Vidyapeeth before commencing the study. Prior permission was obtained from school authorities. The study was conducted among 6–12 year aged school children (n = 300) in Vadodara City, Gujarat State. An consent was obtained from the participants before oral examination and finger print recording.
After explaining the purpose of the study, the demographic details, decayed, missing, and filled teeth (DMFT) index, and Angle’s malocclusion were recorded in a pro forma. The hands of the participants were cleaned and dried, duplicating ink was applied to the distal phalanges of all the fingers and the fingerprint impressions were obtained on a white pro forma sheet with blocks for each finger. Prints were dried and studied using a magnifying lens to identify the finger patterns. The fingertip patterns were analyzed according to the classical method and configurational types.[8,9]
1. Arch patterna. Simpleb. Tented
2. Whorl patterna. Spiralb. Symmetricalc. Double loop
3. Loop patterna. Ulnarb. Radial.
The data obtained were entered in a Microsoft Excel SpreadSheet (MS Office 2007) and then subjected to statistical analysis.
RESULTS
Two independent quantitative variables were measured in this study. The dermatoglyphic pattern and the DMFT score and malocclusion were analyzed [Figure 1].
This study showed an increase in the loop pattern in both the hands. A significant correlation was seen between the ulnar loop pattern and malocclusion, with a higher occurrence of ulnar loop pattern in individuals with malocclusion [Table 1].
There was increased loop pattern seen in the 3rd and 5th digits of both the hands in Angle’s Class I malocclusion group [Figure 2a and b].
In case of Angle’s Class II malocclusion, the loop pattern in the 5th digit of both the hands was predominant [Figure 3a and b].
There was total absence of arch pattern in both the hands among the Angle’s Class III malocclusion group, right hand digits 1, 3, and 4 showed an equal distribution of whorl and loop pattern, whereas the left hand digits 1, 2, and 4 showed an increase in the whorl pattern [Figure 4a and b].
Figure 1: Different dermatoglyphics patterns observed in study
Table 1: Correlation between angles’ malocclusion and dermatoglyphic patternDermatoglyphic pattern Angle’s malocclusion P valueType Subtype Class I Class II Class IIIArch Simple 49 5 0 0.03
Tented 173 14 1Loop Ulnar 1328 163 44 0.03
Radial 49 12 2Whorls Symmetrical 121 19 4 0.03
Spiral 699 76 34Double loop 158 16 4

Deepti, et al.: Dermatoglyphics in dental caries and malocclusion
34 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
This study shows an increased loop pattern among the study group followed by the whorl pattern; however, an increased ulnar loop pattern was seen in both caries positive and caries negative subjects. Similarly, spiral whorl pattern was predominant among both caries positive and caries negative subjects [Table 2].
Loop pattern was increased in the right hand digits 3 and 5 among the caries positive subjects; similarly an increased loop pattern was present in the left hand digits 1, 3, and 5; the 4th digit of both the hands showed an increase in the whorl pattern [Figure 5a and b].
DISCUSSION
Fingers, palm, and sole impressions are expressions of the environmental changes taking place and are inherited in
nature. It has been proved scientifically that no two individuals, even monozygotic twins contain the same finger prints and thus make them a unique characteristic of every individual.
Figure 5: (a) Graphical distribution of fingerprint patterns of right hand digits with caries positive participants. (b) Graphical distribution of fingerprint patterns of right hand digits with caries positive participants
b
a
Figure 4: (a) Graphical distribution of right hand digits in Angle’s Class III malocclusion. (b) Graphical distribution of right hand digits in Angle’s Class III malocclusion
b
a
Figure 3: (a) Graphical distribution of right hand digits in Angle’s Class II malocclusion. (b) Graphical distribution of left hand digits in Angle’s Class II malocclusion
b
a
Figure 2: (a) Graphical distribution of fingerprinting pattern in Angle’s Class I malocclusion on right hand. (b) Graphical distribution of fingerprinting pattern in Angle’s Class I malocclusion on Left hand
b
a
Table 2: Correlation between dental caries and dermatoglyphic patternDermatoglyphic pattern Dental caries status P valueType Subtype Caries absent Caries presentArch Simple 31 28 0.03
Tented 109 103Loop Ulnar 807 728 0.03
Radial 36 27Whorl Symmetrical 82 62 0.03
Spiral 391 418Double loop 107 71

Deepti, et al.: Dermatoglyphics in dental caries and malocclusion
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 35
Once formed, they remain constant and do not alter in the lifetime due to disease process, aging, or any other reason.[1]
The dermal ridges take their origin from the fetal volar pads that appear in the 6–7th week of embryonic life, i.e., at the same time as that of tooth formation in intraembryonic life. This means that the genetic message contained in the genome (normal or abnormal) is deciphered during this period and is also reflected by dermatoglyphics.[1]
In this study, loop and whorl pattern of finger print were equally distributed in all individuals with malocclusion. These results are contrary to those of Tikare et al.[1] who found whorl pattern to be equally distributed in all the three classes of malocclusion.
Eighty‑one percent loop pattern was observed in digit 5 (little finger) of the right hand in Class II malocclusion, as consistent with the study results of Reddy et al.[10]
The participants in this study of Class II malocclusion showed decrease in number of arch pattern in all digits of right and left hand. These results are contrary to those of Trehan et al.,[11] who found an increase in whorl pattern in Class I and III and an increase in loop and arch pattern in Class II.
In this study, we found no significant difference in the frequency distribution of loop pattern in all digits when compared with caries free and caries positive participants. However, we found increase frequency of loop in right hand digit 3 and 5 (middle and little finger) in caries positive participants in this study, whereas caries‑free participants showed an increase in frequency of loop in all digits of left hand as compared to whorls. These results are in contrast to those of Abhilash et al.[12] who found an increase in whorl pattern in caries positive and decrease in loop pattern in caries‑free group.
Dermatoglyphic patterns may be utilized effectively to study genetic basis of dental caries and malocclusion. The results of this study provide some insight into specific fingerprint patterns for dental caries and malocclusion. These could be used as potential noninvasive anatomical tools for screening of dental caries and guiding future research, with respect to early diagnosis, instituting preventive strategies, and more
effective treatment modalities in individuals with dental caries and malocclusion. More studies with large sample size may validate the use of dermatoglyphics in oral and dental pathologies.
CONCLUSION
Dermatoglyphics can be used as a non invasive mass screening tool to examine population at risk for dental caries and malocclusion.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Tikare S, Rajesh G, Prasad KW, Thippeswamy V, Javali SB.
Dermatoglyphics – A marker for malocclusion? Int Dent J 2010;60:300‑4.2. Shuler CF. Inherited risks for susceptibility to dental caries. J Dent Educ
2001;65:1038‑45.3. Wright JT, Hart TC. The genome projects: Implications for dental
practice and education. J Dent Educ 2002;66:659‑71.4. Ahmed RH, Aref MI, Hassan RM, Mohammed NR. Dermatoglyphic
study on patients with dental caries restored with dental fillings and its correlation to apoptosis induced by dental fillings. Nat Sci 2010;8:54‑7.
5. Foxman B, Srinivasan U, Wen A, Zhang L, Marrs CF, Goldberg D, et al. Exploring the effect of dentition, dental decay and familiality on oral health using metabolomics. Infect Genet Evol 2014;22:201‑7.
6. Mossey PA. The heritability of malocclusion: Part 1 – Genetics, principles and terminology. Br J Orthod 1999;26:103‑13.
7. Mossey PA. The heritability of malocclusion: part 2. The influence of genetics in malocclusion. Br J Orthod 1999;26:195‑203.
8. Prathibha R, Abhilash PR, Sherlin HJ, Anuja N, Premkumar P, Chandrasekar T, et al. Conventional dermatoglyphics – Revived concept: A review. Int J Pharma Biosci 2011;2:B446‑58.
9. Schaumann B, Alter M. Dermatoglyphics in Medical Disorders. New York: Springer‑Verlag; 1976. p. 27‑87.
10. Reddy S, Prabhakar AR, Reddy VV. A dermatoglyphic predictive and comparative study of class I, class II, div 1, div. 2 and class III malocclusions. J Indian Soc Pedod Prev Dent 1997;15:13‑9.
11. Trehan M, Kapoor DN, Tandon P, Sharma VP. Dermatoglyphic study of normal occlusion and malocclusion. J Indian Orthod Soc 2000;33:11‑6.
12. Abhilash PR, Divyashree R, Patil SG, Gupta M, Chandrasekar T, Karthikeyan R. Dermatoglyphics in patients with dental caries: A study on 1250 individuals. J Contemp Dent Pract 2012;13:266‑74.

36 © 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow
INTRODUCTION
In the field of oral and maxillofacial surgery, hybrid ameloblastoma is a seldom occurrence,[1‑4] portraying histologically a marked stromal desmoplasia. In treating this type of tumor, it is important to evaluate the clinical types in the lesion, localization, and size of the tumor.
To enhance knowledge of this pathologic entity, we contribute another case of hybrid ameloblastoma.
CASE REPORT
A 38‑year‑old male patient reported to the department with a chief complaint of pain and swelling in lower right posterior region of the jaw since 6 months. The patient presented a history of enucleation and curettage along with extraction of the third molar for the similar complaint 23 years back. The patient was disease free till this lesion recurred 8 years after initial surgery, requiring second intervention. A local
dentist aspirated the cystic cavity along with extraction of the first and second mandibular molars. The size of the swelling subsequently decreased. Presently, the patient endured this lesion once again since last 6 months.
The patient was otherwise in good health, and his medical and family history was noncontributory.
Extraoral examination presented with a swelling in relation to the angle of the mandible on the right side extending anteroposteriorly from body to the angle of the mandible and superoinferiorly from the line corresponding to the tragus of the ear till the angle of the mandible. The overlying skin was smooth and normal in color [Figure 1]. On palpation, swelling
Unicystic Ameloblastoma Developing into a Hybrid Lesion of Rare Entity ‑ with Review of
LiteratureSavina Gupta, Mukul Nandkumar Padhye, Gokul Venkateshwar, Sandhya Tamgadge, Hirkani Attarde
Department of Oral and Maxillofacial Surgery, D.Y. Patil University, School of Dentistry, Nerul, Navi Mumbai, Mumbai, Maharashtra, India
ABSTRACTExistence of unicystic ameloblastoma with desmoplasia is a seldom occurrence. It was first described by Waldron and El‑Mofty in the year 1987 as the term hybrid ameloblastoma. Here, we account a case of hybrid lesion depicting outstanding unicystic, follicular ameloblastoma with desmoplasia and mucus cell differentiation showing inductive changes. The patient is a 38-year-old male with a swelling in the lower right posterior region of the jaw. Radiologically, a mixed radiopaque-radiolucent lesion was sighted in this region. Taking into account of patient’s complaint, clinical, radiographic, and histologic features; diagnosis of ameloblastic fibrodentinoma was made. It was followed by complete excision of the tumor. The challenge in the management of this tumor was to render complete excision as recurrence may occur in incomplete removal and also to reconstruct the bony defect to give a moderate cosmetic and functional result to the patient. The excisional biopsy report was established to be of hybrid ameloblastoma. Since there are few cases reported in the past of this lesion, the present case is an addition for better perception of this odontogenic tumor. This article identifies some profound concepts and new developments in the histopathologic design of ameloblastoma and its hybrid variant. It also briefly reviews the literature referring to this rare tumor entity. Considering the characteristics of ameloblastoma, priority of surgical management for hybrid lesion is also described.
Key words: Desmoplastic, hybrid, unicystic ameloblastoma
Case Report
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Savina Gupta, Department of Oral and Maxillofacial Surgery, D.Y. Patil University, School of Dentistry, Nerul, Navi Mumbai ‑ 400 706, Mumbai, Maharashtra, India. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???.

Gupta, et al.: Hybrid odontogenic tumour
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 37
was tender, firm, nonfluctuant, and noncompressible. There was no significant lymphadenopathy detected.
On intraoral examination, the overlying mucosa of the lesion was pink in color. Dimensions of the lesion were 4 cm × 3 cm, with well‑defined margins, extending anteroposterior from the mandibular second premolar to the anterior border of the ramus of the mandible and superoinferiorly from the edentulous ridge of 46, 47, and 48 obliterating vestibule of the mandible [Figure 2]. On palpation, both buccal and lingual cortices were involved. The swelling was firm, tender, and noncompressible. All neighboring teeth were vital with no evidence of other dental abnormalities.
Orthopantomogram revealed multilocular radiolucency with soap bubble appearance extending from coronoid process till the body of the mandible. The locules had mixed radiolucent and radiopaque appearance [Figure 3].
Computed tomography illustrated an osteolytic, space occupying lesion at the posterior part of the right mandible. The axial section demonstrated buccal and lingual cortical thinning in the area of 46, 47, and 48 regions [Figure 4]. The sagittal section exhibited a multilocular hypodense region ranging from coronoid process till the base of the mandible. Base of the mandible had thinned out [Figure 5]. Three‑dimensional computed tomography presented involvement of coronoid process till the distal aspect of the second premolar with a small breach in the buccal cortex involving the inferior alveolar nerve in the lesion [Figure 6].
An incisional biopsy was conducted on the ascending ramus region under local anesthesia. The histopathological diagnosis obtained was ameloblastic fibrodentinoma.
The management was done by segmental resection on the right side of the jaw, from posterior aspect of the second premolar, salvaging the condyle, and coronoid process via extraoral approach [Figure 7]. Immediate reconstruction was done with 2.4 mm locking reconstruction plates.
Excised specimen was sent for histopathological diagnosis. It was reported to be a hybrid lesion of unicystic, follicular, desmoplastic with mucus cell differentiation and numerous foci of inductive changes.
Deviation of the mandible toward the left side was observed after 2 weeks postoperatively [Figure 8]. Patient was evaluated in regular monthly intervals. Patient is apparently disease free, with no marked complaints regarding the surgery since 2 years.
DISCUSSION
Odontogenic tumors develop from odontogenic epithelium, which has the capability for various differentiations and mesenchymal induction. Histologically, ameloblastoma occurs in different patterns, as plexiform, follicular, basal
Figure 1: Extraoral preoperative view of the patient
Figure 2: Intraoral preoperative view of the patient
Figure 3: Preoperative orthopantomogram Figure 4: Preoperative computed tomography axial section

Gupta, et al.: Hybrid odontogenic tumour
38 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
cell, granular, desmoplastic, and acanthomatous. Hybrid lesion is a variant of ameloblastoma in which follicular and plexiform exist together with areas of pronounced stromal desmoplasia.[5,6]
Hybrid ameloblastoma was first identified by Waldron and El‑Mofty in 1987.[6] It is a benign, locally invading, intraosseous, infiltrative ameloblastoma.[7] From the review of the literature, hybrid ameloblastoma is rarely found.[8,9] So far, only 30 cases of hybrid ameloblastoma have been reported.[10] They are reported to be 4–13% of all ameloblastomas.[6] Clinical findings of 26 cases of hybrid ameloblastoma have been summarized in Table 1.
Regarding on age, sex distribution, and site of occurrence of this lesion; it usually appears at the age of 42.9 years, higher for males (45.9 years) than for females (39.7 years), male/female ratio is 1:1.[6,9] The usual site of lesion is anterior portion of the jaws,[7] and the ratio of maxilla/mandible is 1:0.9.[6] In our case, the lesion was observed in the posterior aspect of the mandible.
Radiologically, conventional ameloblastoma is classified as unilocular or multilocular radiolucency with well‑defined
borders. The radiographic characteristics of the case in this article demonstrated a combination of two distinctive visual aspects as in mixed radiolucent‑radiopaque multilocular areas. This indicates the presence of hybrid lesion of ameloblastoma. Recurrence after initial surgical treatment is an outcome of the infiltrative growth of ameloblastoma through the adjacent bone. This new bone formation leads to mixed radiolucency and radiopacity.[11] Moreover, most ameloblastomas show multilocularity, whereas unicystic ameloblastomas depict large unilocular radiolucency. Seldom, we encounter a multilocular lesion in unicystic ameloblastoma; which was observed in the present case.[12]
The unicystic ameloblastoma commonly appears as a cystic lesion with either an intraluminal or an intramural proliferation of the cystic lining.[13] Histopathological examination of the surgical specimen showed a unicystic ameloblastoma of intraluminal and mural type. Intraluminal proliferation was of plexiform pattern, and mural proliferation showed unusual histopathological findings, which revealed follicular, acanthomatous areas coexisting with desmoplastic areas. This mural picture was similar to the so‑called “hybrid lesion of ameloblastoma.” The lesion also revealed a distinctive picture of extensive collagenized stroma containing small islands of tumor epithelium with scanty inclination to form cystic structures. The ameloblastoma also displayed evidence of focal mucus cell differentiation [Figure 9]. The occurrence of mucous cells in ameloblastoma is an exceptionally rare phenomenon
Figure 5: Preoperative computed tomography sagittal section Figure 6: Three‑dimensional computed tomography
Figure 7: Segmental resection of the mandible, intraoperative view
Figure 8: Postoperative view of the patient

Gupta, et al.: Hybrid odontogenic tumour
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 39
and up to now 6 cases of ameloblastoma showing mucous cells are reported.[14] In this article, we make an addition of one more of such a case. This is a unique case report of desmoplastic ameloblastoma with mucous cell differentiation in posterior mandible as all the earlier published cases showed occurrence in anterior jaws.[14,15] The probable pathogenesis for mucous cell differentiation expresses the pluripotential character of the odontogenic epithelium.
With respect to histologic features, these hybrid lesions are also known to have a combination of desmoplastic and conventional ameloblastoma.[9] The odontogenic epithelium occurs as irregular, stellate, or follicular islands and cords; central part frequently appears hypercellular with spindle‑shaped or squamatoid cells. Peripheral columnar or cuboidal cells seldom disclose ameloblastic appearance. Therefore, vaguely mimicking a follicular ameloblastoma with acanthomatous characteristics. Furthermore, spectacularly there is extensive stromal desmoplasia with copious thick collagen fibers compressing epithelial islands.[6] According to Sun et al.,[9] scattered epithelial nests and extensive desmoplasia were salient features of desmoplastic ameloblastoma. The neoplastic epithelial islands seen in
Figure 9: (a) Photomicrograph of an incisional biopsy shows odontogenic epithelium consisting of tall columnar ameloblast‑like cells and stellate reticulum‑like cells suggestive of unicystic ameloblastoma. (b) Photomicrograph of an excisional biopsy shows odontogenic island in the connective tissue capsule. (c) Photomicrograph of an excisional biopsy shows odontogenic island in the connective tissue capsule showing cystic degeneration. (d) Photomicrograph of an excisional biopsy shows desmoplasia with compressed odontogenic island in the connective tissue capsule along with calcifications
dc
ba
Table 1. Clinico pathologic features of 26 compiled cases of Hybrid AmeloblastomaAuthor and year Number
of casesAge/sex Location Radiologic features
Waldron and El mofty, 1987 5 25-82 years/2 males 4- mandible, posterior NAHiguchi et al., 1991 2 58 years/male
70 years/maleMandible, anterior to posteriorMandible, posterior
Soap bubble and MulticysticMulticystic
Philipsen et al., 1992 1 55 years/male Mandible, anterior canine to molar region
Multilocular RL with follicular RO. Root resorption
Ashman et al., 1993 1 53 years/male Mandible, anterior Well circumscribed mixed RL and ROTakata et al., 1999 1 48 years/male Mandible, lateral incisor to 1st
molarHoney comb appearance in anterior regionUnicystic RL in molar region
Wakoh et al., 2002 1 35 years/female Mandible, canine- premolar region Mixed RL and RO with adjacent cystic radiolucent area
Hirota et al., 2005 1 17 years/female Maxilla, canine and premolar regions
Mixed RL and RO with well defined borders
Santos et al., 2006 1 36 years/male Mandible, anterior- premolar region Ill defined RLDesai et al., 2006 1 32 years/male Mandible, posterior Well defined unilocular RLSivapathasundaram et al., 2009
2 31years/female40 years/male
Mandible, anterior- premolarMaxilla, anterior- molar region
Mixed RL and RO with poorly defined bordersMixed RL and ROwith ill defined borders
Yazdi et al., 2009 1 48 years/female Mandible, anterior Mixed RL and RO with ill defined bordersGade et al., 2010 1 35 years/female Maxilla, anterior Mixed RL with radiopaque specksGupta et al., 2011 1 35 years/female Mandible, anterior Ill defined hazy RL with flecks of RO Vardhan et al., 2011 1 29 years/female Mandible, anterior right body Well defined irregular RLLawal et al., 2011 2 50 years/female
29 years/maleMandible, anteriorMandible, anterior
Multilocular RLMultilocular RL
Acharya et al., 2011 1 50 years/male NA NAAngadi et al., 2011 1 64 years/female Maxilla, anterior-molar Ill defined hazy RL and RO, root
resorptionO A Effiom et al., 2013 1 50 years/female Mandible anterior-molar Mixed RL and ROPresent case 1 38 years/male Mandibular posterior Mixed RL and RO
NA: Not Available; years, RL: Radiolucency, RO: Radiopacity

Gupta, et al.: Hybrid odontogenic tumour
40 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
desmoplastic ameloblastoma are small and ameloblastic cells are rare.[16] A hybrid odontogenic tumor incorporating two distinct lesions is highly uncommon,[17] and the present case is depicting this seldom occurrence.
In our case, the incisional biopsy report derived was of ameloblastic fibrodentinoma. As preoperative biopsy does not illustrate the entire lesion, it may result in incorrect categorization of the lesion. Thus, the true nature of the lesion is manifested only after the entire specimen is available for microscopy. The treatment plan was formulated according to clinical examination and biopsy reports.
Ameloblastoma is a polymorphic neoplasm for which the surgical intervention is established by a number of clinical and histological factors. The method of surgery consists of radical surgery (segmental resection) and conservative method (enucleation with bone curettage). Aggressive lesions demand more radical surgical approach ensuing large jaw defects. Recurrence rates of ameloblastoma are reportedly as high as 15–25% after radical treatment and 75–90% after conservative treatment.[13] Of late, the progress in comprehending the biologic conduct of ameloblastoma reveals that unicystic lesions are well localized by the fibrous capsule of the cyst, with few tumors broaching peripheral tissues, whereas multicystic and solid lesions are known to have aggressive infiltration to adjacent tissue.[13] Gardner recommended that solid and multicystic ameloblastoma should be treated radically, whereas unicystic ameloblastoma can be cured by curettage.[18] The intraluminal subtype of unicystic ameloblastoma may respond well with enucleation, but the intramural subtype may not; and since this more aggressive treatment is recommended.[19]
Philipsen et al. advocated treating these kinds of cases such as other variants of infiltrative ameloblastoma till they the diagnosis is histopathologically confirmed.[7] Sun et al.[9] reviewed desmoplastic ameloblastoma and concluded that resection reduces recurrence rate as compared to enucleation of the lesion and the average period of recurrence was 36.9 months.
To a large extent, recurrence is the result of performing an inadequate initial procedure. Therefore, radical and aggressive surgery is a more favored option for recurrent ameloblastoma management.[20] In the present scenario, the patient already had recurrence twice previously; therefore, the preferred choice of surgery was radical resection. Moreover, the prognosis of recurrence appears to be associated with the surgical planning before evaluation of the histologic subtype.
Therefore, complete excision is advocated for conventional and desmoplastic variants of ameloblastoma. The unicystic type requires additional subtyping to determine the best treatment approach.
Ameloblastoma carries a certain risk of developing local recurrences depending on histology and the type of surgical treatment.[21] Long‑term follow‑up is advised in such cases.
CONCLUSION
Hybrid ameloblastoma is a variation of ameloblastoma presenting distinguishable clinical, radiological, and histological features as compared with conventional ameloblastoma.
A unicystic ameloblastoma developing into a hybrid lesion is a benign, locally invasive odontogenic tumor with a probable recurrence rate with an unsuitable initial therapeutic approach. When the tumor recurrence is detected, the ideal treatment method is bone resection. This can be performed by either marginal or segmental resection depending on location and extent of recurrence.
Most cases of this rare variant of ameloblastoma need to be retrospectively analyzed to categorically explain their behavior, aggressiveness, and prognosis. The diagnosed and treated cases should be kept under regular follow‑up to rule out any evidence of recurrence and malignant transformation.
This reported case reinforces that patients presenting with hybrid odontogenic lesions of this grade should undergo close follow‑up for few decades after surgical treatment.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Yoon JH, Kim HJ, Yook JI, Cha IH, Ellis GL, Kim J. Hybrid odontogenic
tumor of calcifying odontogenic cyst and ameloblastic fibroma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98:80‑4.
2. Ide F, Obara K, Mishima K, Saito I. Ameloblastoma ex calcifying odontogenic cyst (dentinogenic ghost cell tumor). J Oral Pathol Med 2005;34:511‑2.
3. Cheng Y, Long X, Li X, Bian Z, Chen X, Yang X. Clinical and radiological features of odontogenic ghost cell carcinoma: Review of the literature and report of four new cases. Dentomaxillofac Radiol 2004;33:152‑7.
4. Zhang W, Chen YU, Geng N, Bao D, Yang M. A case report of a hybrid odontogenic tumour: Ameloblastoma and adenomatoid odontogenic tumour in calcifying odontogenic tumour. Oral Oncol Extra 2006;42:287‑90.
5. dos Santos JN, De Souza VF, Azevêdo RA, Sarmento VA, Souza LB. “Hybrid” lesion of desmoplastic and conventional ameloblastoma: Immunohistochemical aspects. Braz J Otorhinolaryngol 2006;72:709‑13.
6. Waldron CA, el‑Mofty SK. A histopathologic study of 116 ameloblastomas with special reference to the desmoplastic variant. Oral Surg Oral Med Oral Pathol 1987;63:441‑51.
7. P h i l i p s e n H P, Re i c h a r t PA , Ta ka t a T. D e s m o p l a s t i c ameloblastoma (including “hybrid” lesion of ameloblastoma). Biological profile based on 100 cases from the literature and own files. Oral Oncol 2001;37:455‑60.

Gupta, et al.: Hybrid odontogenic tumour
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 41
8. Lawal AO, Adisa AO, Olusanya AA, Adeyemi BF. “Hybrid” ameloblastoma: A report of two cases. Afr J Med Med Sci 2011;40:413‑5.
9. Sun ZJ, Wu YR, Cheng N, Zwahlen RA, Zhao YF. Desmoplastic ameloblastoma – A review. Oral Oncol 2009;45:752‑9.
10. Effiom OA, James O, Akeju OT, Salami AS, Odukoya O. Hybrid ameloblastoma in a Nigerian: Report of a case and a review of literature. Open J Stomatol 2013;3:347‑53.
11. Chaubey SS, Mishra SS, Degwekar SS, Chaubey S. A rare presentation of hybrid odontogenic tumor involving calcifying cystic odontogenic tumor and plexiform ameloblastoma. Contemp Clin Dent 2013;4:406‑8.
12. Nagalaxmi V, Sangmesh M, Maloth KN, Kodangal S, Chappidi V, Goyal S. Unicystic mural ameloblastoma: An unusual case report. Case Rep Dent 2013;2013:957418.
13. Dandriyal R, Gupta A, Pant S, Baweja HH. Surgical management of ameloblastoma: Conservative or radical approach. Natl J Maxillofac Surg 2011;2:22‑7.
14. Punnya AV, Rekha K. Ameloblastoma with mucous cells: Review of literature and presentation of 2 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:e20‑6.
15. Tamgadge S, Tamgadge A, Bhalerao S, Pierera T. Mucous cell differentiation in desmoplastic ameloblastoma: Unique presentation in posterior mandible. Int J Oral Maxillofac Pathol 2012;2 :61‑4.
16. Hirota M, Aoki S, Kawabe R, Fujita K. Desmoplastic ameloblastoma featuring basal cell ameloblastoma: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:160‑4.
17. Philipsen HP, Reichart PA. Unicystic ameloblastoma. A review of 193 cases from the literature. Oral Oncol 1998;34:317‑25.
18. Gardner DG. A pathologist’s approach to the treatment of ameloblastoma. J Oral Maxillofac Surg 1984;42:161‑6.
19. Pogrel MA, Montes DM. Is there a role for enucleation in the management of ameloblastoma? Int J Oral Maxillofac Surg 2009;38:807‑12.
20. Becelli R, Morello R, Renzi G, Matarazzo G, Dominici C. Treatment of recurrent mandibular ameloblastoma with segmental resection and revascularized fibula free flap. J Craniofac Surg 2011;22:1163‑5.
21. Eckardt AM, Kokemüller H, Flemming P, Schultze A. Recurrent ameloblastoma following osseous reconstruction – A review of twenty years. J Craniomaxillofac Surg 2009;37:36‑41.

42 © 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow
INTRODUCTION
Lymphomas are a heterogeneous group of malignancies arising from lymphoreticular system. They range clinically from indolent to highly aggressive and fatal neoplasm and are of two types: Hodgkin’s lymphoma (HL) (10%) and non‑HL (NHL) (90%).[1‑3] NHL of B‑cell origin is more common and occurs commonly in the extranodal sites.
Diffuse large B‑cell lymphoma (DLCBL) is a subtype of NHL constituting about 30% and rarely occurs in the mandible 8% whereas isolated types constitute 0.6% only making mandible a rare site of presentation for DLCBL. Parker and Jackson in 1939 first proposed the term “primary reticular cell sarcoma of bone” for extranodal lymphomas arising at a primary site in bone. However, the term “primary lymphoma of bone” was introduced by Ivins and Dahlin in 1963.[4] Coley in 1950 suggested the criteria for diagnosis of primary lymphoma of bone, later modified by WHO as:• Lymphomapresentinginasingleosseoussite• Histologicalconfirmation• Noevidenceofdiseaseelsewhereforatleast6months
after diagnosis.[1]
CASE REPORT
A 50‑year‑old male presented with a painful swelling in the left lower 3rd of the face [Figure 1]. History revealed extraction of mobile 34, 35, and 36, 2 months earlier with nonhealing tooth sockets and fever, anorexia, swelling, and paresthesia of the left lower lip. The lesion did not respond to three cycles of broad spectrum antibiotics and anti‑inflammatory medication. Intraoral examination revealed a bony hard swelling in relation to the nonhealing sockets. Orthopantomogram revealed diffuse, ill‑defined osteolytic areas with enlargement of mandibular canal and mental foramen [Figure 2]. Whole‑body scan did not reveal any deposits elsewhere in the body. Excisional biopsy was done under general anesthesia and histopathology showed diffuse infiltrates of medium to large size atypical lymphoid cells with scant to moderate cytoplasm, hyperchromatic to vesicular nuclei, few with prominent nucleoli [Figure 3]. Nuclei were hyperchromatic, moderately pleomorphic and mitotically active with irregular nuclear
Centroblastic Variant of Non‑Hodgkin’s Lymphoma of Mandible: A Rare Case Report
Anuradha E. Sunil, P. C. Anila Namboodiripad, Archana Mukunda, Neethu Kadar, K. A. Jassim
Department of Oral and Maxillofacial Pathology, Royal Dental College, Palakkad, Kerala, India
ABSTRACTNon-Hodgkin’s lymphoma (NHL) is the most common lymphoma that presents in extranodal areas without lymphoid tissue. It occurs in <5% of cases in the jaws and the maxilla are more commonly involved than mandible. The most common symptom is that of a nonpathognomic swelling mimicking odontogenic pathology with a mobile tooth. The lesion usually gets aggravated after extraction and presents as a painful nonhealing socket with symptoms of paresthesia. Diffuse large B-cell lymphoma is the most common subtype and has a better prognosis and overall survival in patients. The treatment of NHL is by a combination of chemotherapy and radiotherapy. We present a rare case report of occurrence of NHL in the least preferred site of mandible with nonhealing socket following extraction of mobile tooth, diagnosed on histopathology and confirmed by immunohistochemistry.
Key words: Centroblastic diffuse large B-cell lymphoma, diffuse large B-cell lymphoma, intraosseous lymphoma, non-Hodgkin’s lymphoma
Case Report
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Anuradha E. Sunil, Department of Oral and Maxillofacial Pathology, Royal Dental College, Iron Hills, Chalissery, Palakkad, Kerala, India. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???

Sunil, et al.: Non-Hodgkin’s lymphoma of mandible
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 43
membrane. Prominent nucleoli with foci of necrosis were present. Based on the above findings, a diagnosis of large cell NHL was established. Immunohistochemistry (IHC) staining revealed that the atypical lymphoid cells were positive for CD20, MIB1, BCl‑2, and BCl‑6 [Figures 4 and 5] and negative for Epstein–Barr virus‑Latent membrane protein, CD10, CD138, and CD3. Based on the above findings, a diagnosis of DLBCL‑centroblastic variant was established. The patient was referred to an oncologist for chemotherapy and radiotherapy and is currently responding well to the treatment.
DISCUSSION
NHLs are heterogeneous malignancies of lymphoid system that vary in clinical behavior, morphologic appearance, immunologic, and molecular phenotype. They originate in lymph nodes, extranodal sites, and even in sites without lymphoid tissue.[2,3] NHL’s etiology is unknown; however, patients with immunosuppression as in HIV have an increased risk to develop NHL.[2]
The peak incidence of occurrences is 40–80 years and rare in children and young adults.[1,4] Males are more commonly
affected than females in the ratio of 3:2.[5] Extranodal lesions arise in nearly any site or organ, but gastrointestinal tract is the most common (25–30%), followed by head and neck area (11–13%).[6] Here, Waldeyer’s ring is commonly involved and 2.5% of cases occur in the oral and paraoral areas.[2] Oral lesions of soft tissues appear as a painless local mass with superficial ulceration without any unique findings.[7]
NHL rarely occurs in the jaw bones (<5%) and is more frequent in the maxilla than the mandible with palate and gingiva involved in 70% of cases.[7,8] Posterior region is preferred over anterior as reported by Rinaggio et al.[4,8] Paresthesia of inferior alveolar nerve is a common finding in 20%.[1] The radiographic findings of NHL’s are not pathognomonic showing features of nonspecific osteolysis. However, few cases have also shown diffuse enlargement of the mandibular canal.[9] The clinical and radiological features of NHL are nonspecific, and hence, the diagnosis in jaw bone is often delayed. The diagnosis is usually established with the help of histopathology and IHC.[1]
Commonly used histological classification for NHLs is the 1982 International Working Formulation, which divides NHL into three prognostic groups such as low, intermediate, and high grade. Revised European‑American Lymphoma (REAL) in 1994 classifies lymphomas according to clinical and
Figure 1: Extraoral photograph showing a diffuse swelling in the left body of the mandible
Figure 2: Orthopantomogram shows a diffuse osteolytic lesion with enlargement of mandibular canal
Figure 3: Showing diffuse infiltrates of medium to large size lymphoid cells with hyperchromatic to vesicular nuclei, scant cytoplasm and prominent nucleoli, (H and E, ×400)
Figure 4: Immunohistochemistry with CD20 displaying diffuse cytoplasmic and membrane positivity for these lymphoid cells. Nuclei are negative

Sunil, et al.: Non-Hodgkin’s lymphoma of mandible
44 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
pathological behavior as low grade/indolent, intermediate grade/aggressive, or high grade/very aggressive; WHO IV edition classification gives the subtypes of DLBCL [Table 1].[4,10]
DLBCL is the most common type of NHL (40%) in adults.[4] Although REAL and WHO classifications are based on genetics and immunophenotype, the diagnosis of DLBCL is still mainly based on morphology showing large B‑cell with nuclear size equal to or exceeding macrophage nuclei with a diffuse growth pattern.[11]
It is an aggressive tumor which can arise in almost any part of the body. The first sign typically is observation of a rapidly growing mass infiltrating tissues or obstructing organs. It may be associated with fever, weight loss, night sweats, etc. It may arise as a primary tumor de novo or as a result of progression and transformation of a less aggressive lymphoma of a lower grade such as lymphocytic, follicular, or marginal lymphoma.[4,10] The chromosomal abnormality is mapped to 3q27 in DLBCL.[12]
The common variants of DLBCL defined by Keil and WHO IV edition classification are as follows:[1,4,13]
a. Centroblastic variant is the most common subtype and is comprised predominant population of medium to large lymphoid cells with scant to moderate amphophilic cytoplasm, round to oval 2–4 membrane‑bound nuclei and vesicular chromatin. Immunoblasts present are always <90% of the cells in the tumor. A variant seen in centroblastic form is centroblast with multilobulated nuclei. These are commonly seen histopathological features in primary lymphoma of the bone and in other extranodal sites
b. Immunoblastic variant has >90% of immunoblastic large cells with more abundant cytoplasm, large nuclei, vesicular chromatin, and single large centrally placed nucleoli. These cells can sometimes demonstrate plasmacytoid differentiation
c. Anaplastic variant shows large to very large cells with pleomorphic nuclei that may, in part, resemble tumor cells of the anaplastic large cell lymphoma or even Reed‑Sternberg cells.[11,13]
Centroblastic lymphoma is the most common subtype with better prognosis (and overall survival) when compared with immunoblastic and anaplastic variants.[4,10]
The treatment of NHL depends on histological classification and clinical staging of the tumor. It is usually a combination of surgery and chemotherapy‑radiotherapy. Localized (stage I and stage II) low‑grade extranodal lymphomas in the head and neck are treated primarily with radiation therapy whereas localized intermediate grade lymphomas are treated with radiation and chemotherapy. High‑grade and advanced stage NHLs are treated with aggressive chemotherapy regimen.[4] It is noted that prognosis is excellent with survival rate of 95%.[1,14]
The prognosis and clinical outcome of NHL depend on its histological subtype, stage, presence of symptoms, primary site, size, age of patient, type of treatment, and association with immunosuppression.[2,15] Periodic recall is must to rule out recurrences and dissemination.
CONCLUSION
Diagnosis of NHL in the jaw bones is challenging as there is low index of clinical suspicion, and malignant tumor may
Figure 5: Immunohistochemistry with MIB1 displaying high proliferation index ~80%, (staining nuclei)
Table 1: Diffuse large B‑cell lymphoma subtypes according to the IV edition of the WHO classification of tumors of the hemopoietic and lymphoid tissuesDiffuse large B‑cell lymphoma, NOSCommon morphologic variants
CentroblasticImmunoblasticAnaplastic
Rare morphologic variantsMolecular subgroups
GCB-likeABC-like
Immunohistochemical subgroupsCD5-positive DLBCLGCB-likeNon-GCB-like
Diffuse large B-cell lymphoma subtypes/entitiesPrimary mediastinal (thymic) large B-cell lymphomaT-cell/histiocyte-rich large B-cell lymphomaIntravascular large B-cell lymphomaPrimary DLBCL of the CNSPrimary cutaneous DLBCL, leg typeDLBCL associated with chronic inflammationALK-positive DLBCLLarge B-cell arising in HHV8-associated multicentric Castleman diseasePlasmablastic lymphoma and primary effusion
Borderline casesB‑cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin’s lymphoma
GCB: Germinal‑center B‑cell, ABC: Activated B‑cell, NOS: Not otherwise specified, ALK: Anaplastic lymphoma kinase, DLBCL: Diffuse large B-cell lymphoma

Sunil, et al.: Non-Hodgkin’s lymphoma of mandible
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 45
mimic common oral and dental pathological conditions. Hence, NHLs should be included in differential diagnosis in all cases of nonhealing sockets and periodontal diseases without favoring etiology. Early and prompt diagnosis favors treatment, prognosis, and survival and eliminates dissemination and advanced treatment options.
Declaration of patient consentThe authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Dinakar J, Priya L, Reddy S. Primary non‑Hodgkin’s lymphoma of the
mandible. J Oral Maxillofac Pathol 2010;14:73‑6.2. Walter C, Ziebart T, Sagheb K, Rahimi‑Nedjat RK, Manz A, Hess G.
Malignant lymphomas in the head and neck region – A retrospective, single‑center study over 41 years. Int J Med Sci 2015;12:141‑5.
3. Shaik MA, Waghray S, Kaleem SM, Morrthy S, Shaheen N. Primary extranodal B‑cell lymphoma. Int J Exp Dent Sci 2012;1:30‑3.
4. Nayak PB, Desai D, Pandit S, Rai N. Centroblastic variant of diffuse large
B‑cell lymphoma: Case report and review of literature. J Oral Maxillofac Pathol 2013;17:261‑5.
5. Kini R, Saha A, Naik V. Diffuse large B‑cell lymphoma of mandible: A case report. Med Oral Patol Oral Cir Bucal 2009;14:e421‑4.
6. Hanna E, Wanamaker J, Adelstein D, Tubbs R, Lavertu P. Extranodal lymphomas of the head and neck. A 20‑year experience. Arch Otolaryngol Head Neck Surg 1997;123:1318‑23.
7. Agrawal MG, Agrawal SM, Kambalimath DH. Non‑Hodgkins lymphoma of maxilla: A rare entity. Natl J Maxillofac Surg 2011;2:210‑3.
8. Rinaggio J, Aguirre A, Zeid M, Hatton MN. Swelling of the nasolabial area. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:669‑73.
9. Buric N, Jovanovic G, Radovanovic Z, Buric M, Tijanic M. Radiographic enlargement of mandibular canal as first feature of non‑Hodgkin’s lymphoma. Dentomaxillofac Radiol 2010;39:383‑8.
10. Piccaluga PP, Bacci F, Sabatlini E, Rossi M, Gazzola A, Sapienza MR, et al. Large cell non‑Hodgkins lymphoma: What is new in the WHO classification? Hematol Meet Rep 2009;3:43‑5.
11. Gurbuxani S , Anastas i J , Hyjek E. Di f fuse large B ‑cel l lymphoma – More than a diffuse collection of large B cells: An entity in search of a meaningful classification. Arch Pathol Lab Med 2009;133:1121‑34.
12. Chen CY, Yao M, Tang JL, Tsay W, Wang CC, Chou WC, et al. Chromosomal abnormalities of 200 Chinese patients with non‑Hodgkin’s lymphoma in Taiwan: With special reference to T‑cell lymphoma. Ann Oncol 2004;15:1091‑6.
13. Engelhard M, Brittinger G, Huhn D, Gerhartz HH, Meusers P, Siegert W, et al. Subclassification of diffuse large B‑cell lymphomas according to the Kiel classification: Distinction of centroblastic and immunoblastic lymphomas is a significant prognostic risk factor. Blood 1997;89:2291‑7.
14. Beal K, Allen L, Yahalom J. Primary bone lymphoma: Treatment results and prognostic factors with long‑term follow‑up of 82 patients. Cancer 2006;106:2652‑6.
15. Panduric DG, Kuna T, Katanec D. Pain after tooth extraction masking primary extranodal non‑Hodgkin’s lymphoma of the oral cavity. Acta Stomatol Croat 2007;41:366‑74.

46 © 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow
INTRODUCTION
Dental trauma is a common injury, especially in children. In permanent dentition, a high incidence of traumatic injuries is seen for boys aged 8–10 years, probably related to more vigorous play characteristic of this age group.[1,2] The majority of dental injuries in permanent dentition involve the anterior region of maxilla, of which luxation injuries comprise 15–61% of the dental traumas that include lateral, intrusive, and extrusive luxation injuries.[1] The most commonly involved tooth is the maxillary central incisor followed by lateral incisor. Intrusion injury has a rarer occurrence in permanent dentition when compared with other types of luxation injuries. It comprises 3% of traumatic injuries in the permanent dentition.[3] The primary etiological factors are bicycle accidents, sports injury, falls, and fights.[1] Multiple injuries in the form of lateral luxation and intrusion although less common than single tooth injuries are seen in case of accidental and sport‑related trauma.
Traumatic luxation is a type of injury that involves eccentric displacement of the tooth, accompanied by communication or fracture of alveolar socket. The accepted treatment for lateral luxation is repositioning of the tooth at the
earliest and stabilization with a splint up to 3 weeks.[1,4] For intrusion, it is recommended to wait for spontaneous re‑eruption.[1,3,5] The greatest frequency (64%)[1] of pulp necrosis is encountered among intrusions followed by lateral luxation and extrusion, more frequently in teeth with fully developed roots. A thorough follow‑up period can disclose a number of complications such as pulp canal obliteration, pulp necrosis, inflammatory root resorption, and loss of marginal bone support.[1,3,5,6]
In terms of prevention of dentoalveolar injuries, the widespread use of mouthgaurd is an important measure in contact sports.[7] Thus, judicious use of diagnostic aids such as radiography and vitality testing and prompt surgical and endodontic intervention, with sufficient follow‑up are keys to the successful management of dentoalveolar fracture.
This paper reports the management of dentoalveolar trauma involving lateral and intrusive luxation in incisor teeth in mixed dentition period with stabilization, endodontic
Management of Dentoalveolar Trauma in Late Mixed Dentition
Rupinder V. Bhatia, Ashwin Jawdekar1, Namrata R. Mathrawala
Department of Pediatric and Preventive Dentistry, DY Patil University School of Dentistry, 1Department of Paediatric and Preventive Dentistry, Y.M.T. Dental College and Research Institute, Navi Mumbai, Mumbai, Maharashtra, India
ABSTRACTDentoalveolar trauma leading to intrusion and lateral luxation of maxillary lateral and central permanent incisor in late mixed dentition phase is reported. The laterally luxated central incisor tooth was splinted for 3 weeks. Endodontic treatment of the same with intracanal calcium hydroxide dressing and subsequent obturation with gutta-percha was accomplished after splint removal. The intruded lateral incisor was kept under observation to allow spontaneous re-eruption. Clinical and radiographic follow-up to 9 months revealed satisfactory periodontal healing of the repositioned maxillary central incisor and passive re-eruption of intruded lateral incisor. The central incisor was esthetically restored and mouthgaurd was fabricated to prevent future injuries to the dentition.
Key words: Dentoalveolar trauma, intrusion, luxation, mouthgaurds, splinting
Case Report
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Rupinder V. Bhatia, Department of Pediatric and Preventive Dentistry, D.Y. Patil University School of Dentistry, Nerul, Navi Mumbai ‑ 400 706, Mumbai, Maharashtra, India. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???.

Bhatia, et al.: Dentoalveolar trauma in mixed dentition
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 47
therapy, reestablishment of function and esthetics as well as prevention through fabrication of mouthguard and follow‑up.
CASE REPORT
A 12‑year‑old male child presented to the Department of Pediatric and Preventive Dentistry with traumatized upper front teeth and bleeding from mouth as a result of a direct, unintentional impact while swimming. The patient was brought to the clinic a day after injury where he received immediate attention. The child was conscious; there was no evidence of bleeding from nose and ears, with no episode of vomiting/convulsion, suggestive of any central nervous system injury. The child revealed a history of rheumatic heart disease 5 years back. The immunization status of the child was satisfactory. The child had been administered injection tetanus toxoid and advised antibiotics and analgesics by a general physician.
On clinical examination, laceration of the upper lip, alveolar mucosa, and palatal mucosa was noticed. The maxillary left central incisor was fractured at the incisal third of the crown and luxated buccally. The maxillary right central incisor was also fractured at the incisal third of the crown. Both teeth showed mobility. The maxillary left lateral incisor appeared intruded due to trauma [Figures 1 and 2]. The dental age of the child was approximately 10–11 years, indicative of late mixed dentition stage.
On the day of the examination, a treatment plan was presented to the parents that included soft tissue care, splinting of mobile teeth, commencement of endodontic treatment, and watchful supervision for the eruption of maxillary lateral incisor on the left side. The soft tissues were cleaned with irrigation using diluted betadine and saline. The patient was advised ice application on the upper lip intermittently to prevent soft tissue edema. An intraoral periapical (IOPA) radiograph was obtained [Figure 3]. The child was advised to complete blood investigations as a routine preparation for surgery. A pediatrician’s opinion and consent was sought in view of rheumatic heart disease and antibiotic cover before the commencement of the dental treatment.
Within 24 h, the child was taken for surgery. The child was administered bilateral infraorbital blocks. Blood clots were debrided by irrigation with normal saline. The maxillary left central incisor was relocated with gentle digital pressure and then, a composite wire splint extending from the maxillary left central incisor to the maxillary right first premolar was placed to keep luxated teeth in position [Figure 4]. Sutures were given to approximate the labial and palatal mucosa [Figure 4]. The child was instructed to have soft diet, gentle brushing, and thorough rinsing with betadine mouthwash and continue amoxicillin 500 mg tid for 5 days and ibuprofen 200 mg qid SOS. The splint was maintained for
15 days and then removed with care [Figure 5]. A necrosed bony sequestrum present between the left and right central
Figure 1: Preoperative photograph showing 21 displaced buccally, 22 intruded, and fracture involving enamel and dentin of 11 and 21 (facial view)
Figure 2: Preoperative photograph showing 21 displaced buccally, 22 intruded, and fracture involving enamel and dentin of 11 and 21 (palatal view)
Figure 3: Intraoral periapical radiograph showing widening of periodontal ligament space in relation to 21 and intrusion of 22

Bhatia, et al.: Dentoalveolar trauma in mixed dentition
48 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
incisors was removed under local anesthesia following the removal of splint [Figure 6].
Endodontic treatment was started for the maxillary left central incisor on the same day of splinting to prevent surface resorption, and IOPA radiograph exhibited apical widening of periodontal ligament (PDL) space. After obtaining access palatally, the pulp was extirpated, and the root canal was filled with calcium hydroxide. In the following visits, instrumentation of the canal followed by obturation of the tooth with gutta‑percha was done [Figure 7]. The fractured left and right central incisors were then restored with composite under rubber dam isolation [Figure 8]. The left lateral incisor was kept under observation.
Follow‑up radiographs were taken after 1 month and every 3 monthly for a period of 9 months [Figure 9]. The teeth 11, 21, and 22 were kept under close observation. Follow‑up radiographs up to 9 months show radiographic evidence of healing. Teeth 22 that appeared to have intruded showed marked coronal movement and now appears stable since 3 months in the present location with maintained vitality [Figure 10]. The child was counseled regarding the
prevention of dentofacial injuries, and a custom mouthgaurd made of thermoplastic polyvinyl resin was fabricated for wearing during contact sports activities [Figure 11].
DISCUSSION
The accepted treatment for luxation injury is immediate repositioning of the extruded tooth and stabilization, if necessary.[1] The most important factor in determining the treatment plan for luxated teeth is the presence or absence of significant apical displacement at the time of injury.[6] If there is radiographic evidence that the apex has moved out of its normal position, then there is a very high probability of compression of apical neurovascular bundle. Consequently, the tooth is likely to require root canal therapy, irrespective of whether it is mature or immature. Electric pulp testing of mechanically loosened teeth immediately after injury is not a reliable criterion for assessing vitality.[2] According to Andreason, the factor of the time interval from injury to repositioning of displaced
Figure 4: Photograph showing immobilization with wire composite splint extending from 21 to 14 and sutures in place
Figure 5: Photograph showing the presence of bony sequestrum between 11 and 21
Figure 6: Photograph after the removal of splint (2 weeks postoperative)
Figure 7: Intraoral periapical radiograph showing completed endodontic treatment of 21

Bhatia, et al.: Dentoalveolar trauma in mixed dentition
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 49
teeth appears critical causing root surface resorption.[1] Teeth treated within 90 min after injury show a very low frequency of root resorption compared with teeth treated at a later time. Since the child reported to us only after 24 h, as the risk of pulp necrosis increases with the extent of injury to the pulp and PDL and in teeth with complete root formation, prophylactic extirpation of the pulp has been recommended to prevent inflammatory root resorption.[1,3] Dressing of the root canal with calcium hydroxide has been shown to give a high frequency of healing.[5] In the present case, endodontic therapy was started early, followed by calcium hydroxide dressings to promote healing of periodontal tissues for 2 weeks. The conventional endodontic treatment was completed with a postendodontic composite restoration in 2–3 weeks after splint removal. The healing after endodontic treatment has been satisfactory both clinically and radiographically.
In the present case, IOPA radiograph showed widening in the apical third for the left maxillary central incisor, and lateral luxation with apical displacement usually shows a PDL space that has “empty” radiolucent space apically.[6]
Although there is no consensus reached on the optimal treatment of intruded permanent teeth in literature,[1] the options include allowing spontaneous re‑eruption of the tooth, immediate surgical repositioning and fixation, and
orthodontic repositioning.[3] It is recommended to wait for re‑eruption up to 3 weeks for immature teeth because of their high potential for eruption.[8] Furthermore, although such teeth often require endodontic treatment,[3] in the reported case here, we did not treat the tooth pulpally since the tooth has been vital till date.
Semi‑rigid splinting is commonly used to maintain the proper anatomical position of the tooth and prevent further trauma.[1,2,6] This splinting technique allows physiological tooth movement, preventing points of ankylosis from becoming permanent. Splinting is recommended for all loosened or displaced teeth, but in the case of intrusion, a period of careful observation is recommended to allow spontaneous re‑eruption to take place.[2,8] The maxillary left lateral incisor that showed incomplete root apex formation was not included in the splinting to allow spontaneous re‑eruption. The splinting included teeth as follows: 21, 11, 12, and 14.
It is important in all cases of luxation of teeth that assessment must be undertaken at 6 monthly intervals for at least 2 years following the removal of splint or on re‑eruption of the teeth following intrusion.[1,8] Follow‑up of 9 months has been reported in the present case. Periodic vitality testing and radiographs have been carried out.
Currently, there are three main types of mouthgaurds available to athletes. These are stock, mouth‑formed (i.e., boil and
Figure 8: Intraoral photograph showing esthetic restoration of 11 and 21
Figure 9: Intraoral periapical radiographs 3 months, 6 months, and 9 months postoperative
Figure 10: Photograph showing passive eruption in stable occlusion of intruded 22 after 9 months
Figure 11: Intraoral photograph of custom mouthgaurd in place

Bhatia, et al.: Dentoalveolar trauma in mixed dentition
50 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
bite) and custom‑fabricated mouthgaurds.[2,9] Custom‑made mouthgaurds offer advantages of optimal adaptation, maximum retention, superior comfort, and minimal interference with both breathing and speech.[9,10] The patient was of an athletic personality, constantly at a risk for trauma. The child was counseled regarding the prevention of sports injuries. In addition, a custom‑made mouthgaurd was fabricated to protect the patient from future dentoalveolar injury.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Andreasen FM, Andreasen JO. Luxation injuries. In: Andreasen JO,
Andreasen FM, editors. Textbook and Colour Atlas of Traumatic Injuries to the Teeth. 3rd ed. Copenhagen: Munksgaard Publishers; 1994.
2. Finn SB, Ripa L. The care of injuries to anterior teeth of children. In:
Finn S, editors. Textbook of Clinical Pedodontics. 4th ed. Philadelphia: W.B. Saunders; 1991.
3. Güngör HC, Cengiz SB, Altay N. Immediate surgical repositioning following intrusive luxation: A case report and review of the literature. Dent Traumatol 2006;22:340‑4.
4. Martins WD, Westphalen VP, Perin CP, Da Silva Neto UX, Westphalen FH. Treatment of extrusive luxation by intentional replantation. Int J Paediatr Dent 2007;17:134‑8.
5. de Alencar AH, Lustosa‑Pereira A, de Sousa HA, Figueiredo JH. Intrusive luxation: A case report. Dent Traumatol 2007;23:307‑12.
6. Berman LH, Blanco L, Cohen S, editors. Luxation injuries. In: A Clinical Guide to Dental Traumatology. St. Louis: Elsevier Health Sciences; 2006.
7. Santos Filho PC, Quagliatto PS, Simamoto PC Jr., Soares CJ. Dental trauma: Restorative procedures using composite resin and mouthguards for prevention. J Contemp Dent Pract 2007;8:89‑95.
8. Flores MT, Andersson L, Andreasen JO, Bakland LK, Malmgren B, Barnett F, et al. Guidelines for the management of traumatic dental injuries. I. Fractures and luxations of permanent teeth. Dent Traumatol 2007;23:66‑71.
9. Del Rossi G, Leyte‑Vidal MA. Fabricating a better mouthguard. Part I: Factors influencing mouthguard thinning. Dent Traumatol 2007;23:149‑54.
10. Mathewson RJ, Primosch CR, editors. Trauma to anterior teeth. In: Textbook of Fundamentals of Pediatric and Preventive Dentistry. 3rd ed. Chicago: Quintessence Pub. Co.; 1995.

© 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow 51
INTRODUCTION
Reactive lesions are one of the most common findings of oral cavity. Among these, peripheral ossifying fibroma (POF) contributes to 10% and pyogenic granuloma constitutes 80% of cases.[1] Ossifying fibroma can have central and peripheral variety. Endosteum or periodontal ligament (PDL) adjacent to the root apex is considered to be origin for central variety, whereas peripheral originates mostly from soft tissue overlying the alveolar process.[2,3] POF is defined as any solitary growth on the gingiva thought to arise from the PDL; most commonly at the region of the interdental papilla.[4]
Other terms used for POF are peripheral odontogenic fibroma, ossifying fibroma epulis, ossifying fibroma with calcification,[5] calcifying fibroma, peripheral cemento‑ossifying fibroma, ossifying fibroepithelial polyp, and calcifying fibroblastic granuloma.[6]
Hereby, we are reporting a case of POF in a female patient of age 22 years in maxillary anterior region of jaw. Since patient did not report any history of trauma and also considering the fact that local factors were minimal, these two could be easily excluded from being the etiological agent. Patient was in the 2nd decade of her life and therefore hormonal changes could be the reason.
CASE REPORT
A 22‑year‑old female patient [Figure 1] reported to the Department of Oral Medicine and Radiology, with a chief
complaint of swelling on the upper front region of mouth since last 6 months [Figure 2]. On eliciting the history of present illness, the swelling was insidious in onset. Initially, it was small peanut sized and progressively increased to present size. Occasionally, it was associated with pain. Patient did not give any history of trauma, injury, or food impaction and there was no significant medical history.
Intraoral examination revealed a well‑defined, solitary, sessile swelling oval in shape, size approximately 2 cm × 2 cm seen in interdental area of 11 and 21. Swelling extended from attached gingiva till gingival margin superoinferiorly and from mesial surface of 11 to mesial surface of 21 mesiodistally. It had smooth surface and distinct edges. The overlying surrounding mucosa was apparently normal [Figure 2].
On palpation, the gingival growth was nontender, firm to hard in consistency, nonreducible, noncompressible and fixed to underlying structures. No bleeding on probing was seen. Pathological migration and midline diastema could be observed between 11 and 21. Based on history and clinical examination, a provisional diagnosis of pyogenic granuloma and differential diagnosis of inflammatory gingival hyperplasia and POF was considered.
Intraoral periapical radiograph was taken in relation to 11, 21, and few flecks of calcification were seen in interdental of 11,
Peripheral Ossifying FibromaSonal Srivastava, Manaswita Tripathy, B. R. Chethan, Joel Dsilva1
Departments of Oral Medicine and Radiology and 1Oral and Maxillofacial Surgery, KVG Dental College, Sullia, Karnataka, India
ABSTRACTPeripheral ossifying fibroma is classified under reactive lesions of oral cavity. They are relatively uncommon gingival growth and constitute about 10% of all reactive lesions. Chronic irritation and trauma are considered to be etiological agent. Usually occur in young adults with a female predominance and are solitary in nature. We report a case of peripheral ossifying fibroma in a 22‑year old female.
Key words: Interdental, nonneoplastic, ossifying fibroma
Case Report
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Sonal Srivasatava, C1/25, Sector‑F, Jankipuram, Lucknow, Uttar Pradesh, India. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???.

Srivastava, et al.: A case report on peripheral ossifying fibroma
52 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
21 [Figure 3]. Oral prophylaxis was performed and lesion was excised by raising the flap form 13 to 23 region under local anesthetic [Figure 4]. Thereafter, excised specimen [Figure 5] was subjected to histopathologic examination. Histological examination revealed predominant fibrocellular connective tissue stroma consisting of one or more bundles of collagen fibers. Furthermore, spindle‑ and stellate‑shaped fibroblast with few areas of basophilic calcified masses, cellular inclusions, and reversal lines were seen which was suggestive of POF [Figure 6]. Patient was recalled after 2 week for follow‑up [Figure 7].
DISCUSSION
First description of ossifying fibroma was given by Menzel in 1872 while the term was given by Montgomery in 1927. It was first described as relatively uncommon, solitary, nonneoplastic gingival growth by Eversol and Robin.[7,8]
POF is found exclusively on the gingiva and does not arise in other oral mucosal location.[9] Can appear as pedunculated or
sessile, nodular mass. Usually, seen in the 1st and 2nd decade of life with predilection for females. Most commonly, it is found in incisor‑cuspid region of maxillary arch.[10] Usually, the mass is pink to red in color, slow growing, and asymptomatic. Consistency can vary from firm to hard based on the amount of calcification and ossification.[3]
Trauma and chronic irritation from subgingival plaque and calculus are considered to be the most common etiologic agent for POF. It is thought to be originating from PDL. Following reasons have been given for such consideration – exclusively seen on gingiva mostly interdental, lesion are in close proximity to PDL, within some lesions oxytalan fibers can be seen, age which is inversely proportional to a number of permanent teeth, and fibrocellular response which is similar to other gingival lesions of PDL origin.[11]
Howsoever, pathogenesis is still unclear. Certain hypothesis that has been given are – since these are clinically and histologically similar to pyogenic granuloma, some author thought it to be originating secondary to fibrosis of granulation tissue.[12] Similarly, these have a high predilection
Figure 1: Profile view of patientFigure 2: Clinical picture of lesion
Figure 3: Intraoral periapical radiograph showing few flecks of calcification in interdental area of 11 and 21 and midline diastema Figure 4: Surgical excision of lesion by raising flap from 13 to 23

Srivastava, et al.: A case report on peripheral ossifying fibroma
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 53
for female and the 2nd decade of life hormones are thought to play an important role. Most widely accepted hypothesis states that the presence of local irritants such as plaque,
calculus, overhanging restoration, and ill‑fitting denture can lead inflammatory reaction which in turn leads to inflammatory hyperplasia of cells of periodontium and PDL.[5]
Clinically, it is similar to peripheral fibroma, but histopathologic examination always reveals immature bone and osteoid within the lesion.[13]
Radiographically, it appears as radio‑opaque flecks or patches. Sometimes, separation of the adjacent teeth and occasionally resorption of the adjacent teeth may occur.[14]
Surgical excision is considered to be treatment of choice.[15] Improper removal can lead to recurrence. Recurrence rate of POF is high and varies from 7% to 45%.[10] Neville et al.[10] suggested that the lesion is removed from periosteum, and the adjacent teeth should be scaled to remove any remaining irritants. This helps in reducing the rate of recurrence. Furthermore, ill‑fitting dental appliance and rough restoration if any should be removed.[10]
There are high chances that these cases can be misdiagnosed as pyogenic granuloma, peripheral giant cell granuloma, or odontogenic tumors, and therefore histopathological examination is essential for accurate diagnosis.[16] Literature shows that most of the cases of POF have a range of 1st–2nd decades, more common in females and maxillary anterior region. Same were the finding of the present case. Hormonal changes were thought to be main etiological agent for the present case; however, minimal plaque could be seen in the region. Therefore, along with surgical excision of lesion removal of risk factor was considered as the treatment of choice.
CONCLUSION
A slowly growing soft tissue mass with speckled calcifications in the anterior oral cavity of young adults or children should raise a suspicion of a reactive gingival lesion such as POF. Histopathological examination is essential for accurate diagnosis. Once diagnosed, POF should be treated by total excision to prevent recurrence.
Declaration of patient consentThe authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
Figure 5: Excised specimen
Figure 6: Fibrocellular connective tissue consisting of dense collagen fibers interspersed with bony trabeculae and areas of dystrophic calcification
Figure 7: Follow‑up picture after 2 weeks

Srivastava, et al.: A case report on peripheral ossifying fibroma
54 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
REFERENCES
1. Babu KB, Pavankumar K, Naag S, Kumar AP. Peripheral ossifying fibroma. KDJ 2010;33:219‑21.
2. Singh AP, Raju MS, Mittal M. Peripheral ossifying fibroma: A case report. J Nepal Dent Assoc 2010;11:70‑2.
3. Kumar SK, Ram S, Jorgensen MG, Shuler CF, Sedghizadeh PP. Multicentric peripheral ossifying fibroma. J Oral Sci 2006;48:239‑43.
4. Bhaskar SN, Jacoway JR. Peripheral fibroma and peripheral fibroma with calcification: Report of 376 cases. J Am Dent Assoc 1966;73:1312‑20.
5. Agarwal P, Agarwal M, Bhattacharya H, Saluja M. Peripheral ossifying fibroma. J Dent Sci Oral Rehabil 2012;3:51‑2.
6. Nelson A, Mathew P, Sakthivel S, Austin RD. Peripheral ossifying fibroma – A case report and review of literature. J Adv Med Dent Sci 2014;2:127‑30.
7. Vhanmane P, Waghmare A, Savitha B, Bagde H. Peripheral cemento ossifying fibroma – Case report. Int J Dent Case Rep 2012;2:15‑8.
8. Chhina S, Rathore AS, Ahuja A. Peripheral ossifying fibroma of gingiva:
A case report. Int J Case Rep Imag 2011;2:21‑4.9. Jain A, Deepa D. Recurrence of peripheral ossifying fibroma: A case
report. People’s J Sci Res 2010;3:23‑5.10. Neville BW. Oral and Maxillofacial Pathology, 2nd ed. Philadelphia: WB
Saunders; 2002, p. 451‑2.11. Miller CS, Henry RG, Damm DD. Proliferative mass found in the gingiva.
J Am Dent Assoc 1990;121:559‑60.12. Yadav R, Gulati A. Peripheral ossifying fibroma: A case report. J Oral
Sci 2009;51:151‑4.13. Martins JC, Keim FS, Kreibich MS. Peripheral ossifying fibroma of the
maxilla: Case report. Int Arch Otorhinolaryngol 2008;12:295‑9.14. Glick G. Text book of Burket’s Oral Med Diag and Treatment 10th ed.
BC Decker: Ontario Haniton; 2003. p. 142.15. Rajendran R. Benign and malignant tumors of oral cavity. In: Shafer WG,
Hine MK, Levy BM, editors. Shafer’s Textbook of Oral Pathology. 5th ed. Philadelphia, PA: W.B. Saunders Co.; 2006. p. 113‑308.
16. Buduneli E, Buduneli N, Unal T. Long term follow up of peripheral ossifying fibroma report of three cases. J Period Cline Invest 2001;23:11‑4.

© 2016 Indian Journal of Oral Health and Research | Published by Wolters Kluwer ‑ Medknow 55
INTRODUCTION
Jaffe originally coined the term “giant cell reparative granuloma.” According to him, the lesion was a response to intraosseous hemorrhage resulting from jaw trauma.[1] Other researchers prefer the term “giant cell granuloma” to describe this lesion, noting the inconsistent history of trauma and lack of significant elements of reparative terms. Thus, the word “reparative” was omitted.[2]
Central giant cell granuloma (CGCG) is a bony lesion mainly affecting adolescents and young adults, preferably younger than 20 years. The etiology of the lesion is still debatable. Some considered it to be a reactive lesion to an unknown stimulus and some considered it to be a neoplastic lesion. The lesion is more often located in the mandible.[1] The presenting symptom in majority of the cases is painless swelling. Although the histologic appearance of the lesion is benign, some maxillary lesions may have malignant characteristics.
CASE REPORT
A 20‑year‑old female patient presented to the department of oral medicine and radiology with a chief complaint of swelling on the left side of the face for 1 year as shown in Figure 1, which was insidious on onset and started as a swelling in the
upper left posterior palatal region, which gradually increased to involve the entire palate and the left side of the face.
On extraoral examination, the face was grossly asymmetrical. Swelling was present on the left side of the face which extended superoinferiorly from the left infraorbital region to 1 cm above the left inferior border of the mandible and mediolaterally from the left lateral nasal process to approximately 3 cm in front of the tragus. The nasolabial fold and philtrum were obliterated. The swelling had well‑defined margins on palpation with firm consistency, and was nontender and compressible. The temperature over the swelling was normal. Cervical lymph nodes were not palpable.
On intraoral examination, a firm swelling was noted involving the entire hard and soft palate extending from the mesial aspect of the maxillary right central incisor to the distal aspect of the maxillary left second molar causing obliteration of the left vestibule as shown in Figure 2. Overlying mucosa was slightly purplish at the posterior palatal region. Teeth
An Unusual Case of Maxillary Central Giant Cell Granuloma
Ruchika Kapoor, Freny Rashmiraj Karjodkar, Kaustubh Sansare, Amaresh Chandra Dora
Department of Oral Medicine and Radiology, Nair Hospital Dental College, Mumbai, Maharashtra, India
ABSTRACTCentral giant cell granuloma, formerly known as giant cell reparative granuloma, is considered as a reactive lesion to an unknown stimulus or a neoplastic lesion. The lesion mainly affects young adults and commonly involves mandible more than maxilla. When present in the maxilla, it is usually seen anterior to cuspids, but in this case, it was the posterior maxilla which was involved making it an unusual site for its occurrence. This case report describes a 20-year-old female patient presenting with a chief complaint of swelling of the left side of the face for 1‑year. Depending on the clinical features and radiographic findings, a diagnosis of giant cell granuloma was made, which was surgically excised.
Key words: Giant cells, hyperparathyroidism, maxilla
Access this article online
Website:
www.ijohr.org
Quick Response Code
DOI:
***
Corresponding Author: Dr. Ruchika Kapoor, Department of Oral Medicine and Radiology, Nair Hospital Dental College, Mumbai ‑ 400 008, Maharashtra, India. E‑mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: ???.
Case Report

Kapoor, et al.: Maxillary central giant cell granuloma
56 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
number 21, 22, 23, 24, 25, 26, and 27 were Grade II mobile and extruded with spacing as shown in Figure 3.
Panoramic radiograph revealed a well‑defined expansile lesion within the left maxilla extending mediolaterally from the mesial aspect of 13 to the distal aspect of 27 and superoinferiorly from the floor of the left orbit to the crest of the maxillary alveolar bone. Displacement, extrusion, and root resorption were seen in teeth 11, 21, 22, 23, 24, 25, 26, and 27. Root of 13 was distally tilted. Borders of the left maxillary sinus were not traceable [Figure 4].
Computed tomography revealed partial cortication with expansion of the bone. Perforation was present at the lateral and inferior aspects of the left maxilla. Internal structure had wispy septae. Obliteration of the left maxillary sinus was noted [Figure 5].
Serum calcium, phosphorous, alkaline phosphatase, and parathyroid hormone (PTH) levels were within normal limits. Brown tumor of hyperparathyroidism was excluded on the basis of age and laboratory investigations.
Figure 1: Profile photograph shows diffuse swelling of the left side of the face
Figure 4: Panoramic radiograph showing well‑defined expansile lesion involving the left maxilla with displacement of teeth, root resorption, and obliteration of sinus
Based on clinical features, radiographic findings, and serum levels, a diagnosis of giant cell lesion was made.
Excision of tumor with free fibula flap reconstruction was done, and the patient is kept on follow‑up for any recurrence [Figures 6 and 7].
Histopathological examination revealed numerous multinucleated giant cells with a background of plump proliferating mesenchymal cells with extravasated red blood cells favoring aggressive giant cell lesion as shown in Figure 8.
DISCUSSION
CGCG, formerly known as giant cell reparative granuloma, is considered as reactive lesion to an unknown stimulus. The lesion mainly affects young adults and involves mandible more than maxilla.
The most common presenting sign is painless swelling. The overlying mucosa appears normal unless traumatized. The lesion predominately involves the region anterior to the first molar in the mandible and anterior to cuspids in the maxilla. The lesion sometimes crosses the midline. When present in the maxilla, it is usually seen anterior to cuspids, but in this
Figure 2: Swelling involving the entire hard and soft palate
Figure 3: Swelling and obliteration of the left side vestibule

Kapoor, et al.: Maxillary central giant cell granuloma
Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016 57
case, it was the posterior maxilla which was involved, making it an unusual site for its occurrence.
Although considered as benign reactive osseous lesion, CGCG has been classified into two types based on its clinicoradiologic features as nonaggressive lesion which is usually asymptomatic and slow growing, and an aggressive type which is most of the times painful, grows rapidly into a large size, perforating the cortex causing root resorption, and has a tendency to recur.[2,3] The radiographic appearance of the lesion can be unilocular or multilocular. As the lesion grows slowly, it usually produces well‑defined margins. In certain cases, there is no evidence of cortication and may have ill‑defined margins, especially in the maxilla as was seen in this case. Small lesion may not show any evidence of internal structure. Large lesion may have ill‑defined wispy septa. Septa arising at the right angle from the periphery of the lesion with small indentation of the expanded cortical plate at the origin of the septa make the diagnosis of CGCG most likely. As the radiographic findings are not pathognomonic of the disease, the final diagnosis depends on the histopathology.
The differential diagnosis of CGCG includes brown tumor of primary hyperparathyroidism, aneurysmal bone cyst,
ameloblastoma, and odontogenic myxoma. Ameloblastoma and odontogenic myxoma are found in older age group. PTH levels, alkaline phosphatase, and serum calcium levels need to be checked to rule out the brown tumor of primary hyperparathyroidism, which is increased in hyperparathyroidism. Ameloblastoma has coarse, curved, well‑defined trabeculae and odontogenic myxoma has sharp and straight septae and do not expand to such an extent as seen in this case.
Treatment of CGCG includes curettage and resection of the jaw.[4]
Alternative therapies such as intralesional injections of corticosteroids, subcutaneous administration of calcitonin, or interferon alpha have also been tried with variable success rates.[5,6] Aggressive lesion curettage for young patients is not an effective treatment for aggressive lesions; en bloc resection is the treatment of choice. Even though radical resection is an effective modality for aggressive lesions, it leads to functional disturbances.[7,8]
Figure 5: Coronal computed tomography scan shows partial cortication, expansion with perforation of the left maxillary sinus
Figure 6: Postoperative facial profile
Figure 7: Postoperative panoramic radiograph of the patient showing graft placement and bony plates
Figure 8: High power histopathological picture of giant cell lesion

Kapoor, et al.: Maxillary central giant cell granuloma
58 Indian Journal of Oral Health and Research / Vol. 2 / Issue 1 / Jan-Jun 2016
Follow‑up at regular interval is mandatory to rule out any occurrence. Recurrences are rare and are more common in the maxilla.[9,10]
Declaration of patient consentThe authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
REFERENCES
1. Motamedi MH, Eshghyar N, Jafari SM, Lassemi E, Navi F, Abbas FM, et al. Peripheral and central giant cell granulomas of the jaws: A
demographic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:e39‑43.
2. Whitaker SB, Waldron CA. Central giant cell lesions of the jaws. A clinical, radiologic, and histopathologic study. Oral Surg Oral Med Oral Pathol 1993;75:199‑208.
3. Chuong R, Kaban LB, Kozakewich H, Perez‑Atayde A. Central giant cell lesions of the jaws: A clinicopathologic study. J Oral Maxillofac Surg 1986;44:708‑13.
4. de Lange J, van den Akker HP, van den Berg H. Central giant cell granuloma of the jaw: A review of the literature with emphasis on therapy options. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:603‑15.
5. Adornato MC, Paticoff KA. Intralesional corticosteroid injection for treatment of central giant‑cell granuloma. J Am Dent Assoc 2001;132:186‑90.
6. Pogrel MA. Calcitonin therapy for central giant cell granuloma. J Oral Maxillofac Surg 2003;61:649‑53.
7. Eisenbud L, Stern M, Rothberg M, Sachs SA. Central giant cell granuloma of the jaws: Experiences in the management of thirty‑seven cases. J Oral Maxillofac Surg 1988;46:376‑84.
8. Roberts J, Shores C, Rose AS. Surgical treatment is warranted in aggressive central giant cell granuloma: A report of 2 cases. Ear Nose Throat J 2009;88:E8‑13.
9. Stavropoulos F, Katz J. Central giant cell granulomas: A systematic review of the radiographic characteristics with the addition of 20 new cases. Dentomaxillofac Radiol 2002;31:213‑7.
10. White SC, Pharoah MJ. Oral Radiology: Principles and Interpretation. 6th ed. Missouri: Mosby; 2009. p. 442‑5.