Embed Size (px)
Citation preview

Primary Progressive Aphasia: PPA and theLanguage Network
Sreepadma P. Sonty, BA,1 M.-Marsel Mesulam, MD,1–3 Cynthia K. Thompson, PhD,1,2,4
Nancy A. Johnson, PhD,1,3 Sandra Weintraub, PhD,1,3 Todd B. Parrish, PhD,1,5
and Darren R. Gitelman, MD1,2,5,6
Primary Progressive Aphasia (PPA) is a behaviorally focal dementia syndrome with deterioration of language functionsbut relative preservation of other cognitive domains for at least the first two years of disease. In this study, PPA patientswith impaired word finding but intact comprehension of conversational speech and their matched control subjects wereexamined using voxel-based morphometry (VBM) and functional magnetic resonance imaging (fMRI). fMRI comparedsignal changes during phonological and semantic language tasks with those during a control task (matching letters). PPApatients showed longer reaction times and reduced accuracy versus controls on the language tasks, but no performancedifferences on the control task. VBM demonstrated reduced gray matter in left superior temporal and inferior parietalregions in the PPA group. However, these patients showed a normal pattern of activation within the classical languageregions. In addition, PPA patients showed activations, not seen in normals, in fusiform gyrus, precentral gyrus, andintra-parietal sulcus. These activations were found to correlate negatively with measures of naming and task performance.The additional activations in PPA may therefore represent a compensatory spread of language-related neural activity ora failure to suppress activity in areas normally inhibited during language tasks.
Ann Neurol 2003;53:35–49
Primary progressive aphasia is a dementia syndromecharacterized by the insidious onset and gradual pro-gression of deficits that can involve any aspect of lan-guage, including word finding, object naming, fluency,syntax, and word comprehension. The initial symp-toms occur in the absence of major deficits in othercognitive domains, particularly memory, for at least thefirst 2 years after onset.1–4 Although isolated cases ofprogressive language dissolution had been described inthe late 19th and early 20th centuries,5–9 the first re-port focusing on a series of patients with slowly pro-gressive aphasia was published in 1982 and led to thesubsequent delineation of the primary progressiveaphasia (PPA) syndrome.1,4
Patients with PPA can have a fluent or nonfluentaphasia and can display variable deficits of languagecomprehension. The related term “semantic dementia”has been used to denote a type of progressive aphasiacharacterized by preserved fluency and impaired lan-guage comprehension. Semantic dementia is also occa-sionally accompanied by visual face and object recog-nition deficits such as prosopagnosia.10–13 When free
of face and object recognition deficits, semantic de-mentia constitutes a subtype of PPA with poor com-prehension of verbal semantics. The patients in thisstudy had intact comprehension of conversationalspeech and therefore represent a PPA clinical subtypedistinct from semantic dementia.
Neuropathological reports in nearly 50 patients withPPA have identified abnormalities in frontal, perisyl-vian, and temporal cortices.2,14–16 Approximately 60%of patients have shown nonspecific focal atrophy, alsoknown as neuronal loss with gliosis lacking in distinctivehistopathological features.2 Fewer than 20% show thepathology of Alzheimer’s disease. Some of these pa-tients have an unusual perisylvian and temporal neo-cortical distribution of neurofibrillary tangles, whichoccasionally spares medial temporal lobe structures.17
Another 20% show the tau-positive, intracytoplasmicbodies of Pick’s disease.18 In patients without Alzhei-mer’s disease pathology, PPA can be considered one ofthe focal variants of frontotemporal dementia.
Computerized tomography and magnetic resonanceimaging (MRI) of the brain have largely corroborated
From the 1Cognitive Neurology and Alzheimer’s Disease Centerand Departments of 2Neurology, 3Psychiatry, 4Communication Sci-ences and Disorders, and 5Radiology, Northwestern University,Chicago, IL; and 6VA Chicago Lakeside Division, Chicago, IL.
Received Oct 2, 2001, and in revised form Feb 27 and Aug 6,2002. Accepted for publication Aug 6, 2002.
Address correspondence to Dr Gitelman, 320 E. Superior Street,Searle 11-470, Chicago, IL 60611.E-mail: [email protected]
This article is a US Government work and, as such, is in the public do-main in the United States of America.
Published 2002 by Wiley-Liss, Inc. 35

the focality of anatomical involvement and have shownpredominant atrophy in the left lateral temporal lobe(superior, middle, and inferior gyri) in patients withPPA.19–21 Moreover, positron emission tomography(PET) and single-photon emission computerized to-mography in patients with PPA have shown resting-state deficits in cortical metabolism and blood flow inleft anterior and posterior perisylvian regions.2,22–24 Al-though some right-sided abnormalities have beenfound in a few cases, the metabolic state of the righthemisphere generally has been within normal limits inthese studies. Thus, resting functional imaging datahave largely reflected the clinical focality of PPA.
To date, few functional neuroimaging studies havebeen performed with PPA patients. Grabowski and col-leagues performed an 15O-PET imaging study in a sin-gle patient with PPA, who showed abnormal activationin the left middle frontal and inferotemporal regions,and deactivations in the right hemisphere.25 Another15O-PET study compared normal subjects with fourpatients with progressive fluent aphasia and poor com-prehension (ie, semantic dementia). This study demon-strated decreased activity in the left posterior inferiortemporal gyrus and increased activity in left premotor,left anterior superior temporal, and right temporopari-etal areas during the pyramids-and-palm trees test ofvisual semantic categorization.26 The regions of func-tional abnormality were anatomically distinct from an-terolateral temporal areas that showed decreased graymatter density as estimated by voxel-based morphom-etry (VBM) in the same patients. These findings led tothe hypothesis that semantic dementia may reflect adisruption of functional connectivity involving the pos-terior inferior temporal lobe, and that this disruptioncould even include areas showing minimal atro-phy.26,27
PPA and its variants provide a unique opportunityto study how the language network changes in responseto an apparently focal and slowly progressive diseaseprocess. This report is based on a sample of PPA pa-tients with impaired word finding but preserved com-prehension of conversational speech. Preliminary re-sults on a subset of these patients have been reported inabstract form.28 The specific aims of this study were todetermine how this subtype of PPA alters the func-tional anatomy of language networks, whether thefunctional changes are distinct from areas of corticalatrophy, and whether these two markers of PPA arerelated to language abilities.
Subjects and MethodsSubjectsFourteen patients (mean age, 64 � 6.6 years; 8 men, 6women) who fulfilled the diagnostic criteria for PPA,4 (Table1) and who demonstrated relatively intact verbal comprehen-sion on clinical examination were recruited for this study.
The clinical impression of intact comprehension was basedon the patient’s ability to comprehend conversational speechand intact comprehension of object names during formaltesting. Patients were additionally classified as fluent or non-fluent. The designation of “nonfluent” reflected the presenceof one or more of the following criteria: (1) reduced numberof words expressed per minute, (2) decreased phrase length,or (3) frequent word-finding pauses either in spontaneousspeech output or on the Oral Cookie Theft subtest of theBoston Diagnostic Aphasia Examination (BDAE).29 Four-teen older normal control subjects (mean age, 63 � 8.6; 8men, 6 women) with no history of significant medical, neu-rological, or psychiatric illness also were recruited. All sub-jects were right-handed as assessed by the modified Edin-burgh inventory30 with an average handedness score of�95 � 7.75 for the PPA subjects and �90 �14.4 for thenormal subjects (p � 0.05). All subjects specified English astheir first language. Informed consent was obtained from allsubjects, and the study protocols were approved by the In-stitutional Review Board at Northwestern University.
Neuropsychological TestingMost of the PPA patients, as well as most of the controls,underwent neuropsychological testing within 6 months ofscanning for characterization of their cognitive functioningin a variety of domains including attention, language, mem-ory, comportment, executive, and visuospatial functions. Asubset of the following neuropsychological batteries were ad-ministered to each subject: language measures: WesternAphasia Battery,31 Boston Diagnostic Aphasia Examination(selected subtests),29 Boston Naming Test (BNT)32; nonlan-
Table 1. Diagnostic Criteria for PPA (Mesulam4)
1. Insidious onset and gradual progression of word-finding,object-naming, or word comprehension impairments asmanifested during spontaneous conversation or as as-sessed through formal neuropsychological testing of lan-guage.
2. All limitation of daily living activities can be attributedto the language impairment, for at least 2 years afteronset.
3. Intact premorbid language functions (except for devel-opmental dyslexia).
4. Absence of significant apathy, disinhibition, forgetfulnessfor recent events, visuospatial impairment, visual recogni-tion deficits, or sensorimotor dysfunction within the ini-tial 2 years of illness. This criterion can be fulfilled byhistory, survey of daily living activities, or formal neuro-psychological testing.
5. Acalculia and ideomotor apraxia can be present even inthe first 2 years. Mild constructional deficits and perse-veration (eg, as assessed by the go no-go task) are alsoacceptable as long as neither visuospatial deficits nor dis-inhibition influence daily living activities.
6. Other domains may become affected after the first 2years, but language remains the most impaired functionthroughout the course of the illness and deterioratesfaster than other affected domains.
7. Absence of “specific” causes such as stroke or tumor asascertained by diagnostic neuroimaging.
PPA � primary progressive aphasia.
36 Annals of Neurology Vol 53 No 1 January 2003

guage measures: Mini-Mental Status Exam,33 Consortium toEstablish a Registry for Alzheimer’s Disease (CERAD) WordList Learning,34 CERAD Word List Recognition, WechslerMemory Scale–Revised Logical Memory I and II, WordList Generation (category fluency: animals and lexicalfluency),35,36 Judgment of Line Orientation,37 Trail MakingTest,38 and the Geriatric Depression Scale.39
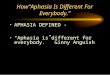
Behavioral TasksAll participants performed two tasks, identical in design andtime course, while undergoing fMRI. During the active con-dition of both tasks, subjects were presented visually withpairs of words and were asked to make a judgment aboutthese words (Fig 1). In the phonological task (HOM), sub-jects viewed a pair of words and pushed a button only if thewords were homonyms (ie, had identical pronunciation butdissimilar orthography and meaning). In the semantic task(SYN), subjects responded only if the words in a pair weresynonyms (ie, had a very similar meaning but dissimilar or-thography and phonology). The words presented in the twotasks were obtained from the on-line Oxford PsycholinguisticDatabase and were controlled for length (four to seven char-acters) and a Kucera–Francis frequency of 10 to 500.40
For the reference control condition in both tasks(STRINGS), subjects were presented with pairs of all-consonant letter strings of the same average length as thewords in the active task and were asked to respond if theletter strings were identical. Subjects responded in all casesby pressing a response button held in their right hand. Re-action times were recorded for all responses. Task accuracywas determined from the percentage of correct behaviors,that is, (no. of hits � no. of correct rejections)/total no. ofstimuli.
The tasks followed a block design and consisted of eightblocks each of the control and active conditions presentedalternately. The stimuli were presented every 5,505 millisec-
onds, and individual blocks lasted 30 seconds. Stimuli werepresented and responses were collected using Superlab soft-ware (Cedrus, San Pedro, CA) running on a Power Macin-tosh computer (Apple, Cupertino, CA). The stimuli wereprojected onto a custom-designed nonmagnetic rear-projection screen using a Proxima active matrix liquid crystaldisplay projector (San Diego, CA). Subjects viewed thescreen, located approximately 170cm from their eyes,through a nonmagnetic mirror.
Subjects went through an initial training period on abbre-viated versions of the two tasks while outside the scanner.Ultimate inclusion of subjects in the group analysis was de-pendent on relatively intact language comprehension andabove-chance performance (�62.5% accuracy, 24/40 cor-rect), on each of the three conditions during the actual ex-perimental session. Accuracy estimates were based on the bi-nomial test. These criteria were met by 10 of the 14 subjectsfor the homonym task and by 11 subjects for the synonymtask. The remaining PPA patients were excluded from anal-ysis, giving a final group size of 10 patients for the HOMtask analysis and 11 patients for the SYN task analysis. Thecontrol group for both tasks contained 11 cognitively intactindividuals chosen to match the overall group of 11 PPApatients for age, gender, and education (Table 2).
Functional Magnetic Resonance ImagingSubjects were imaged using a 1.5T Siemens Vision scanner(Erlangen, Germany). The subjects’ heads were immobilizedusing a vacuum pillow (VacFix, Bionix, Toledo, OH) in ad-dition to the restraint calipers built into the head coil, tominimize head movements during the scanning procedure.41
Laterality for image processing was indicated using a vitaminE capsule taped to the left temporal region.
Single-shot echo planar images were obtained in 32 slicesparallel to the anterior commisure-posterior commisure (AC-PC) line according to parameters in our previous studies forblock-designed tasks: TR/TE, 4,350/40 milliseconds; flip an-gle, 90 degrees; field of view, 240mm; matrix, 64 � 64; andslice thickness, 4mm.42 At the beginning of each functionalrun, the MR signal was allowed to equilibrate over fourscans, which were excluded from analysis. In addition, high-resolution, T1-weighted anatomical images were acquired us-ing a three-dimensional fast low-angle shot sequence (TR/TE, 22/5.6 milliseconds; flip angle, 25 degrees; field of view,256mm; matrix, 256 � 256; slice thickness, 1mm). A satu-ration band was located inferior to the imaging volume to
Fig 1. Graphical representations of the phonological (HOM)and semantic (SYN) tasks. Arrowheads indicate the targetstimuli in the active and control conditions for each task.
Table 2. Subject Demographics
DemographicPPA Group(n � 11)
Normal Group(n � 11)
Age (yr) 63.4 � 4.6 66.5 � 6.7M:F ratio 5:6 5:6Education (yr) 16.5 � 3.4 16.0 � 1.9Mean disease duration
(yr)3.0 � 1.5 n/a
Handedness 95.9 � 7.4 96.8 � 6.4
PPA � primary progressive aphasia; n/a � not applicable.
Sonty et al: Language Network Changes 37

null the signal from the arteries and reduce pulsation artifactsin the temporal lobes. The final voxel size was 1mm3.
Functional Magnetic Resonance Data AnalysisfMRI data were analyzed on UNIX/Linux workstations un-der the Matlab software environment (Mathworks, Sherborn,MA) using SPM99 (Wellcome Department of CognitiveNeurology, London, UK; http://www.fil.ion.ucl.ac.uk/spm).43–46 All functional images were time acquisition cor-rected to the slice obtained at 50% of the TR. The imageswere realigned to the functional scan immediately precedingthe anatomical T1 image. All images (anatomical and func-tional) were normalized to the Montreal Neurological Insti-tute (MNI-305) template, which approximates the anatomi-cal space delineated by Talairach and Tournoux.47
Functional images then were smoothed with a 10mm fullwidth half maximal height isotropic Gaussian kernel for in-clusion in the group analyses.
Condition-specific effects at each voxel were estimated us-ing the general linear model.44 Linear contrasts were set upto test for voxelwise effects of signal differences between theactive and control conditions, and SPM(t) maps were calcu-lated for individual subjects. Within-group and intergroupcomparisons were performed using a random effects modelto account for the effects of intersubject variability. The ran-dom effects analysis was performed by first generating pa-rameter effects images for each contrast within a subject. Forexample, in the SYN task, a parameter effect image of SYNversus STRINGS was generated for each PPA patient or nor-mal subject. These images then were entered into second-level analyses using one-sample t tests for effects withingroups, and two-sample t tests for effects between groups.Significance was assigned to the resulting t-fields using thetheory of Gaussian random fields.44,46 The random effectsSPM(t) maps were thresholded at a p value less than or equalto 0.001 uncorrected, and activations were considered signif-icant at a p value of less than or equal to 0.05 after correc-tion for multiple comparisons across the volume. Additionalanalyses included simple regression analyses, which tested forcorrelations of activity with reaction times or accuracy foreach of the subject groups.
To test for possible relationships between the patients’clinical fluency subtype and the functional or structural im-aging results, we designated PPA patients as fluent or non-fluent (by two neurologists, D.R.G. and M.-M.M.) on thebasis of the clinical neurological examination. The examinerswere blinded to the subjects’ MRI results when rating them.The patients’ fluency status then was used as a covariate inan analysis. Other analyses included simple regression to ex-amine the relationship between activations and language testperformance as estimated by the PPA patients’ score on theBNT. The BNT was chosen because all subjects received thistest (see Table 4).
In addition to the whole-brain analyses specified above,the described correlation and regression analyses were per-formed on the areas identified as active by the intergroupcomparisons for each language task. These regions of interest(ROI) analyses were performed to reduce the impact of mul-tiple comparisons on the calculation of significance for theseregions. The use of regions defined by the intergroup con-
trasts was valid because the correlational and regression anal-yses were orthogonal to these contrasts.
Masked AnalysesTo assess whether intergroup comparisons were significantbecause of increased activity in the PPA group or decreasedactivity in the normal group, we inclusively masked the anal-yses comparing both groups by the respective main effects.Masking analysis ensures that the results at least reflect thepresence of a positive simple main effect. For example, re-sults from the intergroup homonym contrast (PPAHOM �PPASTRINGS) � (NLHOM � NLSTRINGS) were masked byPPAHOM � PPASTRINGS. This analysis therefore displays re-gions that showed greater activation in the PPA than in thenormal group and had to be present in the PPAHOM �PPASTRINGS comparison. Thus, the activation could not justreflect deactivations in the NLHOM � NLSTRINGS contrast.A second analysis masked (NLSTRINGS � NLHOM) �(PPASTRINGS � PPAHOM) by (NLSTRINGS � NLHOM). Thisanalysis showed areas that were significantly deactivated inthe normal group. Similar analyses were performed for thesynonym task. In all cases, the functional image determiningthe mask was thresholded at a p value of less than 0.05 un-corrected. Note that the masking procedure does not affectthe final statistics, which always used a significance level of por equal to less than 0.05 corrected.48
Plot of Parameter EstimatesTo further examine the fMRI response for each task in eachgroup, we extracted and compared the parameter estimatesfrom the voxels showing significant differences betweengroups from each of the individual subjects. The parameterestimates provide a measure of the fMRI response for eachcontrast (eg, HOM � STRINGS or SYN � STRINGS).Because SPM99 normalizes the signal to a value of 100, theresponse is proportional to percentage signal change betweenactive and control conditions and can be compared withinand between subject groups.
Voxel-based MorphometryThe T1-weighted structural MRI scans were preprocessed bynormalization to the MNI-305 template, followed by seg-mentation of gray and white matter.49–51 The gray matterimage segments were multiplied by the Jacobian determi-nants of the deformation fields that were defined during nor-malization. This step has the effect of transforming gray mat-ter per unit volume in normalized space into a densitymeasure in native space and essentially conserves the amountof gray matter before and after normalization (ie, gray matteris not added if there is regional stretching of the brain, orlost if it is compressed).50 Segmented gray matter imageswere smoothed with a 12mm isotrophic Gaussian kernel andanalyzed at each voxel for changes in gray matter density inPPA patients relative to the controls, as an indirect measureof neuronal loss. A confound for global signal was includedin this analysis so that inferences pertain to regionally specificeffects and not global measures of atrophy. Significance wasassigned to the resulting t-fields using the theory of Gaussianrandom fields,44,46 and the resulting statistical map wasthresholded at p values less than or equal to 0.001 uncor-
38 Annals of Neurology Vol 53 No 1 January 2003

rected. Significance was based on p values less than or equalto 0.05 corrected for multiple comparisons. The entire lefthemisphere was designated as an a priori region of inter-est based on previous studies defining the general location ofatrophy in PPA patients.2,14–16,20,21As with the functionalMRI data, whole-brain regression and analysis of variance, aswell as region of interest analyses based the areas of signifi-cant anatomical difference between groups, were conductedon gray matter segment images to examine the correlationsbetween the pattern of atrophy and clinical subtype (fluency)or disease severity (based on the BNT).
ResultsNeurological ExaminationThe neurological examination in all patients showedword-finding and naming deficits and variable degreesof dysgraphia. Comprehension was relatively preservedin conversation, although 8 of 11 patients had diffi-culty comprehending grammatically complex sentenceswith embedded clauses. A subset of the patients (8 of11) was nonfluent, as reflected by decreased phraselength, frequent word-finding pauses either in sponta-
Table 3. Clinical Language Characteristics of PPA Patients
Demographics Language Findings at Initial Evaluation
SubjectNo.
OnsetAge/
GenderYears ofAphasiaa Conversational Speechb Repetitionc
AuditoryComprehension Naming Writing Fluentd
F087 67/F 2 Pauses, rare paraphasias Mild gram-maticalerrors
Relatively intact exceptpassive voice
Normal, exceptgeometricshapes
Moderatedysgraphia
No
F179 60/M 2 Pauses, short phraselength, occasionalparaphasias
Nouns intact,grammati-cal errors
Relatively intact exceptpassive voice
Mild to mod-erate
Not assessed No
F204 62/F 5 Pauses, short phraselength, frequentparaphasias, circum-locution, emptyspeech
Grammaticalerrors
Intact Severely im-paired
Severe dys-graphia
No
F224 54/M 3 Normal phrase length,phonemic parapha-sia, grammatical er-rors
Mild forwords, se-vere forsentences
Relatively intact, milddifficulties in con-versation
Severely im-paired
Mild dys-graphia,spellingerrors
Yes
F240 53/M 6 Few words per minute,normal phraselength, word-findingdifficulty, phonemicparaphasia, circumlo-cution
Severely im-paired forgrammar
Intact except for run-ning conversationand complex sen-tences
Impaired forparts of ob-jects
Severe dys-graphia
No
F269 63/M 4 Pauses, rare phonemicparaphasia, normalphrase length
Intact Relatively intact exceptpassive voice
Impaired forparts of ob-jects
Severe dys-graphia
Yes
F350 65/M 2 Normal phrase length,mild dysarthria, pho-nemic paraphasia
Mildly im-paired
Intact Intact Preserved,somespellingerrors
Yes
F363 58/F 2 Reduced words perminute and phraselength, omission offunction words
Intact Intact, except for com-plex sentences withpossessives
Mildly im-paired forparts of ob-jects
Dysgraphia No
F364 63/F 2 Reduced words perminute, pauses forword finding, milddysarthria
Intact Intact, except passivevoice
Mildly im-paired forparts of ob-jects
Dysgraphia No
F437 69/F 2 Severe dysarthria, re-duced words perminute and phraselength
Impaired Intact Severe for oral,mildly im-paired forwritten
Relativelypreserved
No
F452 63/F 2 Reduced words perminute and phraselength, pauses, sim-plification
Intact Intact except for rarelexical lacunes andcomplex sentences
Intact, at raretimes hesi-tant
Relativelypreserved
No
aBefore appearance of other symptoms.bArticulation, flow (words per minute); phrase length means words per utterance; pauses means word-finding pauses; normal/abnormal gram-matical structure, meaningful/empty, circumlocution, phonemic paraphasia.cWhole words, sentences, grammatical terms.dNonfluent defined by reduced number of words per minute, reduced phrase length, and/or frequent word finding pauses in conversationalspeech or on the Oral Cookie Theft subtest of the Boston Diagnostic Aphasia Examination.
PPA � primary progressive aphasia.
Sonty et al: Language Network Changes 39

neous speech output or on the Oral Cookie Theftsubtest of the Boston Diagnostic Aphasia Examination,or a decreased number of words per minute in conver-sation.29 Three of the patients were largely fluent,showing relatively preserved phrase length and flow,and infrequent word-finding pauses (Table 3).
Neuropsychological TestingPPA patients showed impairments on some tests oflanguage, for example, BNT and verbal fluency (lex-ical and categorical). However, these patients per-formed within normal limits on auditory verbal com-prehension subtests taken from either the WesternAphasia Battery or the Boston Diagnostic Aphasia Ex-amination.29 Some patients also showed impairmentson neuropsychological tests that required verbal com-prehension or response (eg, Mini-Mental StatusExam, CERAD Word Lists, CERAD Logical Mem-ory I & II [recall]). However, a clinical review ofdaily living activities and knowledge of current eventsfor each patient did not provide evidence for any im-pairment of episodic memory. In addition, when ver-bally mediated tests were adapted to reduce the needfor a spoken response, subjects displayed preserved re-tention of information. Therefore, the low scores onsome nonlanguage tests were attributed to interfer-ence from the language impairment. PPA patientsshowed less impairment in CERAD Word List recog-
nition, Visual Target Cancellation, Judgment of LineOrientation, and Visual-Verbal, representing tests ofmemory, visuospatial functions, and reasoning andexecutive functions, respectively. Normal controlsshowed no impairments on any of the neuropsycho-logical tests. Scores on a subset of the language andnonlanguage neuropsychological tests for both groupsare shown in Table 4.
Task PerformancePatients with PPA (n � 10 for HOM and n � 11 forSYN) showed significantly increased reaction timeswhen compared with the normal control group (n �11) for both phonological (HOM; PPAHOM �2,209 � 360 milliseconds vs NLHOM � 1,714 � 423milliseconds; p � 0.05) and semantic (SYN; PPASYN
� 2,596 � 430 milliseconds vs NLSYN � 1,792 �513 milliseconds; p � 0.001) tasks. Accuracy also wasreduced significantly for PPAs on both phonological(PPAHOM � 0.84 � 0.11 vs NLHOM � 0.96 � 0.04;p � 0.05) and semantic (PPASYN � 0.87 � 0.11 vsNLSYN � 0.97 � 0.03; p � 0.01) tasks comparedwith normal subjects. However, scores were signifi-cantly greater than chance for all patients.
On the letter strings control task, reaction timeswere comparable for the two groups (PPASTR �2,746 � 326 milliseconds vs NLSTR � 2,678 � 411milliseconds; p � 0.05). Accuracy on the control task
Table 4. Neuropsychological Scores for PPA and Normal Subject Groups
SubjectGroup
Age/Gender
Language General
WAB orBDAE
(% correct)*BNT(60)
CategoryFluency
(animals)
LexicalFluency(FAS)
MMSE(30)
Word ListRecog.(10)
Trails A(secs)
JLO(% correct)
PPA 69/F 96 52 13 23 27 10 n/a n/a62/M 87 55 15 30 20 10 n/a 8767/F 94.40 22 8 17 25 10 n/a 7357/M 80.50 9 12 12 26 10 37 10059/M 100 36 18 12 23 10 44 10067/M 86.10 31 11 21 21 10 47 8767/M 100 55 15 17 n/a n/a 46 n/a58/F 84.50 51 13 11 29 10 35 7365/F 96.50 34 8 8 22 10 76 6771/F 96 53 14 17 28 10 45 7765/F 100 55 12 13 30 10 46 87
NL (n � 9),mean � SD
—a 58 � 2.4 24.2 � 3.4 45.4 � 7.4 29.6 � 0.7 10 39.7 � 16 81 � 17%
*Underlined scores were from the BDAE, others from the WAB.Boldface scores are greater than 1 SD from the mean score for normal subjects.aNormal data not available.
PPA � primary progressive aphasia; WAB � Western Aphasia Battery (auditory comprehension); BDAE � Boston Diagnostic Aphasia Ex-amination–auditory comprehension (indicated by underlines in row one); BNT � Boston Naming Test, MMSE � Mini-Mental Status Exam;Word List Recog. � CERAD (Consortium to Establish a Registry for Alzheimer’s Disease) Word List Recognition; Trails A � TrailmakingTest A; JLO � Judgment of Line Orientation; n/a � not available at time of scanning.
40 Annals of Neurology Vol 53 No 1 January 2003

was slightly reduced for the PPA group relative to thenormal group (PPASTR � 0.97 � 0.04 vs NLSTR �0.99 � 0.02; p � 0.05). However, PPA patients weresignificantly more accurate on the STRINGS task thanon either of the language tasks (p � 0.05 vs each task).Reaction times and accuracy for the two groups on allthree tasks are shown in Figure 2.
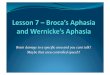
Voxel-Based Morphometry ResultsAnalysis of gray matter density of the structural MRIsshowed an area of reduced gray matter in PPA patients(n � 11) compared with normal subjects (n � 11)spanning the posterior perisylvian temporal and infe-rior parietal lobes (Fig 3a). Voxels with significantlyreduced gray matter for the group of PPA patientscompared with controls were found in the left inferiorparietal lobule, and in the left superior temporal gyrus.An examination of gray matter density in these regionsfor each of the individual subjects is shown in Figure 4.
The coordinates and corresponding p values for the sig-nificant voxels are listed in Table 5.
The fluent and nonfluent PPA groups showed some-what different patterns of atrophy when comparedwith controls. The nonfluent patients showed inferopa-rietal and dorsolateral prefrontal cortex reduced graymatter (xyz � �62 �42 27, p � 0.002; xyz � �50�46 48, p � 0.003; and xyz � �49 11 50, p �0.003), whereas fluent patients showed nonsignificantsuperior temporal gray matter reduction (xyz � �70�19 4; p � 0.11). However, there was no significantdifference in the pattern of atrophy when directly com-paring the nonfluent and fluent PPA groups.
ROI analyses of fluency, based on the areas listed inTable 5, showed a trend toward reduced gray matter innonfluent compared with fluent subjects in the moresuperior and medial of the inferior parietal lobule foci(xyz � �62 �43 37; p � 0.061; see Fig 4). Simpleregression analysis of BNT scores versus whole-braingray matter density showed no significant correlationbetween naming deficit and atrophy. Moreover, noneof the three regions in the inferior parietal lobule orsuperior temporal gyrus (see Table 5) was found to sig-nificantly correlate with BNT on ROI analysis.
Functional Magnetic Resonance Imaging Results:Homonym versus Letter StringsFor the homonym task relative to the control task(HOM � STRINGS), both PPA patient (n � 10) andcontrol (n � 11) subject groups activated a commonnetwork of areas, including the “classic” left perisylvianfrontal and temporal language areas. These activationsincluded the left inferior frontal gyrus (ie, Broca’s area,broadly defined as including BA 44/45/46), left poste-rior middle temporal gyrus (ie, Wernicke’s area � BA22/37), and the anterior cingulate gyrus (BA 32). ThePPA patient group showed an additional activation inthe left middle frontal gyrus. Phonological activationsfor both groups are shown in Figure 3b and c andlisted in Table 6.
Synonym versus Letter StringsFor the synonym task relative to the control task(SYN � STRINGS), activations in the control group(n � 11) included bilateral inferior frontal gyri (BA44/45), bilateral superior temporal sulci (BA 21/22),and the left temporoparietal junction. Activations notquite meeting threshold were seen in the left anteriorcingulate gyrus and right insula (see Fig 3d and Ta-ble 6).
The PPA group (n � 11) appeared to activate a sub-set of the regions seen in the normal group for theSYN � STRINGS contrast. These regions were bilat-eral inferior frontal gyri (BA 44/45), anterior cingulategyrus (BA 32), left intraparietal sulcus, and right in-sula. The left posterior superior temporal sulcus was
Fig 2. Task performance results. (a) Reaction times (millisec-onds) and (b) accuracy (percentage) scores for the PPA patients(shaded bars) and normal subjects (unshaded bars) for thethree task conditions. Significant differences (p � 0.05) be-tween the two groups are indicated by asterisks. Error barsrepresent standard error of the mean for each group.
Sonty et al: Language Network Changes 41

Fig 3. Voxel-based morphometry (VBM) and functional magnetic resonance imaging (fMRI) results. (a) VBM results showing sig-nificant gray matter density decreases for the primary progressive aphasia (PPA) group in the left superior temporal gyrus and leftinferior parietal lobule (iPL). Representative fMRI activations: (b) normal group homonym task (HOM; n � 11), (c) PPA HOM(n � 10), (d) normal synonym (SYN; n � 11), (e) PPA SYN (n � 11). The cerebellar activation is not pictured. Areas of signif-icant activation for PPA � control in (f) phonology (HOM) and (g) semantics (SYN) include intraparietal sulcus (iPS), fusiformgyrus (Fus), and precentral gyrus (prCG). No areas of significant activation for control � PPA were present for either task. iFG �inferior frontal gyrus; mFG � middle frontal gyrus; mTG � posterior middle temporal gyrus; aCG � anterior cingulate gyrus;TPJ � temporoparietal junction; iPS � intraparietal sulcus; sTS � superior temporal sulcus; sTG � superior temporal gyrus;Lt � left; Rt � right; Thal � thalamus; lns � insula; pCG � posterior cingulate gyrus.
42 Annals of Neurology Vol 53 No 1 January 2003

slightly below threshold (p � 0.055). An additionalarea of activation included the right cerebellum. Theseactivations are shown in Figure 3e and are listed inTable 6.
Areas of Significant Difference between SubjectGroups: Primary Progressive Aphasia versus ControlsDirect intergroup comparison showed several areas ofgreater task-related activation in the PPA subject grouprelative to the normal control group. For the homonymgroup-by-task interaction (HOMPPA � STRINGSPPA)versus (HOMNL � STRINGSNL), the PPA groupshowed foci of significantly increased activation in rightfusiform gyrus and left intraparietal sulcus, with theright intraparietal sulcus showing a trend toward signif-
icance (see Fig 3f and Table 7). The synonym group-by-task interaction (SYNPPA � STRINGSPPA) versus(SYNNL � STRINGSNL) showed activations in rightfusiform gyrus, left and right precentral gyri, and leftintraparietal sulcus in PPA patients (see Fig 3g and Ta-ble 7).
The control subjects showed no areas of significantlyincreased activation relative to the PPA patient group,although one focus in the left temporoparietal junction(xyz � �42 �63 18) showed a trend toward signifi-cance for the synonym task (p � 0.07).
Masking the intergroup contrasts provided infor-mation about signal increases or decreases in eachgroup. Masking the HOM � STRINGS contrast(PPAHOM � PPASTRINGS) � (NLHOM � NLSTRINGS)by PPAHOM � PPASTRINGS showed that PPA patientssignificantly activated the right fusiform gyrus. Mask-ing the same contrast by NLSTRINGS � NLHOM
showed that normal subjects significantly deactivatedthe right fusiform gyrus and left intraparietal sulcus.For the accordingly masked SYN � STRINGS con-trast, the only areas significantly activated in PPA pa-tients were right fusiform gyrus and left precentral gy-rus, whereas areas significantly deactivated in thenormal subjects included right fusiform gyrus, left in-traparietal sulcus, and right precentral gyrus.
The plot of parameter estimates, shown in Figure 5,demonstrates that both subject groups showed task-related activations in Broca’s and Wernicke’s areas; thatis, the parameter estimates were consistent with greateractivation for the language tasks (HOM or SYN) ver-sus the control task (STRINGS). The situation wasquite different in the areas that differentiated PPAs andcontrols. In these areas, the normal subjects displayeddeactivations when language tasks were compared withletter strings, whereas PPA patients showed relative ac-tivations. Neither whole-brain analyses nor region ofinterest analyses in areas of significant intergroup dif-ference showed any effect for fluency on activation in-creases for either of the tasks. However, in a ROI anal-ysis, signal in right fusiform regions for HOM �STRINGS and SYN � STRINGS showed significantinverse correlation with BNT (r � �0.57 and �0.64,respectively; p � 0.05 after correction for multiplecomparisons), as did signal in right precentral gyrus forthe SYN � STRINGS contrast (r � �0.70; p �0.05). Signal in left intraparietal sulcus showed a trendtoward inverse correlation with BNT (r � �0.51; p �0.055). Plots of signal in these regions for the individ-ual subjects versus BNT score are shown in Figure 6.Linear regressions between signal in each of the areasshowing anomalous activations in PPA (dependentvariable) and task performance (independent variable)showed different relationships between PPA patientsand normal control subjects (Fig 7). Activity in rightfusiform gyrus in the HOM � STRINGS contrast was
Fig 4. Individual regional voxel-based morphometry (VBM)gray matter density values for primary progressive aphasia(PPA) and normal control groups. PPA patients showed ana-tomical involvement in all three regions relative to the normalcontrol group. Although fluency showed a trend towards corre-lation with atrophy in the left inferior parietal lobule, thedifference was not significant, probably because of the presenceof outliers and the relatively small sample sizes. L IPL � leftinferior parietal lobule (medial/lateral), L STG � left supe-rior temporal gyrus. (circles) Nonfluent PPA; (crosses) fluentPPA; (triangles) normal control; (horizontal lines) meanvalue for each subject group.
Table 5. VBM Results (Normal — PPA)
Region XYZmm Zscore Pcorrected
Left superior temporalgyrus
�68 �18 6 4.47 0.047
Left inferior parietallobule
�62 �43 37 4.91 0.009
�50 �46 48 4.71 0.019
VBM � voxel-based morphometry; PPA � primary progressiveaphasia.
Sonty et al: Language Network Changes 43

found to predict both reaction time and task accuracyon the HOM task only for the PPA subject group,with increased activity correlated with longer reactiontimes and reduced accuracy (p � 0.023 and 0.025,respectively).
Increased signal in left precentral gyrus for theSYN � STRINGS contrast was found to be associatedwith reduced task accuracy on the SYN task (p �0.038), again, only for the PPA group (Fig 8). No sig-nificant relationships were found between signal andtask performance in the normal control group for ei-ther task. No other correlations between anomalouslyactivated regions in the PPA group and performancewere found. All p values were corrected for multiplecomparisons across the correlations.
DiscussionThis report examines the neuroanatomical and func-tional substrates of PPA in a group of patients withword-finding deficits and relatively preserved compre-hension. The neural substrates for language alterationsin this group of PPA patients with its particular con-stellation of clinical features were studied using behav-ioral measures, VBM, and fMRI. Statistical compari-sons were made using random effects analyses, whichaccount for intersubject variance. This type of analysisis less susceptible to the presence of outliers. Thus, thefindings represent effects over the group of PPA pa-tients as a whole. The relative homogeneity of the find-ings also was demonstrated by examining the parame-ter estimates for the PPA and normal groups for boththe VBM and functional activation results (see Figs 4and 5).
We found that the PPA patients were slower and lessaccurate than normal subjects in the language-relatedportions of the tasks but performed nearly equivalentlyto normal subjects on a demanding control task.Therefore, we propose that the changes in activationthat we observed in the PPA patients appear to reflectspecific changes in language function rather than anygeneralized slowing of behavior or an inability to un-derstand the task requirements. Although our group ofPPA patients demonstrated relatively intact compre-hension for conversational speech on clinical testing,they were impaired on the synonym task, a task that isquite challenging because of its rapid pace and lack ofcontextual cues.
VBM demonstrated areas of significant gray matterdensity reduction for the group of PPA patients in thesuperior temporal gyrus and the inferior parietal lobulein the left hemisphere (see Figs 3a and 4). This pattern
Table 6. Coordinates for Regions of Task-Related Activation for Each Subject Group
Location
HOM—STRINGS SYN—STRINGS
Normals (n � 11) PPA (n � 10) Normals (n � 11) PPA (n � 11)
xyzmm pcorr xyzmm pcorr xyzmm pcorr xyzmm pcorr
Left iFG �45 54 �9 3.7e-13 �48 42 �15 0.000 �45 39 �12 0.008 �39 33 �15 0.000Left mFG �42 6 36 0.01Left posterior mTG �51 �45 0 1.4e-05 �57 �45 �3 0.002Left aCG �9 51 39 1.8e-06 �3 27 36 0.006 �6 21 39 0.054 �3 30 36 1.4e-04Left TPJ �39 �60 24 0.000Left iPS �42 �69 30 0.036 �42 �57 42 4.7e-09Right iFG 42 33 �15 8.3e-07 57 30 �6 5.8e-05Right Insula 45 �9 15 0.193 39 �15 6 0.003Bilateral sTS �45 �27 0 0.007 �57 �39 0 0.551
51 �24 �3 4.0e-10Right cerebellum 21 �78 �30 2.0e-04
Activations are significant at p � 0.05 corrected, unless italicized.PPA � primary progressive aphasia; iFG � inferior frontal gyrus; mFG � middle frontal gyrus; mTG � posterior middle temporal gyrus;aCG � anterior cingulate gyrus; TPJ � temporoparietal junction, iPS � intraparietal sulcus, sTS � superior temporal sulcus.
Table 7. Coordinates for Regions of Significant Differencebetween the PPA and Control Groups for Each Task
Region RegionCoordinates
(XYZmm) pcorrected
HOM(PPA-NL)
Right fusiformgyrus
30 �54 �21 0.005
Left intraparietalsulcus
�27 �57 51 0.020
Right intraparietalsulcus
39 �51 60 0.056
SYN(PPA-NL)
Left precentralgyrus
�54 3 15 0.011
Right precentralgyrus
51 3 21 0.035
Right fusiformgyrus
27 �69 �18 0.001
Left intraparietalsulcus
�27 �60 54 0.041
Activations are significant at p � 0.05 corrected, unless italicized.PPA � primary progressive aphasia.
44 Annals of Neurology Vol 53 No 1 January 2003

is consistent with previous computerized tomographyand MRI studies of atrophy in PPA.19–21 However,the pattern is distinct from that reported in VBM stud-ies of semantic dementia, in which the combination offluent aphasia and comprehension deficits were associ-ated with bilateral temporopolar and inferofrontal at-rophy.26,27 We did not observe significant effects offluent versus nonfluent patient subtype or naming def-icit severity on the whole-brain or ROI-based morpho-metric analyses of PPAs or controls. However, the ab-sence of a significant clinical–anatomical relationship
in this study may have reflected the low power to de-tect such a relationship given the relatively small sam-ple size of each patient fluency subgroup (n � 3 forfluent and n � 8 for nonfluent).
During fMRI, language-related activations in thenormal subject group were consistent with those re-ported in the literature.52–56 For the phonological(HOM) task, these activations included left-sided infe-rior frontal and posterior temporal regions within thetraditional boundaries of “Broca’s” and “Wernicke’s”areas and surrounding regions, as well as the anteriorcingulate gyrus. These areas have been implicated pre-viously in phonological analysis,54 and response selec-tion.53 The semantic processing task additionally dem-onstrated left-sided inferior parietal and left anteriortemporal activations, as well as right-sided activationsin inferior frontal, anterior insular, and superior tem-poral regions, areas that have been implicated in access-ing word meaning.52,55,57
Despite their somewhat reduced performance on thelanguage tasks, the PPA subject group activated verysimilar left hemisphere areas as the normal subjects inboth tasks. Contrary to expectations, PPA-relatedfMRI abnormalities also were detected outside of thecanonical language areas and took the form of excessiverather than diminished activations, as determined bymasking with the relevant language task versus letterstring contrast (see Fig 3f and g). In the homonym taskversus letter string contrast, the PPA group showedgreater activation than the normal group in the left in-traparietal sulcus and right fusiform gyrus, whereas inthe synonym task versus letter string contrast, the PPAgroup showed greater activation in bilateral precentralgyri, left intraparietal sulcus, and right fusiform gyrus.This combination of findings deviates notably fromlanguage-related functional imaging findings in seman-tic dementia. In that disorder, bilateral temporopolaratrophy was associated with significantly reduced activ-ity in regions distant to the areas of atrophy.26 How-ever, the two patient groups (PPA patients in this studyand those with semantic dementia) differ fundamen-tally from each other in that the progressive aphasiapatients had minimal deficits in single-word compre-hension, whereas impaired comprehension is a hall-mark feature of semantic dementia.12 One similarity inthe activations for the semantic task in this study andthe one used by Mummery and colleagues (1999) isthat both patient groups showed abnormally increasedactivity in left precentral gyrus.26 The aberrant activa-tions shown in Figure 3 are based on contrasting thePPA with the normal group. The areas of abnormalitytherefore represent either excessive neuronal recruit-ment or defective inhibition in the PPA group. Fur-thermore, either possibility could arise from an abnor-mal neural response to either the language task or tothe letter-string control task. The latter possibility (ie,
Fig 5. Individual fMRI responses for (a) phonology (HOM �STRINGS) and (b) semantics (SYN � STRINGS) at Broca’sarea (Broca), Wernicke’s area (Wernicke), and regions of sig-nificant and subthreshold activation for PPAs greater thancontrols for both tasks. PPA patients activated Broca’s andWernicke’s areas to an equivalent degree as the normal controlsubjects, and also showed increased activations in several non-language regions. There was no clear relationship between pa-tient fluency and activity in these regions. Key: L iPS � leftintra-parietal sulcus; R iPS � right intra-parietal sulcus; RFus � right fusiform gyrus; L prCG � left precentral gyrus;R prCG � right precentral gyrus; (circles) Nonfluent PPA;(crosses) fluent PPA; (triangles) normal control.
Sonty et al: Language Network Changes 45

that the PPA-related differences result from aberrantresponses to the letter strings task) is unlikely becausePPA patients demonstrated intact performance, compa-rable to that of the normal subject group, in the letter-string task. However, this alternative explanation needsto be addressed more directly with the help of event-related task designs. The distribution of neuronal ac-tivity in response to a cognitive task, including lan-guage, reflects a complex pattern of excitations andinhibitions.58 Figure 5 indicates that normal subjectsshowed deactivations in areas where PPA subjects hadaberrant task-related activity. Thus, the abnormality inPPA appears to represent a failure to inhibit activationsoutside of the language network in a task-related man-ner. This abnormality could reflect either impaired in-hibitory control emanating from the atrophic areas orfrom the compensatory recruitment of additional areasdue to dysfunction within the language network. Notethat the classic language areas responded to languagetasks with nearly equivalent activations in both PPApatients and normal subjects (see Fig 4). Moreover, in-creased activity in nonlanguage regions appeared tocorrelate with longer reaction times and reduced taskaccuracy for the PPA subject group, but not for thenormal control group (see Figs 7 and 8). These resultsmay indicate that the functional involvement of theseregions did not enhance performance in the tasks, andthat activity in these regions might potentially interferewith language processing and task performance. Activ-ity in nonlanguage regions furthermore was related toincreased naming deficit severity (see Fig 6), illustratingthe relevance of abnormal fMRI activations to clinicalfeatures of the aphasia. Functional activation in poste-rior parietal regions is seen primarily in attentionaltasks, including tasks of verbal working memory.42,59
The increased activation in the left intraparietal sulcusin PPA therefore could also reflect increased task-related attentional or working memory demands arisingfrom the decreased efficiency of the language network.In normal subjects, word reading is a highly learned,automatic task. In PPA, this process may lose its auto-maticity and may become increasingly more dependenton laborious grapheme-to-phoneme transformations,such as those that are necessary for reading unfamiliarpseudowords.
Š Fig 6. Boston Naming Test (BNT) score versus regional fMRIresponse for PPA patients: a) right fusiform gyrus for (HOM �STRINGS), n � 10; and b) right fusiform gyrus, c) rightprecentral gyrus, and d) left intra-parietal sulcus for (SYN �STRINGS) n � 11. PPA patients showed significant relation-ships between fMRI responses and naming deficit severity inthese regions of anomalous activation. r � Pearson’s linearcorrelation coefficient; R Fus � right fusiform gyrus; r prCG� right precentral gyrus; L iPS � left intraparietal sulcus.
46 Annals of Neurology Vol 53 No 1 January 2003

Fiez and Petersen suggested that primary motor cor-tex participates in the transformation from phonologi-cal to articulatory representations.54 Furthermore, acti-vation in left precentral gyrus has been seen in normalsubjects and adult dyslexic patients readingpseudowords.60,61 Lexical decision tasks involvingpseudowords also have shown greater activity in leftprecentral gyrus than tasks of word reading or featuredetection.57 A recent event-related study of word–pseudoword processing in a lexical decision task hasshown activation of the left ventral precentral sulcusfor pseudowords when compared with commonwords.62 These findings support the contention that
the aberrant precentral area of activity seen in PPAmay reflect an altered approach to the task so thatwords require more intensive processing as if they werepseudowords.
In summary, a comparison of word reading to letterstring identification tasks showed aberrant activationsin PPA at sites that are not typically activated by nor-mal subjects performing the same tasks. The magni-tude of these aberrant activations was correlated withtask performance during the imaging session as well aswith scores on the BNT. These aberrant activation sitescould reflect either the emergence of compensatoryneuronal strategies for language processing or the dis-integration of neuronal pathways, which normally in-hibit the spread of neural activity to areas outside ofthe relevant network. The areas of PPA-related atro-phy, mostly confined to the left temporoparietal re-gion, did not show abnormal activations or deactiva-tions in this set of tasks, indicating that the residualneurons in atrophic areas maintain at least some oftheir premorbid response characteristics.
This work was supported by the Howard Hughes Medical Institute(S.P.S.), the Illinois Department of Public Health Alzheimer’s Dis-ease Research Fund Early Researcher Award (S.P.S), the RubensteinFoundation, the Thomas E. Tuft Fund for PPA Research (M.M.),the National Institute on Aging (AG00940, D.R.G.), and theNorthwestern Alzheimer’s Disease Center funded by the NIA(AG13854, M.M.).
Fig 7. Interaction between subject group and regional fMRIresponse versus (HOM � STRINGS) task performance: a)right fusiform response (HOM � STRINGS) versus HOMreaction time; b) right fusiform response (HOM - strings) ver-sus HOM percent accuracy for PPA (n � 10) and normalcontrol (n � 11) groups. Both regressions for the PPA groupare significant at the p � � 0.05 level, while regressions forthe normal control group are not significant, indicating adisease-specific relationship between activation in these regionsand language function. r � Pearson’s linear correlation coeffi-cient; R Fus � right fusiform.
Fig 8. Interaction between subject group and regional fMRIresponse (SYN � STRINGS) versus SYN task performance(accuracy) for PPA and control groups (n � 11 for bothgroups). The regression for the PPA group is significant at thep � � 0.05 level, while the regression for the normal controlgroup is not significant, illustrating the disease specificity ofthe relationship between activation in these regions and lan-guage function. r � Pearson’s linear correlation coefficient; LprCG � left precentral gyrus.
Sonty et al: Language Network Changes 47

References1. Mesulam M-M. Slowly progressive aphasia without generalized
dementia. Ann Neurol 1982;11:592–598.2. Mesulam M-M, Weintraub S. Spectrum of primary progressive
aphasia. In: Rossor MN, ed. Unusual dementias. London: Bail-liere Tindall, 1992:583–609.
3. Weintraub S, Rubin NP, Mesulam M-M. Primary progressiveaphasia. Longitudinal course, neuropsychological profile, andlanguage features. Arch Neurol 1990;47:1329–1335.
4. Mesulam M-M. Primary progressive aphasia. Ann Neurol 2001;49:425–432.
5. Pick A. Uber die Beziehungen der senilen Hirnatrophie zurAphasie. Prager Med Wochenschr 1892;17:165–167.
6. Serieux P. Sur un cas de surdite verbale pure. Rev Med 1893;13:733–750.
7. Dejerine J, Serieux P. Un cas de surdite verbale pure termineepar aphasie sensorielle, suivie d’autopsie. C R Seances Soc BiolFil 1897;49:1074–1077.
8. Franceschi F. Gliosi perivasculare in un caso de demenza afa-sica. Annali di Neurologia 1908;26:281–290.
9. Rosenfeld M. Die partielle Grosshirnatrophie. J Psychol Neurol1909;14:115–130.
10. Warrington EK. The selective impairment of semantic memory.Q J Exp Psychol 1975;27:635–657.
11. Snowden JS, Goulding PJ, Neary D. Semantic dementia: aform of circumscribed cerebral atrophy. Behav Neurol 1989;2:167–182.
12. Hodges JR, Patterson K, Oxbury S, Funnell E. Semanticdementia: progressive fluent aphasia with temporal lobe atro-phy. Brain 1992;115:1783–1806.
13. Neary D, Snowden J, Gustafson L, et al. Frontotemporal lobardegeneration: a consensus on clinical diagnostic criteria. Neu-rology 1998;51:1546–1554.
14. Harasty JA, Halliday GM, Kril JJ, Code C. Specific temporopa-rietal gyral atrophy reflects the pattern of language dissolutionin Alzheimer’s disease. Brain 1999;122:675–686.
15. Turner RS, Kenyon LC, Trojanowski JQ, et al. Clinical, neu-roimaging, and pathologic features of progressive nonfluentaphasia. Ann Neurol 1996;39:166–173.
16. Chin SS-M, Goldman JE, Devenand DR, et al. Thalamic de-generation presenting as primary progressive aphasia. BrainPathol 1994;4:515.
17. Galton CJ, Patterson KE, Xuereb JH, Hodges JR. Atypical andtypical presentations of Alzheimer’s disease: a clinical, neuroim-aging, and pathological study of 13 cases. Brain 2000;123:484–498.
18. Kertesz A, Hudson L, MacKenzie IRA, Munoz DG. The pa-thology and nosology of primary progressive aphasia. Neurology1994;44:2065–2072.
19. Abe K, Ukita H, Yanagihara T. Imaging in primary progressiveaphasia. Neuroradiology 1997;39:556–559.
20. Sinnathamby R, Antoun NA, Freer CEL, et al. Neuroradiologi-cal findings in primary progressive aphasia: CT, MRI and ce-rebral perfusion SPECT. Neuroradiology 1996;38:232–238.
21. Westbury C, Bub D. Primary progressive aphasia: a review of112 cases. Brain Lang 1997;60:381–406.
22. Chawluk JB, Mesulam M-M, Hurtig H, et al. Slowly progres-sive aphasia without generalized dementia: studies with positronemission tomography. Ann Neurol 1986;19:68–74.
23. Tyrrell PJ, Warrington EK, Frackowiak RSJ, Rossor MN. Het-erogeneity in progressive aphasia due to focal cortical atrophy.Brain 1990;113:1321–1336.
24. Kempler D, Metter EJ, Riege WH, et al. Slowly progressiveaphasia: three cases with language, memory, CT and PET data.J Neurol Neurosurg Psychiatry 1990;53:987–993.
25. Grabowski TJ, Damasio H, Anderson SW. Physiologic corre-lates of defective word retrieval in progressive anomic aphasia.Soc Neurosci Abstr 1997;23:416.
26. Mummery CJ, Patterson K, Wise RJS, et al. Disrupted tempo-ral lobe connections in semantic dementia. Brain 1999;122:61–73.
27. Mummery CJ, Patterson K, Price CJ, et al. A voxel-based mor-phometry study of semantic dementia: relationship betweentemporal lobe atrophy and semantic memory. Ann Neurol2000;47:36–45.
28. Gitelman DR, Nobre AC, Sonty S, et al. Phonological and se-mantic activations in primary progressive aphasia. NeuroImage2000;11:S122.
29. Goodglass H, Kaplan EF. The Boston Diagnostic Aphasia Ex-amination. Philadelphia: Lea and Febiger, 1983.
30. Oldfield RC. The assessment of analysis of handedness: the Ed-inburgh inventory. Neuropsychologia 1971;9:97–113.
31. Kertesz A. Western aphasia battery (WAB). San Antonio, TX:The Psychological Corporation, 1982.
32. Kaplan E, Goodglass H, Weintraub S. The Boston NamingTest. Philadelphia: Lea and Febiger, 1983.
33. Spreen O, Benton A. Neurosensory Center Comprehensive Ex-amination for Aphasia. Victoria, BC: Neuropsychological Lab-oratory, Department of Psychology, University of Victoria,1969.
34. Spreen O, Benton A. Neurosensory Center Comprehensive Ex-amination for Aphasia (NCCEA) Rev ed. Victoria, BritishColumbia: University of Victoria, Neuropsychology Laboratory,1977.
35. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. Apractical method for grading the cognitive state of patients forthe clinician. J Psychiatr Res 1975;12:189–198.
36. Morris JC, Edland S, Clark C, et al. The Consortium to Es-tablish a Registry for Alzheimer’s Disease (CERAD). Part IV.Rates of cognitive change in the longitudinal assessmentof probable Alzheimer’s disease. Neurology 1993;43:2457–2465.
37. Benton A, Hamsher KdS, Varney N, Speen O. Contributionsto neuropsychological assessment. 2nd ed. New York: OxfordUniversity Press, 1998.
38. Halstead W. Brain and intelligence. Chicago: University ofChicago Press, 1947.
39. Yesavage JA, Brink TL, Rose TL, et al. Development and val-idation of a geriatric depression screening scale: a preliminaryreport. J Psychiatr Res 1983;17:37–49.
40. Kucera H, Francis WN. Computational analysis of present-dayAmerican English. Providence, RI: Brown University Press,1967.
41. Parrish TB, Gitelman DR, Kim Y-H, et al. Clinical fMRI: ispatient motion really an issue? NeuroImage 1998;7:S560.
42. Gitelman DR, Nobre AC, Parrish T, et al. A large-scale distrib-uted network for covert spatial attention: further anatomical de-lineation based on stringent behavioral and cognitive controls.Brain 1999;122:1093–1106.
43. Friston KJ, Ashburner J, Frith CD, et al. Spatial registrationand normalization of images. Hum Brain Mapp 1995;3:165–189.
44. Friston KJ, Holmes AP, Worsley KJ, et al. Statistical parametricmaps in functional imaging: a general linear approach. HumBrain Mapp 1995;2:189–210.
45. Friston KJ, Holmes A, Poline J-B, et al. Detecting activationsin PET and fMRI: levels of inference and power. NeuroImage1996;4:223–235.
46. Worsley KJ, Marrett S, Neelin P, et al. A unified statisticalapproach for determining significant signals in images of cere-bral activation. Hum Brain Mapp 1996;4:58–73.
48 Annals of Neurology Vol 53 No 1 January 2003

47. Talairach J, Tournoux P. Co-planar stereotaxic atlas of the hu-man brain. New York: Thieme Medical Publishers, 1988.
48. Moore CJ, Price CJ. A functional neuroimaging study of thevariables that generate category-specific object processing differ-ences. Brain 1999;122:943–962.
49. Gitelman DR, Ashburner J, Friston KJ, et al. Voxel-based mor-phometry of herpes simplex encephalitis. NeuroImage 2001;13:623–631.
50. Ashburner J, Friston KJ. Voxel-based morphometry—the meth-ods. NeuroImage 2000;11:805–821.
51. Evans AC, Kamber M, Collins DL, MacDonald D. An MRI-based probabilistic atlas of neuroanatomy. In: Shorvon S, FishD, Andermann F, et al., eds. Magnetic resonance scanning andepilepsy. NATO ASI Series A, Life Sciences. Vol 264. NewYork: Plenum Press, 1994:263–274.
52. Demonet JF, Chollet F, Ramsay S, et al. The anatomy of pho-nological and semantic processing in normal subjects. Brain1992;115:1753–1768.
53. Petersen SE, Fiez JA. The processing of single words studiedwith positron emission tomography. Annu Rev Neurosci 1993;16:509–530.
54. Fiez JA, Petersen SE. Neuroimaging studies of word reading.Proc Natl Acad Sci USA 1998;95:914–921.
55. Price CJ. The anatomy of language: contributions from func-tional neuroimaging. J Anat 2000;197:335–359.
56. Price CJ, Wise RJ, Frackowiak RS. Demonstrating the implicitprocessing of visually presented words and pseudowords. CerebCortex 1996;6:62–70.
57. Price CJ, Wise RJ, Watson JD, et al. Brain activity during read-ing—the effects of exposure duration and task. Brain 1994;117:1255–1269.
58. Binder JR, Price CJ. Functional neuroimaging of language. In:Cabeza R, Kingstone A, eds. Handbook of functional neuroim-aging of cognition. Cambridge, UK: The MIT Press, 2001:187–252.
59. LaBar KS, Gitelman DR, Parrish TB, et al. Overlap of fronto-parietal activations during covert spatial attention and verbalworking memory in the same set of subjects: an fMRI study.Soc Neurosci Abstr 1998;24:1896.
60. Brunswick N, McCrory E, Price CJ, et al. Explicit and implicitprocessing of words and pseudowords by adult developmentaldyslexics: a search for Wernicke’s Wortschatz? Brain 1999;122:1901–1917.
62. Paulesu E, Demonet JF, Fazio F, et al. Dyslexia: culturaldiversity and biological unity. Science 2001;291:2165–2167.
63. Binder JR, McKiernan KA, Parsons MW, et al. The neural cor-relates of semantic processing: an event-related fMRI study.NeuroImage 2001;13:S507.
Sonty et al: Language Network Changes 49