Embed Size (px)
Citation preview

Prevention of the Acute Respiratory
Distress Syndrome
Patient Engagement, Systems Science, and the Elimination of Preventable Harm
Daniel Talmor M.D., M.P.H.
Anesthesia, Critical Care and Pain Medicine

Acute Respiratory Distress Syndrome
Ware and Mathay, NEJM 2001

ARDS Research
• Despite improved understanding of ARDS, the clinical
impact has been limited to improvements in supportive
treatment
– Mechanical ventilation, fluid management, sedation,
rehabilitation
– Mechanistic treatments uniformly negative
• When applied late in the course of illness?
• Surprisingly little research has been done on the
prevention of ARDS

Potentially Preventable Complications of
Critical Illness
• Stress ulcer bleeding
• Pulmonary embolism
• Ventilator associated pneumonia
• Nosocomial infections
Why not ARDS?

ALI : “Multiple hit” Hypothesis

What can we do?
Not Modifiable
• Age
• Restrictive lung disease
• Pneumonia
• Trauma
• Sepsis
• Increasing ASA score
• Initial P/F ratio
• Acidemia
Modifiable
• Transfusion
• Positive net fluid
balance
• Delayed resuscitation
• Aspiration
• Disynchrony
• Injurious ventilation

Li et al AJRCCM 2011

ARDS in Olmstead County
Li et al AJRCCM 2011

Community-Acquired ARDS Hospital-Acquired ARDS
Li et al AJRCCM 2011
ARDS in Olmstead County

AJRCCM 2010
Barriers to Prevention of ARDS
• Need to identify those at high risk for ARDS
early during their hospital presentation.
• Under-utilization and practice variation in
clinical practices that may influence
development and outcome of ARDS.
• Lack of safe and effective pharmacologic
therapies to prevent ARDS.

Mount Sinai School of Medicine
Temple University School of Medicine
The Johns Hopkins University
University of Medicine and Dentistry of New Jersey
Denver Health Medical Center
Hospital of the University of Pennsylvania
Brigham and Women's Hospital
Mayo Clinic Rochester
U of Michigan University Hospital
University of Washington, Harborview Medical Center
Parkland Health and Hospital System Dallas, Texas
University of Illinois at Chicago
Wake Forest University Health Sciences
Mayo Clinic Jacksonville
Bridgeport Hospital, Yale New Haven Health
Massachusetts General Hospital
Akdeniz University Hospital, Turkey
Beth Israel Deaconess Medical Center
Miami Valley Hospital
Emory University, Atlanta
Uludag University School of Medicine, Turkey
University of Missouri - Columbia
• The first USCIIT Group
study in 22 hospitals who
joined USCIITG-LIPS1.
• Researchers in emergency
medicine, trauma surgery,
anesthesiology and
pulmonary medicine.
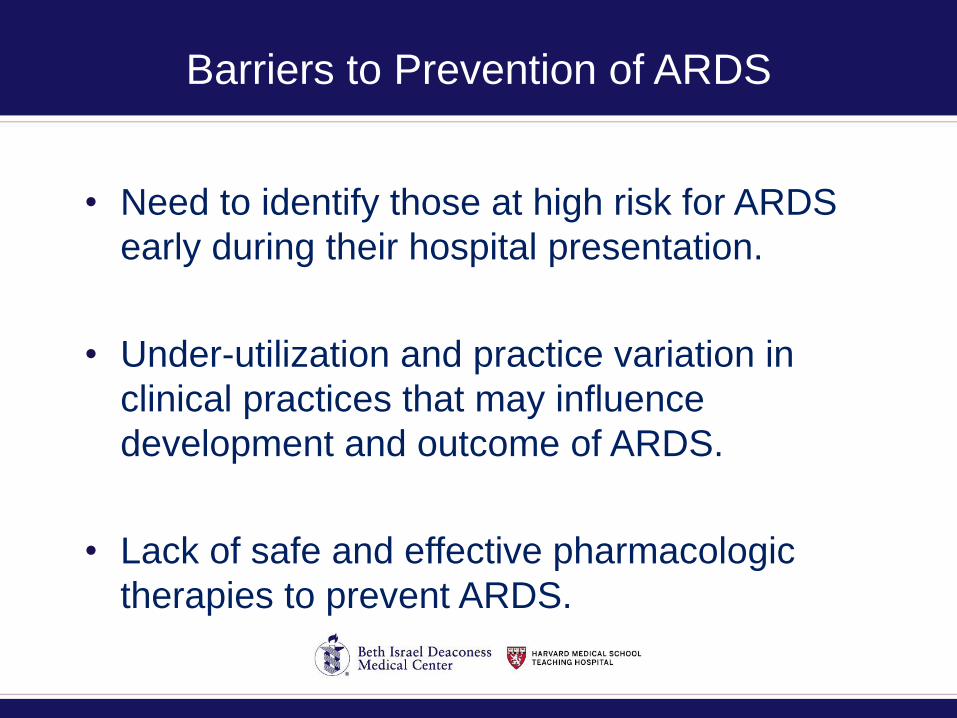
5992 Patients with at least one
predisposing condition at the time of ED
evaluation of hospital admission for
elective surgery
5584 Patient enrolled
Excluded:• 166 ALI on admission
• 124 Hospital transfer
• 44 Readmission
• 28 comfort care
• 46 other (died in the ED, no research
authorization – prisoner, incomplete
records)
377 ALI/ARDS 5213 NO ALI/ARDS
148 ALI 229 ARDS
A minority of Patients at Risk Develop ARDS

Results
% ALI development according to predisposing
conditions
0
5
10
15
20
25
30
Sm
oke
inha
latio
n 7/
27
Sho
ck 7
2/40
3
Asp
iratio
n 35
/212
Aor
tic sur
gery
21/
127
Lung
con
tusion
27/
190
Car
diac
sur
gery
55/
541
Acu
te a
bdom
en 2
7/29
5
Traum
atic b
rain in
jury
45/
495
Pne
umon
ia 1
02/1
234
Mul
tiple fr
actu
res 26
/332
Sep
sis 12
4/18
15
Thora
cic
surg
ery 7/
175
Spine
sur
gery
16/
486
Pan
crea
titis 9
/325
Gajic et al Am J Resp Crit Care Med 2011

LIPS Score
Gajic et al. Am J Resp Crit Care Med 2011
AUC=0.80 (95% CI 0.79 to 0.80)

Can We Improve on the LIP Score?
Agrawal AJRCCM 2013

Can We Improve on the LIP Score?
Agrawal AJRCCM 2013

Barriers to prevention of ARDS
• Need to identify those at high risk for ARDS
early during their hospital presentation. • → LIPS: Lung Injury Prediction Score
• Under-utilization and practice variation in
clinical practices that may influence
development and outcome of ARDS.
• Lack of safe and effective pharmacologic
therapies to prevent ARDS.
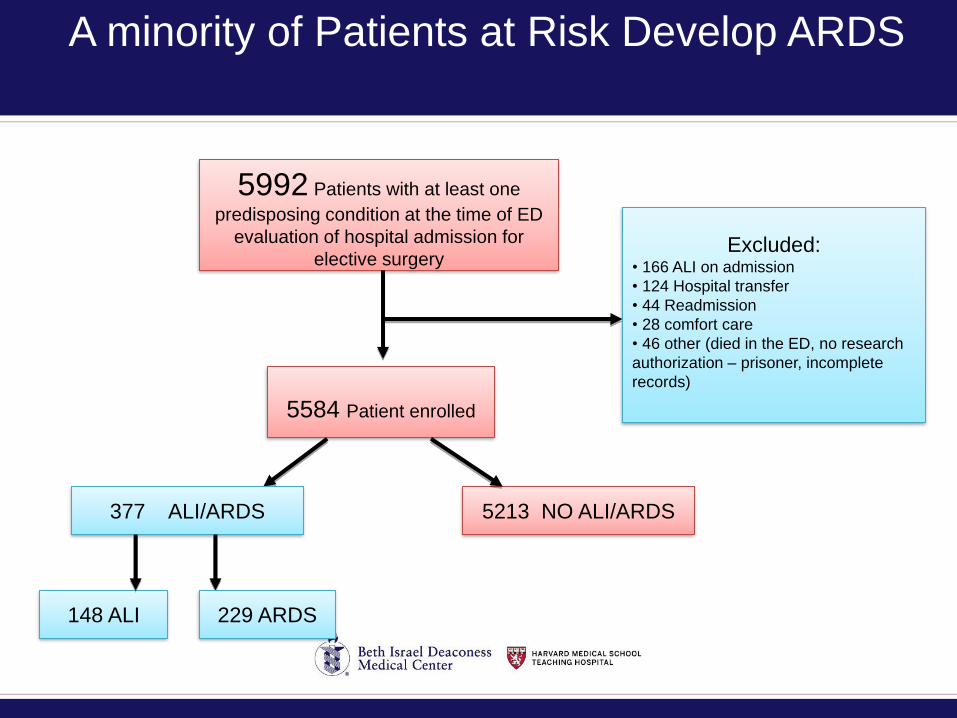
CLIP Element Clinically Supported Practices AHA grade
Adequate empiric antimicrobial treatment and source control
According to suspected site of infection, health care exposure, and immune suppression
Class I
Lung protective mechanical ventilation Tidal volume <6-8 mL/kg predicted body weight and plateau pressure <25 cm H2O; PEEP≥5 cm H2O, minimize FIO2 (target O2sat 88-92%)
Class Iia-IIb
Aspiration precautions Rapid sequence intubation supervised by experienced providers, elevated head of the bed, oral care with chlorhexidine, gastric acid neutralization
Class IIA-IIb
Early reassessment of noninvasive ventilation (to prevent delayed intubation)
Early reassessment of the work of breathing 30 minutes into the onset of noninvasive ventilation
Class IIb
Fluid management:
- Early fluid administration in septic shock
-Limiting fluid overload after resuscitation
- Resuscitation according to institutional protocol and IHI sepsis bundle
- Modified ARDSnet FACCT protocol after early shock (first 12 hours)
Class IIa
Class IIa
Restrictive transfusion Hemoglobin target >7 g/dL in the absence of acute bleeding and/or ischemia
Class IIa
Appropriate handoff of patients at risk Structured handoff such as SBAR Class IIa
Checklist for Lung Injury Prevention: CLIP


% Patients on Acid Blocker
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
VentDay 1
VentDay 2
VentDay 3
VentDay 4
VentDay 5
VentDay 6
VentDay 7
Pre-CLIP
Post-CLIP
CLIP Study
Tidal volume by Vent Day after Intubation
6
6.5
7
7.5
8
8.5
9
9.5
10
Initial VentDay 1
VentDay 2
VentDay 3
VentDay 4
VentDay 5
VentDay 6
VentDay 7
Pre-CLIP
Post-CLIP

Barriers to Prevention of ARDS
• Need to identify those at high risk for ARDS
early during their hospital presentation. • → LIPS: Lung Injury Prediction Score
• Under-utilization and practice variation in
clinical practices that may influence
development of ARDS or outcomes of
patients at risk for ARDS.• → CLIP: Checklist for Lung Injury Prevention
• Lack of safe and effective pharmacologic
therapies to prevent ARDS.

Membrane
Injury
Inflammation
Coagulation
Oxidative
stress
Mechanical
Chemical
Biological
$$_
QALY
Capillary stress failure
Acid aspiration
Direct – SARS, Influenza, RSV, PCP
Indirect – SIRS, reperfusion, IL2, TRALI
+
Pathophysiology of ARDS

Katz et al. Chest 2011;139:658-668
Platelets and Platelet-Neutrophil
Interactions in ARDS

Looney et al. JCI 2009
Platelet Depletion Reduces ARDS
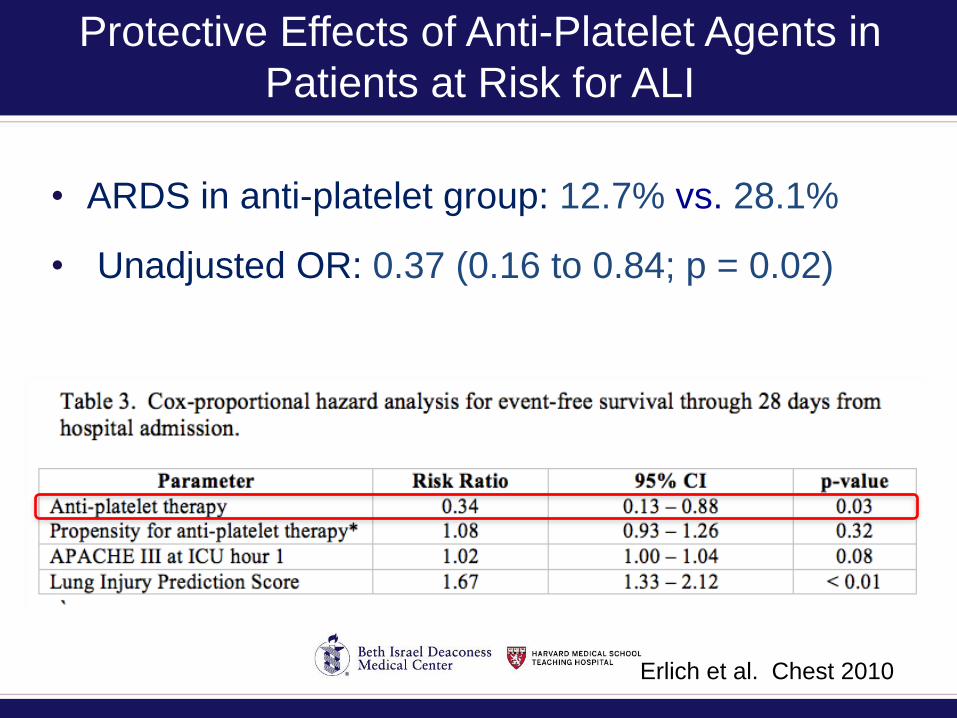
Protective Effects of Anti-Platelet Agents in
Patients at Risk for ALI
• ARDS in anti-platelet group: 12.7% vs. 28.1%
• Unadjusted OR: 0.37 (0.16 to 0.84; p = 0.02)
Erlich et al. Chest 2010

Emergency
Room Visit
Planned Hospital
Admission
LIPS score ≥ 4R
and
om
ization
Aspirin 325 mg and then 81 mg
PO/NG once daily
vs.
Placebo
Assessment for adverse events
• Bleeding risk
•Renal dysfunction
•Allergic reaction
Outc
om
e A
sse
ssm
en
t
• ∆ PaO2/FiO2
• ∆ SaO2/FiO2
• ∆ LIS
• ALI/ARDS
• ∆ Mortality
• Length of Stay
• Duration of
ventilation
Inclusion Criteria
Age < 18 years
Current anti-
platelets
Bleeding
Diathesis
Planned surgery
Allergy to aspirin
No consent
Exclusion Criteria
Baselin
e
Pla
sm
a
Day 3
Pla
sm
a
Clinical Outcomes
Physiologic Outcomes
Plasma Evaluation
• Thromboxane B2
• 15-epi lipoxins
• IL-6, PAI-1, RAGE
< 12 hours 7days

Screening Burden
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
Site14
Site07
Site02
Site16
Site13
Site08
Site15
Site12
Site01
Site04
Site10
Site06
Site05
Site11
Site09
Percentage of screened patients who were enrolled

Main Exclusions: All Screened Pt with LIPS >=4
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%

Characteristics of Screened v. Enrolled:
Predisposing Conditions
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
Enrolled
Not enrolled

Barriers to prevention of ARDS
• Need to identify those at high risk for ARDS
early during their hospital presentation. • → LIPS: Lung Injury Prediction Score
• Under-utilization and practice variation in
clinical practices that may influence
development of ARDS or outcomes of
patients at risk for ARDS.• → CLIP: Checklist for Lung Injury Prevention
• Lack of safe and effective pharmacologic
therapies to prevent ARDS.• → LIPS-A: Lung Injury Prevention Study - Aspirin


Is Preventing ARDS Important?
• ARDS is a difficult outcome to adjudicate.
• ARDS is not a patient centered outcome.
• ARDS per se may not be associated with
increased mortality.
What is the appropriate outcome?
Rubenfeld. AJRCCM

PETAL Network
• Goals– Conduct 3-5 Phase III clinical treatment trials which
PREVENT or provide EARLY treatment for patients at risk for, or with, ARDS.
– Establish and utilize a central IRB.
– Collect and bank high quality biospecimens for molecular definitions of illness, recovery, susceptibility.
• Mechanism– 12 Clinical Sites – each with at least one satellite.
• Two PIs – one ED, one Critical Care
– 1 Clinical Coordinating Center – MGH
– SC Chair – Roy Brower, JHU

Differences Between PETAL and ARDSNet
• Prevention and Early Treatment
• Acute Care/EM/Trauma + Critical Care
• Dialog, Collaboration, Exchange
– International Partnership Committee
– Canadian Critical Care Trials Group Representative
– International Scientific Advisory Committee with
members from CCTG, UK-CRN, ANZIC, etc.
– Website portal for feedback and suggestions
http://petalnet.org

ROSE: Reevaluation Of Systemic Early
neuromuscular blockade (NMB)
• Objective: To assess the efficacy and safety of
early NMB in reducing mortality and morbidity in
patients with moderate-severe ARDS in
comparison to a control group with no routine
early NMB.
• Hypothesis: Early NMB will improve mortality
prior to discharge home before day 90, in
patients with moderate-severe ARDS.
ROSE NMB Version III PETAL Network August 31, 2015

VIOLET: Vitamin D to Improve Outcomes
by Leveraging Early Treatment
Rationale for Vitamin D-ARDS Prevention:
(1) Vitamin D deficiency common in critical illness;
(2) Strong preclinical data, plausible mechanisms;
(3) Observational data key ARDS risk factor;
(4) Phase II data vitamin D repletion cheap, simple/rapid, safe, and improves outcomes in infection and non-infection ARDS prevention

LOTUS: Low Tidal volume Universal
ventilator Support
• Objective: A pragmatic trial of lung protective
ventilation in patients with acute respiratory
failure to improve patient-centered outcome(s)
• Hypothesis: Patients with acute respiratory
failure who received low tidal volume ventilation
(< 6 cc/kg PBW) will have improved patient-
centered outcome(s) than patients receiving
tidal volumes as set by usual care.

Conclusions
• ARDS is a potentially preventable complication.
• Early identification of patients at risk-– Avoid “second hit” exposures
– Facilitate mechanistic studies and prevention trials
– Mechanistic treatments may have a better chance to work early in the course of illness
• Appropriate therapies need to be identified.
• When such therapies are identified they should be tested in rapid cycle phase 2 trials.
• Appropriate endpoints need to be worked out.

Prevention of the Acute Respiratory
Distress Syndrome
Patient Engagement, Systems Science, and the Elimination of Preventable Harm
Daniel Talmor M.D., M.P.H.
Anesthesia, Critical Care and Pain Medicine
ABCs of ARDS prevention
• LIPS-A Aspirin
• LIPS-B Inhaled steroids (nebulized budesonide)
• LIPS-C Curcumin
• LIPS-D Vit D
• LIPS-H Inhaled heparin
• LIPS-Z…..