Embed Size (px)
DESCRIPTION
Preventing Vascular Effects on Brain Injury and Cognition
Citation preview

REVIEW
Preventing Vascular Effects on Brain Injury and CognitionLate in Life: Knowns and Unknowns
Owen Carmichael
Received: 16 May 2014 /Accepted: 23 July 2014 /Published online: 2 August 2014# Springer Science+Business Media New York 2014
Abstract For some researchers, the relationship betweenprevalent cardiovascular risk factors and late-life cognitivedecline is not worthy of further study. It is already known thateffective treatment of vascular risk factors lowers risk of suchmajor outcomes as stroke and heart attack, the argument goes;thus, any new information about the relationship betweenvascular risk factors and another major outcome - late-lifecognitive decline– is unlikely to have an impact on clinicalpractice. The purpose of this review is to probe the logic ofthis argument by focusing on what is known, and what is notknown, about the relationship between vascular risk factorsand late-life cognitive decline. The unknowns are substantial:in particular, there is relatively little evidence that currentvascular risk factor treatment protocols are adequate to pre-vent late-life cognitive decline or the clinically silent braininjury that precedes it. In addition, there is relatively littleunderstanding of which factors lead to differential vulnerabil-ity or resilience to the effects of vascular risk factors on silentbrain injury. Differential effects of different classes of treat-ments are similarly unclear. Finally, there is limited under-standing of the impact of clinically-silent neurodegenerativedisease processes on cerebrovascular processes. Further studyof the relationships among vascular risk factors, brain injury,and late-life cognitive decline could have a major impact ondevelopment of new vascular therapies and on clinical man-agement of vascular risk factors, and there are promisingavenues for future research in this direction.
Keywords BrainMRI . Vascular risk factors . Silent braininjury . Cognitive decline . Clinical trials . Aging
Introduction
Vascular risk factors including hypertension (HTN), diabetesmellitus type II (DM) and hyperlipidemia (HYP) are highlyprevalent among individuals older than 60 years of age(Crawford et al. 2010; Go et al., 2013; Kannel and Gordan1978; Wolf, D’Agostino, Belanger, and Kannel 1991) andaccount for a high percentage of direct health expendituresin the United States. Besides being major risk factors for heartdisease, stroke, and early mortality (Alexander et al. 2003;Chobanian et al. 2003), each of these risk factors is associatedwith decline in cognitive abilities late in life, including clinicaldementia syndromes (Debette et al. 2011; Joas et al. 2012;Kivipelto et al. 2001; Stewart et al. 2009; Whitmer, Sidney,Selby, Johnston, and Yaffe 2005). Vascular risk factors arebelieved to increase risk of cognitive decline by promotingprogressive, clinically silent brain injury over the course ofyears or even decades (Debette et al. 2011; Knopman et al.2011; Korf et al. 2004; Maillard et al. 2012; Tan et al. 2011).Such brain injury, manifested through lesions, tissue loss, andneural dysfunction on brain MRI, is among the most consis-tently replicated risk factors for late-life cognitive decline todate (Bombois et al. 2008; Carlson et al. 2008; Kuller et al.2003; Lopez et al. 2003; O'Sullivan et al. 2004).
Because each one of these vascular risk factors is modifi-able, these findings have led to the possibility that treatment ofvascular risk factors might lessen the burden of late life braininjury, and in turn lower risk for future dementia (Gorelicket al. 2011). There is certainly much room for improvement invascular risk factor treatment: for example, despite increasingpublic awareness, less than 7% of individuals with concurrentDM, HTN, and HYP achieve defined treatment goals(Schroeder et al. 2012). If it were actually true that sustained,effective treatment of vascular risk factors could reduce risk oflate life cognitive decline, the potential effects are astounding:for example, in a population attributable risk analysis that
O. Carmichael (*)Pennington Biomedical Research Center, 6400 Perkins Road,Baton Rouge, LA 70808, USAe-mail: [email protected]
Neuropsychol Rev (2014) 24:371–387DOI 10.1007/s11065-014-9264-7

makes assumptions about how many dementia cases areuniquely attributable to individual risk factor exposure, a25 % decrease in a handful of risk factors (predominantlyvascular ones) is projected to prevent as many as half ofdementia cases that will emerge moving forward (Barnesand Yaffe 2011) (see also (Launer et al. 2010)).
However, the purpose of this review is to build the case thatfurther clarification of the relationship between vascular riskfactors and late-life cognitive decline is needed. The overarch-ing point is that even if current treatment protocols are adequateto lower risk of heart attack, stroke, and early mortality, it is notknown whether they are also adequate for lowering the burdenof silent brain injury and the risk of late-life cognitive decline.This is true for a number of reasons: there is a lack of convinc-ing clinical trial evidence; differential vulnerability or resilienceto brain effects of vascular risk factor exposure is not wellunderstood; and relationships between vascular risk factorsand prevalent, clinically-silent neurodegenerative disease pro-cesses are not well understood. As a result, it is possible thatmany individuals who have effectively avoided heart attack andstroke by addressing their vascular risks may have done littlemore than set themselves up for cognitive decline later in life. Incontrast, hypothetical vascular risk factor treatment protocolsthat avoid this “out of the frying pan, into the fire” scenario byreducing risk for cognitive decline as well as heart attack andstroke could benefit the growing population of elderly individ-uals, and potentially reduce the steadily increasing global bur-den of late-life cognitive decline.
The following sections will provide a review of what iscurrently known, and what is currently unknown, about therelationship between vascular risk factors and both silent braininjury and cognitive decline late in life. A set of ways to moveforward is then presented for the field to better understand theability of treatment protocols to reduce late life cognitivedecline risk.
What is Known
Vascular Risk Factors Increase Risk for Brain Injuryand Cognitive Decline
A growing number of studies suggest that middle-aged indi-viduals exposed to vascular risk factors such as DM, HTN,and HYP go on to have elevated risk of dementia and cogni-tive decline in their elderly years (Debette et al. 2011; Joaset al. 2012; Stewart et al. 2009; Swan et al. 1998; Whitmeret al. 2005), suggesting that cumulative exposure to vascularconditions, accumulated over possibly decades of life, may bea key driver of risk. These results are highly robust becausethey have been reproduced across a variety of study designs,nations of origins, and methodologies for assessment of bothvascular risk and cognitive decline. This well-established link
between vascular risk factors and late-life cognitivedecline forms the starting point for investigation of vascularrisk factor treatment as a preventive strategy against late-lifecognitive decline.
Brain injury, as measured by in vivo brain MRI, is believedto be a key intermediary in the relationship between vascularrisk factor exposure and late-life cognitive decline. The totalvolume of parenchymal tissue and CSF, as well as the vol-umes of brain tissue in specific compartments, from T1-weighted sequences, provide proxy measures of the accumu-lated burden of neuronal death, while the volume of whitematter hyperintensities from T2-weighted sequences providemeasures of accumulated protein-rich fluid hypothesized to besecondary to myelin breakdown, neuronal damage, or gliosis(Fazekas et al. 1998). Both T1-weighted and T2-weightedMRI are used to identify clinically-silent infarcts as anothermeasure of brain injury that is vascular in origin (Vermeer,Longstreth, and Koudstaal 2007). More recently, diffusionMRI has provided more sensitive and fine-grained measuresof white matter injury (Le Bihan 2003). Brain dysfunction thatarises either as a manifestation of underlying neuronal injuryor as a symptom of modified coupling between neural activityand vascular or metabolic processes can also be measuredusing neuroimaging. Cerebral hemodynamics—i.e., localizedcerebrovascular changes that are caused by proximal neuronalactivity– can be measured by dynamic MRI methods that aresensitive to blood oxygenation (such as blood oxygenationlevel dependent or BOLD functional MRI (Logothetis andPfeuffer 2004)) or blood flow (such as perfusion MRI witharterial spin labeling (Petersen et al. 2006)). Acquiring thisdata under varying neural stimuli or vascular conditions (suchas carbon dioxide challenge) allows for proxy measurement ofthe hemodynamic response function, which can be used as anindicator of neurovascular coupling. In the absence of exter-nally imposed neural and/or vascular conditions, BOLD func-tional MRI can also be used to measure functional connectiv-ity—i.e., synchrony of spontaneous blood oxygenation fluc-tuations between distinct brain regions (van den Heuvel andHulshoff Pol 2010). Low functional connectivity may be anindicator of disrupted synchrony of underlying neural activity,modified coupling of spontaneous neural activity to the vas-cular supply, or both. Brain glucose metabolism, includingchanges in local glucose metabolism due to changes in localneural stimuli, can be measured via positron emission tomog-raphy (PET) with the radiolabeled glucose tracerfluorodeoxyglucose (FDG). Numerous reports have sug-gested that all of the indicators of brain injury noted abovebecome more prevalent late in the lifespan (Biswal et al. 2010;Carmichael and Lockhart 2012; D’Esposito et al. 1999; Debetteand Markus 2010; DeCarli et al. 2005; Loessner et al. 1995;Parkes et al. 2004; Raz et al. 2005; Vermeer et al. 2007).
Evidence has accumulated from several large epidemiolog-ical studies that individuals exposed to vascular risk factors,
372 Neuropsychol Rev (2014) 24:371–387

either in midlife or late in life, show a greater burden of braininjury that is clinically silent—that is, not accompanied byclinically evident cognitive deficits (Au et al. 2006; Carmelliet al. 1999; Das et al. 2008; Jeerakathil et al. 2004; Korf et al.2004; Moran et al. 2013; Prabhakaran et al. 2008; Seshadriet al. 2004; Swan et al. 1998) (DeCarli et al. 1995; Hsu et al.2012; Jeerakathil et al. 2004). While the majority of thisevidence is focused on the relationship between vascular riskfactors and white matter hyperintensities, there is increasingevidence that gray matter is affected by vascular risk as well(Brundel et al. 2010; Cardenas et al. 2012). In addition, severallarge studies have suggested that elderly individuals who arecognitively intact, yet manifest increased levels of clinically-silent brain injury on MRI, are at increased risk of clinically-relevant cognitive decline in the future (Carmichael et al.2007; Debette and Markus 2010). Large-scale autopsystudies complement this evidence by documenting: 1.clinically-silent brain injury in individuals who died cogni-tively intact (Morris and Price 2001); and 2. greater burden ofsilent brain injury in individuals who had experienced greaterexposure to vascular risk factors over the lifespan (Knopmanand Roberts 2010).
Taken together, this evidence strongly supports the notionthat vascular risk factors contribute to increased dementia riskby elevating the burden of clinically silent brain injury thataccumulates in the aging brain over the course of years ordecades. But, it is important to note that the vast majority ofsuch supporting evidence comes from observational trials inwhich trajectories of vascular risk factor exposure and treat-ment, as well as adherence to and efficacy of treatment, werenot standardized or manipulated by the study. This makes itdifficult to establish a causal relationship between vascularrisk factor treatment and prevention of silent brain injury. Asoutlined in the next section, clinical trials of vascular riskfactor treatments with brain MRI outcomes could providestronger evidence to support this association, but such trialshave been remarkably small in number.
Multiple Pathways Lead from Vascular Risk Factors to BrainInjury
The observed association between vascular risk factor expo-sure and clinically silent brain injury naturally leads to thequestion regarding which biological mechanisms could leadfrom one to the other. To answer this question, investigatorshave sought to clarify the mechanisms by which vascular riskfactors disrupt cerebrovascular function (i.e., the functioningof the blood vessels that supply brain tissue), with an under-standing that damage to neuronal tissue is a likely conse-quence (Fig. 1). At least three mechanisms have been pro-posed. First, elevated blood pressure is believed to promotearterial stiffness, i.e. lack of compliance of the central arteries.One result of increased arterial stiffness is transfer of cardiac
flow pulsatility to the less compliant small blood vessels of thebrain, resulting in increased mechanical stress on those vesselsthat eventually culminates in microhemmorhage (Henskenset al. 2008; Mitchell et al. 2011; O’Rourke and Safar 2005;Ohmine et al. 2008; Tsao et al. 2013; Zieman, Melenovsky,and Kass 2005) (Kiechl and Willeit 1999). Another result ofincreased arterial stiffness is enhancement of cardiac wavereflection, i.e., a greater amount of oxygenated bloodreturning back up the descending aorta toward the heart ratherthan further down the vascular tree, resulting in less efficientoxygen transfer to smaller blood vessels including those in thebrain. Second, elevated cholesterol promotes deposition ofatherosclerotic plaque, leading to ischemic infarction andalterations to the fluid dynamics of blood flow through ste-notic blood vessels supplying the brain (Amarenco et al. 1994;Manolio et al. 1999; Tell et al. 1988). Third, chronic glucoseintolerance is associated with inflammation of the endotheli-um that culminates in decreased efficiency of cerebral perfu-sion (Miranda et al. 2005). These disparate mechanisms ap-pear to interact with and reinforce each other; for example,inflammation may potentiate atherosclerotic plaque deposi-tion by changing the adhesion properties of the vessel wall(Libby et al. 2002), arterial stiffness may similarly predisposeto plaque deposition (van Popele et al. 2001), and inflamma-tion may exacerbate arterial stiffness (Schnabel et al. 2008).Mutual reinforcement of disparate mechanismsmaymean thatit is difficult to reverse any one of them individually onceinitiated. Altered cerebral perfusion, hemorrhage, and infarc-tion contribute to a complex cascade of secondary injuryprocesses including apoptosis, necrosis, oxidative stress, andexcitotoxicity (Dirnagl et al. 1999; Madamanchi et al. 2005),each of which promote neuronal injury.
Several in vivo neuroimaging studies support these hypoth-esized mechanisms (Bots et al. 1993; Dai et al. 2008; Mulleret al. 2012; Poels et al. 2010; Vermeer et al. 2007). Individualswith greater exposure to vascular risk factors are at greater riskof clinically silent infarcts, identified on T1- and T2-weightedMRI (Das et al. 2008; Vermeer et al. 2007), as well as micro-hemorrhages visible on highly-sensitive T2*-weightedsequences such as susceptibility-weighted imaging(Cordonnier et al. 2007; Goos et al. 2010; Poels et al. 2010).Deficits in cerebral perfusion, measured using perfusion MRIwith arterial spin labeling, have been demonstrated in elderlyindividuals possessing vascular risk factors, especially hyper-tension (Dai et al. 2008; Hajjar et al. 2010; Muller et al.2012). Atheroslerosis of the blood vessels supplying the brainis most often measured at isolated locations, such as thecarotid bifurcation, and is usually summarized in terms ofunivariate measures such as the carotid intima-media thick-ness based on ultrasound examination; however MRI se-quences have the capability of providing more sensitive mea-sures of plaque burden covering a greater extent of the vascu-lature. Using these techniques, a number of studies have
Neuropsychol Rev (2014) 24:371–387 373

suggested that elderly individuals with a greater burden ofvascular risk factors have a greater risk of carotid atheroscle-rotic plaque (Ebrahim et al. 1999; O’Leary et al. 1992;Salonen and Salonen 1991). Greater burden of systemic in-flammation, measured through blood biomarkers, has beenassociated with silent infarcts, as well as greater burden ofother indicators of silent brain injury (Fornage et al. 2008;Hoshi et al. 2005; Ishikawa et al. 2007; Jefferson et al. 2007;Miwa et al. 2011; van Dijk 2005; Wright et al. 2009).
In turn, there is increasing evidence that cerebrovasculardysfunction is associated with clinically-silent brain injury(Pantoni and Garcia 1997). Greater burden of carotid athero-sclerosis has been associated with greater burden of whitematter hyperintensities and greater brain atrophy both cross-sectionally and longitudinally (Kin et al. 2007; Manolio et al.1999; Majon Muller et al. 2011; Pico et al. 2002). Cerebralperfusion deficits, likewise, have been associated with bothforms of silent brain injury in healthy elders (Appelman et al.2008; van Es et al. 2010). Finally, autopsy findings of cere-brovascular pathology have been shown to be associated withgreater burden of silent brain injury seen in corresponding pre-mortem brain MRI (Jagust et al. 2008).
Taken together, this evidence strongly supports the notionthat vascular effects on clinically silent brain injury, and thuscognition, are determined by multiple biological processes. Itfollows that any attempt to prevent vascular effects on cogni-tion would require a complex, multi-pronged interventionapproach aimed at multiple biological targets, including tar-gets that may be specific to the brain. Thus, it is not entirelyclear that current protocols for treatment of vascular riskfactors, which may or may not neutralize the biological pro-cesses implicated in the pathway from vascular processes tosilent brain injury, are adequate to prevent silent brain injury.
Cerebrovascular Injury Commonly co-Occurswith Other Neurodegenerative Diseases
As described above, any putative strategy for preventing theeffects of vascular risk factors on late life cognition is compli-cated by the multiplicity of biological processes implicated inthe pathway from vascular risk, to cerebrovascular dysfunction,to clinically silent brain injury and subsequent cognitive decline.An additional problem is that any putative treatment strategymust be sensitive to other neurobiological processes of agingthat co-occur with the various vascular-related processes. A
growing body of evidence from large-scale autopsy studiessupports the notion that cerebrovascular dysfunction commonlyco-occurs with, and likely interacts with, other neurobiologicalprocesses of aging. These studies suggest that among individ-uals who die clinically demented, a common autopsy finding isan admixture of cerebrovascular, Alzheimer, and Lewy bodypathologies (Brayne et al. 2009; Schneider et al. 2007a; Whiteet al. 2005a). Further studies suggest that each of the implicatedpathologies may be clinically relevant to cognitive functioning;individuals with a certain level of a particular pathology atautopsy were more likely to have reduced cognitive functioningnear the end of life when additional pathologies were alsopresent at autopsy (Schneider et al. 2007b).
In vivo studies of the co-occurrence of cerebrovascularinjury and additional pathologies have been limited by therelative expense and technical requirements of measuringAlzheimer pathology in vivo using cerebrospinal fluid assaysor positron emission tomography imaging. In addition, thesestudies have been limited by the relative lack of sensitive,robust, and circumspect measures of in vivo cerebrovascularinjury burden. Small-scale studies of convenience samplesdisagree on the degree to which cerebral amyloid burdenand white matter hyperintensity burden are correlated witheach other (Grimmer et al. 2012; Hedden et al. 2012;Marchant et al. 2012). Other studies have observed that cere-bral amyloid burden and white matter hyperintensity burdenare independently associated with greater brain atrophy andhypometabolism (Barnes et al. 2013; Guzman et al. 2013;Haight et al. 2013), and additional studies support the viewthat the co-occurrence of amyloid and white matterhyperintensities is clinically relevant among those clinicallydiagnosed with Alzheimer’s disease (Provenzano et al. 2013).To the degree that white matter hyperintensities are a mani-festation of cerebrovascular dysfunction, the in vivo data canbe used to support the notion that cerebrovascular injury andAlzheimer’s disease may have additive or multiplicative del-eterious effects on the brain that hasten cognitive deteriora-tion. While there is strong support for the view that whitematter hyperintensities are primarily driven by cerebrovascu-lar injury in the absence of Alzheimer pathology (Fazekaset al. 1993; Pantoni and Garcia 1997), there is a possibilityAlzheimer’s pathology itself could contribute to white matterhyperintensities (Chen et al. 2006; Gouw et al. 2011), thuscomplicating conclusions that can be drawn about the twodistinct processes from these data.
Fig. 1 Conceptual model in which vascular injury processes lead to preclinical cerebrovascular injury, which in turn contributes to brain injury andsubsequent cognitive decline
374 Neuropsychol Rev (2014) 24:371–387

There are plausible biological mechanisms through whichcerebrovascular injury processes may facilitate or reinforcethose of other neurobiological processes of aging, particularlyAlzheimer’s disease. For example, there is increasing evidencethat the normal metabolism of cerebral amyloid involves clear-ance along perivascular spaces, and thus vascular compromisecould hypothetically lead to amyloid accumulation in interstitialspaces (Preston et al. 2003) (Iliff et al. 2012). Failure of suchvascular clearance mechanisms is one explanation for the com-mon finding of cerebral amyloid angiopathy—amyloid accu-mulation within the cerebral blood vessels (Vinters and Gilbert1983). In turn, such vascular amyloidosis is believed to be itsown cause of microhemorrhage (Gilbert and Vinters 1983).Cholesterol metabolism and amyloid metabolism are alsoclosely linked (Dietschy and Turley 2001; Liu et al. 2007;Simons et al. 1998), although the precise effects of chronicallyelevated circulating cholesterol on this linkage are currentlyunclear (Höglund et al. 2004; Pappolla et al. 2003; Refolo et al.2000). Amyloid itself, especially in its oligomeric form, ap-pears to be pro-inflammatory, and thus has the potential toexacerbate the inflammatory effects of cerebrovascular process-es (Salminen et al. 2009; White et al. 2005b). Taken together,this evidence suggests that even if effective treatment of vas-cular risk factors is able to halt the progression of cerebrovas-cular injury, this might have no major impact on downstreambrain injury if additional processes such as cerebral amyloidosishave emerged and are able to continue to damage brain tissueon their own. This interaction between cerebrovascular injuryand other aging processes casts further doubt on the notion thatthe putative treatment of vascular risk factors according tocurrent treatment protocols has an easy-to-predict, straightfor-ward effect on downstream brain injury and, eventually, late lifecognitive decline.
What is Not Currently Known
It is not Clear That Effective Vascular Risk Factor TreatmentPrevents Cognitive Decline and Clinically Silent Brain Injury
Clinical trials examining the possibility that effective treatmentof vascular risk factors may modify risk of clinically-relevantcognitive decline in the elderly have provided conflicting re-sults (Novak and Hajjar 2010). A Cochrane review did not findconsistent high-level evidence that anti-hypertensives reducerisk of incident dementia or decline in cognitive test scoresamong elderly individuals (McGuinness et al. 2009). Anothermeta analysis suggested that successful blood pressure lower-ing may be associated with both improvement in, and dimin-ishment of, cognitive abilities, depending on which cognitivemeasurements were used (Birns, Morris, Donaldson, and Kalra2006). To date, a very small number of clinical trials of vasculartherapies have considered neuroimaging measures of silent
brain injury as an outcome of interest. The largest such study(N=192) found that antihypertensive treatment significantlyreduced the risk of progression of white matter hyperintensitiesamong individuals with prevalent clinical stroke (Dufouil et al.2005). Smaller pilot studies, each including roughly tens ofindividuals, have suggested that effective treatment with anti-hypertensive therapies may be associated with preservation ofcerebrovascular functioning in the face of vascular challenge,as well as preservation of glucose metabolism (Hajjar et al.2013; Imabayashi et al. 2011; Kimura et al. 2010; Matsumotoet al. 2009). However it should be emphasized that to date,studies with brain injury outcomes have not been performed ona similar scale to those with cognitive indicators as the primaryoutcome (i.e., with thousands of participants).
The lack of concurrence between trials is perhaps notsurprising, as those conducted to date have been highly vari-able along a number of critical dimensions. Background char-acteristics of study participants have been particularly vari-able, with mean ages ranging from the 50s to the 80s, andtarget populations varying from those with isolated hyperten-sion to those with prevalent clinical stroke. Treatment classesof interest have varied, as have individual treatments withinclasses. Treatment histories of participants have varied as well.Treatment protocols, especially the definition of successfulblood pressure lowering and treatment modifications in theevent of unsuccessful lowering, are another source of variabil-ity. In addition to these known differences among diversetrials, heterogeneity in study results may have been influencedby differences in latent characteristics of study participantsthat the trial failed to measure. In particular, most trials (out-side of those performed in clinical stroke populations) did notattempt to sample participants based on their burden of pre-existing brain injury or neurodegenerative disease that wasclinically silent. Thus, the results of these trials may have beenconfounded by pre-existing brain characteristics that pre-disposed participants to cognitive decline in spite of treatment.
Outside of clinical trials, several large observational studiessupport the notion that individuals with a history of successfulvascular risk factor treatment possess lower levels of silentbrain injury (Godin et al. 2011; Hajjar et al. 2012; Kuller et al.2010; Valeo 2013). In particular, two of these studies found anassociation between use of specific classes of antihypertensivetreatment—beta blockers and angiotensive receptorblockers—and lower burden of neuropathology at autopsy.The other studies found that individuals who effectivelylowered blood pressure showed a lower burden of, or slowerprogression of, white matter hyperintensities on MRI. Thesestudies were not prospectively designed to sample individualsbased on trajectories of vascular risk factor exposure andtreatment however, and they were not designed to manipulatevascular risk factors to determine the effect of this manipula-tion on the brain. While these studies provide valuable hintsthat effective treatment of vascular risk factors may potentially
Neuropsychol Rev (2014) 24:371–387 375

ameliorate brain injury burden, this notion has not beenstrongly demonstrated in any large-scale, prospective, ran-domized controlled trial to date.
It is not Known Whether There is a Critical TreatmentWindow for Prevention of Vascular Effects on the Brainand Cognition
Many of the aforementioned clinical trials focused on individ-uals who were elderly and relatively likely to experiencecognitive decline over a fairly brief follow-up interval(McGuinness et al. 2009). However, accumulating evidencesuggests that vascular effects on silent brain injury may com-mence in mid-life, possibly as early as the fourth decade of life(Maillard et al. 2012), even among individuals whose vascularinjury burden is so mild that they do not meet criteria forrecognized clinical conditions such as hypertension. The ef-fects of vascular conditions on silent brain injury appear toaccumulate steadily between early midlife years and elderlyyears, until elderly individuals possessing decades of exposureto vascular risks have a substantial burden of silent braininjury and an elevated risk of consequent cognitive decline(Debette et al. 2011; Havlik et al. 2002; Knopman et al., 2001;Korf et al. 2004; Swan et al. 1998). For this reason there is agrowing belief that the clinical trials in elderly populationsmay simply have been “too little, too late”—attempting toarrest the effects of vascular processes on the brain long afterthose processes have wrought the major damage leading tocognitive decline.
An obvious consequence of the “too little, too late” prob-lem is that clinical trials of vascular risk factor therapies aspreventive agents for late-life cognitive decline should beperformed earlier. But the key unanswered question is when,exactly. In other words, there may be a critical treatmentwindow, i.e. a period of the lifespan during which emergingvascular injury processes must be controlled to prevent even-tual consequences for the brain and cognition. If treatment in75-year-olds is too little, too late, it is unclear whether treat-ment in 65-year-olds, or 55-year-olds, is any different.Another possibility is that the key determinant of the brainbenefits of treatment is not chronological age per se, butduration of exposure to vascular risks. The emergence andtrajectory of vascular risk factors such as hypertension ishighly variable across the population, with blood pressurerising to elevated levels at variable points in the lifespan. Itcould be that to prevent effects on the brain, it is critical toaggressively treat vascular risks soon after they emerge, re-gardless of when in the lifespan they emerge. If such a criticaltreatment window were established, it could have tremendousimplications for the surveillance of vascular risk factors andprotocols for treatment initiation: for example, if vasculareffects on silent brain injury are evident even among 30-year-olds as suggested above, and it is critical to arrest these
effects in the 30s, careful surveillance of vascular measuresand aggressive pursuit of treatment may be warranted even inthis young age group, contrary to current practice. Whethersuch critical treatment windows exist, and what their param-eters are, is currently unknown due to a lack of studies relatingvascular risk factor treatment to brain outcomes across a widerange of ages.1
It is not Known Whether Achieving Current TreatmentTargets is Adequate to Prevent Silent Brain Injury
Clinical trials with cardiovascular disease outcomes (Vasanet al. 2001) have carefully considered how obtained levels ofblood pressure, cholesterol, blood glucose, and other relevantparameters of vascular risk relate to relevant outcomes. Thecumulative result of these trials is a set of treatment targets:optimal ranges of these parameters that should be sought inorder to minimize risks of cardiovascular outcomes. Treatmentprotocols then index success of treatment against the ability tomove vascular parameters into the target range. There does notappear to have been any such attempt to identify treatmenttargets for prevention of silent brain injury or cognitive decline,or at least to determine whether currently accepted treatmenttargets for cardiovascular outcomes should be considered opti-mal targets for prevention of silent brain injury or cognitivedecline. One possibility is that while current treatment targetsmay be adequate for lowering risk of heart attack, stroke, orother major outcomes, they may be less than adequate forlowering risk of silent brain injury and cognitive decline. Forexample, while attainment of a systolic blood pressure of 130may be considered adequate for cardiovascular outcomes, per-haps going even lower (for example, to 110) may be required tolower risk of silent brain injury. One reason this possibility mayhave merit is that there may be a continuous relationshipbetween healthier values of vascular parameters and lesserburden of silent brain injury, across a very broad range ofvascular parameter values, even to values considered quitelow in terms of current treatment targets (Maillard et al.2012). In other words, there is not a strong base of evidencefor a lower bound for the vascular parameter beyond whichfurther lowering would incur no benefit in terms of brain injuryprevention. This suggests that lowering vascular parameterseven lower than current treatment targets could have benefitsfor brain injury and cognitive outcomes. Establishing treatmenttargets for reduction of risk of brain injury and cognitive declinecould clearly have major implications for clinical practice, butdue to a lack of clinical trials measuring brain injury outcomes
1 Note that a similar “too little, too late” problem is widely agreed to be acritical failure in most clinical trials of treatments for Alzheimer’s disease,and that a major focus of current research is testing promising treatmentsearlier in the trajectory.
376 Neuropsychol Rev (2014) 24:371–387

in individuals who achieved varying levels of vascular param-eters through treatment, such targets are currently unknown.
It is not Known Whether Some Individuals are EspeciallyVulnerable to Vascular Effects on the Brain, and if soWhetherThey Should be Treated Differently
As described above, many prior studies suggested that greaterlevels of vascular risk factor burden are associatedwith greaterlevels of silent brain injury burden. However, a more precisesummary of findings from these studies is that while there is ageneral population-level trend in this direction, there is evi-dence of a great deal of inter-individual heterogeneity, suchthat some individuals appear to be differentially vulnerable—i.e., possessing a high level of silent brain injury relative totheir low burden of vascular risk—and some individuals ap-pear to be differentially resilient—i.e., possessing a low levelof silent brain injury relative to their high burden of vascularrisk. While numerous biological factors could be hypothe-sized to explain this inter-individual variability, data on thisphenomenon is scarce. For example, a number of geneticfactors that increase risk of dementia are implicated in thesame general biological pathways that lead from vascular riskfactors to brain injury; one prominent example is apolipopro-tein E, a cholesterol transport protein that is by far the mostwidely replicated genetic risk factor for Alzheimer’s disease(Roses and Allen 1996; Yip et al. 2005). Similarly, severalother genes implicated in pro-inflammatory pathways alsoincrease risk of AD, potentially by exacerbating the effectsof vascular-driven systemic inflammatory processes on thebrain (McGeer and McGeer 2001). The presence ofgenetically-driven vascular brain injury diseases such asCADASIL (Ruchoux and Maurage 1997), along with theemergence of genetic risk factors for cerebral infarction(Chou et al. 2013; Debette et al. 2010), further supportsthe notion of differential vulnerability to vascular-driven brain injury arising from background factors.However, the concept that the effects of vascular risk factorson silent brain injury could be influenced by differentialvulnerability does not appear to have been explored indepth.2
The concept of differential vulnerability to disease, identi-fied by background factors such as family history of disease,ethnic background, or genetic markers; or by presence ofconcomitant risk factors, is a guiding concept governing sur-veillance for a variety of chronic diseases, and it increasingly
influences personal health recommendations for those deemeddifferentially vulnerable. Thus, it should be clear that identi-fication of individuals differentially vulnerable to the effectsof vascular risk factors on the brain could have a major impacton clinical management of vascular risks, with those individ-uals followed especially closely and treatment pursued themost aggressively. However, such at-risk groups have notbeen identified, due to a lack of studies that measure the levelof vulnerability—i.e. measure the level of brain injury indexedagainst the level of vascular risk factor burden—and relate thisvulnerability to predictors such as family history or geneticmarkers. In addition, as mentioned above, the functioning ofthe cerebral vasculature is generally under-studied in the rela-tionship between vascular risk factors and silent brain injury.Further study with measurement of vascular risk, the cerebralvasculature, and brain tissue is needed to clarify whethervulnerable individuals feel an especially severe impact ofvascular risk factors on the cerebral vasculature itself, orwhether relatively mild damage to cerebrovascular function-ing culminates in especially severe damage to brain tissue, orwhether both of these are true.
It is not Known if Different TreatmentsHave Different Protective Effects on the Brain
Prior studies supporting an association between effectivetreatment of vascular risk factors and lower burden ofbrain injury and cognitive decline were not designed toanswer the question of whether differing treatmentsprovide differing benefits to the brain. There have onlybeen a limited number of reports related to this ques-tion. One preliminary report suggested an associationbetween antihypertensive treatment use and lesser bur-den of neuropathology on autopsy, but only within oneclass of medication (beta blockers) (White et al. 2013).There is a larger group of studies suggesting that an-giotensin receptor blockers have specific neuroprotectiveeffects (Hajjar et al. 2012; Thöne-Reineke et al. 2004; Wilms,Rosenstiel, Unger, Deuschl, and Lucius 2005). These reportslargely arose from observational studies that were notdesigned to sample participants according to treatmentregimen, nor control for duration of treatment exposureor adherence to treatment. Nonetheless, they raise thepossibility that effects on the brain could enter the alreadycomplex calculus about risk and benefit of differingtreatments.
It should be clear that an understanding of neuropro-tective effects of specific classes of vascular risk factortreatments could have a major impact on clinical man-agement of these conditions. But a lack of studies designed tocompare brain and cognitive outcomes between treatmentcategories has prevented such an understanding fromdeveloping.
2 While differential vulnerability of brain tissue to vascular processesdoes not appear to be a major research focus currently, differentialvulnerability of cognitive functioning to brain injury is. Cognitive resil-ience to such brain injury is referred to as “cognitive reserve.”Differentialvulnerability of brain tissue to cerebral amyloidosis (i.e., differential“amyloid toxicity”) is under study as well.
Neuropsychol Rev (2014) 24:371–387 377

How Time Courses of Vascular Brain Injury Relate to TimeCourses of Neurodegenerative Brain Injury is not WellUnderstood
As stated above, there is a growing body of evidence that inindividuals clinically diagnosed with dementia, cerebrovascu-lar injury commonly co-occurs with neurodegenerative pa-thology, especially that associated with Alzheimer’s disease.But the strongest evidence comes from large autopsy studies,along with in vivo studies that are for the most part cross-sectional and small. This means that the time course of cere-brovascular injury accrual, and how it relates to the timecourses of neurodegenerative pathology accrual and conse-quent development of silent brain injury, is poorly understood.Better understanding the relative time courses of these twoprocesses could have major implications for the viability ofvascular risk factor treatment as a preventive strategy againstsilent brain injury and consequent cognitive decline. For ex-ample, evidence that cerebrovascular injury tends to build upprior to Alzheimer’s disease pathology would suggest thatpreventing cerebrovascular injury through vascular risk factortreatment could potentially forestall cognitive decline byforestalling accrual of silent brain injury, even if such braininjury is destined to eventually accumulate due to the effectsof Alzheimer’s disease processes. Current epidemiologicalevidence tends to support this scenario, as vascular risk factorsand their brain effects become detectable earlier in the lifespanthan Alzheimer’s disease pathology does (Berenson et al.1998; Maillard et al. 2012). Nonetheless, evidence that it ismore typical for cerebrovascular injury to accumulate second-ary to Alzheimer’s pathology may suggest that in individualswith Alzheimer’s pathology, efforts to treat vascular risk fac-tors could be futile for prevention of cerebrovascular injury. Inaddition, better understanding the relative time courses ofthese two processes could clarify various additional aspectsof treatment strategies: for example, it could clarify whethervarious aspects of the time course of vascular risk factorexposure (such as the time of onset and fluctuations in thelevel of severity over time) place one in a higher-risk categoryfor accumulation of Alzheimer’s pathology, or whether thecritical period for applying a hypothetical Alzheimerpreventive agent is earlier or later in individuals exposed tovascular risk factors. Longitudinal studies that chart the rela-tive time courses of these two processes are needed to clarifythese issues.
Ways Forward
The previous section presented the case that numerous aspectsof the relationship between vascular risk factor treatment andsilent brain injury and cognitive decline are poorly under-stood, and a better understanding could have major
implications for efforts to prevent and treat vascular riskfactors in a clinical setting. In this section, the most promisingavenues for enhancing the state of scientific knowledge in thisarea are presented.
Conduct More Clinical Trials of Vascular Risk FactorTreatments with Cerebrovascular Function and Silent BrainInjury as Primary Outcomes of Interest
Possibly the greatest impediment to understanding the viabil-ity of vascular approaches to cognitive decline prevention is alack of clinical trials that measure what happens to the cerebralvasculature and brain tissue in groups of individuals whoseprior exposures to cardiovascular risk factors and treatmentsare matched to the greatest degree possible, and whose keydifference is exposure to a novel treatment agent. If a hypo-thetical treatment is beneficial for cardiovascular endpointsand if the cerebral vasculature and brain tissue are bettermaintained in those on treatment, this would be the strongestevidence to date for the vascular hypothesis. Clinical trials ofthis nature seem to be the only way to rigorously assess moredetailed aspects of the relationship between vascular riskfactor treatment and the brain, such as dose–response relation-ships and optimal treatment. The major difference betweenconventional clinical trials and these proposed ones is thelongitudinal assessment of brain outcome measures usingMRI; collecting and using such data in a large-scale clinicaltrial setting is feasible in middle aged and elderly individualsas shown by large-scale studies such as ADNI.
Develop and Validate Sensitive Measures of SystemicVascular Injury and Cerebrovascular Injury
As described above, multiple biological pathways could leadfrom vascular risk factors to cerebrovascular dysfunction,silent brain injury, and consequent cognitive decline, but it isnot clear how specifically vascular risk factor treatments im-pact each of these pathways, and it is not clear whetherarresting individual pathways is adequate to prevent conse-quent cerebrovascular dysfunction. Clinical trials of vascularrisk factor treatments with brain and cognitive outcomeswould thus be enhanced by measuring sensitive and robustmarkers of these pathways to determine which pathways, inwhich individuals, are engaged by the proposed treatment. Fortreatments that fail to enhance brain outcomes, such bio-markers would help to determine whether the treatment failedto modify the systemic processes that impinge upon the brain,or whether engaging those pathways was inadequate to pre-vent cerebrovascular dysfunction. A result of these bio-markers could be the development of relationships betweenthe systemic vascular biomarkers and cerebrovascular dys-function markers, to give a better sense of what target levelsof systemic markers must be achieved to meaningfully benefit
378 Neuropsychol Rev (2014) 24:371–387

the cerebral vasculature. In the long term, such biomarkerscould motivate biologically-driven combination therapiesthat, taken together, engage all of the multiple pathways thatmust be modified to preserve the cerebral vasculature and thusprotect brain tissue. Promising brain-relevant vascular bio-markers are described in the remainder of this section.
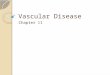
Arterial stiffness is now commonly assessed indirectly, bymeasuring pulse wave velocity—the speed with which bloodejected from the heart travels through various levels of thevascular tree (Hansen et al. 2006). The basic intuition behindpulse wave velocity is that compliant blood vessels are able toexpand, increasing their volume to accommodate a bolus ofnewly-arriving blood from the heart; the newly arriving bloodis thus more able to reside in the expanded vessel and travelthrough it more slowly. In contrast, less-compliant vesselscannot expand and thus have no choice but to immediatelysend the newly arriving blood down the vessel at a high speed.Non-invasive, tonometric devices are now available that mea-sure the blood pressure waveform at multiple arteries (forexample, at the carotid and femoral arteries) and quantify thedifference in arrival times of the pulse wave between the two(i.e., the “carotid-femoral pulse wave velocity”) as a proxymeasure of the velocity of the pulse wave through the centralarteries. Measurements of this type are relatively straightfor-ward to acquire and are easily tolerated by patients. However,there is some debate over which pair of arteries provides validproxy measures of the pulse wave velocity in which parts ofthe vasculature (Tanaka et al. 2009), and the correlation be-tween the proxymeasures and the true speed of the pulse wavedown any individual vessel is not perfect (Yamashina et al.2002). MRI techniques, meanwhile, are able to directly mea-sure the velocity of the pulse wave as it flows through specificarteries whose caliber is large enough to surpass the inherentspatial resolution limits ofMRI. Figure 2 shows an example ofMRI measurement of pulse wave velocity in the descendingaorta. MRI and ultrasound are also capable of directly
measuring variations in the diameter of large blood vesselsover the course of the cardiac cycle; together with concurrentmeasurement of blood pressure or flow in the vessel, thesemeasurements provide direct measurement of vessel compli-ance that is the primary physiological parameter of interest inarterial stiffness (Lehmann et al. 1993). However, compliancemeasurements are complicated by the fact that vessel diameterchanges may be quite small relative to the spatial resolution ofMRI or ultrasound. In summary, while sophisticated measuresof arterial stiffening are still under development, emergingclinical trials are now able to collect validated biomarkersthrough tonometric devices or imaging modalities.
Numerous markers of systemic inflammatory processeshave been developed and are commonly deployed in researchand clinical practice. Traditional, indirect measures of system-ic inflammation include C-reactive protein and homocysteine,while more modern markers include the suite of inflammatorycytokines (e.g., IL-1, IL-6, TNF-alpha) (Dinarello 1996) andvascular adhesion molecules (e.g., VCAM, ICAM, P-selectin,E-selectin) (Gearing and Newman 1993). While these mea-sures can be collected from cerebrospinal fluid, the assessmentof neuroinflammation, in particular the spatial distribution ofinflammatory activity throughout the brain, has remained anelusive target. Development of positron emission tomographyligands that specifically target inflammatory activity has beenongoing for many years, with PK11195 emerging as the firstviable compound. Due to its limited specificity, a number ofreplacements for PK11195 have emerged (Chauveau, Boutin,Van Camp, Dollé, and Tavitian 2008), many of which bindselectively to translocator protein 18 kDa (TSPO), which isupregulated in activated microglia (previously, TSPO hadbeen referred to as the peripheral benzodiazepine receptor orPBR) (Ching et al. 2012). There is currently no consensus onwhich of the several TSPO binding compounds is the mostspecific and easy to deploy. In addition, complications toTSPO as a neuroinflammation target have arisen, including
Fig. 2 Left: Phase-contrast MRI provides time series of 3D blood veloc-ity vectors in the aortic arch and descending aorta, and analytic softwaremeasures instantaneous blood flow rate at a set of user-defined analysisplanes (numbered). Center: Pulse wave velocity is estimated by dividing
the distance between analysis planes by the time interval (Δt) betweensystolic upstroke curves at those planes. Right: Pulse wave velocities of 4subjects are within the expected range of values and show an expectedgeneral trend of increase with age
Neuropsychol Rev (2014) 24:371–387 379

inter-individual variability in the binding affinity of TSPOligands driven by genetic variability in the TSPO gene(Owen et al. 2012). However, as TSPO ligands and otherneuroinflammation PET agents come on line, incorporatingthem into clinical trials of vascular risk factor treatmentstargeting inflammatory processes would be essential to under-standing benefits these treatments have for the brain.
Quantitative measures of atherosclerotic plaque burdenfrom ultrasound or MRI are also prominent due to theirrelevance to stroke, but more fine-grained measures of steno-sis and blood flow within the blood vessels supplying thebrain could provide deeper insight into the effects of athero-sclerotic plaque on cerebrovascular function. Typically, ultra-sound examination provides summary measures of stenosisand flow at isolated sites deemed differentially vulnerable toplaque deposition, such as the carotid bifurcation (Touboulet al. 2006). Atherosclerosis-orientedMRI methods, similarly,can provide a characterization of plaque composition at asmall number of carotid artery cross-sections (Yuan andKerwin 2004). However, MRI angiography techniques arenow capable of providing high-resolution characterization ofthe structure of arteries throughout the brain, thus enabling abrain-wide view of the capability of the cerebral vasculature todeliver blood to all brain tissue. An example angiogram, anddata showing vessel structural differences between young andelderly individuals, are shown in Fig. 3. Such characterizationof arterial structure could allow modeling at an individuallevel of what parts of the brain are differentially vulnerableto injury due to inadequate vascularization.While methods forisolating the structure of the cerebral vasculature from imag-ery have been presented (for example, (Flasque et al. 2001)), itis unclear what summary measures should be extracted fromsuch a structural description to best characterize vulnerabilityto cerebrovascular dysfunction. Identifying the best summarymeasures, and clarifying the utility of whole-brain arterialstructure in studies of cerebrovascular injury, is a promisingavenue for future research.
Develop Better Ways to Measure Duration and Severityof Vascular Injury Processes over Years or Decades
There is a key knowledge gap in how the time course ofexposure and severity of vascular risk factors relates to thetime course of brain injury accrual. Some evidence suggeststhat the duration of exposure is a crucial variable. For exam-ple, silent brain injury among the elderly appears to be morestrongly determined by the presence of vascular risk factors atmidlife rather than concurrently (Ninomiya et al. 2011); ifmidlife exposure is a valid proxy measure of duration ofexposure, this suggests that duration of exposure is a strongerdeterminant of effects on the brain. If both duration andseverity of exposure are key factors promoting silent braininjury, clinical trials of treatments to prevent silent brain injury
should ideally recruit participants that are well characterizedand homogeneous in terms of both of these variables; other-wise, those with greater duration of more severe vascular riskfactor exposure could be predisposed to poorer brain out-comes regardless of their current vascular risk factor status.Several epidemiological studies have been able to gather suchlong-term exposure data by measuring vascular parametersevery several years in roughly thousands of research partici-pants over the course of years to decades (Guo et al. 2009;Stewart et al. 2009; Wills et al. 2011, 2012). However, tradi-tionally such long-term exposure data has been limited to arelatively small pool of epidemiological cohorts, and thevascular measurements have been temporally sparse enoughthat they risk failing to provide an adequately fine-grainedcharacterization of vascular risk factor trajectory. In addition,these epidemiological studies had limited ability to provide afine-grained characterization of treatment trajectories, includ-ing initiation, adherence, and changes or cessation. Luckily,the ability to capture fine-grained trajectories of vascular riskfactor surveillance, exposure, and treatment have emergedwithin the past decade, with the development of electronicmedical record (EMR) databases that record each and everyclinical assessment, lab result, and pharmacy interaction oc-curring longitudinally in tens to hundreds of thousands ofhealth system enrollees. A few health care systems that wereearly adopters of EMR and invested heavily in the medicalinformatics technology required to characterize long timecourses of exposure are now positioned to recruit participantsfor research studies based on decade-long trajectory informa-tion (two examples are the Veterans Affairs system (Siegelet al. 2007) and Kaiser Permanente (Adams, Uratsu, Dyer, andet al. 2013)). However, there are still a number of technicalhurdles to such studies. First, automated extraction of suchtrajectory information from individual EMR databases re-mains a difficult task due to the complexity and heterogeneityof represented clinical interaction data. While much of therelevant data is in a standardized, easy to manipulate format,some critical data remain in freely-typed notes that are pro-hibitively time consuming to parse manually and difficult toextract information from automatically. Large-scale, multi-sitestudies have been stymied by a lack of data standardizationacross disparate EMR systems. Finally, while modeling ofindividual longitudinal trajectory data is already a major re-search problem in biostatistics (see for example (Harvey et al.2003)), fine-grained EMR data poses additional analytic prob-lems due to the presence of multiple, correlated, high-dimensional trajectories (of vascular parameters, clinical in-teractions, and treatment behaviors) per individual.Addressing these technical challenges will provide a majoropportunity to design studies that better characterize vasculareffects on the brain in the context of lifetime exposures.
Even within EMR databases, measurement of vascularparameters over time requires interaction with patients in a
380 Neuropsychol Rev (2014) 24:371–387

clinical setting. This is especially problematic given the earliercontention that vascular injury processes, and vascular effectson the brain, may commence early in the lifespan, amongnominally healthy young individuals that are otherwiseasymptomatic and unlikely to believe that frequent, routineclinical evaluations confer much benefit to them (Berensonet al. 1998; Maillard et al. 2012). In addition, recent researchsuggests that office measurement of certain vascular parame-ters, especially blood pressure, provides an inadequate char-acterization of vascular status (Sega et al. 2005; Verdecchiaet al. 1994). Wearable electronic health monitors that haveemerged in recent years have the potential to provide surveil-lance of systemic vascular processes around the clock in anunobtrusive manner. Various devices are able to providechronic measurement of blood pressure, pulse rate, bloodglucose, and even the electrophysiology of the heart. Timecourses of data from these devices can then be transmittedfrom devices to cell phones and onward to health care pro-viders who can incorporate this fine-grained longitudinal vas-cular characterization into EMR. The comfort and conve-nience of these devices, as well as the threat of electronic theft
of such highly sensitive personal health data, are ongoingconcerns. Nonetheless, continued development of wearablehealth devices could provide vastly superior characterizationof time courses of vascular risk duration and severity at agranularity never seen before, and this information could beused to better control clinical trials for the vascular history ofparticipants.
Conclusion
While there is ample evidence that individuals possessing ahistory of vascular risk factor exposure have poorer outcomeslate in life with respect to clinically-silent brain injury andclinically relevant cognitive decline, there is a relatively littleconvincing evidence that current protocols for vascular riskfactor treatment are adequate to prevent these outcomes.Identifying vascular risk factor treatment protocols that opti-mally reduce risk of late-life silent brain injury and cognitivedecline will require investigating critical treatment windows,interactions between vascular and other biological processes
Fig. 3 Fine grained MRI measurement of internal carotid artery (ICA)radii. Top left: The ICA is clearly visible on a 3D time-of-flight MRangiography. Topmiddle: 3Dmodeling of the vessel allows identificationof a vessel center line and calculation of vessel radius at each point alongthe vessel. Top right: Plot of local radius of the ICA as a function ofposition along the ICA center line reveals intra- and inter-individualvariability in ICA radius in a typical young and elderly participant.
Lower left: The ratio of minimum to maximum vessel radius along theICA was significantly smaller (p<0.001, bottom left) among a group of10 elderly individuals compared to a group of 10 young adults. Lowermiddle: Lesser values of this ratio, a summary measure of stenosis, wasassociated with lesser gray matter volume in the older subjects (p=0.02,bottom right)
Neuropsychol Rev (2014) 24:371–387 381

of aging, differential vulnerability to silent brain injury, andoptimal targets for vascular parameters. Clinical trials of vas-cular treatments with brain injury outcomes are desperatelyneeded to investigate these questions. Sensitive and robustbiomarkers of the cerebral and central vasculature, and bettercharacterization of time courses of vascular risk factor expo-sure are needed to clarify what insights should be derivedfrom these trials. It is expected that longitudinal biomedicalimaging, data mining of electronic medical records, andchronic ecological monitoring devices will play a critical rolein this characterization effort.
Acknowledgments This work was supported by NIH grants P30AG010129 and K01 AG030514, as well as grants from the CaliforniaState Department of Public Health and the Alzheimer’s Association.
References
Adams, A., Uratsu, C., Dyer, W., et al. (2013). Health systemfactors and antihypertensive adherence in a racially and eth-nically diverse cohort of new users. JAMA Internal Medicine,173(1), 54–61.
Alexander, C. M., Landsman, P. B., Teutsch, S. M., Haffner, S. M., ThirdNational, H, Nutrition Examination, S, & National CholesterolEducation, P. (2003). NCEP-defined metabolic syndrome, diabetes,and prevalence of coronary heart disease among NHANES IIIparticipants age 50 years and older. Diabetes, 52(5), 1210–1214.
Amarenco, P., Cohen, A., Tzourio, C., Bertrand, B., Hommel, M.,Besson, G., & Bousser, M. G. (1994). Atherosclerotic disease ofthe aortic arch and the risk of ischemic stroke. The New EnglandJournal of Medicine, 331(22), 1474–1479. doi:10.1056/NEJM199412013312202.
Appelman, A. P., van der Graaf, Y., Vincken, K. L., Tiehuis, A. M.,Witkamp, T. D., Mali, W. P., & Geerlings, M. I. (2008). Totalcerebral blood flow, white matter lesions and brain atrophy: theSMART-MR study. Journal of Cerebral Blood Flow andMetabolism, 28(3), 633–639.
Au, R.,Massaro, J.M.,Wolf, P. A., Young,M. E., Beiser, A., Seshadri, S.,& DeCarli, C. (2006). Association of white matter hyperintensityvolume with decreased cognitive functioning: the FraminghamHeart Study. Archives of Neurology, 63(2), 246–250.
Barnes, D. E., & Yaffe, K. (2011). The projected effect of risk factorreduction on Alzheimer's disease prevalence. Lancet Neurology,10(9), 819–828. doi:10.1016/S1474-4422(11)70072-2.
Barnes, J., Carmichael, O. T., Leung, K. K., Schwarz, C., Ridgway, G. R.,Bartlett, J. W., & Biessels, G. J. (2013). Vascular and Alzheimer’sdisease markers independently predict brain atrophy rate inAlzheimer’s disease neuroimaging initiative controls. Neurobiologyof Aging, 34(8), 1996–2002.
Berenson, G. S., Srinivasan, S. R., Bao, W., Newman,W. P., Tracy, R. E.,& Wattigney, W. A. (1998). Association between multiple cardio-vascular risk factors and atherosclerosis in children and youngadults. New England Journal of Medicine, 338(23), 1650–1656.
Birns, J., Morris, R., Donaldson, N., & Kalra, L. (2006). The effects ofblood pressure reduction on cognitive function: a review of effectsbased on pooled data from clinical trials. Journal of Hypertension,24(10), 1907–1914.
Biswal, B. B., Mennes,M., Zuo, X. N., Gohel, S., Kelly, C., Smith, S.M.,& Milham, M. P. (2010). Toward discovery science of human brainfunction. Proceedings of the National Academy of Sciences of the
United States of America, 107(10), 4734–4739. doi:10.1073/pnas.0911855107.
Bombois, S., Debette, S., Bruandet, A., Delbeuck, X., Delmaire, C., Leys,D., & Pasquier, F. (2008). Vascular subcortical hyperintensitiespredict conversion to vascular and mixed dementia in MCI patients.Stroke, 39(7), 2046–2051.
Bots, M. L., Breteler, M. M. B., Hofman, A., Grobbee, D. E., vanSwieten, J. C., van Gijn, J., & de Jong, P. T. V. M. (1993).Cerebral white matter lesions and atherosclerosis in the RotterdamStudy. The Lancet, 341(8855), 1232–1237.
Brayne, C., Richardson, K., Matthews, F. E., Fleming, J., Hunter, S.,Xuereb, J. H., & The Cambridge City over-75 s Cohort studyneuropathology, c. (2009). Neuropathological correlates of dementiain over-80-year-Old brain donors from the population-basedCambridge city over-75 s cohort (CC75C) study. Journal ofAlzheimer's Disease, 18(3), 645–658.
Brundel, M., van den Heuvel, M., de Bresser, J., Kappelle, L. J., Biessels,G. J., & Utrecht Diabetic Encephalopathy Study, G. (2010).Cerebral cortical thickness in patients with type 2 diabetes.Journal of Neurological Sciences, 299(1–2), 126–130. doi:10.1016/j.jns.2010.08.048.
Cardenas, V. A., Reed, B., Chao, L. L., Chui, H., Sanossian, N., Decarli,C. C., & Weiner, M. W. (2012). Associations among vascular riskfactors, carotid atherosclerosis, and cortical volume and thickness inolder adults. Stroke. doi:10.1161/STROKEAHA.112.659722.
Carlson, N. E., Moore, M. M., Dame, A., Howieson, D., Silbert, L. C.,Quinn, J. F., & Kaye, J. A. (2008). Trajectories of brain loss in agingand the development of cognitive impairment. Neurology, 70(11),828–833.
Carmelli, D., Swan, G. E., Reed, T., Wolf, P. A., Miller, B. L., & DeCarli,C. (1999). Midlife cardiovascular risk factors and brain morphologyin identical older male twins. Neurology, 52(6), 1119.
Carmichael, O., & Lockhart, S. (2012). The role of diffusion tensorimaging in the study of cognitive aging. Current Topics inBehavioral Neurosciences, 11, 289–320. doi:10.1007/7854_2011_176.
Carmichael, O. T., Kuller, L. H., Lopez, O. L., Thompson, P. M., Dutton,R. A., Lu, A., & Becker, J. T. (2007). Ventricular volume anddementia progression in the cardiovascular health study.Neurobiology of Aging, 28(3), 389–397.
Chauveau, F., Boutin, H., Van Camp, N., Dollé, F., & Tavitian, B. (2008).Nuclear imaging of neuroinflammation: a comprehensive review of[11C] PK11195 challengers. European Journal of NuclearMedicineand Molecular Imaging, 35(12), 2304–2319.
Chen, Y., Gurol, M., Rosand, J., Viswanathan, A., Rakich, S., Groover, T.,& Smith, E. (2006). Progression of white matter lesions and hemor-rhages in cerebral amyloid angiopathy. Neurology, 67(1), 83–87.
Ching, A. S. C., Kuhnast, B., Damont, A., Roeda, D., Tavitian, B., &Dollé, F. (2012). Current paradigm of the 18-kDa translocator pro-tein (TSPO) as a molecular target for PET imaging in neuroinflam-mation and neurodegenerative diseases. Insights into imaging, 3(1),111–119.
Chobanian, A. V., Bakris, G. L., Black, H. R., Cushman,W. C., Green, L.A., Izzo, J. L., Jr., & Roccella, E. J. (2003). The seventh report of thejoint national committee on prevention, detection, evaluation, andtreatment of high blood pressure: the JNC 7 report. JAMA, 289(19),2560–2572. doi:10.1001/jama.289.19.2560.
Chou, S.-Y., Shulman, J., Keenan, B., Secor, E., Buchman, A., Schneider,J., & De Jager, P. (2013). Genetic susceptibility for ischemic infarc-tion and arteriolosclerosis based on neuropathologic evaluations.Cerebrovascular Diseases, 36(3), 181–188.
Cordonnier, C., Al-Shahi Salman, R., &Wardlaw, J. (2007). Spontaneousbrain microbleeds: systematic review, subgroup analyses and stan-dards for study design and reporting. Brain, 130(8), 1988–2003.
Crawford, A. G., Cote, C., Couto, J., Daskiran,M., Gunnarsson, C., Haas,K., & Schuette, R. (2010). Prevalence of obesity, type II diabetes
382 Neuropsychol Rev (2014) 24:371–387

mellitus, hyperlipidemia, and hypertension in the united states:findings from the GE centricity electronic medical record database.Population Health Management, 13(3), 151–161. doi:10.1089/pop.2009.0039.
D’Esposito, M., Zarahn, E., Aguirre, G. K., & Rypma, B. (1999). Theeffect of normal aging on the coupling of neural activity to the boldhemodynamic response. NeuroImage, 10(1), 6–14.
Dai, W., Lopez, O. L., Carmichael, O. T., Becker, J. T., Kuller, L. H., &Gach, H. M. (2008). Abnormal regional cerebral blood flow incognitively normal elderly subjects with hypertension. Stroke,39(2), 349–354.
Das, R. R., Seshadri, S., Beiser, A. S., Kelly-Hayes,M., Au, R., Himali, J.J., & Wolf, P. A. (2008). Prevalence and correlates of silent cerebralinfarcts in the Framingham offspring study. Stroke, 39(11), 2929–2935.
Debette, S., & Markus, H. S. (2010). The clinical importance of whitematter hyperintensities on brain magnetic resonance imaging: sys-tematic review and meta-analysis. BMJ, 341, c3666.
Debette, S., Bis, J. C., Fornage, M., Schmidt, H., Ikram, M. A.,Sigurdsson, S., & van der Lugt, A. (2010). Genome-wide associa-tion studies of MRI-defined brain infarcts meta-analysis from theCHARGE consortium. Stroke, 41(2), 210–217.
Debette, S., Seshadri, S., Beiser, A., Au, R., Himali, J. J., Palumbo, C., &DeCarli, C. (2011). Midlife vascular risk factor exposure acceleratesstructural brain aging and cognitive decline. Neurology, 77(5), 461–468.
DeCarli, C., Murphy, D. G., Tranh, M., Grady, C. L., Haxby, J. V.,Gillette, J. A., et al. (1995). The effect of white matter hyperintensityvolume on brain structure, cognitive performance, and cerebralmetabolism of glucose in 51 healthy adults. Neurology, 45(11),2077–2084.
DeCarli, C., Massaro, J., Harvey, D., Hald, J., Tullberg, M., Au, R., &Wolf, P. A. (2005). Measures of brain morphology and infarction inthe Framingham heart study: establishing what is normal.Neurobiology of Aging, 26(4), 491–510.
Dietschy, J. M., & Turley, S. D. (2001). Cholesterol metabolism in thebrain. Current Opinion in Lipidology, 12(2), 105–112.
Dinarello, C. (1996). Role of pro-and anti-inflammatory cytokines duringinflammation: experimental and clinical findings. Journal ofBiological Regulators and Homeostatic Agents, 11(3), 91–103.
Dirnagl, U., Iadecola, C., & Moskowitz, M. A. (1999). Pathobiology ofischaemic stroke: an integrated view. Trends in Neurosciences,22(9), 391–397.
Dufouil, C., Chalmers, J., Coskun, O., Besancon, V., Bousser, M.-G.,Guillon, P., & PROGRESS MRI Substudy Investigators. (2005).Effects of blood pressure lowering on cerebral white matterhyperintensities in patients with stroke. Circulation, 112(11),1644–1650. doi:10.1161/circulationaha.104.501163.
Ebrahim, S., Papacosta, O., Whincup, P., Wannamethee, G., Walker, M.,Nicolaides, A. N., & Rumley, A. (1999). Carotid plaque, intimamedia thickness, cardiovascular risk factors, and prevalent cardio-vascular disease in men and women the British regional heart study.Stroke, 30(4), 841–850.
Fazekas, F., Kleinert, R., Offenbacher, H., Schmidt, R., Kleinert, G., Payer,F., & Lechner, H. (1993). Pathologic correlates of incidental MRIwhite matter signal hyperintensities. Neurology, 43(9), 1683–1683.
Fazekas, F., Schmidt, R., Kleinert, R., Kapeller, P., Roob, G., & Flooh, E.(1998). The spectrum of age-associated brain abnormalities: theirmeasurement and histopathological correlates. Journal of NeuralTransmission, Supplement, 53, 31–39.
Flasque, N., Desvignes, M., Constans, J.-M., & Revenu, M. (2001).Acquisition, segmentation and tracking of the cerebral vascular treeon 3D magnetic resonance angiography images. Medical ImageAnalysis, 5(3), 173–183.
Fornage, M., Chiang, Y. A., O’Meara, E. S., Psaty, B. M., Reiner, A. P.,Siscovick, D. S., & Longstreth, W. T. (2008). Biomarkers of
inflammation and MRI-defined small vessel disease of the brain:the cardiovascular health study. Stroke, 39(7), 1952–1959. doi:10.1161/strokeaha.107.508135.
Gearing, A. J., & Newman,W. (1993). Circulating adhesion molecules indisease. Immunology Today, 14(10), 506–512.
Gilbert, J., & Vinters, H. (1983). Cerebral amyloid angiopathy: incidenceand complications in the aging brain. I. Cerebral hemorrhage.Stroke, 14(6), 915–923.
Go, A. S., Mozaffarian, D., Roger, V. L., Benjamin, E. J., Berry, J. D.,Borden,W. B.,… Stroke Statistics, S. (2013). Heart disease and strokestatistics–2013 update: a report from the American heart association.Circulation, 127(1), e6–e245. doi:10.1161/CIR.0b013e31828124ad.
Godin, O., Tzourio, C., Maillard, P., Mazoyer, B., & Dufouil, C. (2011).Antihypertensive treatment and change in blood pressure Are asso-ciated with the progression of white matter lesion VolumesClinicalperspective the three-city (3C)–Dijon magnetic resonance imagingstudy. Circulation, 123(3), 266–273.
Goos, J. D., Henneman, W. J., Sluimer, J. D., Vrenken, H., Sluimer, I. C.,Barkhof, F., & van der Flier, W. M. (2010). Incidence of cerebralmicrobleeds: a longitudinal study in a memory clinic population.Neuro logy, 74 (24) , 1954–1960 . do i :10 .1212 /WNL.0b013e3181e396ea.
Gorelick, P. B., Scuteri, A., Black, S. E., Decarli, C., Greenberg, S. M.,Iadecola, C., & Seshadri, S. (2011). Vascular contributions to cog-nitive impairment and dementia: a statement for healthcare profes-sionals from the American heart association/american stroke asso-ciation. Stroke, 42(9), 2672–2713. doi:10.1161/STR.0b013e3182299496.
Gouw, A. A., Seewann, A., van der Flier, W.M., Barkhof, F., Rozemuller,A. M., Scheltens, P., & Geurts, J. J. (2011). Heterogeneity of smallvessel disease: a systematic review of MRI and histopathologycorrelations. Journal of Neurology, Neurosurgery & Psychiatry,82(2), 126–135.
Grimmer, T., Faust, M., Auer, F., Alexopoulos, P., Förstl, H., Henriksen,G., & Drzezga, A. (2012). White matter hyperintensities predictamyloid increase in Alzheimer’s disease. Neurobiology of Aging,33(12), 2766–2773.
Guo, X., Pantoni, L., Simoni, M., Bengtsson, C., Björkelund, C., Lissner,L., & Skoog, I. (2009). Blood pressure components and changes inrelation to white matter lesions.Hypertension, 54(1), 57–62. doi:10.1161/hypertensionaha.109.129700.
Guzman, V. A., Carmichael, O. T., Schwarz, C., Tosto, G., Zimmerman,M. E., & Brickman, A.M. (2013).White matter hyperintensities andamyloid are independently associated with entorhinal cortex volumeamong individuals with mild cognitive impairment. Alzheimer’s &Dementia, 9(5), s124–s131.
Haight, T., Carmichael, O., Landau, S., Schwarz, C., DeCarli, C., &Jagust, W. (2013). Dissociable effects of Alzheimer’s Disease andwhite matter hyperintensities on brain metabolism. Archives ofneurology, In Press.
Hajjar, I., Zhao, P., Alsop, D., & Novak, V. (2010). Hypertension andcerebral vasoreactivity a continuous arterial spin labeling magneticresonance imaging study. Hypertension, 56(5), 859–864.
Hajjar, I., Brown, L., Mack, W. J., & Chui, H. (2012). Impact of angio-tensin receptor blockers on Alzheimer disease neuropathology in alarge brain autopsy SeriesARB impact on AD neuropathology.Archives of Neurology, 69(12), 1632–1638.
Hajjar, I., Hart, M., Chen, Y. L., Mack, W., Novak, V., Chui, H., &Lipsitz, L. (2013). Antihypertensive therapy and cerebral hemody-namics in executive mild cognitive impairment: results of a pilotrandomized clinical trial. Journal of the American GeriatricsSociety, 61(2), 194–201. doi:10.1111/jgs.12100.
Hansen, T. W., Staessen, J. A., Torp-Pedersen, C., Rasmussen, S., Thijs,L., Ibsen, H., & Jeppesen, J. (2006). Prognostic value of aortic pulsewave velocity as index of arterial stiffness in the general population.Circulation, 113(5), 664–670.
Neuropsychol Rev (2014) 24:371–387 383

Harvey, D., Laurel, B., & Mungas, D. (2003). Multivariate modeling oftwo associated cognitive outcomes in a longitudinal study. Journalof Alzheimer’s Disease, 5(5), 357–365.
Havlik, R. J., Foley, D. J., Sayer, B., Masaki, K., White, L., & Launer, L.J. (2002). Variability in midlife systolic blood pressure is related tolate-life brain white matter lesions. Stroke, 33(1), 26–30. doi:10.1161/hs0102.101890.
Hedden, T., Mormino, E. C., Amariglio, R. E., Younger, A. P., Schultz, A.P., Becker, J. A., & Rentz, D. M. (2012). Cognitive profile of amyloidburden and white matter hyperintensities in cognitively normal olderadults. The Journal of Neuroscience, 32(46), 16233–16242.
Henskens, L. H., Kroon, A. A., van Oostenbrugge, R. J., Gronenschild, E.H., Fuss-Lejeune, M. M., Hofman, P. A., & de Leeuw, P. W. (2008).Increased aortic pulse wave velocity is associated with silent cere-bral small-vessel disease in hypertensive patients. Hypertension,52(6), 1120–1126.
Höglund, K., Wiklund, O., Vanderstichele, H., Eikenberg, O.,Vanmechelen, E., & Blennow, K. (2004). Plasma levels of β-amyloid (1–40), β-amyloid (1–42), and total β-amyloid remainunaffected in adult patients with hypercholesterolemia after treat-ment with statins. Archives of Neurology, 61(3), 333–337.
Hoshi, T., Kitagawa, K., Yamagami, H., Furukado, S., Hougaku, H., &Hori, M. (2005). Relations of serum high-sensitivity C-reactiveprotein and interleukin-6 levels with silent brain infarction. Stroke,36(4), 768–772.
Hsu, J. L., Chen, Y. L., Leu, J. G., Jaw, F. S., Lee, C. H., Tsai, Y. F., &Leemans, A. (2012). Microstructural white matter abnormalities intype 2 diabetes mellitus: a diffusion tensor imaging study.NeuroImage, 59(2), 1098–1105. doi:10.1016/j.neuroimage.2011.09.041.
Iliff, J. J., Wang, M., Liao, Y., Plogg, B. A., Peng, W., Gundersen, G. A.,& Goldman, S. A. (2012). A paravascular pathway facilitates CSFflow through the brain parenchyma and the clearance of interstitialsolutes, including amyloid β. Science Translational Medicine,4(147), 147ra111–147ra111.
Imabayashi, E., Matsuda, H., Yoshimaru, K., Kuji, I., Seto, A., Shimano,Y., & Araki, N. (2011). Pilot data on telmisartan short-term effectson glucose metabolism in the olfactory tract in Alzheimer’s disease.Brain and behavior, 1(2), 63–69.
Ishikawa, J., Tamura, Y., Hoshide, S., Eguchi, K., Ishikawa, S., Shimada,K., & Kario, K. (2007). Low-grade inflammation is a risk factor forclinical stroke events in addition to silent cerebral infarcts inJapanese older hypertensives the Jichi Medical School ABPMStudy, wave 1. Stroke, 38(3), 911–917.
Jagust, W. J., Zheng, L., Harvey, D. J., Mack, W. J., Vinters, H. V.,Weiner, M. W., & Chui, H. C. (2008). Neuropathological basis ofmagnetic resonance images in aging and dementia. Annals ofNeurology, 63(1), 72–80. doi:10.1002/ana.21296.
Jeerakathil, T., Wolf, P. A., Beiser, A., Massaro, J., Seshadri, S.,D’Agostino, R. B., & DeCarli, C. (2004). Stroke risk profile predictswhite matter hyperintensity volume: the Framingham Study. Stroke,35(8), 1857–1861.
Jefferson, A., Massaro, J., Wolf, P., Seshadri, S., Au, R., Vasan, R., &Lipinska, I. (2007). Inflammatory biomarkers are associated withtotal brain volume the Framingham heart study. Neurology, 68(13),1032–1038.
Joas, E., Bäckman, K., Gustafson, D., Östling, S., Waern, M., Guo, X., &Skoog, I. (2012). Blood pressure trajectories from midlife to late lifein relation to dementia in women followed for 37 years.Hypertension, 59(4), 796–801.
Kannel, W. B., & Gordan, T. (1978). Evaluation of cardiovascular risk inthe elderly: the Framingham study. Bulletin of the New YorkAcademy of Medicine, 54(6), 573–591.
Kiechl, S., &Willeit, J. (1999). The natural course of atherosclerosis. PartII: vascular remodeling. Bruneck Study Group. ArteriosclerThrombosis Vascular Biology, 19(6), 1491–1498.
Kimura, Y., Kitagawa, K., Oku, N., Kajimoto, K., Kato, H., Tanaka, M.,& Hatazawa, J. (2010). Blood pressure lowering with valsartan isassociated with maintenance of cerebral blood flow and cerebralperfusion reserve in hypertensive patients with cerebral small vesseldisease. Journal of Stroke and Cerebrovascular Diseases, 19(2),85–91.
Kin, T., Yamano, S., Sakurai, R., Kajitani, M., Okahashi, Y., Nishiura, N.,& Ueno, S. (2007). Carotid atherosclerosis is associated with brainatrophy in Japanese elders. Gerontology, 53(1), 1–6. doi:10.1159/000095385.
Kivipelto, M., Helkala, E. L., Laakso, M. P., Hanninen, T., Hallikainen,M., Alhainen, K., & Nissinen, A. (2001). Midlife vascular riskfactors and Alzheimer’s disease in later life: longitudinal, populationbased study. BMJ, 322(7300), 1447–1451.
Knopman, D. S., & Roberts, R. (2010). Vascular risk factors: imaging andneuropathologic correlates. Journal of Alzheimer’s Disease, 20(3),699–709. doi:10.3233/JAD-2010-091555.
Knopman, Boland, L. L., Mosley, T., Howard, G., Liao, D., Szklo, M., &Atherosclerosis Risk in Communities Study, I. (2001).Cardiovascular risk factors and cognitive decline in middle-agedadults. Neurology, 56(1), 42–48.
Knopman, D. S., Penman, A. D., Catellier, D. J., Coker, L. H., Shibata, D.K., Sharrett, A. R., & Mosley, T. H., Jr. (2011). Vascular risk factorsand longitudinal changes on brainMRI: the ARIC study.Neurology,76(22), 1879–1885.
Korf, E. S. C., White, L. R., Scheltens, P., & Launer, L. J. (2004). Midlifeblood pressure and the risk of Hippocampal atrophy. Hypertension,44(1), 29–34. doi:10.1161/01.HYP.0000132475.32317.bb.
Kuller, L. H., Lopez, O. L., Newman, A., Beauchamp, N. J., Burke, G.,Dulberg, C., & Haan, M. N. (2003). Risk factors for dementia in thecardiovascular health cognition study. Neuroepidemiology, 22(1),13–22. doi:10.1159/000067109.
Kuller, L. H., Margolis, K. L., Gaussoin, S. A., Bryan, N. R., Kerwin, D.,Limacher, M., & Robinson, J. G. (2010). Relationship of hyperten-sion, blood pressure, and blood pressure control with white matterabnormalities in the Women’s health initiative memory study(WHIMS)—MRI trial. The Journal of Clinical Hypertension,12(3), 203–212.
Launer, L. J., Hughes, T., Yu, B., Masaki, K., Petrovitch, H., Ross, G.W.,& White, L. R. (2010). Lowering midlife levels of systolic bloodpressure as a public health strategy to reduce late-life dementia:perspective from the Honolulu heart program/Honolulu Asia agingstudy. Hypertension, 55(6), 1352–1359. doi:10.1161/HYPERTENSIONAHA.109.147389.
Le Bihan, D. (2003). Looking into the functional architecture of the brainwith diffusion MRI. Nature Review Neuroscience, 4(6), 469–480.doi:10.1038/nrn1119.
Lehmann, E., Parker, J., Hopkins, K., Taylor, M., & Gosling, R. (1993).Validation and reproducibility of pressure-corrected aortic distensi-bility measurements using pulse-wave-velocity Doppler ultrasound.Journal of Biomedical Engineering, 15(3), 221–228.
Libby, P., Ridker, P. M., & Maseri, A. (2002). Inflammation and athero-sclerosis. Circulation, 105(9), 1135–1143.
Liu, Q., Zerbinatti, C. V., Zhang, J., Hoe, H.-S., Wang, B., Cole, S. L., &Bu, G. (2007). Amyloid precursor protein regulates brain apolipo-protein E and cholesterol metabolism through lipoprotein receptorLRP1. Neuron, 56(1), 66–78.
Loessner, A., Alavi, A., Lewandrowski, K. U., Mozley, D., Souder, E., &Gur, R. E. (1995). Regional cerebral function determined by FDG-PET in healthy volunteers: normal patterns and changes with age.Journal of Nuclear Medicine, 36(7), 1141–1149.
Logothetis, N. K., & Pfeuffer, J. (2004). On the nature of the BOLD fMRIcontrast mechanism. Magnetic Resonance Imaging, 22(10), 1517–1531. doi:10.1016/j.mri.2004.10.018.
Lopez, O. L., Jagust, W. J., Dulberg, C., Becker, J. T., DeKosky, S. T.,Fitzpatrick, A., & Kuller, L. H. (2003). Risk factors for mild
384 Neuropsychol Rev (2014) 24:371–387

cognitive impairment in the cardiovascular health study cognitionstudy: part 2. Archives of Neurology, 60(10), 1394–1399.
Madamanchi, N. R., Vendrov, A., & Runge, M. S. (2005). Oxidativestress and vascular disease. Arteriosclerosis, Thrombosis, andVascular Biology, 25(1), 29–38. doi:10.1161/01.atv.0000150649.39934.13.
Maillard, P., Seshadri, S., Beiser, A., Himali, J., Au, R., Fletcher, E., &DeCarli, C. (2012). Effects of systolic blood pressure on whitematter integrity in young adults: from the Framingham heart study.The Lancet Neurology, 11(12), 1039–1047.
Manolio, T. A., Burke, G. L., O’Leary, D. H., Evans, G., Beauchamp, N.,Knepper, L., & Ward, B. (1999). Relationships of cerebral MRIfindings to ultrasonographic carotid atherosclerosis in older adults :the cardiovascular health study. CHS Collaborative ResearchGroup. Arterioscler Thrombosis Vasculaer Biology, 19(2), 356–365.
Marchant, N. L., Reed, B. R., DeCarli, C. S., Madison, C.M.,Weiner, M.W., Chui, H. C., & Jagust, W. J. (2012). Cerebrovascular disease,beta-amyloid, and cognition in aging.Neurobiology of Aging, 33(5),1006. e1025–1006. e1036.
Matsumoto, S., Shimodozono, M., Miyata, R., & Kawahira, K. (2009).Effect of the angiotensin II type 1 receptor antagonist olmesartan oncerebral hemodynamics and rehabilitation outcomes in hypertensivepost-stroke patients. Brain Injury, 23(13–14), 1065–1072.
McGeer, P. L., & McGeer, E. G. (2001). Polymorphisms in inflammatorygenes and the risk of Alzheimer disease. Archives of Neurology,58(11), 1790–1792.
McGuinness, B., Todd, S., Passmore, P., & Bullock, R. (2009). Bloodpressure lowering in patients without prior cerebrovascular diseasefor prevention of cognitive impairment and dementia. CochraneDatabase Syst Rev, (4), CD004034. doi: 10.1002/14651858.CD004034.pub3 [doi].
Miranda, P. J., DeFronzo, R. A., Califf, R. M., & Guyton, J. R. (2005).Metabolic syndrome: definition, pathophysiology, and mechanisms.American Heart Journal, 149(1), 33–45. doi:10.1016/j.ahj.2004.07.013.
Mitchell, G. F., van Buchem, M. A., Sigurdsson, S., Gotal, J. D.,Jonsdottir, M. K., Kjartansson, Ó., & Gudnason, V. (2011).Arterial stiffness, pressure and flow pulsatility and brain structureand function: the Age, Gene/Environment Susceptibility–ReykjavikStudy. Brain, 134(11), 3398–3407.
Miwa, K., Tanaka, M., Okazaki, S., Furukado, S., Sakaguchi, M., &Kitagawa, K. (2011). Relations of blood inflammatory marker levelswith cerebral microbleeds. Stroke, 42(11), 3202–3206.
Moran, C., Phan, T. G., Chen, J., Blizzard, L., Beare, R., Venn, A., &Srikanth, V. (2013). Brain atrophy in type 2 diabetes: regionaldistribution and influence on cognition. Diabetes Care. doi:10.2337/dc13-0143.
Morris, J. C., & Price, A. L. (2001). Pathologic correlates of nondementedaging, mild cognitive impairment, and early-stage Alzheimer’s dis-ease. Journal of Molecular Neuroscience, 17(2), 101–118.
Muller, M., van der Graaf, Y., Algra, A., Hendrikse, J., Mali, W. P., &Geerlings, M. I. (2011). Carotid atherosclerosis and progression ofbrain atrophy: the SMART-MR study. Annals of Neurology, 70(2),237–244. doi:10.1002/ana.22392.
Muller, M., van der Graaf, Y., Visseren, F. L., Mali, W. P., Geerlings, M.I., & for the, S. S. G. (2012). Hypertension and longitudinal changesin cerebral blood flow: the SMART-MR study. Annals of Neurology.doi:10.1002/ana.23554.
Ninomiya, T., Ohara, T., Hirakawa, Y., Yoshida, D., Doi, Y., Hata, J., &Kiyohara, Y. (2011).Midlife and late-life blood pressure and dementiain Japanese elderly the hisayama study. Hypertension, 58(1), 22–28.
Novak, V., & Hajjar, I. (2010). The relationship between blood pressureand cognitive function. Nature Reviews Cardiology, 7(12), 686–698. doi:10.1038/nrcardio.2010.161.
O’Leary, D., Polak, J., Kronmal, R., Kittner, S., Bond, M., Wolfson, S.,Jr., & Savage, P. (1992). Distribution and correlates of
sonographically detected carotid artery disease in the cardiovascularhealth study. The CHS Collaborative Research Group. Stroke,23(12), 1752–1760.
O’Rourke, M. F., & Safar, M. E. (2005). Relationship between aorticstiffening and microvascular disease in brain and kidney cause andlogic of therapy. Hypertension, 46(1), 200–204.
O’Sullivan,M., Morris, R. G., Huckstep, B., Jones, D. K.,Williams, S. C.R., & Markus, H. S. (2004). Diffusion tensor MRI correlates withexecutive dysfunction in patients with ischaemic leukoaraiosis.Journal Neurology Neurosurgery Psychiatry, 75(3), 441–447.
Ohmine, T., Miwa, Y., Yao, H., Yuzuriha, T., Takashima, Y., Uchino, A.,& Sasaguri, T. (2008). Association between arterial stiffness andcerebral white matter lesions in community-dwelling elderly sub-jects. Hypertension Research, 31(1), 75–81.
Owen, D. R., Yeo, A. J., Gunn, R. N., Song, K., Wadsworth, G., Lewis,A., & Parker, C. A. (2012). An 18-kDa translocator protein (TSPO)polymorphism explains differences in binding affinity of the PETradioligand PBR28. Journal of Cerebral Blood Flow&Metabolism,32(1), 1–5.
Pantoni, L., & Garcia, J. H. (1997). Pathogenesis of leukoaraiosis : areview. Stroke, 28(3), 652–659. doi:10.1161/01.str.28.3.652.
Pappolla, M., Bryant-Thomas, T., Herbert, D., Pacheco, J., Garcia, M. F.,Manjon,M., & Zambon, D. (2003).Mild hypercholesterolemia is anearly risk factor for the development of Alzheimer amyloid pathol-ogy. Neurology, 61(2), 199–205.
Parkes, L. M., Rashid, W., Chard, D. T., & Tofts, P. S. (2004). Normalcerebral perfusion measurements using arterial spin labeling: repro-ducibility, stability, and age and gender effects.Magnetic Resonancein Medicine, 51(4), 736–743. doi:10.1002/mrm.20023.
Petersen, E. T., Zimine, I., Ho, Y. C., & Golay, X. (2006). Non-invasivemeasurement of perfusion: a critical review of arterial spin labellingtechniques. The British Journal of Radiology, 79(944), 688–701.doi:10.1259/bjr/67705974.
Pico, F., Dufouil, C., Levy, C., Besancon, V., de Kersaint-Gilly, A.,Bonithon-Kopp, C., & Alperovitch, A. (2002). Longitudinal studyof carotid atherosclerosis and white matter hyperintensities: theEVA-MRI cohort. Cerebrovasc Dis, 14(2), 109–115.
Poels, M. M., Vernooij, M. W., Ikram, M. A., Hofman, A., Krestin, G. P.,van der Lugt, A., & Breteler, M. M. (2010). Prevalence and riskfactors of cerebral microbleeds: an update of the Rotterdam scanstudy. Stroke, 41(10 Suppl), S103–106.
Prabhakaran, S., Wright, C. B., Yoshita, M., Delapaz, R., Brown, T.,DeCarli, C., & Sacco, R. L. (2008). Prevalence and determinants ofsubclinical brain infarction: the northern Manhattan study.Neurology, 70(6), 425–430. doi:10.1212/01.wnl.0000277521.66947.e5.
Preston, S. D., Steart, P. V., Wilkinson, A., Nicoll, J. A., & Weller, R. O.(2003). Capillary and arterial cerebral amyloid angiopathy inAlzheimer’s disease: defining the perivascular route for the elimina-tion of amyloid beta from the human brain. Neuropathology andApplied Neurobiology, 29(2), 106–117.
Provenzano, F. A., Muraskin, J., Tosto, G., Narkhede, A., Wasserman, B.T., Griffith, E. Y., & Brickman, A. M. (2013). White matterhyperintensities and cerebral amyloidosis: necessary and sufficientfor clinical expression of Alzheimer disease? JAMA Neurology,70(4), 455–461.
Raz, N., Lindenberger, U., Rodrigue, K. M., Kennedy, K. M., Head, D.,Williamson, A., & Acker, J. D. (2005). Regional brain changes inaging healthy adults: general trends, individual differences andmodifiers. Cerebral Cortex, 15(11), 1676–1689.
Refolo, L. M., Pappolla, M. A., Malester, B., LaFrancois, J., Bryant-Thomas, T., Wang, R., & Duff, K. (2000). Hypercholesterolemiaaccelerates the Alzheimer’s amyloid pathology in a transgenicmouse model. Neurobiology of Disease, 7(4), 321–331.
Roses, M., & Allen, D. (1996). Apolipoprotein E alleles as risk factors inAlzheimer’s disease. Annual Review of Medicine, 47(1), 387–400.
Neuropsychol Rev (2014) 24:371–387 385

Ruchoux, M.-M., & Maurage, C.-A. (1997). CADASIL: cerebral auto-somal dominant arteriopathy with subcortical infarcts andleukoencephalopathy. Journal of Neuropathology & ExperimentalNeurology, 56(9), 947–964.
Salminen, A., Ojala, J., Kauppinen, A., Kaarniranta, K., & Suuronen, T.(2009). Inflammation in Alzheimer’s disease: amyloid-β oligomerstrigger innate immunity defence via pattern recognition receptors.Progress in Neurobiology, 87(3), 181–194.
Salonen, R., & Salonen, J. T. (1991). Determinants of carotid intima‐media thickness: a population‐based ultrasonography study in east-ern Finnish men. Journal of Internal Medicine, 229(3), 225–231.
Schnabel, R., Larson, M. G., Dupuis, J., Lunetta, K. L., Lipinska, I.,Meigs, J. B., & Newton-Cheh, C. (2008). Relations of inflammatorybiomarkers and common genetic variants with arterial stiffness andwave reflection. Hypertension, 51(6), 1651–1657.
Schneider, J. A., Arvanitakis, Z., Bang, W., & Bennett, D. A. (2007a).Mixed brain pathologies account for most dementia cases incommunity-dwelling older persons. Neurology, 69(24), 2197–2204.
Schneider, J. A., Boyle, P. A., Arvanitakis, Z., Bienias, J. L., & Bennett,D. A. (2007b). Subcortical infarcts, Alzheimer’s disease pathology,and memory function in older persons. Annals of Neurology, 62(1),59–66.
Schroeder, E. B., Hanratty, R., Beaty, B. L., Bayliss, E. A., Havranek, E.P., & Steiner, J. F. (2012). Simultaneous control of diabetes mellitus,hypertension, and hyperlipidemia in 2 health systems. Circulation.Cardiovascular Quality and Outcomes, 5(5), 645–653. doi:10.1161/CIRCOUTCOMES.111.963553.
Sega, R., Facchetti, R., Bombelli, M., Cesana, G., Corrao, G., Grassi, G., &Mancia, G. (2005). Prognostic value of ambulatory and home bloodpressures compared with office blood pressure in the general popula-tion follow-up results from the pressioni arteriose monitorate e loroassociazioni (PAMELA) study. Circulation, 111(14), 1777–1783.
Seshadri, S., Wolf, P. A., Beiser, A., Elias, M. F., Au, R., Kase, C. S., &DeCarli, C. (2004). Stroke risk profile, brain volume, and cognitivefunction: the FraminghamOffspring Study.Neurology, 63(9), 1591–1599.
Siegel, D., Lopez, J., & Meier, J. (2007). Antihypertensive medicationadherence in the department of veterans affairs. The AmericanJournal of Medicine, 120(1), 26–32.
Simons, M., Keller, P., De Strooper, B., Beyreuther, K., Dotti, C. G., &Simons, K. (1998). Cholesterol depletion inhibits the generation ofβ-amyloid in hippocampal neurons. Proceedings of the NationalAcademy of Sciences, 95(11), 6460–6464.
Stewart, R., Xue, Q. L.,Masaki, K., Petrovitch, H., Ross, G.W.,White, L.R., & Launer, L. J. (2009). Change in blood pressure and incidentdementia: a 32-year prospective study. Hypertension, 54(2), 233–240. doi:10.1161/HYPERTENSIONAHA.109.128744.
Swan, G. E., DeCarli, C., Miller, B. L., Reed, T.,Wolf, P. A., Jack, L.M., &Carmelli, D. (1998). Association of midlife blood pressure to late-lifecognitive decline and brain morphology. Neurology, 51(4), 986–993.
Tan, Z. S., Beiser, A. S., Fox, C. S., Au, R., Himali, J. J., Debette, S., &Seshadri, S. (2011). Association of metabolic dysregulation withvolumetric brainmagnetic resonance imaging and cognitivemarkersof subclinical brain aging in middle-aged adults: the FraminghamOffspring Study. Diabetes Care, 34(8), 1766–1770. doi:10.2337/dc11-0308.
Tanaka, H., Munakata, M., Kawano, Y., Ohishi, M., Shoji, T., Sugawara,J., & Sawayama, T. (2009). Comparison between carotid-femoraland brachial-ankle pulse wave velocity as measures of arterialstiffness. Journal of Hypertension, 27(10), 2022–2027.
Tell, G. S., Crouse, J. R., & Furberg, C. D. (1988). Relation betweenblood lipids, lipoproteins, and cerebrovascular atherosclerosis. Areview. Stroke, 19(4), 423–430.
Thöne-Reineke, C., Zimmermann, M., Neumann, C., Krikov, M., Li, J.,Gerova, N., & Unger, T. (2004). Are angiotensin receptor blockersneuroprotective? Current Hypertension Reports, 6(4), 257–266.
Touboul, P.-J., Hennerici, M., Meairs, S., Adams, H., Amarenco, P.,Bornstein, N., & Fatar, M. (2006). Mannheim carotid intima-mediathickness consensus (2004–2006). Cerebrovascular Diseases, 23(1),75–80.
Tsao, C.W., Seshadri, S., Beiser, A. S., Westwood, A. J., DeCarli, C., Au,R., & Mitchell, G. F. (2013). Relations of arterial stiffness andendothelial function to brain aging in the community. Neurology,81(11), 984–91.
Valeo, T. (2013). NEWS FROM THE AAN ANNUAL MEETING:autopsied brains show seniors on beta blockers Had fewer signs ofdementia. Neurology Today, 13(5), 1–6.
van den Heuvel, M. P., & Hulshoff Pol, H. E. (2010). Exploring the brainnetwork: a review on resting-state fMRI functional connectivity.European Neuropsychopharmacology, 20(8), 519–534.
van Dijk, E. J. (2005). C-Reactive Protein and Cerebral Small-VesselDisease: The Rotterdam Scan Study. Circulation, 112(6), 900–905.doi:10.1161/circulationaha.104.506337.
van Es, A. C., van der Grond, J., ten Dam, V. H., de Craen, A. J., Blauw,G. J., Westendorp, R. G., & Group, P. S. (2010). Associationsbetween total cerebral blood flow and age related changes of thebrain. PloS One, 5(3), e9825. doi:10.1371/journal.pone.0009825.
van Popele, N. M., Grobbee, D. E., Bots, M. L., Asmar, R., Topouchian,J., Reneman, R. S., & Witteman, J. C. (2001). Association betweenarterial stiffness and atherosclerosis: the Rotterdam Study. Stroke,32(2), 454–460.
Vasan, R. S., Larson, M. G., Leip, E. P., Evans, J. C., O’Donnell,C. J., Kannel, W. B., & Levy, D. (2001). Impact of high-normal blood pressure on the risk of cardiovascular disease. TheNew England Journal of Medicine, 345(18), 1291–1297. doi:10.1056/NEJMoa003417.
Verdecchia, P., Porcellati, C., Schillaci, G., Borgioni, C., Ciucci, A.,Battistelli, M., & Santucci, A. (1994). Ambulatory blood pressure.An independent predictor of prognosis in essential hypertension.Hypertension, 24(6), 793–801.
Vermeer, S. E., Longstreth, W. T., Jr., & Koudstaal, P. J. (2007). Silentbrain infarcts: a systematic review. Lancet Neurology, 6(7), 611–619.
Vinters, H., & Gilbert, J. (1983). Cerebral amyloid angiopathy: incidenceand complications in the aging brain. II. The distribution of amyloidvascular changes. Stroke, 14(6), 924–928.
White, J. A., Manelli, A. M., Holmberg, K. H., Van Eldik, L. J., & LaDu,M. J. (2005a). Differential effects of oligomeric and fibrillar amy-loid-β1–42 on astrocyte-mediated inflammation. Neurobiology ofDisease, 18(3), 459–465.
White, L., Small, B. J., Petrovitch, H., Ross, G. W., Masaki, K., Abbott,R. D., & Markesbery, W. (2005b). Recent clinical-pathologic re-search on the causes of dementia in late life: update from theHonolulu-Asia aging study. Journal of Geriatric Psychiatry andNeurology, 18(4), 224–227. doi:10.1177/0891988705281872.
White, L., Gelber, R., Launer, L., Zarow, C., Sonnen, J., Uyehara-Lock, J.,Petrovitch, H. (2013). Beta Blocker Treatment of Hypertensive OlderPersons Ameliorates the Brain Lesions of Dementia Measured atAutopsy: The Honolulu-Asia Aging Study. Paper presented at theAmerican Academy of Neurology Annual Meeting, San Diego.
Whitmer, R. A., Sidney, S., Selby, J., Johnston, S. C., & Yaffe, K. (2005).Midlife cardiovascular risk factors and risk of dementia in late life.Neurology, 64(2), 277–281. doi:10.1212/01.wnl.0000149519.47454.f2.
Wills, A. K., Lawlor, D. A., Matthews, F. E., Sayer, A. A., Bakra, E.,Ben-Shlomo, Y., & Kivimaki, M. (2011). Life course trajectories ofsystolic blood pressure using longitudinal data from eight UKcohorts. PLoS Medicine, 8(6), e1000440.
Wills, A. K., Lawlor, D. A., Muniz-Terrera, G., Matthews, F., Cooper, R.,Ghosh, A. K., & Hardy, R. (2012). Population heterogeneity intrajectories of midlife blood pressure. Epidemiology (Cambridge,Mass), 23(2), 203–11.
386 Neuropsychol Rev (2014) 24:371–387

Wilms, H., Rosenstiel, P., Unger, T., Deuschl, G., & Lucius, R. (2005).Neuroprotection with angiotensin receptor antagonists. AmericanJournal of Cardiovascular Drugs, 5(4), 245–253.
Wolf, P. A., D’Agostino, R. B., Belanger, A. J., & Kannel, W. B. (1991).Probability of stroke: a risk profile from the Framingham Study.Stroke, 22(3), 312–318.
Wright, C. B., Moon, Y., Paik, M. C., Brown, T. R., Rabbani, L., Yoshita,M., & Elkind, M. S. (2009). Inflammatory biomarkers of vascularrisk as correlates of leukoariosis. Stroke, 40(11), 3466–3471.
Yamashina, A., Tomiyama, H., Takeda, K., Tsuda, H., Arai, T., Hirose,K., & Yamamoto, Y. (2002). Validity, reproducibility, and clinical
significance of noninvasive brachial-ankle pulse wave velocity mea-surement. Hypertension Research, 25(3), 359–364.
Yip, A., McKee, A., Green, R., Wells, J., Young, H., Cupples, L., &Farrer, L. (2005). APOE, vascular pathology, and the AD brain.Neurology, 65(2), 259–265.
Yuan, C., & Kerwin, W. S. (2004). MRI of atherosclerosis. Journal ofMagnetic Resonance Imaging, 19(6), 710–719. doi:10.1002/jmri.20070.
Zieman, S. J., Melenovsky, V., & Kass, D. A. (2005). Mechanisms,pathophysiology, and therapy of arterial stiffness. Arteriosclerosis,Thrombosis, and Vascular Biology, 25(5), 932–943.
Neuropsychol Rev (2014) 24:371–387 387
![Resveratrol: preventing properties against vascular …...of CHD have been attributed partly to the consumption of red wine, which contains high levels of polyphenols [3]. Similarly,](https://img.dokumen.tips/doc/110x75/5f4b698ae6e83c688c3235c5/resveratrol-preventing-properties-against-vascular-of-chd-have-been-attributed.jpg)