Embed Size (px)
Citation preview
Preterm : Risk identification and prevention
YURI YANASE
M.D., DIPLOMA IN OB & GYN, MFM, MRTCOG
Maternal-Fetal Medicine, Obstetric and Gynecology Department,, Nakornping Hospital, Chiang Mai, Thailand
นิยาม
การคลอดก่อนก าหนด (Preterm birth) เป็นสาเหตกุารตายของ
ทารกแรกเกิดท่ีพบบ่อย
มีการพฒันาทางการแพทยแ์ละการพยาบาลอย่างมาก
สถานการณ์ทางเศรษฐกิจและสงัคมของสตรีตัง้ครรภท่ี์ดีกว่าเดิม
มีการศึกษาค้นคว้าวิจยัอย่างกว้างขวาง
นิยาม การเจบ็ครรภค์ลอดก่อนก าหนด (Preterm labor)
The suggested criteria for diagnosis include the following.
* อายคุรรภต์ัง้แต่ 20 สปัดาห ์จนถึงก่อนครบ 37 สปัดาห ์
* มีการหดรดัตวัของมดลกูสม า่เสมอ(4ครัง้ใน 20 นาทีหรือ 8 ครัง้
ใน 1 ชัว่โมง) ร่วมกบั
# มีการเปล่ียนแปลงของปากมดลกู หรือ
# มีการบางตวัของปากมดลกูตัง้แต่ร้อยละ 80 หรือ
# ปากมดลกูเปิดเกิน 1 ซม.ขึน้ไป
(Oh W, Merenstein G. Guidelines for perinatal care. 4th ed. Elk Grove Village, IL and Washington, DC : American Academy of Pediatrics and the American College of Obstetricians and Gynecologists, 1997; 128)
นิยาม
การวินิจฉัยยงัคงเป็นปัญหา ในเวชปฏิบติัเน่ืองจากจะต้องแยกจากการ
เจบ็ครรภเ์ตือน (false labor pain) และการหดตวัมดลกูชนิด Braxton
Hicks
มีการศึกษาพบว่าภาวะดงักล่าวเป็นสาเหตขุองการรกัษาการเจบ็ครรภ์
คลอดก่อนก าหนดท่ีไม่จ าเป็น ถึงร้อยละ 80
(Steer P, Flint C. ABC of labour care : preterm labour and premature rupture of membranes. BMJ 1999; 318 : 1059-62.)
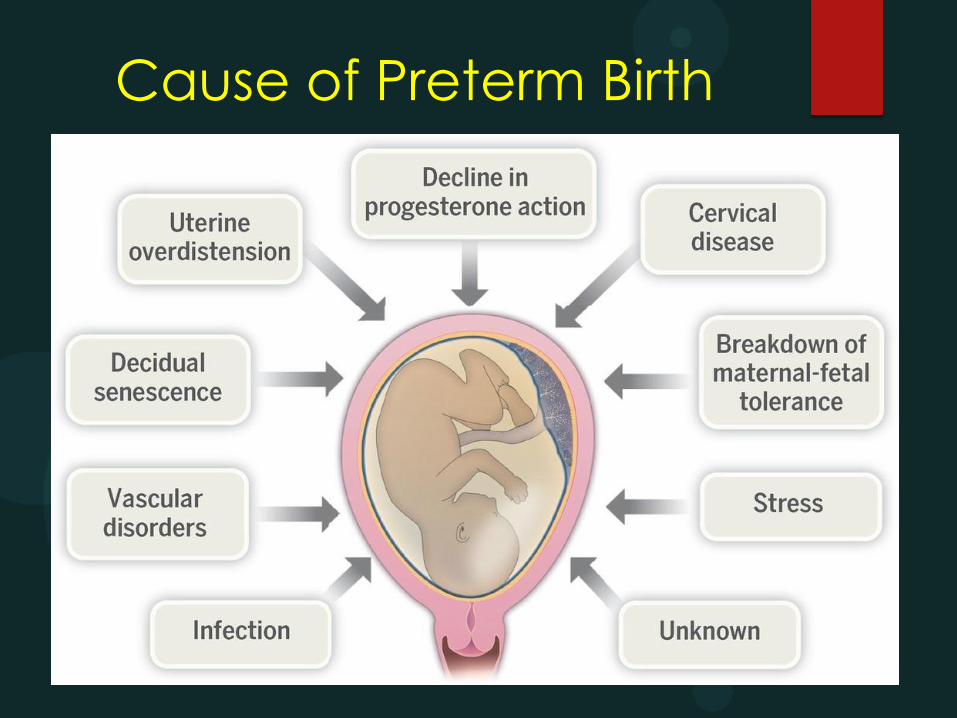
Cause of Preterm Birth
Preterm Birth
Spontaneous preterm
Indicated preterm
Maternal heart disease
Pre-eclampsia with severe feature
Abruptio placentae

Spontaneous Preterm
The major risk factors
Previous preterm birth
Cervical shortening in the second trimester
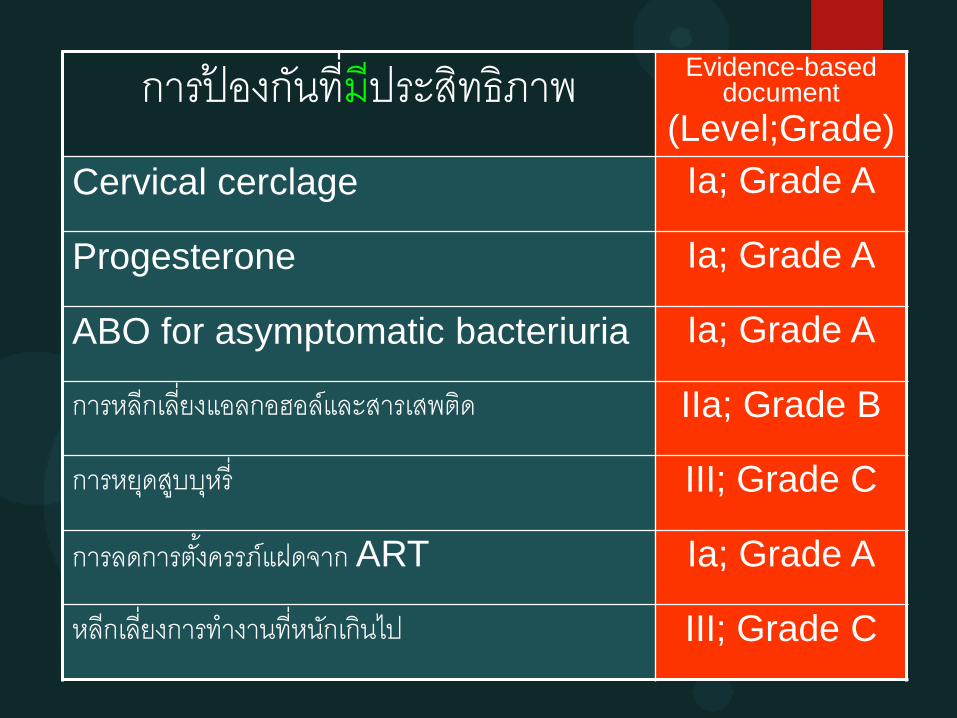
การป้องกนัท่ีมีประสิทธิภาพ Evidence-based document
(Level;Grade)
Cervical cerclage Ia; Grade A
Progesterone Ia; Grade A
ABO for asymptomatic bacteriuria Ia; Grade A
การหลีกเลี่ยงแอลกอฮอล์และสารเสพติด IIa; Grade B
การหยดุสบูบหุร่ี III; Grade C
การลดการตัง้ครรภ์แฝดจาก ART Ia; Grade A
หลีกเลี่ยงการท างานท่ีหนกัเกินไป III; Grade C
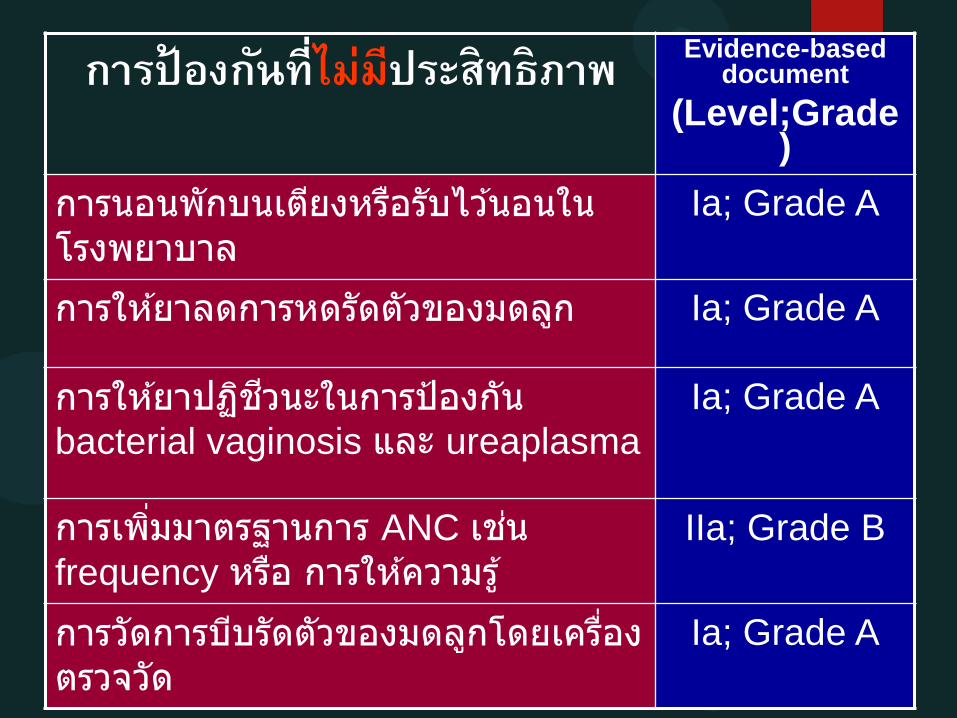
การป้องกนัท่ีไม่มีประสิทธิภาพ Evidence-based document
(Level;Grade)
การนอนพักบนเตยีงหรอืรับไวน้อนในโรงพยาบาล
Ia; Grade A
การใหย้าลดการหดรัดตัวของมดลกู Ia; Grade A
การใหย้าปฏชิวีนะในการป้องกนั bacterial vaginosis และ ureaplasma
Ia; Grade A
การเพิม่มาตรฐานการ ANC เชน่ frequency หรอื การใหค้วามรู ้
IIa; Grade B
การวัดการบบีรัดตัวของมดลกูโดยเครือ่งตรวจวัด
Ia; Grade A
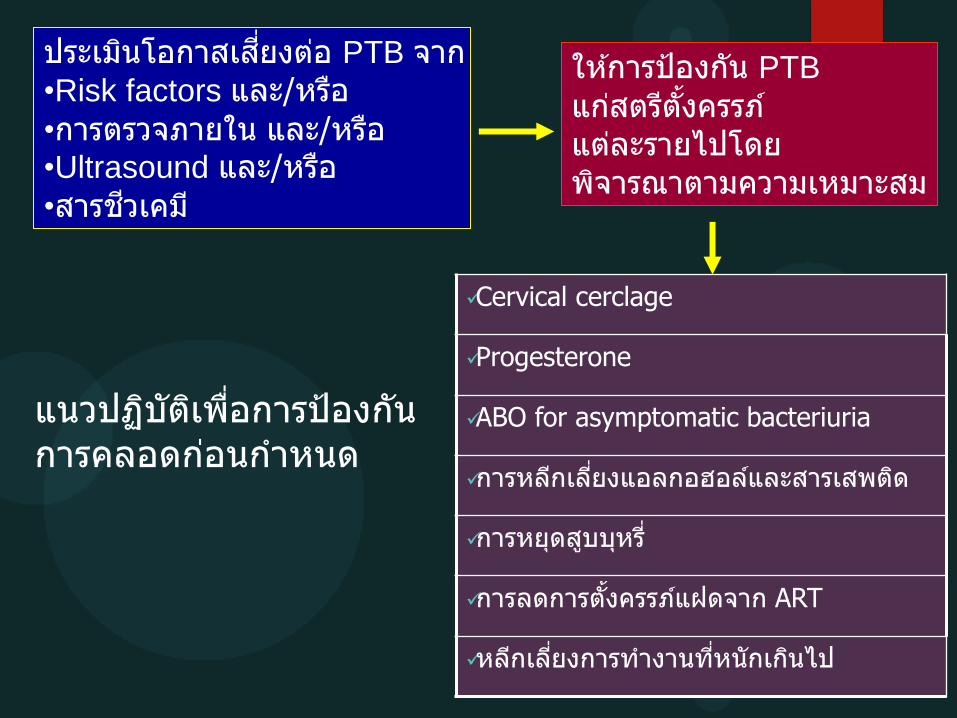
ประเมนิโอกาสเสีย่งตอ่ PTB จาก •Risk factors และ/หรอื
•การตรวจภายใน และ/หรอื •Ultrasound และ/หรอื
•สารชวีเคม ี
ใหก้ารป้องกนั PTB
แกส่ตรตีัง้ครรภ ์แตล่ะรายไปโดย พจิารณาตามความเหมาะสม
Cervical cerclage
Progesterone
ABO for asymptomatic bacteriuria
การหลกีเลีย่งแอลกอฮอลแ์ละสารเสพตดิ
การหยดุสบูบหุรี ่
การลดการตัง้ครรภแ์ฝดจาก ART
หลกีเลีย่งการท างานทีห่นักเกนิไป
แนวปฏบิตัเิพือ่การป้องกนั การคลอดกอ่นก าหนด
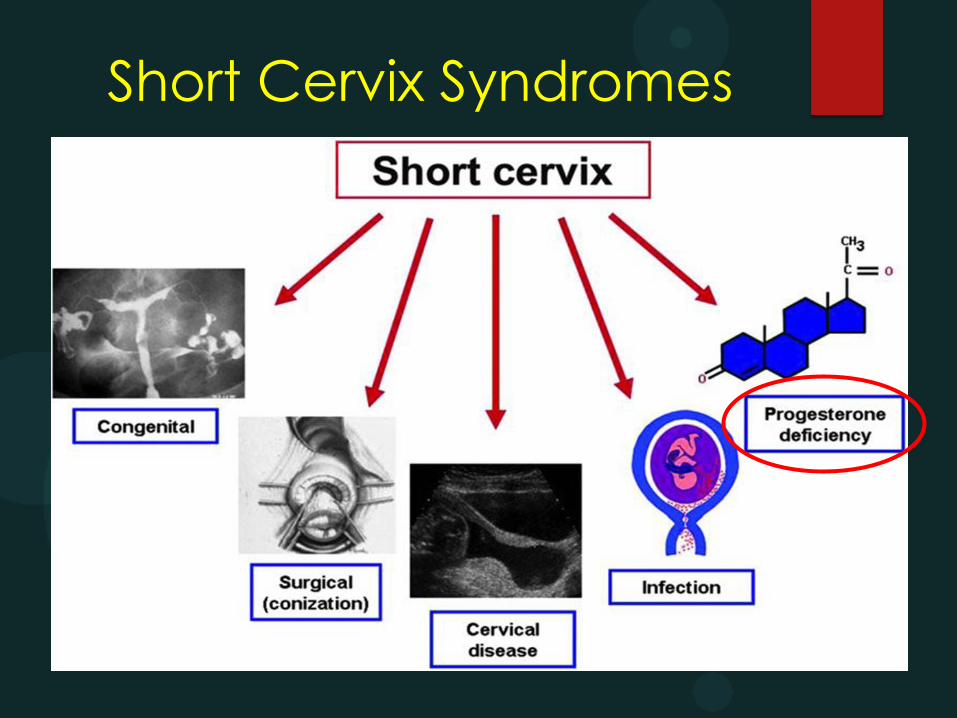
Short Cervix Syndromes
“Progesterone deficient state”
has been proposed to be a
mechanism of disease in preterm labor
1. Decrease prostaglandin synthesis
2. Reduce cervical stromal degradation in cervix
3. Reduce contraction frequency in myometrium

Mechanisms of Progesterone for Prevent Preterm
Myometrial quiescence
Inhibit cervical ripening
Progesterone: a key hormone for
pregnancy maintenance
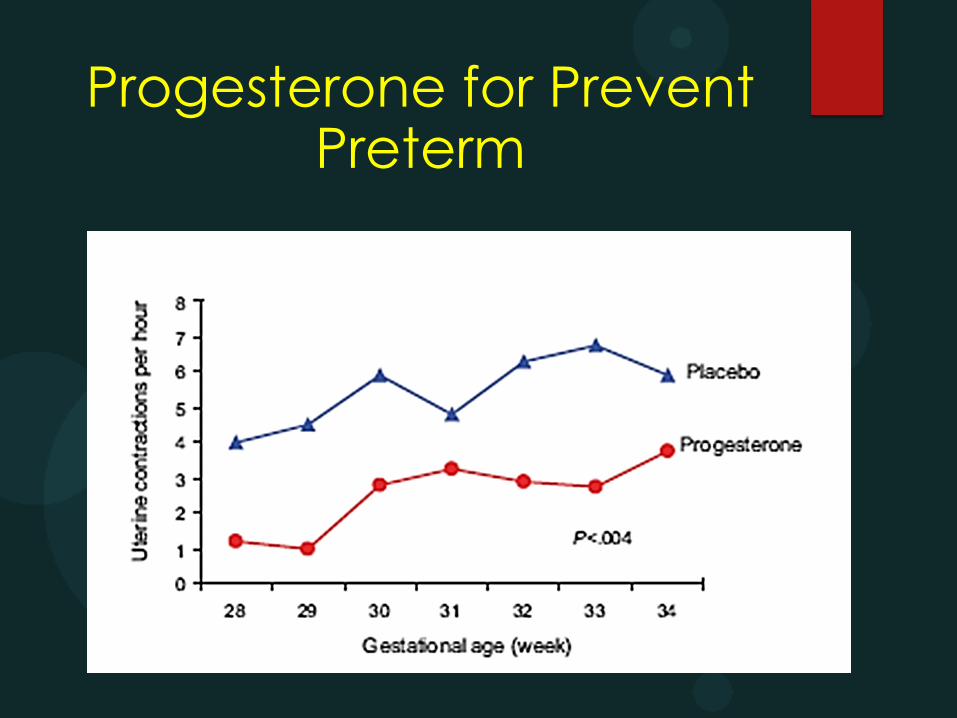
Progesterone for Prevent Preterm
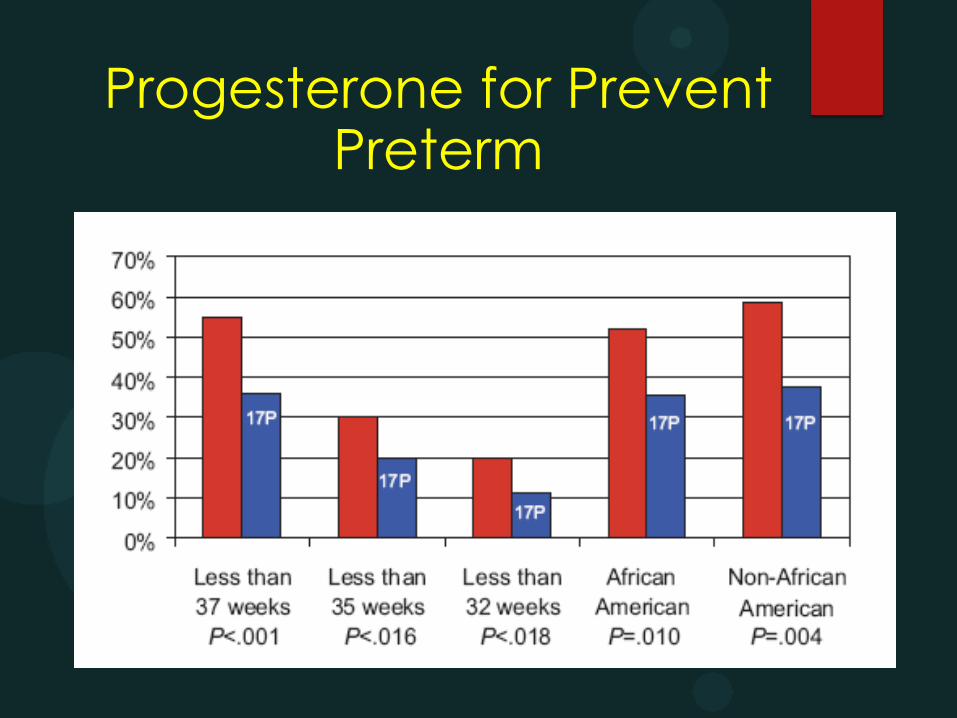
Progesterone for Prevent Preterm

Side Effects
Maternal :
headache, nausea,coughing, local irritation, and breast tension GDM ?
Fetal:
No teratogenic effects
No significant differences in health status or
physical examination, including genital anomalies, and scores for gender specific roles
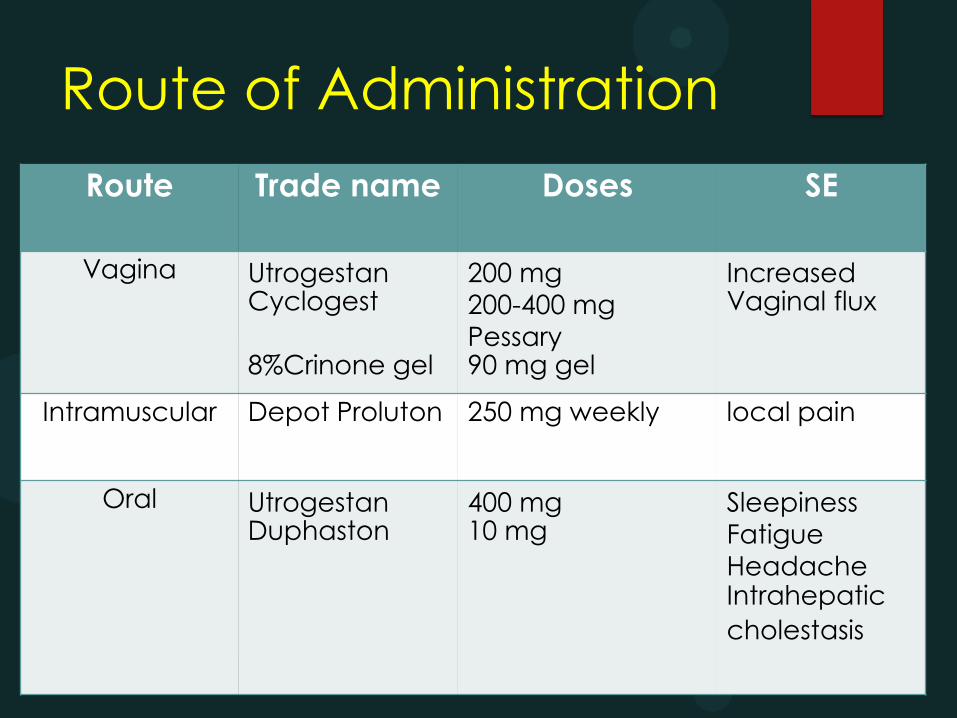
Route of Administration
Route Trade name Doses SE
Vagina Utrogestan Cyclogest 8%Crinone gel
200 mg
200-400 mg
Pessary 90 mg gel
Increased Vaginal flux
Intramuscular Depot Proluton 250 mg weekly local pain
Oral Utrogestan Duphaston
400 mg 10 mg
Sleepiness
Fatigue
Headache Intrahepatic cholestasis
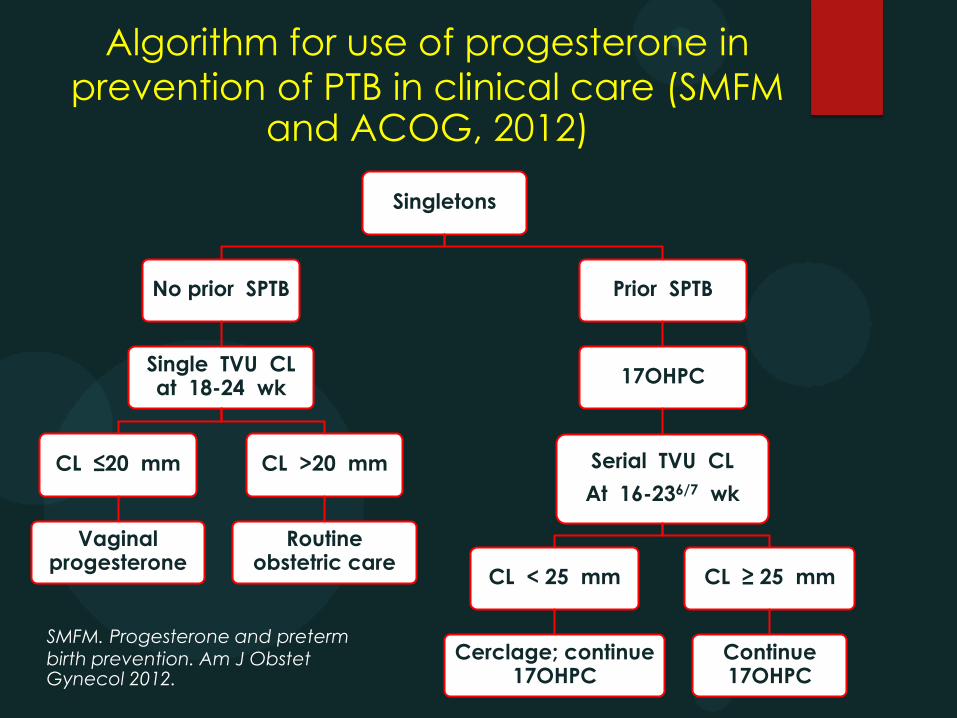
Algorithm for use of progesterone in
prevention of PTB in clinical care (SMFM and ACOG, 2012)
Singletons
No prior SPTB
Single TVU CL at 18-24 wk
CL ≤20 mm
Vaginal progesterone
CL >20 mm
Routine obstetric care
Prior SPTB
17OHPC
Serial TVU CL
At 16-236/7 wk
CL < 25 mm
Cerclage; continue 17OHPC
CL ≥ 25 mm
Continue 17OHPC
SMFM. Progesterone and preterm birth prevention. Am J Obstet Gynecol 2012.
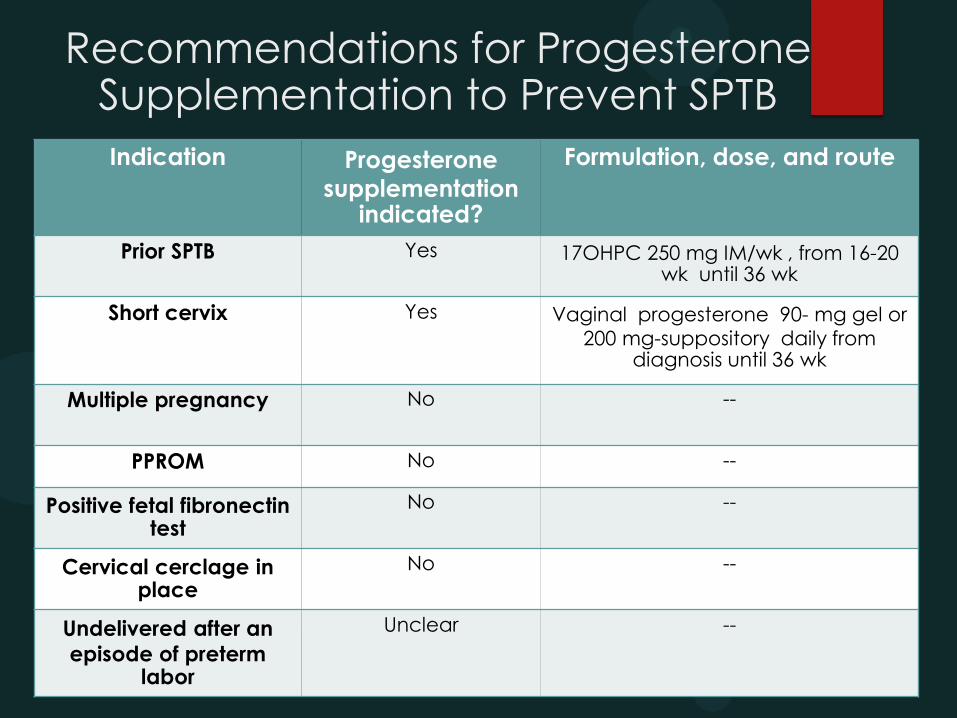
Recommendations for Progesterone Supplementation to Prevent SPTB
Indication Progesterone
supplementation indicated?
Formulation, dose, and route
Prior SPTB Yes 17OHPC 250 mg IM/wk , from 16-20 wk until 36 wk
Short cervix Yes Vaginal progesterone 90- mg gel or
200 mg-suppository daily from diagnosis until 36 wk
Multiple pregnancy No --
PPROM No --
Positive fetal fibronectin test
No --
Cervical cerclage in place
No --
Undelivered after an
episode of preterm labor
Unclear --
Progesterone
ACOG Recommendation Level A
Vaginal progesterone is recommended
as a management option to reduce risk
of preterm in
Asymptomatic
Singleton
Without previous preterm
Very short cervix < 2 cm.
GA < 24 weeks

ACOG Recommendation Level A
Progesterone supplement start at
16-24 weeks
Singleton gestation
Prior spontaneous preterm
Regardless of transvaginal ultrasound
ACOG Recommendation Level A
Progesterone treatment does not reduce in
Multiple gestation
Short Cervix
At GA 14-30 wk, mean cervical length = 35-40 mm
TVS CL; GA 16-28 wk
≤ 20 mm in women with no prior PTB
< 25 mm in women with a prior PTB
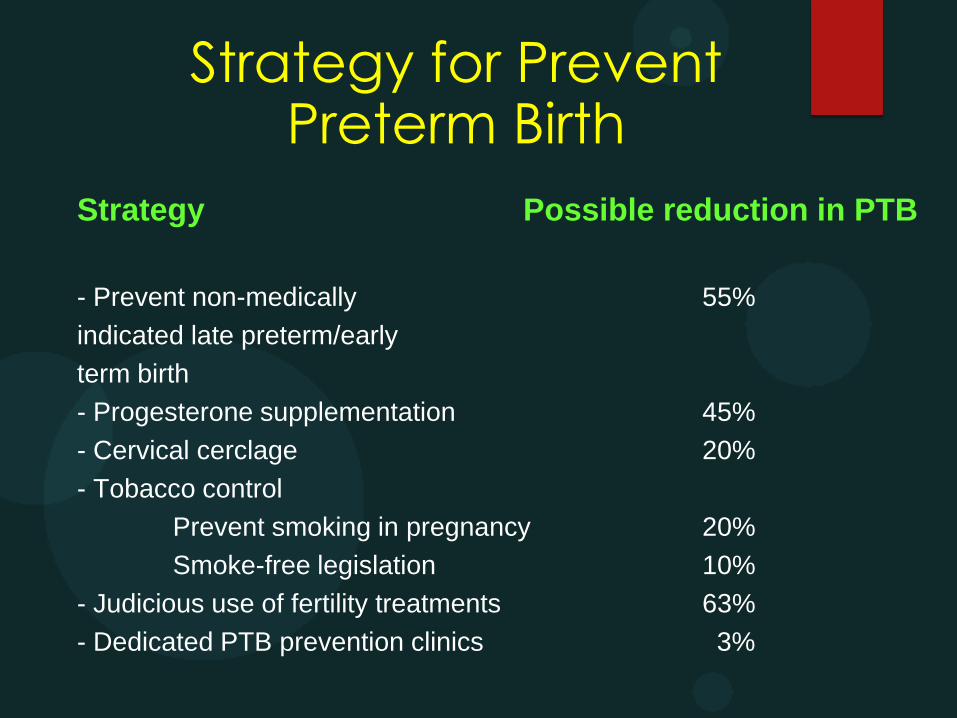
Strategy for Prevent Preterm Birth
Strategy Possible reduction in PTB
- Prevent non-medically 55%
indicated late preterm/early
term birth
- Progesterone supplementation 45%
- Cervical cerclage 20%
- Tobacco control
Prevent smoking in pregnancy 20%
Smoke-free legislation 10%
- Judicious use of fertility treatments 63%
- Dedicated PTB prevention clinics 3%
Take Home Messages
Progesterone is preterm prevention drug.
True criteria
Short cervix <2 cm.(Vg, Oral)
Previous spontaneous preterm.(IM, Vg,
Oral)
Progesterone is not tocolytic drug
Efficacy of vaginal rout > Oral rout

Thank You










![뉴론틴 100 mg, 300 mg, 400 mg ( Neurontin Capsules 100 mg, … · 2016. 10. 11. · Neurontin Capsules 100 mg, 300 mg, 400 mg (gabapentin) [원료약품의 분량] 100 mg: 매](https://img.dokumen.tips/doc/110x75/60ca7a47df0935746f0cdf4d/ee-100-mg-300-mg-400-mg-neurontin-capsules-100-mg-2016-10-11-neurontin.jpg)


















