Embed Size (px)
Citation preview

ACTA OPHTHALMOLOGICA VOL. 57 1979
XXlV MEETING OF NORDIC OPHTHALMOLOGISTS
Oslo, Norway 13-16 June 1979
Departmrnt of Ophthalmolotgi (Hrnd: E . Crrgerten), and Section of Cardiolo,g (Head: A . Tybjm7;g Hansrnj
Mrdicnl Depnrtmrnt R, Ri,qtho,spitnlrt, Copmhngrn
PRESENILE CORNEAL ARCUS IN HEALTHY PERSONS.
A POSSIBLE CARDIOVASCULAR RISK INDICATOR IN YOUNGER ADULTS
BY
L.VARNEK, P. SCHNOHR and G. JENSEN
The results of blood-lipid screening of 200 39-49-year-old participants with incidentally diagnosed corneal arcus from the Copenhagen City Heart Study are reported. A large sample of study-participants of the same age-group without arcus served as controls. In general, the arcus-group had higher se.-cholesterol than the control-group (P<O.Ol in males and <0.02 in females). The se.-triglycerides in the two groups did not differ. A trend towards positive correlation between arcus-intensity and cholesterol- level was demonstrated by non-parametrical statistics. By use of the same statistics, an association between lipids and arcus-localisation was searched out. Dense arcus in the nasalilower limbal regions occurred together with hyper- cholesterolemia more often than did a marked upperiouter arcus. Consequently, based on the present investigation, se.-cholesterol-screening of middle-aged persons with marked lowerinasal arcus seems justified, since hvpercholesterolemia might will be an underlying cause. Finally, the importance of diagnosing and treating hypercholesterolemia is briefly discussed.
KPV uiord\; corneal arcus, slit lamp grading - prevalence in middle-age - hvpercholesterolemia - se.-triglycerides - se.-glucose - arcus-intensity - arcus- localisation.
755 4x*

L. Varnek, P. Schnohr and G. J a s e n
Our present knowledge regarding corneal arcus in relation to lipid-abnormalities and cardiovascular diseaseideath dates from several sources. A connexion between arcus in pre-middle-age and acute myocardial infarction has been established in a
large scale prospective population study, the Western Collaborative Study Group (Jaeger & Eisenhauer 1977), whereas others have reported a lack of connexion between atherosclerosis, verified by authopsy, and arcus-prevalence (Immich et al. 1967).
Screenings for arcus-prevalence and arcus-degree have established strong corre- lations between hyperlipidemia, especially hypercholesterolemia, and early arcus (Jaeger & Eisenhauer 1977). The same investigators further stressed the specific importance of lower (= inferiorly located) arcus in relation to blood lipid-abnorma- lities.
Reports on lipid-screening on normals with incidentally diagnosed corneal arcus are rare, and the results are controversial (Parwaresch et al. 1976).
To our knowledge no earlier attempts have been done on a larger scale to clarify the clinical importance of both arcus-intensity and prevailing arcus-localisation in symptom-free individuals.
So, the aim of the present study is to analyse the correlations between blood lipids, in this case cholesterol and triglyceride, and corneal arcus in a group of presumed healthy pre-middle-aged persons.
Material
From the total group of participants in the Copenhagen City Heart Study (abbreviated CCHS), aged 39-49 years in 1977, those persons were selected for the study, in whom a corneal arcus was macroscopically diagnosed by the participating cardiologists. Before inclusion into the study, the persons underewent slit-lamp examination to verify the arcus and to exclude persons with gross local corneal pathology from the study.
As blood-parameters, the non-fasting values of se.-cholesterol, se.-triglyceride d se.-glucose (mmolil) were chosen.
Out of 270 persons, 200 persons, 115 males and 85 females, participated in the study and constitute our arcus-group.
As blood-sample-controls served the total group of participants in the CCHS aged 39-49 years in 1977 (1440 males and 1705 females). They were, because of the data-registration available, accepted as controls because of the low arcus prevalence in the group, about 6.8%.
756

Cornml Army and Blood Lzpzdc zn the MzddlP-aged
Methods a) Preliminary procedures
The ophthalmic investigations were performed by one of us (L. Varnek) over seven months. Prior to the slit-lamp examinations, every person received a letter explaining why, where and when to meet. Eighty-five % of those, who received the letter. attended for examination.
b) Examination proper
Slit-lamp examination was performed on right eyes only by the use of a Haag-Streit slit-lamp (type 500) supplied with tungsten light, magnification x 6 and fixed, white, diffuse, 6 V illumination. The corneal arcus was given a total score ranging from 0-12 and a quadrant score ranging from 0-3 in any of the four quadrants: upper, lower, nasal, temporal, based on both surface-extension and surface- intensity of the arcus. Fig. 1 gives examples of this scoring system.
Finally, the cornea under investigation was photographed with a Zeiss slit lamp camera (Ectachrome, magnification x 2).
c) Scoring methodology remarks
Methodological difficulties in obtaining an “exact” arcus-scoring were experienced, since both arcus-surface-extension and arcus-surface-intensity varied along the limbal circumference.
The subjective way of scoring, which has been employed by the single observer in
this study, was controlled by means of the photographs taken.
d) Registration
Each person in the study received four registration sheets, one for name, address etc., one for registration of known diabetes, earlier cerebral strokes or myocardial infarction, one for registration of the blood sample analyses (these three sheets were taken as photocopies from
0-3 0) + O - 3 0-3
0-3
0 1 2 3 Fig. 1.
Schematic illustration of the employed arcus-scoring system. Total score values obtainable 0-12. N o arcus = score 0. Weak arcus = score 1. Intermed. = score 2. Strong arcus = score 3.
757

L. Varnek, P. Schnohr and G. Jmwn
the journals on the persons in the CCHS), and finally one for corneal arcus scoring and supplementary corneal remarks, when necessary.
Because of the separated sheets, the lipid values of the persons, when receiving an arcus-score, were unknown to the slit-lamp investigator.
Results
To assess significance of the observed associations a probability level of P < 0.05 was used.
In the arcus group, the mean age of the examined males was 46.5 years (SI) + 3.4 years) and females 46.6 years (SD k 3.1 years).
T h e two sexes had the same mean total arcus score value of 5.3. Comparing the whole arcus group with the controls, a significantly higher mean
cholesterol level was demonstrated in the arcus group, and in both sexes (see Fig. 2 a) (P < 0.01 in males and < 0.02 in females).
In the two sexes there were no differences between arcus group and controls as concerns triglyceride and glucose levels (see Fig. 2 b and c).
Correlations between arcus-intensity (score 0- 12) and se.-analyses were calcu- lated by non-parameterical, statistical methods (Kruskal Wallis) (see Table I). Especially in females, but also in males, there was a trend towards a p0ri t i - i~ correlation between arcus-degree and cholesterol-values, which in the females nearly reached significance (P < 0.074).
Table I1 shows a significantly higher frequency of high cholesterol values in the female group of “high-arcus-scorers” as compared with “low-arcus-scorers” ( P < 0.01), but not in the corresponding male groups (P > 0.05).
Finally, we wanted to establish, whether arci with shifting localisations (up, down, temporal, nasal) were equally often combined with, and thereby the visible expression of, an underlying hypercholesterolemia.
T h e arcus-areas selected for investigation were the upper, lower, nasal and temporal limbal quadrants.
Again, by use of the non-parametrical Kruskal Wallis analysis (see Figs. 3 a-c), and based on the arcus-scoring system from 0-3 in the quadrants, earlier defined, correlations between increasing score-values at the four chosen limbal sites and the blood sample analyses in either sex were calculate, and in total 24 P-values resulted.
Out of the 24 possible correlations examined, three significant correlations, all cholesterol-attached. were established:
1. Females showed a positive correlation between degree of n c d arcus and cholesterol values (P < 0.05).
758

Cmnrnl Arcus and Blood Lipid\ in thr Mzddlr-aged
cz] dA MEAN CHOLESTEROL(mmol/l) . .... 4
6
2a 4
2
p<O 004 p<O 015 MEAN TRIGLVCERIDE (mmol / I 1
234 2-
p<0.530 p<O 321 MEAN GLUCOSE (mmolII)
2 c
p<0.68
Fig$. 2 a-c. Column diagrams showing the mean arithmetic values for non fasting cholesterol (Fig. 2 a), triglyceride (Fig. 2 b) and glucose (Fig. 2 c) in mmolil in males and females of the arcus and control groups. Cl , males, control group. 0 , males, arcus group. 'E , females, control group. , females, arcus group. The two first columns (left) show the absence of a sex-difference in se.-cholesterol and the presence of a sex-difference as for se.-triglyceride and se.-glucose. In the last four columns (right), sample means of arcus and control groups are apposed (see text). Numbers within columns shows the size of the group under consideration. Numbers at top of the columns show the arithmetic mean value of the relevant blood sample. Number at bottom of columns: obtained P-values in comparing sample means
(Student's t-test, computer assisted).
759

L. Varnek, P. Schnohrand G.Jensen
Males
Table I . Correlation between arcus-intensity and cholesterol, triglyceride and glucose in males and females in the arcus-group. A slight positive trend between arcus-score and blood- cholesterol is demonstrated especially in females, statistically insignificant, however, at a 5 %
level (Kruskal Wallis).
Females Males Females Males Females
Cholesterol 1 Triglyceride Glucose I
No. of persons
Persons with se.-cholesterol > 7.0 mmol/l
Persons with se.-cholesterol > 8.0 mmolil
No. 5% No. 7c
Table II . Absolute and relative occurrence of se.-cholesterol values higher than 7.0 mmolil (left) and higher than 8.0 mmolil (right), in males and females of the arcus group, further divided into high and low “total-arcus-scores”, The relative frequency of high cholesterol values in the “high-arcus-score-group” is impressive. Significance levels (x2 tests) between low and high
“arcus-scorers” are shown in brackets.
Females Low arcus score 0-5 55 3 5.5 1 1.8
High arcus score (0.01 > P > 0.001) (0.05 > P > 0.02) 6-12 30 10 33.3 4 13.3
760

Corneal Arcus and Blood Lzpids in the Middle-ugd
p<O 684 p<O.329
p<06%(& oop<O.lll
p<o 955 p<O 346
b
CHOLESTEROL, ARBITRARY UNITS
p<O 137 p<O 033
TRlGLYCERlDE
p<o 118 p<O 232
TEMPO RAL ~ @NASA, 1 p a l 7 4 ‘;COl?7 82
DOWN p 4 541 p<O 767
I b
76 1
L. Vurnek, P. Schnohr and G. Jensen
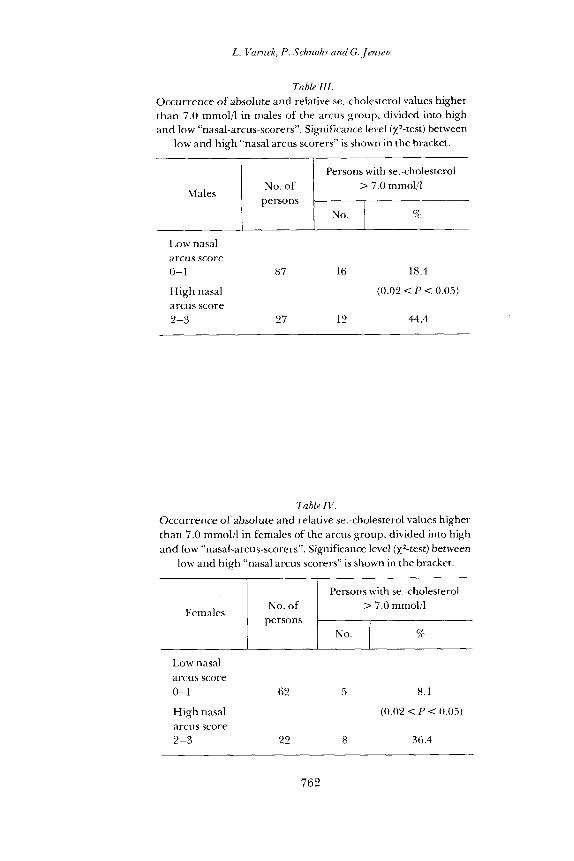
Table I I I . Occurrence of absolute and relative se.-cholesterol values higher than 7.0 mmolil in males of the arcus group, divided into high and low “nasal-arcus-scorers”. Significance level (Xz-test) between
low and high “nasal arcus scorers” is shown in the bracket.
Persons with se.-cholesterol No. of > 7.0 mmolil
persons Males
Low nasal arcus score 0-1 87 16 18.4
High nasal (0.02 < P < 0.05) arcus score 2-3 27 12 44.4
Table IV. Occurrence of absolute and relative se.-cholesterol values higher than 7.0 mmolil in females of the arcus group, divided into high and low “nasal-arcus-scorers”. Significance level (X2-test) between
low and high “nasal arcus scorers” is shown in the bracket.
Persons with se.-cholesterol
L,ow nasal arcus score 0-1 62 5 8.1
High nasal arcus score 2-3 22 8 36.4
(0.02 < P < 0.05)
762

Corneal Arcuc and Blood Ltpzdc zn the MzddlP-agpd
Table V . Occurrence of absolute and relative se.-cholesterol values higher than 7.0 mmol/l in females of the arcus group, divided into high and low “inferior (lower) arcus-scorers”. Significance level (xz- test) between low and high “inferior-arcus-scorers” is shown in
the bracket.
I 1 Persons with se.-cholesterol
Low inferior arcus score 0- 1 37 2 5.4
High inferior arcus score 2-3 47 1 1 23.4
(0.02 < P < 0.05)
2 . Males showed a positive correlation between degree of nasal arcus and cholesterol values ( P = 0.05).
3. Females also showed a positive correlation between degree of inferiorly situated arcus and cholesterol values (P < 0.04).
Tables 111, IV and V give support to the three significant correlations. The other 2 1 P-values, none of which were significant at a 0.05 level, are shown in
Figs. 3 a-c. The uniformly high P-values (cholesterol-attached) in relation to upper arcus-formation are remarkable.
Discussion
Most authors agree upon the existence of a correlation between arcus and hypercholesterolemia in younger age-groups; this association, however, disappears in the older age-groups, where local corneal factors are thought to dominate in arcus-formation (Cogan 1974; Immich et al. 1967; Parwaresch et al. 1976; Rosenmann et al. 1974). Regarding the intermediate age-groups, opinions are diverging, one group of authors claiming lack of significance (Immich et al. 1967), another an obligate co-existence of underlying lipid-abnormalities (Parwaresch et al. 1976). The latter view, however, cannot be true, since the prevalence of lipid-abnormalities in the
763

L. Varnek, P. Schnohr and G.,Jmsm
total population (Wood et al. 1972) does not at all reach that of arcus in the age group under study (39-49 years) (10-25%, Forsius 1954; Jaeger & Eisenhauer 1977).
As concerns our own results, the higher mean cholesterol levels in the male and female arcus groups are in agreement with results, obtained by others (Cogan 1974; Immich et al. 1967; Jaeger & Eisenhauer 1977; Rosenmann et al. 1974). While the total occurrence of hypercholesterolemia (se.-cholesterol higher than 7.0 mmol/l) in the arcus group is 20% (males: 25%, females: 15%) (Table 11), the estimated occurrence of hypercholesterolemia (Fredencksson 11) in the general population is only 3.7% (Wood et al. 1972).
Our correlation between arcus-intensity and se.-cholesterol, demonstrated in women only, has gained less support in the literature. Forsius (1954) correlated increasing arcus intensity in both sexes to increasing blood cholesterol levels, but only in his younger arcus-groups. In contrast, Parwaresch et al. (1976) briefly mentioned a lack of correlation between arcus-degree and blood lipids.
Regarding the significance of arcus-localisation, we found, in accordance with suggestions in the literature (Forsius 1954; Jaeger & Eisenhauer 1977), a positive correlation between dense lower arcus formation in females, but not in males, and high cholesterol values.
We also think, that the obvious lack of correlation between dense upper arcus and blood cholesterol levels deserves to be mentioned.
Our most significant finding, the correlation between marked arcus-formation nasally in both sexes and high cholesterol values, seems to be entirely new. To our knowledge, at least, a distinction in iportance between nasally situated arci and arci situated elsewhere has not previously been put forward.
Since several limbal affections preferentially develop nasally, e. g. pterygiae, pingueculae and spheroid degeneration, possibly because of local, degenerative factors in this region, degenerative corneal changes might be responsible for the above associations. However, a lack of underlying degenerative corneal changes in arcus-formation speaks against this (Cogan & Kuwabara 1959).
Summing up, marked arcus-formation in both sexes, but especially in females, and marked nasal arcus in both sexes should arouse suspicion of underlying hyper- cholesterolemia, at least within the age group studied (39-49 years).
Since familiar hypercholesterolemia is associated with serious cardiovascular complications, if untreated (Research Committee 197 1; Coronary Project 1975) it should deserve early recognition.
The cholesterol-lowering effect of diet-restrictions and lowering of caloric intake is well established (Parwaresch et al. 1976), but during the last few years (Lancet 1978) treatment with lipid lowering agents, especially atromidin and niacin, earlier considered safe and free from disturbing side effects, has come into miscredit
764

Corneal Arcus and Blood Lipads in the Middlr-agtd
becaused of stated connexion with gall-stones (atromidin) and skin disorders (niacin) and suspected connexions with gastro-intestinal malignancies, precipitation of cardiac arrhythmias and sudden death.
Although the clinical benefice of diagnosing hypercholesterolemia in a n other- wise symptom-free person thus seems debatable, better and safer treatment might become available for fu ture use, and until then the above-mentioned lipid lowering
agents are still in widespread use. We would therefore, as a prophylactic precaution against hypercholesterolemia,
suggest lipid screening on any pre-middle-aged person with marked, especially nasally marked , corneal arcus.
References
Cogan D. G. (1974) The corneal arcus. N. En$. J . Med. 291, 1356. Cogan D. G. & Kuwabara T. (1959) Arcus senilis, its pathology and histochemistry. Arch.
Committee of Principal Investigators (1978) Clofibrate: a final verdict? Lancet I, 113 1-1 132. Coronary Drug Project Research Group (1975) Clofibrate and niacin in coronary heart
Forsius H. (1954) Arcus sen& corneae. Acta ophthal. (Kbh.), Suppl. 42, 1-78. Groups of Physicians of the Newcastle upon Tyne Region (1971) Trial of clofibrate in the
treatment of ischaemic heart disease. Brit. Med. J . 4, 767-775. Immich H., Jansen H. H. & Pisani K. (1967) Die beziehungen zwischen Arcus Lipoides der
Hornhaut und Arteriosklerose. Vergleichende Untersuchungen von 500 Sektionsfallen. Klin. Wschr. 45, 1017-1020.
Jaeger W. & Eisenhauer G. G. (1977) Der diagnostische Wert der Arcus corneae als Hinweis auf Lipoidstoffwechselstorungen. Klin. Mbl. Augenheilk. 171, 32 1-330.
Parwaresch M. R., Haacke H.M., Mader Ch. & Godt Ch. (1976) Arcus lipoides corneae und Hyperlipoproteinamie. Klin. Wschr. 54,495497.
Post D. (1966) Modellversuche zur Entstehung des Arcus Lipoides corneae im Geldiffusions- versuche nach Ouchterlony. Albrecht 11. Grarfes Arch. klin, exp. Ophthal. 170, 123-126.
Research Committee of the Scottish Society of Physicians (1971) Ischaemic heart disease: A secondary prevention trial using clofibrate. Brit. Med.J . 4 , 775-784.
Rosenman R. H., Brand R. J., Sholtz R. 1. &Jenkins C. D. (1974) Relation of corneal arcus to cardiovascular risk factors and the incidence of coronary disease. N. En&. J . Med. 291, 1322-1 324.
Wood P. D. S., Stern M. P., Solvers A,, Reaven G. M. & Groeben J. v. d. (1972) Prevalence of plasma lipoprotein abnormalities in a free living popoulation of the Central Valley, California. Circulation XLV, 114-126.
Ophthal. (Chicago) 61,553-560.
disease. J . Amer. med. Ass. 231, 360-380.
Author’s address: L. Varnek, Eye Department. Gentofte Hospital, DK-2900, Hellerup, Denmark
765





























