Embed Size (px)
Citation preview
www.rush.edu
Prenatal Care in Adolescent Pregnancy
Tiffany Aossey, Chelsea Humpal, Jacqueline Lagman, Abbey McGrath
www.rush.edu ©2009%Rush%University%Medical%Center%
In 2012, 300,000 babies were born to teen mothers, age 15-19 (CDC Teen Pregnancy, 2014). Pregnancy in adolescents is associated with preeclampsia, labor dystocia, and preterm birth. Pregnant adolescents are are at an increased risk of experiencing psychosocial issues (Debiec et al., 2010). In adolescent teens, the risk for preterm labor is 8 times higher when no prenatal care is initiated (Debiec et al., 2010). Healthy People 2020: Maternal, Infant, and Child Health: Increase proportion of pregnant women who receive prenatal care in first trimester by 10% (MICH-10.1) (2014).
Background & Significance
www.rush.edu
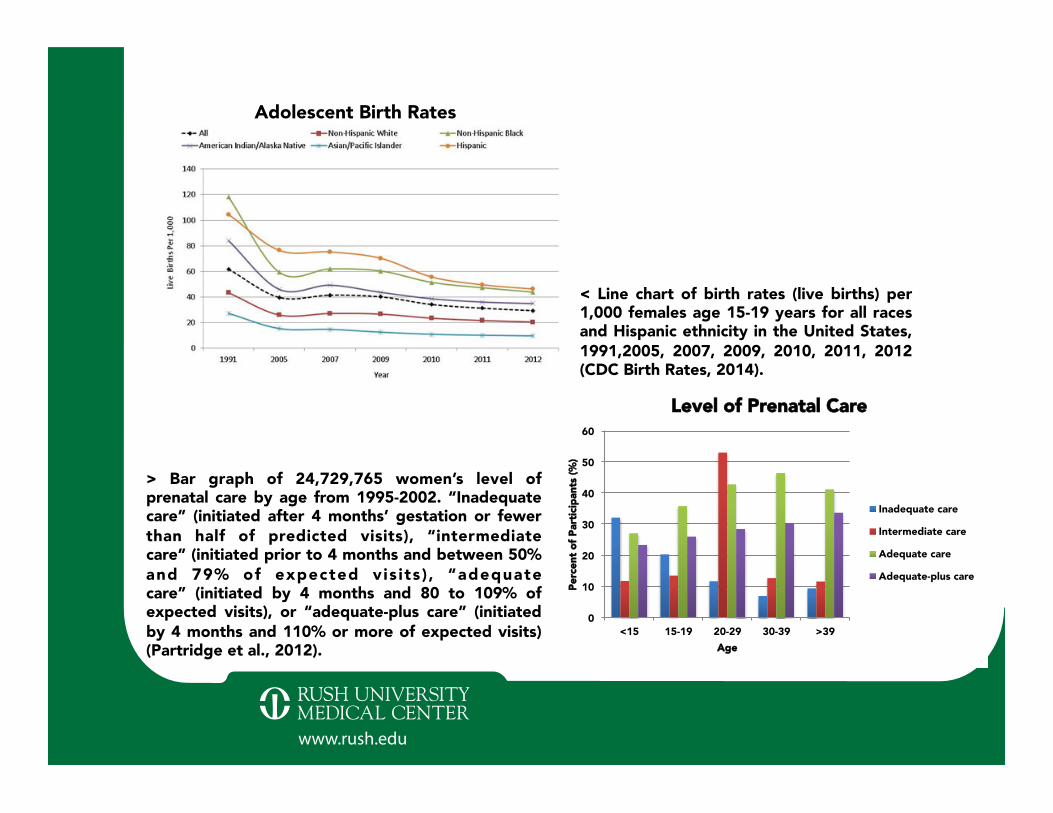
Adolescent Birth Rates
< Line chart of birth rates (live births) per 1,000 females age 15-19 years for all races and Hispanic ethnicity in the United States, 1991,2005, 2007, 2009, 2010, 2011, 2012 (CDC Birth Rates, 2014).
> Bar graph of 24,729,765 women’s level of prenatal care by age from 1995-2002. “Inadequate care” (initiated after 4 months’ gestation or fewer than half of predicted visits), “intermediate care” (initiated prior to 4 months and between 50% and 79% of expected vis its ) , “adequate care” (initiated by 4 months and 80 to 109% of expected visits), or “adequate-plus care” (initiated by 4 months and 110% or more of expected visits) (Partridge et al., 2012).
0
10
20
30
40
50
60
<15 15-19 20-29 30-39 >39
Perc
ent o
f Par
ticip
ants
(%)
Age
Level of Prenatal Care
Inadequate care
Intermediate care
Adequate care
Adequate-plus care
www.rush.edu
Despite ongoing decline in adolescent birth rates, U.S. rates (31.3%) remain one of the highest among industrialized nations (Cypher, 2013). 15.3% of adolescents wait until after the first trimester to initiate prenatal care compared with 4.4% of adult women (Kingston et al., 2014). 44% of adolescents <15 and 33.8% of adolescents 15-19 receive inadequate or intermediate care (Partridge et al., 2012). In 2009, infants of teenage mothers had the highest rate of mortality at 9.05 per 1,000 births (Planned Parenthood, 2013).
Prevalence of Problem
www.rush.edu
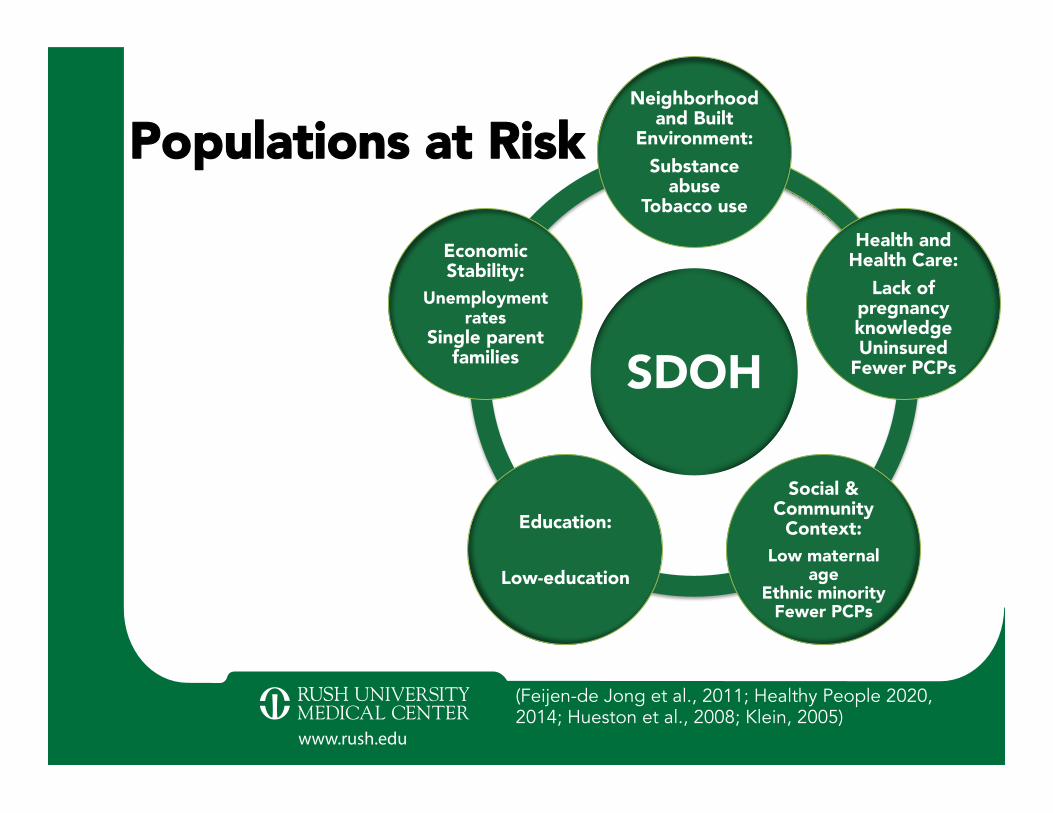
Populations at Risk
SDOH
Neighborhood and Built
Environment: Substance
abuse Tobacco use
Health and Health Care:
Lack of pregnancy knowledge Uninsured
Fewer PCPs
Social & Community
Context: Low maternal
age Ethnic minority
Fewer PCPs
Education:
Low-education
Economic Stability:
Unemployment rates
Single parent families
(Feijen-de Jong et al., 2011; Healthy People 2020, 2014; Hueston et al., 2008; Klein, 2005)
www.rush.edu
Purpose of Inquiry • Determine evidence-based prenatal care strategies
effective for adolescents Search Strategy • CINAHL • Pubmed • CDC National Vital Statistics • DHHS Search terms: “adolescent pregnancy”; “prenatal care” Exclusion criteria: published before 2001
Prenatal Care in U.S. Adolescents
www.rush.edu ©2009%Rush%University%Medical%Center%
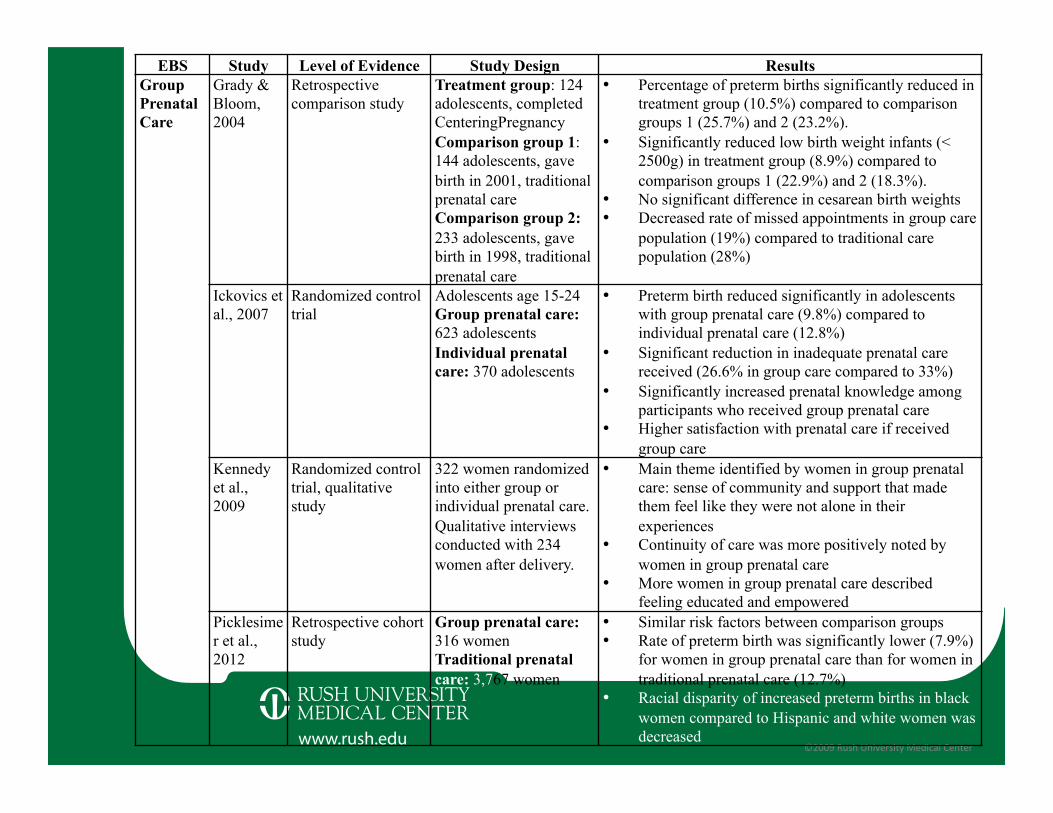
EBS Study Level of Evidence Study Design Results Group Prenatal Care
Grady & Bloom, 2004
Retrospective comparison study
Treatment group: 124 adolescents, completed CenteringPregnancy Comparison group 1: 144 adolescents, gave birth in 2001, traditional prenatal care Comparison group 2: 233 adolescents, gave birth in 1998, traditional prenatal care
• Percentage of preterm births significantly reduced in treatment group (10.5%) compared to comparison groups 1 (25.7%) and 2 (23.2%).
• Significantly reduced low birth weight infants (< 2500g) in treatment group (8.9%) compared to comparison groups 1 (22.9%) and 2 (18.3%).
• No significant difference in cesarean birth weights • Decreased rate of missed appointments in group care
population (19%) compared to traditional care population (28%)
Ickovics et al., 2007
Randomized control trial
Adolescents age 15-24 Group prenatal care: 623 adolescents Individual prenatal care: 370 adolescents
• Preterm birth reduced significantly in adolescents with group prenatal care (9.8%) compared to individual prenatal care (12.8%)
• Significant reduction in inadequate prenatal care received (26.6% in group care compared to 33%)
• Significantly increased prenatal knowledge among participants who received group prenatal care
• Higher satisfaction with prenatal care if received group care
Kennedy et al., 2009
Randomized control trial, qualitative study
322 women randomized into either group or individual prenatal care. Qualitative interviews conducted with 234 women after delivery.
• Main theme identified by women in group prenatal care: sense of community and support that made them feel like they were not alone in their experiences
• Continuity of care was more positively noted by women in group prenatal care
• More women in group prenatal care described feeling educated and empowered
Picklesimer et al., 2012
Retrospective cohort study
Group prenatal care: 316 women Traditional prenatal care: 3,767 women
• Similar risk factors between comparison groups • Rate of preterm birth was significantly lower (7.9%)
for women in group prenatal care than for women in traditional prenatal care (12.7%)
• Racial disparity of increased preterm births in black women compared to Hispanic and white women was decreased
www.rush.edu ©2009%Rush%University%Medical%Center%
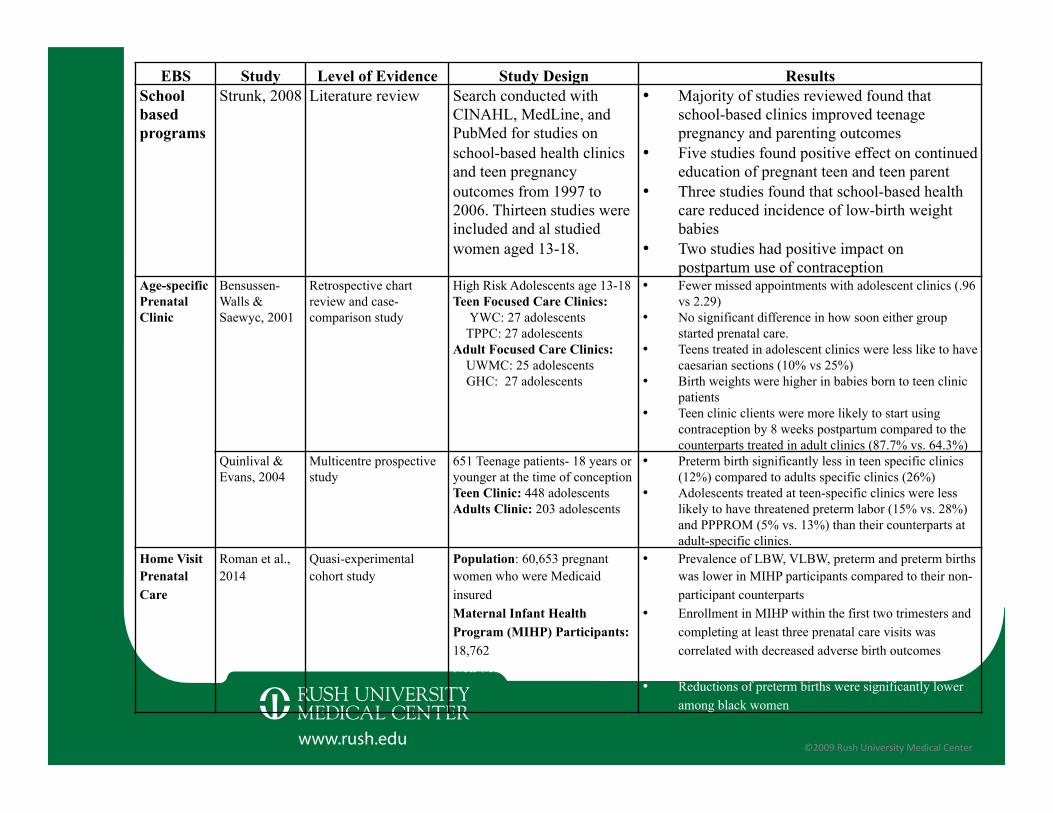
EBS Study Level of Evidence Study Design Results School based programs
Strunk, 2008 Literature review Search conducted with CINAHL, MedLine, and PubMed for studies on school-based health clinics and teen pregnancy outcomes from 1997 to 2006. Thirteen studies were included and al studied women aged 13-18.
• Majority of studies reviewed found that school-based clinics improved teenage pregnancy and parenting outcomes
• Five studies found positive effect on continued education of pregnant teen and teen parent
• Three studies found that school-based health care reduced incidence of low-birth weight babies
• Two studies had positive impact on postpartum use of contraception
Age-specific Prenatal Clinic
Bensussen-Walls & Saewyc, 2001
Retrospective chart review and case-comparison study
High Risk Adolescents age 13-18 Teen Focused Care Clinics: YWC: 27 adolescents TPPC: 27 adolescents Adult Focused Care Clinics: UWMC: 25 adolescents GHC: 27 adolescents
• Fewer missed appointments with adolescent clinics (.96 vs 2.29)
• No significant difference in how soon either group started prenatal care.
• Teens treated in adolescent clinics were less like to have caesarian sections (10% vs 25%)
• Birth weights were higher in babies born to teen clinic patients
• Teen clinic clients were more likely to start using contraception by 8 weeks postpartum compared to the counterparts treated in adult clinics (87.7% vs. 64.3%)
Quinlival & Evans, 2004
Multicentre prospective study
651 Teenage patients- 18 years or younger at the time of conception Teen Clinic: 448 adolescents Adults Clinic: 203 adolescents
• Preterm birth significantly less in teen specific clinics (12%) compared to adults specific clinics (26%)
• Adolescents treated at teen-specific clinics were less likely to have threatened preterm labor (15% vs. 28%) and PPPROM (5% vs. 13%) than their counterparts at adult-specific clinics.
Home Visit Prenatal Care
Roman et al., 2014
Quasi-experimental cohort study
Population: 60,653 pregnant women who were Medicaid insured Maternal Infant Health Program (MIHP) Participants: 18,762 Non-MIHP Participants: 41,891
• Prevalence of LBW, VLBW, preterm and preterm births was lower in MIHP participants compared to their non-participant counterparts
• Enrollment in MIHP within the first two trimesters and completing at least three prenatal care visits was correlated with decreased adverse birth outcomes (LBW, VLBW, preterm births) for all races
• Reductions of preterm births were significantly lower among black women
www.rush.edu ©2009%Rush%University%Medical%Center%
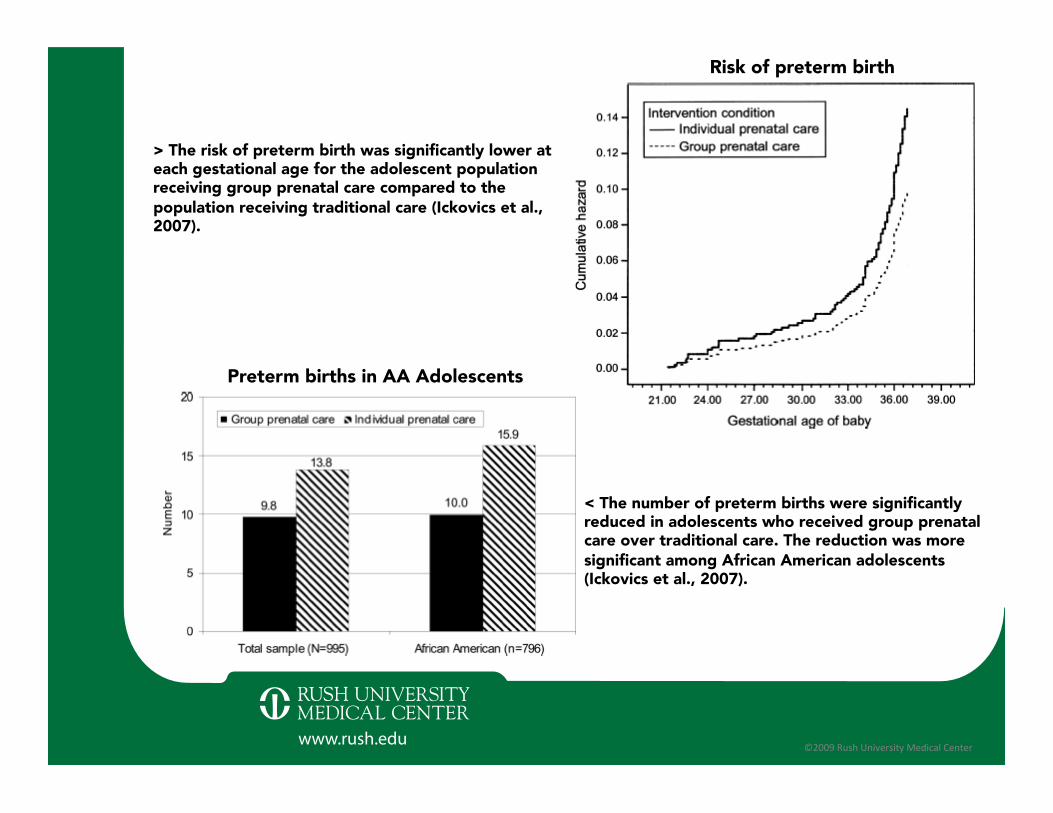
< The number of preterm births were significantly reduced in adolescents who received group prenatal care over traditional care. The reduction was more significant among African American adolescents (Ickovics et al., 2007).
> The risk of preterm birth was significantly lower at each gestational age for the adolescent population receiving group prenatal care compared to the population receiving traditional care (Ickovics et al., 2007).
Preterm births in AA Adolescents
Risk of preterm birth
www.rush.edu ©2009%Rush%University%Medical%Center%
Group prenatal care models, age-specific clinics, and school-based health centers are effective in adolescent populations at: • Decreasing adverse perinatal outcomes • Decreasing missed appointment rates
Home visit prenatal care were effective reaching low income populations and decreasing adverse birth outcomes especially in black women • More research is needed in adolescent population
Evidence Based Strategies
www.rush.edu ©2009%Rush%University%Medical%Center%
Group prenatal care: discussion based format increased health education, skills development, peer support, continuity of care, patient satisfaction Age-specific clinics: multidisciplinary case management focused on developing trust, rapport, emphasizing confidentiality School-based clinics: focus on increased early access to prenatal care and maintaining access to education Home visit care: decreasing barriers to early access
Overcoming SDOH in Adolescents
www.rush.edu
Limited research in prenatal care among adolescents • Little research addressing evidence based strategies
for increasing early prenatal care utilization in teens • No research focused on overcoming barriers to care • Some research focused on high risk populations, no
research on cultural competency
Healthy People 2020: Maternal, Infant, and Child Health • Increase proportion of pregnant women who receive
prenatal care in first trimester by 10% (MICH-10.1) (2014)
• No evidence based recommendations to achieve goal
Gaps in Current Body of Evidence
www.rush.edu
Gaps are indicative of specific areas where nursing research should be conducted: • Outpatient & inpatient MBU APNs & RNs can
organize data collection to survey pregnant adolescents
• Public health nurses collect data in the community Research should address: • Barriers preventing early prenatal care • Factors promoting access to care in 1st trimester • Nurses should expand indicators for initiation of
prenatal care: e.g. time between conception and 1st prenatal appointment
Implications for Nursing Research

www.rush.edu ©2009%Rush%University%Medical%Center%
As nurses we can: • Advocate for creation and funding of group prenatal
classes, school based programs and age based prenatal clinics especially in areas of low SES and where access is limited
• Advocate to government (local and national), community leaders, join committees
• Lead group prenatal classes, school based classes and age based prenatal clinics
• Educate adolescents on the importance of prenatal care, where and how to access prenatal care
Implications for Nursing Practice
www.rush.edu ©2009%Rush%University%Medical%Center%
CICS Ralph Ellison High School: 9-12th grade • Primarily African American and Latino students • Teen Birth Rates (2009) (City of Chicago, 2011)
Auburn Gresham: 83.1 per 1000 females Chicago: 57 per 1000 females
Nursing Role: • School nurse as a resource • CPS sexual health course
Focus on: • Signs and symptoms of pregnancy • Importance of prenatal care • Awareness of available resources
Clinical Site

www.rush.edu ©2009%Rush%University%Medical%Center%
Bensussen-Walls, W. & Saewyc, E. M. (2002). Teen-focused care versus adult-focused care for the high-risk pregnant adolescent: An outcomes evaluation. Public Health Nursing, 18(6), 424-435 doi: 10.1046/j.1525-1446.2001.00424.x City of Chicago. (2011). Public health statistics: Birth to mothers age 15-19 years old in Chicago, by year, 1999-2009. Retrieved from https://data.cityofchicago.org/Health-Human-Services/Public-Health-Statistics-Births-to-mothers-aged-15/9kva-bt6k Centers for Disease Control and Preventions. (2014). Birth rates (live births) per 1,000 females aged 15–19 years, by race and hispanic ethnicity, Select Years [Graph]. Retrieved from http://www.cdc.gov/teenpregnancy/longdescriptors.htm Centers for Disease Control and Preventions. (2014). CDC - About teen pregnancy - Teen pregnancy - reproductive health. Retrieved from http://www.cdc.gov/teenpregnancy/aboutteenpreg.htm Cypher, R. L. (2013). Collaborative approaches to prenatal care: Strategies to successful adolescent programs Journal of Perinatal Neonatal Nursing, 27(2), 134-144. Retrieved from http://www-ncbi-nlm-nih-gov.ezproxy.rush.edu/pubmed/23618934 Debiec K. E., Paul , K. J., Mitchell, C. M., & Hitti, J. E. (2010). Inadequate prenatal care and risk of preterm delivery among adolescents: a retrospective study over 10 years. American Journal of Obstetrics and Gynecology, 203(2), l22.e1-e6. doi: 10.1016/j.ajog.2010.03.001 Feijen-de Jong, E. I., Jansen, D. E., Baarveld, F., van der Schans, C. P., Schellevis, F. G., & Reijneveld, S. A. (2011). Determinants of late and/or inadequate use of prenatal healthcare in high-income countries: a systematic review. The European Journal of Public Health, ckr164. doi: 10.1093/eurpub/ckr164
References
www.rush.edu ©2009%Rush%University%Medical%Center%
Grady, M. A., & Bloom, K. C. (2004). Pregnancy outcomes of adolescents enrolled in a CenteringPregnancy program. Journal of Midwifery & Women’s Health, 49(5), 412-420. doi 10.1016/j.jmwh.2004.05.009 Healthy People 2020. (2014). Maternal, infant, and child health. Retrieved from http://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health/objectives Healthy People 2020. (2014). Maternal, infant, and child health. Retrieved from http://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health/objectives Healthy People 2020. (2014). Social determinants of health. Retrieved from http://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-health es/topic/social-determinants-health Hueston, W. J., Geesey, M. E., & Diaz, V. (2008). Prenatal care initiation among pregnant teens in the United States: an analysis over 25 years. Journal of Adolescent Health, 42(3), 243-248. doi: 10.1016/j.jadohealth.2007.08.027 Ickovics, J. R., Kershaw, T. S., Westdahl, C., Magriples, U., Massey, Z., Reynolds, H., & Rising, S. S. (2007). Obstetrics & Gynecology, 110(2), 330-339 doi 10.1097/01.AOG.0000275284.24298.23 Kennedy, H. P., Farrell, T., Paden, R., Hill, S., Jolivet, R., Willetts, J., & Rising, S. S. (2009). “I wasn’t along”--a study of group prenatal care in the military. Journal of Midwifery and Women’s Health, 54(3), 176-183. doi 10.1016/j.jmwh.2008.11.004 Kingston, D., Heaman, M., Fell, D., & Chalmers, B. (2012). Comparison of adolescent, young adult, and adult women’s maternity experiences and practices. Pediatrics, 129(5), e1228-e1237. doi: 10.1542/peds.2011-1447
References
www.rush.edu ©2009%Rush%University%Medical%Center%
References Klein, J. D. (2005). Adolescent pregnancy: Current trends and issues. Pediatrics, 116(1), 281-286. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/?term=Klein%2C+J.+D.+(2005).+Adolescent+pregnancy%3A+Current+trends+and+issues.+Pediatrics%2C+116(1)%2C+281-286. Mathews, T., S., M., MacDorman, M., & Division of Vital Statistics. (2013). Infant mortality statistics from the 2009 period linked birth/infant death data set. National Vital Statistics Report, 61(8), 1-28. Retrieved from http://www.cdc.gov/nchs/data/nvsr/nvsr61/nvsr61_08.pdf Partridge, S., Balayla, J., Holcroft, C. A., & Abenhaim, H. A. (2012). Inadequate prenatal care utilization and risks of infant mortality and poor birth outcome: A retrospective analysis of 28,729,765 US deliveries over 8 years. American Journal of Perinatology, 29(10), 787. Picklesimer, A. H., Billings, D., Hale, N., Blackhurst, D., & Covington-Kolb, S. (2012). The effect of CenteringPregnancy group prenatal care on preterm birth in a low-income population. American Journal of Obstetric Gynecology, 206(5), 415.e1-7. doi 10.1016/ j.ajog.2012.01.040 Planned Parenthood Federation of America. (2013, June). Pregnancy and Childbearing Among U.S. Teens. Retrieved from http://www.plannedparenthood.org/files/2013/9611/7570/Pregnancy_And_Childbearing_Among_US_Teens.pdf Quinlivan, J. A., & Evans, S. F. (2004). Teenage antenatal clinics may reduce the rate of preterm birth: A prospective study. BJOG: An International Journal of Obstetrics & Gynaecology, 111(6), 571-578. Retrieved from http://www.ncbi.nih.gov/pubmed/?term=Quinlivan%2C+J.+A.%2C+%26+Evans%2C+S.+F.+(2004).+Teenage+antenatal+clinics+may+reduce+the+rate+of+preterm+birth%3A+a+prospective+study.+BJOG%3A+An+International+Journal+of+Obstetrics+%26+Gynaecology%2C+111(6)%2C+571-578.
www.rush.edu ©2009%Rush%University%Medical%Center%
References Roman, L., Raffo, J. E., Zhu, Q., & Meghea, C. I. (2014). A statewide medicaid enhanced prenatal care program: Impact on birth outcomes. JAMA Pediatrics, 168(3), 220-227. doi: 10.1001/jamapediatrics.2013.4347 Rotundo, G. (2011) Centering pregnancy: The benefits of group prenatal care. Nursing for Women’s Health, 15(6), 508-517. doi 10.1111/j.1751-486X.2011.01678.x Strunk, J. A. (2008). The effect of school-based health clinics on teenage pregnancy and parenting outcomes: An integrated literature review. The Journal of School Nursing, 24(1), 13-20. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/?term=Strunk+JA.+The+effect+of+school-based+health+clinics+on+teenage+pregnancy+and+parenting+outcomes%3A+an+integrated+literature+review.+J+Sch+Nurs.+2008%3B24%3A13%E2%80%932