Embed Size (px)
Citation preview

Predictors of Unsuccessful Electrical Cardioversion inAtrial Fibrillation
Abdou Elhendy, MD, PhD, Federico Gentile, MD, Bijoy K. Khandheria, MD,Stephen C. Hammill, MD, Bernard J. Gersh, MB, ChB, DPhil, Kent R. Bailey, PhD,
Samantha Montgomery, MSc, Kelli Burger, BSc, and James B. Seward, MD
Restoration of sinus rhythm improves functionalcapacity and alleviates palpitations in patients
with atrial fibrillation (AF).1,2 The advantages of di-rect-current cardioversion include the immediate res-toration of sinus rhythm, as opposed to the unpredict-able time to cardioversion in pharmacologic interven-tion, and the avoidance of potential adverse drugreactions.3 Although direct-current cardioversion isthought to have a higher success rate than pharmaco-logic intervention, it may fail to restore sinus rhythmin 5% to 30% of procedures.4–9 Few data are availableregarding the association between clinical variablesand the failure of direct-current cardioversion. Also,the relation between abnormalities of cardiac functionand the success of direct-current cardioversion has notbeen studied in a large number of patients. This studyassesses the success rate of direct-current cardiover-sion in patients with AF and the relation betweenclinical and echocardiographic variables and the suc-cess of direct-current cardioversion.
• • •We studied 692 patients (459 men [66%] and 233
women [34%], mean age � SD 67 � 13 years) withAF who had a first elective direct-current cardiover-sion at Mayo Clinic (Rochester, Minnesota). Thisstudy was approved by the Institutional Review Boardof the Mayo Foundation. The duration of AF was �48hours in 653 patients (94%) and �48 hours in 39patients (6%). All patients underwent transthoracicechocardiography before cardioversion. Transesopha-geal echocardiography was performed in 201 patients(29%) before cardioversion.
A history of coronary artery disease was consid-ered present if the patient had had a previous myocar-dial infarction, myocardial revascularization, signifi-cant coronary artery stenosis on angiography, or typ-ical anginal complaints. Valvular heart disease wasconsidered present if the patient had more than mildstenosis or regurgitation of �1 cardiac valve. Idio-pathic dilated cardiomyopathy was defined as leftventricular dilatation and global hypokinesia withoutsignificant coronary artery disease. The duration ofAF was determined by the time of documentation ofAF on the electrocardiogram or the onset of symp-toms, whichever occurred earlier.
Two-dimensional and M-mode imaging were per-
formed with commercially available echocardio-graphic machines equipped with 2.5- and 3.5-MHzphased-array transducers. M-mode echocardiographywas used to measure cardiac dimensions and wallthickness. A left atrial diameter of � 40 mm definedleft atrial dilatation. This was considered mild forvalues �50 mm and marked for values �50 mm.Ejection fraction at rest was measured using a previ-ously validated modification of the method of Qui-nones in Dujardin et al10 or by visual estimation.11
Structural heart disease was defined as any of thefollowing: valvular heart disease, coronary heart dis-ease, cardiomyopathy, or ejection fraction �50%.
All procedures were performed with electrocardio-graphic monitoring and full equipment for cardiopul-monary resuscitation. Digitalis preparations werewithheld for 24 to 48 hours before the procedure.After administration of intravenous sedation, synchro-nized direct-current monophasic shock was adminis-tered using the anteroposterior paddle position (sternalbody angle of the left scapula). If sinus rhythm wasnot restored after the first shock, the procedure wasrepeated (up to 4 times) using a larger number ofjoules (up to 360 J). The number of joules with whichcardioversion was initiated was determined for eachpatient according to physician discretion. Electrocar-diography was performed before and after the proce-dure to verify cardiac rhythm. Successful cardiover-sion was defined as restoration of sinus rhythm afteradministration of direct-current shock.
Unless specified, data are presented as mean values� SD or as frequency percentages. The rank sum andchi-square tests were used to compare differencesbetween continuous variables and proportions, respec-tively. Univariate and multivariate stepwise logisticregression models were used to identify individual andjoint predictors of unsuccessful cardioversion. Analy-ses of success were done using both the patient and theindividual shock as the unit of observation to harvestinformation when multiple shocks were needed. Dif-ferences were considered significant if the null hy-pothesis could be rejected at the 0.05 probability level.
These diseases were present in the study popula-tion: systemic hypertension in 355 patients (51%),coronary artery disease in 233 patients (34%), valvu-lar heart disease in 227 patients (33%), and cardiomy-opathy (idiopathic dilated, restrictive, or hypertrophic)in 125 patients (18%). Cardioversion was successfulin 592 patients (86%) and unsuccessful in 100 (14%).The mean number of shocks was 2.1 � 1.2/patient.The mean number of joules was 222 � 100. In 74patients, 50 J was used initially, with success achieved
From the Division of Cardiovascular Diseases and Internal Medicineand the Section of Biostatistics, Mayo Clinic, Rochester, Minnesota.Dr. Khandheria’s address is: Mayo Clinic, 200 First Street SW,Rochester, Minnesota 55905. Manuscript received June 13, 2001;revised manuscript received and accepted September 6, 2001.
83©2002 by Excerpta Medica, Inc. All rights reserved. 0002-9149/02/$–see front matterThe American Journal of Cardiology Vol. 89 January 1, 2002 PII S0002-9149(01)02172-5
in 29 (39%). Of 398 patients receiving 100 J, cardio-version was successful in 118 (30%). Of 426 patientsreceiving 200 J, cardioversion was successful in 240(56%). The clinical characteristics of the patients withsuccessful cardioversion and unsuccessful cardiover-sion are listed in Table 1. The groups did not differsignificantly in terms of age, gender, or prevalence ofprevious myocardial infarction, systemic hyperten-sion, diabetes mellitus, coronary artery disease, val-vular heart disease, or structural heart disease. Patients
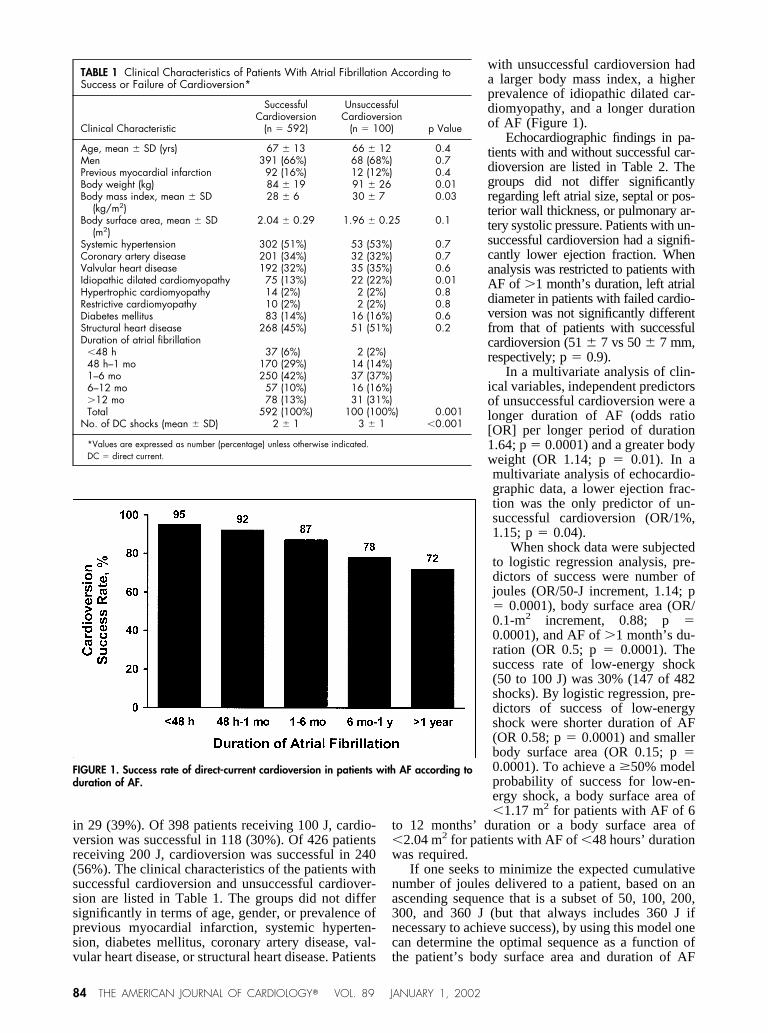
with unsuccessful cardioversion hada larger body mass index, a higherprevalence of idiopathic dilated car-diomyopathy, and a longer durationof AF (Figure 1).
Echocardiographic findings in pa-tients with and without successful car-dioversion are listed in Table 2. Thegroups did not differ significantlyregarding left atrial size, septal or pos-terior wall thickness, or pulmonary ar-tery systolic pressure. Patients with un-successful cardioversion had a signifi-cantly lower ejection fraction. Whenanalysis was restricted to patients withAF of �1 month’s duration, left atrialdiameter in patients with failed cardio-version was not significantly differentfrom that of patients with successfulcardioversion (51 � 7 vs 50 � 7 mm,respectively; p � 0.9).
In a multivariate analysis of clin-ical variables, independent predictorsof unsuccessful cardioversion were alonger duration of AF (odds ratio[OR] per longer period of duration1.64; p � 0.0001) and a greater bodyweight (OR 1.14; p � 0.01). In amultivariate analysis of echocardio-graphic data, a lower ejection frac-tion was the only predictor of un-successful cardioversion (OR/1%,1.15; p � 0.04).
When shock data were subjectedto logistic regression analysis, pre-dictors of success were number ofjoules (OR/50-J increment, 1.14; p� 0.0001), body surface area (OR/0.1-m2 increment, 0.88; p �0.0001), and AF of �1 month’s du-ration (OR 0.5; p � 0.0001). Thesuccess rate of low-energy shock(50 to 100 J) was 30% (147 of 482shocks). By logistic regression, pre-dictors of success of low-energyshock were shorter duration of AF(OR 0.58; p � 0.0001) and smallerbody surface area (OR 0.15; p �0.0001). To achieve a �50% modelprobability of success for low-en-ergy shock, a body surface area of�1.17 m2 for patients with AF of 6
to 12 months’ duration or a body surface area of�2.04 m2 for patients with AF of �48 hours’ durationwas required.
If one seeks to minimize the expected cumulativenumber of joules delivered to a patient, based on anascending sequence that is a subset of 50, 100, 200,300, and 360 J (but that always includes 360 J ifnecessary to achieve success), by using this model onecan determine the optimal sequence as a function ofthe patient’s body surface area and duration of AF
TABLE 1 Clinical Characteristics of Patients With Atrial Fibrillation According toSuccess or Failure of Cardioversion*
Clinical Characteristic
SuccessfulCardioversion
(n � 592)
UnsuccessfulCardioversion
(n � 100) p Value
Age, mean � SD (yrs) 67 � 13 66 � 12 0.4Men 391 (66%) 68 (68%) 0.7Previous myocardial infarction 92 (16%) 12 (12%) 0.4Body weight (kg) 84 � 19 91 � 26 0.01Body mass index, mean � SD
(kg/m2)28 � 6 30 � 7 0.03
Body surface area, mean � SD(m2)
2.04 � 0.29 1.96 � 0.25 0.1
Systemic hypertension 302 (51%) 53 (53%) 0.7Coronary artery disease 201 (34%) 32 (32%) 0.7Valvular heart disease 192 (32%) 35 (35%) 0.6Idiopathic dilated cardiomyopathy 75 (13%) 22 (22%) 0.01Hypertrophic cardiomyopathy 14 (2%) 2 (2%) 0.8Restrictive cardiomyopathy 10 (2%) 2 (2%) 0.8Diabetes mellitus 83 (14%) 16 (16%) 0.6Structural heart disease 268 (45%) 51 (51%) 0.2Duration of atrial fibrillation
�48 h 37 (6%) 2 (2%)48 h–1 mo 170 (29%) 14 (14%)1–6 mo 250 (42%) 37 (37%)6–12 mo 57 (10%) 16 (16%)�12 mo 78 (13%) 31 (31%)Total 592 (100%) 100 (100%) 0.001
No. of DC shocks (mean � SD) 2 � 1 3 � 1 �0.001
*Values are expressed as number (percentage) unless otherwise indicated.DC � direct current.
FIGURE 1. Success rate of direct-current cardioversion in patients with AF according toduration of AF.
84 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 89 JANUARY 1, 2002
(�1 month or �1 month). For example, for a patientwith a body surface area of 1.2 m2 and AF of �1 month’sduration, the cumulative number of joules can beminimized by selecting the sequence (50 J, 360 J),with an expected cumulative number of joules of 226.Similarly, for a patient with a body surface area of 1.2m2 and AF of �1 month’s duration, the same se-quence (50 J, 360 J) is optimal, with an expectedcumulative number of joules of 167. However, a pa-tient with a body surface area of 3.0 m2 and AF of �1month’s duration should receive 1 shock at 360 J tominimize the expected cumulative number of joules.In Table 3 we provide a model for calculating theprobability of successful cardioversion at each joulelevel for a given patient when the body surface areaand the duration of AF are known.
• • •In this study, we assessed the predictors of success
of direct-current cardioversion in 692 patients withAF. Sinus rhythm was restored in 86% of patients.The success of cardioversion was not related to age,gender, presence of systemic hypertension, coronaryartery disease, or valvular heart disease.
Clinical variables associated withhigher likelihood of unsuccessfulcardioversion were a greater bodyweight, a longer duration of AF, andthe presence of idiopathic dilatedcardiomyopathy as the underlyingheart disease. The association of un-successful cardioversion with agreater body weight and body massindex may reflect a weight-relatedincrease of electrical impedance thatimpairs conduction of the direct-cur-rent shock to the atria. The associa-tion of unsuccessful cardioversionwith AF duration may indicate atrialelectrical and mechanical remodel-ing. This concept implies that AFbegets AF by a number of mecha-nisms that bring about a reducedatrial effective refractory period andthe generation of multiple wavelets,which leads to an increased atrialrate12,13 and consequently a lowerlikelihood of conversion to sinusrhythm. AF has also been associatedwith structural changes of left atrial
myocytes, which may be adaptive (de-differentiationof cardiomyocytes) or maladaptive (degeneration ofcells with replacement fibrosis).14 These changes aremore profound in patients with AF of longer durationand may partly explain the lower success rate ofcardioversion in patients with AF of longer duration.Nevertheless, 72% of the 109 patients with AF for�12 months were restored to sinus rhythm in thisstudy.
Idiopathic dilated cardiomyopathy was the onlyunderlying cardiac disease associated with a higherrate of unsuccessful cardioversion. In dilated cardio-myopathy the reduction of systolic function and sub-sequent elevation of left atrial filling pressure mayaffect the electrical activity of the atria. However, amore plausible explanation is that the atria are in-volved in the structural and functional changes thatoccur in idiopathic dilated cardiomyopathy. Left atrialsystolic dysfunction, unexplained by altered loadingconditions, has been reported in idiopathic dilatedcardiomyopathy, suggesting left atrial involvement inthe myopathic process.15 These changes may indepen-dently affect the response of AF to cardioversion inpatients with dilated cardiomyopathy.
No significant difference in left atrial size, septal orposterior wall thickness, or pulmonary artery systolicpressure was detected between patients with success-ful and those with unsuccessful cardioversion. Pa-tients with unsuccessful cardioversion had a signifi-cantly lower ejection fraction. These findings indicatethat a larger left atrial dimension should not be con-sidered a contraindication to attempted cardioversion;cardioversion was successful in 83% of patients witha greatly enlarged left atrium. In a study using chron-ically implanted defibrillation leads in 8 adult sheep,Power et al16 found that the minimal energy require-
TABLE 2 Echocardiographic Findings in Patients With Atrial Fibrillation Accordingto Success or Failure of Cardioversion*
Echocardiographic Findings
SuccessfulCardioversion
(n � 592)
UnsuccessfulCardioversion
(n � 100) p Value
Left atrial sizeNormal 111 (19%) 16 (16%)Mildly enlarged 242 (41%) 47 (47%)Markedly enlarged 239 (40%) 37 (37%)
Total 592 (100%) 100 (100%) 0.6LA diameter (range) (mm) 50 � 8 (29–93) 51 � 8 (35–84) 0.3LV end-diastolic diameter
(range) (mm)53 � 9 (32–81) 54 � 10 (42–76) 0.3
LV end-systolic diameter(range) (mm)
38 � 11 (15–74) 40 � 12 (17–67) 0.2
Septal wall thickness (diastole)(range) (mm)
11 � 3 (5–28) 11 � 3 (7–25) 0.7
Posterior wall thickness (diastole)(range) (mm)
11 � 2 (6–24) 11 � 2 (7–20) 0.5
Ejection fraction (range) 0.50 � 0.15 (10–80) 0.47 � 0.16 (10–85) 0.04Pulmonary artery systolic pressure
(range) (mm Hg)43 � 12 (24–106) 44 � 15 (23–140) 0.7
Presence of intracardiac thrombi 6 (1%) 0 (0%) 0.6Spontaneous echo contrast (TEE) 86/166 (52%) 14/35 (40%) 0.2
*Values are expressed as number (percentage) or mean � SD.LA � left atrial; LV � left ventricular; TEE � transesophageal echocardiography.
TABLE 3 Logistic Model for Calculating Probability ofSuccessful Cardioversion in Patients With Atrial Fibrillation
Variable Coefficient
Intercept a 2.184Shock energy (J) b1 0.00260Body surface area (m2) b2 1.3186Duration of atrial fibrillation b3 0.6884
Probability of successful cardioversioneL
�1 � eL�, where e is the Napierian
natural base of 2.71828 and L � a � (b1·number of joules) � (b2·bodysurface area) � (b3·[1 if duration of atrial fibrillation �1 month, 0 otherwise]).
BRIEF REPORTS 85

ments for successful cardioversion were not signifi-cantly changed by ongoing left atrial dilatation. Theresults of our study confirm these findings, becauseleft atrial size was not predictive of cardioversionsuccess or the number of joules at which cardioversionwas successful.
Direct-current cardioversion was a successfulmethod for restoring sinus rhythm in 86% of patientswith AF undergoing a first elective cardioversion.Failure of cardioversion was related to a longer dura-tion of AF, a greater body weight, a lower ejectionfraction, and the presence of idiopathic dilated cardio-myopathy. Left atrial diameter was not related to thesuccess of cardioversion or the shock energy at whichcardioversion succeeded. We have provided an equa-tion by which the probability of success of cardiover-sion at a particular shock level can be derived if theduration of AF and the body surface area are known.
Patients with AF should not be deferred fromcardioversion on the basis of left atrial enlarge-ment. The use of low-energy shock should be re-stricted to patients with AF of shorter duration anda smaller body surface area to achieve successfulcardioversion with the fewest cumulative joules.
1. Gosselink AT, Crijns HJ, van den Berg MP, van den Broek SA, Hillege H,Landsman ML, Lie KI. Functional capacity before and after cardioversion ofatrial fibrillation: a controlled study. Br Heart J 1994;72:161–166.2. Kieny JR, Sacrez A, Facello A, Arbogast R, Bareiss P, Roul G, Demangeat JL,Brunot B, Constantinesco A. Increase in radionuclide left ventricular ejectionfraction after cardioversion of chronic atrial fibrillation in idiopathic dilatedcardiomyopathy. Eur Heart J 1992;13:1290–1295.3. Van Gelder IC, Tuinenburg AE, Schoonderwoerd BS, Tieleman RG, Crijns HJ.
Pharmacologic versus direct-current electrical cardioversion of atrial flutter andfibrillation. Am J Cardiol 1999;84(suppl):147R–151R.4. Lown B. Electrical reversion of cardiac arrhythmias. Br Heart J 1967;29:469–489.5. Lown B, Perlroth MG, Kaidbey S, Abe T, Harken DE. “Cardioversion” ofatrial fibrillation. A report on the treatment of 65 episodes in 50 patients. N EnglJ Med 1963;269:325–331.6. Jensen JB, Humphries JO, Kouwenhoven WB, Jude JR. Electroshock for atrialflutter and atrial fibrillation. Follow-up studies on 50 patients. JAMA 1965;194:1181–1184.7. Bjerkelund CJ, Orning OM. The efficacy of anticoagulant therapy in prevent-ing embolism related to D.C. electrical conversion of atrial fibrillation. Am JCardiol 1969;23:208–216.8. DeSilva RA, Graboys TB, Podrid PJ, Lown B. Cardioversion and defibrilla-tion. Am Heart J 1980;100:881–895.9. Levy S, Lauribe P, Dolla E, Kou W, Kadish A, Calkins H, Pagannelli F, MoyalC, Bremondy M, Schork A, et al. A randomized comparison of external andinternal cardioversion of chronic atrial fibrillation. Circulation 1992;86:1415–1420.10. Dujardin KS, Enriquez-Sarano M, Rossi A, Bailey KR, Seward JB. Echo-cardiographic assessment of left ventricular remodeling: are left ventriculardiameters suitable tools? J Am Coll Cardiol 1997;30:1534–1541.11. Stamm RB, Carabello BA, Mayers DL, Martin RP. Two-dimensional echo-cardiographic measurement of left ventricular ejection fraction: prospective anal-ysis of what constitutes an adequate determination. Am Heart J 1982;104:136–144.12. Wijffels MC, Kirchhof CJ, Dorland R, Power J, Allessie MA. Electricalremodeling due to atrial fibrillation in chronically instrumented conscious goats:roles of neurohumoral changes, ischemia, atrial stretch, and high rate of electricalactivation. Circulation 1997;96:3710–3720.13. Tieleman RG, Van Gelder IC, Crijns HJ, De Kam PJ, Van Den Berg MP,Haaksma J. Early recurrences of atrial fibrillation after electrical cardioversion: aresult of fibrillation-induced electrical remodeling of the atria? J Am Coll Cardiol1998;31:167–173.14. Thijssen VL, Ausma J, Liu GS, Allessie MA, van Eys GJ, Borgers M.Structural changes of atrial myocardium during chronic atrial fibrillation. Car-diovasc Pathol 2000;9:17–28.15. Triposkiadis F, Moyssakis I, Hadjinikolaou L, Makris T, Zioris H, Hatziza-harias A, Kyriakidis M. Left atrial systolic function is depressed in idiopathic andpreserved in ischemic dilated cardiomyopathy. Eur J Clin Invest 1999;29:905–912.16. Power JM, Beacom GA, Alferness CA, Raman J, Farish SJ, Tonkin AM.Effects of left atrial dilatation on the endocardial atrial defibrillation threshold: astudy in an ovine model of pacing induced dilated cardiomyopathy. Pacing ClinElectrophysiol 1998;21:1595–1600.
Effect of Weight Loss in Congestive Heart Failure fromIdiopathic Dilated Cardiomyopathy on
Electrocardiographic QRS Voltage
John E. Madias, MD, Himanshu Agarwal, MD, Moethu Win, MD, andLalitha Medepalli, MD
I t was appreciated in the 1950s and 1960s that pa-tients with congestive heart failure (CHF) had lower
QRS voltages on their electrocardiograms than theyhad when compensated.1–4 Also, 30 years ago Ish-ikawa et al5 documented an increase in ECG voltagesin 12 patients after treatment of CHF, whereas adecrease in the QRS amplitudes occurred in 3 patientswith poor response to therapy.5 Recently, a phenom-enon consisting of a reduction in ECG amplitude
commensurate with weight gain in patients with ana-sarca was reported6; the involved patients had a vari-ety of critical illnesses, mainly sepsis, and requiredadministration of large volumes of intravenous fluids.During the last month of implementation of thisstudy,6 we encountered in the coronary care unit 3patients with CHF who had the reverse phenomenon,i.e., an increase in the amplitude of electrocardio-grams in response to treatment of CHF, and a resultantloss of weight. These were the only patients admittedin the course of 1 month, with CHF and visible “pit-ting” peripheral edema in the pretibial aspect of theirlegs and the dorsum of their feet. Daily weights andstandard electrocardiograms were obtained. Measure-ments to the nearest 0.5 mm of the amplitude (highestpositive � lowest negative deflections) of the QRScomplex of all 12 leads were obtained by 1 of the
From the Zena and Michael Wiener Cardiovascular Institute, MountSinai/New York University Medical Center Health System; and Divi-sion of Cardiology, Elmhurst Hospital Center, Mount Sinai School ofMedicine, New York, New York. Dr. Madias’ address is: Division ofCardiology, Elmhurst Hospital Center, 79-01 Broadway, Elmhurst,New York 11373. E-mail: [email protected]. Manuscript receivedJuly 9, 2001; revised manuscript received and accepted August 27,2001.
86 ©2002 by Excerpta Medica, Inc. All rights reserved. 0002-9149/02/$–see front matterThe American Journal of Cardiology Vol. 89 January 1, 2002 PII S0002-9149(01)02173-7

![Sciorschen ISSN 2379-769X Journal of Heart Health · 2018-02-05 · unsuccessful [2]. The cardioversion procedure itself takes only a few seconds once all the preparatory setups described](https://img.dokumen.tips/doc/110x75/5f2827d06cd6042626129754/sciorschen-issn-2379-769x-journal-of-heart-health-2018-02-05-unsuccessful-2.jpg)
![Rate versus rhythm control in atrial fibrillation and ... · maintaining sinus rhythm with electrical cardioversion and/or antiarrhythmic agents) [5]. Rhythm control mainte-nance](https://img.dokumen.tips/doc/110x75/5f3fa535a6a94664fc482e5c/rate-versus-rhythm-control-in-atrial-fibrillation-and-maintaining-sinus-rhythm.jpg)


























