Embed Size (px)
Citation preview

Preconditioning ischemia time determines the degree of glycogen depletion and infarct size reduction in rat hearts
Vania Barbosa, MD, Richard E. Sievers, BS, Christian E. Zaugg, PhD, and Christopher L. Wolfe, MD
San Francisco, Calif.
The cardioprotective effect of preconditioning is associated with glycogen depletion and attenuation of intracellular ac- idosis during subsequent prolonged ischemia. This study determined the effects of increasing preconditioning is- chemia time on myocardial glycogen depletion and on infarct size reduction. In addition, this study determined whether infarct size reduction by preconditioning correlates with glycogen depletion before prolonged ischemia. Anes- thetized rats underwent a single episode of preconditioning lasting 1.25, 2,5, 5, or 10 minutes or multiple episodes cumulating in 10 (2 x 5 min) or 20 minutes (4 x 5 or 2 x 10 min) of preconditioning ischemia time, each followed by 5 minutes of reperfusion. Then both preconditioned and con- trol rats underwent 45 minutes of ischemia induced by left coronary artery (LCA) occlusion and 120 minutes of reper- fusion. After prolonged ischemia, infarct size was deter- mined by dual staining with triphenyltetrazolium chloride and phthalocyanine blue dye. Glycogen levels were deter- mined by an enzymatic assay in selected rats from each group before prolonged ischemia. We found that increasing preconditioning ischemia time resulted in glycogen deple- tion and infarct size reduction that could both be described by exponential functions. Furthermore, infarct size reduc- tion correlated with glycogen depletion before prolonged ischemia (r= 0.98; p < 0.01). These findings suggest a role for glycogen depletion in reducing ischemic injury in the preconditioned heart. (AM HEART J 1996;131:224-30.)
Brief repeated episodes of ischemia followed by rep- effusion protect the heart against subsequent pro- longed ischemia, a phenomenon first described by Murry et al. 1 and termed ischemic preconditioning.
From the Cardiovascular Research Institute and Department of Medicine (Cardiology Division), University of California, San Francisco.
Supported in part by a Grant-in-Aid from the American Heart Association (Grant 92007600). Dr. Barbosa is a recipient of an overseas scholarship from CNPq, Brazil.
Received for publication June 16, 1995; accepted July 31, 1995.
Reprint requests: Christopher L. Wolfe, MD, University of California, San Francisco, Moffitt Hospital, M-1186, 505 Parnassus Ave., San Francisco, CA 94143-0124.
Copyright © 1996 by Mosby-Year Book, Inc. 0002-8703/96/$5.00 + 0 4/1/68628
Other investigators induced ischemic precondition- ing by a variety of protocols by using multiple episodes or a single episode of coronary occlusion and reperfusion in several different species, 1"7 including human beings, s-l° Ischemic preconditioning protects the heart against myocardial necrosis by reducing infarct size 1, n and against other detrimental conse- quences of ischemia/reperfusion injuries, such as postischemic contractile dysfunction 12 and arrhyth- mias. 13-16
Proposed mechanisms for preconditioning protec- tive effects include protein kinase C activation, 17 ac- tivation of adenosine receptors, ls-2° opening of ade- nosine triphosphate (ATP)-sensitive potassium chan- nels, 21 reduced energy demand, 22 Ot 1 adrenergic receptor activation, 23 and reduction in intracellular acidosis.n, 24-26 Reduction in intracellular acidosis after ischemic preconditioning could be caused by glycogen depletion before prolonged ischemia, as suggested in a previous study from our laboratory. 11 According to this study, glycogen depletion after preconditioning may limit the degree ofintracellular acidosis during prolonged ischemia by limiting avail- ability of substrate for anaerobic glycolysis and may reduce the osmotic load on injured cells after reper- fusion by reducing lactate accumulation, n More- over, the loss of these protective effects paralleled the time course of glycogen recovery, n
Therefore this study in rat hearts in vivo was de- signed to determine the effects of increasing precon- ditioning ischemia time on myocardial glycogen de- pletion and on infarct size reduction. In addition, the study aimed to determine whether infarct size re- duction by preconditioning correlates with glycogen depletion before prolonged ischemia. For this pur- pose, rats were subjected to various protocols aimed at increasing preconditioning ischemia time by vary- ing duration and number of the ischemic precondi- tioning episodes.
224
Volume 131, Number 2 American Heart Journal Barbosa et al. 225
- - ] Ischemia
Reperfusion
4x5min F til!iiiiiiiili~iiii!!l~
2x lOmin
1 x 2.5 rain
lx5min L
1 x 10 min I
2 X 5 min I li~i~i!!~ii]iI!!iil
li!i!ililIiii! Jiiiii iiiii iiiIiii!l
Glycogen Infarct Size
Con ,o j,sr.,olii!iiiiiii
1x1.25min I lii!!!!iliiiiiiili!i!!iiii
Iiiili!ii;ltiI/iiit] IIiiiillilitI!!ll Ii!iiiiliit!iii!iiiiliiiiiil liiiiiiiliiiii#iiiiiil ltiiiiilti!iiii!ii!iiiiitili It!ii IiltiiiiilIl =
5 rain
45min i~ ~ I
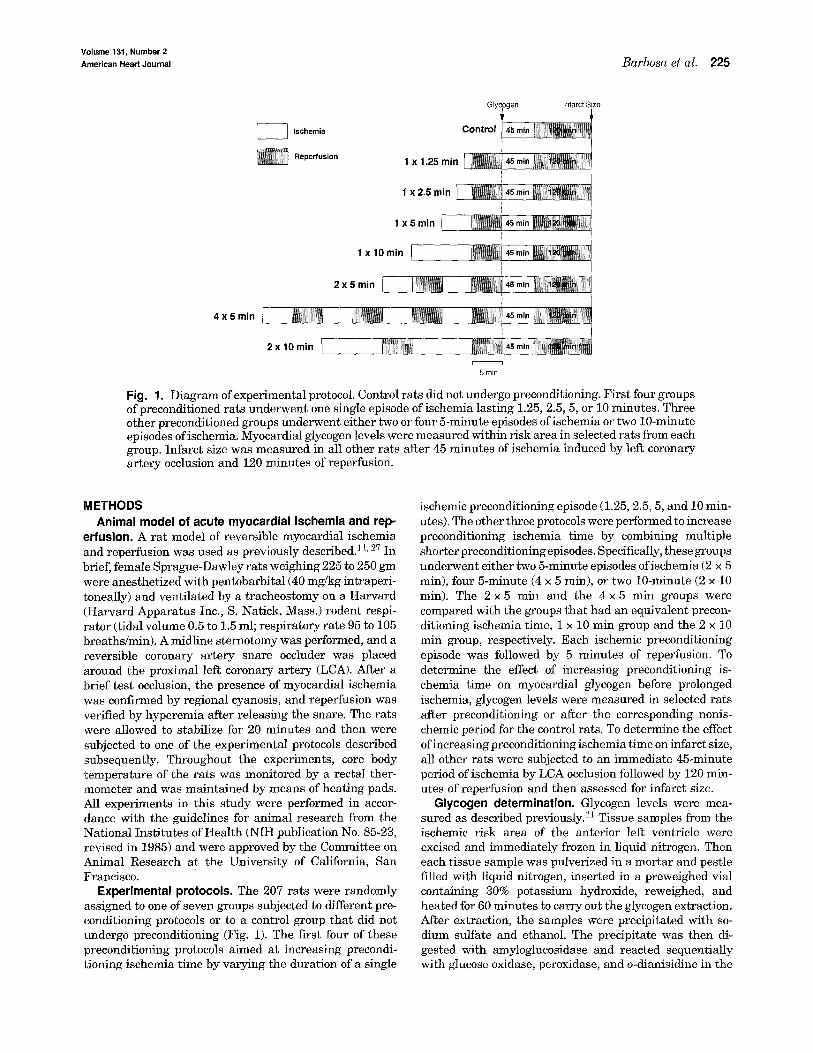
Fig. 1. Diagram of experimental protocol. Control rats did not undergo preconditioning. First four groups of preconditioned rats underwent one single episode ofischemia lasting 1.25, 2.5, 5, or 10 minutes. Three other preconditioned groups underwent either two or four 5-minute episodes ofischemia or two 10-minute episodes ofischemia. Myocardial glycogen levels were measured within risk area in selected rats from each group. Infarct size was measured in all other rats after 45 minutes of ischemia induced by left coronary artery occlusion and 120 minutes of reperfusion.
METHODS Animal model of acute myocardial ischemia and rep-
erfusion. A rat model of reversible myocardial ischemia and reperfusion was used as previously described. 11' 27 In brief, female Sprague-Dawley rats weighing 225 to 250 gm were anesthetized with pentobarbital (40 mg/kg intraperi- toneally) and ventilated by a tracheostomy on a Harvard (Harvard Apparatus Inc., S. Natick, Mass.) rodent respi- rator (tidal volume 0.5 to 1.5 ml; respiratory rate 95 to 105 breaths/min). A midline sternotomy was performed, and a reversible coronary artery snare occluder was placed around the proximal left coronary artery (LCA). After a brief test occlusion, the presence of myocardial ischemia was confirmed by regional cyanosis, and reperfusion was verified by hyperemia after releasing the snare. The rats were allowed to stabilize for 20 minutes and then were subjected to one of the experimental protocols described subsequently. Throughout the experiments, core body temperature of the rats was monitored by a rectal ther- mometer and was maintained by means of heating pads. All experiments in this study were performed in accor- dance with the guidelines for animal research from the National Institutes of Health (NIH publication No. 85-23, revised in 1985) and were approved by the Committee on Animal Research at the University of California, San Francisco.
Experimental protocols. The 207 rats were randomly assigned to one of seven groups subjected to different pre- conditioning protocols or to a control group that did not undergo preconditioning (Fig. 1). The first four of these preconditioning protocols aimed at increasing precondi- tioning ischemia time by varying the duration of a single
ischemic preconditioning episode (1.25, 2.5, 5, and 10 min- utes). The other three protocols were performed to increase preconditioning ischemia time by combining multiple shorter preconditioning episodes. Specifically, these groups underwent either two 5-minute episodes ofischemia (2 x 5 min), four 5-minute (4 x 5 rain), or two 10-minute (2 x 10 min). The 2 x 5 min and the 4 x 5 rain groups were compared with the groups that had an equivalent precon- ditioning ischemia time, 1 x 10 rain group and the 2 x 10 min group, respectively. Each ischemic preconditioning episode was followed by 5 minutes of reperfusion. To determine the effect of increasing preconditioning is- chemia time on myocardial glycogen before prolonged ischemia, glycogen levels were measured in selected rats after preconditioning or after the corresponding nonis- chemic period for the control rats. To determine the effect of increasing preconditioning ischemia time on infarct size, all other rats were subjected to an immediate 45-minute period ofischemia by LCA occlusion followed by 120 min- utes of reperfusion and then assessed for infarct size.
Glycogen determination. Glycogen levels were mea- sured as described previously. 11 Tissue samples from the ischemic risk area of the anterior left ventricle were excised and immediately frozen in liquid nitrogen. Then each tissue sample was pulverized in a mortar and pestle filled with liquid nitrogen, inserted in a preweighed vial containing 30% potassium hydroxide, reweighed, and heated for 60 minutes to carry out the glycogen extraction. After extraction, the samples were precipitated with so- dium sulfate and ethanol. The precipitate was then di- gested with amyloglucosidase and reacted sequentially with glucose oxidase, peroxidase, and o-dianisidine in the
February 1996
226 Barbosa et al. A m e r i c a n Hear t Journa l
12
8
E v
4 O U
8 • mean <> control o 1 episode of ischemia A 2 or 4 5-min epsiodes
0 o [] 2 lO-min episodes
I I I I
0 5 10 15
Preconditioning Ischemia Time (min)
[] [] I ^ l~W
I
2O
~, I00]
80
< 0 o A
v 6 0 - i | 8 8 o o
an ~ ~ O o A 0
~ 20
o oa o 8o o
I I , I I
5 10 15
Preconditioning Ischemia Time (min)
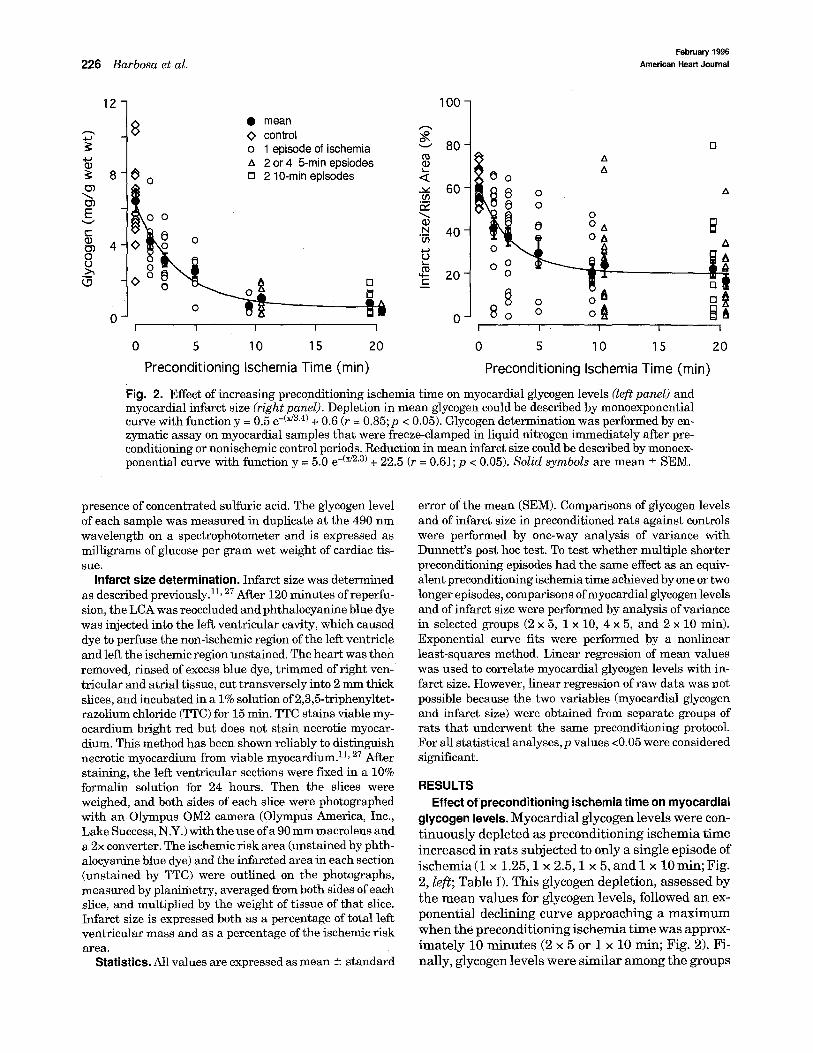
Fig. 2. Effect of increasing preconditioning ischemia time on myocardial glycogen levels (left panel) and myocardial infarct size (rightpanel). Depletion in mean glycogen could be described by monoexponential curve with function y = 0.5 e -(x/3'4) + 0 .6 ( r = 0 .85 ; p < 0 .05) . Glycogen determination was performed by en- zymatic assay on myocardial samples that were freeze-clamped in liquid nitrogen immediately after pre- conditioning or nonischemic control periods. Reduction in mean infarct size could be described by monoex- ponential curve with function y = 5.0 e -(x/2"3) + 22.5 (r = 0.61; p < 0.05). Solid symbols are mean _+ SEM.
B t~
I
2O
presence of concentrated sulfuric acid. The glycogen level of each sample was measured in duplicate at the 490 nm wavelength on a spectrophotometer and is expressed as milligrams of glucose per gram wet weight of cardiac tis- sue.
Infarct size determination. Infarct size was determined as described previously.ll, 27 After 120 minutes of reperfu- sion, the LCA was reoccluded and phthalocyanine blue dye was injected into the left ventricular cavity, which caused dye to perfuse the non-ischemic region of the left ventricle and left the ischemic region unstained. The heart was then removed, rinsed of excess blue dye, trimmed of right ven- tricular and atrial tissue, cut transversely into 2 mm thick slices, and incubated in a 1% solution of 2,3,5-triphenyltet- razolium chloride (TTC) for 15 min. TTC stains viable my- ocardium bright red but does not stain necrotic myocar- dium. This method has been shown reliably to distinguish necrotic myocardium from viable myocardium. 11, 27 After staining, the left ventricular sections were fLxed in a 10% formalin solution for 24 hours. Then the slices were weighed, and both sides of each slice were photographed with an Olympus OM2 camera (Olympus America, Inc., Lake Success, N.Y.) with the use of a 90 mm macrolens and a2x converter. The ischemic risk area (unstained by phth- alocyanine blue dye) and the infarcted area in each section (unstained by TTC) were outlined on the photographs, measured by planimetry, averaged from both sides of each slice, and multiplied by the weight of tissue of that slice. Infarct size is expressed both as a percentage of total left ventricular mass and as a percentage of the ischemic risk area.
Statistics. All values are expressed as mean _+ standard
error of the mean (SEM). Comparisons of glycogen levels and of infarct size in preconditioned rats against controls were performed by one-way analysis of variance with Dunnett's post hoc test. To test whether multiple shorter preconditioning episodes had the same effect as an equiv- alent preconditioning ischemia time achieved by one or two longer episodes, comparisons of myocardial glycogen levels and of infarct size were performed by analysis of variance in selected groups (2 x 5, 1 x 10, 4 x 5, and 2 x 10 rain). Exponential curve fits were performed by a nonlinear least-squares method. Linear regression of mean values was used to correlate myocardial glycogen levels with in- farct size. However, linear regression of raw data was not possible because the two variables (myocardial glycogen and infarct size) were obtained from separate groups of rats that underwent the same preconditioning protocol. For all statistical analyses, p values <0.05 were considered significant.
RESULTS Effect of preconditioning ischemia time on myocardial
glycogen levels. Myocardial glycogen levels were con- t inuously depleted as precondit ioning ischemia t ime increased in ra ts subjected to only a single episode of ischemia (1 x 1.25, 1 x 2.5, 1 x 5, and 1 x 10 rain; Fig. 2, left; Table I). This glycogen depletion, assessed by the m e a n values for glycogen levels, followed an ex- ponent ia l declining curve approaching a m a x i m u m when the precondit ioning ischemia t ime was approx- imate ly 10 minutes (2 x 5 or 1 x 10 min; Fig. 2). Fi- nally, glycogen levels were similar among the groups

Volume 131, Number 2
American Heart Journal Barbosa et al. 227
Table I. Effect of increasing preconditioning ischemia time on glycogen in rat hearts in vivo
N um ber of Glycogen Group hearts (mg /gm wet wt)
Control 15 6.42 _+ 0.59
1 x 1.25 min 11 4.16 _+ 0.43*
1 x 2.5 m i n 11 3.14 _+ 0.39*
1 x 5 ra in 10 2.48 _+ 0.31"
1 x 10 min 5 0.53 _+ 0.20*
2 x 5 ra in 10 0.98 _+ 0.20*
2 x 10 ra in 6 0.31 - 0.08*
4 x 5 m i n 10 0.70 _+ 0.19"
Glycogen was measured after preconditioning or nonischemic control period by enzymatic assay. Each ischemic preconditioning episode was followed by 5 minutes of reperfusion. 1 x 1.25 rain, 1 x 2.5 rnin, 1 × 5.0 re!n, and I × 10 rain, Rats that underwent a single episode of ischemic preconditioning for 1.25, 2.5, 5.0 and 10 min- utes, respectively; 2 x 5 rain and 4 x 5 rain, rats preconditioned with two or four 5-minute episodes of ischemia; 2 × 10 rain, rats preconditioned with two 10-minute episodes efischemia. Values expressed as mean -+ SEM. *p < 0.05 versus control.
that underwent 10 minutes (2 x 5 rain and 1 × 10 rain) and 20 minutes (4 × 5 min and 2 × 10 min) of preconditioning ischemia time (p = 0.123).
Effect of preconditioning ischemia time on infarct size. Similar to glycogen levels, infarct size decreased continuously as preconditioning ischemia time in- creased in rats subjected to a single episode of ischemia (Fig. 2, right panel; Table II). This reduc- tion of infarct size after preconditioning, assessed by mean values for infarct size, also followed an expo- nential declining curve, approaching a maximum when the cumulative ischemia time was approxi- mately 10 minutes. Infarct size was similar in rats subjected to multiple ischemic preconditioning epi- sodes, cumulating in 10 (2 × 5 and 1 x 10 min) and 20 minutes (4 x 5 and 2 x 10 rain) of preconditioning is- chemia time (p = 0.694). There were no significant differences in the size of the ischemic risk area between groups (Table II).
Relation between glycogen levels and infarct size. The depletion of myocardial glycogen levels and the reduction of infarct size both as functions of increas- ing preconditioning ischemia time could be described by similar exponential functions (time constants 3.4 and 2.3 minutes, respectively; Fig. 2). Moreover, there was a strong direct correlation between myo- cardial glycogen levels after preconditioning and in- farct size after prolonged ischemia in this precondi- tioning model in vivo (r = 0.98; p < 0.01; Fig. 3).
DISCUSSION
This study in rat hearts in vivo shows that in- creasing preconditioning ischemia time results in
o~ v 60
<
--~ 40 £E
N . m
O3
~ 2o
1--
, • r = 0 .98 p < 0.001
0 0
I I I I i I I
2 4 6 8
Glycogen (mg/g wet wt)
Fig. 3. Relation between myocardial glycogen (mean _+ SEM) after preconditioning and infarct size (mean _+ SEM) after prolonged ischemia in control rats and precondi- tioned rats. Because glycogen and infarct size determina- tions were made in separate groups of rats, linear regres- sion was done on means of both glycogen levels and infarct sizes, rather than on raw data. Infarct size reduction was directly correlated with depletion in myocardial glycogen levels (y = 15.97 + 6.48 x).
continuous depletion of myocardial glycogen and in continuous infarct size reduction. In addition, infarct size reduction by preconditioning correlates with glycogen depletion before prolonged ischemia.
We found that increasingpreconditioning ischemia time reduced both glycogen levels and infarct size, following similar exponential functions (with similar time constants 3.4 and 2.3 minutes, respectively; Fig. 2). Myocardial glycogen depletion after ischemic preconditioning has been shown in a previous study from our laboratory 11 and in other studies. 22,2s However, in this study, as the preconditioning is- chemia time increased, mean myocardial glycogen was depleted in an exponential fashion, becoming maximally depleted after approximately 10 minutes of preconditioning ischemia. Likewise, increasing preconditioning ischemia time resulted in an expo- nential reduction of mean infarct size after prolonged ischemia, also expressed by the mean values (Fig. 3, Table II). Thus in contrast to previous studies, 29-32 we found that preconditioning protected the myo- cardium in a continuous manner described by an ex- ponential function and not as an all-or-nothing response with a sharp time threshold.
Our finding that reduction of infarct size after is- chemic preconditioning correlated well with the de- pletion of myocardial glycogen before prolonged is- chemia (Fig. 3) provides further evidence for the hy- pothesis that glycogen depletion and reduction in

February 1996 228 Barbosa et al. American Heart Journal
Table ,. Effect of increasing preconditioning ischemia time on infarct size in rat hearts in vivo
Number of Risk area / L V mass Infarct mass /LV mass Infarct mass~risk area Group hearts (%) (%) (%)
Control 22 53.83 ± 1.41 32.16 ± 1.20 59.78 -+ 1.62 1 x 1.25 rain 18 50.43 ± 1.69 20.76 ± 2.50* 40.79 ± 4.86* 1 x 2.5 rain 20 53.85 -~ 1.53 19.66 ± 2.26* 36.75 ± 4.15" 1 x 5 min 9 48.85 ± 2.45 14.79 ± 3.97* 29.23 ± 7.11' I x 10 min 16 50.23 _+ 2.22 10.34 +_ 1.78" 20.15 ± 4.40* 2 x 5 rain 17 50.40 ± 1.74 11.50 ± 2.60* 23.78 ± 5.40* 2 x 10 man 14 50.09 _+ 2.25 10.81 ± 1.88" 22.26 ± 4.00* 4 x 5 man 13 49.29 +- 1.69 8.16 +- 6.24* 16.32 ± 3.41"
All values are expressed as mean +- SEM. Risk area was measured by absence of phthalocyanine blue staining. Infarct size was measured after prolonged ischemia and reperfusion by absence of triphenyltetrazolium staining. Each ischemic preconditioning episode was followed by 5 minutes of reperfusion. LV, Left ventricle; groups defined as in Table I. *p < 0.05 versus control.
intracellular acidosis may play a role in ischemic preconditioning, protecting the myocardium from ir- reversible ischemic injury, u In that study, hearts from rats preconditioned with four 5-minute epi- sodes of ischemia-reperfusion had greater glycogen depletion, developed less intracellular acidosis dur- ing prolonged ischemia, and had smaller infarcts af- ter reperfusion than did control hearts. Moreover, in rats that were allowed to recover after precondition- ing, the loss of these protective effects paralleled the time course of glycogen recovery and was accompa- nied by more severe intracellular acidosis, li Reduc- tion of intracellular acidosis has also been reported as an important mediator of the preconditioning cardioprotection in other studies. 24-26, 28
The relation between myocardial glycogen levels and intracellular acidosis during ischemia has been shown in early studies. 33-35 Isolated glycogen-de- pleted rat hearts developed less intracellular acido- sis than did the control hearts during ischemia, sug- gesting that the major source of protons in ischemic myocardium is the breakdown of glycogen to lac- tate 33 In addition, glycogen-depleted perfused hearts had less lactate accumulation during ischemia and greater recovery of ventricular function after reper- fusion than did control hearts. 34 Conversely, glyco- gen-loaded isolated rat hearts had increased lactate production and increased intracellular acidosis dur- ing ischemia. 35
The beneficial effects of glycogen depletion and the harmful effects of glycolytic metabolites during is- chemia and reperfusion have been reported previ- ously. Neely and Grotyohann 34 showed in isolated rat hearts that glycogen depletion by anoxic preper- fusion before ischemia resulted in less lactate accu- mulation during ischemia and in better recovery of ventricular function after reperfusion. Similarly, glycogen depletion before ischemia was also associ- ated with improve d postischemic left ventricular
functional recovery in normal and hypertrophied hearts. 36 According to these studies, 34, 36-38 the accu- mulation of glycolytic metabolites, as measured by lactate, rather than the loss of adenosine triphos- phate (ATP), plays a pivotal role in the pathogenesis of myocardial injury after ischemia and reperfusion.
Our findings also are consistent with those from other preconditioning studies, which showed deple- tion in myocardial glycogen stores after precondi- tioning. A depletion of nearly 50% of myocardial gly- cogen reserves and a significant decrease in the lac- tate accumulation during ischemia in preconditioned dog hearts has been previously reported. 2~ Similar depletion of myocardial glycogen was shown in isolated perfused rat hearts. 28
However, our findings appear to contrast with those of other investigators, who showed a cardio- protective effect of glycogen loading before ischemia. In isolated working rat hearts, glycogen loading by fasting the animals improved recovery of contractile function after global ischemia. 39 Similarly, glycogen loading by pretreatment with glucose and insulin improved left ventricular function of the rabbit heart after hypothermic ischemic arrest. 4° Conversely, glycogen depletion failed to improve left ventricular function of the rabbit heart after hypothermic is- chemic arrest. 41 The discrepancies between these findings and ours may be explained by the use of dif- ferent end points for preconditioning cardioprotec- tion (left ventricular function vs infarct size), by dif- ferent protocols of glycogen loading and depletion and by the differences in the animal models, as well as by species-dependent differences in myocardial glycogen content. 42
In spite of intensive investigation, the actual mechanism by which ischemic preconditioning de- lays irreversible ischemic injury and reduces infarct size is still unknown. It is likely that the cardiopro- tection mediated by ischemic preconditioning results

Volume 131, Number 2 American Heart Journal Barbosa et al. 2 2 9
not from a single mechanism but from an interaction between multiple mechanisms. The observation in this study that reduction of infarct size after precon- ditioning strongly correlates with myocardial glyco- gen could eventually be linked to some of the pro- posed mechanisms for preconditioning.
Because glycogen is the major substrate for anaer- obic glycolysis in the ischemic heart, 38, 43 depletion of glycogen could potentially accelerate ATP depletion and exacerbate ischemic injury. However, it has been demonstrated that, in addition to increased toler- ance to ischemia, preconditioning appears to reduce glycolytic rate and reduce high-energy phosphate u s e . 22 Therefore the reduction in energy demand af- ter preconditioning may explain why glycogen de- pletion did not have a detrimental effect on the via- bility of ischemic myocardium in our experiments. Considerable emphasis has been given to the mech- anism that ischemic preconditioning in the rabbit heart is mediated by the activation of adenosine re- ceptors.iS, 19 Furthermore, adenosine pretreatment has been reported to decrease glycolytic rates and reduce lactate accumulation during ischemia in rat hearts. 44 Nevertheless, the role of adenosine as a modulating factor of the glucose metabolism in the heart, 45-47 as well as its role in ischemic precondi- tioning in the rat model, 48 remains controversial.
In spite of the demonstrated correlation between myocardial glycogen levels and infarct size, we have not shown a cause-and-effect relation between myo- cardial glycogen depletion before prolonged ischemia and reduction of infarct size after prolonged ischemia in preconditioned hearts. However, these findings suggest that the magnitude of infarct size reduction in preconditioned rat hearts is associated with the degree of myocardial glycogen depletion before pro- longed ischemia, likely resulting in reduced lactate production, attenuation ofintracellular acidosis dur- ing prolonged ischemia, and less irreversible is- chemic injury.
In conclusion, this study in rat hearts in vivo shows that increasing preconditioning ischemia time re- stilts in continuous myocardial glycogen depletion and continuous infarct size reduction. In addition, infarct size reduction by preconditioning correlates with glycogen depletion before prolonged ischemia. Although the exact mechanism for preconditioning cardioprotection remains to be determined, these data suggest a role for glycogen depletion in reduc- ing ischemic injury in the preconditioned heart.
We t h a n k M a r k S inger a n d S teven D. Rosen for t he i r advice in pe r fo rming the glycogen assay ; Kev in Cla rk for he lp wi th com- p u t e r p rograming ; a n d M i mi Zeiger for a s s i s t ance wi th t he m a n u s c r i p t .
REFERENCES
1. Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation 1986;74:1124-36.
2. Li GC, Vasquez JA, Gallagher KP, Lucchesi BR. Myocardial protection with preconditioning. Circulation 1990;82:609-19.
3. Thornton J, Striplin S, Liu GS, Swafford A, Stanley AW, Van Winkle DM, Downey JM. Inhibition of protein synthesis does not block myocardial protection afforded by preconditioning. Am J Physiol 1990;259:H1822-5.
4. Minra T, Gore M, Urabe K, Endoh A, Shimamoto K, Iimura O. Does myocardial stunning contribute to infarct size limitation by ischemic preconditioning? Circulation 1991;84:2504-12.
5. Schott l~J, Rohmann S, Braun ER, Schaper W. Ischemic precondition- ing reduces infarct size in swine myocardium. Circ Res 1990;66:1133- 42.
6. Li YW, Whittaker P, Kloner RA. The transient nature of the effect of ischemic preconditioning on myocardial infarct size and ventricular arrhythmia. AM HEART J 1992;123:346-53.
7. Liu Y, Downey JM. Ischemic preconditioning protects against infarc- tion in rat heart. Am J Physiol 1992;263:Hl107-12.
8. Deutsch E, Berger M, Kussmaul WG, Hirshfeld J Jr, Herrmarm HC, Laskey WK. Adaptation to ischemia during percutaneous transluminal coronary angioplasty. Clinical, hemodynamic, and metabolic features [Comments]. Circulation 1990;82:2044-51.
9. Yellon DM, All~hulaifi AM, Pugsley WB. Preconditioning the human myocardium. Lancet 1993;342:276-7.
10. Tomai F, Crea F, Gaspardone A, Versaci F, De Patflis R, Penta de Peppo A, Chiariello L, Gioffre PA. Iscbemic preconditioning during coronary angioplasty is prevented by glibenclamide, a selective ATP-sensitive K + channel blocker. Circulation 1994;90:700-5.
11, Wolfe CL, Sievers RE, Visseren FL, Donnelly TJ. Loss of myocardial protection after preconditioning correlates with the time course of gly- cogen recovery within the preconditioned segment. Circulation 1993; 87:881-92.
12. Cohen MV, Lin GS, Downey JM. Preconditioning causes improved wall motion as well as smaller infarcts after transient coronary occlusion in rabbits. Circulation 1991;84:341-9.
13. Vegh A, Szekeres L, Parratt JR. Protective effects of preconditioning of the isehaemic myocardium involve cyclo-oxygenase products. Cardio- vasc Res 1990;24:1020-3.
14. Shiki K, Hearse DJ. Preconditioning ofischemic myocardium: reperfu- siominduced arrhythmias. Am J Physiol 1987;253:H1470-6.
15. Hagar JM, Hale SL, Kloner RA. Effect of preconditioning ischemia on reperfusion arrhythmias after coronary artery occlusion and reperfu- sion in the rat. Cire Res 1991;68:61-8.
16. Osada M, Sate T, Komori S, Tamura K. Protective effect of precondi- tioning on reperfusion induced ventricular arrhythmias of isolated rat hearts. Cardiovasc Res 1991;25:441-4.
17. Ytrehus K, Lin Y, Downey JM. Preconditioning protects ischemic rab- bit heart by protein kinase C activation. Am J Physio11994;266:Hl145- 52.
18. Liu GS, Thornton J, Van Wilflde DM, Stanley AW, Olsson RA, Downey JM. Protection against infarction afforded by preconditioning is medi- ated by AI adenosine receptors in rabbit heart. Circulation 1991; 84:350-6.
19. Thornton JD, Liu GS, Olsson RA, Downey JM. Intravenous pretreat- ment with Al-selective adenosine analogues protects the heart against infarction [Comments]. Circulation 1992;85:659-65.
20. Armstrong S, Ganote CE. Adenosine receptor specificity in precondi- tioning of isolated rabbit cardiomyecytes: evidence of -43 receptor involvement. Cardiovasc Res 1994;28:1049-56.
21. Gross GJ, Auchampach JA. Blockade of ATP-sensitive potassium channels prevents myocardial preconditioning in dogs. Circ Res 1992; 70:223-33.
22. Murry CE, Richard V J, Reimer KA, Jennings RB. Ischemic precondi- tioning slows energy metabolism and delays ultrastructural damage during a sustained ischemic episode. Circ Res 1990;66:913-31.
23. Banerjee A, Locke-Winter C, Rogers KB, Mitchell MB, Brew EC, Cairns CB, Bensard DD, Harken AH. Preconditioning against myocardial dysfunction after ischemia and reperfnsion by an alpha l-adrenergic mechanism. Circ Res 1993;73:656-70.
24. Kida M, Fujiwara H, Ishida M, Kawai C, Ohura M, Miura I, Yabuuchi

February 1996 2 3 0 Barbosa et al. American Heart Journal
Y. Ischemic preconditioning preserves creatine phosphate and intra- cellular pH. Circulation 1991;84:2495-503.
25. Steenbergen C, Perlman ME, London RE, Murphy E. Mechanism of preconditioning. Ionic alterations. Circ Res 1993;72:112-25.
26. Albuquerque CP, Gestenb]ith G, Weiss RG. Importance of metabolic inhibition and cellular pH in mediating preconditioning contractile and metabolic effects in rat hearts. Circ Res 1994;74:139-50.
27. Hutter MM, Sievers RE, Barbosa V, Wolfe CL. Heat-shock protein in- duction in rat hearts. A direct correlation between the amount of heat- shock protein induced and the degree of myocardial protection. Circu- lation 1994;89:355-60.
28. Asimakis GK, Inners-McBride K, Medellin G, Conti VR. Ischemic pre- conditioning attenuates acidosis and postischemic dysfunction in iso- lated rat heart. Am J Physiol 1992;263:H887-94.
29. Van Winkle DM, Thornton JD, Downey DM, Downey JM. The natural history of preconditioning: cardioprotection depends on duration of transient ischemia and time to subsequent ischemia. Coronary Artery Dis 1991;2:613-9.
30. Walker DM, Yellon DM. Ischaemic preconditioning: from mechanisms to exploitation. Cardiovasc Res 1992;26:734-9.
31. Miara T, Limura O: Infarct size limitation by preconditioning: its phe- nomenological features and the key role of adenosine. Cardiovasc Res 1993;27:36-42.
32. Downey JM. Ischemic preconditioning nature's own cardioprotective intervention. Trends Cardiovasc Med 1992;2:170-6.
33. Garlick PB, Radda GK~ Seeley PJ. Studies of acidosis in the ischaemic heart by phosphorus nuclear magnetic resonance. Biochem J 1979; 184:547-54.
34. Neely JR, Grotyohann LW. Role of glycolytic products in damage to is- chemic myocardium. Dissociation of adenosine triphosphate levels and recovery of function ofreperfusedischemic hearts. CircRes 1984;55:816- 24.
35. Bailey IA, Radda GK, Seymour AM, Williams SR. The effects of insu- lin on myocardial metabolism and acidosis in normoxia and ischaemia. A ~IP-NMR study. Biochim Biophys Acta 1982;720:17-27.
36. Allard MF, Kamimura CT, English DR, Henning SL. Preischemic gly- cogen reduction or glycolytic inhibition improves pestischemic recovery of hypertrophied rat hearts. Am J Physiol 1994;267:H66-74.
43.
44.
45.
- 37. Rovetto MJ, Lamberton WF, Neely JR. Mechanisms of glycolytic inhi- bition in ischemic rat hearts. Circ Res 1975;37:742-5L
38. Kupriyanov W , Lakomkin VL, Steinschneider A, Severina M, Kapelko VI, Ruuge EK, Saks VA. Relationships between pre-ischemic ATP and glycogen content and post-ischemic recovery of rat heart. J Mol Cell Cardiol 1988;20:1151-62.
39. Schneider CA, Taegtmeyer H. Fasting in vivo delays myocardial cell damage after brief periods ofischemia in the isolated working rat heart. Circ Res 1991;68:1045-50.
40. McElroy DD, Walker EW, Taegtmeyer H. Glycogen loading improves left ventricular function of the rabbit heart after hypothermic ischemic arrest. J Appl Cardiol 1989;4:455-65.
41. Largestrom FC, Walker EW, Taegtmeyer H. Failure of glycogen deple- tion to improve left ventricular function of the rabbit heart after hypo- thermic ischemSc arrest. Circ Res 1988;63:81-6.
42. van der Vasse GJ, Renemann RS. Glycogen and lipids (endogenous substrates). In: Drake-Holland AJ, Noble MIM, eds. Cardiac metabo- lism. Chichester: John Wiley, 1983:218-9. Wollenberger A, Krause EG. Metabolic control characteristics of the acutely ischemic myocardium. Am J Cardiol 1968;22:349~59. Finegan BA, Lopaschuk GD, Coulson CS, Clanachan AS. Adenosine alters glucose use during ischemia and reperfusion in isolated rat hearts. Circulation 1993;87:900-8. Dale WE, Hale CC, Kim HD, Rovetto MJ. Myocardial glucose utiliza- tion. Failure of adenosine to alter it and inhibition by the adenosine analogue N6-(L-2-phenylisopropyl)adenosine. Circ Res 1991;69:791-9.
46. Wyatt DA, Edmunds MC, Rubio R, Berne RM, Lasley RD, Mentzer R Jr. Adenosine stimulates glycolytic flux in isolated perfused rat hearts by Al-adenosine receptors. Am J Physiol 1989;257:H1952-7.
47. Lasley RD, Mentzer R Jr. Adenosine increases lactate release and de- lays onset of contracture during global low flow ischaemia. Cardiovasc Res 1993;27:96-101.
48. Li Y, Kloner RA. The cardioprotective effects of ischemic "precondi- tioning" are not mediated by adenosine receptors in rat hearts. Circu- lation 1993;87:1642-8.
![AMPK Signaling Pathway - Ozyme · Sterol/Isoprenoid Synthesis Fatty Acid Oxidation Lipolysis Glycolysis Glycogen Synthesis [cAMP] Low Glucose, Hypoxia, Ischemia, Heat Shock AICAR](https://img.dokumen.tips/doc/110x75/5cabd8f388c99319398dfb0b/ampk-signaling-pathway-ozyme-sterolisoprenoid-synthesis-fatty-acid-oxidation.jpg)