Embed Size (px)
Citation preview

Pre-competitive projects can work to deliver science and change culture

• Established 2003
• 200 scientists; labs in Toronto, Oxford and Stockholm
• Funded by - Private: GSK, Merck, Novartis, Lilly, Pfizer, Life
Tech- Govt: Canada, Ontario, Sweden - Charities: Wellcome Trust, Wallenberg Foundation
The SGC: A model for sharing in experimental science

SGC: open access works• 1000 human protein structures – all available without
restriction– ~30% of novel human proteins in PDB per annum– Structures used to be “competitive”
• >100 structures of proteins from parasitic protozoa– Chemical validation for drug targets in toxoplasmosis (Nature,
2010) and sleeping sickness (Nature, 2010)
• 500 cDNA clones distributed freely every year (academia, biotech, pharma)
• 75 visiting scientists per annum

Why does the SGC model work?
• SGC model allows opportunity to work with the very best – 200+ collaborations
• SGC model drives fast data dissemination– On average, each SGC structure enters public domain 18-24
months in advance of academic norms
• SGC model promotes collaboration– Average of >3 non-SGC authors for each paper
• SGC model focuses on milestones– 1000 structure target (2004-2011); 1,100 achieved to date
• No IP

In biomedicine, the system is the greatest hurdle to the discovery of innovative medicines

The funding system does not support “innovation”

HUMAN PROTEIN KINASES (ordered by most citations 1950-2002)
CITA
TIO
NS
(nor
mal
ized
)
Citations as a function of time
1950-2002
2003-2008
2009
How have we responded to the genome?
Another way of looking at it
• 65% of 2009 kinase publications on the 10% of the kinome that was “hot” in early 1990’s
• 5% of 2009 kinase publications on the 300 kinases that were the least studied in 2002

Others also feel trapped by the system

What should the scientific community do?
1. Pay less attention to the literature2. Be more daring when funding research3. Support young scientists to dream bigger

NUCLEAR HORMONE RECEPTOR
CITA
TIO
NS
Another path emerges from examining the history of nuclear hormone receptor research (1950-2010)
ERa PR
PPARgRARa
MR
PXRLX
Ra
PPARdCAR
NGFIBa
RARgTR
aDAX
SHP
ERRa
RORg
Rev-erb
a
NGFIBg
RXRgTR
2ER
RbTR
4TL
X
COUP30
5000
10000
15000
20000
25000
30000
35000

CITA
TIO
NS
ERa
PPARa PRRARa
MR
LXRa
PPARdTR
bRORg
ERb
HNF4a
SHP
SF1
Rev-erb
a
COUP2TR
aLR
H1
NGFIBg
RXRaRXRg
ERRb
GCNFTR
2
COUP30
500
1000
1500
2000
2500
3000
NUCLEAR HORMONE RECEPTOR
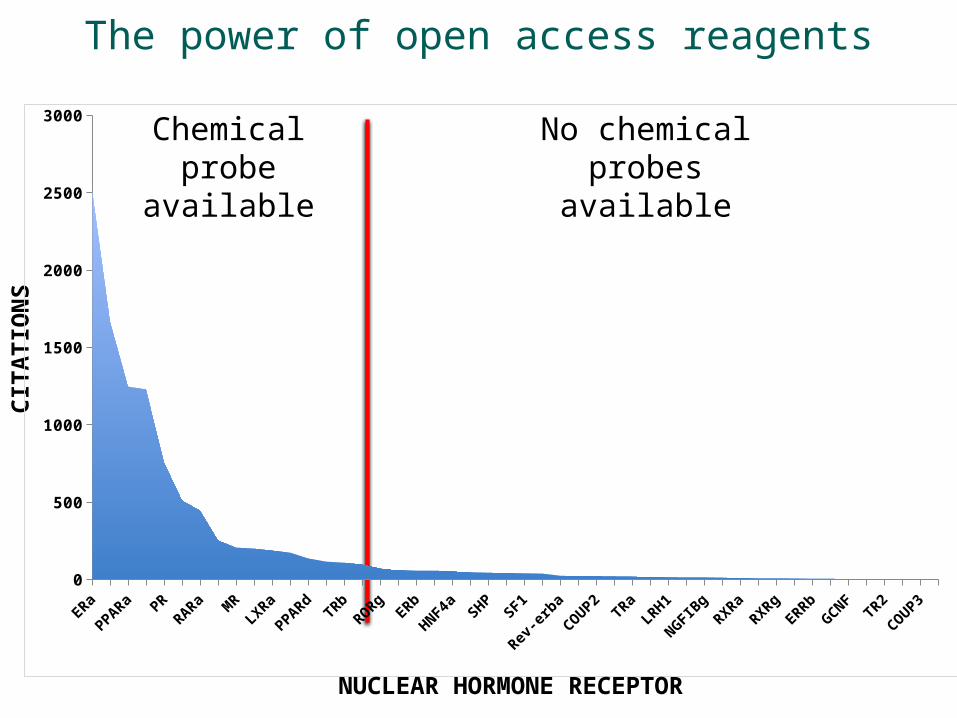
In 2009, the research is even more biased

Pre- and post-genome NR citations
1950-1995
2009
0
1000
2000
3000
4000
5000
6000
7000
**** *
**
*
CITA
TIO
NS
Chemical probe available
ERa
PPARa PRRARa
MR
LXRa
PPARdTR
bRORg
ERb
HNF4a
SHP
SF1
Rev-erb
a
COUP2TR
aLR
H1
NGFIBg
RXRaRXRg
ERRb
GCNFTR
2
COUP30
500
1000
1500
2000
2500
3000
NUCLEAR HORMONE RECEPTOR
The power of open access reagents
No chemical probes available

Can we be proactive?Epigenetics – a pioneer area of science and medicine
Number of Citations
Fam
ily m
embe
r

CloningExpression
& Purification
Crystallography
The SGC: Delivered(ing) on its core mandate
Construct Design
Wellcome Trust
Sweden
CanadaOntario
GSKNovartisMerck
• >2000 purified human proteins
• >1000 human crystal structures

CloningExpression
& Purification
Crystallography
Pushing the pre-competitive boundary
Construct Design
Wellcome Trust
Sweden
CanadaOntario
GSKNovartisMerck
• >2000 purified human proteins
• >1000 human crystal structures
Medicinal Chemistry
Oxford:SGCChemistryBiochemistry
Toronto SGCUNC CICBDD
OICR
More than 50 universitiies
GSKPfizerLillyNovartis
• Epigenetics Chemical Probes Consortium
• Pre-competitive tools for new drug target validation

IndustryPublicDomain
Public/PrivatePartnership
ChemicalProbes
ScreeningChemistryStructureBioavailability
TargetValidation
No IPNo restrictionsPublication
DrugDiscovery
(re)ScreeningChemistryLead optimizationPharmacologyDMPKToxicologyChemical developmentClinical development
Our Model for Pre-Competitive Chemistry
Creative commons Proprietary

Jan 09
Well. Trust (£4.1M)NCGC (20HTSs)
GSK (8FTEs)
Ontario ($5.0M)
OICR(2FTEs)
UNC(3FTEs)
April 09
June 09July 11
Lilly, Pfizer
(8FTEs)
Epigenetics Chemical Probes ConsortiumAccessing expertise, assays and resource quickly
Sweden ($3.0M)
15 acad. labs
….more than $50M of resource
Novartis(8FTEs)

It’s working. The BET probe
797 403
0
20
40
60
80
100
Vehicle JQ1 Vehicle JQ1
Ki6
7 P
osi
tive
( %
)
250+ labsacross the globe
IdentifiedJan 10
PublishedSep 10
DistributedJan 11

Take home message:
SGC and its pharma partners have moved the pre-competitive boundary to medicinal chemistry

SGC OxfordSGC Toronto SGC Stockholm
How is this linked to the development of new medicines?
Structural Genomics Consortium

The Challenge of Pioneer Drug Discovery
• Number of pioneer drugs (Priority Reviewed NCEs) has not increased from 1993-2008
• Investment in pharmaceutical R&D has risen dramatically over this period
• >90% failure rate in clinical trials for pioneer drugs due to lack of efficacy
19931994
19951996
19971998
19992000
20012002
20032004
20052006
20072008
13121018
91619
97 7 9
1713
6 77 0
20
40
60
80
100
120
Yearly FDA Approvals
New Drug ApprovalsNew Chemical EntitiesPriority Reviewed NCEs
Public Data from Center of Drug Evaluation and Research: www.fda.gov/cder/

Impact on pharma and biotech in 2009
• $100B in R&D
• 21 drugs approved (7 truly novel)
• 70,000 pharma employees let go
• Investment houses writing that pharma should “get out of R&D”
• Industry relying on academia for “innovation”

How industry acceses “innovation”

What’s the “innovative” drug discovery process?
Target ID/
Discovery
Hit/ Probe/ Lead
ID
Clinical candidate
ID
Toxicology/ Pharmacy
Phase I
Phase IIa/ b
HTS LO
10% 30% 30% 90+%50%
Hypothesis generated
And tested
Failure rates

And here is how industry currently works
Target ID/
Discovery
Hit/ Probe/ Lead
ID
Clinical candidate
ID
Toxicology/ Pharmacy
Phase I
Phase IIa/ b
HTS
30% 30% 90+%
Target ID/
Discovery
Hit/ Probe/ Lead
ID
Clinical candidate
ID
Toxicology/ Pharmacy
Phase I
Phase IIa/ b
30% 30% 90+%
Target ID/
Discovery
Hit/ Probe/ Lead
ID
Clinical candidate
ID
Toxicology/ Pharmacy
Phase I
Phase IIa/ b
30% 30% 90+%
Target ID/
Discovery
Hit/ Probe/ Lead
ID
Clinical candidate
ID
Toxicology/ Pharmacy
Phase I
Phase IIa/ b
30% 30% 90+%
Target ID/
Discovery
Hit/ Probe/ Lead
ID
Clinical candidate
ID
Toxicology/ Pharmacy
Phase I
Phase IIa/ b
30% 30% 90+%
Target ID/
Discovery
Hit/ Probe/ Lead
ID
Clinical candidate
ID
Toxicology/ Pharmacy
Phase I
Phase IIa/ b
30% 30% 90+%
Target ID/
Discovery
Hit/ Probe/ Lead
ID
Clinical candidate
ID
Toxicology/ Pharmacy
Phase I
Phase IIa/ b
10% 30% 30% 90+%50%
LO

One example of the real worldTotal number of patents on TRPV1
Source: Derwent World Patent Index

Aurora Kinase Inhibitors
AT9283 PF03814735 AS703569 AMG-900 KW-2449 CYC116 AZD-1152 MLN-8054 MLN-8237 VX-667 PHA-739358 SU-6668 VX-680 SNS-314 ENMD-981693
Preclinical Phase I Phase II
• Antimitotic kinase – potential treatment for numerous cancer types
• Will also affect healthy proliferating cells – risk of low TI
• >60 separate organizations have pre-clinical programs with patents
• 11 compounds in Phase I
• Further 4 compounds in Phase II
• Estimated total expenditure >£200M
• No data available on outcomes of clinical studies, apart from rumours
>60
11
4

SGC OxfordSGC Toronto SGC Stockholm
What can we do?
Structural Genomics Consortium

Why not change the system?

Let’s imagine….
• A steady stream of pioneer targets whose links to disease have been validated in humans
• Engagement of top scientists and clinicians• A process in which regulators can fully collaborate to solve
key scientific problems• An engaged citizenry that promotes science and
acknowledges risk• Mechanisms to avoid bureaucratic and administrative
barriers• Sharing of knowledge to more rapidly achieve
understanding of human biology

Imagine…
• Pooled public and private sector funding into independent organization• Public sector provides stability and new ideas• Private sector brings focus and experience• Funding can focus explicitly on high-risk targets
• A pre-competitive model to test hypotheses• Disassociates science from financial gain• Will attract top scientists and clinicians• Will allow regulators to participate as scientists• Will reduce perceived conflicts of interests – engages citizens/patients• Will reduce bureaucratic and administrative overhead• Will allow rapid dissemination of information without restriction -
informs public and private sectors and reduces duplication

Progress
• arch2POCM concept• University of Toronto, University of Oxford, University of
California, San Francisco committed• CIHR and Genome Canada helping drive• Six large pharma engaged (none committed yet!)• Regulators (FDA) keen to be involved as participants• Patient groups fully engaged• Therapeutic foci selected
• Oncology, neuroscience and inflammation
• Business plan being written

What is needed
• A set of public funders keen to take the “risk” and drive the concept (Canada???)
• Leadership identified
• A core set of pharmaceutical funders

And when we succeed?• Less duplication• Broader scientific assessment• Faster dissemination of data• Pool academic and multiple pharma strengths and
funding – shared risk• Increasing knowledge of human biology (which will in
turn reduce attrition?)
More clinical POCs on novel targets….more clinically validated targets …..more novel drugs
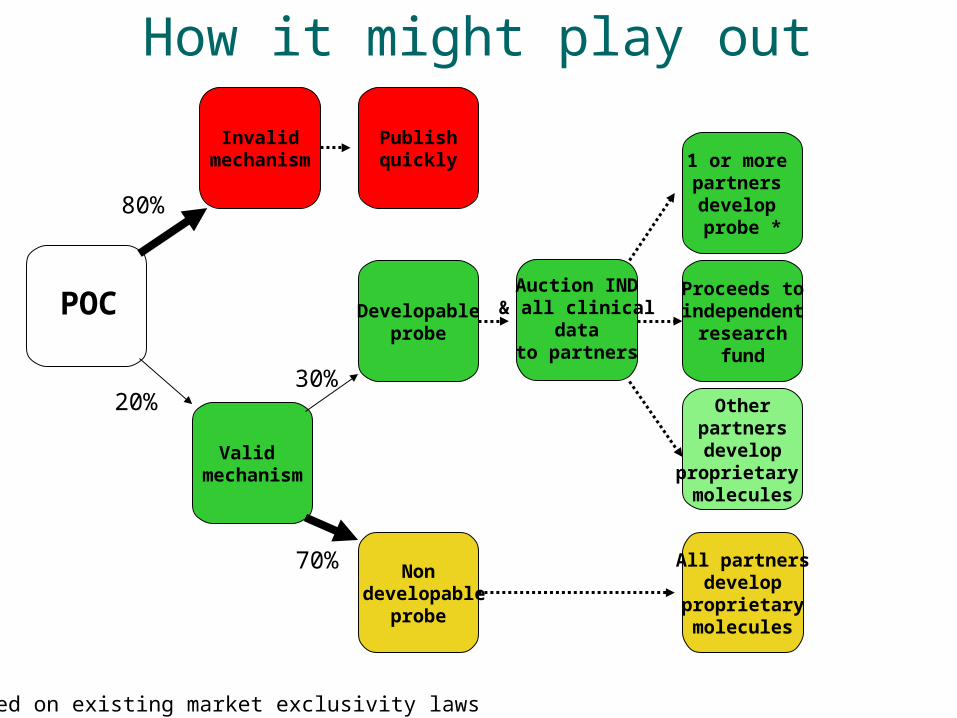
How it might play out
1 or more partners develop probe *
Non developable
probe
Developableprobe
Otherpartnersdevelop
proprietary molecules
All partnersdevelop
proprietarymolecules
Invalidmechanism
Publishquickly
Proceeds toindependent
researchfund
Valid mechanism
POCAuction IND & all clinical
datato partners
80%
20%30%
70%
*Based on existing market exclusivity laws

Market size: ~$20B up for grabs
Potential opportunities for research and business
1. Academic partnerships that deliver new targets2. High value clinical trials3. Contract research organizations with leading edge science4. Biotech companies with compounds and technologies
Potential impact
5. More industry funding for University and Hospital-based research6. A business community built on high value service7. A clinical trial network that works on innovative targets8. Better business climate for biotech due to enhanced links with industry
Commercial opportunities for Canada in the new “open access” drug discovery ecosystem





























