Embed Size (px)
Citation preview

Gene Mediated Cytotoxic Immunotherapy (GMCI™)
dvantagene Jefferies 2015 Healthcare Conference
Estuardo Aguilar-Cordova
Chief Executive Officer
June 4, 2015
2 Gene Mediated Cytotoxic Immunotherapy
dvantagene
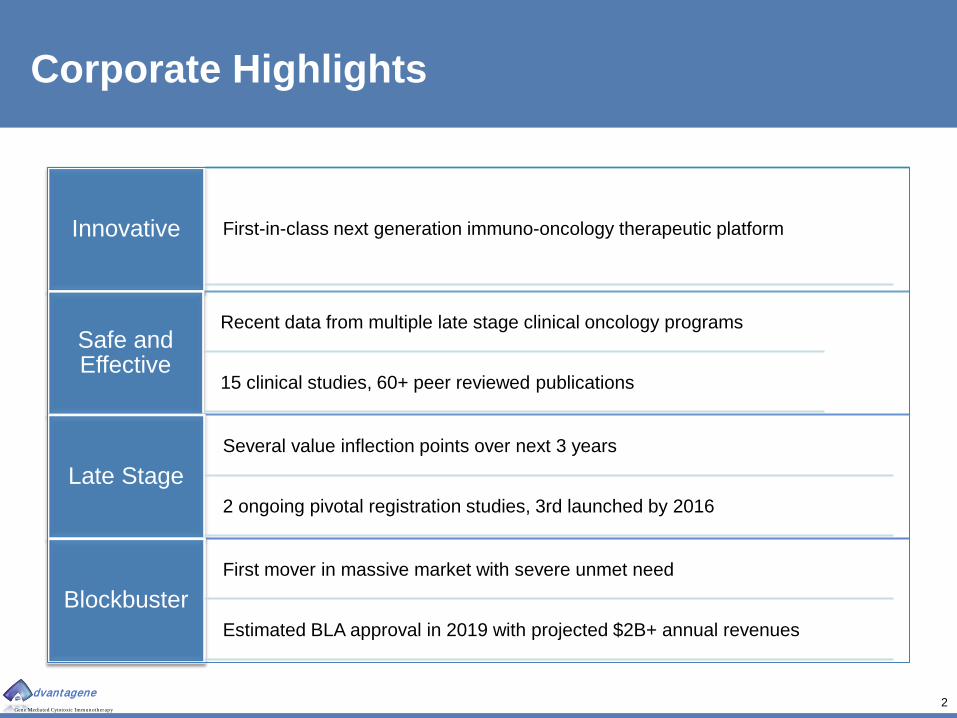
Corporate Highlights
Innovative First-in-class next generation immuno-oncology therapeutic platform
Safe and Effective
Recent data from multiple late stage clinical oncology programs
15 clinical studies, 60+ peer reviewed publications
Late Stage Several value inflection points over next 3 years
2 ongoing pivotal registration studies, 3rd launched by 2016
Blockbuster First mover in massive market with severe unmet need
Estimated BLA approval in 2019 with projected $2B+ annual revenues

3 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Key Clinical Investigators and Advisors Peter T. Scardino MD Chair, Department of Surgery Memorial Sloan Kettering Theodore L. DeWeese, MD Chair, Department of Radiation Oncology Johns Hopkins Medical Institutions E. Antonio Chiocca, MD PhD Chair, Department of Neurosurgery Brigham and Women’s Hospital Mark Bloomston, MD Medical Director, GI Cancer Service Ohio State University Tanios Bekaii-Saab, MD Section Chief , Gastrointestinal Oncology The Ohio State University Steven M. Albelda, MD Associate Chief, Pulmonary, and Critical Care Director, Thoracic Oncology Research Laboratory University of Pennsylvania Daniel H. Sterman, MD Director, Pulmonary, Critical Care, and Sleep Medicine New York University
Advantagene Leadership and Advisors Key Management Estuardo Aguilar-Cordova,MDinf,PhD Chief Executive Officer and Chairman Harvard University, Baylor College of Medicine, Cetus FDA: BRMAC, VRPAC, NIH:RAC Laura Aguilar, MD, PhD Chief Medical Officer Harvard University, Baylor College of Medicine Stephen Rocamboli, JD, CLP Chief Business Officer Fordham Law, Orion Biomedical Fund, WRY&P, Paramount Brian Guzik, PhD, MBA Director, Business Development University of Virginia, UCSD/HHMI, Cornell Capital Partners
Board of Directors Mitchell Finer, PhD CSO bluebird bio; Founder Avalanche Biotechnologies; (Novocell; Gencell; Abgenix; Cell Genesys) Fred Mermelstein, PhD Partner, Leviathan Biopharma (Javelin, PolaRx, Cardiome, Paramount Capital) Udi Merav, PhD CEO enVerid Systems (Luminus Devices; Cliniworks; Stata Venture Partners, Strategic Decisions Group) Normand F. Smith, JD Partner, Burns and Levinson
4 Gene Mediated Cytotoxic Immunotherapy
dvantagene
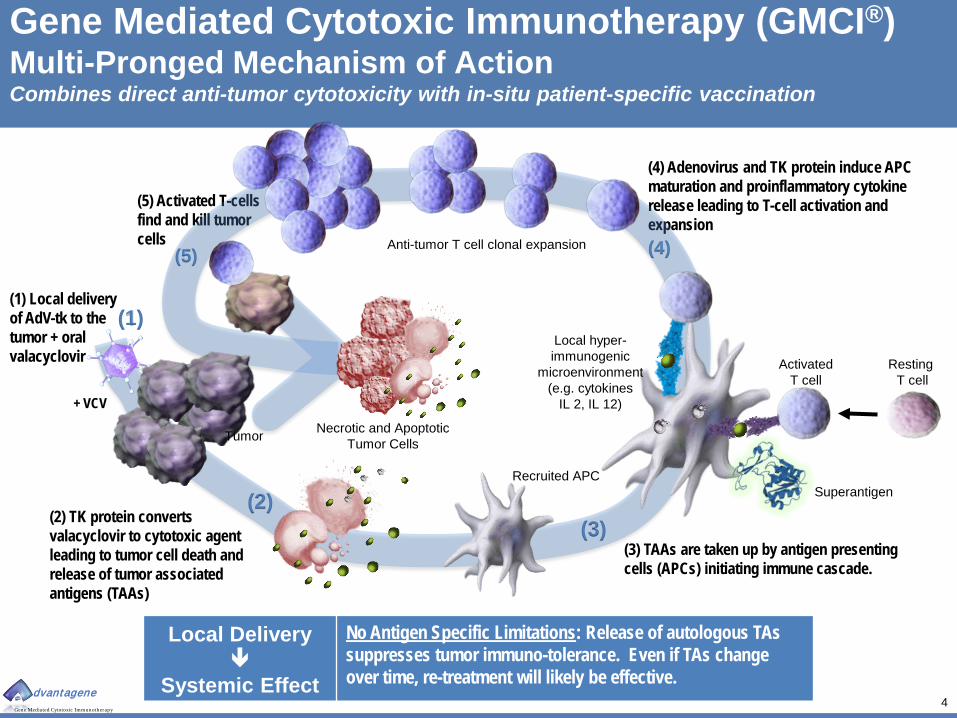
(5) Activated T-cells find and kill tumor cells
(4) Adenovirus and TK protein induce APC maturation and proinflammatory cytokine release leading to T-cell activation and expansion
(3) TAAs are taken up by antigen presenting cells (APCs) initiating immune cascade.
(1) Local delivery of AdV-tk to the tumor + oral valacyclovir
(2) TK protein converts valacyclovir to cytotoxic agent leading to tumor cell death and release of tumor associated antigens (TAAs)
Gene Mediated Cytotoxic Immunotherapy (GMCI®) Multi-Pronged Mechanism of Action Combines direct anti-tumor cytotoxicity with in-situ patient-specific vaccination
Recruited APC
Resting T cell
(2)
(4)
(1)
+ VCV
(3)
Tumor
Local Delivery
Systemic Effect
No Antigen Specific Limitations: Release of autologous TAs suppresses tumor immuno-tolerance. Even if TAs change over time, re-treatment will likely be effective.
Local hyper-immunogenic
microenvironment (e.g. cytokines
IL 2, IL 12)
Anti-tumor T cell clonal expansion (5)
Activated T cell
Necrotic and Apoptotic Tumor Cells
Superantigen

5 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Evidence of Single Agent Activity in Humans Cytotoxicity immune response in multiple tumor types and studies
0.02.04.06.08.0
10.012.014.0
-100 0 100 200 300 400
Tota
l PSA
Day of Treatment
Patient: 11-1
Clinical response Tumor shrinkage by CT scan (mesothelioma, brain) PET response (mesothelioma) Despite limited distribution, long-term effects consistent
with immune mechanism
Cytopathic / Immune effects Widespread necrosis and apoptosis (prostate, brain) Decreased vascularity (prostate, brain) Loss of glandular architecture (prostate) Widespread immune-cell infiltrate
Biochemical markers PSA response Increased PSA doubling time (PSADT) CEA reduction (ovarian) (not shown)
Pre-Rx 2 months post Rx
Vasculitis in Glioma Necrosis in Pre-Prostatectomy
Lymphocytic Infiltrate
17%
70%
0%10%20%30%40%50%60%70%80%
Partial Response Stable Disease
% o
f Pat
ient
s
Biochemical Response
Monotherapy, single dose in 18 XRT failure prostate cancer
patients
Rapid Response and Persistent effects consistent with immune
mechanism
Limited Transduction

6 Gene Mediated Cytotoxic Immunotherapy
dvantagene
0
20
40
60
80
100
120
140
CD4+ Pre-Tx CD4+ Post-Tx
CD8+ Pre-Tx CD8+ Post-Tx
1A03
2A02
3A01
3A02
3A03
4A01
4A02
Case Number
Clinical Immune Stimulation & Checkpoint Response PaTK01 patient samples
21.4 Fold Average Increase 1.3 Fold Average Increase
Pre AdV-tk Post AdV-tk
CD8+ T-cells CD4+ T-cells
Cells
Per
Hig
h-Po
wer
ed F
ield
Quantification of Cellular Infiltrate
Pre AdV-tk Post AdV-tk Pre AdV-tk Post AdV-tk
PD-L1+ Tumor Cells
General Up-regulation
Cellular Staining

7 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Cancer Immunotherapy Desirable Characteristics GMCI® fulfillment
Characteristic Rationale GMCI®
“off the shelf” • More accessible than autologous “ex-vivo” therapies • Dramatically lower COGS • Long shelf life
Target multiple antigens
• Single antigen products have limited utility • Low immune-escape rates
Autologous • Patient specific response Non-replicating
• Negligible antigen masking concerns • No “shedding” issues • Low handling, administration and disposal costs
Low Toxicity • Ability to target early stage, low symptomatic disease • Ability to use in combination therapy
8 Gene Mediated Cytotoxic Immunotherapy
dvantagene
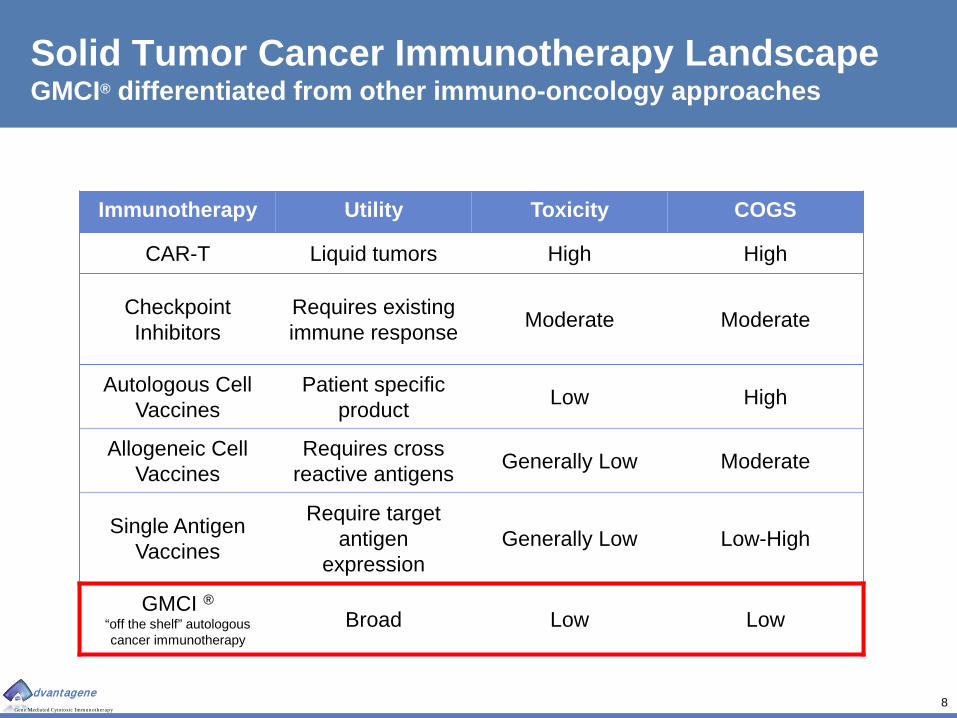
Solid Tumor Cancer Immunotherapy Landscape GMCI® differentiated from other immuno-oncology approaches
Immunotherapy Utility Toxicity COGS
CAR-T Liquid tumors High High
Checkpoint Inhibitors
Requires existing immune response Moderate Moderate
Autologous Cell Vaccines
Patient specific product Low High
Allogeneic Cell Vaccines
Requires cross reactive antigens Generally Low Moderate
Single Antigen Vaccines
Require target antigen
expression Generally Low Low-High
GMCI ® “off the shelf” autologous cancer immunotherapy
Broad Low Low
9 Gene Mediated Cytotoxic Immunotherapy
dvantagene
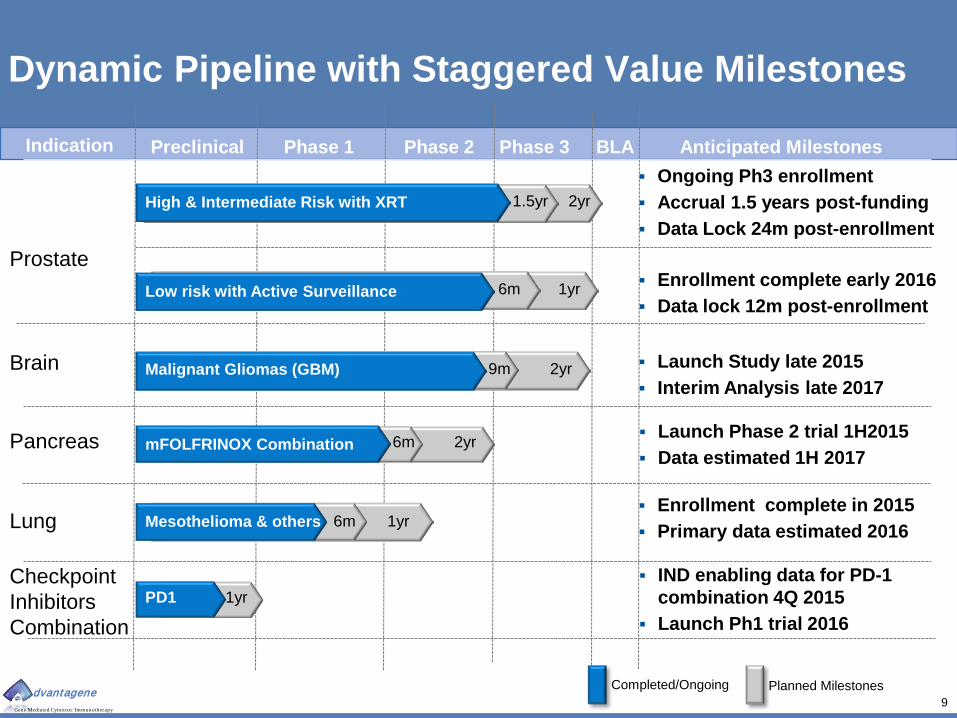
Dynamic Pipeline with Staggered Value Milestones
Preclinical Phase 1 Phase 2 Indication Anticipated Milestones
High & Intermediate Risk with XRT
Low risk with Active Surveillance
mFOLFRINOX Combination
Mesothelioma & others
PD1
Malignant Gliomas (GBM)
Phase 3
Completed/Ongoing
Ongoing Ph3 enrollment Accrual 1.5 years post-funding Data Lock 24m post-enrollment
Launch Phase 2 trial 1H2015 Data estimated 1H 2017
Enrollment complete in 2015 Primary data estimated 2016
IND enabling data for PD-1 combination 4Q 2015
Launch Ph1 trial 2016
Launch Study late 2015 Interim Analysis late 2017
Enrollment complete early 2016 Data lock 12m post-enrollment
BLA
1.5yr 2yr
6m 1yr
9m
6m 2yr
2yr
6m
1yr
1yr
Planned Milestones
Prostate
Brain
Pancreas
Lung
Checkpoint Inhibitors Combination
10 Gene Mediated Cytotoxic Immunotherapy
dvantagene
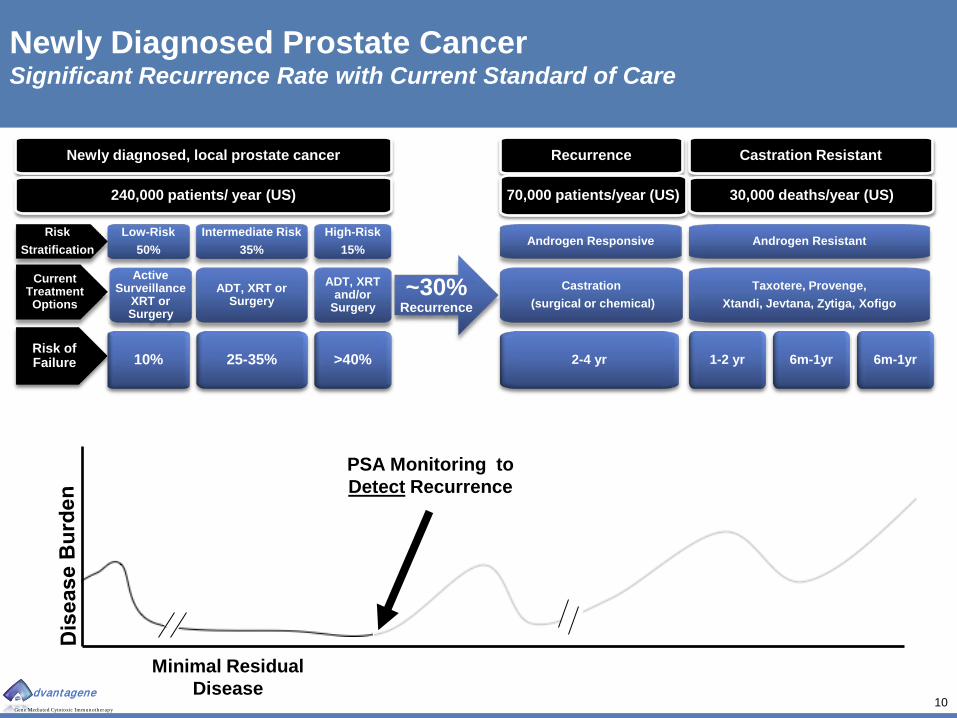
Newly Diagnosed Prostate Cancer Significant Recurrence Rate with Current Standard of Care
Active Surveillance
XRT or Surgery
Minimal Residual Disease
Newly diagnosed, local prostate cancer
Current Treatment Options
Low-Risk 50%
Intermediate Risk 35%
ADT, XRT or Surgery
High-Risk 15%
ADT, XRT and/or
Surgery
Risk of Failure 10% 25-35% >40%
Risk Stratification
Recurrence
Castration (surgical or chemical)
Castration Resistant
Androgen Responsive
Taxotere, Provenge, Xtandi, Jevtana, Zytiga, Xofigo
Androgen Resistant
2-4 yr 1-2 yr 6m-1yr 6m-1yr
PSA Monitoring to Detect Recurrence
~30% Recurrence
240,000 patients/ year (US) 70,000 patients/year (US) 30,000 deaths/year (US)

11 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Newly Diagnosed Intermediate-High Risk Prostate Cancer Significant Recurrence Rate with Current Standard of Care
Active Surveillance
XRT or Surgery
Minimal Residual Disease
Newly diagnosed, local prostate cancer
Current Treatment Options
Low-Risk 50%
Intermediate Risk 35%
ADT, XRT or Surgery
High-Risk 15%
ADT, XRT and/or
Surgery
Risk of Failure 10% 25-35% >40%
Risk Stratification
Recurrence
Castration (surgical or chemical)
Castration Resistant
Androgen Responsive
Taxotere, Provenge, Xtandi, Jevtana, Zytiga, Xofigo
Androgen Resistant
2-4 yr 1-2 yr 6m-1yr 6m-1yr
PSA Monitoring to Detect Recurrence
~30% Recurrence
240,000 patients/ year (US) 70,000 patients/year (US) 30,000 deaths/year (US)
Forecast with ProstAtak®
X
X Immunotherapy to PREVENT
Recurrence
Die of something other than prostate
cancer

12 Gene Mediated Cytotoxic Immunotherapy
entagen
Pre-Prostatectomy Patients- Evidence of Biological Activity Durable response after single administration in high-risk patients
0
5
10
15
20
25
30
-6 12 30 48 66 84 102 120
PSA
(ng/
ml)
Time (mos)
Biochemical Failure (>0.4ng/ml)
• ProstAtak administered pre-prostatectomy
• 10 patients treated • 1 pre-surgery dropout • 3 intermediate or low risk • 6 high risk at surgery
• 6 with positive margins
• 1 with seminal vesicle involvement
• 11.3 year median follow-
up • Durable PSA suppression • No clinical progression • No significant related SAEs
or late toxicities • Avoiding ADT is a clinical
benefit
Rojas-Martinez et al CGT 2013
Summary of Outcomes
Ten Year PSA Follow-Up No Additional Treatment Castration Avoided

13 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Phase 2 N=71 Newly diagnosed localized prostate
cancer
Arm A (33 pts)
Low-Risk (T1-T2a, Gleason <7, PSA<10)
2 cycles of AdV-tk, valacyclovir (VCV) plus
XRT
Arm B (33 pts)
Intermediate-High-Risk (T2b-T3, Gleason >6,
PSA≥10)
3 cycles of AdV-tk, VCV, androgen deprivation
(ADT), plus XRT
Arm C* (5 pts)
Stage D1 (positive lymph node)
Same as Arm B, plus XRT to pelvic lymphatics
Radiation Therapy Patients- Evidence of Efficacy Simple outpatient procedure delivered with standard of care
Pre-radiotherapy Radiotherapy Post-radiotherapy
First course: 15 days-8 weeks prior to radiotherapy
Second course: 0-3 days prior to radiotherapy
Third course: 15-22 days after previous injection
14 days
+/- Short-term androgen deprivation therapy
14 days 14 days Valacyclovir pills

14 Gene Mediated Cytotoxic Immunotherapy
dvantagene
ProstAtak® Phase 2 Results Indicate Significant Benefit to Patients Improved Durable Clinical Response
0%
5%
10%
15%
20%
Peeters(2006)
Dearnaley(2007)
Zelefsky(2006)
Advantagene(Teh 2004;
Aguilar, 2006)
16% 15% 11%
0%
Low Risk Group
0%
5%
10%
15%
20%
25%
30%
35%
Peeters(2006)
Dearnaley(2007)
Zelefsky(2006)
D'Amico(2008)
D'Amico(2008)
Advantagene(Teh 2004;
Aguilar,2006)
21% 21% 22%
34%
25%
5%
Intermediate Risk Group
( - ADT) (+ ADT)
Perc
ent T
reat
men
t Fai
lure
Perc
ent T
reat
men
t Fai
lure
Pe
rcen
t Tre
atm
ent F
ailu
re
5 4.3 7 8.2 8.2 5.7 Median
Follow-Up (Years )
~75% Reduction in Phase 2
0%5%
10%15%20%25%30%35%40%45%
Peeters(2006)
Dearnaley(2007)
Zelefsky(2006)
Advantagene(Teh 2004;
Aguilar, 2006)
44% 43%
33%
20%
High Risk Group
5 4.3 7 5.7 Median F/U (yrs )
5 4.3 7 5.7 Median F/U (yrs. )
ProstAtak outside 95% C.I. for all risk groups’ Mean Event rate/person*year
Long-Term Freedom From Failure Rates
15 Gene Mediated Cytotoxic Immunotherapy
dvantagene
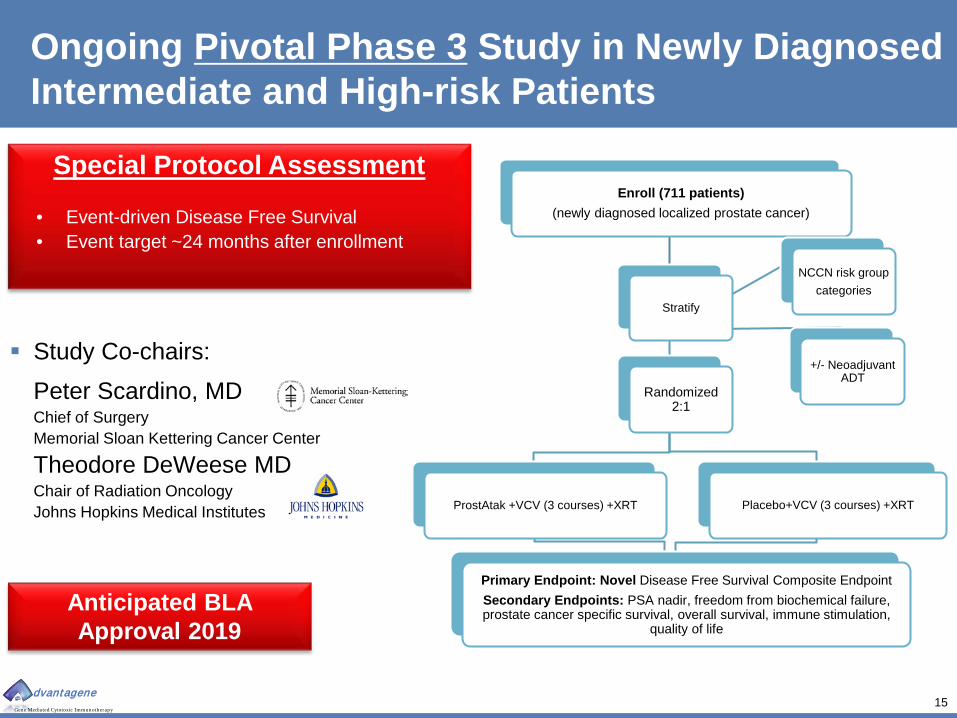
Ongoing Pivotal Phase 3 Study in Newly Diagnosed Intermediate and High-risk Patients
Study Co-chairs: Peter Scardino, MD Chief of Surgery Memorial Sloan Kettering Cancer Center
Theodore DeWeese MD Chair of Radiation Oncology Johns Hopkins Medical Institutes
Enroll (711 patients) (newly diagnosed localized prostate cancer)
Stratify
Randomized 2:1
ProstAtak +VCV (3 courses) +XRT Placebo+VCV (3 courses) +XRT
Primary Endpoint: Novel Disease Free Survival Composite Endpoint Secondary Endpoints: PSA nadir, freedom from biochemical failure, prostate cancer specific survival, overall survival, immune stimulation,
quality of life
NCCN risk group categories
+/- Neoadjuvant ADT
Anticipated BLA Approval 2019
Special Protocol Assessment
• Event-driven Disease Free Survival • Event target ~24 months after enrollment
16 Gene Mediated Cytotoxic Immunotherapy
dvantagene
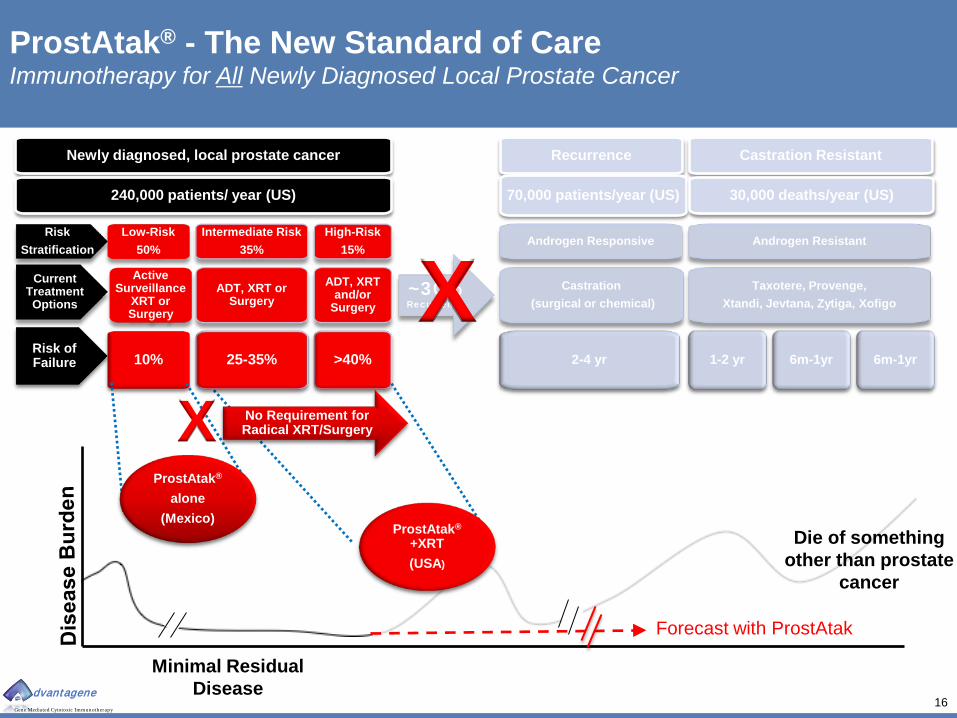
Active Surveillance
XRT or Surgery
Minimal Residual Disease
Newly diagnosed, local prostate cancer
Current Treatment Options
Low-Risk 50%
Intermediate Risk 35%
ADT, XRT or Surgery
High-Risk 15%
ADT, XRT and/or
Surgery
Risk of Failure 10% >40%
Risk Stratification
Recurrence
Castration (surgical or chemical)
Castration Resistant
Androgen Responsive
Taxotere, Provenge, Xtandi, Jevtana, Zytiga, Xofigo
Androgen Resistant
2-4 yr 1-2 yr 6m-1yr 6m-1yr
~30% Recurrence
240,000 patients/ year (US) 70,000 patients/year (US) 30,000 deaths/year (US)
Die of something other than prostate
cancer
Forecast with ProstAtak
No Requirement for Radical XRT/Surgery
ProstAtak® alone
(Mexico) ProstAtak®
+XRT (USA)
X
ProstAtak® - The New Standard of Care Immunotherapy for All Newly Diagnosed Local Prostate Cancer
X 25-35%
17 Gene Mediated Cytotoxic Immunotherapy
dvantagene
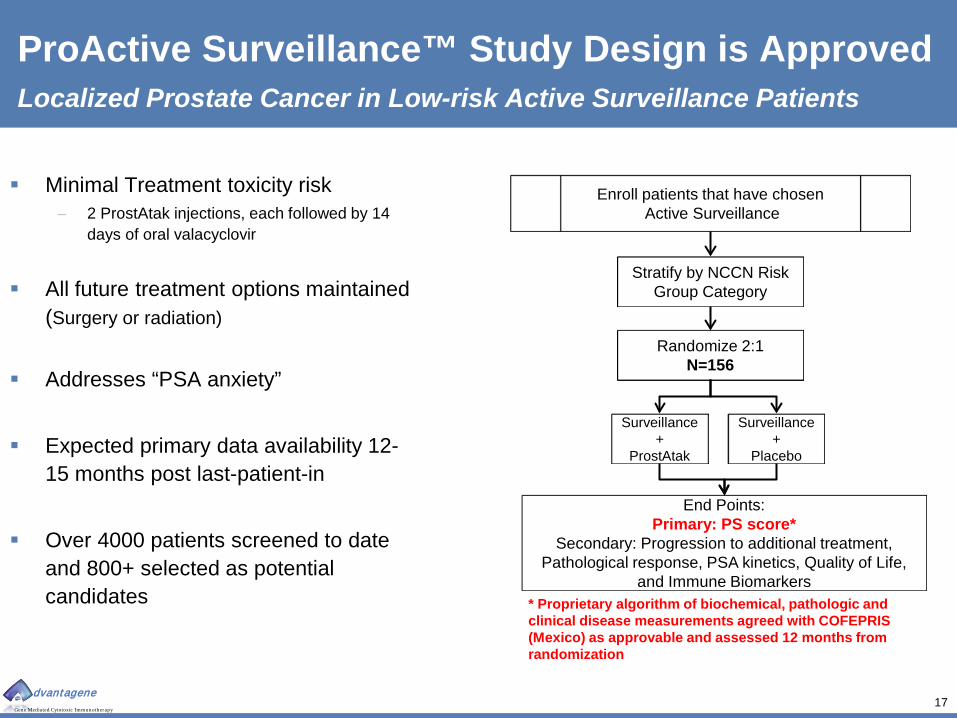
ProActive Surveillance™ Study Design is Approved Localized Prostate Cancer in Low-risk Active Surveillance Patients
Minimal Treatment toxicity risk – 2 ProstAtak injections, each followed by 14
days of oral valacyclovir
All future treatment options maintained (Surgery or radiation)
Addresses “PSA anxiety”
Expected primary data availability 12-15 months post last-patient-in
Over 4000 patients screened to date
and 800+ selected as potential candidates
Enroll patients that have chosen Active Surveillance
Stratify by NCCN Risk Group Category
Randomize 2:1 N=156
Surveillance +
ProstAtak
Surveillance +
Placebo
End Points: Primary: PS score*
Secondary: Progression to additional treatment, Pathological response, PSA kinetics, Quality of Life,
and Immune Biomarkers * Proprietary algorithm of biochemical, pathologic and clinical disease measurements agreed with COFEPRIS (Mexico) as approvable and assessed 12 months from randomization

18 Gene Mediated Cytotoxic Immunotherapy
dvantagene
ProstAtak® Projected Annual Net Sales Localized Intermediate to High Risk Prostate Cancer Only (USA & EU)
12 years market exclusivity for biologics
Additional approval for “Active Surveillance” will increase revenues by ~50% - ~75%

19 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Malignant Glioma Completed Phase 2 Shows Improved OS
Annual Diagnoses: ~20,000 Annual Deaths: ~15,000 Survival: median < 15 mos; 2yr ~26% Key Products: temozolomide (Merck; Est Peak Sales > $1B)
Program Status Two Phase 1 studies: Recurrent disease and newly diagnosed Phase 2 Study: Newly diagnosed in combination with standard of care Phase 2b: target launch late-2015
Principal Clinical Investigator: E. Antonio Chiocca, M.D, Ph.D. Chairman, Neurosurgery
Overview of 48 Patient Multisite Phase 2 Study
Outcomes compared with preplanned control cohort
No DLT or significant toxicity observed Overall Survival benefit in entire treated population
Dramatic benefit in patients with total resection
(>95% tumor removal)
AdV-tk delivered to tumor cells via tumor bed injection, Valacyclovir prodrug -orally for 14 days
20 Gene Mediated Cytotoxic Immunotherapy
dvantagene
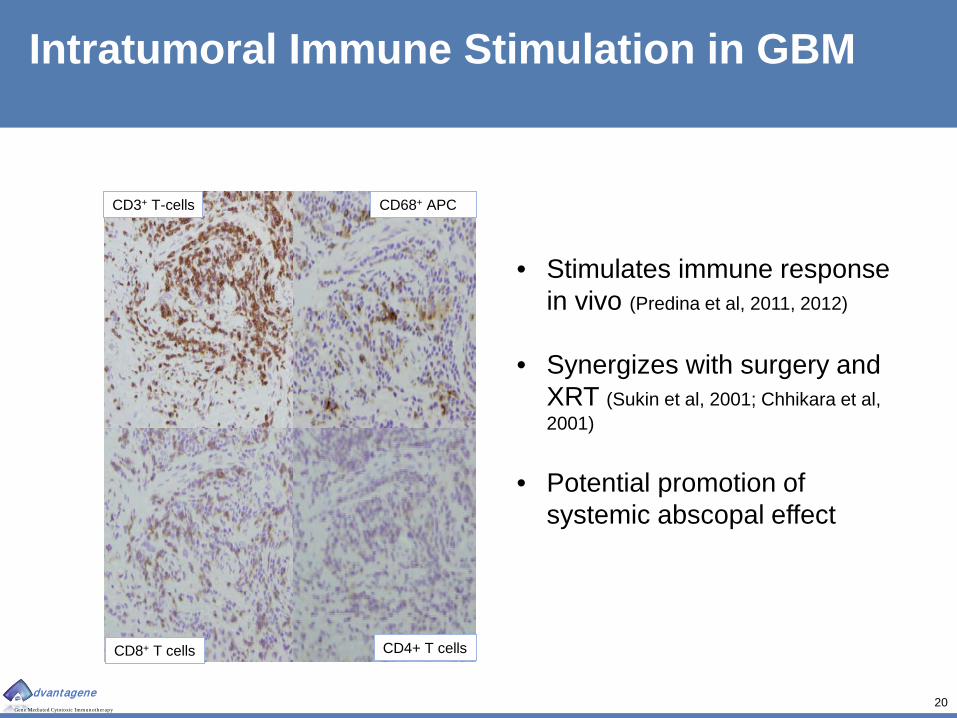
Intratumoral Immune Stimulation in GBM
CD3+ T-cells CD68+ APC
CD4+ T cells CD8+ T cells
• Stimulates immune response in vivo (Predina et al, 2011, 2012)
• Synergizes with surgery and
XRT (Sukin et al, 2001; Chhikara et al, 2001)
• Potential promotion of
systemic abscopal effect
21 Gene Mediated Cytotoxic Immunotherapy
dvantagene
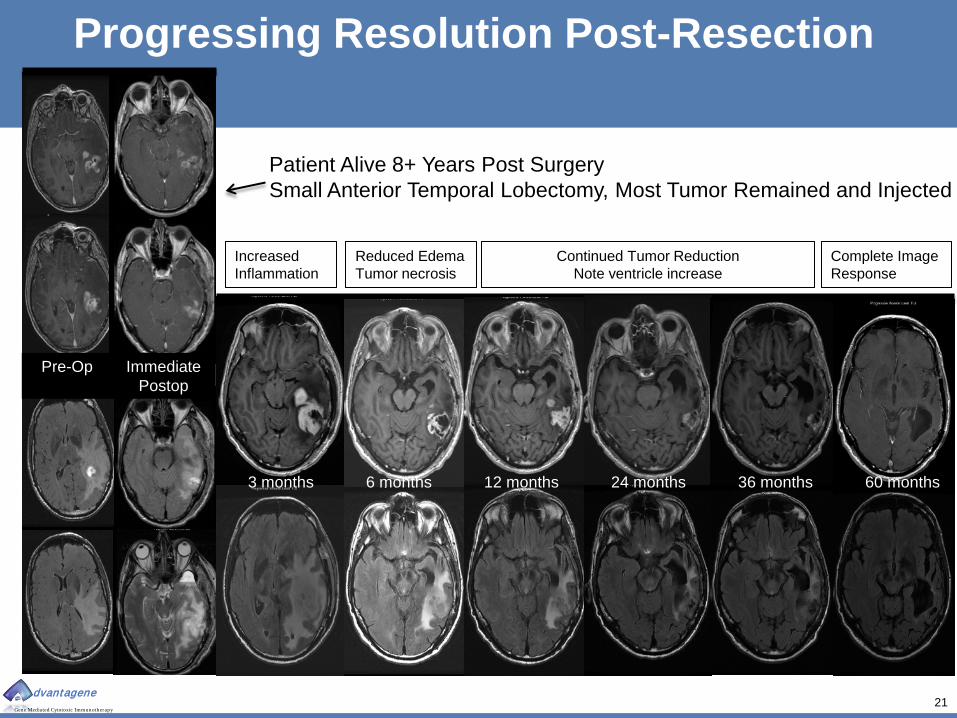
Increased Inflammation
Reduced Edema Tumor necrosis
Continued Tumor Reduction Note ventricle increase
Complete Image Response
3 months 6 months 12 months 24 months 36 months 60 months
Pre-Op Immediate Postop
Patient Alive 8+ Years Post Surgery Small Anterior Temporal Lobectomy, Most Tumor Remained and Injected
Progressing Resolution Post-Resection
22 Gene Mediated Cytotoxic Immunotherapy
dvantagene
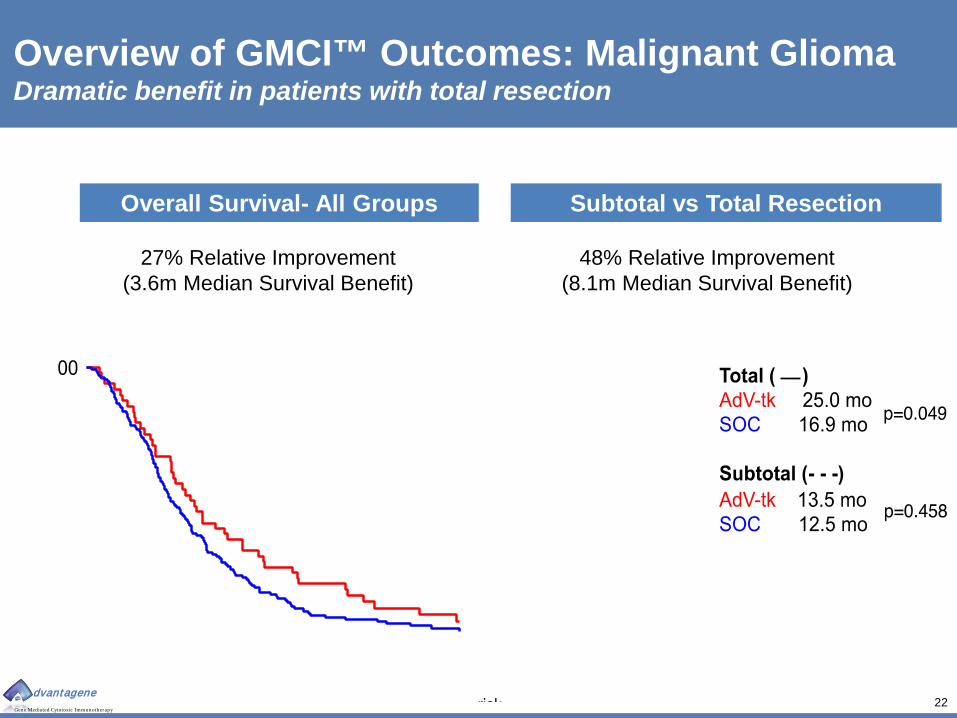
Overview of GMCI™ Outcomes: Malignant Glioma Dramatic benefit in patients with total resection
Subtotal vs Total Resection Overall Survival- All Groups
27% Relative Improvement (3.6m Median Survival Benefit)
48% Relative Improvement (8.1m Median Survival Benefit)

23 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Expanding Advantage in Survival Rate Dramatic benefit in patients with total resection
Study Cohort
N
OS 12 Months
(%)
OS 24 Months
(%)
OS 36 Months
(%)
Median OS
(mos) p value Group Subgroup Treatment
All H
isto
logi
es
(GBM
, AA,
and
AO
) All Resections
GMCI 48 66.7 35.4 18.8* 17.1 (0.0417)
SOC 134 56.7 21.6 7.5 13.5
Gross Total
Resection
GMCI 19 89.5 52.6 31.6* 25.0 (0.0492)
SOC 47 63.8 27.7 6.4 16.9
Subtotal Resection
GMCI 29 51.7 24.1 10.3 13.5 (0.4584)
SOC 87 52.9 18.4 8.0 12.5
GBM
Onl
y
All Resections
GMCI 43 62.8 32.6 14.0 16.7 (0.2073)
SOC 128 57.8 21.9 7.0 13.7
Gross Total
Resection
GMCI 18 88.9 55.6* 33.3* 25.1 (0.0120) SOC 44 63.6 27.3 4.5 16.3
Subtotal Resection
GMCI 25 44.0 16.0 0.0 10.6 (0.2231)
SOC 84 54.8 19.0 8.3 12.8
*Statistically significant (p<0.05) using two-tailed Fisher Exact probably test
24 Gene Mediated Cytotoxic Immunotherapy
dvantagene
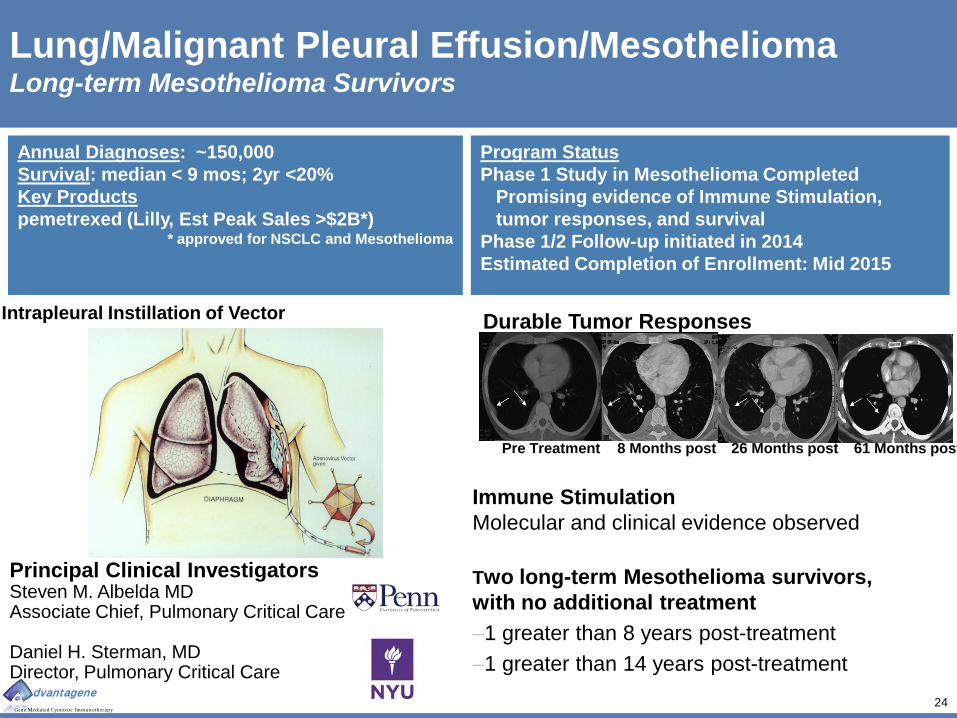
Lung/Malignant Pleural Effusion/Mesothelioma Long-term Mesothelioma Survivors
Annual Diagnoses: ~150,000 Survival: median < 9 mos; 2yr <20% Key Products pemetrexed (Lilly, Est Peak Sales >$2B*)
* approved for NSCLC and Mesothelioma
Pre Treatment 8 Months post 26 Months post 61 Months post
Two long-term Mesothelioma survivors, with no additional treatment –1 greater than 8 years post-treatment –1 greater than 14 years post-treatment
Durable Tumor Responses
Immune Stimulation Molecular and clinical evidence observed
Program Status Phase 1 Study in Mesothelioma Completed Promising evidence of Immune Stimulation, tumor responses, and survival Phase 1/2 Follow-up initiated in 2014 Estimated Completion of Enrollment: Mid 2015
Intrapleural Instillation of Vector
Principal Clinical Investigators Steven M. Albelda MD Associate Chief, Pulmonary Critical Care Daniel H. Sterman, MD Director, Pulmonary Critical Care

25 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Pancreatic Cancer Increased Survival and Immuno-reactivity with No Increased Toxicity
Program Status Phase 1/2 Study- 24 patients Completed with Positive Data Phase 2b launch estimated 1H2015
• CD8+ lymphocytic infiltrate • Enhanced PD-L1 expression
Immune Stimulation Observed
0
10
20
30
40
50
60
Median PFS(mo)
Median OS(mo)
1-Yr Survival(%)
Toxicity(rel units)
5-FU
5-FU + AdV-tk
Gemcitabine
Annual Diagnoses: ~45,000 Annual Deaths: ~ 40,000 Survival: median < 11 mos; 1yr <50% Key Products: gemcitabine (Lilly, Est Peak Sales $3.5B*) albumin-bound paclitaxel (Celgene, Est Peak Sales $2.1B*)
*Multiple tumor types
Preclinical studies ongoing to enable GMCI + anti-PD1 combination study
0 Wk 3-4 Wk 9 q 3-4mos
AdV-tk
Valacyclovir
Valacyclovir
Arm A: Surgery
CT scans and CA19-9 Arm B: 5-FU Chemoradiation
AdV-tk
Red=Standard of care procedures
Primary Clinical Investigator: Mark Bloomston, MD Tanios Bekaii-Saab, MD Phase 1/2 Study: Completed 24 evaluable pancreatic cancer patients 3 clinical sites: Ohio State University, City of Hope and Scripps
Locally Advanced Pancreatic Cancer
25% Response Rate by RESIST Criteria

26 Gene Mediated Cytotoxic Immunotherapy
dvantagene
0
20
40
60
80
100
120
140
CD4+ Pre-Tx CD4+ Post-Tx
CD8+ Pre-Tx CD8+ Post-Tx
1A03
2A02
3A01
3A02
3A03
4A01
4A02
Case Number
Clinical Immune Stimulation & Checkpoint Response PaTK01 patient samples
21.4 Fold Average Increase 1.3 Fold Average Increase
Pre AdV-tk Post AdV-tk
CD8+ T-cells CD4+ T-cells
Cells
Per
Hig
h-Po
wer
ed F
ield
Quantification of Cellular Infiltrate
Pre AdV-tk Post AdV-tk Pre AdV-tk Post AdV-tk
PD-L1+ Tumor Cells
General Up-regulation
Cellular Staining
IND enabling studies with GMCI® and checkpoint inhibitors are underway
27 Gene Mediated Cytotoxic Immunotherapy
dvantagene
Summary
Safe & Effective Multiple Phase 1 and Phase 2 clinical studies complete >350 patients treated, >650 patients doses in multiple oncology settings Long term follow-up data (up to 5-14 years) Blockbuster potential Multiple late stage clinical programs (first line prostate, glioma, pancreas, lung) Significant advancement in prostate first line SOC
Differentiated No marketed products or late stage R&D programs for first line prostate cancer Favorable pharmacoeconomics Experienced Executive Team Successfully designed and completed multiple large clinical trials 14 FTEs Premier KOL’s

Gene Mediated Cytotoxic Immunotherapy (GMCI™)
dvantagene
Thank You!





























