Embed Size (px)
DESCRIPTION
The Role of Surgery in Malignant Pleural Mesothelioma presented by Harvey Pass, MD of NYU at the Mesothelioma Applied Research Foundation's conference in New York, NY on September 28, 2012. www.curemeso.org
Citation preview
Surgery for Mesothelioma: The Broad Stroke of a Paintbrush
Harvey I. Pass MD Stephen A. Banner Professor of Thoracic Oncology Vice-Chairman, Research, Cardiothoracic Surgery
NYU Langone Medical Center
Surgery for Mesothelioma
• What is the use of surgery in pleural mesothelioma?
• What are the present limitations in deciding whether a patient should have surgery for pleural mesothelioma?
• Why is there so much controversy about surgery for pleural mesothelioma?
• What are the types of operations for pleural mesothelioma and who are they suited for?
• What, if anything, should be combined with surgery for pleural mesothelioma?
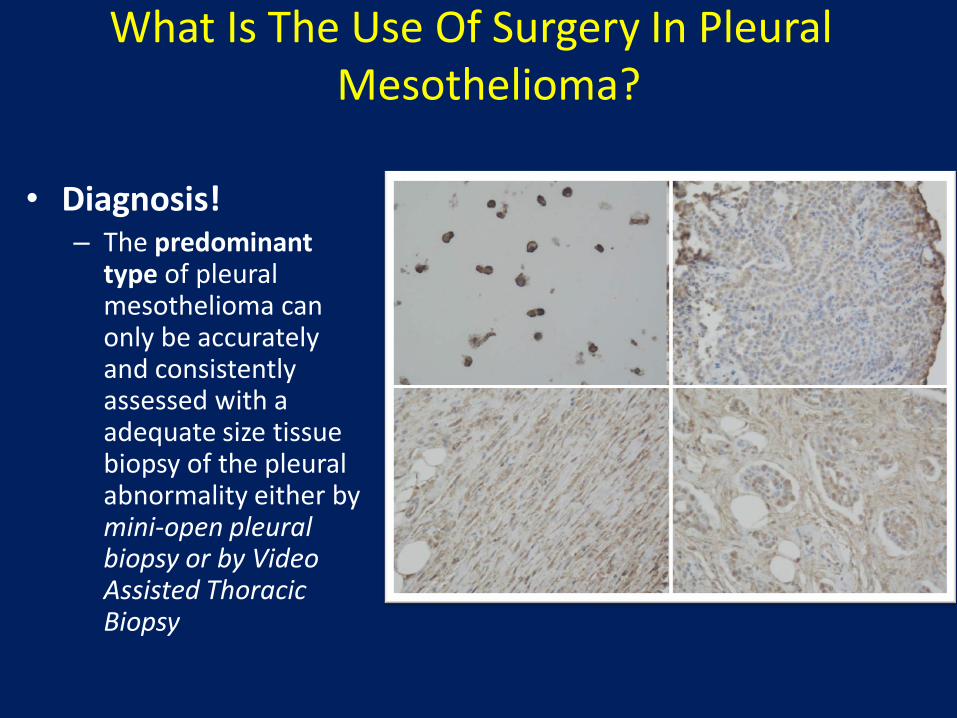
What Is The Use Of Surgery In Pleural Mesothelioma?
• Diagnosis!
– The predominant type of pleural mesothelioma can only be accurately and consistently assessed with a adequate size tissue biopsy of the pleural abnormality either by mini-open pleural biopsy or by Video Assisted Thoracic Biopsy
What Is The Use Of Surgery In Pleural Mesothelioma
Effusion Control
• Video Assisted Thoracoscopic Pleurodesis
• PleurX or Bard Aspira Catheter
But what about trying to possibly cure pleural mesothelioma by
involving surgery?
What are the present limitations in deciding whether a patient should have surgery for pleural mesothelioma?
• It is very difficult to cure mesothelioma with surgery because – The biology of the disease makes it difficult for mesothelioma
physicians to accurately tell patients how aggressive the disease and this prevents the physicians from guaranteeing that the disease will not recur shortly after surgery
– The staging system for pleural mesothelioma is not good
– The disease usually presents at a more advanced stage
– The surgery is demanding and patients who can have surgery must have a good performance status
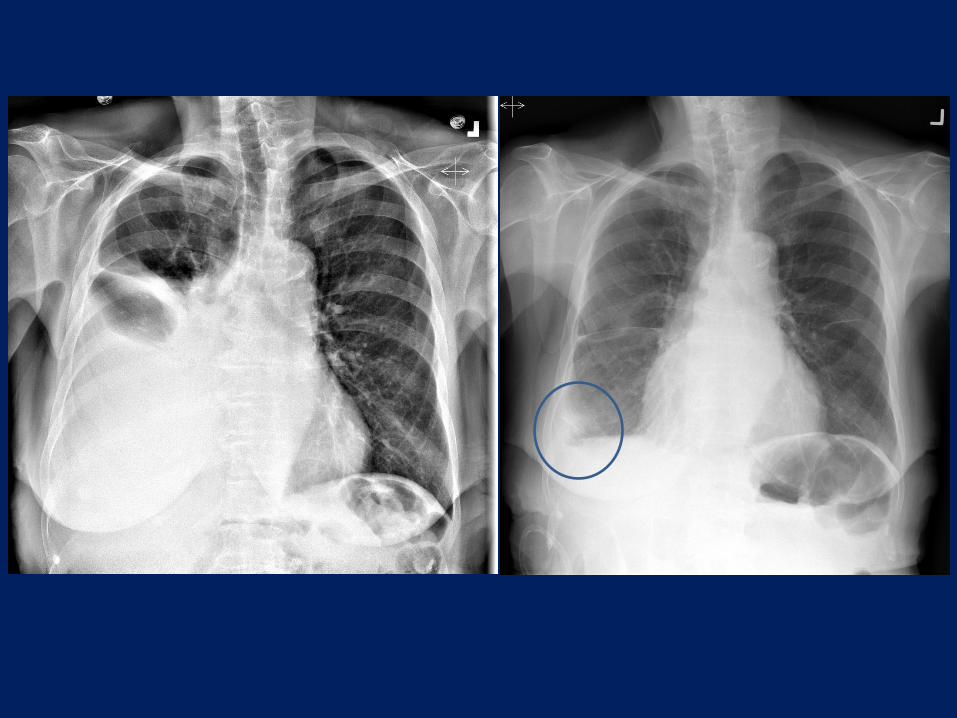
– The disease usually presents as a combination of solid disease and fluid which contains mesothelioma cells
– By its very nature, pleural mesothelioma is a diffuse, not a localized disease
What are the present limitations in deciding whether a patient should have surgery for pleural mesothelioma?
• How can we chose patients better for surgery?
– Clinical Factors:
• Age, sex, functional status, white blood cell count, platelet count, chest pain
– Pathologic Factors:
• Type of mesothelioma, evidence of spread
– Physiologic Factors:
• Performance status, heart and lung function
– Molecular Biology Factors:
• Gene, protein, RNA and DNA profiles
What are the present limitations in deciding whether a patient should have surgery for pleural mesothelioma?
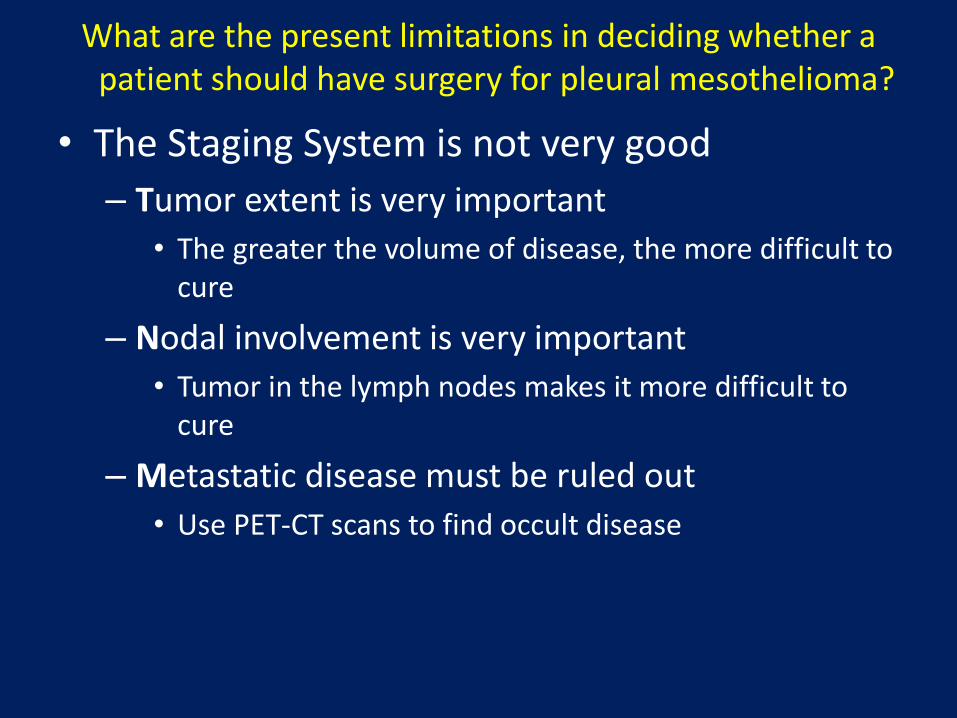
• The Staging System is not very good
– Tumor extent is very important
• The greater the volume of disease, the more difficult to cure
– Nodal involvement is very important
• Tumor in the lymph nodes makes it more difficult to cure
– Metastatic disease must be ruled out
• Use PET-CT scans to find occult disease
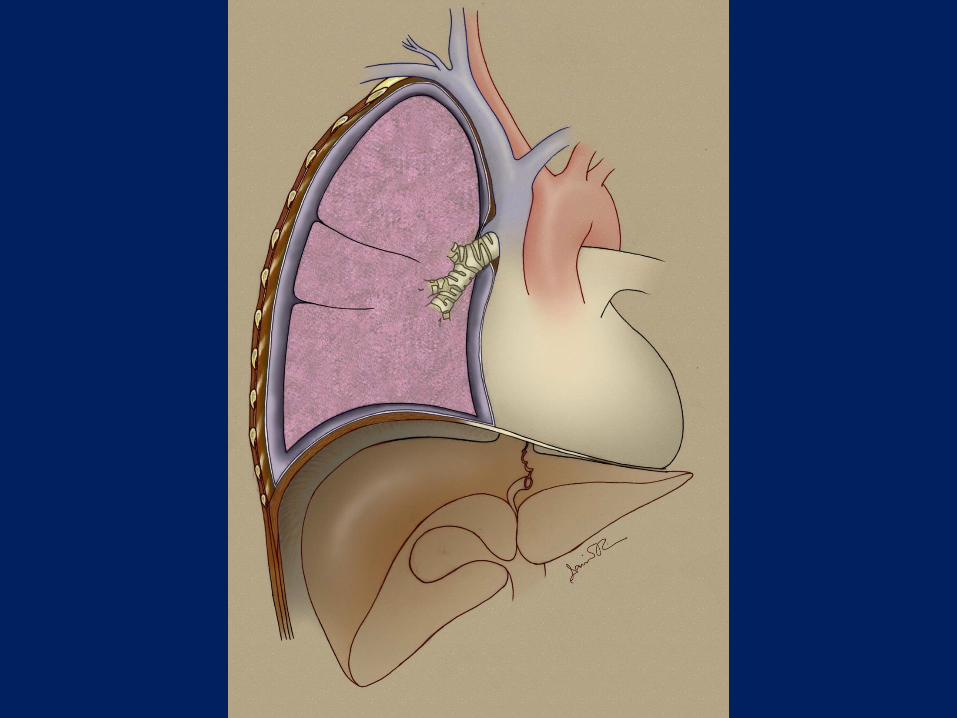
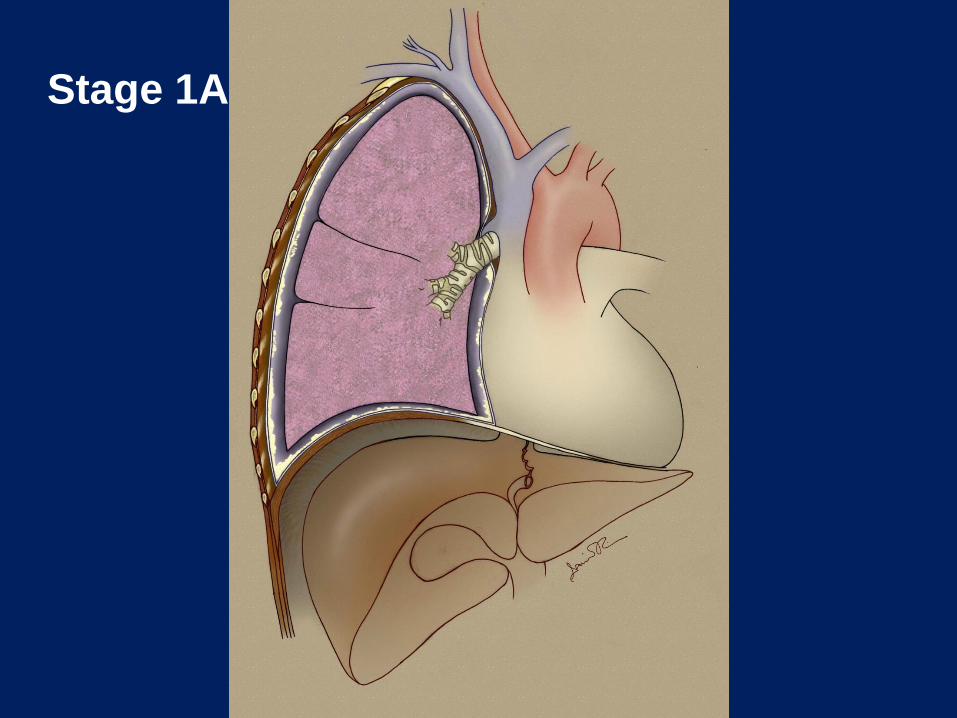
Stage 1A
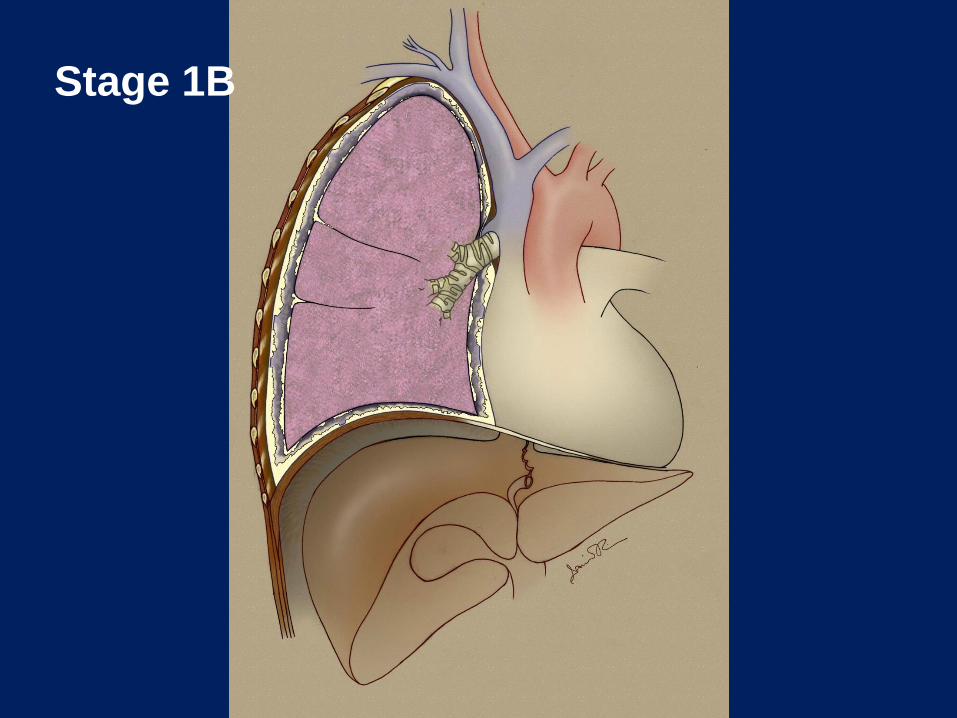
Stage 1B
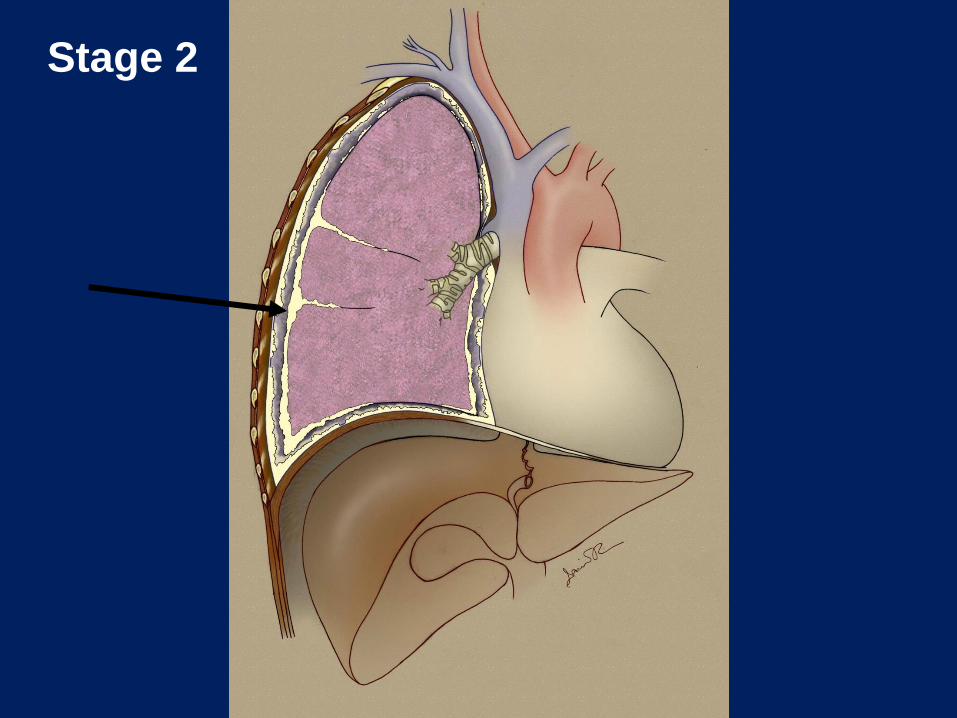
Stage 2
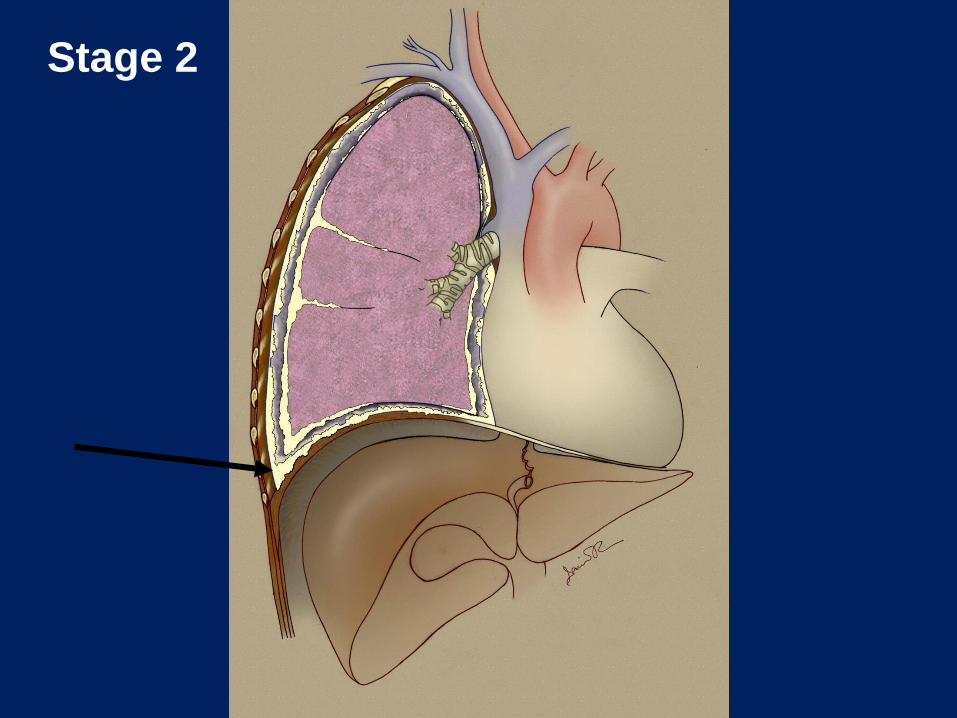
Stage 2
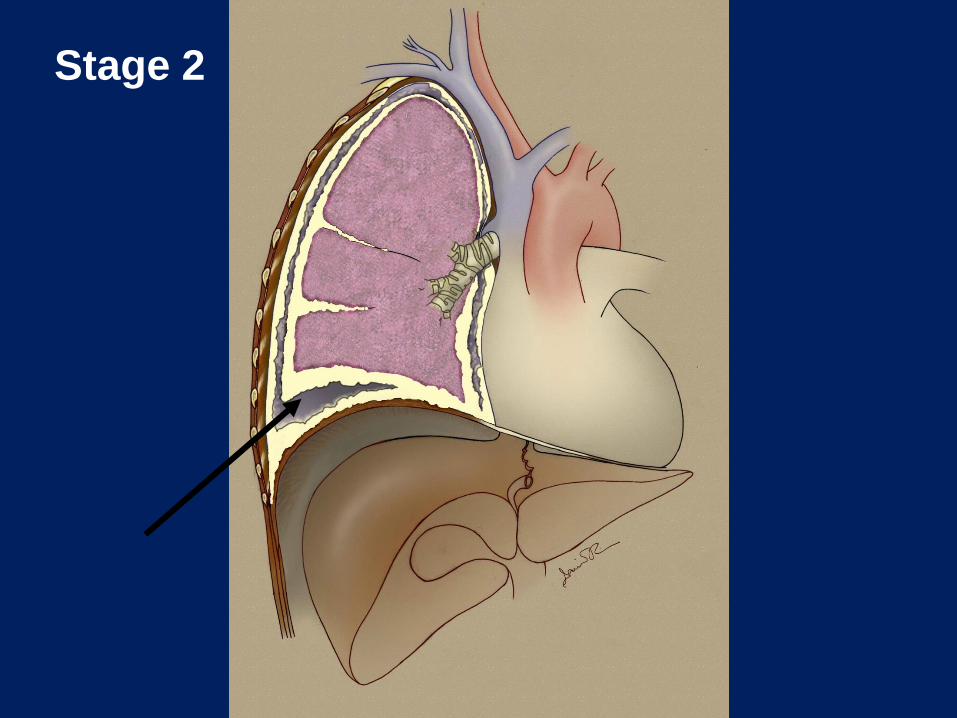
Stage 2
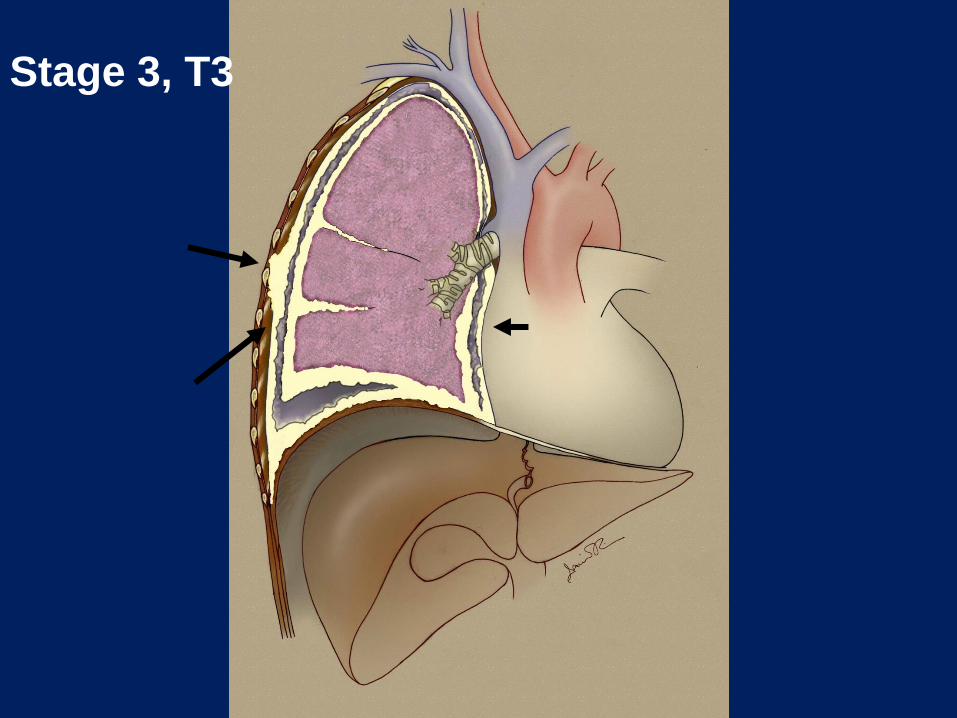
Stage 3, T3
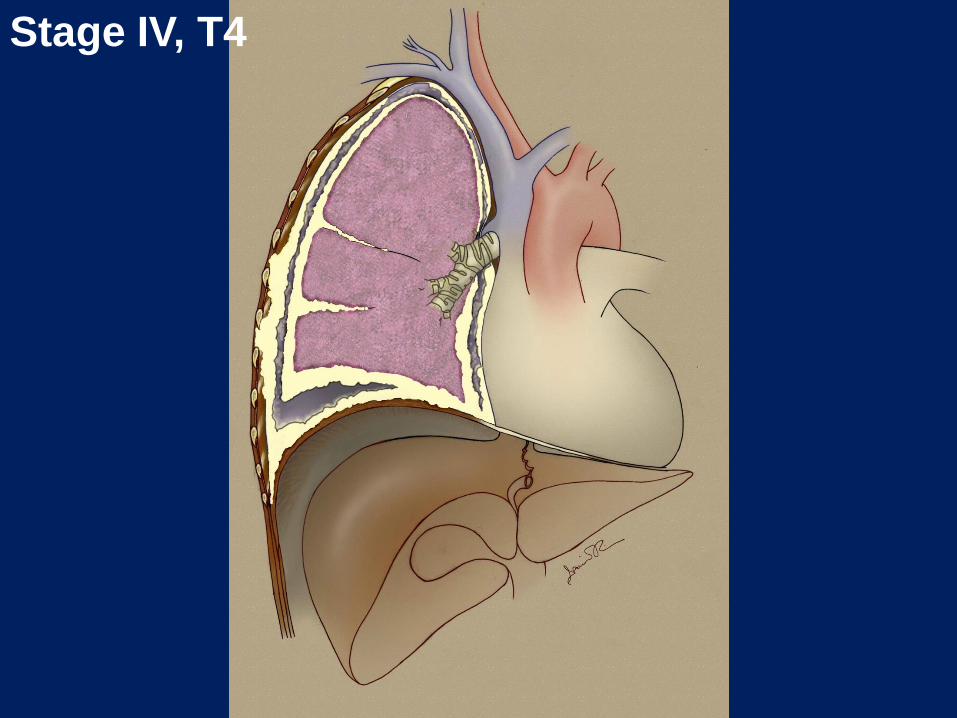
Stage IV, T4
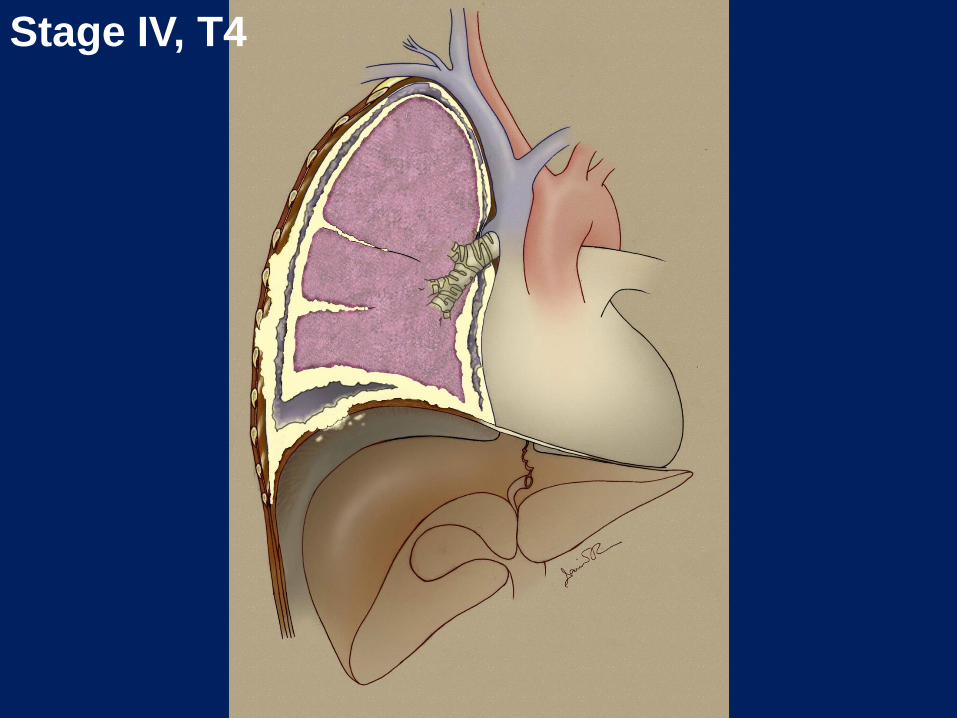
Stage IV, T4
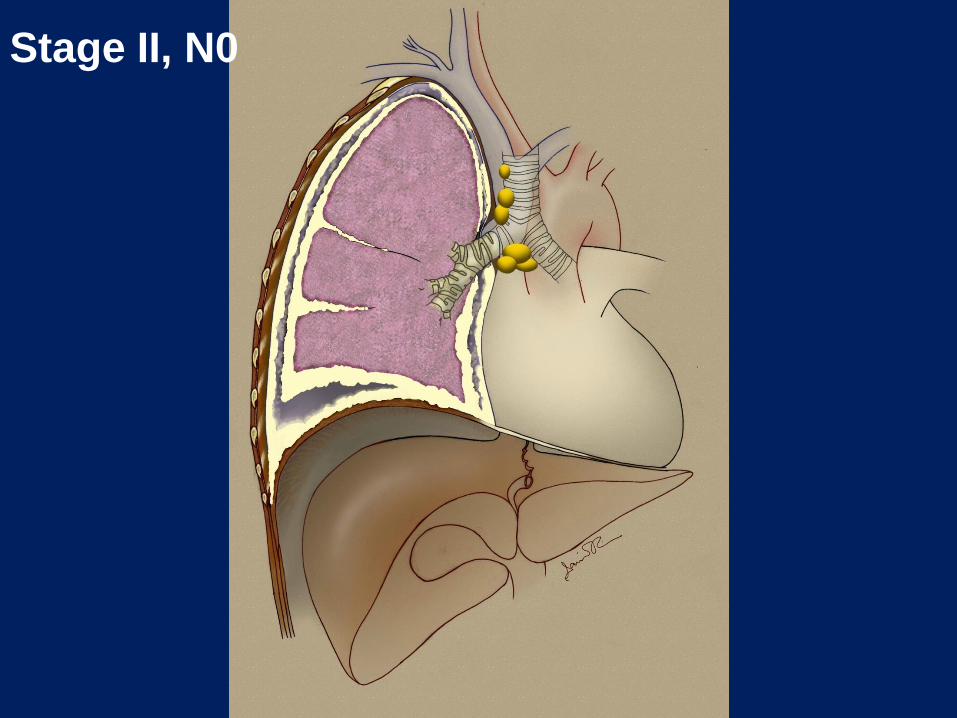
Stage II, N0
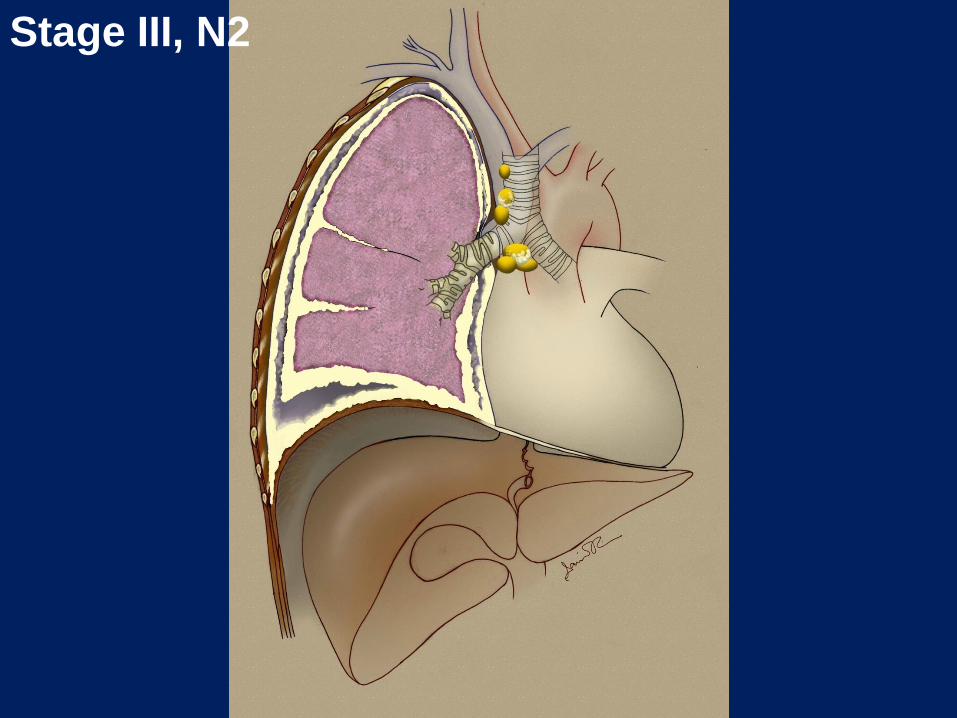
Stage III, N2
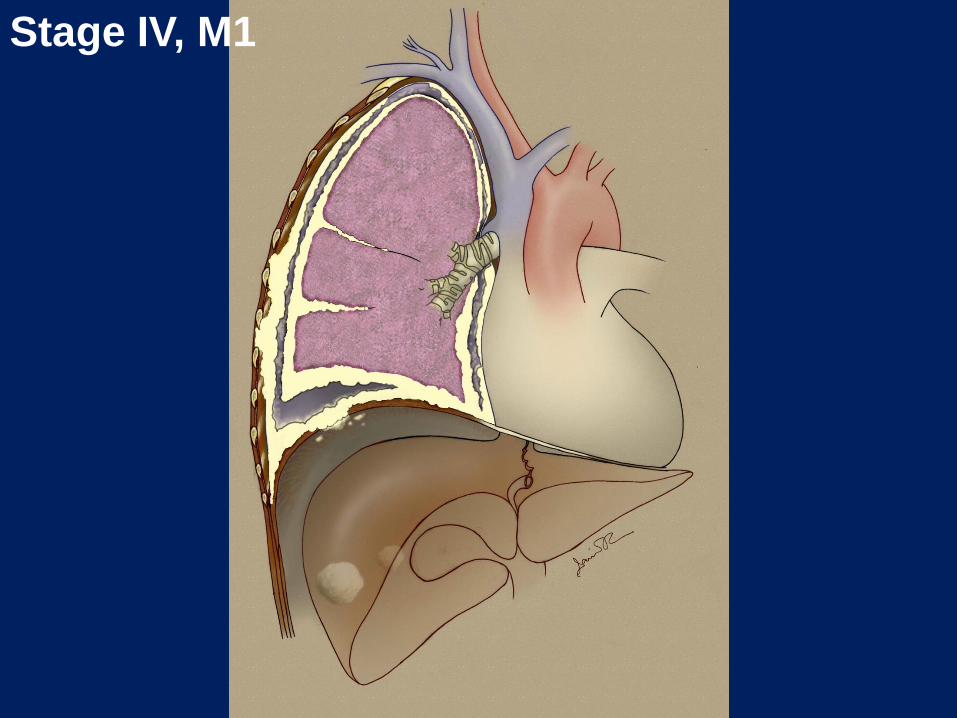
Stage IV, M1
Why is there so much controversy about surgery for pleural mesothelioma?
• These are big operations in frequently elderly individuals
• There has not been a uniform definition of the operations so everybody is on the same wavelength
• There is a bias among mesothelioma physicians that – NO operation is useful in mesothelioma or
– CERTAIN operations are not useful in mesothelioma
• Surgeons who do these operations are only now beginning to understand that one size does not fit all
What are the types of operations for pleural mesothelioma and who are they suited for?
• Pleurectomy Decortication (PD: Standard or Extended) – Usually less bulky disease – Great operation for Stage I mesothelioma – Patient remains functional since the lung is spared – Risk and Morbidity is lower than EPP – Recurrence usually within the same chest
• Extrapleural Pneumonectomy (EPP) – More extensive/Invasive disease where a PD would
leave non-functional, useless lung – Functional status must be very good preoperatively – Higher mortality and morbidity than PD but
acceptable in expert hands – Recurrence is usually outside the same chest
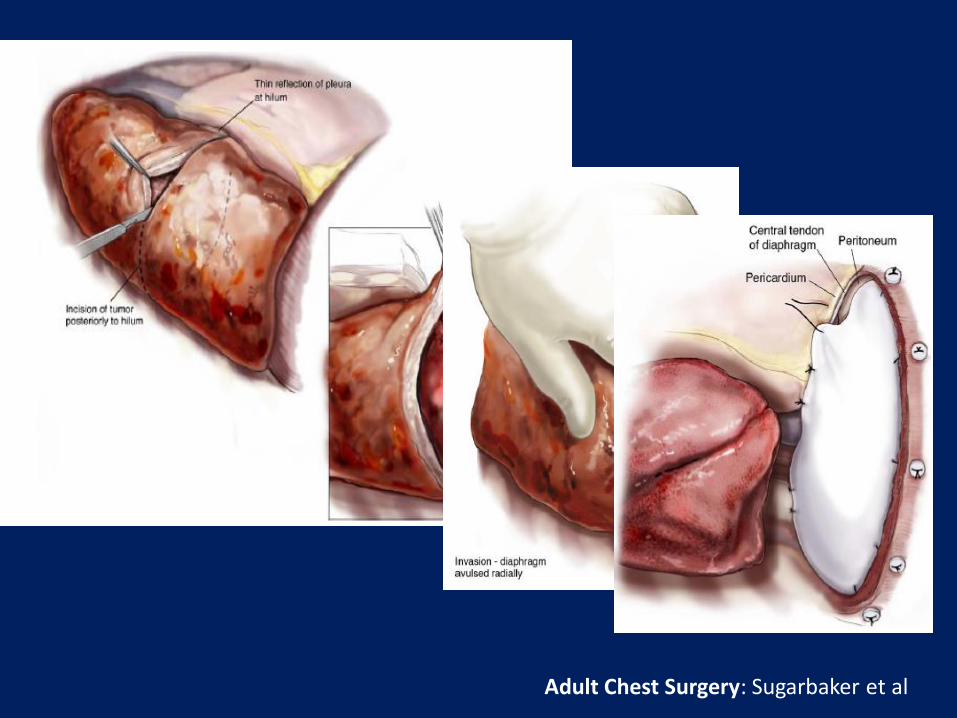
Adult Chest Surgery: Sugarbaker et al

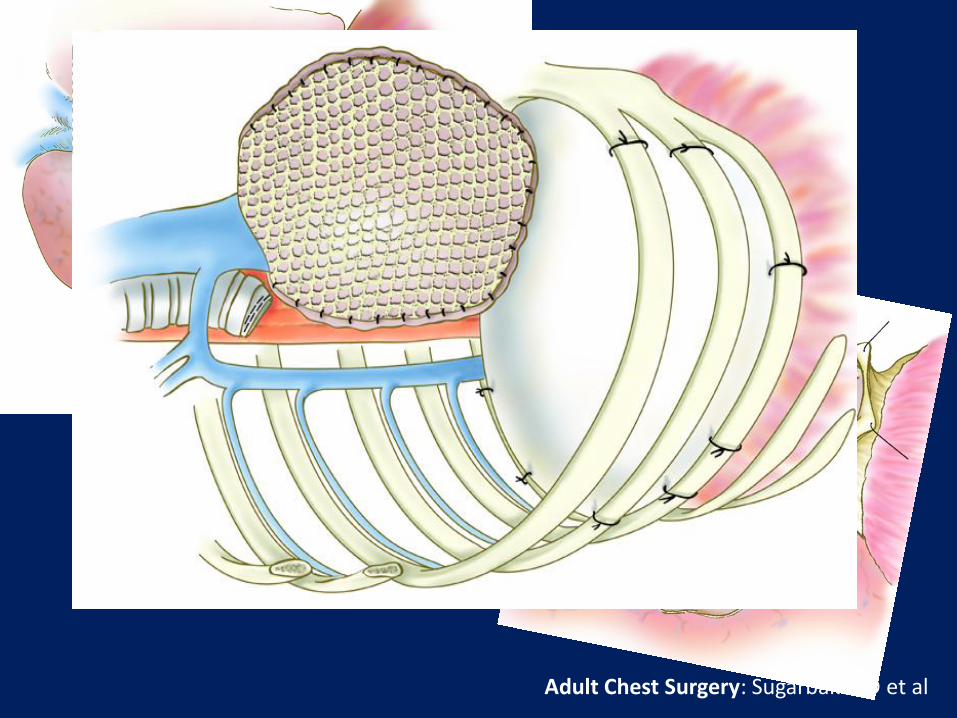
Adult Chest Surgery: Sugarbaker D et al
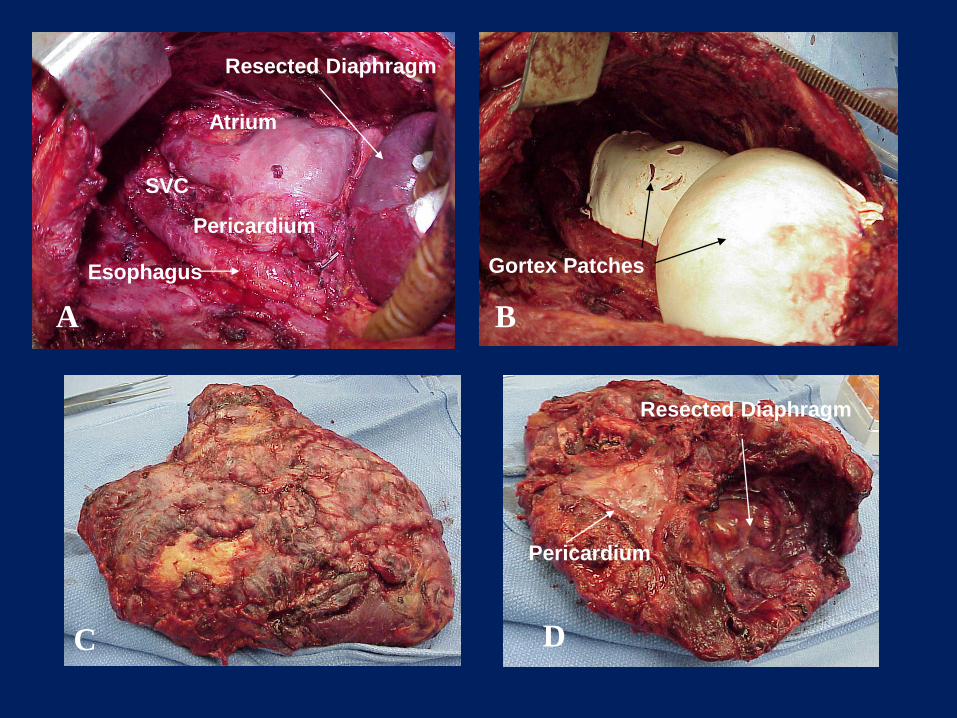
Esophagus
Resected Diaphragm
SVC
Atrium
Pericardium
Gortex Patches
Pericardium
Resected Diaphragm
A B
C D
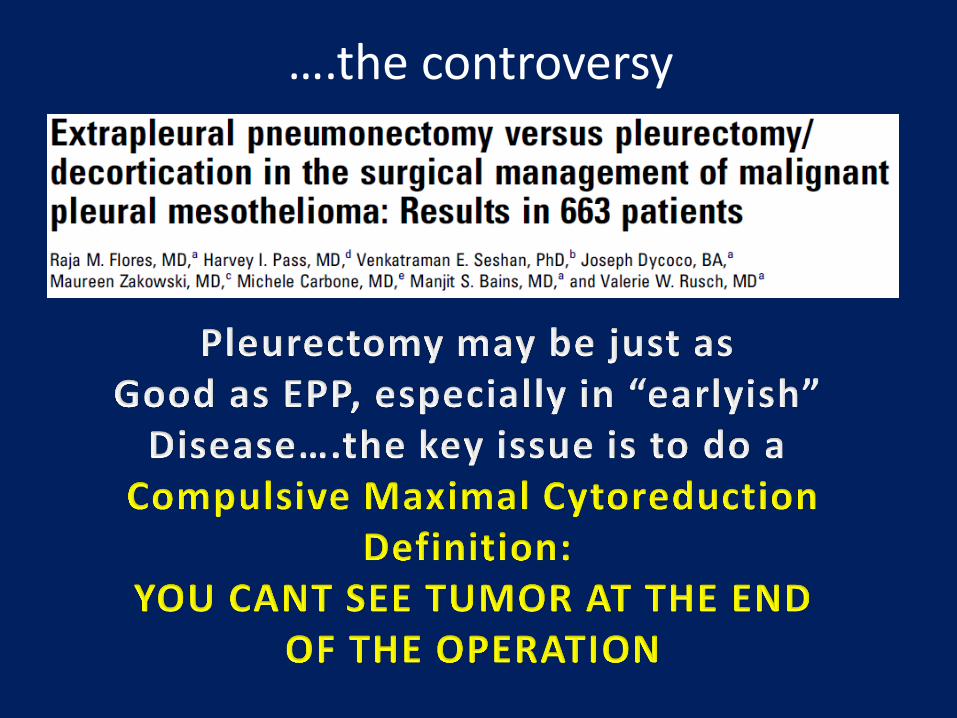
….the controversy
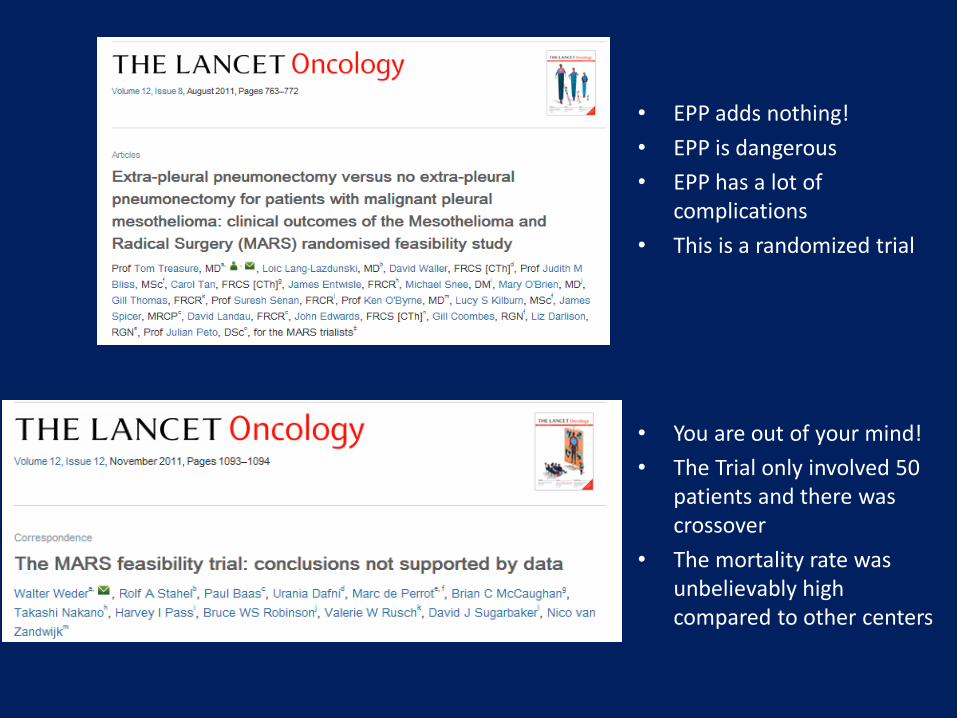
• EPP adds nothing!
• EPP is dangerous
• EPP has a lot of complications
• This is a randomized trial
• You are out of your mind!
• The Trial only involved 50 patients and there was crossover
• The mortality rate was unbelievably high compared to other centers
EPP BOSTON
SWISS
AUSSIE
PD UPENN
UCLA
UK
MSKCC Sinai NYU
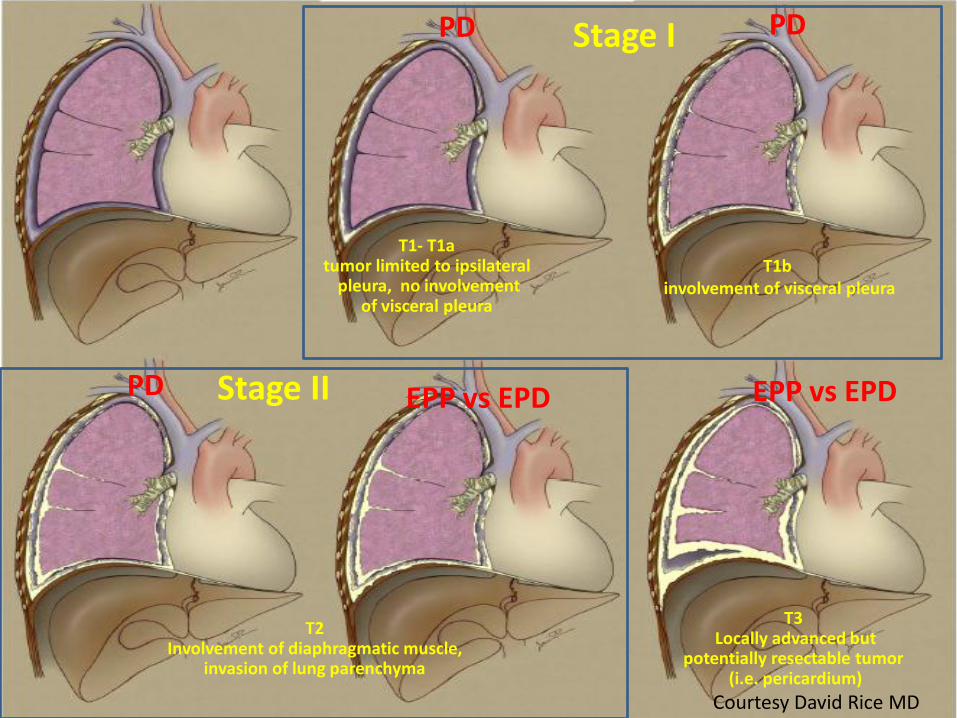
What are the evolving thoughts regarding the approach to the potentially
cytoreducible mesothelioma patient?
T1- T1a tumor limited to ipsilateral
pleura, no involvement of visceral pleura
T2 Involvement of diaphragmatic muscle,
invasion of lung parenchyma
T1b involvement of visceral pleura
T3 Locally advanced but
potentially resectable tumor (i.e. pericardium)
EPP vs EPD PD
PD PD Stage I
Stage II
Courtesy David Rice MD
EPP vs EPD
What is NOT controversial????
YOU MUST COMBINE SURGERY WITH OTHER MODALITIES
• Chemotherapy either preoperative or postoperative – Documented safety and documented improved
survival
• Radiation Therapy postoperatively and possibly preoperatively – Potentially enhanced “local” control
• Intraoperative Therapy – Heated chemoperfusion
– Photodynamic Therapy
Finally….
• If you have surgery for pleural mesothelioma, you must be followed very closely, usually be CT scans
– At this time, there aren’t any good blood tests to really monitor the disease besides SMRP, but stay tuned.
• Use all the resources at your disposal to hear about mesothelioma centers and novel experimental approaches
– The MesoFoundation is a great resource for this





























